
Dementia with Lewy Bodies - University of Pittsburgh
13
10/30/2020 1 Dementia with Lewy Bodies Sarah B. Berman, M.D., Ph.D. Associate Professor Department of Neurology Director of DLB Programs Alzheimer Disease Research Center Pittsburgh Institute for Neurodegenerative Diseases University of Pittsburgh October 29, 2020 Outline • What is Dementia with Lewy Bodies? – How it differs from Alzheimer’s disease – How it differs from Parkinson’s disease • Diagnosis • Treatment strategies – Multi-faceted • Research/Future directions Dementia with Lewy Bodies • Second most common neurodegenerative dementia – Second only to Alzheimer’s disease • Prevalence – About 5% (1-25%) of all dementias 1 2 3
Transcript of Dementia with Lewy Bodies - University of Pittsburgh
10/30/2020
1
Dementia with Lewy Bodies
Sarah B. Berman, M.D., Ph.D.
Associate Professor
Department of Neurology
Director of DLB Programs
Alzheimer Disease Research Center
Pittsburgh Institute for Neurodegenerative Diseases
University of Pittsburgh
October 29, 2020
Outline
• What is Dementia with Lewy Bodies?
– How it differs from Alzheimer’s disease
– How it differs from Parkinson’s disease
• Diagnosis
• Treatment strategies
– Multi-faceted
• Research/Future directions
Dementia with Lewy Bodies
• Second most common neurodegenerative
dementia
– Second only to Alzheimer’s disease
• Prevalence
– About 5% (1-25%) of all dementias
1
2
3
10/30/2020
2
Lewy Body Diseases
• Dementia with Lewy Bodies (DLB)
• Parkinson’s Disease and
Parkinson’s Disease Dementia
• Multiple Systems Atrophy (MSA)
• All have Lewy Body pathology
– Abnormal protein aggregates; contain
ubiquitin and a-synuclein
– DLB: in cortical and brainstem neurons
– Also termed ‘Synucleinopathies’
– Very common for people with DLB to
also have Alzheimer’s pathology Spillantini et al., Nature 1997
Lewy Bodies
Clinical Features
• DLB has both cognitive and motor signs
– can be confused with both Alzheimer’s and
Parkinson’s disease
– Will focus on how to differentiate each one
1) cognitive changes
2) motor changes
Dementia with Lewy Bodies
Dementia
4
5
6

10/30/2020
3
Prominent Patterns of Cognitive Changes
DLB
• Executive Function
• Visuospatial
• Memory usually later
Other features
• Fluctuating consciousness
• Hallucinations
– Usually well-formed
(people, animals)
– Illusions also
Alzheimer’s disease
• Memory
• Language, executive
function
Hallucinations, fluctuations
less common
Dementia with Lewy Bodies
Cognitive Changes
Dementia
Hallucinations
Changes in alertness
Parkinsonism
“Motor” Symptoms:• Rest tremor
• Bradykinesia (Slowness of
movement)
• Rigidity
• In DLB, usually symmetric
• Balance difficulty
• Shuffling gait
• Stooped posture
• Softer voice; less facial
expression
• Smaller writing
Rest tremor
Turning ‘en bloc’
Stooped posture
Medlink Neurology
www.medlink.com
Video removed
7
8
9

10/30/2020
4
Postural instability
Medlink Neurology
www.medlink.com
Video removed
Freezing of gait
Medlink Neurology
www.medlink.com
Video removed
Signs can be subtle- Rest tremor
- Bradykinesia
Nutt JG and Wooten GF. Diagnosis and
Initial Management of Parkinson's
Disease. N Engl J Med
2005;353(10):1021-7.
Video removed
10
11
12

10/30/2020
5
Dementia with Lewy Bodies
Cognitive Changes
Dementia
Hallucinations
Fluctuating
consciousness
Parkinsonism
REM sleep disorder
REM Sleep Behavior Disorder (RBD)
• During REM sleep, when dreams occur, the
body is normally paralyzed (atonia)
• In RBD, the paralysis doesn’t occur
– Acting out dreams
– Talking in sleep
– Can be violent
Dementia with Lewy Bodies
Cognitive Changes
Dementia
Hallucinations
Fluctuating
consciousness
Parkinsonism
REM sleep disorder
Supportive Features
• Autonomic insufficiency
• Hyposmia
• Delusions
• Anxiety/depression
• Sensitivity to
antipsychotic
medications
13
14
15

10/30/2020
6
DLB DiagnosisMcKeith et al, 2017 Consensus Criteria
Dementia
2+ Core Features
• Parkinsonism
• Visual Hallucinations
• REM sleep disorder
• Fluctuating
consciousness
Dementia should start within 1
year of Parkinsonian motor
signs
• or else classified as Parkinson’s
disease dementia
Dementia
One Core Feature
• Parkinsonism
• Hallucinations
• REM sleep disorder
• Fluctuating
consciousness
Positive Biomarker
DLB DiagnosisMcKeith et al, 2017 Consensus Criteria
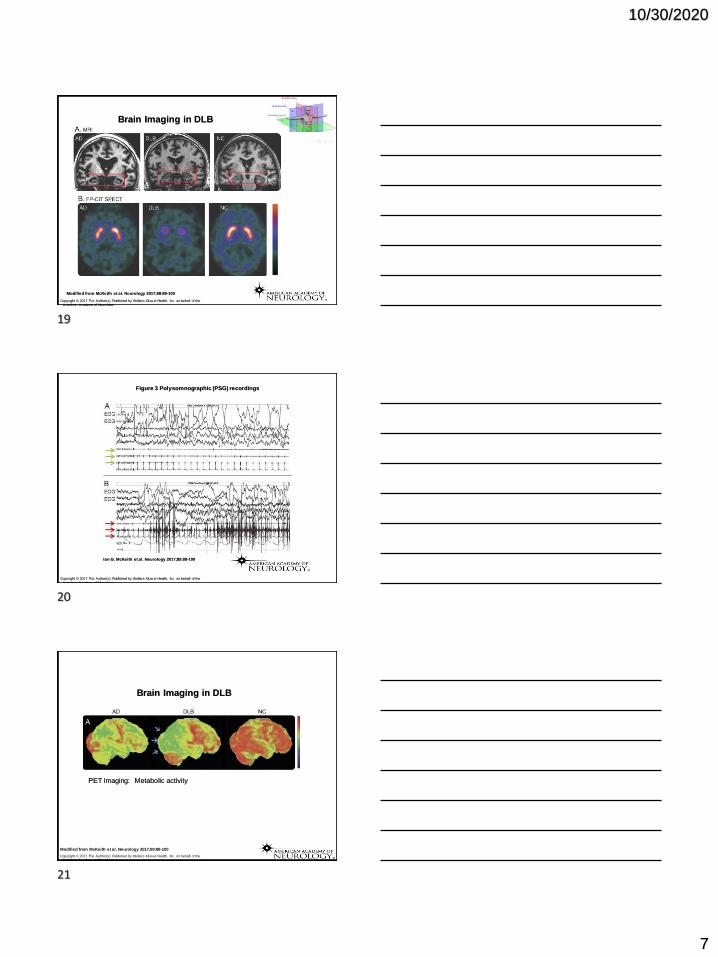
Biomarkers
Used in diagnosis
• Dopamine transporter SPECT (DaTscan)
– Motor symptoms of DLB due to loss of dopamine neurons
– Measures loss of striatal dopamine axons
• Cardiac MIBG scintigraphy
– Measures loss of sympathetic innervation
• Polysomnography
– Documents RBD (REM sleep without atonia)
Supportive but not used in diagnosis
• Diminished occipital metabolism (PET or SPECT scan)
16
17
18
10/30/2020
7
Brain Imaging in DLB
Modified from McKeith et al. Neurology 2017;89:88-100
Copyright © 2017 The Author(s). Published by Wolters Kluw er Health, Inc. on behalf of the
American Academy of Neurology.
My-ms.org
Figure 3 Polysomnographic (PSG) recordings
Ian G. McKeith et al. Neurology 2017;89:88-100
Copyright © 2017 The Author(s). Published by Wolters Kluw er Health, Inc. on behalf of the
American Academy of Neurology.
Modified from McKeith et al. Neurology 2017;89:88-100
Copyright © 2017 The Author(s). Published by Wolters Kluw er Health, Inc. on behalf of the American Academy of Neurology.
Brain Imaging in DLB
PET Imaging: Metabolic activity
19
20
21

10/30/2020
8
Dementia with Lewy Bodies
Dementia
Core Features
• Parkinsonism
• Hallucinations
• REM sleep disorder
• Fluctuating
consciousness
Biomarkers
Supportive Features
• Autonomic insufficiency
• Hyposmia
• Delusions
• Anxiety/depression
• Sensitivity to
antipsychotic
medications
Treatment Strategies
• Multifactorial and individualized
– No disease-modifying therapy available
– Address specific symptoms
• Complexities of treatment interactions
Treatment Strategies
Cognitive changes
• Acetylcholinesterase inhibitors
– Donepezil
– Rivastigmine (oral or transdermal)
– Galantamine
(Modified from Parsons et al.,
Neurotox Res, 2013)
X
XOften more noticeable
benefit in DLB than in AD
22
23
24
10/30/2020
9
Treatment Strategies
Psychosis (hallucinations, delusions)
• Cholinesterase inhibitors might be helpful
• AVOID typical antipsychotics (e.g., haloperidol)
• If necessary, the atypical antipsychotic quetiapine is a
better choice
– Less parkinsonism, better tolerated
– Or clozapine (but requires monitoring)
• Future targets?
– Serotonin-targeting medications
• Pimavanserin (Nuplazid) - Approved for PD psychosis, under review
by FDA for dementia-related psychosis
Treatment Strategies
Parkinsonism (motor symptoms)
• PT/OT/Speech/Exercise programs
• Levodopa
– How it works
– Risks in DLB
X
25
26
27

10/30/2020
10
Dopamine metabolism
L-DOPA DOPAMINE
3,4-DOPAC
3-Methoxytyramine
HVA
Dopamine metabolism
L-DOPA DOPAMINE
3,4-DOPAC
3-Methoxytyramine
HVABlood-brain barrier
DOPAMINE
Dopamine metabolism
L-DOPA DOPAMINE
3,4-DOPAC
3-Methoxytyramine
HVABlood-brain barrier
carbidopa
SINEMET®: L-DOPA + CarbidopaDOPAMINE
X
28
29
30

10/30/2020
11
Carbidopa/Levodopa
• Can help with
– Slowness
– Stiffness
– Shuffling walk/freezing
– Tremor
• Not as useful as in Parkinson’s disease
– Potential side effects
• Worsening hallucinations
DLB Complexities
Dopamine-related treatments
Levodopa
Quetiapine
Other anti-psychotics
DOPAMINE LEVELS
Parkinsonian motor sx
Hallucinations, Delusions
Treatment Strategies
Sleep Disturbance
• REM sleep behavior disorder (RBD)
– Melatonin, Low-dose clonazepam
Depression/Anxiety• SSRIs
– e.g., sertraline, escitalopram
• SNRIs
– e.g., venlafaxine
31
32
33

10/30/2020
12
Treatment Strategies
Apathy• Can be disabling and very difficult to treat
• SSRIs
• Cholinesterase inhibitors
• Stimulants?
• Dopaminergic medications
Treatment Strategies
Autonomic disturbances
• Orthostatic hypotension
– Conservative and Pharmacologic measures:
compression stockings, fludrocortisone, midodrine
• Urinary incontinence
– Try to avoid anti-cholinergics for urinary symptoms
• Constipation
– Diet, miralax or other agents
Treatments to AVOID
• Dopamine antagonists– Such as MOST antipsychotics (haloperidol, risperidone)
– If needed, consider Clozaril or Seroquel
– Includes anti-emetics Reglan, Compazine
• Anticholinergics– Such as Benadryl, over the counter sleep aids
• Dopamine agonists– Pramipexole, ropinirole, rotigotine
– Frequently worsen hallucinations, can cause encephalopathy,
behavioral changes
– Frequently used if misdiagnosed as Parkinson’s disease
34
35
36
10/30/2020
13
• We can ONLY treat the symptoms
• We don’t know how to stop or even slow
the disease
Neuroprotective therapies
– What causes the pathology?
– How do we stop the progression?
Therapeutic Challenges
Research/Future Directions
• Basic research studies
– Genetics
– Animal models
– Etiology of neuropathology and underlying mechanisms
• Clinical studies
– Multiple studies underway to characterize clinical progression
and biomarkers
– Critical for outcomes for future neuroprotective therapy trials
• Goals:
– Develop effective neuroprotective therapies to slow/prevent
progression
– Develop better symptomatic therapies
Lewy Body Disease Local
Research Opportunities
• Dementia with Lewy Bodies Consortium (DLBC) study: o Longitudinal study at Pitt ADRC and 8 other sites, with matching clinical and
imaging and CSF/blood biomarker data
o Goal: Support clinical research to discover biomarkers that will improve efficiency and outcome of Phase II clinical trials for DLB
o If interested in referring potential participants for evaluation:
o Donna Simpson, CRNP, MPH, Clinical Research Coordinator, ADRC
Phone: (412) 692-2717
• Mito-PET Brain Imaging Studyo MJFF-funded pilot study of a new PET brain imaging tracer
o May be a biomarker in DLB, PD, and PD dementia
o Goal is to develop biomarkers of early changes in the brain that can be used to
monitor therapeutic trials
o If interested in referring potential participants for evaluation:
o Patricia McGeown, RN, BSN, Clinical Research Coordinator, ADRC
Phone: (412) 692-2722
37
38
39


















