DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS · DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS ......
25
Transcript of DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS · DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS ......

1
DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS
Amendments to Chapter 12-15
Hawaii Administrative Rules
Workers’ Compensation
Relating to Medical Fee Schedule
August 23, 2017
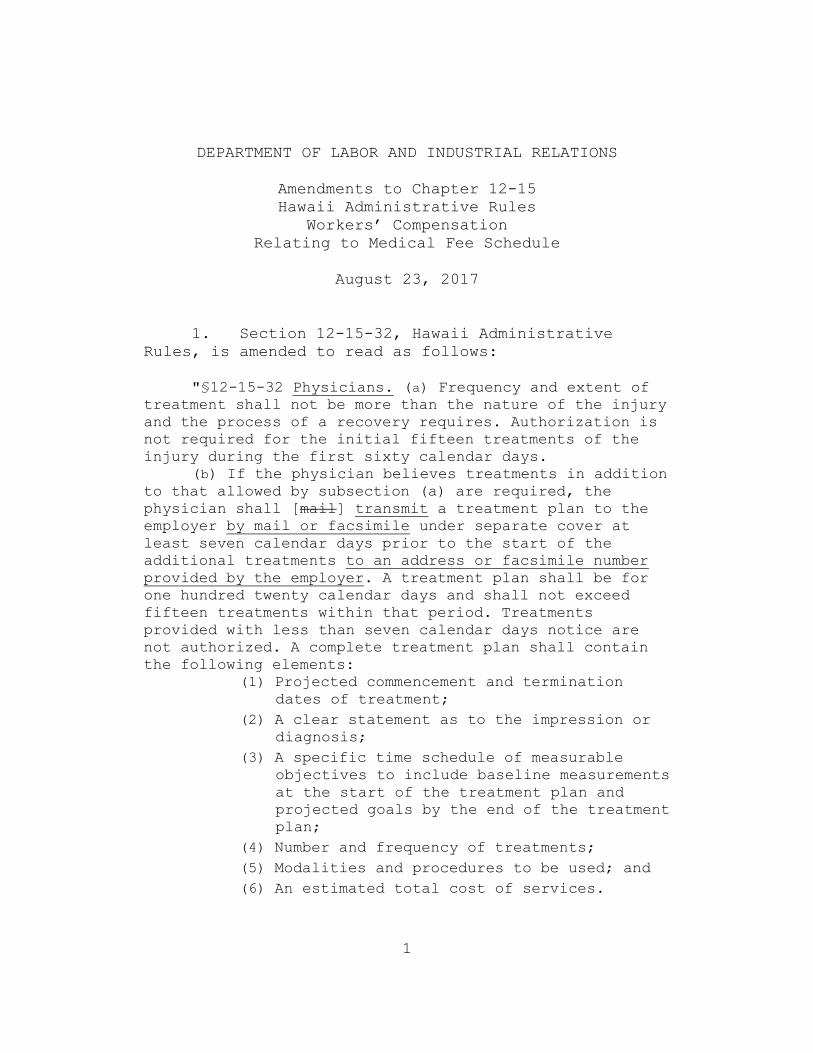
1. Section 12-15-32, Hawaii Administrative
Rules, is amended to read as follows:
"§12-15-32 Physicians. (a) Frequency and extent of
treatment shall not be more than the nature of the injury
and the process of a recovery requires. Authorization is
not required for the initial fifteen treatments of the
injury during the first sixty calendar days.
(b) If the physician believes treatments in addition
to that allowed by subsection (a) are required, the
physician shall [mail] transmit a treatment plan to the
employer by mail or facsimile under separate cover at
least seven calendar days prior to the start of the
additional treatments to an address or facsimile number
provided by the employer. A treatment plan shall be for
one hundred twenty calendar days and shall not exceed
fifteen treatments within that period. Treatments
provided with less than seven calendar days notice are
not authorized. A complete treatment plan shall contain
the following elements:
(1) Projected commencement and termination
dates of treatment;
(2) A clear statement as to the impression or
diagnosis;
(3) A specific time schedule of measurable
objectives to include baseline measurements
at the start of the treatment plan and
projected goals by the end of the treatment
plan;
(4) Number and frequency of treatments;
(5) Modalities and procedures to be used; and
(6) An estimated total cost of services.

2
Treatment plans which do not include the above specified
elements but which are reasonable and necessary may not
be denied by the employer, but upon written notification
from the employer, the physician shall correct the
deficiency(s) and the employer’s liability is deferred as
long as the treatment plan remains deficient. Neither the
injured employee nor the employer shall be liable for
services provided under a treatment plan that remains
deficient. Both the front page of the treatment plan and
the envelope in which the plan is mailed or the cover
sheet if the plan is sent by facsimile shall be clearly
identified as a “WORKERS’ COMPENSATION TREATMENT PLAN” in
capital letters and in no less than ten point type.
(c) A treatment plan shall be deemed received by an
employer when the plan is sent by mail or facsimile with
reasonable evidence showing that the treatment plan was
received.
[(c)](d) The employer may file an objection to the
treatment plan with documentary evidence supporting the
denial and a copy of the denied treatment plan with the
director, copying the physician and the injured employee.
Both the front page of the denial and the envelope in
which the denial is filed shall be clearly identified as
a “TREATMENT PLAN DENIAL” in capital letters and in no
less than ten point type. The employer shall be
responsible for payment for treatments provided under a
complete treatment plan until the date the objection is
filed with the director. Furthermore, the employer’s
objection letter must explicitly state that if the
attending physician or the injured employee does not
agree with the denial, they may request a review by the
director of the employer’s denial within fourteen
calendar days after postmark of the employer’s denial,
and failure to do so shall be construed as acceptance of
the employer’s denial.
[(d)](e) The attending physician or the injured
employee may request in writing that the director review
the employer’s denial of the treatment plan. The request
for review shall be filed with the director, copying the
employer, within fourteen calendar days after postmark of
the employer’s denial. A copy of the denied treatment
plan shall be submitted with the request for review. Both
the front page of the request for review and the envelope
in which the request is filed shall be clearly identified

3
as a “REQUEST FOR REVIEW OF TREATMENT PLAN DENIAL” in
capital letters and in no less than ten point type. For
cases not under the jurisdiction of the director at the
time of the request, the injured employee shall be
responsible to have the case remanded to the director’s
jurisdiction. Failure to file a request for review of the
employer’s denial with the director within fourteen
calendar days after postmark of the employer’s denial
shall be deemed acceptance of the employer’s denial.
[(e)](f) The director shall issue a decision, after
a hearing, either requiring the employer to pay the
physician within thirty-one calendar days in accordance
with the medical fee schedule if the treatments are
determined to be reasonable and necessary or disallowing
the fees for treatments determined to be unreasonable or
unnecessary. Disallowed fees shall not be charged to the
injured employee.
[(f)](g) The decision issued pursuant to subsection
[(e)](f) shall be final unless appealed pursuant to
section 386-87, HRS. The appeal shall not stay the
director’s decision.
[(g)](h) The psychiatric evaluation or psychological
testing with the resultant reports shall be limited to
four hours unless the physician submits prior
documentation indicating the necessity for more time and
receives pre-authorization from the employer. Fees shall
be calculated on an hourly basis as allowed under
Medicare.
[(h)](i) For physical medicine, treatments may
include up to four procedures, up to four modalities, or
a combination of up to four procedures and modalities,
and the visit shall not exceed sixty minutes per injury.
When treating more than one injury, treatments may
include up to six procedures, up to six modalities, or a
combination of up to six procedures and modalities, and
the entire visit shall not exceed ninety minutes.
[(i)](j) Any physician who exceeds the treatment
guidelines without proper authorization shall not be
compensated for the unauthorized services.
[(j)](k) No compensation shall be allowed for
preparing treatment plans and written justification for
treatments which exceed the guidelines.
4
[(k)](l) Failure to comply with the requirements in
this section may result in denial of fees.
[(l)](m) Treatment, prescribed on an in-patient
basis in a licensed acute care hospital where the injured
employee’s level of care is medically appropriate for an
acute setting as determined by community standards, are
excluded from the frequency of treatment guidelines
specified herein." [Eff 1/1/96; am 1/1/97; am
] (Auth: HRS §§386-21, 386-21.2, 386-26, 386-72) (Imp:
HRS §§386-21, 386-21.2, 386-26, 386-27)
2. Section 12-15-34, Hawaii Administrative
Rules, is amended to read as follows:
"§12-15-34 Providers of service other than
physicians. (a) Frequency and extent of treatment shall
not be more than the nature of the injury and the process
of a recovery require. Any health care treatment or
service performed by a Hawaii licensed or certified
provider of service other than a physician shall be
directed by the attending physician based on a written
prescription signed, dated, and approved by the attending
physician. The prescription may authorize up to an
initial fifteen treatments of the injury during the first
sixty calendar days. For therapists, the prescription may
authorize up to an initial twenty treatments of the
injury during the first sixty calendar days.
(b) If the attending physician believes treatments
in addition to that allowed by subsection (a) are
required, the provider of service other than a physician,
in lieu of the attending physician, may [mail] transmit a
treatment plan for review and approval to the attending
physician who shall, after approval, [mail] transmit the
treatment plan to the employer by mail or facsimile under
separate cover at least seven calendar days prior to the
start of the additional treatments to an address or
facsimile number provided by the employer. A treatment
plan shall be for one hundred twenty calendar days and
shall not exceed fifteen treatments within that period.
Treatments provided with less than seven calendar days
notice are not authorized. A complete treatment plan
shall contain the following elements:

5
(1) Projected commencement and termination
dates of treatment;
(2) A clear statement as to the impression or
diagnosis;
(3) A specific time schedule of measurable
objectives to include baseline measurements
at the start of the treatment plan and
projected goals by the end of the treatment
plan;
(4) Number and frequency of treatments;
(5) Modalities and procedures to be used; and
Treatment plans which do not include the above specified
elements but which are reasonable and necessary may not
be denied by the employer, but upon written notification
from the employer, the physician or the provider of
service, with approval by the attending physician, shall
correct the deficiency(s) and the employer’s liability is
deferred as long as the treatment plan remains deficient.
Neither the injured employee nor the employer shall be
liable for services provided under a treatment plan that
remains deficient. Both the front page of the treatment
plan and the envelope in which the plan is mailed or the
cover sheet if the plan is sent by facsimile shall be
clearly identified as a “WORKERS’ COMPENSATION TREATMENT
PLAN” in capital letters and in no less than ten point
type.
(c) A treatment plan shall be deemed received by an
employer when the plan is sent by mail or facsimile with
reasonable evidence showing that the treatment plan was
received.
[(c)](d) The employer may file an objection to the
treatment plan with documentary evidence supporting the
denial and a copy of the denied treatment plan with the
director, copying the attending physician, the provider
of service and the injured employee. Both the front page
of the denial and the envelope in which the denial is
filed shall be clearly identified as a “TREATMENT PLAN
DENIAL” in capital letters and in no less than ten point
type. The employer shall be responsible for payment for
treatments provided under a complete treatment plan until
the date the objection is filed with the director.
Furthermore, the employer’s objection letter must
explicitly state that if the attending physician or the

6
injured employee does not agree with the denial, they may
request a review by the director of the employer’s denial
within fourteen calendar days after postmark of the
employer’s denial, and failure to do so shall be
construed as acceptance of the employer’s denial.
[(d)](e) The attending physician or the injured
employee may request in writing that the director review
the employer’s denial of the treatment plan. The request
for review shall be filed with the director, copying the
employer, within fourteen calendar days after postmark of
the employer’s denial. A copy of the denied treatment
plan shall be submitted with the request for review. Both
the front page of the request for review and the envelope
in which the request is filed shall be clearly identified
as a “REQUEST FOR REVIEW OF TREATMENT PLAN DENIAL” in
capital letters and in no less than ten point type. For
cases not under the jurisdiction of the director at the
time of the request, the injured employee shall be
responsible to have the case remanded to the director’s
jurisdiction. Failure to file a request for review of the
employer’s denial with the director within fourteen
calendar days after postmark of the employer’s denial
shall be deemed acceptance of the employer’s denial.
[(e)](f) The director shall issue a decision, after
a hearing, either requiring the employer to pay the
provider of service other than a physician within thirty-
one calendar days in accordance with the medical fee
schedule if the treatments are determined to be
reasonable and necessary or disallowing the fees for
treatments determined to be unreasonable or unnecessary.
Disallowed fees shall not be charged to the injured
employee.
[(f)](g) The decision issued pursuant to subsection
[(e)](f) shall be final unless appealed pursuant to
section 386-87, HRS. The appeal shall not stay the
director’s decision.
[(g)](h) The provider of service other than a
physician shall submit reports at least monthly to the
attending physician and employer regarding an injured
employee’s progress. The preparation and submission of
written reports or progress notes to the employer by the
provider of service other than a physician are an
integral part of the service fee.

7
[(h)](i) Treatments may include up to four
procedures, up to four modalities, or a combination of up
to four procedures and modalities, and the visit shall
not exceed sixty minutes per injury. When treating more
than one injury, treatments may include up to six
procedures, up to six modalities, or a combination of up
to six procedures and modalities, and the entire visit
shall not exceed ninety minutes. This section applies to
providers of service other than physicians including
physical therapists, occupational therapists, massage
therapists, and acupuncturists.
[(i)](j) Any provider of service other than a
physician who exceeds the treatment guidelines without
proper authorization shall not be compensated for the
unauthorized services.
[(j)](k) No compensation shall be allowed for
preparing treatment plans and written justification for
treatments which exceed the guidelines.
[(k)](l) Failure to comply with the requirements in
this section may result in denial of fees.
[(l)](m) Therapy by physical therapists and
occupational therapists, prescribed on an in-patient
basis in a licensed acute care hospital where the injured
employee’s level of care is medically appropriate for an
acute setting as determined by community standards or,
prescribed on an out-patient post-surgery basis not to
exceed thirty calendar days, are excluded from the
frequency of treatment guidelines specified herein."
[Eff 1/1/96; am 1/1/97; am ] (Auth:
HRS §§386-21, 386-21.2, 386-26, 386-72) (Imp: HRS §§386-
21, 386-21.2, 386-26, 386-27)
3. Section 12-15-90, Hawaii Administrative
Rules, is amended to read as follows:
“§12-15-90 Workers’ compensation medical fee
schedule. (a) Charges for medical services shall not
exceed one hundred ten per cent of participating fees
prescribed in the Medicare Resource Based Relative
Value Scale System fee schedule (Medicare Fee
Schedule) applicable to Hawaii or listed in exhibit A,
located at the end of this chapter and made a part of
this chapter, entitled “Workers’ Compensation
8
Supplemental Medical Fee Schedule”, dated [January 1,
2014] January 1, 2018. The Medicare Fee Schedule in
effect on January 1, 1995 shall be applicable through
June 30, 1996. Beginning July 1, 1996 and each
calendar year thereafter, the Medicare Fee Schedule in
effect as of January 1 of that year shall be the
effective fee schedule for that calendar year.
(b) If maximum allowable fees for medical
services are listed in both the Medicare Fee Schedule
and the Workers’ Compensation Supplemental Medical Fee
Schedule, dated [January 1, 2014] January 1, 2018,
located at the end of this chapter as exhibit A,
charges shall not exceed the maximum allowable fees
allowed under the Workers’ Compensation Supplemental
Medical Fee Schedule, dated [January 1, 2014]
January 1, 2018, located at the end of this chapter as
exhibit A.
(c) If the charges are not listed in the
Medicare Fee Schedule or in the Workers’ Compensation
Supplemental Medical Fee Schedule, dated [January 1,
2014] January 1, 2018, located at the end of this
chapter as exhibit A, the provider of service shall
charge a fee not to exceed the lowest fee received by
the provider of service for the same service rendered
to private patients. Upon request by the director or
the employer, a provider of service shall submit a
statement to the requesting party, itemizing the
lowest fee received for the same health care,
services, and supplies furnished to any private
patient during the one-year period preceding the date
of a particular charge. Requests shall be submitted
in writing within twenty calendar days of receipt of a
questionable charge. The provider of service shall
reply in writing within thirty-one calendar days of
receipt of the request. Failure to comply with the
request of the employer or the director shall be
reason for the employer or the director to deny
payment.
(d) Fees listed in the Medicare Fee Schedule
shall be subject to the current Medicare Fee Schedule
bundling and global rules if not specifically
addressed in these rules. The Health Care Financing
9
Administration Common Procedure Coding System (HCPCS)
alphabet codes adopted by Medicare will not be
allowed, except for injections and durable medical
equipment, unless specifically adopted by the
director. The director may defer to a fee listed in
the Medicare HCPCS Fee Schedule when a fee is not
listed in the Workers’ Compensation Supplemental
Medical Fee Schedule, Exhibit A.
(e) Providers of service will be allowed to add
the applicable Hawaii general excise tax to their
billing.” [Eff 1/1/96; am 1/1/97; am 11/22/97;
am 12/17/01; am 12/13/04; am 11/6/06; am 12/14/07; am
2/28/11; am 12/30/13; am ] (Auth:
HRS §§386-21, 386-26, 386-72) (Imp: HRS §§386-21,
386-26)

10
4. Material, except source notes, to be
repealed is bracketed. New material is underscored.
5. Additions to update source notes to reflect
these amendments are not underscored.
6. These amendments to Title 12, Chapter 15,
Hawaii Administrative Rules, relating to the Hawaii
Workersꞌ Compensation Medical Fee Schedule shall take
effect ten days after filing with the Office of the
Lieutenant Governor.
I certify that the foregoing are copies of the
rules drafted in the Ramseyer format, pursuant to the
requirements of section 91-4.1, Hawaii Revised
Statutes, which were adopted on (date to be inserted
upon adoption) and filed with the Office of the
Lieutenant Governor.
____________________________
Director
APPROVED AS TO FORM:
__________________________
Deputy Attorney General

CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-1
EXHIBIT A
Chapters 12-15Hawaii Administrative Rules
WORKERS’ COMPENSATION SUPPLEMENTALMEDICAL FEE SCHEDULE
January 1, 2018
The codes in the Workers’ Compensation Supplemental Medical Fee Schedule are obtained fromthe American Medical Association, the American Dental Association or the State Department ofLabor and Industrial Relations.
The five character codes included in the Workers’ Compensation Supplemental Medical FeeSchedule are obtained from 2017 Current Procedural Terminology (CPT®), copyright 2016 by theAmerican Medical Association (AMA). CPT is developed by the AMA as a listing of descriptiveterms and five character identifying codes and modifiers for reporting medical services andprocedures performed by physicians.
The responsibility for the content of the Workers’ Compensation Supplemental Medical FeeSchedule is with DLIR and no endorsement by the AMA is intended or should be implied. TheAMA disclaims responsibility for any consequences or liability attributable or related to any use,nonuse or interpretation of information contained in the Workers’ Compensation SupplementalMedical Fee Schedule. Fee schedules, relative value units, conversion factors and/or relatedcomponents are not assigned by the AMA, are not part of CPT, and the AMA is not recommendingtheir use. The AMA does not directly or indirectly practice medicine or dispense medical services.The AMA assumes no liability for data contained or not contained herein. Any use of CPT outsideof the Workers’ Compensation Supplemental Medical Fee Schedule should refer to the most currentCPT codes and descriptive terms. Applicable FARS/DFARS apply.
CPT is a registered trademark of the American Medical Association
The five character codes starting with the letter “D” included in the Workers’ CompensationSupplemental Medical Fee Schedule are obtained from Current Dental Terminology 2017,copyright 2016 by the American Dental Association (ADA). CDT is developed by the ADA toachieve uniformity, consistency and accurate reporting of dental treatment.

CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-2
TABLE OF CONTENTS
TITLE CODES PAGESURGERY
Integumentary System 10060-17004 A-4Musculoskeletal System 20520-29916 A-4Respiratory System 31231-32551 A-6Cardiovascular System 35206-36620 A-6Digestive System 45378-49653 A-6Urinary System 51700, 51798 A-6Male Genital System 55520 A-6Female Genital System 57288 A-6Maternity Care and Delivery 59025 A-6Nervous System 62270-64856 A-6Eye and Ocular Adnexa 65205-68815 A-7Auditory System 69200, 69210 A-7Operating Microscope 69990 A-7
RADIOLOGYDiagnostic Radiology (Diagnostic Imaging) 70030-76377 A-7Diagnostic Ultrasound 76512-76942 A-8Radiologic Guidance 77001, 77012 A-8Bone/Joint Studies 77073, 77080 A-8Radiation Oncology 77290-77336 A-8Nuclear Medicine 78104-78806 A-8
MEDICINEVaccines, Toxoids 90636-90746 A-9Psychiatry 90791-90847 A-9Biofeedback 90901 A-9Gastroenterology 91035, 91110 A-9Ophthalmology 92002-92310 A-9Special Otorhinolaryngologic Services 92507-92611 A-9Cardiovascular 93000-93351 A-9Noninvasive Vascular Diagnostic Studies 93926-93976 A-10Pulmonary 94010-94762 A-10Neurology and Neuromuscular Procedures 95805-95972 A-10Central Nervous System Assessments/Tests 96101 A-10Health and Behavior Assessment/Intervention 96150, 96152 A-10Hydration, Therapeutic, Prophylactic, Diagnostic
Injections and Infusions, and Chemotherapy andOther Highly Complex Drug or Highly ComplexBiologic Agent Administration 96360-96376 A-10
Physical Medicine and Rehabilitation 97010-97760 A-10Acupuncture 97810-97814 A-10Chiropractic Manipulative Treatment 98940 A-10Special Services, Procedures and Reports 99000-99053 A-11Qualifying Circumstances for Anesthesia 99100 A-11Other Services and Procedures 99173, 99183 A-11
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-3
TITLE CODES PAGEDENTAL SERVICES
Diagnostic D0120-D0470 A-11Preventive D1110 A-11Restorative D2160-D2954 A-11Endodontics D3310 A-11Periodontics D4211 A-11Prosthodontics, Removable D5110-D5820 A-11Implant Services D6010-D6104 A-11Prosthodontics, Fixed D6240-D6750 A-11Oral and Maxillofacial Surgery D7140-D7953 A-12Adjunctive General Services D9110-D9942 A-12
EVALUATION AND MANAGEMENTOffice or Other Outpatient Services 99201-99215 A-12Hospital Inpatient Services 99232 A-12Consultations 99241-99255 A-12Emergency Department Services 99281-99285 A-12Critical Care Services 99292 A-12Case Management Services 99366-99368 A-12Preventive Medicine Services 99395, 99408 A-12Non-Face-to-Face Services 99441-99443 A-12Special Evaluation and Management Services 99456A, 99456B A-13

CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-4
SURGERY
Integumentary System
Maximum Maximum MaximumCode Fee Code Fee Code Fee
10060 $157.6410061 $275.0310120 $207.9510121 $389.0611000 $77.1411001 $30.1911010 $704.3411043 $311.9211044 $435.7111055 $61.9311056 $74.4711601 $280.4811602 $309.4811719 $17.8511730 $144.2211740 $73.7911750 $335.4011760 $315.2812001 $177.2512002 $188.5512004 $214.6612005 $268.32
12007 $362.2312011 $189.7012013 $209.9012014 $234.7812015 $285.0912031 $365.5912032 $486.3312034 $472.9112035 $550.0612041 $352.1712042 $456.1412044 $533.2912051 $385.7112052 $432.6712053 $526.5812054 $566.8313100 $446.0813101 $603.7213121 $630.5513122 $167.7013131 $513.1613132 $818.38
13133 $231.4313151 $613.7813152 $791.5413153 $254.9013160 $980.0114040 $1,120.2415004 $478.2615050 $675.4815100 $1,021.3815101 $223.2715120 $1,136.5815240 $1,119.9715260 $1,428.8015738 $1,716.0616000 $93.9116020 $114.0416025 $201.2416030 $244.8417003 $11.5717004 $190.91
Musculoskeletal System
20520 $275.0320525 $741.2320526 $90.5620550 $80.5020551 $80.5020552 $73.7920553 $83.8520600 $77.1420605 $90.5620610 $103.9720612 $73.7920900 $653.3320902 $611.9120924 $647.6720926 $522.8620930 $230.3020931 $132.3720936 $212.9620937 $228.0721310 $177.7621320 $402.4821360 $673.0421365 $1,369.0521390 $989.2721395 $1,232.63
21407 $804.0321408 $1,105.8021423 $981.3021470 $1,492.0522551 $2,623.2522552 $575.1722554 $1,846.2422558 $2,143.2122585 $480.1722600 $1,612.6722612 $2,015.7522614 $523.2222630 $1,947.7822632 $380.0722633 $2,224.8022634 $589.9522830 $988.3822840 $975.6522842 $1,076.6322845 $1,072.2722849 $1,565.0122850 $879.7122852 $843.5122856 $1,961.7923120 $722.81
23130 $771.7223350 $181.1223405 $765.1423410 $1,204.0923412 $1,203.4223420 $1,425.4523430 $1,056.5123440 $924.0823455 $1,428.8023500 $274.6623552 $805.5923570 $288.4223620 $327.1423650 $415.9023655 $586.9523700 $241.7424149 $1,445.4024305 $712.8224340 $755.2424341 $1,113.5324342 $1,044.4724343 $896.2224344 $1,337.4024357 $607.0724358 $707.69

Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-5
24359 $882.1024366 $836.0224515 $1,075.7524600 $496.3924605 $707.6924665 $807.1124666 $933.5324685 $807.8225000 $494.6325024 $950.4425105 $598.1025111 $440.3425118 $501.8225240 $532.0025246 $204.8025260 $910.3325270 $734.9225272 $816.4325290 $541.3925295 $648.4925310 $765.8325320 $1,221.8925337 $1,101.2925390 $946.9525400 $985.6225405 $1,268.4625440 $945.8625447 $1,021.8125505 $768.0725545 $841.6425605 $828.4425606 $819.2625607 $922.9725608 $1,094.2725609 $1,327.4725628 $925.7425645 $728.4925825 $969.3126020 $539.7126035 $1,052.6426055 $788.1926075 $405.1726080 $486.9226105 $415.2626110 $402.1526115 $705.0126145 $634.3426320 $439.7326340 $432.6726350 $1,026.3226356 $1,703.8326410 $811.6726418 $831.7926426 $768.1626433 $664.4326440 $780.7426445 $730.0026480 $943.7926525 $820.0826540 $942.47
26541 $990.8426548 $964.8726560 $724.9226567 $843.4126600 $409.1926605 $390.0926608 $604.4226686 $766.5726720 $292.0326725 $466.2126727 $670.8026735 $868.6926742 $440.8626750 $258.2626756 $521.8726765 $684.2226770 $368.9426860 $709.9826951 $812.4226952 $802.2427096 $308.5727130 $2,049.2927216 $1,306.3027227 $2,020.0127228 $2,290.9727235 $1,161.2027236 $1,460.7927245 $1,843.4327248 $972.9527350 $801.0927370 $200.5427380 $754.0027385 $811.6727403 $786.0227405 $860.7827427 $872.9627446 $1,412.6927447 $2,190.1627457 $1,154.9927486 $1,715.4727487 $2,259.1827506 $1,891.6627524 $1,069.9327530 $482.7227535 $1,157.1327536 $1,452.5427560 $435.2427570 $198.8227603 $741.2327625 $713.9427640 $1,021.3827650 $972.6627652 $931.7927658 $463.5127675 $605.3327680 $562.2027687 $562.3827691 $923.0827695 $591.5027698 $842.56
27724 $1,536.8927750 $422.9027758 $1,091.9227759 $1,301.3527760 $400.9627766 $812.3827786 $383.9527792 $932.4127810 $572.2127814 $1,116.8827823 $1,279.5627827 $1,436.5627828 $1,677.5427840 $455.4527842 $608.2227870 $1,260.5328002 $562.9428008 $534.8128090 $583.3328122 $769.7928222 $628.8628238 $818.8828300 $801.6428400 $303.9428415 $1,382.8828445 $1,423.6728475 $318.4928485 $623.8428510 $154.6028725 $960.1828730 $905.2729065 $140.8729075 $127.4529105 $127.4529125 $100.6229130 $60.3729200 $37.7629240 $35.8429260 $35.8829280 $36.1029405 $120.7429425 $124.1029445 $168.0129515 $103.9729520 $39.6829530 $35.8429540 $32.2729550 $23.8029580 $64.0329581 $82.8829584 $93.2429700 $78.9729806 $1,509.3029807 $1,472.4129820 $707.6929821 $778.1329822 $751.3029823 $895.5229824 $859.1429825 $747.56

Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-6
29826 $297.0029827 $1,517.7229828 $1,304.7129835 $620.5529837 $647.0729838 $754.4729844 $636.2429846 $665.8529848 $644.7829862 $996.5129867 $1,623.86
29873 $686.8829874 $700.1329875 $670.7529876 $832.9229877 $885.4629879 $942.4729880 $960.0129881 $896.8529882 $929.5229884 $788.0229887 $910.84
29888 $1,401.9729891 $829.7929897 $620.4129898 $746.8529905 $837.8629906 $853.6529914 $1,219.8729915 $1,243.1429916 $1,244.58
Respiratory System
31231 $295.1531240 $195.12
31570 $408.3231575 $139.42
32551 $187.59
Cardiovascular System
35206 $930.9935207 $962.3836245 $1,676.0036246 $1,063.21
36247 $1,969.1336410 $23.7636415 $4.3436430 $46.91
36569 $321.5836600 $40.2536620 $60.85
Digestive System
45378 $516.2349505 $670.3849507 $704.1149520 $774.5849560 $884.14
49568 $315.2649585 $545.8049587 $574.6849650 $528.3649651 $672.45
49652 $891.8449653 $1,111.71
Urinary System
51700 $93.90 51798 $25.86
Male Genital System
55520 $550.26
Female Genital System
57288 $869.84
Maternity Care and Delivery
59025 $59.78
Nervous System
62270 $202.8662362 $469.4062368 $70.7662369 $154.9562370 $162.3663030 $1,368.4363035 $271.6763042 $1,654.9863045 $1,545.83
63047 $1,560.2463048 $301.6363075 $1,949.9463655 $1,002.5863663 $997.1963685 $446.5063688 $453.2664405 $129.3864415 $146.81
64421 $189.6064445 $164.7964450 $147.5864455 $59.0064479 $299.2264480 $142.3664483 $345.4664484 $187.8264491 $113.76
Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
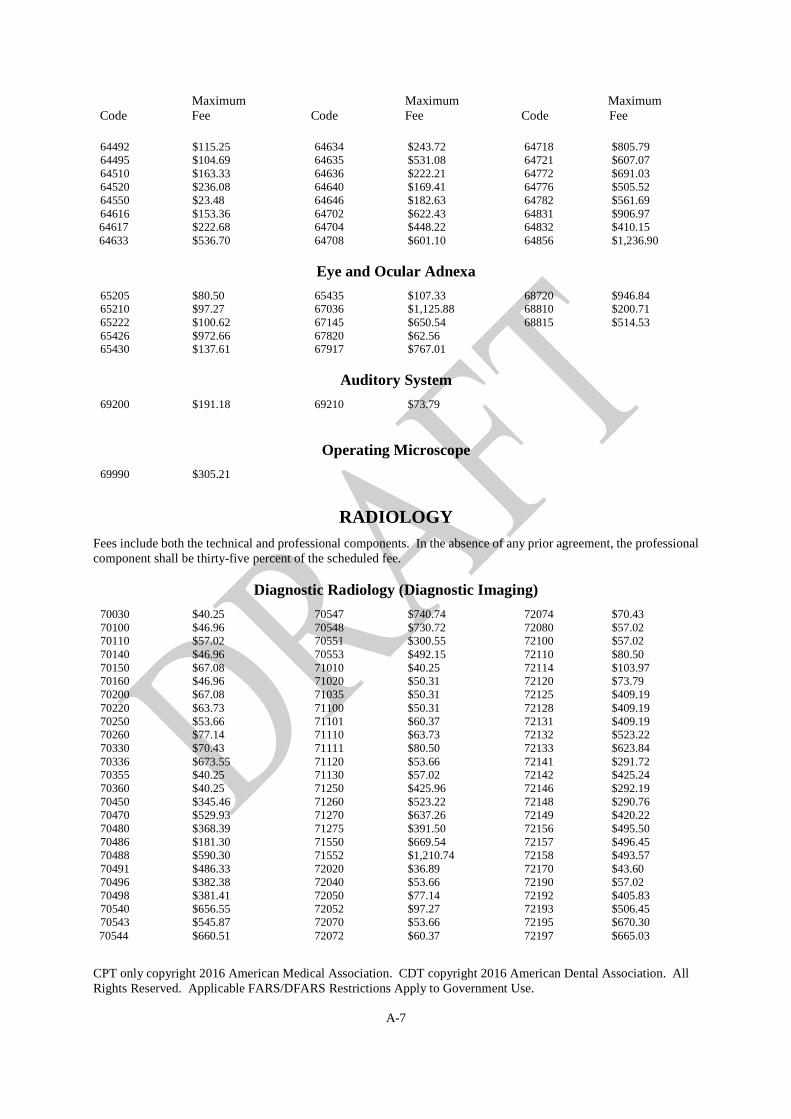
A-7
64492 $115.2564495 $104.6964510 $163.3364520 $236.0864550 $23.4864616 $153.3664617 $222.6864633 $536.70
64634 $243.7264635 $531.0864636 $222.2164640 $169.4164646 $182.6364702 $622.4364704 $448.2264708 $601.10
64718 $805.7964721 $607.0764772 $691.0364776 $505.5264782 $561.6964831 $906.9764832 $410.1564856 $1,236.90
Eye and Ocular Adnexa
65205 $80.5065210 $97.2765222 $100.6265426 $972.6665430 $137.61
65435 $107.3367036 $1,125.8867145 $650.5467820 $62.5667917 $767.01
68720 $946.8468810 $200.7168815 $514.53
Auditory System
69200 $191.18 69210 $73.79
Operating Microscope
69990 $305.21
RADIOLOGY
Fees include both the technical and professional components. In the absence of any prior agreement, the professionalcomponent shall be thirty-five percent of the scheduled fee.
Diagnostic Radiology (Diagnostic Imaging)
70030 $40.2570100 $46.9670110 $57.0270140 $46.9670150 $67.0870160 $46.9670200 $67.0870220 $63.7370250 $53.6670260 $77.1470330 $70.4370336 $673.5570355 $40.2570360 $40.2570450 $345.4670470 $529.9370480 $368.3970486 $181.3070488 $590.3070491 $486.3370496 $382.3870498 $381.4170540 $656.5570543 $545.8770544 $660.51
70547 $740.7470548 $730.7270551 $300.5570553 $492.1571010 $40.2571020 $50.3171035 $50.3171100 $50.3171101 $60.3771110 $63.7371111 $80.5071120 $53.6671130 $57.0271250 $425.9671260 $523.2271270 $637.2671275 $391.5071550 $669.5471552 $1,210.7472020 $36.8972040 $53.6672050 $77.1472052 $97.2772070 $53.6672072 $60.37
72074 $70.4372080 $57.0272100 $57.0272110 $80.5072114 $103.9772120 $73.7972125 $409.1972128 $409.1972131 $409.1972132 $523.2272133 $623.8472141 $291.7272142 $425.2472146 $292.1972148 $290.7672149 $420.2272156 $495.5072157 $496.4572158 $493.5772170 $43.6072190 $57.0272192 $405.8372193 $506.4572195 $670.3072197 $665.03

Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-8
72200 $43.6072202 $53.6672220 $46.9672265 $264.9772275 $171.0572295 $385.7173000 $43.6073010 $43.6073020 $36.8973030 $46.9673040 $167.7073050 $54.0873060 $46.9673070 $40.5173080 $50.3173090 $43.6073100 $43.6073110 $50.3173115 $147.5873120 $40.2573130 $46.9673200 $382.3673201 $479.6273218 $656.66
73220 $658.2873221 $309.7673222 $497.7373223 $618.1073525 $157.6473560 $43.6073562 $50.3173564 $57.0273565 $44.9773580 $194.5373590 $43.6073600 $40.2573610 $46.9673620 $40.2573630 $46.9673650 $40.2573660 $40.2573700 $382.3673701 $479.6273706 $465.1673718 $567.9973720 $661.6373721 $309.2873722 $502.05
73723 $618.5974000 $43.6074020 $60.3774022 $70.4374150 $405.8374160 $533.2974175 $400.5974176 $258.2874178 $461.8374181 $669.8974183 $666.4675635 $849.8975710 $643.9775716 $677.5175736 $643.9775774 $560.1276000 $62.3676001 $211.3076100 $118.8976376 $29.8776377 $90.31
Diagnostic Ultrasound
76512 $164.5576513 $150.9376514 $19.0676519 $122.7176700 $197.8976705 $147.5876770 $187.82
76775 $150.9376801 $160.5876815 $110.5476817 $126.9276856 $167.7076857 $61.4976870 $167.70
76881 $151.1076882 $43.4976937 $40.2476942 $76.68
Radiologic Guidance
77001 $110.55 77012 $158.81
Bone/Joint Studies
77073 $45.95 77080 $53.78
Radiation Oncology
77290 $674.15 77334 $264.97 77336 $140.87
Nuclear Medicine
78104 $348.8278122 $258.2678300 $234.78
78305 $318.6378306 $355.5278320 $415.90
78452 $646.2978805 $271.6778806 $496.39

Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-9
MEDICINE
Fees include both the technical and professional components. In the absence of any prior agreement, the professionalcomponent shall be thirty-five percent of the scheduled fee.
Vaccines, Toxoids
90636 $99.0790714 $21.90
90715 $46.9690732 $86.62
90746 $63.32
Psychiatry
90791 $154.6890792 $173.7390832 $84.86
90834 $99.6990837 $167.7490846 $126.80
90847 $151.70
Biofeedback
90901 $53.27
Gastroenterology
91035 $626.61 91110 $1,217.70
Ophthalmology
92002 $110.6892004 $201.2492012 $110.6892014 $160.9992015 $23.5092020 $42.4292025 $48.21
92071 $45.4392082 $62.5792083 $83.4692132 $39.7592133 $47.7392134 $52.2192136 $115.85
92225 $34.4492235 $169.7292250 $86.0192284 $82.7192285 $27.4792286 $49.1792310 $78.69
Special Otorhinolaryngologic Services
92507 $97.3792511 $144.5192526 $106.6892541 $69.7492542 $67.0892545 $50.3992547 $23.4892548 $140.87
92550 $25.2492551 $13.5292557 $63.4092567 $26.8392570 $38.4292577 $29.6092587 $69.4392588 $96.86
92590 $74.9492591 $99.1192592 $35.5192595 $51.3392610 $106.7192611 $107.45
Cardiovascular
93000 $33.4593005 $20.1293010 $11.2193015 $135.8293016 $26.8693017 $83.8593018 $20.12
93040 $16.8493042 $10.0693224 $187.9693225 $57.0293226 $93.9193280 $73.1993282 $79.37
93289 $82.2893306 $298.7993308 $137.1593325 $80.5093351 $353.39
Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
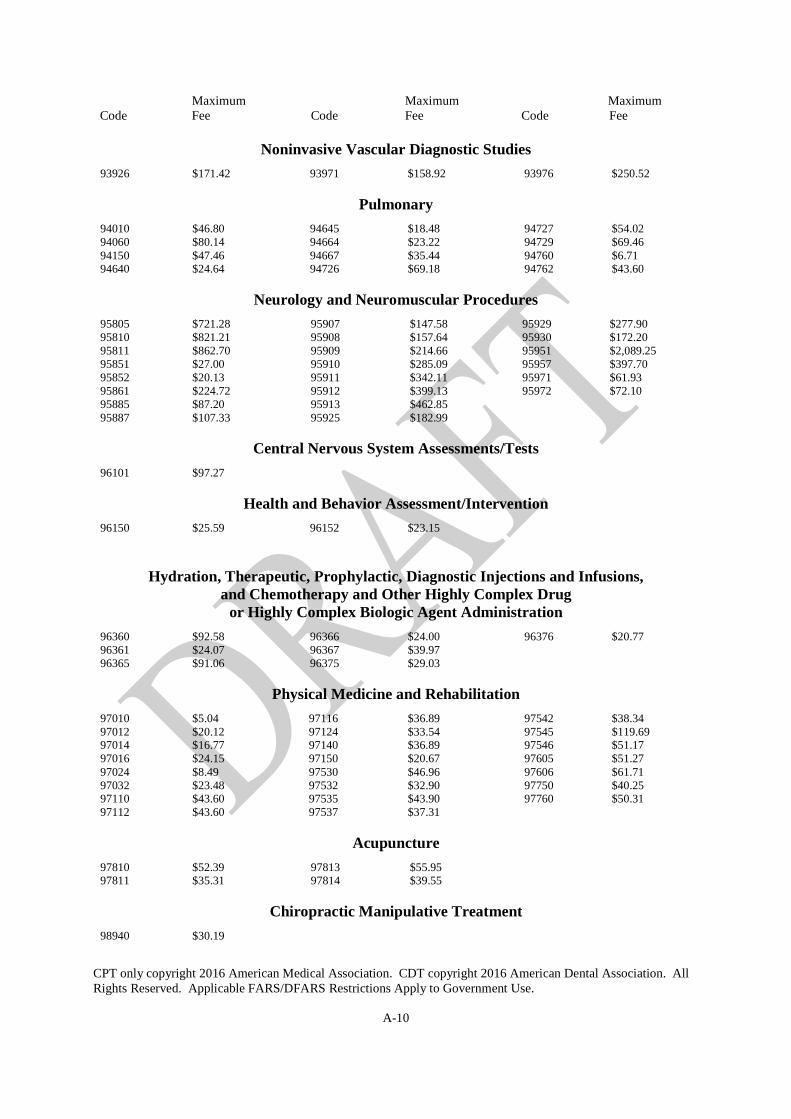
A-10
Noninvasive Vascular Diagnostic Studies
93926 $171.42 93971 $158.92 93976 $250.52
Pulmonary
94010 $46.8094060 $80.1494150 $47.4694640 $24.64
94645 $18.4894664 $23.2294667 $35.4494726 $69.18
94727 $54.0294729 $69.4694760 $6.7194762 $43.60
Neurology and Neuromuscular Procedures
95805 $721.2895810 $821.2195811 $862.7095851 $27.0095852 $20.1395861 $224.7295885 $87.2095887 $107.33
95907 $147.5895908 $157.6495909 $214.6695910 $285.0995911 $342.1195912 $399.1395913 $462.8595925 $182.99
95929 $277.9095930 $172.2095951 $2,089.2595957 $397.7095971 $61.9395972 $72.10
Central Nervous System Assessments/Tests
96101 $97.27
Health and Behavior Assessment/Intervention
96150 $25.59 96152 $23.15
Hydration, Therapeutic, Prophylactic, Diagnostic Injections and Infusions,and Chemotherapy and Other Highly Complex Drug
or Highly Complex Biologic Agent Administration
96360 $92.5896361 $24.0796365 $91.06
96366 $24.0096367 $39.9796375 $29.03
96376 $20.77
Physical Medicine and Rehabilitation
97010 $5.0497012 $20.1297014 $16.7797016 $24.1597024 $8.4997032 $23.4897110 $43.6097112 $43.60
97116 $36.8997124 $33.5497140 $36.8997150 $20.6797530 $46.9697532 $32.9097535 $43.9097537 $37.31
97542 $38.3497545 $119.6997546 $51.1797605 $51.2797606 $61.7197750 $40.2597760 $50.31
Acupuncture
97810 $52.3997811 $35.31
97813 $55.9597814 $39.55
Chiropractic Manipulative Treatment
98940 $30.19
Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
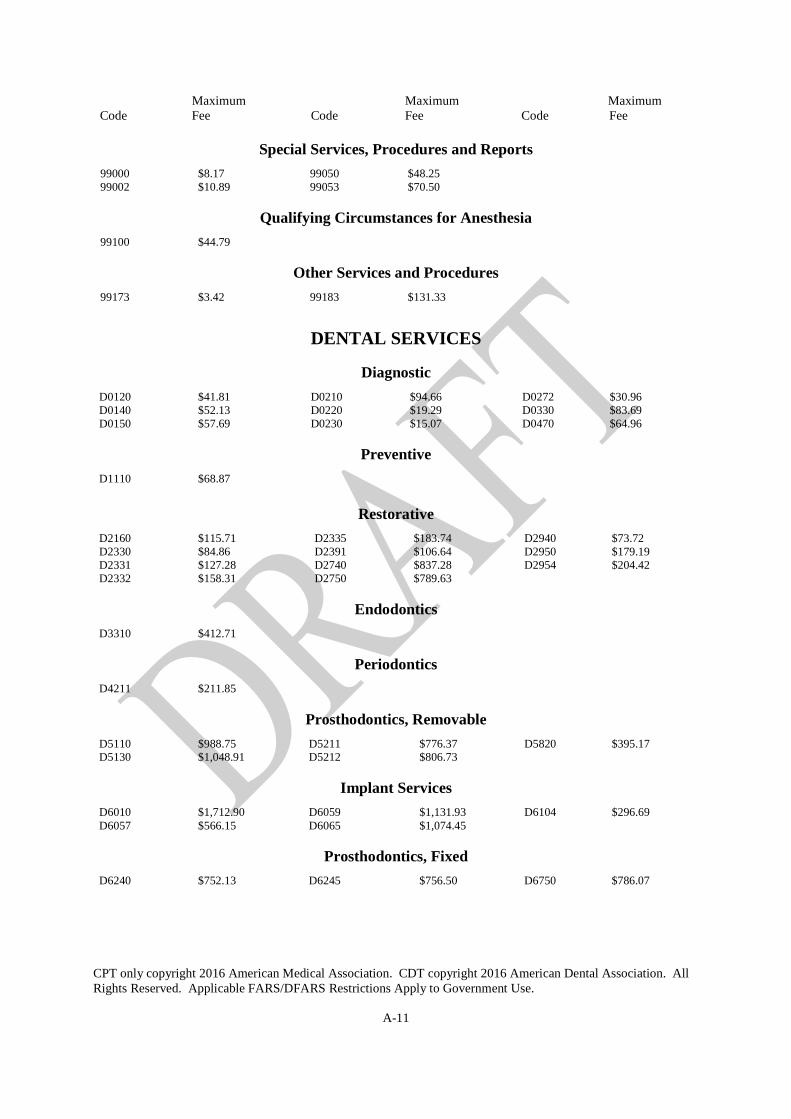
A-11
Special Services, Procedures and Reports
99000 $8.1799002 $10.89
99050 $48.2599053 $70.50
Qualifying Circumstances for Anesthesia
99100 $44.79
Other Services and Procedures
99173 $3.42 99183 $131.33
DENTAL SERVICES
Diagnostic
D0120 $41.81D0140 $52.13D0150 $57.69
D0210 $94.66D0220 $19.29D0230 $15.07
D0272 $30.96D0330 $83.69D0470 $64.96
Preventive
D1110 $68.87
Restorative
D2160 $115.71D2330 $84.86D2331 $127.28D2332 $158.31
D2335 $183.74D2391 $106.64D2740 $837.28D2750 $789.63
D2940 $73.72D2950 $179.19D2954 $204.42
Endodontics
D3310 $412.71
Periodontics
D4211 $211.85
Prosthodontics, Removable
D5110 $988.75D5130 $1,048.91
D5211 $776.37D5212 $806.73
D5820 $395.17
Implant Services
D6010 $1,712.90D6057 $566.15
D6059 $1,131.93D6065 $1,074.45
D6104 $296.69
Prosthodontics, Fixed
D6240 $752.13 D6245 $756.50 D6750 $786.07
Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
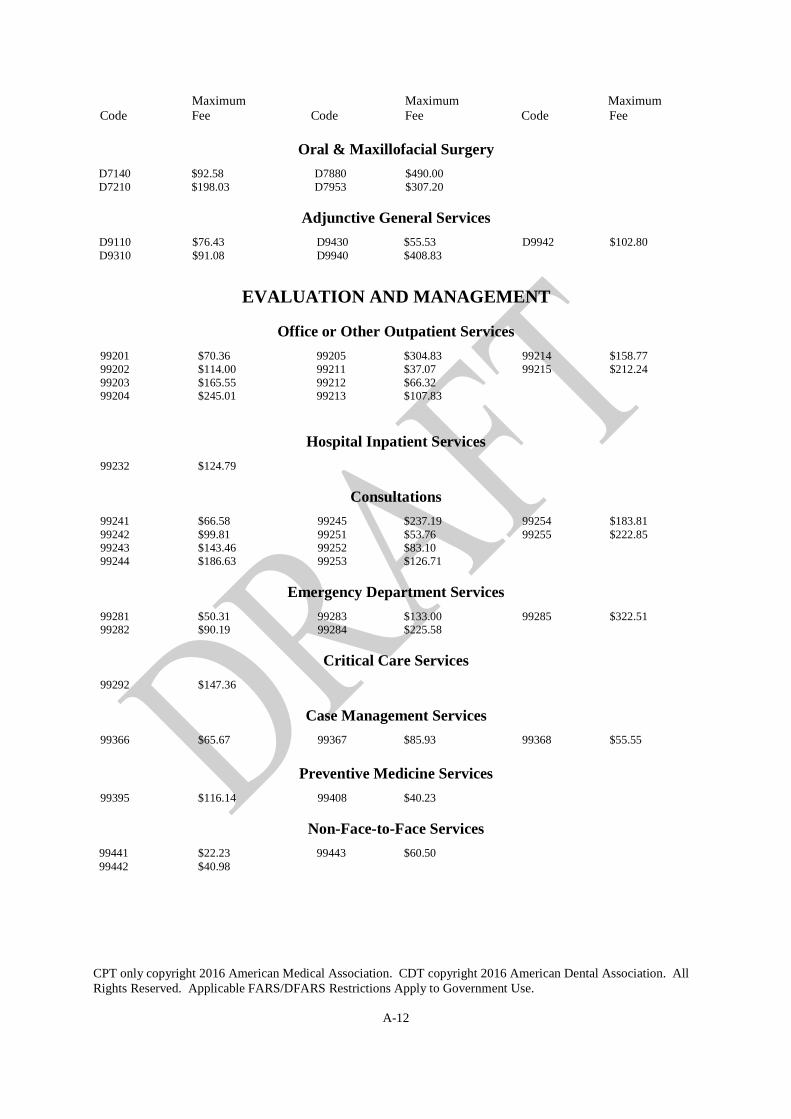
A-12
Oral & Maxillofacial Surgery
D7140 $92.58D7210 $198.03
D7880 $490.00D7953 $307.20
Adjunctive General Services
D9110 $76.43D9310 $91.08
D9430 $55.53D9940 $408.83
D9942 $102.80
EVALUATION AND MANAGEMENT
Office or Other Outpatient Services
99201 $70.3699202 $114.0099203 $165.5599204 $245.01
99205 $304.8399211 $37.0799212 $66.3299213 $107.83
99214 $158.7799215 $212.24
Hospital Inpatient Services
99232 $124.79
Consultations
99241 $66.5899242 $99.8199243 $143.4699244 $186.63
99245 $237.1999251 $53.7699252 $83.1099253 $126.71
99254 $183.8199255 $222.85
Emergency Department Services
99281 $50.3199282 $90.19
99283 $133.0099284 $225.58
99285 $322.51
Critical Care Services
99292 $147.36
Case Management Services
99366 $65.67 99367 $85.93 99368 $55.55
Preventive Medicine Services
99395 $116.14 99408 $40.23
Non-Face-to-Face Services
99441 $22.2399442 $40.98
99443 $60.50

Maximum Maximum MaximumCode Fee Code Fee Code Fee
CPT only copyright 2016 American Medical Association. CDT copyright 2016 American Dental Association. AllRights Reserved. Applicable FARS/DFARS Restrictions Apply to Government Use.
A-13
Special Evaluation and Management ServicesMaximum
Code Description Fee99456A* Complex consultation pursuant to Section 386-79, HRS - work related or medical disability
examination by other than the treating physician that includes: completion of a medical history commensurate with the patient’s condition; performance of an examination commensurate with the patient’s condition; formulation of a diagnosis, assessment of capabilities and stability, and calculation of
impairment; development of future medical treatment plan; completion of necessary documentation/certificates and report; and review of records relating to the patient’s condition.First hour ................................................................................................................................................... $207.25
99456B* Each additional 30 minute increment (an increment must be at least 30 minutes.) ............................. $103.63
*Department of Labor Code
Bundled Services: Certain codes, such as telephone calls, are considered by the Health Care Financing Administration (HCFA) tobe “bundled” services. Bundled services are not payable, nor should they be billed, when performed incidentto or in conjunction with another service even if the other service is performed on a different day. Whenservices that are designated as bundled are denied, the physician may not collect from the patient.