Advances in Dental Ceramics / orthodontic courses by Indian dental academy
Upload
anamika-thakur-ranaCategory
view
1.044download
7
Seminar -3
DENTAL CERAMICS DENTAL CERAMICS
CONTENT
Introduction History Structure Classification Composition Properties Strengthening of dental porcelain Condensation of dental porcelain Firing procedure Stages of maturity Metal -ceramic All ceramics Application of ceramics Conclusion References
INTRODUCTION :
Man has been obsessed with duplicating, restoring and replacing various lost body parts like the limbs, ear, nose and eyes with artificial prosthesis and teeth being no exception.
The quest for an artificial prosthesis similar to the natural tooth, both in function and aesthetics, in the oral environment still remains as a foremost concern to the dentist, which has led to the use of CERAMICS in dentist.
WHAT ARE CERAMICS?
The term ceramic is derived from the Greek word “keramos,” which means “potter” or “pottery.” This is related to a Sanskrit term meaning “burned earth,” because the basic components were clays from the earth that were heated to form pottery.1
Ceramic is an inorganic compound with non-metallic properties typically composed of metallic (or semi metallic) and non-metallic elements (example AI2O3, CaO)
- Kenneth J. Anusavice
1

Seminar -3
Dental ceramic is an inorganic compound with non-metallic properties typically consisting of oxygen and one or more metallic or semi metallic elements (e.g. Al, Ca, Li, Mg, K, Si, Na, Sn, Ti and Zr) that is formulated to produce the whole or part of a ceramic based dental prosthesis.
HISTORICAL EVOLUTION OF CERAMICS :
Till 18th Century dental technologie remian undeveloped .The candidate material for artificial teeth during these days were : Human teeth Animal teeth that were carved to size and shape of human teeth but they were
unstable towards coorosive agents in saliva Ivory : elephant ivory and bone contained pores which got stained easily.2
The current dental ceramics are far from the early ceramics that started being used over 200 years ago.Early records of the first ceramics used as dental materials date back to 1774, when french apothecary alexis duchateau and parisian dentist Nicholas dubois De Cheamnat manufactured the first complete ceramic denture.
Nicholas dubois De Cheamnat
The initial use of ceramics materials in dentistry was in the obtention of complete dentures.Early in the 19th century, Italian dentist Giuseppangelo Fonzi manufactured individual ceramic teeth attached to a metallic substructure which, in turn ,was attached to complete dentures.
2

Seminar -3
Giuseppangelo Fonzi
The restoration of individual ceramic teeth in the oral cavity was delayed until the late 1800s, when Logan constructed ceramic teeth fused to the metallic post so that these posts could function as an intra radicular for the restoration.During last 40 years ,research has foccused on improving metal free systems and developing superior materials regarding esthetics and clinical performances to offer patients several alternatives to restore missing or damaged teeth.3
1958 first dental porcelain for veneering was introduced, which led to the wide spread use of metal –ceramic restoration in the 1960s and beyond, followed by invention of the porcelain jacket crown that was popularized in hte 1960s by Mclean.1970 saw the advent of the early experiments in CAD/CAM crown fabrication, followed by an influx of ceramic based restoration systems from 1980s through to the present day1
STRUCTURE:
The structure of ceramic material is dictated by the type of atoms present, the type of bonding between the atoms and the way atoms are packed together.
The atoms in ceramic materials are held together by a chemical bond and two most common bonds for ceramics are ionic bond(occurs between a metal and nonmetal and involves the attraction of opposite charges when electrons are transferred from the metal to the nonmetal); and covalent occurs between two nonmetals and involves sharing of atoms. The bonding of atoms together is much stronger in covalent and ionic than in metallic bonding. Because of this, metals are ductile and ceramics are brittle.
3

Seminar -3
Many dental ceramics contains a crystal phase and a glass phase based on silica structure. This structure is characterized by a silica tetrahedran in which a Si4+ cations is positioned at the center of a tetrahedran with O- anions at each of the four corners.
The resulting structure is not closely packed and has both covalent and ionic characteristics.
The regular dental porcelain, being glassy in nature, is largely non crystalline, and exhibits only short range order in atomic arrangement, which is referred to as dental glass ceramics. The only true crystalline ceramic used at present in restorative dentistry is alumina (Al2O3), which is hardest and strongest oxide known.4
CLASSIFICATION :
1. Based on chemical composition2. According to type3. According to use4. According to firing température5. According to firing technique
4

Seminar -3
6. According to substrate metal7. Microstructural classification8. Processing technique
1. BASED ON COMPOSITION:
A) SILICATE CERAMICS:
Characterized by an amorphous glass phase with porous structure.
The main components are SiO2 with small addition of crystalline Al2O3, MgO, ZrO2 and or other oxides.
Dental porcelain falls in this category.
B) OXIDE CERAMICS:
Contain principal crystalline phase (e.g., Al2O3, MgO, ThO2 or, ZrO2) with either no glass phase or a small content of glass phase.
C) NON OXIDE CERAMICS:
These are impractical for use in dentistry because of high processing temperatures, complex processing methods or unesthetic color and opacity.
D) GLASS CERAMICS:
These are types of ceramics containing a glass matrix phase and atleast one crystal phase.4
2. ACCORDING TO TYPE
a) Feldspathic porcelain b) Leucite reinforced porcelainc) Aluminous porcelain d) Glass infiltrated aluminous e) Glass infiltrated spinellf) Glass ceramics4
3. ACCORDING TO USE
a) Ceramic for artificial teethb) Jacket crown, inlay and onlay ceramic
5

Seminar -3
c) Metal ceramic d) Anterior bridge ceramic
4. ACCORDING TO FIRING TEMPERATURE a) High fusing - >1300 Cb) Medium fusing - 1101 t0 1300Cc) Low fusing - 850-1101Cd) Ultra low fusing - <850C4
5. ACCORDING TO FIRING TECHNIQUE
1. Air fired (at atmospheric pressure)2. Vacuum fired (at reduced pressure)3. Diffusible gas firing
6. ACCORDING TO SUBSTRATE METAL
1. Cast metal2. Sintered metal3. Swaged metal4. Glass ceramics5. CAD/CAM.4
7. METAL CERAMICS (PORCELAIN FUSED TO METAL)METAL FREE CERAMICS (ALL CERAMICS)
8. MICROSTRUCTURAL CLASSIFICATION At a microstructural level, ceramics can be defined by their composition of glass-to-crystalline ratio. There can be infinite variability of the microstructures of materials; however, they can be divided into four basic compositional categories with a few subgroups:a) Composition Category 1:
Glass-based systems (mainly silica)
b) Composition Category 2: Glass-based systems (mainly silica) with fillers, usually crystalline (Typically Leucite or a different high-fusing glass)
c) Composition Category 3: Crystalline-based systems with glass fillers (mainly alumina)
d) Composition Category 4:
6

Seminar -3
Polycrystalline solids (alumina and zirconia)
COMPOSITION CATEGORY 1:
Glass-Based Systems, Amorphous Glass
Best mimic the optical properties of enamel and dentin. Derived from group of mined minerals called feldspar and are based on y silicon
dioxide (also known as silica or quartz), and alumina (aluminium oxide). Aluminosilicates occurs naturally, and contain various quantities of potassium and
sodium, are known as feldspars. Glasses based on feldspar are
Resistance to crystallization(devitrification) Have low firing ranges biocompatible
COMPOSITION CATEGORY 2
Glass-Based Systems with fillers
Filler particles are added to the glass composition to improve mechanical properties. And to control optical effects such as opalescence ,color, and opacity
It is further subdivided into three groups. The glass composition is similar to the pure glass Category 1. The
difference is varying amounts of crystal types have either been added to or grown in the glassy matrix.
The primary crystal types today are leucite, lithium disilicate, or fluorapatite.
Leucite is created in dental porcelain by increasing the K2O (potassium oxide) content of the aluminosilicates glass. This filler was added to create porcelain that could be successfully fired on to the metal substructures.
Lithium disilicate crystals are made by adding Li2O (lithium oxide) to the aluminosilicates glass. It also acts a flux, lowering the melting temperature of the material.
.
Subcategory 2.1Low-to-Moderate Leucite-Containing Feldspathic Glass These materials have been called feldspathic porcelains by default.
Leucite
coefficient of thermal expansion (CTE),
7

Seminar -3
Inhibit crack propagation, thereby improving the material’s strength. The amount of Leucite may be adjusted in the glass based on the type of
core and required CTE
Subcategory 2.2High-Leucite containing glass
Glassy phase is based on an alumino-silicate glass. These materials have been developed in both powder/liquid, machinable, and
pressable forms. The most widely used version is the original iPs empress® (ivoclar Vivadent,
Amherst, ny) but there are several other products in this category. This material is called a glass ceramic, which has had the crystalline phase grown
within the glass matrix by a process called “controlled crystallization of glass.”
Subcategory 2.3Lithium-Disilicate Glass-Ceramics It is a new type of glass ceramic, where the aluminosilicates glass has lithium oxide added.
E.g. IPS Empress II (now called as IPS e.max),
COMPOSITION CATEGORY 3:
Crystalline-based systems with glass fillers cover the wide scope of all-ceramic restorations, including veneers, inlays, onlay, and anterior/posterior crowns and bridges.
E.g In-Ceram Spinell (alumina and magnesia matrix) is the most translucent, with moderately high strength and is used for anterior crowns.
In-Ceram Alumina (alumina matrix) has high strength and moderate translucency and is used for anterior and posterior crowns.
In-Ceram Zirconia (alumina and zirconia matrix) has very high strength and lower translucency and is used primarily for three-unit posterior bridges.
COMPOSITION CATEGORY 4:
Polycrystalline Solids
Have no glassy component; all atoms are densely packed together without any intervening matrix to form a dense, air-free, glass-free polycrystalline structure.
8

Seminar -3
This structure makes difficult to drive crack through atoms compared to atoms in the less dense and irregular network found in glasses.
These are relatively opaque and hence these high strength ceramics are used as substructure material upon which glassy ceramics are veneered to achieve pleasing aesthetics.
Several processing techniques allow the fabrication of either a solid-sintered aluminous oxide (alumina, Al2O3) or zirconium oxide (ZrO2) framework5.
1. CLASSIFICATION BASED ON PROCESSING TECHNIQUE
Ceramics having same composition may be fabricated by different laboratory techniques and each method of forming results in a different distribution of flaws, opportunity for depth translucency and accuracy of fit.
Ceramics can be classified as:
Powder condensation Slip casting Hot pressing Computer aided design / computer aided manufacturing
Powder condensation
This is the traditional method of forming ceramic prosthesis Moist porcelain powder is applied with an artist brush and excess moisture is
removed to compact powder particles together. The porcelain is further compacted by visual flow of the glassy component during
firing under vacuum. This method results in a large amount of residual porosity. The porosity and discontinuous nature of the crystalline phase lead to relatively low
strength and a wide variation in strength. Have greater translucency than can be achieved using other methods [13], so these
materials are usually applied as the esthetic veneer layers on stronger cores and frameworks.
Slip casting
A slip is a low viscosity slurry or mixture of ceramic powder particles suspended in a fluid (usually water).
9

Seminar -3
Slip casting involves forming a mold or negative replica of the desired framework geometry and pouring a slip into the mold
The mold is made of a material (usually gypsum) that extracts some water from the slip into the walls of the mold through capillary action, and some of the powder particles in the slip become compacted against the walls of the mold forming a thin layer of green ceramic that is to become the framework
The remaining slip is discarded, and the framework can be removed from the mold after partial sintering to improve the strength to a point where the framework can support its own weight.
Ceramics fabricated by slip casting can have higher fracture resistance than those produced by powder condensation because the strengthening crystallineParticles form a continuous network throughout the framework.
E.g. glass infiltration (In-Ceram, Vita Zahnfabrik). Limited application is because of complicated series of steps, which provide a
challenge to achieving accurate fit & may result in internal defects that weaken the material from incomplete glass infiltration
The original In-Ceram and some partially stabilized zirconia blocks are fabricated based on slip casting of alumina or zirconia.
Pressable
Lost wax method is used to fabricate molds for pressable dental ceramics. Available from manufacturers as prefabricated ingots made of crystalline particles
distributed throughout a glassy material. Pressable ingots are heated to a temperature at which they become a highly viscous
liquid, and they are slowly pressed into the lost wax mold. Advantage is its good accuracy of fit Used only as core and framework materials. Pressable may be used for inlays, onlay, veneers, and single-unit crowns E.g. IPS e.max ZirPress (Ivoclar-Vivadent)
CAD/CAM
CAD-CAM ceramics are available as prefabricated ingots CAD-CAM ceramics are available as prefabricated ingots6
Composition:
Dental porcelains, to a large extent, are glassy materials.
10

Seminar -3
Glasses are super-cooled liquids / non-crystalline solids with only a short-range order in their atomic arrangement. During cooling, molten glass solidifies with a liquid structure instead of a crystalline structure. Such a structure is called vitreous and the process of forming it is known as vitrification. The principal anion present in all glasses is O2 ion, which forms very stable bonds with small multivalent cations such as silicon, boron, phosphorous etc. (e.g., in silicon glasses, SiO4 tetrahedral are formed which are responsible for the random network of glass). These ions are termed as glass formers.
For dental applications, only two glass forming oxides – silicon oxide and boron oxide are used to develop the principal network.
Additional properties like low fusion temperature, high viscosity, color and resistance to devitrification is obtained by the addition of other oxides like potassium, sodium, calcium, boron or aluminium oxides to the glass forming lattice, SiO4.
HIGH FUSING PORCELAINS
Traditionally, the basic ingredients of these types of porcelains are feldspar kaolin (clay) and quartz. Feldspar is the primary constituent, and all porcelains based on feldspar are referred to as FELDSPATHIC PORCELAINS. Natural feldspars can be either sodium feldspar (albite) or potassium feldspar (orthoclase / microline) which are minerals composed of potash (K2O), Soda (Na2O) Alumina (Al2O3) and silica (SiO2). These are necessary to increase the thermal expansion compatible with metal coping.For dental purposes, light potassium based feldspar is generally selected because of its increased resistance to pyroplastic flow and an increased viscosity. The pyroplastic flow of dental porcelain should be low in order to prevent
rounding of margins, loss of tooth from andObliteration of surface markings.
Feldspars are present in concentrations of 75 to 85% and undergo incongruent melting at temperatures between 1150C and 1530C. Incongruent melting is the process by which one material melts to form a liquid plus a different crystalline material. Hence a glassy phase is formed and suspended inside it are crystalline potassium alumino silicate crystals known as Leucite.KAOLIN / CLAY
11

Seminar -3
Kaolin / clay (Al2O3, 2SiO2, 2H2O) serves as a binder. When mixed with water, it forms a sticky mass, which allows the unfired porcelain to be easily worked and molded. On heating, it reacts limitedly with feldspar (known as pyrochemical reaction) and thereby provides rigidly. It also adheres to the framework of quartz particles and shrinks considerably during firing. Unfortunately, pure kaolin is white in color and reduces the translucency of porcelain. Consequently, it is included only in small concentrations of 4 to 5%.
PURE QUARTZ Pure quartz is used porcelain as a strengthener. The main function of quartz (silica)
is to impart more strength and firmness, and a greater translucency. Silica remains uncharged at the usual firing temperatures and hence contributes stability to the mass during heating by providing a framework for other constituents. It is present in concentrations of 13 to 14%. Traces of iron may be present as impurities in the quartz and must be removed to prevent discoloration of porcelain.
MEDIUM, LOW AN ULTRA LOW FUSING PORCELAINS The low and medium fusing porcelain powders are glasses which have been ground
from blocks of matured porcelain. For this, the raw ingredients are mixed and fused, and the fused mass is the quenched in water. The rapid cooling induces stresses in the glass to the extent that considerable cracks and fractures occur. This process is referred to as FRITTING and the product so obtained is called a frit. The brittle material is then ground to a fine powder of almost colloidal dimensions. During subsequent firing, little or no pyrochemical reaction occurs, but the glass phase softens and flows slightly. This softening allows the powder particles to coalesce together (sintering) and form a dense solid. However, the temperature must be controlled to minimize the pyroplastic flow.The raw ingredients for the low and medium fusing porcelains are basically the same as for the high fusing porcelain powders but in addition contain balancing oxides / fluxes. These additions tend to modify the properties by interrupting the glass network and hence are also known as glass modifiers.7
GLASS MODIFIERS The sintering temperature of silica is too high for use in veneering esthetic layers
bonded to metal substructure; at such high temperature metal will melt. In addition the thermal contraction of coefficient of crystalline silica is too low for the alloys.
Bond between the silica tetrahedral can be broken by addition of alkali metal ion such as Na,K and Ca.
12

Seminar -3
These alkali decreases the amount of cross-linking between the oxygen and the glass forming elements like silica i.e., they disrupt the continuity of the SiO4 network.
These breakage results in Increased fluidity Lower softening temperature Increases thermal expansion
The modifier concentration should not be too high, Because if too many tetrahedral are disrupted, there may occur crystallization
during the porcelain firing operations reduce the chemical durability (resistance to attack by water ,acids and
alkalis) The most commonly used glass modifiers are potassium, sodium and calcium
oxides. These are introduced as carbonates that revert to oxides on heating. Other oxides added lithium oxide, magnesium oxide, phosphorous pentoxide etc8
INTERMEDIATE OXIDES The addition of glass modifiers not only lowers the softening temperature but also
reduces the viscosity of the glass. To overcome this problem intermediate oxides lie aluminium oxide (Al2O3), are
added .7
BORIC OXIDE Boric oxide (B2O3) serves as a glass modifier as well as a glass former. Decreases viscosity Lowers softening temperature Forms own glass network8
OPACIFYING AGENTS The translucency of porcelain can be decreased by using an opacifying agent. An opacifying agent is generally a metal oxide-ground to a very fine particle size of
<5m. Zirconium oxide is the most common opacifiers The difference between the refractive indices of the glass and the opacifiers is the
basic mechanism behind opalescence. Different wavelength of visible light are scattered differently by the opacifying
particles.
13

Seminar -3
This effect depends upon the size as well as the volume distribution of the particles. Particles in the size range 0.4 to 0.8 m generate a blue tinge in reflecting light and turn yellowish red in transmitted light.
Preferably, the size of the particle should be nearly the same as the wavelength of visible light.7
COLOURING AGENTS Pigmenting or colouring oxides are added to obtain various shades needed to simulate
natural teeth. These pigments are produced by fusing metallic oxides together with fine glass and
feldspar and then regrinding to a powder. This powder is blended with the un-pigmented porcelain powder to obtain the proper
hue and chroma. The different colouring pigments used in dental porcelain are given in the table below.
8
Different coloring pigments used in dental porcelainFerric oxide (black), platinum gray Gray
Chromium oxide, Copper oxide Green
Cobalt Salts Blue
Ferrous oxide, Nickel oxide Brown
Titanium oxideYellowish brown
Manganese oxide Lavender
Chromium-tin, Chromium-alumina Pink
Indium Yellow / Ivory
STAINS AND COLOR MODIFIERS Stains are generally low fusing colored porcelains used to imitate markings like
enamel check lines, calcification spots, fluoresced areas etc. Stains in finely powdered form are mixed with water or glycerine and water or any other special liquid. The wet mix is applied with a brush either on to the surface of porcelain before glazing, or built into the porcelain (internal staining). Internal staining is preferable as it gives more lifelike results and also prevents direct damage to the stains by the surrounding chemical environment.
14

Seminar -3
Color modifiers on the other hand are less concentrated than stains and are used to obtain gingival effects or highlight body colours, and are best used at the same temperature as the dental porcelain. 7
GLAZES AND ADD-ON PORCELAIN Glazing is done so to produce enamel like lustre after occlusal and morphologic
corrections have been made in a porcelain restoration. It also seals pores on the surface of fired porcelain. 7
The aim of glazing is Sealing of open pores in the surface of fired porcelain. Provides transverse strength
Unglazed porcelain lead to abrasive wear of the opposing dentition or increase the rate of plaque accumulation 9
Glazing can be of two types:
Self glazing (auto glazing) Add-on glazing.
Self-glazing Defined as a vitrified layer that forms on the surface of a dental porcelain ceramic
containing a glass phase when the ceramic is heated to a glazing temperature for a specified time.
glazing occurs at temperatures of 955-1065oC. These are medium –fusing feldspathic porcelain is much stronger than ground,
rough, nonglazed porcelain. If the glaze is removed by grinding ,the transverse strength is reduced
By 40-46% compared to unglazed porcelain. Add-on glazes /over glaze
The surface coating of glass formed by using thin layer of glass powder that matures at a lower temperature than that associated with the ceramic substructure.
These are uncolored glasses whose fusing temperatures have been lowered by the addition of glass modifiers.
Add-on porcelains are generally similar to glaze porcelains except for the addition of opacifiers and color pigments.
Add-on porcelains should exclusively be used for simple corrections of tooth contour or contact points
Disadvantages of add-on glazes are o its low chemical durability,
15

Seminar -3
o Difficult to apply evenly and almost impossible to attain a
detailed surface characterization. 8
Many ceramists prefer polishing instead of glazing to control the surface Iustre.9
Studies have shown that porcelain with highly polished surface have comparable strength with glazed porcelain. This observation is of clinical importance because after the porcelain prosthesis is cemented in the mouth, as clinician will adjust the occlusion by grinding the surface of the porcelain with diamond bur, which removes the glaze and markedly weakens the porcelain and surface is left in a rough condition.8
Wiley (1989) stated that many studies have shown that polishing porcelain gives a smooth surface similar to that produced from a natural glaze.9
PROPERTIES Compressive strength - 50,000 psi
Tensile strength - 5,000 psi
Shear strength - 16,000 psi
Elastic modulus - 10X106 psi
Linear coefficient of thermal expansion - 12X10-6 / C
Specific gravity - 2.2 to 2.3
Liner shrinkage - High fusing - 11.5%
Low fusing - 14.0%
Refractive index - 1.52 to 1.54
1. The compressive strength is quite high compare to tensile or shear strength.2. The tensile strength is low because of the unavoidable surface defects.3. The shear strength is low because of lack of ductility in the material.4. Voids and blebs greatly reduce the strength of porcelain.5. Blebs are internal voids tend to reduce the specific gravity of porcelain. 6. Porcelains extremely hard materials and because of this property offer considerable
resistance to abrasion. This could be a disadvantage in that it causes excessive wear of the opposing natural tooth structure or the restorative material.
16

Seminar -3
7. The brittleness 0.1% deformation is sufficient to fracture porcelain before fracture.
8. Uranium oxide / cerium oxide is added to match the fluorescence of porcelain to that of the natural tooth.
9. Porcelain: a. Relatively inert.b. Chemically stable. c. Corrosion resistant. d. Highly biocompatible. e. Conducive to gingival health – as it prevents plaque addition.f. Solubility is less. 7
STRENGTHENING OF DENTAL PORCELAINMETHODS
1. Development of residual compressive stresses 2. Interruption of crack propagation
DEVELOPMENT OF RESIDUAL COMPRESSIVE STRESSES:
Strengthening is gained by virtue of the face that the residual stresses must first be negated by developing tensile stresses before any net tensile stress develops. There are several techniques for introducing these residuals compressive stresses into the surfaces of ceramic articles. Three of these methods are discussed below.
Ion exchange Thermal tempering Thermal Compatibility:
Ion Exchange:
The technique also called chemical tempering. This process involves the exchange of larger potassium ions for the smaller sodium
ions, a common constituent of a variety of glasses. If a sodium-containing glass article is placed in a bath of molten potassium nitrate, potassium ions in the bath exchange places with some of the sodium ions in the surface of the glass article.
The potassium ion is about 35% larger than the sodium ion. The squeezing of the potassium ion into the place formerly occupied by the sodium ion creates large residual compressive stresses (roughly 700 Mpa 100,000 psi) in the surfaces of glasses subjected to this treatment. These residual compressive stresses produce a pronounced strengthening effect.
17

Seminar -3
However, this process is best used on the internal surface of a crown, veneer, or inlay because this surface is protected from grinding and exposure to acids.
One study has shown that grinding of only 100 m from an external surface reduces the strength of the treated structure to its original value. Furthermore, contact with acidulated phosphate fluoride over a cumulative time of 3 hours removes most of the ion-exchanged layer as well.
Not all ceramics are amenable to ion exchange. For example, alumina core materials, DICOR glass-ceramic core material, and some conventional feldspathic porcelain that are highly enriched with potash feldspar (K2O, Al2O3.6SiO2) cannot be sufficiently ion exchanged with potassium to warrant this treatment.
Thermal Tempering:
The most common method for strengthening glass is by thermal tempering. Thermal tempering creates residual surface compressive stress by rapidly cooling
(quenching) the surface of the object while it is hot and in the softened (molten) state. This rapid cooling produces a skin of rigid glass surrounding a soft (molten) core. As the molten core solidifies, it tends to shrink, but the outer skin remains rigid. The pull of the solidifying molten core, as it shrinks, creates residual tensile stresses in the core and residual compressive stresses within the outer surface.
For dental applications, it is more effective to quench hot glass-phase ceramics in silicone oil or other special liquids rather than using air jets as it may not uniformly cool the surface.
Thermal Compatibility:
Most metals expand linearly with temperature up to the melting range. Thus, a metal expands approximately the same amount when heated from 50oC to 60oC as it does from 200oC to 210oC.
Dental porcelains behave differently; they have different values in different temperatures ranges, and, as a result, the thermal expansion or contraction of the porcelain cannot be precisely matched to that of the alloy.
Ideally, the porcelain should be under slight compression in the final restoration. This objective is accomplished by selecting an alloy that contracts slightly more than the porcelain on cooling to room temperature.
Consider three layers of porcelain: the outer two of the same composition and thermal contraction coefficient The middle layer of a different composition and a higher thermal contraction
coefficient.
18

Seminar -3
When the layers are bonded together and the bonded structure is allowed to cool to room temperature.
The inner layer has a higher coefficient of thermal contraction and thus contracts more as it cools. Hence, on cooling to room temperature, the inner layer produces compressive stresses in the outer layers as previously described for thermal tempering.
A similar rationale applies to porcelains and alloys for metal-ceramic restorations. The metal and porcelain should be selected with a slight mismatch in their thermal
contraction coefficients (the metal thermal contraction coefficient is slightly larger), so that the metal contracts slightly more than the porcelain on cooling from the firing temperature to room temperature. This mismatch leaves the porcelain in residual compression and provides additional strength for the restoration.8
INTERRUPTION OF CRACK PROPAGATIONDisruption of Crack Propagation :
A further, yet fundamentally different, method of strengthening glasses and ceramics is to reinforce them with a dispersed phase of a different material that is capable to hindering a crack from propagating through the material. There are two different types of dispersions used to interrupt crack propagation. One type relies on the toughness of the particle to absorb energy from the crack and deplete its driving force for propagation. The other relies on a crystal structural change under stress to absorb energy from the crack. These methods of strengthening are described later
Dispersion of a Crystalline Phase:
When a tough, crystalline material such as alumina (Al2O3) in particulate form is added to a glass, the glass is toughened and strengthened because the crack cannot penetrate the alumina particles as easily as it can the glass. The technique has found application in dentistry in the development of aluminous porcelains (A12O3 particles in a glassy porcelain matrix) for PJCs. Another ceramic dental material that uses reinforcement of a glass by a dispersed crystalline substance is Dicor glass-ceramic. The cast glass crown is subjected to a heat treatment that causes micron-sized mica crystals to grow in the glass. When glass-ceramic restorations are subjected to high tensile stresses, these microscopic crystals will disrupt crack propagation, thereby strengthening the crown. In most instances, the use of a dispersed crystalline phase to disrupt crack propagation requires a close match between the thermal contraction coefficients of the crystalline material and the surrounding glass matrix.
Transformation Toughening:
19

Seminar -3
A new technique for strengthening glasses involves the incorporation of a crystalline material that is capable of undergoing a change in crystal structure when placed under stress. The crystalline material usually used is termed partially stabilized zirconia (PSZ). The energy required for the transformation of PSZ is taken from the energy that allows the crack to propagate. Experimental work has shown that transformation toughening may be a viable method for strengthening dental porcelains. One drawback of PSZ is that its index of refraction is much higher than that of surrounding glass matrix. As a result, the particles of PSZ scatter light as it passes through the bulk of the porcelain, and this scattering produces an opacifying effect that may not be aesthetic in most dental restorations.
CONDENSATION OF DENTAL PORCELAINThe process of bringing the particles closer and of removing the liquid binder is known as condensation.
Distilled water is the liquid binder used most commonly. However, glycerin, propylene glycol or alcohol has also been tried.
The aim of condensation Is to pack the particles as close as possible in order to reduce the amount of porosity Shrinkage during firing. 8
Two important factors, which determine the effectiveness of condensation, are The size and shape of the powder particles. If only one-size particles are used, even the greatest condensation is
expected to leave a void space of 45 percent between the particles. With two sized particles , the void space is reduced to2 5 percent, and with
three or more sized particles, the void space comes down to 22 percent. System that uses three sizes of powder is known as the gap grading
system. The shape of the powder particles also governs the packing density.
Round particles produce better packing compared with angular particles. 7
Several methods of condensation are employed (1) Vibration method; the paste is applied on to the platinum matrix and vibrated slowly. This brings the excess water on to the surface, which is then drawn away with a fine brush or clean tissue. The condensation occurs towards the blotted or brushed area. Excessive vibration should be avoided as it can cause slumping of the mass (2) Spatulation method, a small spatula is used to apply and smooth the wet porcelain. The smoothening action disturbs the particles bringing them closer and also the water rises to the surface, which is removed as described earlier.
20

Seminar -3
(3) Dry brush technique involves placement of dry powder onto the wet surface. The powder is placed by a brush to the side opposite from an increment of wet porcelain. As the water is drawn towards the dry powder, the wet particles are pulled together. 8
(4) Whipping method, a large soft brush is moved in a light dusting action over the wet porcelain. This brings excess water to the surface and the same brush can be used to remove any course surface particles along with the excess water. (5) A combination of the vibration and the whipping methods can also be used. The mix is first vibrated and then whipped with a brush.
The most important factor in condensation is the effect of surface tension. As the liquid is withdrawn, surface tension causes the powder particles to pack closely together. However, sufficient amount of liquid should be present so as to wet all the powder particles.7
CERAMOSONIC CONDENSOR Through its ultrasonic function, it imparts low amplitude, high frequency vibration
enabling Condensation of moist porcelain particle. Improves substructure of the porcelain & dispense trapped air & increase density Less shrinkage during firing Enhanced surface and strength
FIRING PROCEDURE/ SINTERING PROCEDURE Defined as process of heating closely packed particles to achieve interparticle
bonding and sufficient diffusion to decrease the surface area or increase density of the structure. The partial fusion or compaction of glass is referred to as sintering
Most of the thermo chemical reactions in porcelain are completed during the manufacturing process.
The role of firing is simply to sinter the particles of porcelain powder together to form a dense restoration.
STAGES ARE PREHEATING
The condensed mass is placed in front of or below the muffle of a preheated furnace at an approximately 650 C (1200 F) for low fusing porcelain. This permits removal of excess water and prevent the sudden production of steam that could result in voids or fractures
After pre heating for approx 5 min, the porcelain is placed into the furnace and firing cycle is initiated.
21

Seminar -3
FIRING Can be fired by following methods
Temperature controlled method: furnance temperature is raised at a constant rate until a specified temperature is raised
Temperature –time control method : furnace temperature is raised at a given rate until a preset temperature is reached, after which temperature is maintained for specific time till the reaction is completed .preferred method as produces uniform restoration.
At the initial firing temperature the voids are occupied by the atmosphere of the furnace. As the sintering of the particles begins, the porcelain particles bond at their points of contact .as temperature is raised; the sintered glass gradually flows to fill up the air spaces. Second change occurs with a further rise in temperature when the particles fuse together by sintering. As a continuous mass is formed, there occurs a decrease in volume referred to as firing shrinkage (32-37% for low fusing and 28.34% for high fusing). After the mass has been fired, it is cooled very slowly because rapid cooled might result in surface cracking and crazing.
Different media can be employed for firing like:
A) AirB) VacuumC) Diffusible gas
AIR FIRING PROCEDURE:Whenever air-firing methods are employed, a very slow maturation period is
preferred to allow for the maximum amount of entrapped air to escape. During firing slow heating is done .the porcelain is sintered within a range of atleast 30oC to 50oC below the maximum firing temperature. Such a temperature will mature porcelain without loss of color and high densities can be achieved.
POROSITY
Bubbles or voids in the fired porcelain are caused by inclusion of air during firing or in some cases as a by-product of vitrification of feldspar. Porosity reduces both translucency and strength of dental porcelain. Translucency depends on the number and size of the entrapped air bubbles. Large sized particles have fewer but larger air voids between them compared to small sized particles. Fewer bubbles, even of large size, give improved translucency. On the other hand, fine sized particles have multiple small air bubbles present in between them, which make them highly opaque. It is, therefore, clear that porcelain powders fired in air must be of necessarily coarse nature.
22

Seminar -3
VACUUM FIRINGThis technique is used to reduce porosity in dental porcelains. It works on the basis
of removing air or atmosphere from the interstitial spaces before surface sealing occurs. Although the vacuum (760 torr) removes most of the air from interstitial spaces, some of it is left behind. With the increase in temperature and because of surface tension, the remaining air spaces assume a spherical appearance. When air at normal atmospheric pressure is allowed to enter the furnace, it exerts a compressive effect on the surface skin, which further compresses the internal voids to one tenth of their original size. This results in very dense porcelain with very few remaining bubbles and that too of extremely small size.
Factors to be kept in mind while firing porcelain in vacuum are:
1. Porcelain powders must be dried slowly to eliminate the water vapour, and vacuum should be applied before the placement of porcelain in the hot zone of furnace. The interstitial spaces are hence reduced before the surface skin seals off the interior too rapidly.
2. Vacuum should not be applied after the surface skin has sealed and the porcelain has matured. Prolonged application can force the residual air bubbles to rise to the surface and cause surface blistering. Additionally, high temperatures can cause swelling of these blisters.
3. The vacuum should be broken while the work is still in the hot zone of the furnace. This permits the dense skin to hydraulically compress the low-pressure internal voids.
4. Vacuum firing cannot reduce the large sized bubbles to any significant degree. Hence, it is necessary to avoid porcelains with large interstitial spaces i.e., porcelain powders with small sized particles are preferred.
DIFFUSIBLE GAS FIRING In this technique, a diffusible gas like helium, hydrogen or steam is substituted for
the ordinary furnace temperature. Air is driven out of the porcelain powder bed and replaced by the diffusible gas. With these gases, the interstitial spaces do not enlarge under the influence of increasing temperature, but decrease in size or disappear. This occurs because these gases diffuse outward through the porcelain or actually dissolve in porcelain.7-8
23

Seminar -3
VARIOUS STAGES OF MATURITYSeveral stages of dental porcelain have been identified when it is ‘sintered’ or ‘fired’. The common terminology used for describing the surface appearance of unglazed porcelain is ‘bisque’.
Low bisque:
The surface of porcelain is quite porous. The grains of porcelain begin to soften and ‘lense’ at their contact points. Shrinkage is minimal and the fired body is extremely weak or friable.
Medium bisque:
Pores still exist on the surface of porcelain, but the flow of glass grains is increased. As a result, any entrapped furnace atmosphere that could not escape via the grain boundaries becomes trapped and sphere shaped. A definite shrinkage is evident.
High bisque:
The flow of glass grains is further increased, thereby completely sealing the surface and presenting smoothness to the porcelain. In the case of non-Feldspathic porcelains, a slight shine appears at this stage. The fired body is strong and any corrections by grinding can be made prior to final glazing at this stage.7-8
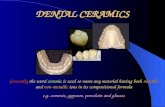
METAL CERAMICS:
The chief objection to the use of dental porcelain as a restorative material is its low strength under tensile and shears stress conditions.
The method by which this disadvantage can be minimized is to bond the porcelain directly to a cast alloy substructure made fit the prepared tooth.
To fabricate this restoration, a metal substructure is waxed, cast, finished and heat treated (oxidized).a thin layer of opaque porcelain is fused to the oxidized metal surface to establish porcelain- metal bond and mask the color of substructure. Then enamel and dentine porcelains referred as incisal and body porcelains, are fused to the opaque porcelain, shaped, staine to improve the esthetic appearance and glazed.8
TYPES OF METAL CERAMIC SYSTEMS
A large number of metal-ceramic systems have been developed for the use in dentistry and they may be classified as follows:
24

Seminar -3
NOBLE METAL ALLOY SYSTEM:
HIGH GOLD :
1. Gold –platinum-palladium alloys2. Gold –platinum-tantalum alloys
LOW GOLD 1. Gold –palladium-silver alloys
GOLD FREE: 1.Palladium silver alloys
BASE METAL ALLOY SYSTEM:
1. Nickel chromium alloy2. Cobalt –chromium alloys10
THE NATURE OF METAL CERAMIC BOND
THE success of metal –ceramic crowns and fixed bridges depends upon the firmness of the bond between metal and ceramic.
Therefore metal porcelain bond can be classified into 3 main components:
1. Mechanical2. Compressive 3. Chemical
MECHANICAL RETENTION:
Depends upon good wetting of the metal or metal oxide surface by the porcelain.
Rough surface enhances the bond resistance against induced shear stresses especially for base metal alloy system.
Advantages of an air abraded surface over smooth surface for noble metal alloys and base metal alloys are:
1. Enhancement of wettability of the metal substrate by porcelain2. Some additive bond strength because of mechanical interlocking of porcelain under
compression.3. Increased surface area for porcelain chemical bonding
Disadvantages are:
1. Excessive roughness resulting in stress conc. at the metal ceramic interface
25

Seminar -3
2. Steep interface angles that may not allow complete wetting and therefore result in air entrapment and voids at the metal ceramic interface.
COMPRESSIVE STRESSES:
COMPRESSIVE STRESSSES Developed during cooling of sintered porcelain veneer will also play a part in improving the bond strength.
CHEMICAL BONDING:
A bulk diffusion of base metal atoms produces an oxide film on the metal surface which forms a chemical bond with porcelain.8
TYPES OF METAL/ PORCELAIN FAILURE:
26
Surface oxides for porcelain bonding can be provided by
Introducing traces of base metals into precious metal
alloys, which on heating will produce thin oxide films
Direct oxide production via the constituents of the alloys (base metal)
3 .Electro deposition of indium or tin on the noble metal
alloys

Seminar -3
1. METAL –PORCELAIN:The interfacial fracture occurs leaving a clean surface of metal,seen when Metal surface is completely depleted of oxide prior to the baking of porcelain or when no oxides are available.May also be due to conyaminated or porous metal surfaces.
2. Metal –oxide porcelain:The metal oxide porcelain at the metal oxide surface leaving the oxide firmly attached to the metal.Common in base metal alloy system.
3. Metal –metal oxide:This is an interfacial fracture in which the metal oside breaks away from the metal substrate an d is left attached to the porcelain.Common in base metal alloy system when there is over production of chromium and nickel oxide athe interface.
4. Metal oxide – metal oxide:This fracture occurs through the metal oxide at the interface and results from an over production of the oxide causing sandwitch effect between metal and porcelain.
5. Cohesive within metalThis type of fracture would only occur in cases for eg. Where the joint areas in the bridges breaks. Most unlikely type of fracture for the individual metal –ceramic crown.
6. Cohesive within the porcelain:This is the optimum type of fracture in which tensile failure occurs within the porcelain.in this case the bond strength exceeds the strength of porcelain.An ideal situation is created when the oxide film is only a few molecules thick and forms a solid solution with the porcelain.this is the most common frature in the high gold content alloys.10
ALL CERAMIC SYSTEMS
The term of “All ceramic” refers to any restorative material composed excessively of ceramic, such as Feldspathic porcelain, glass ceramic, alumina core systems and certain combination of these materials -
J. Esthetic Dent 1997, 9(2):86
Advantages
• Increased translucency
27

Seminar -3
• Improved fluorescence
• Greater contribution of color from the underlying tooth structure
• Inertness
• Biocompatibility
• Resistance to corrosion
• Low temperature / electrical conductivity
CLASSIFICATION7
1. Conventional powder slurry ceramic Hi Ceram – Alumina reinforced porcelain Optec HSP – Leucite reinforced porcelain Duceram LFC – Hydrothermal low fusing ceramic
2. Pressable ceramic IPS Empress Optec Pressable ceramic
3. Infiltrated ceramic In-Ceram
4. Castable ceramic DICOR Cera Pearl
5. Mechinable ceramic Cerec Vitablocs Mark I and II Celay Blocks DICOR MGC
ACCORDING TO Crispin 1994, Rosenblum and Schulman 1997): 11
• Castable Ceramic Systems: They are modelled in a wax (Dicor, Cerapearl). • Infiltrated Ceramic Systems: They are based on the principle of two infiltrated phases, Al 2 O 3 and a glass (In-Ceram). • Machinable Ceramic Systems: They are based on taking an optical impression of a patient’s oral situation and have a restoration milled from a ceramic block chairside with CAD/CAM and copy-milling systems (Cerec Vitablocks, Procera AllCeram, Dicor MGC, Celay). • Pressable Ceramic Systems: They are produced by molding under pressure and heat (IPS Empress, Optec)
28

Seminar -3
ACCORDING TO supporting structure (Van Noort 2002) Reinforced ceramic core systems :
The support for the aesthetic ceramic is provided by another ceramic material, which has the necessary high strength and toughness’ but may lack the desired aesthetics (In-Ceram, Cerec, Celay, Procera All- Ceram).
Resin-bonded ceramic systems : The support of the ceramic is provided by the tooth structure itself, by bonding the aesthetic ceramic directly to the enamel and dentine. In this instance the ceramic provides the necessary aesthetics and the strength is provided by the ability to bond to the tooth tissues. The materials available for resin- bonded ceramic restorations are varieties of glass –ceramics.
Conventional powder slurry ceramic
ALUMINA REINFORCED PORCELAIN
It was introduced by McLean and HUGES in 1965, to improve strength by Prevention of crack propagation.These are based on the principle of dispersion strengthening i.e. dispersing alumina Crystals of high strength and elasticity in a glass matrix. A core structured is formed that has increased flexure Strength, elasticity and fracture toughness compared to conventional porcelains.For dental purpose single crystals of alumina are preferred over fine powdered alumina, to avoid excessive opacity which occurs because of difference in the refractive index of glass porcelain and alumina crystals.The 2 imp requirements when using these filler reinforced porcelains are:
Bond between filler particles and matrixIdentical CTE of the two phased
If CTE of Glass matrix > alumina crystals, there would occur radial compression and tangential tension in the glass matrix on cooling resulting in decrease in Elasticity and strength.Glass used for incorporating alumina crystals is BOROSILICATE GLASS Containing:
Silica Alumina Potash Soda
29

Seminar -3
Lime Boric acid
Strength and opacity of aluminous porcelain is dependent on alumina crystal: Size Shape Concentration
SIZE OF ALUMINA CRYSTALS:
Finer the grain size: greater is strength , but results in increased opacity, due to
high difference in refractive index of the two component ,which causes increased
scattering of light, defeating the esthetics.
Coarse grain size: reduces strength because of the “notched effect” created on glass
boundaries. They are opaque. Grain size on average should be 25 µm (max. being37 µm) that would allow light transmission of atleast 10-15% on 1 mm thick discs and fine enough to give sufficient strengths.
Shape: rounded grains are preferable over angular ones as latter interface with the flow of the glass Phase producing flaws around grains and reducing strength.
Concentration of alumina crystals should range from 40-50% by weight.
Higher concentration Prevent complete flow and wetting by the glass matrix.
Commercially available product is Hi-Ceram (Vita).
Uses:
Forming refractory framework capable of supporting weaker, more translucent Dentin
and enamel Porcelain.7-8
LEUCITE REINFORCED PORCELAIN:
Commercially available as OPTEC HSP Leucite conc. is:50.6% These porcelains contain dispersed LEUCITE {potassium aluminosilicates} in glassy
Matrix.Therefore more stronger than conventional Feldspathic porcelains. Because of its increased strength it does not require core when used to fabricate
All ceramic Restoration as is necessary with aluminous porcelain PJCs. Lecuite and glass matix are fused together during the baking process at 1020 C. The buildup, condensation and contouring is done using powder slurry technique
on special semi permeable die material.
30

Seminar -3
Uses:
Used both for incisal and body portions being more aesthetics
Advantages:
Lack of metal or opaque substructure ,good translucency Moderate flexure strength ,higher than conventional Feldspathic porcelains Ability to be used without any special lab equipments
Disadvantages:
Margins inaccuracy caused by porcelains sintering shrinkage Potential to fracture in posterior teeth High wear of opposing tooth due to high Leucite content
No clinically published studies on Optec HSP
DUCERAM LFC:
Also known as hydrothermal low fusing ceramics. It is a low fusing ceramic, composed of an amorphous glass containing hydroxyl ions. Properties: compared to Feldspathic porcelain
Greater density Higher flexure strength Greater fracture resistance Lower hardness
Because of the absence of Leucite crystals, the hardness of the materials and its ability to abrade the opposing natural tooth structure is reduced.
It is then strengthened by ion exchange mechanism involving h hydroxyl ions thus decreases the surface micro flaws and increase fracture resistance.
However, there are no clinical studies to substantiate the manufactures claim that the material is less abrasive than feldspathic porcelain. However, the result of 1 year clinical study recently conducted for manufacture r seems to indicate that the material wears at a rate equivalent to that of natural tooth enamel ( Showtwell J,Beard CC, Lang B,Lang BR,unpublished data 1990).
Restoration from Duceram LFC is made in 2 layers:
The base layer is Duceram metal ceramics (Leucite containing porcelain) which is placed on refractory die using powder slurry technique and then baked at 930 C.Over the base layer is Duceram LFC is applied using powder slurry technique and then baked at 660 C.
31

Seminar -3
Available in variety of shades and can be characterized by variety of stains and modifiers.
USES: Ceramics inlays, veeners, and full contour crowns
PRESSABLE GLASS CERAMIC
IPS empress Optec pressable ceramics
A glass ceramics is material that is formed into desired shape as a glass, and then subjected to a heat treatment to induce partial devitrification (that is loss of glassy structure by crystallization of the glass).
The crystalline particles, needles or plates formed during this ceramming process serve to interrupt the propagation of the cracks in the material when intraoral force is applied, causing increased strength and toughness.
ADVANTAGES :
Lack of metal Translucent ceramic core Moderately high flexure strength Excellent fit Excellent aesthetics
DISADVANTAGES:
Potential to fracture in posterior areas Use of resin cement to bond crown micromechanically to tooth structure Require special equipment.(pressing oven and die material.)
IPS EMPRESS :
A leucite-reinforced glass-ceramic material was first described by Wohlwend and Scharer12
This type of Feldspathic porcelain is supplied in the ingot form. The ingot are heated and molded under pressure to produce the restoration. A full contour crown is waxed, invested and placed in specialized mold that has an
aluminium plunger.
32

Seminar -3
The ceramic ingots are placed under the plunger, the entire assembly is heated to 1150C and the plunger presses the molten ceramic into the mold.
The final shade of the crown is adjusted by staining or veneering. In the veneering technique, the original wax –up is cut by about 0.3 mm. After molding and baking as described, feldspathic porcelain is added to the surface
to obtain full contour and the correct shade.
OPTEC PRESSEABLE CERAMIC :
Type of Feldspathic porcelain with increased lecucite content, processed by molding under pressure and heat.
Used for – Full contour restoration : inlays, veneers, full crowns. Can be used as core material, for veenering conventional powder alurry
techniques with high Leucite content Feldspathic porcelain, similar to Optec HSP porcelain.
Crystalline Leucite particle size is reduced and content is increased which result in increase in flexural strength
Because of high Leucite content abrasion of opposing natural teeth is high.7,8,11
INFILTERED CERAMICS:
IN-CERAM SADOUN developed INCERAM in 1985
In-ceram is supplied as one of the three core ceramics:
In-ceram spinnel In-ceram alumina In-ceram zirconiaThe slurry of one of these materials is slip cast on a porous refractory die and heated in the furnace to produce a partially sintered coping and framework. The partially sintered core is infiltered with glass at 1100 C for 4 hours to eliminate porosity and to strengthen the slip cast core. 4
Thus A porous infrastructure is produced by slip-casting, sintered, and later infiltrated with a lanthanum-based glass, producing two interpenetrating continuous networks, one composed of the glassy phase and the other being the crystalline infrastructure. Three crystalline phases are available, namely alumina (Al 2 O 3),
spinel (MgAl 2 O 4 ) and
33

Seminar -3
Zirconia-alumina (12 Ce-TZP-Al 2 O 3 ).8Alumina-based slip-cast ceramics contain
68 vol % alumina, 27 vol % glass and 5 vol % porosity12
The microstructure consists of blocky alumina grains of various sizes and shapes. Evidence of grain pull-out, bridging and crack deflection was reported with this type of ceramic indicative of efficient crystalline reinforcement, and accounting for mechanical properties in the range of heat-pressed lithium disilicate glass-ceramics. It has also been suggested that the coefficient of thermal expansion mismatch between the alumina crystals and the infiltration glass could contribute to strengthening due thermal residual stresses. The presence of large alumina crystals with a high refractive index, and a non-negligible amount of porosity, account for some degree of opacity in this all-ceramic system. Spinel-based slip-cast ceramics offer better translucency , similar to that of lithium disilicate heat-pressed ceramics, at the expense of mechanical properties Zirconia-toughened alumina slip-cast ceramics comprise 34 vol % alumina and 33 vol % of 12 mol % ceria-stabilized zirconia (12Ce-TZP). The glass phase represents approximately 23 vol % of the final product, with about 8 vol % residual porosity . The dual crystalline reinforcement in this system allows two types of strengthening mechanisms: (1) The stress-induced transformation in zirconia grains produces compressive stresses within the transformed grains and surrounding glassy matrix, as well as circumferential tensile stresses around the grains, accompanied by micro crack nucleation. Transgranular fracture is difficult in zirconia; this represents an efficient strengthening mechanism. (2) Crack deflection, contact shielding and crack bridging are expected from the presence of large alumina grains The combination of these two strengthening mechanisms explains why alumina-zirconia slip-cast ceramics offer the highest flexural strength and fracture toughness of all slip-cast ceramics.
INDICATION:
In-ceram spinnel:
Anterior single unit inlays,onlays crowns and veeners.
34

Seminar -3
In clinical situations where maximum translucency is needed
In ceram alumina:
Anterior and posterior crowns
Anterior 3 unit prosthesis
Inceram zirconia:
Because of high strength and fracture toughness it is indicated for posterior crowns and FPD.
Fabrication ProcedureAn All-Ceramic restoration system INCERAM is based on the slip casting of an
alumina core with its subsequent glass infusion. After the impression is taken the die is poured with special gypsum supplied with INCERAM, then the INCERAM ALUMINA is applied onto the die.
The alumina powder is mixed with deionized water supplied in pre-measured container. Dispensing agent is added to create a homogenous mix of alumina in water. This mixture is sonicated in VITASONIC thus initiating the dispersion process. Then vacuum is applied to remove the air bubbles.
This solution of alumina is referred to as “slip” which is then painted onto the gypsum die with a brush. The alumina is built up to form a core for the ceramic tooth. The water is removed by the capillary action of the porous gypsum, which packs the particles into a rigid network.
The aluminous core is then placed in the IN-CERAMET furnace and sintered. The cycle involves a slow heating of approximately 2oC/min to 1120oC for 2 hours to produce approximation of the particles with minimal compaction and minimal shrinkage of alumina. Sintering is only about 0.2% thus an interconnected porous network is created connecting pores on the outer surface with those on the inner surface.
Low viscosity lanthanum aluminosilicate glass is used to fill the pores in the alumina. The glass is mixed with water and placed on a platinum – gold alloy sheet. The external surface of the core is placed on the glass, which is heated in the IN-CERMET to 1100oC for 4-6 hours. The glass becomes molten and flows into the pores by capillary diffusion. The excess glass is removed by sandblasting with alumina particles.
35

Seminar -3
The last step is fabrication of INCERAM restoration involves application of aluminous porcelain to the core to produce the final form of restoration. The low viscosity lanthanum glass is used to infiltrate the alumina core in INCERAM. This should be in air environment as recommended by the manufacture. The INCERAM aluminous glass ceramic produced by lanthanum glass infiltration is about 50% translucent as dentin.
In clinical situations where there is a discolored preparation or a cast post and core this increased opacity over the dentin is advantageous were as when maximum translucency is necessary INCERAM ALUMINA is problematic.
CASTABLE GLASS CERAMIC The first commercially available castable ceramic material for dental use, DICOR, was developed by corning glass works and marketed by Dentsply international.
Classification of Castable Dental Glass Ceramics:
Flucoromicas Dicor Apatite glass ceramics pearl Other glass ceramics Lithia ,Calcium Phosphate
DICOR A Polycrystalline glass ceramic is a material that is formed into the desired shape as
a glass and subsequently heat-treated under controlled conditions to induce partial devitrification.
The fabrication method uses lost wax and centrifugal casting technique similar to those used to fabricate alloy castings.
A full contour transparent glass crown is cast at 1350 C then is heat treated at 1075 C for 10 hours. This heat treatment is known as ceramming causes partial crystallization (55%) of tetrasilic mica like crystals.
These crystals function in 2 ways: They create a relatively opaque material out of the initially transparent
crown and increase the fracture resistance and strength of the ceramic. Crystals are also less abrasive to opposing tooth structure.
Properties The physical properties of DICOR are given in the table.
PROPERTY DICORENAMEL
FELDSPATHIC PORCELAIN
Density, g.cm3 2.7 3.0 2.4
36

Seminar -3
Translucency 0.56 0.48 0.27
Modulus of rupture psi 22000 1500 11000
Compressive strength, psi
120000 58000 25000
Modulus of Elasticity, psix106
10.2 12.2 12.0
Microhardness 362 343 450
Esthetic Qualities DICOR restorations are highly esthetic because of their translucency, which closely
matches that of natural tooth enamel. The numerous small mica crystals that constitute castable ceramic closely match the index of refraction to the surrounding glass phase. In addition, the castable ceramic permits a one-piece restoration made entirely of the same material, and no opaque substructure exists to impede light scattering. A chameleon effect is seen with DICOR restorations in which the restoration acquires a part of the color from adjacent teeth and fillings as well as the underlying cement lute. Application of an external coloring system allows independent control over hue, chroma and value. However, as mentioned before, there are chances of losing this external layer thereby defeating the best of esthetics.Precision Of Fit
The resistance of DICOR to chemicals and staining agents also compares favourably with conventional feldspathic porcelains. Little wear of the cast ceramic or the opposing dentition occurs when using DICOR restorations. Two reasons for this property are:
a. Closely matching hardness between the cast ceramic material and natural enamel.b. The DICOR shading porcelains contain minimal abrasive opacifying agents.
Tissue Acceptance DICOR is chemically inert and has shown to pass all the biocompatibility tests. The
periodontal tissue reaction to DICOR is considered quite favorable because 1. There is no need for opaque porcelains to mask the metal substructure. These
coarse grained opaque porcelains generally promote the adherence of plaque.2. The absence of an opaque layer allows the technician to obtain natural contouring
often found in metal ceramic restorations.
37

Seminar -3
Little discomfort occurs on contact with hot or cold foods because of its extremely low thermal conductivity and a coefficient of thermal expansion, which closely matches that of natural enamel.
Radiographic QualitiesThe radiographic density of DICOR is similar to that of enamel allowing proper
evaluation of the underlying structures and the margins.Advantages
1. Excellent marginal fit2. Relatively high strength 3. Surface hardness and occlusal wear is similar to enamel4. Can reproduce wax patterns precisely by using the lost wax technique5. Simple uncomplicated fabrication from wax up to casting, ceramming and colouring6. Ease of adjustment 7. Excellent aesthetics resulting from natural translucency8. Inherent resistance to plaque accumulation (seven times less than on the natural
tooth surfaces).Disadvantages
1. Chances of losing low fusing feldspathic shading porcelains, which have been applied for good colour matching.
Uses Inlays, onlay, complete crowns and possibly partial tooth coverage restorations. It
is not indicated for fixed partial denture or removable partial denture abutments with deep rests or internal attachments.
CERA PEARL Castable apatite ceramic was first developed by Hobo and Bioceram Group as
CaO-P2O5-MgO-SiO2 glass ceramic. Cera Pearl is composed of CaO, P2O5, MgO, SiO2 and traces of other elements.
CaO(45%) and P2O5 (15%) are the main ingredients in glass formation. They are essential for formation of hydroxylapatite crystals as well. MgO (5%) helps in the formation of hydroxyapatite and along with CaO decreases the viscosity of the compound when melted. SiO2(34%) in combination with P2O5 forms the matrix. Further SiO2 regulates the thermal properties.
Because the crystalline constituent is similar to natural enamel, Cera Pearl is quite biocompatible. The Young’s modulus, tensile strength and compressive strength of Cera Pearl are appreciably higher than conventional porcelains.
38

Seminar -3
Physical properties
• Coefficient of thermal expansion: 11.0 x 10-6/oC.
• Young’s modulus – 103 Gpa
• Casting shrinkage – 0.53%
• Flexural strength similar to Dicor
• Biological properties – Dense material, chemically stable, PH similar to natural enamel
• Non toxic / biocompatible
Lithia based glass ceramic
Developed by Urgu
Composition: It contains mica crystals and Beta spodumene crystals of LiO, A12O3.4SiO2
after heat treatment.
Calcium phosphate glass ceramic
• Reported by Kihara and others
• Combination of calcium phosphate and phosphosus pentoxide plus trace elements
• Cast at 1050°C in gypsum investment mold
• Clear cast crown is converted to a crystalline ceramic by heat treating at 645°C for 12 hours
Disadvantages
• Weaker than other castable ceramics
• Opacity reduces the indication for use in anterior teeth
SHRINK FREE CERAMIC CERESTORE
It is a shrink-free alumina crown developed by the Coors Biomedical Co. and later sold to Johnson & Johnson. It is fabricated using lost wax technique and then injection
39

Seminar -3
molding to produce a coping. MgAl2O4 spinell and an alpha-alumina oxide make the core replaced by Alceram. The use of a shrink-free ceramic coping formed on an epoxy die by a transfer molding process overcomes the limits and firing shrinkage of conventionally produced aluminous porcelain jacket crowns. The Cerestore coping is veneered with conventional aesthetic porcelain.
Flexural strength:
It is approximately 150 Mpa.
MACHINABLE CERAMICS:
Brief history:
Development of CAD-CAM (Computer Assisted Design-Computer Aided Manufacturing) system for the dental profession began in 1970’s with DURET in France, ALTSCHULER in US & BRANDESTINI in Switzerland.
From 1971, he began to fabricate crowns with an optical impression of abutment followed by designing and milling.
Later he developed Sopha system. Dr. Mormann developed CEREC System, an innovative approach to fabricate
same day restorations at the chair side in the dental office. Dr.Anderson developed Procera System He attempted to fabricate titanium
copings by spark erosion and introduced CAD/CAM technology into the process of composite veneered restorations.
This system later developed as a processing center networked with satellite digitizers around the world for the fabrication of all ceramic frameworks13
Machinable ceramic:
CAD/CAM ceramics: a ceramic restoration fabricated by use of a computer aided design and computer aided milling
Copy milled ceramics: a process of milling a structure using a device that traces the surface of a metal, ceramic or a polymer pattern and transfers the traced special positions to a cutting station.
The different types of ceramic ingots used in the process as follows: 11
Cerec vitablocks Mark I:This is a feldspathic porcelain which was the first composition used with the Cerec system (Siemens).its composition, strength and wear properties are similar to Feldspathic porcelain used for PFM restorations
40

Seminar -3
Cerec Vitablocks Mark II This is feldspathic porcelains of increased strength and has finer grain size the mark I composition.Less abrasive wear of the opposing teeth.
Dicor MGC (Dentsply L.D caulk Division):This is a machinable glass ceramic composed of flurosilicic mica crystals in a glass matrix. It has greater flexural strength than castable Dicor and Cerec composition.procuses less abrasive wear.
Celay:Can be used CAD-CAM produced restorations or used in the copy-milled technique. It is a fine grained Feldspathic porcelain with reduced wear of opposing tooth .
CAD/ CAM process: A CAD/CAM system utilizes a process chain consisting of scanning, designing and
milling phases. The scanning device converts the shape of the prepared teeth into three
dimensional (3-D) units of Information (voxels). The computer translates this information into a 3-D map (point could).
The operator designs a restoration shape using the computer which generates a tool path, which is used by the milling device to create the shape from a restorative material
CAD CAM SYSTEMS:
CEREC :
An acronym for chair side economic reconstruction of esthetic ceramic .Cerec introduced in 1980s, improved Cerec 2 introduced in 1996 and the advanced 3-D Cerec 3 in 2000. With Cerec 1 and Cerec 2, an optical scanner is used to scan the prepared tooth or impression and a 3-D image is generated on monitor. A milling unit is used to prepare the restoration.
With newer Cerec 3-D, the operator records multiple images within seconds, enabling clinician to prepare multiple teeth in same quadrant and create a virtual cast for the entire quadrant.
Designed restoration is transmitted to a remote milling unit for fabrication. Cerec in-lab is a lab system in which dies are laser scanned and image displayed on screen. After designing VITA In-cream blocks are used for milling. The coping is glass infiltrated and veneer porcelain added.
41

Seminar -3
In vitro evaluation of marginal adaptation of crown of cerec 3-D (47.5 µm ±19.5 µm) was better compared with cerec 2 (97.0±33.8 µm)
DCS PRECIDENT:
Comprises of a Preciscan laser Scanner and Precimill CAM multitool milling centre.
The DCS software automatically suggests connector sizes and pontic forms for bridges. It can scan 14 dies simultaneously and mill up to 30 frameworks unit in one fully automated operation. It is one of the few systems that can mill titanium and fully dense sintered zirconia. An in vitro study showed that marginal discrepancies of alumina and ziroconia based posterior fixed partial denture machined by the DCS system was between 60 µm to 70µm
CERCON:
Commonly referred to as a CAM system, it does not have a CAD component. The system scans the wax pattern and mills a zirconia bridge coping from presintered zirconia blanks, which is sintered at 1,350°C for 6-8 hrs. Veneering is done with a low fusing, leucite free cercon Ceram to provide esthetic contour. Marginal adaptation for cercon all ceramic crowns and fixed partial dentures was reported 31.3µm and 29.3 µm respectively.
PROCERA ALL CERAM SYSTEM
Introduced in 1994, it is the first system which provided outsourced fabrication using a network connection. Once the master die is scanned the 3-D images is transferred through an internet link to processing center where an enlarged die is milled by a computer controlled milling machines. This enlargement compensates for sintering shrinkage. Aluminum oxide powder is compacted on the die and coping is milled by a computer controlled milling machines. This enlargement compensates for sintering shrinkage. Aluminum oxide powder is compacted on the die and coping is milled before sintering at a very high temp (>1550°C). The coping is sent back to the lab for porcelain veneering. According to research data average marginal gap for Procera all Ceram restoration ranges from 54 µm to 64 µm
CICERO SYSTEM (COMPUTER INTEGRATED CROWN RECONSTRUCTION) Introduced by Denison et al in 1999, it includes optical scanning,
42

Seminar -3
metal and Ceramic sintering and computer assisted milling to obtain restoration. Basic reconstruction includes layered life like ceramic for natural esthetics, a precision milled occlusal surface and a machined high strength ceramic core. The aim of CICERO is to mass produce ceramic restoration at one integrated site. It includes rapid custom fabrication of high strength alumina coping and semi finished crowns to be delivered to dental laboratories for porcelain layering / finishing.
LAVA CAD/CAM SYSTEM
Introduced in 2002, used for fabrication of zirconia framework for all ceramic restorations. This system uses yttria stabilized tetragonal zirconia poly crystals (Y-TZP) which have greater fracture resistance than conventional ceramics. Lava system uses a laser optical system to digitize information. The Lava CAD software automatically finds the margin and suggests a pontic. CAM produces an enlarged framework to compensate shrinkage. A partially sintered ziroconia block is selected for milling. Milled framework undergoes sintering to attain final dimensions, density and strength. Studies on marginal adaptation of Y-TZP bridges processed with Lava system for 2 milling times (75 mins Vs 56 mins) did not affect the marginal adaptation (61 25 µm Vs 59 21 µm )16
CAD/CAM Restorative Technique: 15
Consists of Handheld scanning device that digitally records the form and margins of the preparation.
The scanners require a dry field and soft tissue that must be thoroughly separate at the level of the margin from the hard tissue.
The soft tissue diode laser (Odyssey Navigator, Ivoclar Vivadent; GENTLEray 980, Kavo; DioDent Micro 980, HOYA ConBio) is used to expose Subgingival margins. The soft tissue diode laser offer precision, that result in a narrow band of lased tissue, and produces good hemostasis.
43

Seminar -3
SOFT TISSUE DIODE LASER
Alternative soft tissue management techniques include electro surgery and standard manual retraction technique.
Depending on the system used, the clinician can see the preparation magnified on the computer screen as the scan is being processed.
Two basic techniques can be utilized for CAD/CAM restorations.
Chairside – a single-visit technique Integrated Chairside—laboratory CAD/CAM Procedure.
Chairside CAD/CAM Technique: The chairside technique involves scanning the preparation and then fabricating the
restoration in the milling device (CEREC 3, Sirona; E4D, D4D TECH). Prior to scanning, a very thin layer of powder is distributed over the preparation
using the CEREC system. During scanning, the clinician must ensure that all margins of the cavity are
captured by the scan and visualized. The CEREC 3 uses still images, while the E4D uses a laser in the handheld
scanning device A third system, CICERO, was developed in The Netherlands and used a pressing,
sintering, and milling technique prior to laboratory finishing of the restoration. For Chairside CAD/CAM restorations, an esthetic, strong material requiring
minimal post-milling esthetic adjustment to minimize Chairside time is needed. Leucite-reinforced glass ceramics (IPS Empress CAD, Ivoclar Vivadent; Paradigm C, 3M ESPE) lithium disilicate glass ceramics (IPS e.max, Ivoclar Vivadent)
Advantages
44

Seminar -3
One-visit fixed restorative procedure No impression making No temporary restoration required Reduced potential for tooth sensitization No laboratory costs No model or die pouring Accuracy Less opportunity for error compared to traditional technique Aids prep visualization Projects a state-of-the-art image
Disadvantages
Less conservative than direct composite fillings Slightly less exacting fit than laboratory-made Esthetic capabilities are limited 14
Soft tissue management more critical than with traditional technique
Depending on the material and patient, customization may be required
High learning curve Higher production required to cover capital
investment
CASE 1. ANTERIOR ESTHETIC ZONE15
Maxillary incisor pretreatment CAD/CAM milled & finished restoration
45

Seminar -3
Finished CAD/CAM restoration placed
CASE 2. REPLACEMENT OF FAILING AMALGAMS
CAD/CAM conservative preparation design preserves more of the natural tooth structure compared with a crown and offers the clinical longevity of gold without the esthetic drawbacks. When using the current generation bonding adhesives according to the manufacturer’s instructions, the CEREC ceramic will recreate a tooth like strength
Amalgam restoration and caries pre-treatment preparation.
46

Seminar -3
Completed esthetic CAD/CAM restoration (IPSempress CAD)
INTEGRATED CHAIRSIDE—LABORATORY CAD/CAM TECHNIQUE
Requires two visits. The clinician either can scan the preparation directly and then send the scan to the
laboratory, or can take a traditional impression, after which a stone model is poured and the laboratory scans the stone model.
Chairside scanning of a preparation and digital transmission to the laboratory can be achieved by several systems.
CEREC Connect (Sirona) and iTero (Cadent) scans either take a series of stills and send the digital image either to a laboratory for milling of the restoration (CEREC Connect), or for milling of the coping at the manufacturer’s lab (iTero).
ceramic blocks for laboratory-milled restorations are available as Zirconia (zirconium oxide) and lithium disilicate glass blocks.
The external ceramic layer can be created either using press ceramics (in the same manner as for a traditional bridge) or layering ceramic material onto the substructure using a !ne brush and powder/liquid.
Advantages
Automates steps or all of fixed restorative fabrication Accuracy Less opportunity for error compared to traditional technique Opportunity to subcontract CAD/CAM to avoid capital costs Opportunity to focus on artistic ceramics Scanned image transferred directly to the laboratory from the office
47

Seminar -3
Reduced Chairside time Team approach to fixed restorations
Disadvantages
Requires two visits
Case Presentation: Integrated Chairside— Laboratory Technique
Preoperative view: discolored central incisor crown and veneer preparation with disparity in color
48

Seminar -3
Scanning image from dental office impression milled using CAD/CAM
In lab image of crown In lab image of veneer design
Poured model and CAD milled wax CAD ceramic blocks used for the restoration
49

Seminar -3
Milled restoration ceramic layering in process
Final seated crown and veneer
COMPARISON OF THE ALL CERAMIC SYSTEMS: 11
1. STRENGTH: All systems have adequate strength for single units but significantly less than that
of ceramic metal crowns. Ability of bonding to tooth structure provides additional strengthening
mechanism. Dicor is strengthened through the partial recrystallization of the glass through a
ceramming process. In-ceram has highest flexural strength values for all the ceramic system and can
be used for multiple unit bridges. IPS Empress and Optec pressable ceramic, strengthened by dispersion of Leucite
crystals throughout their internal structure. Duceram LFC, strengthened by an ion exchange mechanism involving hydroxyl
ions.2. FABRICATION TECHNIQUES:
With exception of Optec HSP and Duceram system, all ceramic system use specialcialized equipments and techniques. So can be considered disadvantage because of the added cost of fabrication.
50

Seminar -3
3. MARGINAL FITWith exception of the machined ceramics restoration, the fit of the all ceramic crowns to the underlying tooth structure is extremely accurate.Compenstion for discrepancy or gaps can be made by using resin cements.
4. WEAR OF OPPOSING TOOTH STRUCTURE: All of the Leucite containing all ceramic materials wears opposing natural
tooth. IPS Empress>Optec HSP>Optec OPC>Dicor> Duceram
ALL-CERAMIC POSTS AND CORES:
Endodontically treated teeth often need a post and core as foundation for the final restoration.' The restoration of anterior nonvital teeth with metal posts and cores and all-ceramic restorations may lead to compromised aesthetics because of the semi translucence of ceramics and the opacious metal substructure of the underlying post and core. Depending on the thickness and the opacity of the luting cement and the all-ceramic restoration, the metal post and core may shine through or at least decrease the depth of translucency of the restoration.' In addition, metal posts may also shine through in the cervical root areas, thus altering the appearance of thin gingival tissue.'' Furthermore, especially when nonprecious alloys are used for post-and-core fabrication, corrosion products may deposit in the gingival tissues or cause root discoloration. Almost simultaneously with the introduction of the current all-ceramic systems, the use of the all posts and cores was suggested as an alternative to solve the esthetic problems that metal posts and cores exhibit.
ADVANTAGES:
Dentine like shade it is related to the deeper diffusion and absorption of the transmitted light in the ceramic core mass
An all ceramic restorations transmits a certain percentage of the incident light to the ceramic core and the post on which it has been placed thus the color of the final restorations will be derived from an internal shade similar to optical behavior of the natural teeth
Does not reflect intensively through thin gingival tissues. It provides an essential depth of translucency in the cervical root areas
Excellent biocompatibility and does not exhibit galvanic corrosion
51

Seminar -3
DISADVANTAGE:
Relatively low fracture strength and fracture toughness.
Dental Ceramic material used for all ceramic post and core
Ø Conventional dental ceramics
Ø High toughness ceramic - In ceram.
Ø Dense sintered alumina ceramic - Procera.
Ø Zirconium oxide ceramics
Techniques or construction of all ceramic post and core with high toughness ceramic materials
Ø Slip casting technique
Ø Copy milling technique
Ø Two piece technique
Heat press technique
SLIP CASTING TECHNIQUE:
described by Kem and Knode in 1991 core buildup and post are made in 1 piece from the aluminum oxide
ceramic material, In-Ceram. Used only in wide root canals without a crucial reduction of the circumferential
dentin structure.
COPY MILLING RECHNIQUE:
the glass-infiltrated alumina ceramic, In-Ceram, and its fabrication process have been adapted to the Celay copy-milling method (Mikrona), as an alternative to the slip-casting technique. The Celay system involves a rnanually guided copy-milling process in which a predesigned resin pattern is surface traced and copied in ceramic. The ceramic substructures are prefabricated blanks made of presintcrcd aluminum oxide ceramic (Celay Alumina Blanks, Vita Zahnfabrik), In-Ceram ceramic restorations made with the Celay method present a 10% higher flexural strength (about 500 iVlPa) than do conventional In-Ceram restorations.
52

Seminar -3
This method can be used for inlay, onlay, veneer,and crown-and-bridge framework fabrication,as well as for copy-milled In-Ceram posts and cores.
TWO-PIECE TECHNIQUE:
Because the fracture strength of In-Ceram posts and cores is less than that of metal posts and cores, In- Ceram posts and cores have only been recommended
for wide root canals." The cases of regular root canals (smaller than ISO 110), In-Ceram ceramic does not seem to provide a sufficient strength; for that reason, until presently, an all-ceramic post and core was not recommended for such eases. After the recent development of zirconia ceramic posts, it became possible to combine both materials. For a 2-piece post-and- core construction a post made of yttrium oxide-partially stabilized zirconia (ER-Cerapost, Brasseler) is used in conjunction with an all-ceramic core made of alumina or alumina-magnesia'-* ceramics, fabricated either by the copy-milling or the slip-casing technique. The zirconia ceramic posts are commercially available in three ISO sizes (050, 090, 110} and supplement the existing ER-Post system (Brasseler).
HEAT-PRESS TECHNIQUE
The heat-press technique has recently found application to an all-ceramic post-and-core construction. It is based on the well-known IPS Empress system (Ivoclar). In this system, a castable, precerammed Leucite-reinforced glass-ceramic material is heated and pressed in an investment mold after the burnout of the wax analog (lost-wax technique). In the heat-press technique, a glass-ceramic core (EmpressCosmo, Ivoclar) is heat- pressed over a prefabricated zirconium dioxide post (Cosmo Post, Ivoclar), and therefore both materials are fused into a solid post-and-core restoration.17
OTHER APPLICATION OF CERAMICS
Ceramics in Medical Applications
Ceramics are employed in a wide range in the medical specialty such as repair and replacement of human hips, knees, and other body parts ,diseased heart valves. The applications are based on the fact that when used as implants or even as coatings to metal replacements, ceramic materials can stimulate bone growth, promote tissue formation and provide protection from the immune system.
53

Seminar -3
Moreover, modern ceramic materials play an important role in gadgets used for medical diagnosis including both ultrasonic and X-ray computed tomography (CT) systems. Transducers utilizing lead zirconate titanate (PZT) based piezoelectric ceramics are the heart of ultrasonic systems. These transducers generate the ultrasonic acoustic waves and detect the reflected signals to form the image.
Gadgets for Dental Applications.
Various recently introduced diagnostic and working tools of which ceramics play an integral part include:
Radio Visio Graphy (RVG) Pulp tester Apex locators 1st generation - resistance based. 2nd generation - impedance based 3rd generation - frequency based.
Piezo Ceramics
Piezoelectricity can be defined as pressure electricity which is a property of certain classes of crystalline materials including natural crystals of Quartz, Rochelle salt and Tourmaline plus manufactured ceramics such as Barium Titanate and Lead Zirconate Titanates (PZT). When mechanical pressure is applied to one of these materials, the crystalline structure produces a voltage proportional to the pressure. Conversely, when an electric field is applied, the structure changes shape producing dimensional changes in the material. The piezoelectric materials use polycrystalline ceramics instead of natural piezoelectric crystals. They are more versatile with physical, chemical and piezoelectric characteristics able to be tailored to specific applications. The hard, dense ceramics can be manufactured in almost any given shape or size, which are chemically inert and immune to moisture and other atmospheric conditions.
Bioceramics
Bioceramics are a group of ceramics, which are biologically active materials rich in calcium and phosphate. Hydroxyapatite and tricalcium phosphate are similar in composition to bone and teeth and can be used for augmentation of alveolar ridges and filling bony defects. They are manufactured and are available in block, granular and injectable forms. These bioactive materials are packed in the required site providing a scaffold for new bone growth and are Osseo-inductive in nature. The various forms of bioceramics are Single crystals (Sapphire), Polycrystalline (Hydroxyapatite) Glass (Bioactive glass) Glass ceramics (Ceravital) Composites (Stainless steel reinforced Bioglass)
Types of Bioceramics
54

Seminar -3
There are about four types of bioceramics:
INERT: Attached by compact morphological fixation. e.g, Alumina, Carbon
POROUS: Attached by vascularisation through pores. e.g, Porous Alumina.
SURFACE ACTIVE: Directly attach by chemical bonding with bone.e.g, Bioglass, Hydroxyapatite
RESORBABLE Designed to be slowly replaced by bone.e.g, Tricalcium Phosphate4
CONCLUSION:
There has been a revolution in the provision of ceramics for dental restorations in the last 15 years, such that now all-ceramic restorations can be used both anteriorly and posteriorly.There is no doubt that new materials and processing routes will continue to be developed and that ceramics will play a growing role in the provision of aesthetic restorations. Therefore need for dental practitioners to be aware of the rapidly changing field of dental ceramics to ensure that the correct choice is made for each patient.
REFERNCES1. Chu S, Ahmad I. Historical perspectives of synthetic ceramics and traditional
Feldspathic porcelain.Pract Proced Aesthet Dent 2005; 17(9):593-598.2. Kelly JR, Nishimura I, Campbell SD. Ceramics in Dentistry : historical roots and
current perspectives. J Prosthet Dent 1996 ; 75 :18-32.3. Santander SA, Vargas AP, Escobar JS, Monteiro FJ, Tamayo LFR. Ceramics for
Dental restoration –An introduction. Dyna 2010; 77(163):26-36.4. Sukumaran VG, Bharadwaj N. Ceramics in dental applications. Trend
Biomater.Artif.Organs2006; 20(1):7-11.5. Giordano R, McLaren EA Ceramics Overview: Classification by Microstructure and
Processing Methods. The Compendium of Continuing Education in Dentistry 6. Griggs JA. Recent Advances in Materials for All-Ceramic Restorations. Dent Clin
North Am. 2007; 51(3): 713–727.7. Sikri V.textbook of operative dentistry.1st edition,CBS publishers & didtributors,
New Delhi India,chapter 19,pg439-481.8. Anuvanice KJ (Ed) Phillips RW. Phillips Science of Dental Materials. 11th Edition,
WB Saunders Company, Pennsylvania, USA, Chapter 21, pg692.
55

Seminar -3
9. Al-Ajlouni RF, Wahadni AA, Khasawneh S. Dental porcelain: composition,types,glazing and clinical applications. Dental news 1999;6(3):33-37.
10.Mclean JW: The science and art of dental ceramics,vol.1,quintessence publ.co;Chicago,1979,p.72.
11.Rosenblum MA, Schulman .A review of all ceramic restorations.J Am Dent Assoc1997; 128:297-307
12.Qualtrough AJE ,Piddock V.Ceramics update,J Dent 1997;25:9113.Sneha SM, Abhilasha S. Bhasin.CAD/CAM in dental restorations: an overview
Annals and Essences of Dentistry Vol. - II Issue 3 July – Sept. 201014.André V. Ritter,Chairside CAD/CAM in Dentistry JERD15( 2 ), 2002 15.James Klim, Corrales KV .Innovation in Dentistry: CAD/CAM Restorative
Procedures 16.Denry S, Holloway JA. Ceramics for Dental Applications: Review Materials 2010,
3, 351-368.17.Koutayas SO, Kern M. All ceramic posts and cores: the state of the art.
Quintessence international, 1999; 30(6):383-392.
56