Dell hildrens Comprehensive Epilepsy Center - … · Dell hildrens Comprehensive Epilepsy Center...
54
Dell Children’s Comprehensive Epilepsy Center Mark R. Lee, MD, PhD, FACS Pediatric Neurosurgery Co-Director of the Comprehensive Epilepsy Center Dell Children’s Medical Center Dave F. Clarke, MBBS, D-ABPN, D-ABCN, D-ABSM Pediatric Epileptologist Director of the Comprehensive Epilepsy Center Dell Children’s Medical Center
Transcript of Dell hildrens Comprehensive Epilepsy Center - … · Dell hildrens Comprehensive Epilepsy Center...
Dell Children’s Comprehensive Epilepsy Center
Mark R. Lee, MD, PhD, FACS Pediatric Neurosurgery Co-Director of the Comprehensive Epilepsy Center
Dell Children’s Medical Center
Dave F. Clarke, MBBS, D-ABPN, D-ABCN, D-ABSM Pediatric Epileptologist Director of the Comprehensive Epilepsy Center
Dell Children’s Medical Center

Disclosure Information AACPDM 70th Annual Meeting | September 20-24, 2016
Speaker Name:
Disclosure of Relevant Financial Relationships I have the following financial relationships to disclose:
Consultant for: (None)
Speaker’s Bureau for: (Lundbeck, Livanova)
Grant/Research support from: (GW pharmaceuticals, the Anderson Foundation)
Royalties from: (None)
Stockholder in: (None)
Honoraria from: (None)
Employee of: (None)

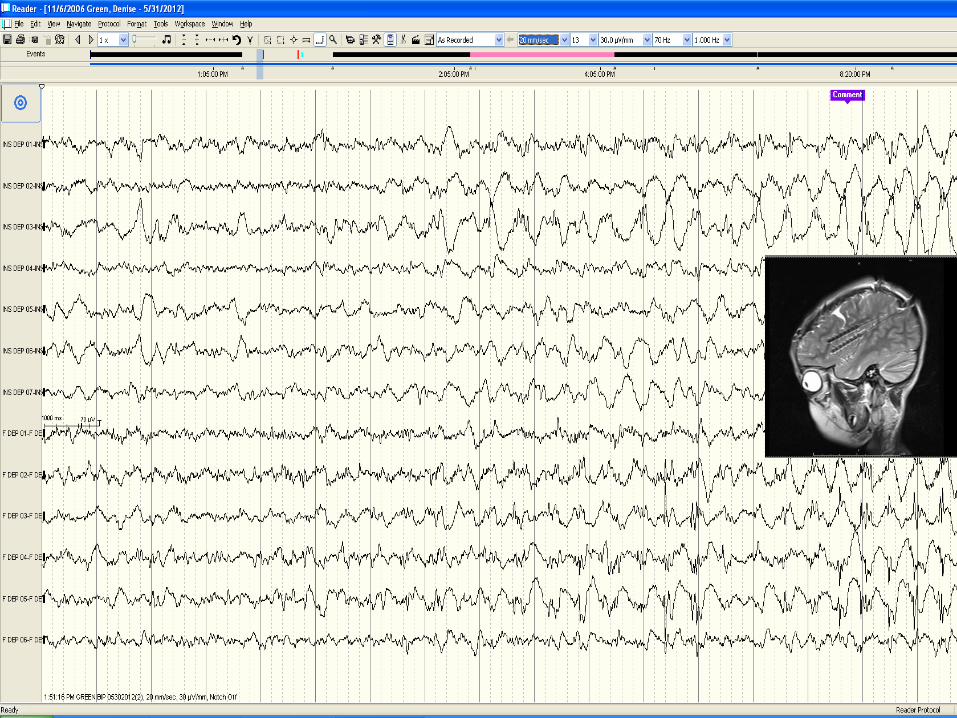
• 5 year old female with Focal onset epilepsy
• Presented in 8/2010 in EPC then focal status
• Eye dev to right, Focal Rt. hemi-body activity face followed by UE>LE
Case 1

Initial treatment of epilepsy Sankar R et al Neurology 2004;63(Suppl 4): S30-S39
Choices: Seizure type and Epilepsy Syndrome (Wheless JW, Clarke DF et al. 2007)
Tolerability Age specific toxicity
Overall Health Learning and Behavior
Phenobarbital and neurocognitive performance (Vining et al. Pediatrics 1987)
Impulsivity and Hyperactivity of Phenobarbital Behavioral adverse effects of Keppra Behavioral and cognitive abn. With Topiramate (Gerber et al.Pediatric Neurol, 2000)
Comorbidities (Dunn DW et al. Psychiatry et al. 1999;53(suppl 2):S17-23)
Depression ADD Migraine Symptoms of ASD ( Clarke DF et al. Epilepsia, 2005; Tuchman R J Autism Dev Disorder, 2000)
Sleepiness – May affect behavior (Clarke DF et al. 2005 )
Seizure frequency
Meds tried in this patient: Keppra, Vimpat, Ativan, Pht, Zonisamide failed to control her seizures
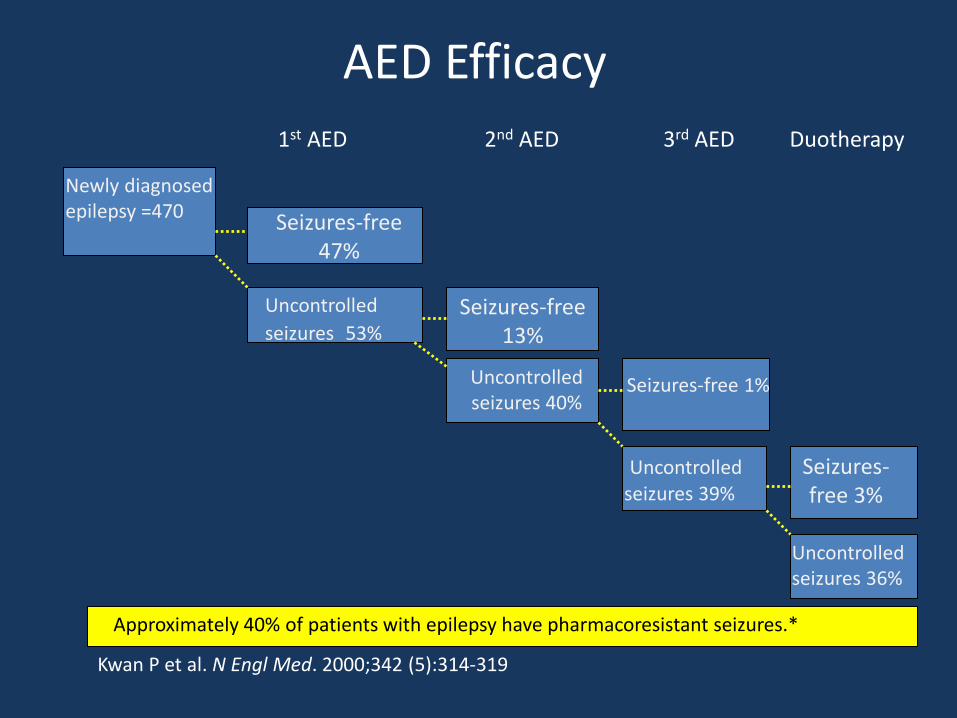
AED Efficacy
1st AED 2nd AED 3rd AED Duotherapy
Newly diagnosed epilepsy =470
Uncontrolled
seizures 53%
Uncontrolled seizures 40%
Uncontrolled seizures 39%
Uncontrolled seizures 36%
Seizures-free 47%
Seizures-free 13%
Seizures-free 1%
Seizures-free 3%
Kwan P et al. N Engl Med. 2000;342 (5):314-319
Approximately 40% of patients with epilepsy have pharmacoresistant seizures.*
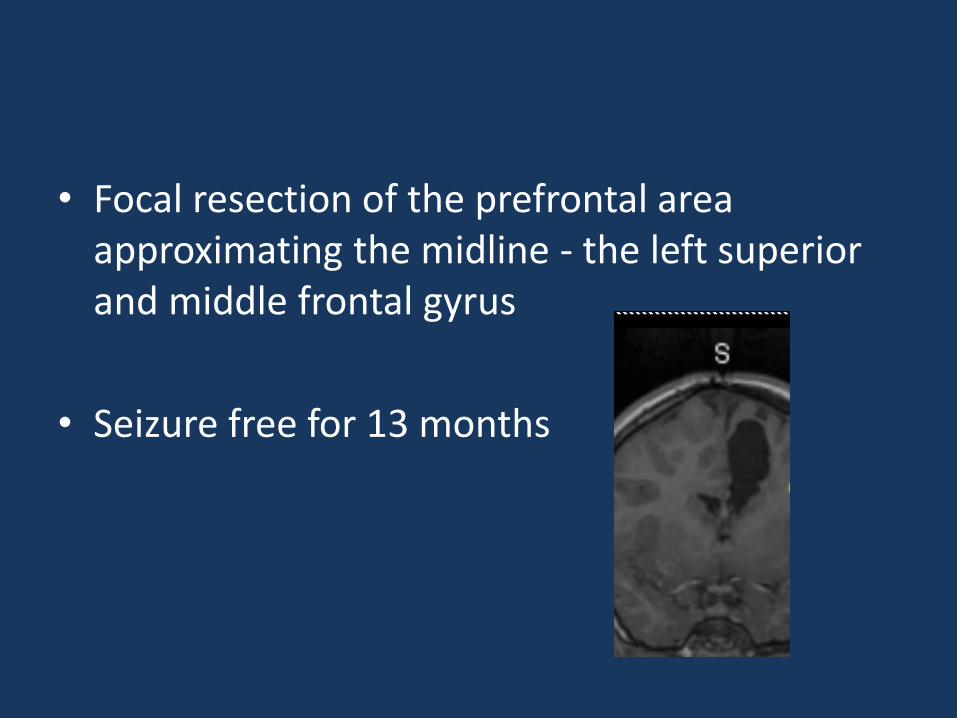
• Focal resection of the prefrontal area approximating the midline - the left superior and middle frontal gyrus
• Seizure free for 13 months
• Neuro-cognitively doing much better, socializing well
• 14 months after resection - Presents with elevation of right or bilateral upper extremity
• 2-3/wk
Does she have Epilepsy?
Tic disorder
Scope of the problem
• Methods: 127 children seen in a tertiary care First Seizure Clinic. (1 month -17 years)
• Results: – Non-epileptic in 31 (24%) and unclassifiable in two (2%).
– Pediatricians were more likely to refer true epileptic events (92%) than ED physicians (76%) or family physicians (65%).
– 15% - developmentally delayed; abnormal neurological exam - 11%.
• Conclusions: One quarter of children were incorrectly diagnosed as having
a seizure while the diagnosis of epilepsy was missed in over one-third of children.
Diagnostic Inaccuracy in Children Referred with “First Seizure”: Role for a First Seizure Clinic (L. D. Hamiwka et al., 2006)

Can we differentiate them clinically? Inter-rater reliability of Video versus EEG-Video
Monitoring (Benbadis SR et al., 2009)
• The video of 22 patients with Video-EEG were shown to 22 observers (Neurologists and epileptologists)
– Other test results were not provided.
– K-coefficients used – overall level of between method agreement beyond chance only.
• PNES – 0.57 moderate agreement
• Epilepsy - 0.69 high agreement
• Physiologic non-epileptic episodes – 0.09 low
Video
Generalized seizures?
Focal Secondarily generalized
Atonic Myoclonic
Video
Video Video
Video

Anti- epileptic drugs
2 or more seizures
EMU
Surgical candidate+/- Phase 2
Ketogenic Diet VNS
no yes
Surgical resection,
CC, Hemispherectomy
+/-
MRI, WADA, MEG, PET etc.
Stereotyped event ? EMU
Clarke DF, et al Epilepsy Surgery. Advance Therapy in Epilepsy, Shelton, CT, BC Decker, PMPH-USA 2009
Other Neuroimaging Modalities
• Single Photon Emission Computer Tomograpy (SPECT) - Evaluates cerebral blood flow
• Positive Emission Tomography (PET) - provides a photographic view of cerebral metabolism
• Magnetoencephalogram (MEG) uses the magnetic fields derived from the brains electric current to localize EEG dipoles
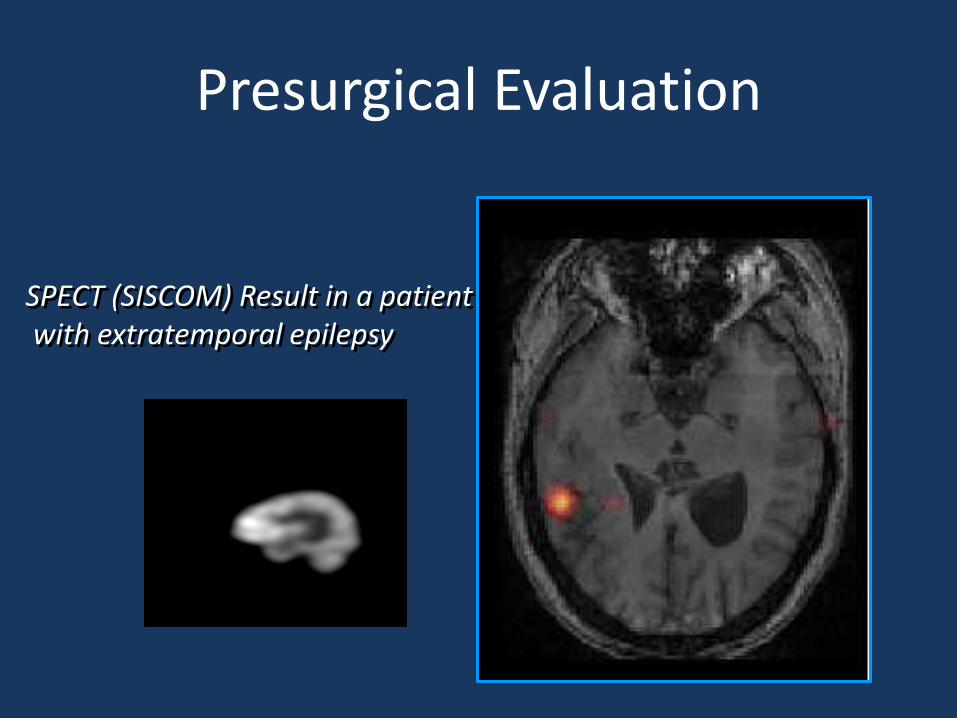
Presurgical Evaluation
SPECT (SISCOM) Result in a patient with extratemporal epilepsy
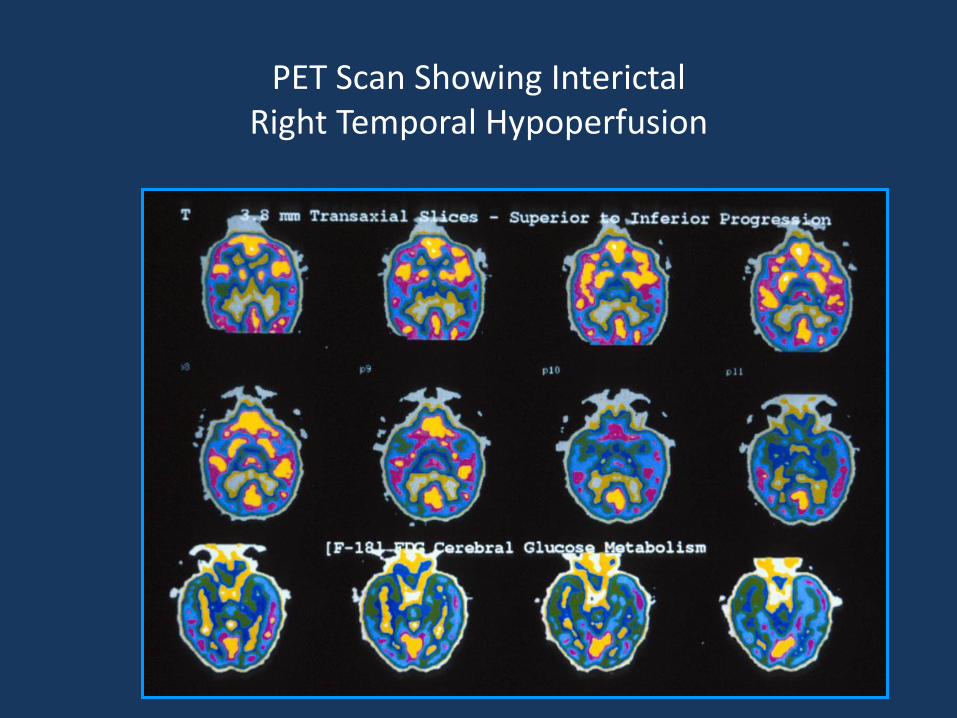
PET Scan Showing Interictal Right Temporal Hypoperfusion

500 milliseconds
MEG Localization of Brain Activity
Epileptic Spike
Magnetic Field Recordings
Magnetic Field Map
MEG/MRI Overlay
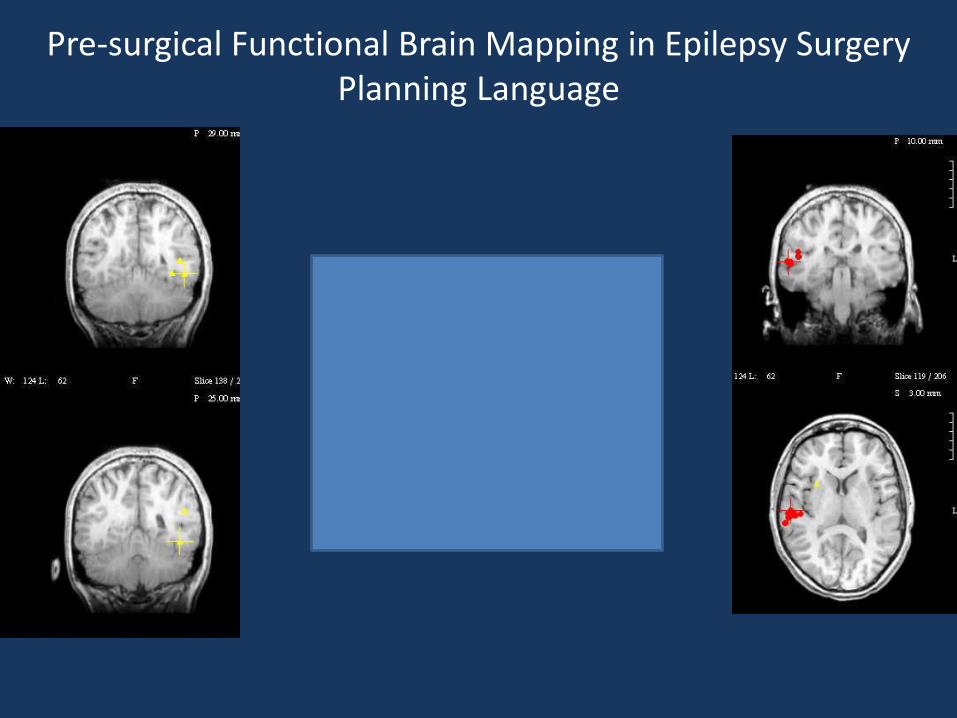
Pre-surgical Functional Brain Mapping in Epilepsy Surgery Planning Language
• Functional MRI (fMRI)
• Diffusion Tensor Imaging (DTI)/Tractography
Presurgical Functional Brain Mapping in Epilepsy Surgery Planning

fMRI
SJCRH Functional Neuroimaging Laboratory
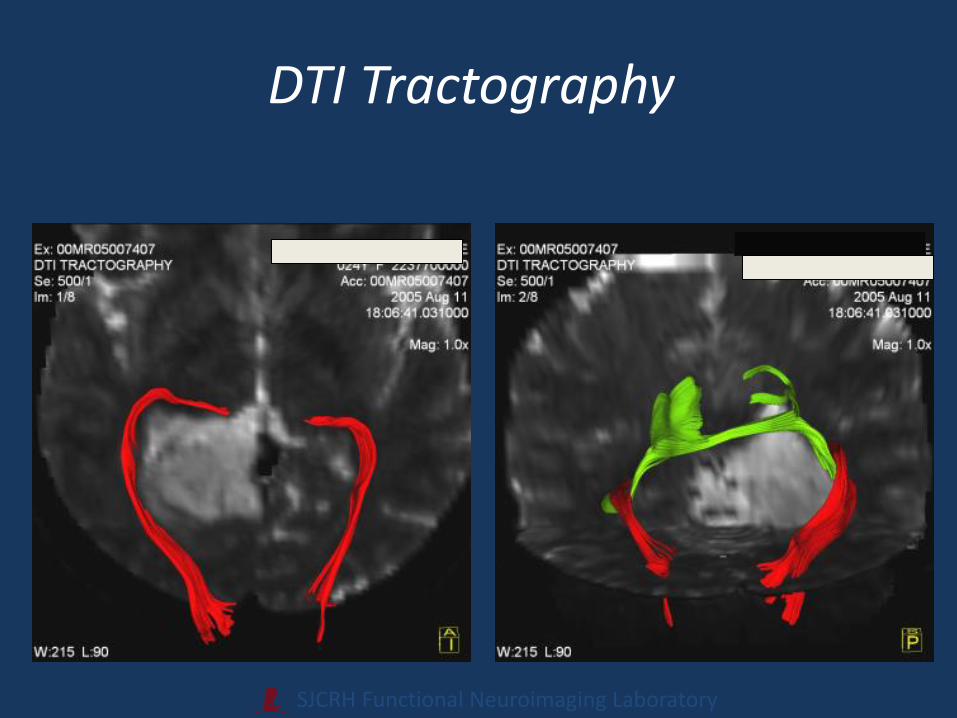
DTI Tractography

No LESION
LESION
Seizure Localization: VEEG +/- MEG, PET, SPECT
Function: fMRI MEG WADA
Subdural Electrodes with Cortical Mapping
LESIONECTOMY Not involving
Eloquent Cortex
Involving Eloquent Cortex or Function
Focal Seizure(s)
Anti-epileptic Medications

Back to the patient

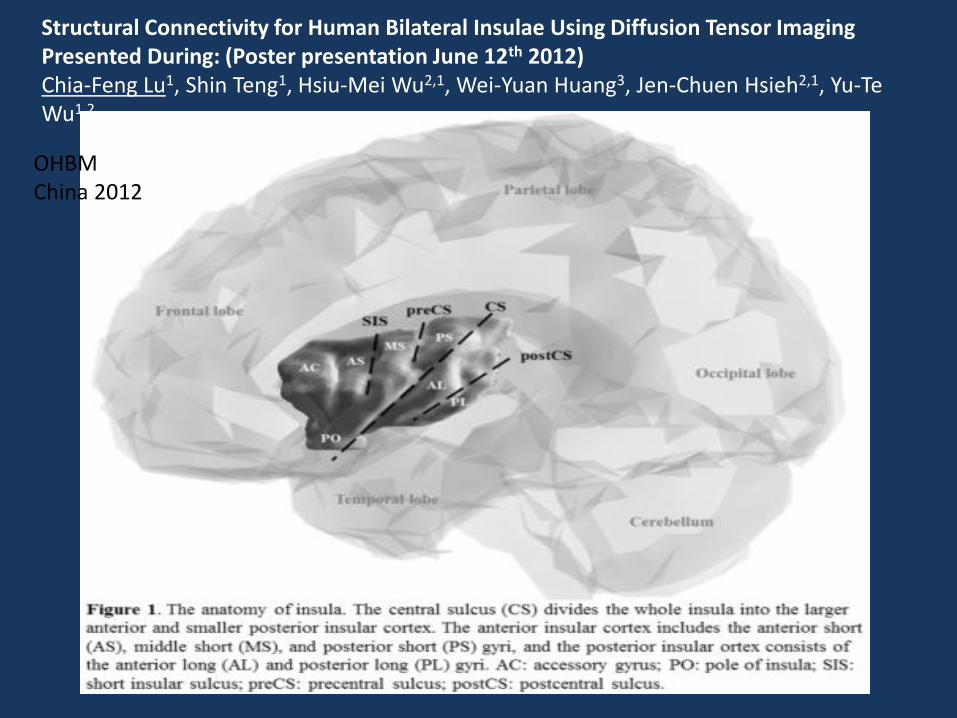
Structural Connectivity for Human Bilateral Insulae Using Diffusion Tensor Imaging Presented During: (Poster presentation June 12th 2012) Chia-Feng Lu1, Shin Teng1, Hsiu-Mei Wu2,1, Wei-Yuan Huang3, Jen-Chuen Hsieh2,1, Yu-Te Wu1,2
OHBM China 2012
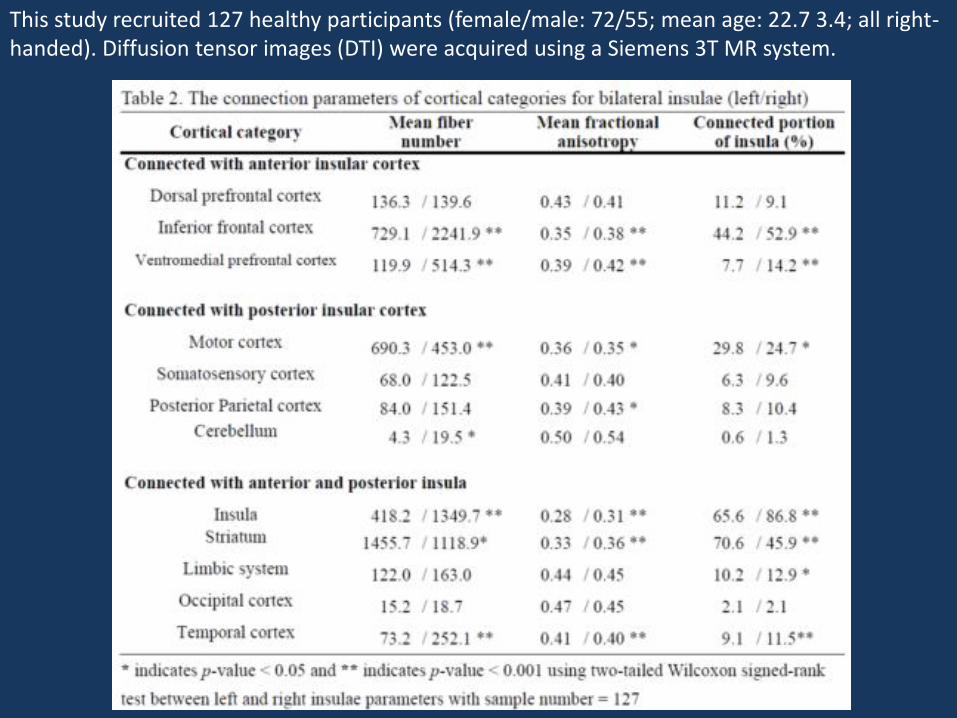
This study recruited 127 healthy participants (female/male: 72/55; mean age: 22.7 3.4; all right-handed). Diffusion tensor images (DTI) were acquired using a Siemens 3T MR system.


Follow up
• The patient is seizure free with no language nor motor deficits.

Epilepsy Surgery
• 60-85% of patients SEIZURE-FREE – cured, off all medications
• Majority of remainder markedly improved
• Traditionally, most epilepsy surgery performed on adults
• Vast majority of adults undergoing epilepsy surgery had seizures since childhood
• Pediatric epilepsy surgery becoming more common
If surgery works, why is epilepsy surgery “rare”?
• Neurologists’ training.
• New drugs.
• “Spontaneous remission”.

Natural History of Intractable Epilepsy
• Spontaneous remission is very rare
• Children with educational compromise – 5% become “normal” adults
• Behavioral and cognitive disorders
• Long-term (temporal lobe epilepsy) – 13 had surgery--all seizure free
– 45 declined surgery • 24 dead or in nursing facility
• none achieved seizure control

Psychosocial Price of Continued Seizures
• Poor peer relations
• Behavioral difficulties
• Poor school performance
• Depression, anxiety, poor self-esteem
• Irreversible disability into adulthood
• Family factors – social and economic
• Impact on cognitive development

Why Consider Brain Surgery for Intractable Epilepsy?
• Chance of seizure control is low
– 5% chance if failed 2 medications
• Multiple anti-epileptic drugs
– can have profound side-effects
– medications affect basic neuronal functioning
• Continued seizures are bad
– natural history and psychosocial price
• Surgery can have a high success rate
This is Brain Surgery
• Major complications are 1-3%
• Risk of surgery is related to location
• Modern techniques
– localization
– image-guided surgery • iMRI
– brain mapping
Ethical Considerations
• Risks of surgery
– serious morbidity or mortality (1-3%)
• Risks of no surgery
– profound influence on social existence
– undesirable effects of anti-epileptic drugs
– injury or death
Both surgical and nonsurgical treatment of intractable epilepsy have risks
Resective Epilepsy Surgery Requirements
• “Absolute” requirement
– epilepsy is focal
• needs to come from a discrete area
• needs to be localized ( “targeted”)
• Relative requirements
– epileptic brain tissue can be “safely” removed
• children make remarkable recoveries
• non-destructive techniques
– epilepsy poorly controlled with medication

Non-resective Epilepsy Surgery (palliative)
• Corpus callosotomy
– Excellent for “drop” seizures
– Anterior 2/3
– Complete
• Vagal nerve stimulation
– 50% patients have 50% decrease in seizures
Epilepsy Surgery
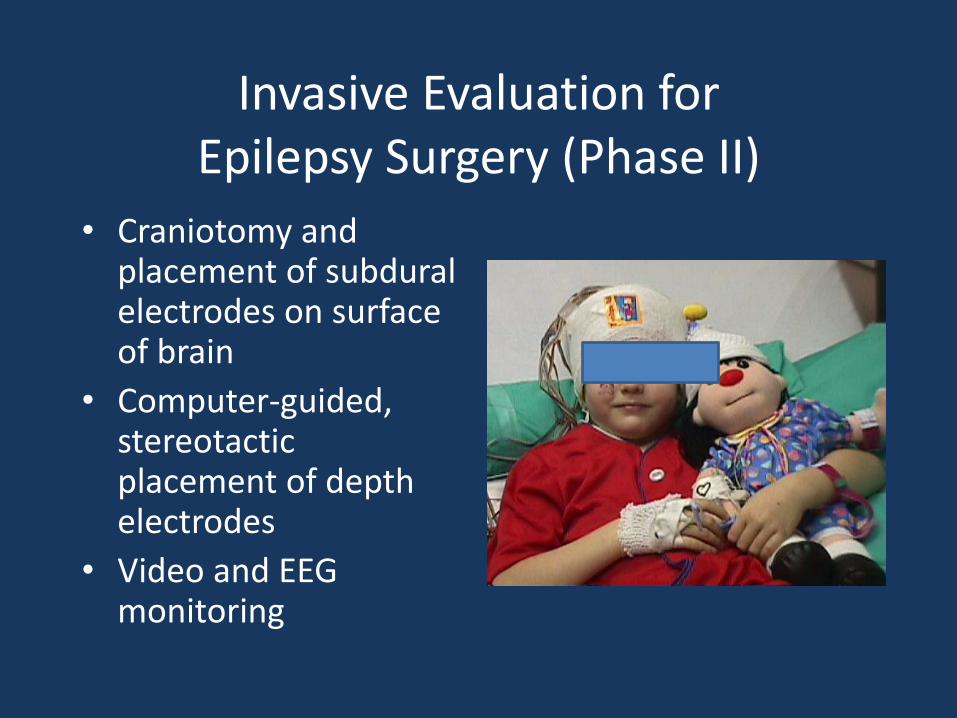
Invasive Evaluation for Epilepsy Surgery (Phase II)
• Craniotomy and placement of subdural electrodes on surface of brain
• Computer-guided, stereotactic placement of depth electrodes
• Video and EEG monitoring

Types of Epilepsy Surgery
• Extra-temporal resection (45%)
• Anterior temporal resection (25%)
• Hemispherectomy operations (15%)
• Corpus callosotomy (10%)
• Multiple subpial transection (5%)
• Vagal Nerve Stimulation
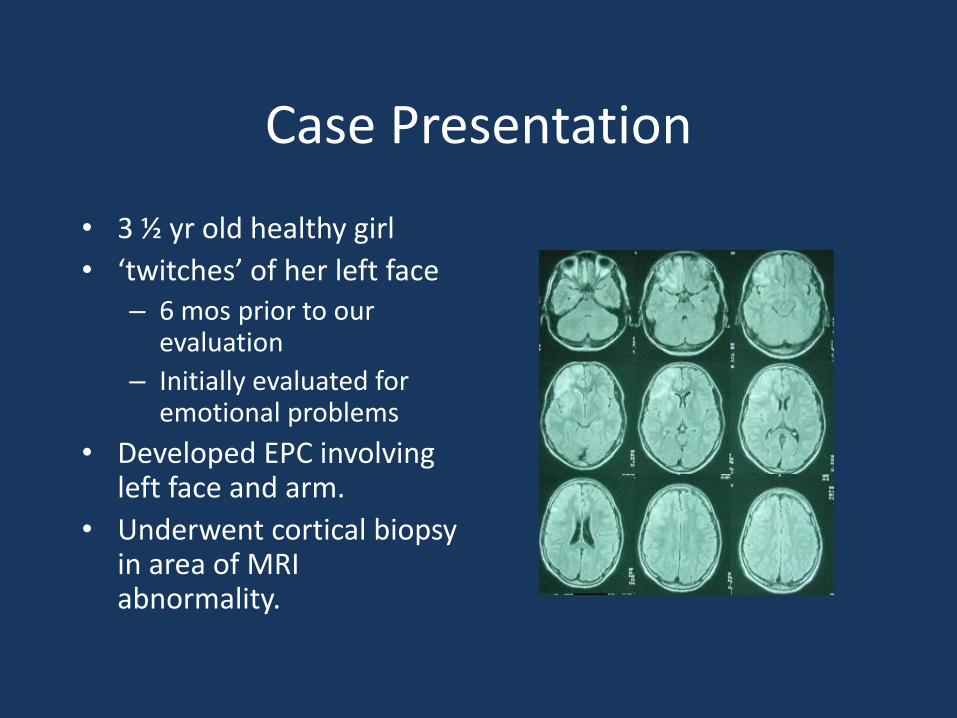
Case Presentation
• 3 ½ yr old healthy girl
• ‘twitches’ of her left face – 6 mos prior to our
evaluation
– Initially evaluated for emotional problems
• Developed EPC involving left face and arm.
• Underwent cortical biopsy in area of MRI abnormality.

Functional Hemispherectomy
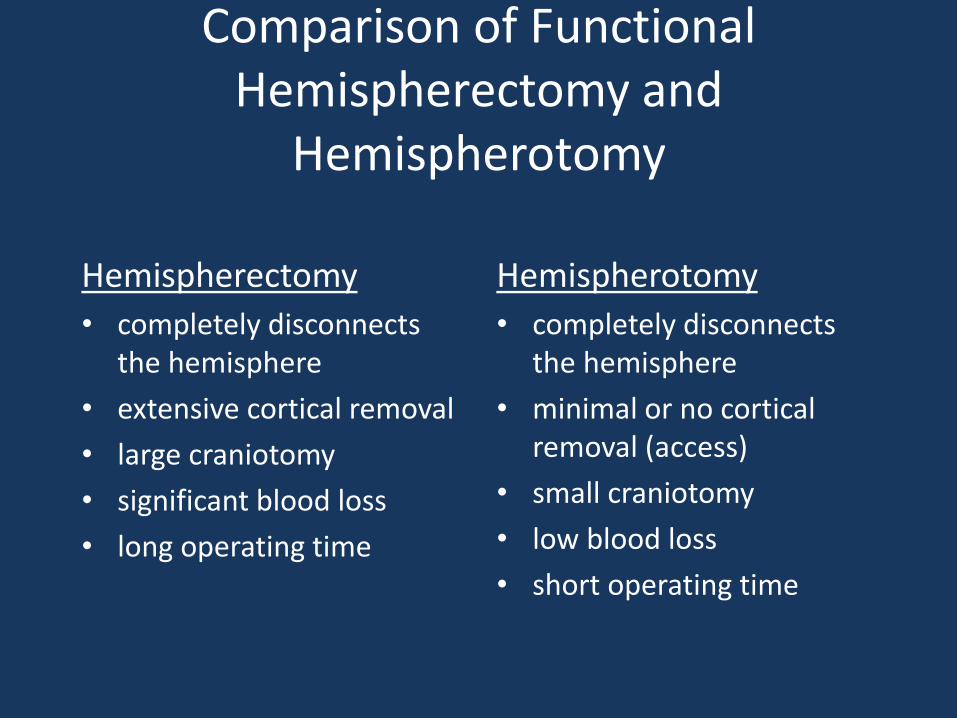
Comparison of Functional Hemispherectomy and
Hemispherotomy
Hemispherectomy
• completely disconnects the hemisphere
• extensive cortical removal
• large craniotomy
• significant blood loss
• long operating time
Hemispherotomy
• completely disconnects the hemisphere
• minimal or no cortical removal (access)
• small craniotomy
• low blood loss
• short operating time
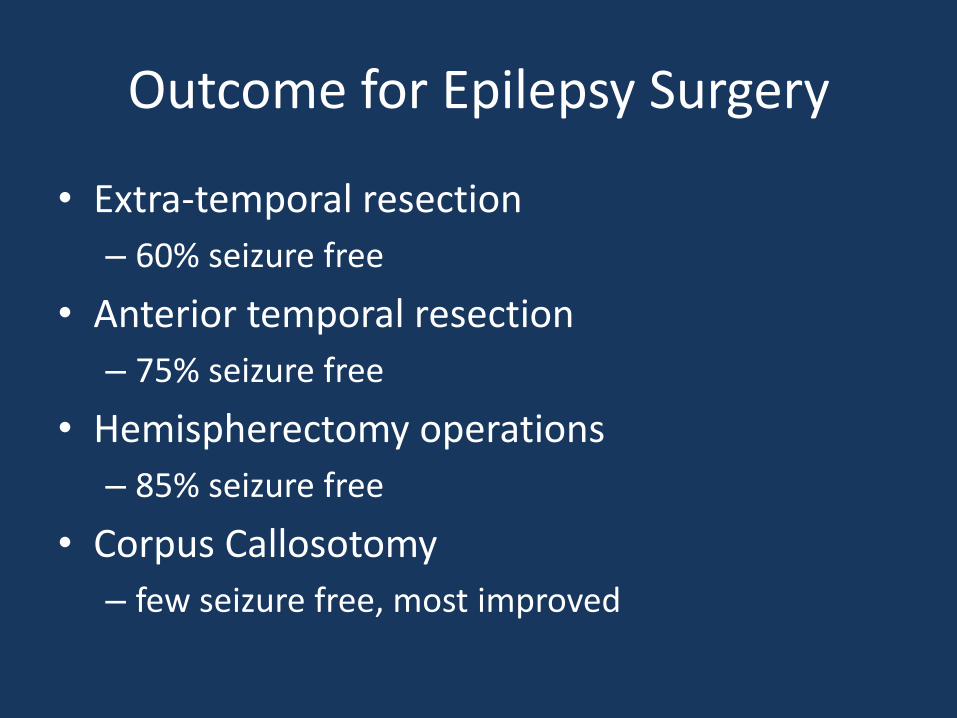
Outcome for Epilepsy Surgery
• Extra-temporal resection
– 60% seizure free
• Anterior temporal resection
– 75% seizure free
• Hemispherectomy operations
– 85% seizure free
• Corpus Callosotomy
– few seizure free, most improved
The Future of the Dell Children’s Medical Center Epilepsy Program
• Recruitment of outstanding clinicians
• Expansion of Epilepsy Monitoring Unit
• Expansion of epilepsy surgery program
• Availability of the best technology
– MEG
• Research
– Human Brain Laboratory
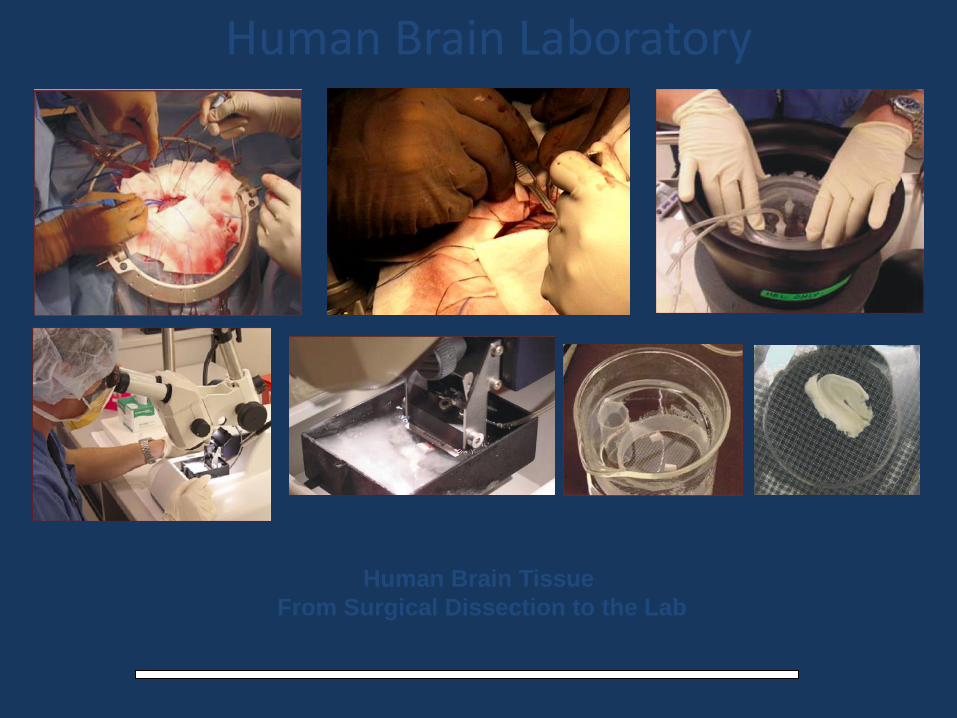
Human Brain Tissue
From Surgical Dissection to the Lab
10 m
Human Brain Laboratory
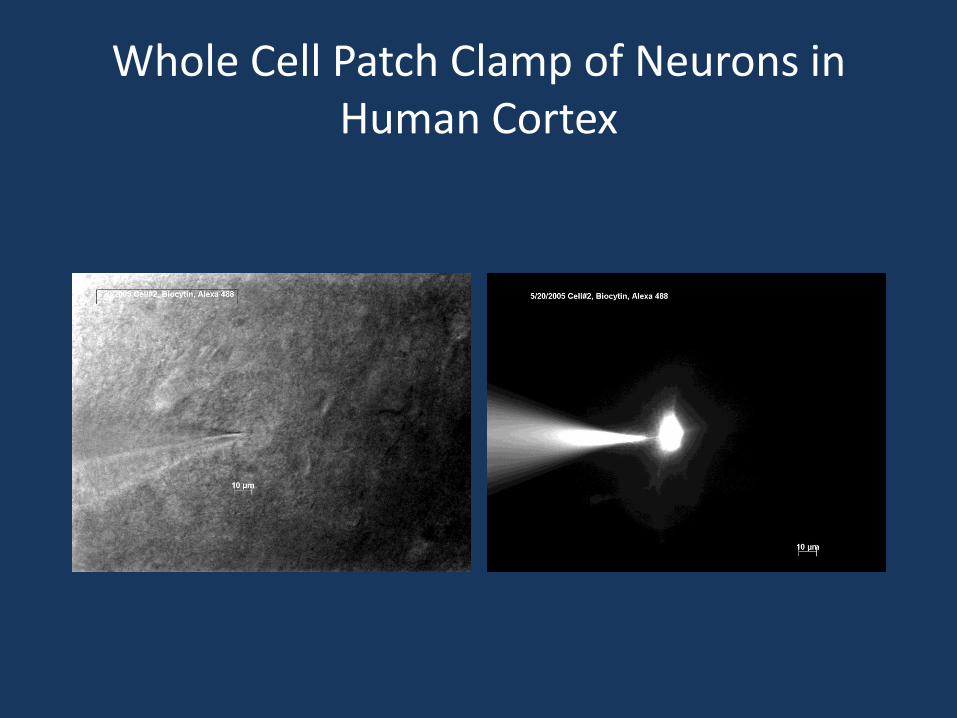
Whole Cell Patch Clamp of Neurons in Human Cortex

Immature Neurons in the Mature Human Epileptic Tissue.
The Role of Excitatory GABA
During development GABA acts as an excitatory neurotransmitter. Hypothesis: Seizure-induced deafferentation results
in pathological recapitulation of this developmental mechanism contributing to the formation of an epileptic network.
Mature cortical neuron. 16 y. old
Immature CA1 neuron. 17 y. old
Mature Immature0
25
50
75
AP
am
plit
ude (
mV
)
Mature Immature0
1
2
AP
half-w
idth
(m
s)
30 mV
100 ms
30 mV
100 ms 20 mV
2 ms
Mature neuron AP
immature neuron AP
800006000040000200000
Time (ms)
IN 0
(pA
)
-1300
-1200
-1100
-1000
-900
-800
-700
-600
-500
-400
-300
-200
0.0 ms
0.0 pA
2
0.0 ms
-378.4 pA
3
0.0 ms
0.0 pA
4
0.0 ms
-378.4 pA
1
GABA-mediated giant depolarizing potentials?
550005400053000520005100050000
Time (ms)
IN 0
(pA
)
-1050
-1000
-950
-900
-850
-800
-750
-700
-650
-600
-550
-500
-450
-400
-350
-300
5 µm
5 µm

Plasticity of Perisynaptic Astroglia during
Epileptogenesis in Human Hippocampus
11µµmm11µµmm
0.5 0.5 µµmm0.5 0.5 µµmm0.5 0.5 µµmm
• Astrogliosis is a prominent feature of
the epileptic brain and post-traumatic
seizures and chronic temporal lobe
epilepsy may originate from gliotic
scars.
• Pathologic activation of astrocytes may
have a role in the genesis of epilepsy,
through release of glutamate.
• Spillover of glutamate from excitatory
synapses contributes to activation of
astrocytic long distance calcium waves
and excite neurons along their path.
• Overall Goal: Reconstruct human
hippocampal normal tissue and epileptic
tissue to quantify ultrastructural
differences at the synaptic level.
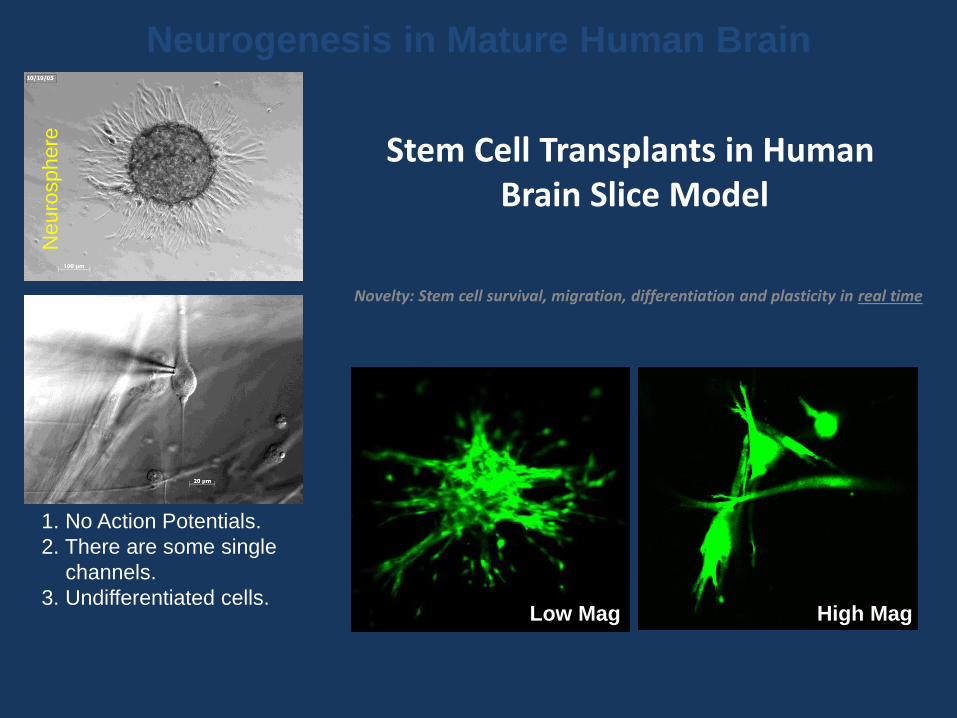
Stem Cell Transplants in Human Brain Slice Model
Novelty: Stem cell survival, migration, differentiation and plasticity in real time
Neurogenesis in Mature Human Brain N
euro
sph
ere
1. No Action Potentials.
2. There are some single
channels.
3. Undifferentiated cells. Low Mag High Mag

Human Human Cortical Slices as a Real-time Model
for Studying and Preventing Ischemic Injury
Funded by MCG Interdisciplinary Research Program
Principal Investigators: S.Kirov, D.Hess
AD
PIDs
Penumbra
PIDs - peri-infarct depolarizations
AD - anoxic depolarization
SD - spreading depression
Ischemic core
SDSD
SD
Control Oxygen-Glucose
Deprivation (OGD)
0 1000 2000 3000 4000
-80
-60
-40
-20
0
Cu
rren
t (p
A)
Time (ms)
0.5 nA
OGD
1 min
Mouse hippocampus Human Cortical Interneuron
Control OGD
13:25 13:45 13:55
500 m
PropagatingAD front
13:15 13:20
Intrinsic optical imaging in human cortical slices
Summary
• Resective epilepsy surgery is very effective and curative in many cases of poorly controlled epilepsy in children
• The Future is Bright!
– Expansion of the DCMC program
– New technologies (iMRI, MEG)
– Research (HBL)