Delirium in critically ill patients bogota043009
38
Acute Brain Dysfunction in the Critically Ill Patient: Data from recent delirium studies Pratik Pandharipande, MD, MSCI Anesthesiology/ Critical Care Vanderbilt University, Nashville, TN
-
Upload
hospira2010 -
Category
Documents
-
view
1.731 -
download
0
Transcript of Delirium in critically ill patients bogota043009

Acute Brain Dysfunction in the Critically Ill Patient:
Data from recent delirium studies
Pratik Pandharipande, MD, MSCIAnesthesiology/ Critical Care
Vanderbilt University, Nashville, TN

…The biggest problem is that “doctors are focused only on the organs that got patients into the hospital, ignoring newly acquired brain problems…”

Delirium• Disturbance of consciousness• Rapid onset• Fluctuating course• Inattention• Impaired ability to receive, process, store and
recall information• Perceptual disturbances- illusions,
hallucinations

Prevalence of ICU Delirium • 60-80% MICU/SICU/TICU ventilated patients develop
delirium • 20-50% of lower severity ICU patients develop
delirium• Hypoactive or mixed forms most common • Majority goes undiagnosed if routine monitoring is not
implemented
Ely EW, ICM 2001;27:1892-900Ely EW, JAMA 2001;286,2703-2710Pandharipande J Trauma 2008;65(1):34-41 Ely EW, CCM 2001;29,1370-79Pandharipande, ICM 2007;33(10):1726-31
Roberts B, Aust Crit Care. 2005;18(1):6, 8-9 Thomason J, Crit Care. 2005;9(4):375-81 Ely EW CCM 2004;32:106-112Peterson JAGS 2006;54(3):479-84Ouimet S, ICM 2007;33(1):66-73

Key Points: ICU Delirium• $15k to $25k higher hospital costs
• Longer hospital stays
• 3 times higher risk of death by 6 months
• Prolonged neuropsychological dysfunction
Milbrandt E et al, Crit Care Med 2004;32:955-962 Ely EW et al, JAMA 2004;291-1753-1762Ouimet S, ICM 2007;33(1):66-73Lin et al, Crit Care Med 2004;32:2254-59

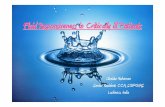
Long-term cognitive impairment (LTCI) after ICU survival
• 10 cohorts (~500 pts) and the largest with neuropsychological testing was 74 patients
• Summary: ~2 out of 3 ICU survivors leave the ICU with long-term cognitive impairment that equates to mild/moderate dementia (sometimes severe)
• Deficits tend to be diffuse and occur in domains including memory, attention/concentration, language, executive functioning
Rothenhausler, Gen Hosp Psych 2001;23:90-96Hopkins, AJRCCM 1999;160:50-56Jackson, Crit Care Med 2003;31;1226-34Hopkins, JINS 2004; 10:1005-1017Hopkins, AJRCCM 2005; 171:340-347
Marquis, AJRCCM 2000;161:A383 (Curtis)Al Saidi, AJRCCM 2003:167:A737 (Herridge) Sukantarat, Anaesthesia 2005;60:847-853Suchyta, AJRCCM 2004; 169:A18Christie, AJRCCM 2004; 169:A781

0
10
20
30
40
50
60
0 5 10 15 20
Days of ICU Delirium
Cog
nitiv
e F
unct
ion
at 1
2 m
onth
s(p
redi
cte
d m
ean
T-s
core
)
Girard TD, et al. 2008, unpublished dataGirard TD, et al. 2008, unpublished data
p=.005
Delirium and Long-Term Cognitive OutcomesDelirium and Long-Term Cognitive Outcomes

Delirium risk factors

Risk Factors, Prevention, and Treatment
• Aging• Baseline dementia• Psychiatric disorders• Underlying illness
– Inflammation
– Coagulation
• Metabolic Disturbances• Hypoxemia• Genetic Predisposition (?)
• Psychoactive Medications• Sleep Deprivation
Inouye, JAMA 1996;275:852-57Dubois, Intens Care Med 2001;27:1297-1304Inouye, NEJM 1999;340:669-676Jacobi, Crit Care Med 2002;30:119-141Milbrandt, Crit Care Med. 2005;33:226-9Ouimet S. Int Care Med 2007;33:66-73

Probability of transitioning from normal to delirium after lorazepam
Lorazepam Dose (mg)
Delirium Risk
Pandharipande et al. Pandharipande et al. Anesthesiology 2006: Anesthesiology 2006: 124:21-6124:21-6
OR 1.2 (1.1-1.4), P=0.003

Surgical Trauma
Users
Non-Users
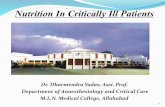
Midazolam
Daily Midazolam Use (Exc. Coma Days)
% D
ays
De
lirio
us
02
04
06
08
01
00
p=0.014p=0.031
Surgical Trauma
Users
Non-Users
Fentanyl
Daily Fentanyl Use (Exc. Coma Days)
% D
ays
De
lirio
us
02
04
06
08
01
00
p=0.007
p=0.936
Midazolam and fentanyl as risk factors for delirium
Pandharipande et al., J Trauma.2008:65;34-41

Sedatives/analgesics in delirium
Pandharipande et al. unpublished dataPandharipande et al. unpublished data

Delirium in surgical ICU patients
• 134 surgical and trauma adult patients requiring mechanical ventilation
• 63% developed delirium • Delirium was associated with more MV days (9.1
vs. 4.9 days, p < 0.01), longer ICU stay (12.2 vs. 7.4 days, p < 0.01), longer hospital stay (20.6 vs. 14.7 days, p < 0.01).
• Greater cumulative lorazepam dose (p = 0.012), and higher cumulative fentanyl dose (p = 0.035) were administered in the delirium group.
Lat I. Crit Care Med. April 2009 (epub)

0
5
10
15
20
25
Discharge One-Year Two-Years
% N
eu
roco
gn
itiv
e S
eq
uela
e
ICU RecallNo Recall
ARDS Patients
Larson MJ. JINS 2007;13:595-605

Psychological outcomes
• Pts with delusional but not factual recall of ICU experience at 2 weeks scored highly for PTSD related symptoms and panic attacks at 8 weeks (p = 0.023 and 0.014 respectively).
Jones C et al. Crit Care Med 2001; 29: 573


How do we prevent/ treat delirium ?
1. Prevention protocols
2. Changing sedation paradigms
-Reducing exposure
-Changing medications
3. Antipsychotics

Prevention protocols
• Reorientation, continuity of care givers
• Improving sleep architecture
• Reducing exposure to deliriogenic medications
• Cognitive stimulation
• Role of geriatrician visits or trained personnel in neuropsychological disorders
Inouye et al. NEJM 1999; 9(340):669-676

Reduce exposure to sedatives and analgesics
Protocol and target based sedation and analgesia
Daily awakening trials
Mascia et al. CCM 2000; 28: 2300-2306Mascia et al. CCM 2000; 28: 2300-2306Brook et al. CCM 1999; 27: 2609-2615Brook et al. CCM 1999; 27: 2609-2615Kress et al. NEJM 2000; 342: 1471-1477Kress et al. NEJM 2000; 342: 1471-1477Brattebo et al. BMJ 2002; 324: 1386-1389Brattebo et al. BMJ 2002; 324: 1386-1389

The ABC Trial(both groups get patient targeted sedation)
O U TC O M ESd e lirium , LO S , 1 2 -m o N P S tes tin g , Q O L
S p o ntan eo u s B rea th ing T ria l (S B T)ve n tila to r o ff
sa fe ly m o n ito red
O U TC O M ESd e lirium , LO S , 1 2 -m o N P S tes tin g , Q O L
S p o ntan eo u s B rea th ing T ria l (S B T)ve n tila to r o ff
sa fe ly m o n ito red
S p on taneo us A w aken ing T ria l (SA T)tu rn se d a tio n /n a rco tics o ff
m o n ito r sa fe ly
M e d ica l IC U o n V en tila to rS u rro g a te In fo rm e d C o nse ntControl Intervention

Study Day
Da
ily D
os
e o
f B
en
zod
iaze
pin
es
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
010
2030
4050
6070
BenzodiazepinesBenzodiazepines
Usual Care+SBTSBT+SAT

Study Day
Da
ily D
os
e o
f O
pia
tes
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
0
2000
4000
6000
Usual Care+SBTSBT+SAT
OpiatesOpiates

SBT- CONTROL
SAT+SBT- INTERVENTION
Treatment group
No YesSepsis
0
10
20
Day
s o
f D
elir
ium
p=.74
Delirium duration in septic patients in ABC studyDelirium duration in septic patients in ABC study
Girard et al. Personal communication
p=.02

Pa
tie
nts
Aliv
e (
%)
00
20
40
60
80
100
60 120 180 240 300 360
Days
Usual Care+SBT (n=168)
SAT+SBT (n=167)
One-Year SurvivalOne-Year Survival
p=.01NNT=7
Girard TD, et al. Lancet 2008;371:126-34Girard TD, et al. Lancet 2008;371:126-34

Hospital Discharge
3-Month Follow-Up
12-Month Follow-Up
1.86 (1.04, 3.34)
2.01 (1.09, 3.71)
2.23 (1.13, 4.41)
0.04
0.02
0.02
Time of Cognitive Assessment Odds Ratio (95% CI) P-value
0 1 2 3 4
Favors Control Favors Intervention
Long-Term Cognitive Outcomes
Jackson JC, et al. 2008, in submission

Changing sedation paradigms
MENDS
SEDCOM

MENDS StudyDouble blind randomized controlled trial
C o n tro lL o ra ze p a m (G A B A )
+ /- F en ta n yl
In te rve n tionD e xm e d eto m id in e (2 )
+ /- F en ta n yl
M IC U /S IC U V en tila ted o n S e da tivesIn fo rm ed C o n se n t
Vanderbilt University Medical Center and Washington Hospital CenterVanderbilt University Medical Center and Washington Hospital Center
Pandharipande P et al. JAMA Dec 2007Pandharipande P et al. JAMA Dec 2007

Delirium/Coma-Free Days
02
46
810
12
p=.01
Delirium-Free Days
p=.09 p=.001
Coma-Free Days
DexmedetomidineLorazepam
Brain DysfunctionBrain Dysfunction
Pandharipande PP, et al. JAMA 2007;298:2644-53

Risk of developing delirium

Septic subgroup analysis

MENDS: Patients Outcomes in Septic subgroupOutcome variable Lorazepam Dexmedetomidine P value
(N=20) (N=19)
Brain Dysfunction Delirium and coma free days 1.5 (1,4) 8 (4,10) 0.002
Delirium free days 7.5 (4, 8) 10 (8, 11) 0.007
Coma free days 7 (1,9) 10 (9, 12) <0.003
Prevalence of delirium 70% 79% 0.52
Prevalence of coma 95% 68% <0.03
Efficacy of sedationDays at Physician RASS goal 35% (0,60) 67% (35,85) 0.016
Pandharipande et al. Critical Care 2008, 12(Suppl 2):P275

28-Day Survival, Sepsis Patients28-Day Survival, Sepsis Patients
0 7 14 21 28
020
4060
8010
0
Days
Pat
ient
s A
live
(%)
Dexmedetomidine
Lorazepam
Pandharipande et al. Critical Care 2008, 12(Suppl 2):P275
HR 0.3 (0.1- 0.9). P=0.04

Data on antipsychotics and delirium in the ICU

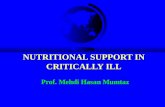
Olanzapine vs. haloperidol: treating delirium in a critical care setting
Mean daily delirium scores
Day
5 4 3 2 1
Mean score
8.0
7.5
7.0
6.5
6.0
5.5
5.0
4.5
4.0
Group
Haloperidol
Olanzapine
Skrobik et al, ICM 2004;30:444-49

Risperidone and delirium
• Double blind randomized trial (DBRT)
• Single dose (1 mg) of risperidone administered after cardiac surgery
• Reduced the incidence of postoperative delirium – 11.1% vs.31.7%, P=0.009– RR=0.35, 95% CI=0.16-0.77)
Prakanrattana et al. Anaesth Intensive Care 2007 Oct;35(5):714-9.

MIND Multicenter Double Blind RCT
MV Surgical, MV Surgical, Medical and Medical and Trauma ICU Trauma ICU
patientspatients
PO haloperidolPO haloperidol PO ziprasidonePO ziprasidone PlaceboPlacebo
Girard T, Pandharipande P et al. in reviewGirard T, Pandharipande P et al. in review

Delirium rates in MIND
Girard T, Pandharipande P et al. in reviewGirard T, Pandharipande P et al. in review

Conclusion– Delirium occurs in majority of mechanically ventilated
patients and is associated with worse outcomes – Easy to diagnose in ICU with new validated instruments– Sedatives and analgesics may be modifiable risks factors– Avoiding benzodiazepines/ using alpha2 agonists may
reduce delirium– No difference between typical and atypical antipsychotics
in delirium management in ICU patients (risperidone in 1 study)
– Prevention protocols with emphasis on restoring sleep may help