Dementia: Together Forever (Mobilising for best care, support and advocacy) E. Anthony Allen...
73
Dementia: Together Forever (Mobilising for best care , support and advocacy ) E. Anthony Allen Consultant Psychiatrist Consultant in Whole Person Health and Church-based Health Ministries Website: www.eanthonyallen.com 1
-
Upload
merry-dawson -
Category
Documents
-
view
230 -
download
0
Transcript of Dementia: Together Forever (Mobilising for best care, support and advocacy) E. Anthony Allen...
1
Dementia:
Together Forever(Mobilising for best care, support and
advocacy)
E. Anthony Allen
Consultant Psychiatrist
Consultant in Whole Person Health and Church-based Health Ministries
Website: www.eanthonyallen.com
2
• DEMENTIA IS THE #1 HEALTH PROBLEM WORLDWIDE FOR THE 21ST CENTURY
• Advances in dementia are far behind those made for Cancer and HIV
3
The Burden of Dementia:Not Uncommon and Exploding
• At least 1 in every 85 persons worldwide (or 1.2%) have dementia
• Approximately 1 in 20 (or 5%) of the population over age 60 in Jamaica
• With the percentage growth of our elderly population it will be 1 in 4 persons (or 25%) over 60 by 2050 !
• From 31.5 now to 115 million worldwide by 2050
• Alzheimer’s affects more than 17,300 persons locally
• The numbers are growing daily
4
The Burden of Dementia:Neglected
• A large percentage of persons undiagnosed locally and worldwide
• 28 million of 36 million persons worldwide with dementia are undiagnosed
5
The Burden of Dementia:Costly
• In the USA annual financial costs of AD patients can average US$25,000.00 for home care and US$50,000.00 for nursing home.
• In the USA, the national cost of caring for people with AD is about $100 billion every year.
• One dollar in every hundred produced by work worldwide is spent on dementia (1% of GMP)
• The worldwide cost is as much as the total money produced by the 18th richest of the 196 countries in the world.
6
Dementia :
Together ForeverWhat should be our collective response?
1. MOBILIZE AS A TEAM FOR BEST CARE TO THE WHOLE PERSON
Gain TEAMWORK AND
WHOLENESS LITERACY
7
For best care we need to understand dementia.
WHAT IS DEMENTIA?
A disease of COGNITION
COGNITION makes us Know and Understand?
8
Cognition is a function of the Brain that involves:
1. memory
2. using language
3. carrying out Learned Motor Behaviour (or doing things)
4. recognition of objects

9
Dementia• Progressive loss of
cognitive functions (two or more)
• Without impairment of
consciousness
(Different from Delerium which involves
both, leading to “Confusional state”)
10
Memory problems ?
Not always dementia ……..

11
• NORMAL AGEING• MILD COGNITIVE IMPAIRMENT
• DEMENTIA
(These can merge into each other)
Disorders of Mild Memory Function
12
NORMAL AGEING
• Aging
– Mild loss of memory: names and dates
– Verbal fluency remain intact and vocabulary may increase
– Intact activities of daily living
13
MILD COGNITIVE IMPAIRMENT: CRITERIA (Amer. Acad. Neurology)
• Memory complaints , by self and others
• Memory impairment identified by objective tests
• Normal cognitive function otherwise
• Intact activities of daily living
• Not demented
Risk increases 10% annually. 85% of persons develop dementia by age 85
.

14
How does Dementia show itself?
15
DEMENTIA: Clinical Presentation includes:
• COGNITIVE CHANGES
• MOOD AND BEHAVIOUR CHANGES
• IMPAIRED ACTIVITIES OF DAILY LIVING
16
Cognitive difficulties in two or more functions:• Memory
Is my forgetting such as names, telephone numbers and
where I put things affecting my function?• Language (Aphasia)
Am I forgetting common words or losing my trend of thought
while conversing?
• Learned motor behavior (doing) (Apraxia),
Do I have difficulty getting dressed or using objects like
the TV remote, telephone or stove?
• Recognizing (Agnosia,)
Am I losing recognition of objects and people’s faces?
• Executive Functions sequencing, planning, organizing
Am I having difficulty doing complex tasks like balancing my
cheque book or following the plot in TV movies and books?
17
DEMENTIA: Other features
• Problem Moods and Behaviors
depression, irritability, aggression, inappropriateness, agitation, apathy
• Changes in Activities of Daily Living
dressing, hygiene, handling money, household appliances, hobbies, social events
• Psychiatric symptoms (e.g. psychosis,
vulnerability to delirium)
18
Why is Dementia under-diagnosed ?
• Persons can compensate and conceal
in early stages
• Have high index of suspicion
• Ask caregivers/surrounding family and
friends

19
How can we screen for dementia?
Available Screening Tests
• Memory Impairment Screen
• Clock Drawing Test
• The AD8 (caregiver responses)
• And others

20
What are the main causes
of dementia?
21
• Degenerative Diseases of the brain– Alzheimer’s disease (Most common)– Lewy body disease (Second most common)– Parkinson’s disease (30% of patients)
• Vascular dementia (10 to 20%)• begins with stroke and progression step-wise, suggesting
recurrent vascular events
• Infectious Disease– Creutzfeldt-Jakob disease (prion proteins)
• Others
-- Huntington’s disease– Frontotemporal dementias – e.g. Pick’s disease– Wilson’s disease
22
Drugs (medication, alcohol), DeliriumDepressionMetabolic Disturbances (e.g. hypothyroidism) Nutritional Disorders (e.g. Vit. B12& Folic acid def.)
Tumors, Toxicity, Trauma to Head (e.g. subdural Hematoma)
Infectious Disorders (e.g. HIV, Syphilis)
REVERSIBLE DEMENTIA CAN OCCURDUE TO:
23
How is a diagnosis made?
1. Interview Diagnostic Instruments
• Mini Mental State Examination (Folstein)
– Maximum score 30
– Score <24 suggests delirium or dementia
– Less sensitive in people with higher levels of
education
24
1. Interview Diagnostic Instruments (contd)
• ADAS-Cog (Alzheimer Disease Assessment Scale-Cognitive)
(more thorough) • St. Louis University Mental Status
Examination (SLUMS) (for Mild Cognitive Impairment and dementia) is more sensitive
2.Neuropsychological testing
25
INVESTIGATIONS used to diagnose “reversible dementia” and causes of irreversible dementia
1.Physical and Neurological exam
2. Laboratory and other tests
• Electrolytes, BUN, creatinine, CA++
• CBC
• Thyroid studies
• ESR
• B 12
• Folate
• VDRL/FTA-Ab, ANA, Anti DsDNA.
• HIV Ab • Drug screen if appropriate
• EKG
• CXR
• CT/MRI
• LP if suspicion of infectious etiology
• Brain biopsy.
26
ALZHEIMER’S DISEASE:DIAGNOSED BY EXCLUSION
•There is no exact clinical test or finding that makes Alzheimer's disease unique.
• Brain imaging: may find brain atrophy due to extensive neuronal loss
•Diagnosis confirmed by histology of post-mortem brain
•These degenerative changes are little understood and thus difficult to treat as we would like
27
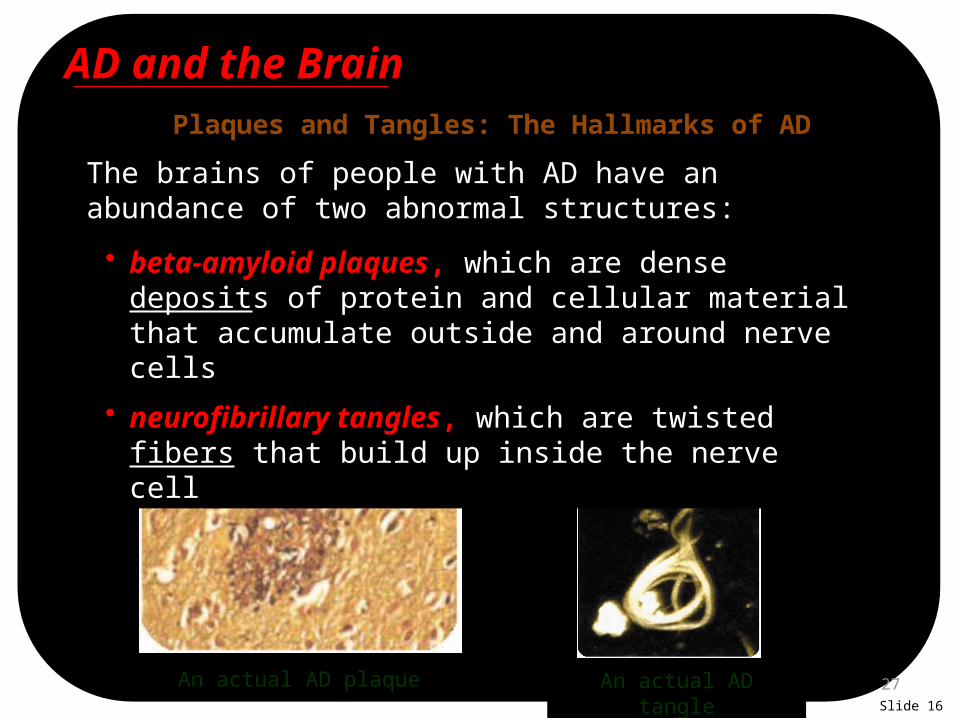
Plaques and Tangles: The Hallmarks of AD
The brains of people with AD have an abundance of two abnormal structures:
An actual AD plaque An actual AD tangle
• beta-amyloid plaques, which are dense deposits of protein and cellular material that accumulate outside and around nerve cells
• neurofibrillary tangles, which are twisted fibers that build up inside the nerve cell
AD and the Brain
Slide 16

28
Biochemical abnormalities in AD
Chemical Deficiencies:Problems with neurotransmitters
• Reduced levels of the acetylcholine (drugs whose side effects lower ACh levels in the brain can
cause reversible memory problems)
• Excessive or erratic glutamate stimulation (impairs learning and can cause neuronal toxicity.)
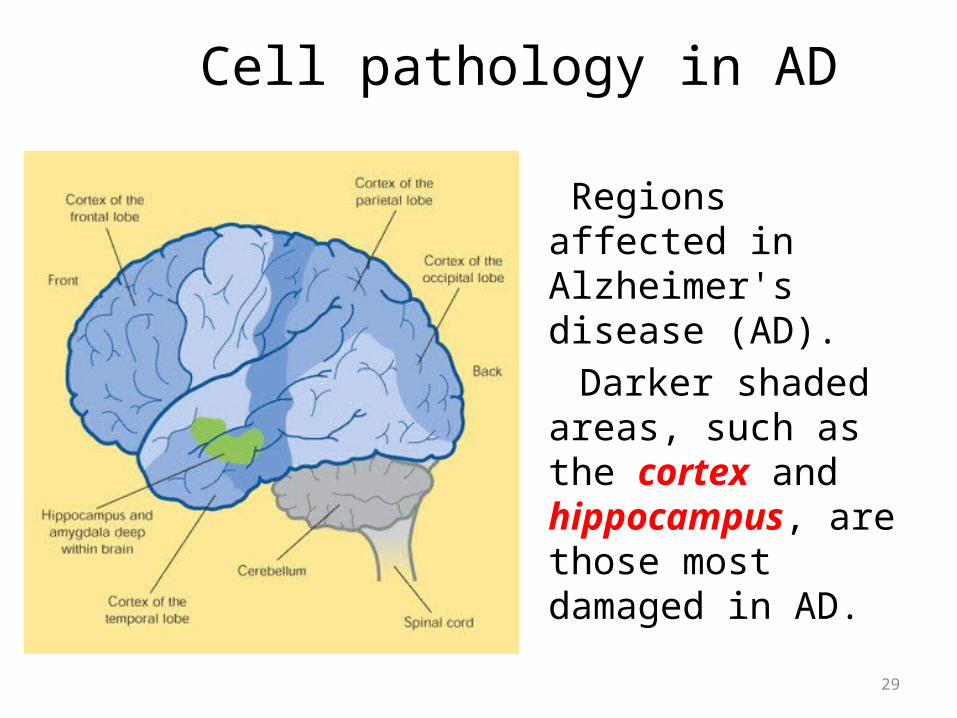
Cell pathology in AD
Regions affected in Alzheimer's disease (AD).
Darker shaded areas, such as the cortex and hippocampus, are those most damaged in AD.
29
30
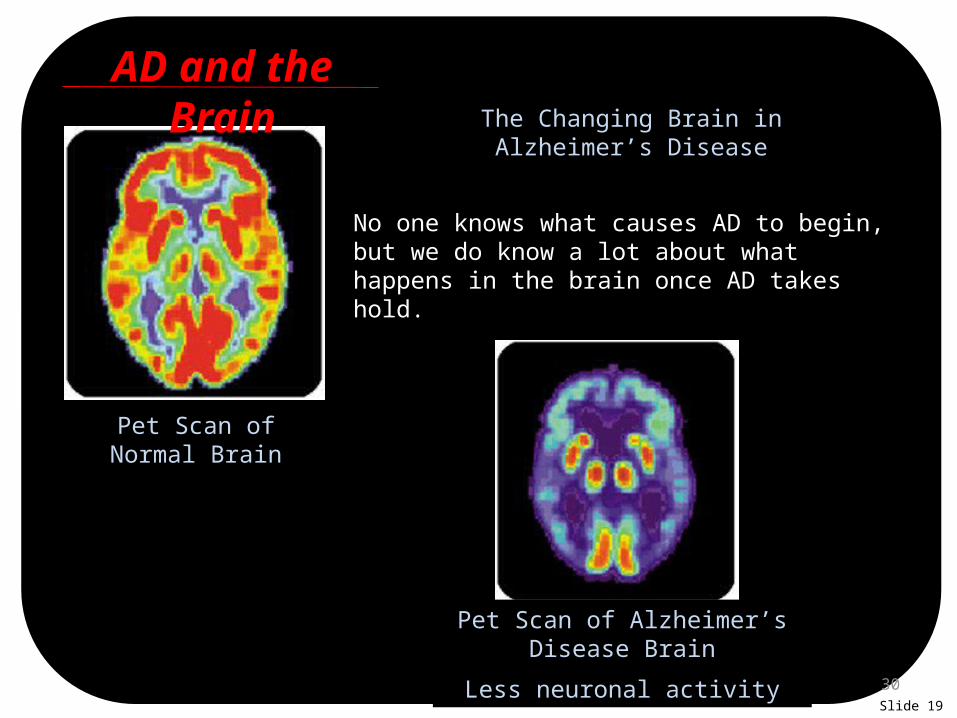
The Changing Brain in Alzheimer’s Disease
No one knows what causes AD to begin, but we do know a lot about what happens in the brain once AD takes hold.
Pet Scan of Normal Brain
Pet Scan of Alzheimer’s Disease Brain
Less neuronal activity
AD and the Brain
Slide 19
31
How does Alzheimer’s Disease progress?
32
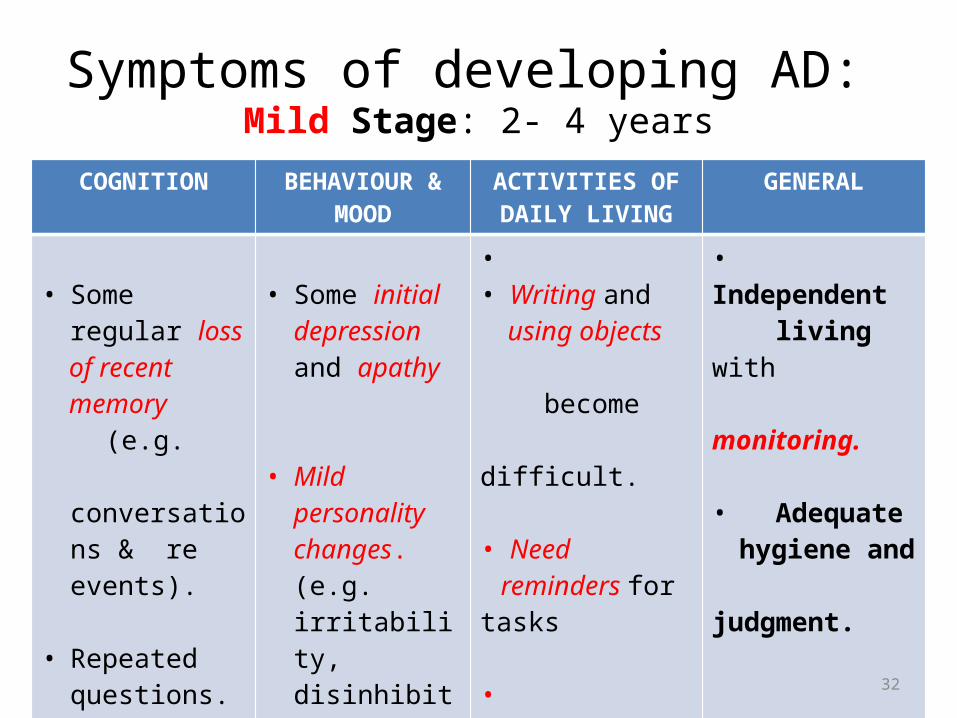
Symptoms of developing AD: Mild Stage: 2- 4 years
COGNITION BEHAVIOUR & MOOD
ACTIVITIES OF DAILY LIVING
GENERAL
• Some regular loss
of recent memory (e.g. conversations
& re events).
• Repeated questions. Problems expressing self and
understanding others
(language)
• Some initial depression and apathy
• Mild personality changes. (e.g. irritability, disinhibition, regression).
• • Writing and using objects become difficult.
• Need reminders for tasks
• Difficulties with sequencing impact driving.
• Independent living with monitoring.
• Adequate hygiene and judgment.
33
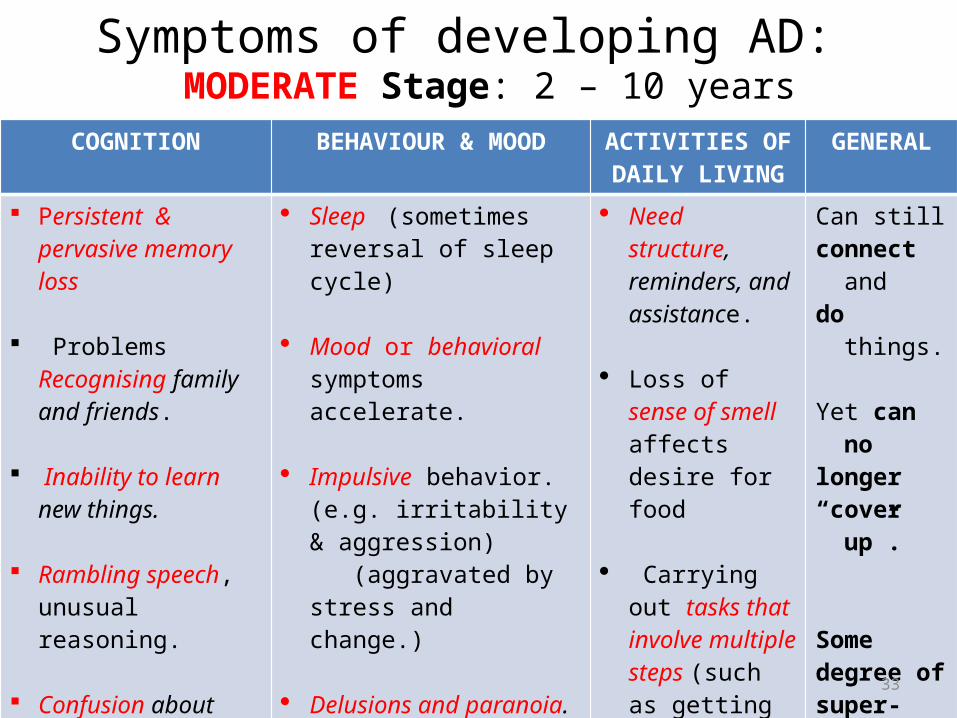
Symptoms of developing AD: MODERATE Stage: 2 – 10 years
COGNITION BEHAVIOUR & MOOD ACTIVITIES OF DAILY LIVING
GENERAL
Persistent & pervasive memory loss
Problems Recognising family and friends.
Inability to learn new things.
Rambling speech, unusual reasoning.
Confusion about current events, time,
and place. Lost in familiar
settings
Sleep (sometimes reversal of sleep cycle)
Mood or behavioral symptoms accelerate.
Impulsive behavior. (e.g.
irritability & aggression)
(aggravated by stress and change.)
Delusions and paranoia. Slowness, rigidity,
tremors, and gait problems impact mobility and coordination.
Need structure, reminders, and assistance.
Loss of sense of smell affects desire for food
Carrying out tasks that involve multiple steps (such as getting dressed)
Problems coping with new situations.
Can stillconnect
anddo things.
Yet can nolonger “cover up”.
Somedegree of super-Vision
needed
34
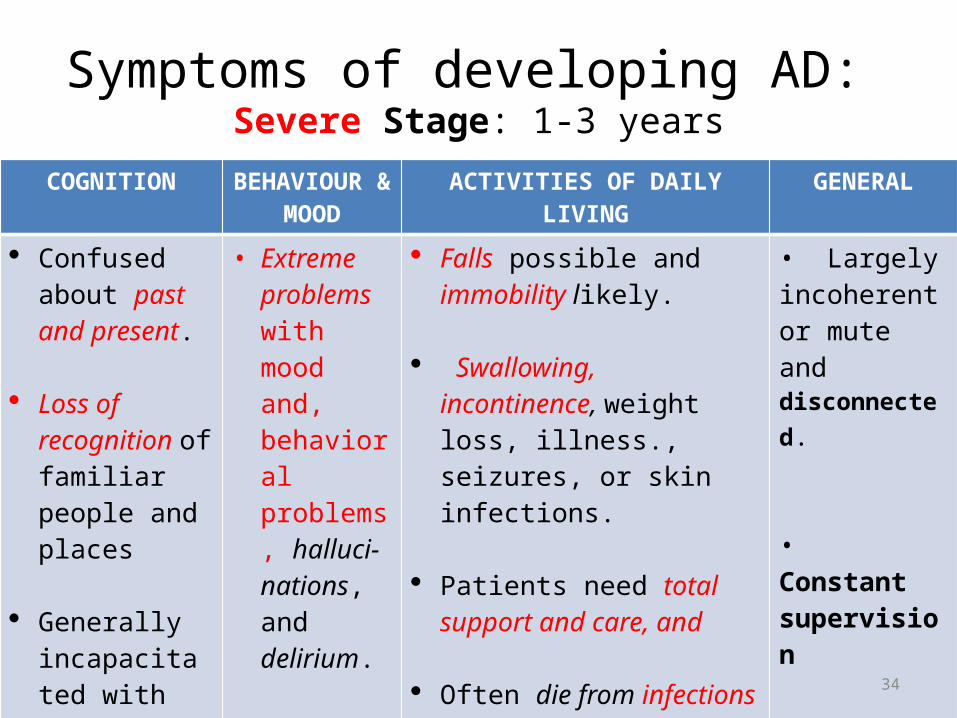
Symptoms of developing AD: Severe Stage: 1-3 years
COGNITION BEHAVIOUR & MOOD
ACTIVITIES OF DAILY LIVING GENERAL
Confused about past and present.
Loss of recognition of familiar people and places
Generally incapacitated with severe to total loss of verbal skills.
• Extreme problems with mood and, behavioral problems, halluci-nations, and delirium.
Falls possible and immobility likely.
Swallowing, incontinence, weight loss, illness., seizures, or skin infections.
Patients need total support and care, and
Often die from infections or pneumonia
• Largely incoherent or mute and disconnected.
• Constant supervision
35
I have Dementia. I need you !You have dementia. You need me !
Dementia:
Together Forever!
36
What is the best care for dementia?
• Goals: - Delay disease progression
- Improve quality of life
- Support dignity, self-respect
• Targets: - Cognition
- Behaviour and mood,
- Activities of daily living (function)
• Types: - Pharmacological
- Non-pharmacological
37
Best Care is –
A TEAM MATTER AND
A WHOLE PERSON MATTER
• The Whole Professional Team,• The Whole Community, and • The Whole Nation
together forever for• The Whole Person

38
Participating teams
• Professional Whole Person Team
Primary care and specialist Physicians, Psychiatrists/psychologists, Nurses, Social Workers, Pastors (Body, Mind, Social, Spirit)
• Community Team
- Patient at the centre! - Family - Other Caregivers- Friends- Neighbours - Congregation- Workplace
• Support and Advocacy Groups• Government Agencies
39
Pharmacological Treatment
• Alzheimer’s Dementia
– Cholinesterase Inhibitors • Donepezil (Aricept)• Galantamine (Remenyl)• Rivastigmine (Exelon)
– Memantine
– SSRI’s
40
Mild to Moderate Dementia
Cholinesterase Inhibitors
• Slows cognitive decline
• Slows ADL decline
• Affects behavioral measures
• Reduces caregiver burden
• Delayed nursing home placement
by 1.2 years

41
Between 70 to 90% of people with AD eventually develop behavioral symptoms, including sleeplessness, wandering and pacing, aggression, agitation, anger, depression, and hallucinations and delusions.
AD Research: Managing Behavioral Symptoms
Slide 35
42
PHARMACOLOGICAL BEHAVIOURAL MANAGEMENT
1. Antipsychotics: increased risk of death in elderly patients with dementia. Atypicals better tolerated.
2. Benzodiazepines: sedation, riskof falls, worsening cognition, repiratory supressant.
• Cautious use for prominent anxiety, infrequently otherwise.
• Lorazepam, Oxazepam have no active metabolites• Consider Buspirone for anxiety.
3. Possible benefit (open verdict): Valproate, Carbemazapine, Citalopram.
4. Periodically reduce or stop to assess ongoing need.
43
What can be done by the team apart from using
medication?

44
Team Factors for Success in Best Care
• Effective Communication• Conflict management for consensus• Appropriate education on Dementia for all• Seek guidance about what to anticipate • Have a plan of action discussed by all
(including the patient)• Exercise compassion & clarity with the patient
45
The Course of Dementia – Alzheimer’s Type
People usually live with AD anywhere from 2-10 years
Some can have it as long as 20 years.
Let us as teams enable the best quality of life possible in patients and our loved ones for these years! …..
Together forever! Team Care makes the difference
46
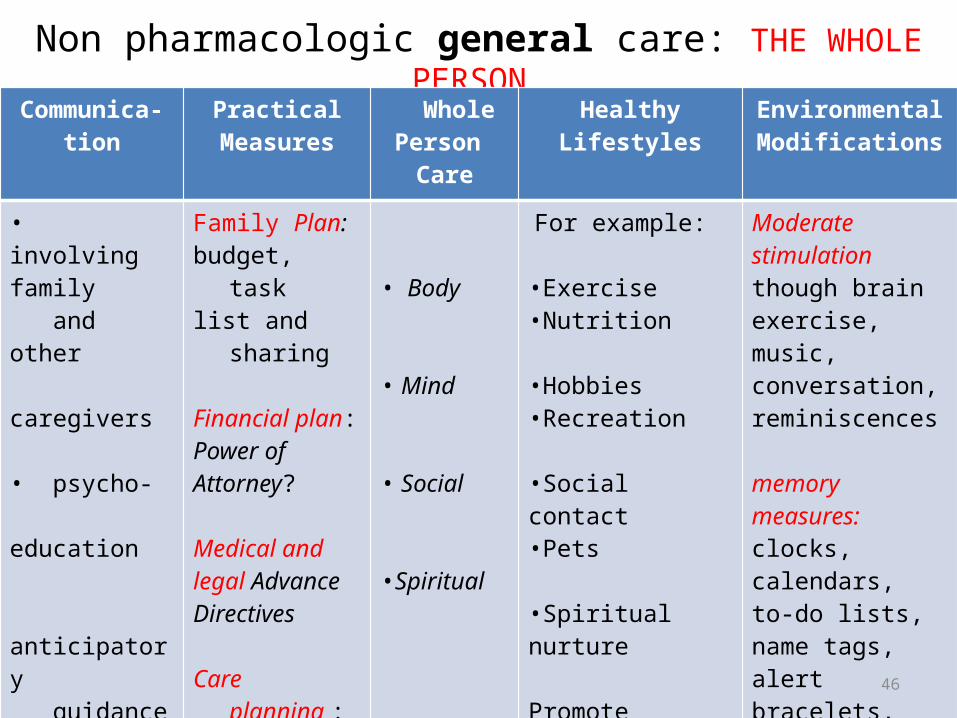
Non pharmacologic general care: THE WHOLE PERSON Communica-
tionPractical
Measures Whole
Person CareHealthy Lifestyles Environmental
Modifications
• involving family and other caregivers
• psycho- education anticipatory guidance • explicit plan
• compassion and clarity
Family Plan:budget, task list and sharing
Financial plan:Power ofAttorney?
Medical andlegal AdvanceDirectives
Care planning :personnel, daycare, assisted living, nursing home?
• Body
• Mind
• Social
•Spiritual
For example: •Exercise•Nutrition
•Hobbies•Recreation
•Social contact •Pets
•Spiritual nurture Promote maximum independence respect, validation and mobility
Moderate stimulation though brain exercise, music, conversation, reminiscences
memory measures:clocks, calendars, to-do lists, name tags, alert bracelets, home modification
Group meetings

47
Non-Pharmacological Behavioural Care:
ASSESS OVERALL SITUATION
ATTEND TO NEEDS
EDUCATE CAREGIVERS
- physical discomfort
- Hunger
- interpersonal issues
- change in living situation
- emotional difficulty
- frustration- boredom,- loneliness
- reassurance
- distraction - behavioral interventions (e.g. counselling, problem - solving)
Stay calm and be understanding
Be patient and flexible. Don’t argue or try to convince.
Acknowledge requests and respond to them.
Try not to take behaviors personally. Remember: it’s the disease talking, not your loved one
Experts encourage caregivers to try non-medical coping strategies first.
48
Dementia :
Together ForeverWhat should be our collective response?
2. WORK AS A TEAM
TO SUPPORT ALL CAREGIVERS
Gain CAREGIVER STRESS LITERACY

49
Where are people with AD cared for?
• family homes• assisted living facilities (those in
the early stages)• nursing homes (special care units)
Slide 6

50
Who are the AD Caregivers?• Spouses – the largest group. Most are older with
their own health problems.• Daughters – the second largest group. Called the
“sandwich generation,” many are married and raising children of their own. These children may need extra support if a parent’s attention is focused on caregiving.
• Grandchildren – may become major helpers. • Daughters-in-law – the third largest group. • Sons – often focus on the financial, legal, and
business aspects of caregiving. • Brothers and Sisters – many are older with
their own health problems.• Helpers, practical and registered nurses –
Often beat the brunt of behavioural problems• Others – friends, neighbors, members of the
faith community.
Support for Caregivers
Slide 37
51
Caregiver risks
• Grief (Denial, anger, bargaining,
depression, acceptance)
• Suspended life plans
• Conflicts of “role reversal”
• Exaggeration of pre-existing family conflicts and abuse
• Elder abuse
• Guilt
• Stress Distress Burnout
52
CARING FOR CAREGIVERS
• Have a Supportive Attitude, Empathy, Patience and promote Mutual Respect
• Provide Respite services (time off, outings etc)• Establish Support Groups• Provide special Skills Training for wholistic dementia team
care• Ensure Conflict resolution at all times with all others involved. • Problem solving• Promote Involvement in a Supportive Teamwork by all• Encourage Healthy lifestyles and health screening annually
and when necessary• Carryout Referral to services and resources for caregiver
needs and crises as necessary

53
Use Technology for Care giving
Computers can provide information and support to family caregivers through:
These features have become very popular among users because they reach many people at once, are private and convenient, and are available around the clock.
• websites• blogs• chat rooms• Q & A modules• medical advice forums
Support for Caregivers
Slide 39

54
Demands of Care giving
AD takes a huge physical and emotional toll. Caregivers must deal with changes in a loved one’s personality and provide constant attention for years. Thus, caregivers are especially vulnerable to physical and emotional stress.
• Peer support programs can help link caregivers with trained volunteers. Other support programs can offer services geared to caregivers dealing with different stages of AD.
• Jamaica Alzheimer’s Outreach Association
• 52 Duke St. 927 8967 [email protected]
Support for Caregivers
55
Dementia :
Together ForeverWhat should be our collective response?
3. Advocacy to prevent risk and suffering in Dementia
Gain WELLNESS PROMOTION LITERACY
56
What are the Common Risk factors for Dementia?
Understanding this will clarify our advocacy about what risks
to prevent, lessen or use to ensure early detection

57
Alzheimer’s Disease Research:
the Search for CausesAD develops
• AD develops when genetic, lifestyle, and environmental factors work together to cause the disease process to start.
Slide 24

58
Genetic Studies
The two main types of AD are early-onset and late-onset:
AD Research: the Search for Causes
• Early-onset AD is rare, usually affecting people aged 30 to 60 and usually running in families. Researchers have identified mutations in three genes that cause early-onset AD.
• Late-onset AD is more common. It usually affects people over age 65.
• Researchers have identified a gene that produces a protein called apolipoprotein E (ApoE). Scientists believe this protein is involved in the formation of beta-amyloid plaques.
Slide 25

59
Biochemical abnormalities in AD
Biochemical Changes in Growth (Trophic) Factors:
It is possible that one reason for nerve cell death
in Alzheimer's patients is a decline in growth-promoting factors that maintain the functioning of brain cells,
On the other hand there can be, a spontaneous
increase in factors that are toxins to brain cells.
60
Addressing MODIFIABLE RISK FACTORS( through Lifestyle & Environment change)
For Alzheimer’s disease as well
• Lacking of mentally stimulating activity & formal education
• Stress • Depression
Inclusive of other dementias as well• Toxins• Trauma
61
PROTECTING THE BRAIN
• Antioxidants: Vitamin E, Blueberries, Turmeric, Selenium
• Brain enhancers: Vitamin B Co, Omega 3 Fatty A’cids (e.g. Fish Oil, flaxseed)
• Lowering of Homocysteine : Fruit and vegetables (7-9 servings)
• Brain Neurotrophic Factor: Exercise
62
We can help prevent the
degree of suffering in Dementia by advocacy for
early detection and treatment
63
Demographic Risk Factors for
Alzheimer’s Disease(Permanent features that we can observe about the person)
– Age : 65 and over
– Female sex
– Family history
– Down’s syndrome
– Race: African American African-Caribbeans in Britain
& Hispanics > Caucasians
64
• Advocate for providing priority screening for these persons
• As well as those with - A high degree of modifiable risk factors - Memory difficulties
Genetic screening will become more accessible in the future
65
Experienced physicians can now diagnose AD with up to 90 percent accuracy. Early diagnosis has advantages:
• Doctors can rule out other and more treatable conditions that may cause dementia.
• If it is AD, families have more time to plan for the future.
• Treatments can start earlier, when they may be more effective for quality of life, costs and support.

66
LET US PREVENT BY ADVOCACY forInstitutional change
• We need a NATIONAL DEMENTIA POLICY by the Government and every institution including:
• 1. Screening skills and tools for every primary care physician,• 2. Specialist Dementia Clinics with Community Services for
all four health regions,• 3. Dementia Education, Day Centres and Caregiver Support
Groups by every community and Church,• 4. A designated officer in the Ministry of Health for
coordinating Dementia services. The integration of Dementia with Programme for Non-Communicable Disease (NCD) prevention.
67
Dementia:
Together ForeverTACKLING THE BURDEN
BY MOBILISING FOR BEST CARE, SUPPORT AND ADVOCACY
68
DEMENTIA:
Together forever!
• Mobilizing for the best quality of life for the Whole
Person
• Together for the best Whole Person Team Care • Together for support to all caregivers
• Together for Advocacy for prevention of risk and suffering
69
Let us mobilize • The Whole Professional Team• The Whole Community • The Whole Nation
together forever for• The Whole Person

70
•Together forever!• WE CAN DO IT !
“Let us live together as brothers and sisters
or perish together as fools” (Martin Luther King)

71
Thank You!

72
References1. Ahmed ,H. U. Dementia: An Overview. Retrieved on 25/03/11. from <http://www.slideworld.org/slideshow.aspx/Dementia-An-Overview-ppt-
2843227>
2. Anderson, H. S. Alzheimer’s Disease. Retrieved on 25/03/11, from< http://emedicine.medscape.com/article/1134817-overview>
3. Caring for Alzheimer’s Disease Patient. A publication of the Geriatric Mental Health Foundation
4. Dementia should be a national priority. (2009, September 17). The Gleaner,p.1.
5. Elizabeth, M. Alzheimer’s Disease: An Understanding of Alzheimer’s Disease. Retrieved on 25/03/11, from
www.curtis1.com/curtis/powerpoints/alzheimers.ppt
6. Johns Hopkins University Bloomberg School of Public Health (2007, June 11). Alzheimer's Disease To Quadruple Worldwide By 2050. Science Daily.
Retrieved March 29, 2011, from < http://www.sciencedaily.com /releases/2007/06/070610104441.htm>
7. Julian, K. Update in the Diagnosis, Treatment and Prevention of Dementia. Retrieved on 25/03/11, fromwww.ucsfcme.com/2009/slides/.../24_Dementia_Julian.pdf

References8. Misah, K. Alzheimer’s Disease and it’s Treatments. Retrieved on 25/03/10. from < http://faculty.smu.edu/jbuynak/alzheimers%20presentation.docx.ppt >
9. Practice Guidelines for the treatment of Psychiatric Disorders. American Psychiatric Association, Virginia
10. Publication on Alzheimer’s Disease. Alzheimer’s Disease: Unraveling the Mystery Retrieved on 25/03/11, from <
http://www.aapina.org/oldsite/GERO/resources/documents/Slides%20UnravelingtheMystery.ppt>
11. Redden, W. M. The Clinical Pharmacology of Approved AD Therapies. Proceedings of
panel discussion on Effective Treatment of Alzheimer’s Disease: Translating Guidelines into Practice at the Annual Meeting of the American Psychiatric Association 2009.
12. Tariq, S. H, Tumosa, N, Chibnall, J. T, Perry, H.M.,& Morley, J.E. November, 2006. The
Saint Louise University Mental Status (SLUMS) Examination for Detecting Mild Cognitive Impairment and Dementia . J am Geriatri Psych .
13. The World Alzheimer’s Report (2010). The Global Economic Impact of Dementia. Alzheimer’s Disease International: London. Retrieved 29/03/11, from <
http://www.alz.co.uk/research/files/WorldAlzheimerReport2010ExecutiveSummary.pdf>
/Datafiles/Wholness/Presentations/Powerpoint/Dementia/ Dementia, Together Forever, final 21.09.12

![WELCOME [] Javed Consultant Psychiatrist, CWPT, UK.; ... Afzal Javed Consultant Psychiatrist, CWPT; President Elect World Psychiatric Association (WPA)](https://static.fdocuments.net/doc/165x107/5b03a9017f8b9a2d518c7d47/welcome-javed-consultant-psychiatrist-cwpt-uk-afzal-javed-consultant.jpg)