DERMOID CYSTS OF THE MESENTERY by Piermarini,12 Sommer ...
6
DERMOID CYSTS OF THE MESENTERY GROVER C. PENBERTHY, M.D., AND KNEALE M. BROWNSQN, M.D. DETROIT, MICH. DERMOID cysts of the mesentery are the rarest of all mesenteric tumors. While the latter are in themselves a rarity, a review of the literature reveals that there have been approximately 500 cases reported since the sixteenth cen- tury when Benivieni first described what is thought to have been a mesenteric tumor. Of these approximate 500 cases there have been less than a score of proved dermoid cysts of the mesentery reported. Cornils,'4 in I920, reported eight cases of mesenteric cysts whiclh he thought were true dermoids. The content of these tumors, however, was a fat-like substance, no hair or other ectodermal derivatives being found. On microscopic examination only an occasional area of what appeared to be plate-like epithelium was found. These findings cast considerable doubt upon the possibility of these cysts having been of dermoid nature. Forster,"5 in I92I, collected i6 cases from the literature, six of which (those of Eppinger, Spencer and Well, Koenig, Langhan, Schutzer and Marie) were undoubtedly true dermoids. The other ten fall under the same shadow of doubt as do those of Cornils. Montgomery and Morest'0 reviewed the literature in I934 and found seven cases reported by Piermarini,12 Sommer, Cortella,13 Ugelli,7 and Judd and Fulcher.11 They also include one of Cornils' cases, bringing the previous number to eight. To this number they also add one observed by themselves. Of the two cases reported by Judd and Fulcher one was found to contain sebaceous-like debris but no ectodermal structures could be found on microscopic examina- tion of its wall. If we can exclude the eight cases reported by Cornils, there remains a total of but I4 cases of proved dermoid cysts of the mesentery in the literature to the present date. The report of the fifteenth case is appended: Case Report.-Hosp. No. CI787: F. McC., colored female, age two, was admitted to the Children's Hospital of Michigan March 8, I937, with a history of having been perfectly well until three days previously when she rather suddenly experienced abdom- inal distress which was located definitely to the right side. At that time the mother first detected a mass in the right side of the abdomen. At the onset of the illness the temperature was thought to be elevated and the child soon became nauseated and vomited repeatedly. A cathartic was administered the following day which resulted in one or two evacuations after 24 hours; the abdominal distress and vomiting, however, had persisted to the time of admission. Physical Examination revealed an intelligent, well-developed, colored girl apparently acutely ill. Other than for some dehydration and the abdominal findings, the general physical examination was essentially negative. There was moderate abdominal distension but no definite step-ladder effect, there were no visible peristalsis or masses apparent. On palpation, however, a mass could be made out in the right lower quadrant, which extended into the flank and as far medially as the midline. The tumor was tender, Submitted for publication October 28, 1937. 566
Transcript of DERMOID CYSTS OF THE MESENTERY by Piermarini,12 Sommer ...

DERMOID CYSTS OF THE MESENTERYGROVER C. PENBERTHY, M.D., AND KNEALE M. BROWNSQN, M.D.
DETROIT, MICH.
DERMOID cysts of the mesentery are the rarest of all mesenteric tumors.While the latter are in themselves a rarity, a review of the literature revealsthat there have been approximately 500 cases reported since the sixteenth cen-tury when Benivieni first described what is thought to have been a mesenterictumor. Of these approximate 500 cases there have been less than a scoreof proved dermoid cysts of the mesentery reported. Cornils,'4 in I920,reported eight cases of mesenteric cysts whiclh he thought were true dermoids.The content of these tumors, however, was a fat-like substance, no hair orother ectodermal derivatives being found. On microscopic examination onlyan occasional area of what appeared to be plate-like epithelium was found.These findings cast considerable doubt upon the possibility of these cystshaving been of dermoid nature. Forster,"5 in I92I, collected i6 cases fromthe literature, six of which (those of Eppinger, Spencer and Well, Koenig,Langhan, Schutzer and Marie) were undoubtedly true dermoids. The otherten fall under the same shadow of doubt as do those of Cornils. Montgomeryand Morest'0 reviewed the literature in I934 and found seven cases reportedby Piermarini,12 Sommer, Cortella,13 Ugelli,7 and Judd and Fulcher.11 Theyalso include one of Cornils' cases, bringing the previous number to eight.To this number they also add one observed by themselves. Of the twocases reported by Judd and Fulcher one was found to contain sebaceous-likedebris but no ectodermal structures could be found on microscopic examina-tion of its wall. If we can exclude the eight cases reported by Cornils, thereremains a total of but I4 cases of proved dermoid cysts of the mesentery inthe literature to the present date. The report of the fifteenth case is appended:
Case Report.-Hosp. No. CI787: F. McC., colored female, age two, was admittedto the Children's Hospital of Michigan March 8, I937, with a history of having beenperfectly well until three days previously when she rather suddenly experienced abdom-inal distress which was located definitely to the right side. At that time the motherfirst detected a mass in the right side of the abdomen. At the onset of the illnessthe temperature was thought to be elevated and the child soon became nauseated andvomited repeatedly. A cathartic was administered the following day which resultedin one or two evacuations after 24 hours; the abdominal distress and vomiting, however,had persisted to the time of admission.
Physical Examination revealed an intelligent, well-developed, colored girl apparentlyacutely ill. Other than for some dehydration and the abdominal findings, the generalphysical examination was essentially negative. There was moderate abdominal distensionbut no definite step-ladder effect, there were no visible peristalsis or masses apparent.On palpation, however, a mass could be made out in the right lower quadrant, whichextended into the flank and as far medially as the midline. The tumor was tender,
Submitted for publication October 28, 1937.566

Volume 107 DERMOID CYSTS OF THE MESENTERYNumber 4
smooth and nonmovable. It could be readily felt by rectal examination. The left sideof the abdomen was tympanitic throughout, but the right side was dull. A scoutroentgenogram of the abdomen at this time revealed the right side of the abdominalcavity to be obscured by the mass which had pushed the bowel upward and to the left.
LABORATORY DATA.-Temperature was IOO.60 F.; leukocytes, I3.500; 54 per cent poly-morphonuclears and 46 per cent lymphocytes. Uranalysis was negative. Blood non-protein nitrogen, I9.8 mg.; urea 6.3 mg.
The patient was treated for a low grade intestinal obstruction and respondedwell. There was considerable conjecture, however, as to the exact nature of theobstructing lesion.
Subsequent Preoperative Couirse.-On the day following admission intravenouspyelography was undertaken, which revealed a normal outline of the kidney pelves
tf~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~J _.....N
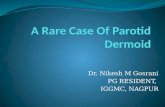
FIG. i.-Anteroposterior roentgenogram of FIG. 2.-Lateral roentgenogram of retro-a right retroperitoneal air injection showing the peritoneal space as outlined by air injection. Thenormal right kidney well outlined by air. The normal right kidney may be seen well demarcatedround shadow in the midline below represents in the upper portion of the space with the darkthe cyst. shadow below representing the cyst.
without distortion of the kidney shadows. It was then felt that the mass was notrelated to the kidney, but some doubt was still present relative to the possibility ofits being intraperitoneal. During the next few days the child continued to have dailyelevations of temperature to 1000 F., and to complain of persistent abdominal distress.On March i6, I937, she was taken home against advice, but was returned two dayslater because of recurrence of the abdominal pain and repeated vomiting. On MarchI9, I937, a retroperitoneal air injection was carried out, which resulted in an excellentoutlining of the retroperitoneal space (Figs. iand 2). This definitely revealed themass to have no relationship to the kidney and to lie anterior to the retroperitoneal space.The tumor also appeared to be smaller at this time and was movable within a shortradius.
Operation.-March 20, I937: Under ether anesthesia, an exploratory celiotomy wasperformed through a right rectus incision. A mass the size of a small grapefruit(Fig. 3) was found lying in the right lower quadrant. It arose from the mesenteryof the lower ileum by a thick, short pedicle which appeared to have been twisted andto have undergone partial necrosis. The tumor encroached upon the ileum and was
567

PENBERTHY AND BROWNSON Annalsof Surgery
adherent to it by recent adhesions. Simple excision of the tumor was effected by ligatingthe pedicle and breaking down the adhesions between it and the bowel. After removalof the mass the small rent in the mesentery at the base of the pedicle was repaired.The postoperative course was essentially uneventful and the child was discharged onthe tenth postoperative day.
Follow-Up.-The patient has remained well to the present time. Gastro-intestinalroentgenologic studies, made June 28, 1937, showed: "No evidence of abnormality incontour or position of the stomach or of any loops of the small bowel; at four hoursthe head of the column was in the transverse colon; after 24 hours only a trace ofbarium remained in the rectum. The colon was empty, and there was no apparentdisplacement of its various segments."
mauig twIn n hal by tre inhs(Fg4 t wa opne ontesd
A.~ ~~ ~~ ~~ ~~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
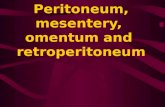
FIG. 3.-Drawing showing the relative size, position and anatomic relations of themesenteric dermoid.
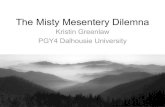
Pathologic Examiiiation.-Gross: The tumor consisted of a tensely fluctuant massmeasuring two and one-half by three inches ( Fig. 4) . It was opened on the sideopposite the attachment of the pedicle, and was found to contain approximately 200 cc.of relatively fresh blood. The wall of the cystic portion measured one-third centimeterin thickness but at the pedicle this increased to one and one-half centimeters. It wason sectioning this region that hair and sebaceous material were found.
Microscopic Examination. "The larger cystic areas are lined by stratified squamousepithelium, and the secondary skin characteristics are present. There are hair folliclesand sweat glands present; in other sections, there are smaller areas which appear to belined by columnar epithelium, about these areas mucous glands are seen, and two piecesof cartilage, similar to that seen about the bronchi, were encountered. There was aconsiderable amount of adipose issue; in the connective tissue trabeculae there werelarge numbers of thin-walled blood vessels; extravasated red blood cells were seen inthe connective tissue. In some areas, the extravasation of these cells was so greatthat this tissue was necrotic." Diagnosis: Dermoid cyst of the mesentery.
DIsCUSSION.-It seems most probable that the pedicle of this small dermoidbecame twisted, resulting in increased venous pressure within the thin-walled
568

Volume 107 DERMOID CYSTS OF THE MESENTERYNumber 4
vessels in the walls of the cysts, which resulted in a hemorrhage into oneof them with the production of a large tumor mass which, in itself, was re-sponsible for the incomplete intestinal obstruction. It is possible that hadthe patient not been operated upon at this time the mass might have recededto its former size. However, further twisting of the pedicle might have pro-duced even greater increase in size with more complete intestinal obstructionor even rupture of the cyst.
........
FIG. 4.-Photograph of the gross specimen of the mesenteric dermoid removed.
It is interesting to theorize upon the etiology of mesenteric dermoids.It is generally accepted that dermoids located elsewhere, in regions wherethey are more commonly observed, have their origin in ectodermal inclusionsduring closure of embryonal plates or fissures, or at the point of union ofectodermal and other structures. While this theory is quite adequate toexplain those arising near the sites of union of embryonic fissures, such asthe orbital region, branchial clefts and in the midline of the trunk, it does notseem adequate to explain those arising in the mesentery. It would seemmore rational to believe that the cells of origin of these dermoids becamesequestrated from their original habitat and wandered into the mesentery,not from the anterior abdominal wall, but from the retroperitoneal regionsduring the process of formation of the mesentery. Dowd,2 and Lexer andTreutinger17 are of the opinion that such cells might have been derived from thewolffian body or the mullerian tube. Ewing16 feels that the majority ofcomplex dermoids are imperfectly developed teratomata, and favors the theoryof origin from sex cells. The exact distinction between teratomata anddermoids has, however, never been satisfactorily made. It seems reasonable to
569

PENBERTHY AND BROWNSON Annals of SurgeryApril, 1938
believe that a gradation of embryonal tumors exists, and that the type oftumor which develops depends upon the potentialities of its original cell.Were this cell totipotent, a complex teratoma would result; were it multi-potent, the result would be a dermoid, and were it unipotent, a simple tumorsuch as a myoma, fibroma or lipoma, would result. The correct solution ofthis problem has not as yet been arrived at.
The symptoms and signs of dermoids of the mesentery do not differ inany respects from those occasioned by other mesenteric tumors. There are nocardinal symptoms, all complaints resulting from purely mechanical disturb-ances. A gradually enlarging abdominal tumor may be noted, or its suddenappearance, as in the case cited, may first attract attention to the abdomen.The onset may be ushered in with intestinal obstruction of any degree.Severe pain is rare, being usually seen only in those cases having a pedicleof sufficient length to permit torsion. The signs are those of an abdominaltumor mass, which, however, may be overshadowed by any one of the possiblecomplications, the most frequent of which is intestinal obstruction. Othersare volvulus, intussusception, adhesions and, perhaps most rare, hemorrhagefrom one of the thin-walled vessels into the mesentery or the peritonealcavity.
An exact diagnosis can be made only after celiotomy and subsequentmicroscopic examination of the cyst wall.
Treatment is entirely surgical. Simple enucleation, if possible, is themethod of choice. If the tumor is of such size that its enucleation would em-barrass the blood supply to the intestine, resection becomes necessary. Mar-supialization, occasionally employed in the treatment of serous cysts of themesentery, has never been undertaken in the treatment of mesenteric dermoids.
Prognosis following excision of the tumor is good. Recurrence, theo-retically, is purely local and should carry no greater incidence than fordermoid tumors elsewhere in the body. There is no history of recurrencein any of the reported cases of proved dermoid cysts of the mesentery.
SUMMARY.-(I). A case of dermoid cyst of the mesentery treated by ex-cision with recovery is reported, bringing the total number in the literatureto I5.
(2). The patient, a girl, age two, is the youngest subject reported havingsuch a tumor.
(3). The rarity of mesenteric dermoids is emphasized.(4). The origin of these tumors is briefly discussed.
BIBLIOGRAPHY'Bowers, L. G.: Tumors of the Mesentery. ANNALS OF SURGERY, 44, 892, I906.' Dowd, C. N.: Mesenteric Cysts. ANNALS OF SURGERY, 32, 515, 1900.'Meyer, K., and Shapiro, P.: Dermoid Cyst of Lesser Omental Bursa. Am. Jour. Surg.,
27, 55I, March, 1935.'Steel, W. A.: Mesenteric Cyst as Cause of Intestinal Obstruction. Brit. Jour. Surg.,
21, I04, July, 1935.'Kendall, A. W.: Mesenteric Tumour. Brit. Jour. Surg., 23, 86o, April, 1936.
570

Volume 107 DERMOID CYSTS OF THE MESENTERYNumber 4
'Phillips, H. A.: Spindle Celled Mesenteric Tumours. Brit. Jour. Surg., 2I, 637, April,'934.
'Ugelli, Libero: Due Casi di cisti dermoidi det mesentere. Policlinico, 40, 1534, I933.'Judd, E. S., and Crisp, W. W.: Primary Tumors of Mesentery. Proc. Staff Meeting
Mayo Clinic, 7, 555, September, I1932.9Rankin, F. W., and Major, S. G.: Tumors of Mesentery. Surg., Gynec. and Obst.,
55, 244, May, I932.Montgomery, J. G., and Morest, F. S.: Dermoid Cysts of the Mesentery. J. MissouriM. A., December, I934.
"Judd, E. S., and Fulcher, 0. H.: Dermoid Cysts of the Abdomen. Surg. Clin. N. Amer.,I3, 835, August, I933.
"Piermarini, Giuseppe: Cisti dermoidi del mesentere. Riforma med., 41, I224, No-vember 21, I925.
3Cortella, Emilio: Cisti dermoidi del mesentere. Policlinico, 39, 2I7, February 8, 1932.1Cornils: Uber Dermoidcysten des Mesenteriums. Deutsche Zeitschrift fur Chirurgie,
3153, 399, 1920.15 Forster, E.: Ueber genuine Cysten des Mesenteriums. Beitrage zur klinischen Chi-
rurgie, I24, ii6, 192I.'Ewing, J.: Neoplastic Diseases, Third edition. Philadelphia, W. B. Saunders Co.,
1934.' Treutinger, J.: Dermoid im Netz bei kaiderseitegen dermoiden der Eierstocke. Arch.
f. Gynak., I55, 595, I934.1 Fisher, W. H.: Mesenteric Tumors. Am. Jour. Surg., 7, 803, 1929.
571