
DELIRIUM AND DEMENTIA - NurseCe4Less.com · nursece4less.com nursece4less.com nursece4less.com...
78
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 1 DELIRIUM AND DEMENTIA DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison control center information specialist. Dana has published numerous CE and journal articles, written NCLEX material and textbook chapters, and done editing and reviewing for publishers such as Elsevier, Lippincott, and Thieme. He has written widely on the subject of toxicology and was recently named a contributing editor, toxicology section, for Critical Care Nurse journal. He is currently employed at the Connecticut Poison Control Center and is actively involved in lecturing and mentoring nurses, emergency medical residents and pharmacy students. ABSTRACT There are many possible causes of dementia and delirium. The more common causes are complex, such as dementia of the Alzheimer’s type or delirium due to drug withdrawal. Other relevant neurological problems include mild cognitive impairment and pseudo-dementia. While detailed and extensive information about the specific causes of these diseases is outside the scope of this study, general information on dementia and delirium, including risk factors, treatments, and nursing considerations are discussed.
Transcript of DELIRIUM AND DEMENTIA - NurseCe4Less.com · nursece4less.com nursece4less.com nursece4less.com...
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 1
DELIRIUM
AND
DEMENTIA
DANA BARTLETT, BSN, MSN, MA, CSPI
Dana Bartlett is a professional nurse and author. His clinical experience includes 16
years of ICU and ER experience and over 20 years of as a poison control center information specialist. Dana has published numerous CE and journal articles, written NCLEX material and
textbook chapters, and done editing and reviewing for publishers such as Elsevier, Lippincott, and Thieme. He has written widely on the subject of
toxicology and was recently named a contributing editor, toxicology section, for Critical Care Nurse journal. He is currently employed at the Connecticut Poison Control Center and is actively involved in lecturing and mentoring
nurses, emergency medical residents and pharmacy students.
ABSTRACT
There are many possible causes of dementia and delirium. The more
common causes are complex, such as dementia of the Alzheimer’s
type or delirium due to drug withdrawal. Other relevant neurological
problems include mild cognitive impairment and pseudo-dementia.
While detailed and extensive information about the specific causes of
these diseases is outside the scope of this study, general information
on dementia and delirium, including risk factors, treatments, and
nursing considerations are discussed.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 2
Accreditation Statement
This activity has been planned and implemented in accordance with
the policies of NurseCe4Less.com and the continuing nursing education
requirements of the American Nurses Credentialing Center's
Commission on Accreditation for registered nurses.
Credit Designation
This educational activity is credited for 4.5 hours. Nurses may only
claim credit commensurate with the credit awarded for completion of
this course activity.
Pharmacology content is 0.5 hours (30 minutes).
Course Author & Planner Disclosure Policy Statements
It is the policy of NurseCe4Less.com to ensure objectivity,
transparency, and best practice in clinical education for all continuing
nursing education (CNE) activities. All authors and course planners
participating in the planning or implementation of a CNE activity are
expected to disclose to course participants any relevant conflict of
interest that may arise.
Statement of Learning Need
Nurses in all practice settings that care for individuals with dementia
and delirium need to understand what defines each disorder, and
diagnostic criteria related to etiology, clinical assessment and signs
and symptoms.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 3
Course Purpose
To provide professional nurses with the information they need to
assess and care for patients who have dementia or delirium.
Target Audience
Advanced Practice Registered Nurses and Registered Nurses
(Interdisciplinary Health Team Members, including Vocational Nurses
and Medical Assistants may obtain a Certificate of Completion)
Course Author & Director Disclosures
Dana Bartlett, RN, BSN, MA, MSN, CSPI, William S. Cook, PhD,
Douglas Lawrence, MS, Susan DePasquale, MSN, FPMHNP-BC - all
have no disclosures.
Acknowledgement of Commercial Support
There is none.
Please take time to complete a self-assessment of knowledge,
on page 4, sample questions before reading the article.
Opportunity to complete a self-assessment of knowledge
learned will be provided at the end of the course.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 4
1. One of the defining characteristics of dementia is
a. inability to perform activities of daily living.
b. severe agitation. c. reversible cognitive impairment.
d. occurrence before age 50.
2. Most cases of dementia are caused by
a. trauma and heavy metal poisoning. b. infections and hemorrhage.
c. Alzheimer’s disease and vascular pathologies. d. hypoxia and Parkinson’s disease.
3. Defining characteristics of delirium include
a. movement disorders and a progressive cognitive decline. b. attention deficits and confusion.
c. expressive aphasia and hypotension. d. hyperthermia and depression.
4. The onset of delirium is
a. acute.
b. slow. c. chronic.
d. fluctuating.
5. Common causes of delirium include
a. Parkinson’s disease and advanced age.
b. drug withdrawal and Lewy body dementia. c. acute blood loss and frontotemporal dementia.
d. drugs and dementia.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 5
Introduction
Dementia and delirium are the major causes of cognitive impairment
in the elderly, and they are syndromes caused by a wide range of
medical, neurological and psychiatric pathologies.1 As clinical
diagnoses, dementia and delirium can be confirmed through
investigation into etiology, laboratory testing, specific physical
findings, or imaging. In addition, the relationship between the two
diseases is complex. There are similarities in their presentation;
dementia is a major risk factor for delirium, and delirium occurs in
many patients who have dementia. Dementia and delirium can be
acute or subacute, and they can be transient and reversible or they
can cause permanent impairment. Both dementia and delirium are
associated with increased morbidity and mortality, and their risk
increases with advancing age. As the population in the U.S. becomes
older the incidence of these pathologies of aging will certainly increase.
Overview Of Delirium And Dementia
Slowing of cognitive function can occur with aging and it is not
uncommon for older people to have mild memory deficits or a
decreased speed with which information is processed. Old age is a
major risk factor for dementia, but advanced age itself does not cause
a decrease in cognitive and intellectual ability that interferes with daily
functioning. In brief, dementia is not an inevitable consequence of
getting old.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 6
Statistics
Dementia and delirium are very common. The incidence and
prevalence rates of dementia and delirium are reflected in the
following prevalence rates.1-5
Delirium is noted in 14%-56% of elderly patients who are
hospitalized and in 40% of patients admitted to intensive care.
Postoperative delirium is seen is approximately 5%-10% of
general surgery patients.
Community-based studies have found a prevalence of dementia
as high as 47% in those 85 years of age and older.
Alzheimer’s disease is the most common cause of dementia and
in 2013 there were approximately 5 million Americans who
suffered from Alzheimer’s disease.
There are many causes of dementia but Alzheimer’s disease
accounts for approximately 60%-80% of all cases.
Delirium occurs in approximately 50% of older hospitalized
patients and 70% of older long-term care patients.
Dementia: Definition, Diagnostic Criteria And Etiology
Dementia can be defined in several ways. Kane, et al. (2013) defines
dementia as “... a clinical syndrome involving a sustained loss of
intellectual functions and memory of sufficient severity to cause
dysfunction in daily living.”1 This definition emphasizes key points
about dementia that are important to remember.
First, the distinguishing aspect of dementia is an inability to
successfully perform the activities of daily living, caused by impaired
cognitive and intellectual capacity. Second, dementia is a syndrome. A
syndrome is a set of signs and symptoms that can have many different

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 7
causes, and that is especially true with dementia. There is a multitude
of etiologies of dementia. And finally, because dementia has no single
cause or type of cause the clinical picture of dementia can be variable.
The Diagnostic and Statistical Manual of Mental Disorders, fifth edition,
(DSM-5) has replaced the term dementia with the terms major
cognitive disorder and mild cognitive disorder.6
Major Neurocognitive Disorder: DSM-5 Diagnostic Criteria
1. Evidence of significant cognitive decline from a previous level of
performance in one or more cognitive domains (complex
attention, executive function, learning and memory, language,
perceptual-motor, or social cognition) based on: a) concern of
the individual, b) a knowledgeable informant or the clinician
finds there has been a significant decline in cognitive function;
and, c) a substantial impairment in cognitive performance,
preferably documented by standardized neuropsychological
testing or, in its absence, another quantified clinical assessment.
The cognitive deficits interfere with independence in everyday
activities (i.e., at a minimum, requiring assistance with complex
instrumental activities of daily living such as paying bills or
managing medications).
2. The cognitive deficits do not occur exclusively in the context of a
delirium.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 8
3. The cognitive deficits are not better explained by another mental
disorder (i.e., major depressive disorder, schizophrenia).
Minor Neurocognitive Disorder: DSM-5 Diagnostic Criteria
1. Evidence of modest cognitive decline from a previous level of
performance in one or more cognitive domains (complex
attention, executive function, learning and memory, language,
perceptual-motor, or social cognition) are based on a) concern of
the individual, b) a knowledgeable informant, c) the clinician’s
assessment of a mild decline in cognitive function, and d) a
modest impairment in cognitive performance, preferably
documented by standardized neuropsychological testing or, in its
absence, another quantified clinical assessment.
2. The cognitive deficits do not interfere with capacity for
independence in everyday activities (i.e., complex instrumental
activities of daily living such as paying bills or managing
medications are preserved, but greater effort, compensatory
strategies, or accommodation may be required).
3. The cognitive deficits do not occur exclusively in the context of a
delirium.
4. The cognitive deficits are not better explained by another mental
disorder (i.e., major depressive disorder, schizophrenia).
When making the diagnosis of major or minor neurocognitive disorder
it must be specified if the disorder is due to one of the following:
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 9
Alzheimer’s disease
Frontotemporal lobar degeneration
Lewy body disease
Vascular disease
Traumatic brain injury
Substance/medication use
HIV infection
Prion disease
Parkinson’s disease
Huntington’s disease
Another medical condition
Multiple etiologies
Unspecified
Dementia can be usefully divided
into two categories: reversible and
irreversible. Most cases of
dementia are irreversible. These
dementias slowly progress and the
patient’s condition worsens over
time.
Degenerative diseases of the
nervous system, infections,
trauma, and vascular disorders
cause irreversible dementias. The
most common irreversible dementias are dementia of Alzheimer’s
disease, frontotemporal dementia, Lewy body dementia, Parkinson’s

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 10
disease, and vascular dementia. Many patients who have dementia
have a neurodegenerative and a vascular pathology.7
Table 1: Irreversible Causes of Dementia1
Acquired immunodeficiency syndrome
Alzheimer disease
Anoxia secondary to cardiac arrest
Arteritis
Binswanger disease
Carbon monoxide poisoning
Cerebrovascular disease, i.e., multi-infarct dementia
Craniocerebral injury, including dementia pugilistica
Creutzfeldt-Jakob disease
Huntington’s disease
Dementia associated with Lewy bodies
Frontotemporal dementia
Infections
Parkinson’s disease
Pick disease
Postencephalitic dementia
Progressive multifocal leukoencephalopathy
Progressive supranuclear palsy
Trauma
Vascular dementias
The reversible dementias are much less common than the irreversible
dementias. Irreversible dementias can be successfully treated but
finding and treating the cause does not guarantee a cure.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 11
Table 2: Reversible/Partially Reversible Causes of Dementia1
Alcoholism
Anoxic brain injury
Autoimmune disorders
Central nervous system vasculitis
Disseminated lupus erythematous
Depression
Drugs
Heavy metal poisoning, i.e., lead, mercury
Infections
Metabolic disorders
Multiple sclerosis
Neoplasms
Normal pressure hydrocephalus
Nutritional disorders, i.e., B6, B12 deficiency
Organic poisons, i.e., pesticides, solvents
Psychiatric disorders
Trauma
Viral infections, i.e., HIV
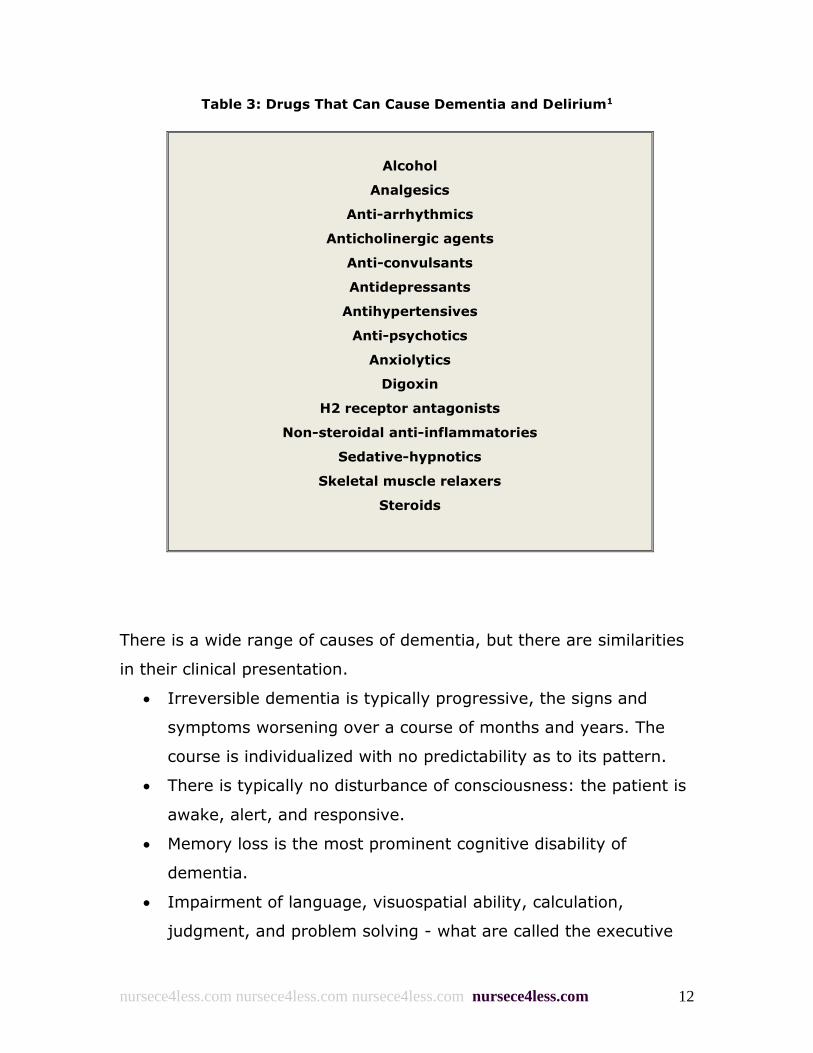
Medications, prescription or illicit, can also cause dementia. In most
cases the dementia caused by a drug is reversible, but not always. The
following Table 3 lists the drugs that can cause dementia and delirium.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 12
Table 3: Drugs That Can Cause Dementia and Delirium1
Alcohol
Analgesics
Anti-arrhythmics
Anticholinergic agents
Anti-convulsants
Antidepressants
Antihypertensives
Anti-psychotics
Anxiolytics
Digoxin
H2 receptor antagonists
Non-steroidal anti-inflammatories
Sedative-hypnotics
Skeletal muscle relaxers
Steroids
There is a wide range of causes of dementia, but there are similarities
in their clinical presentation.
Irreversible dementia is typically progressive, the signs and
symptoms worsening over a course of months and years. The
course is individualized with no predictability as to its pattern.
There is typically no disturbance of consciousness: the patient is
awake, alert, and responsive.
Memory loss is the most prominent cognitive disability of
dementia.
Impairment of language, visuospatial ability, calculation,
judgment, and problem solving - what are called the executive
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 13
brain functions - are also common in patients who have
dementia.
Patients who have dementia often suffer from neuropsychiatric
problems including, but not limited to, agitation, apathy,
delusions, depression, disinhibition, hallucinations, insomnia, and
wandering.
As mentioned previously, the most common causes of irreversible
dementia are Alzheimer’s disease, frontotemporal dementia, Lewy body
dementia, Parkinson’s disease, and vascular dementia. Some of these
may not be familiar to many nurses and a brief description of each one
is provided below.
Alzheimer’s Disease
Alzheimer’s disease is a chronic, progressive neurological disorder that
causes severe behavioral and cognitive deterioration, especially in
memory. The cause, or causes, of Alzheimer’s disease are not
completely understood. Alzheimer’s disease is probably the result of a
convergence of genetic risk factors and environmental stimuli that
produce characteristic lesions in the parietal and temporal lobes,
specifically amyloid plaques and neurofibrillary tangles. These lesions
interrupt the normal metabolism and self-repair of neurons and disrupt
communication between different areas of the brain.
The time from diagnosis to death can be as little as three years. The
signs and symptoms of Alzheimer’s disease are difficult to treat and
there is no cure.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 14
Frontotemporal Lobe Dementia
Frontotemporal lobe dementia is a neurodegenerative disease caused
by atrophy of the frontal and temporal lobe. It is a disease that is
considered clinically and genetically diverse. The hallmark signs of
frontotemporal dementia are behavioral and speech defects, such as
expressive and fluent aphasia and abnormal personal and social
behavior. In most cases the cause is unknown, however, a family
history of the disease is a strong risk factor. Frontotemporal dementia
is chronic, progressive, and there is no cure.
Lewy Body Dementia
Lewy body dementia is a chronic, progressive neurodegenerative
disease that is characterized by the presence of Lewy bodies,
abnormal deposits of protein that accumulate in neurons in specific
areas of the brain. The cause of Lewy body dementia is not known. It
is distinguished from other types of dementia by the Lewy bodies and
by these aspects of the clinical presentation:
Varying levels of alertness and attention, especially reduced
responsiveness
Visual hallucinations
Parkinsonian motor signs
There appears to be some overlap of Lewy body dementia with
Alzheimer’s disease and Parkinson’s disease with dementia. Lewy
bodies are noted in some patients with Alzheimer’s disease (Lewy body
variant of Alzheimer’s disease) and in some patients with Parkinson’s
disease. Additionally, some of the signs of Parkinson’s disease with
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 15
dementia and Lewy body dementia are similar. There is no cure for
Lewy body dementia.
Parkinson’s Disease
Parkinson’s disease is caused by chronic and progressive destruction of
dopamine-producing cells in the substania nigra area of the brain.
Parkinson’s disease often causes dementia, but it is distinguished by
characteristic motor symptoms such as bradykinesia (slowness of
movements), gait disturbances, rigidity, and tremor.
Approximately 10% of all cases of Parkinson’s can be clearly identified
as having a genetic cause, but most cases are considered to be caused
by a convergence of genetic risk factors and environmental stimuli.
There is no cure for Parkinson’s disease but there is effective
symptomatic treatment and the progression of the disease can be
delayed.
Vascular Dementia
Vascular dementia is the second most common cause of dementia and
it often coexists with Alzheimer’s disease. Vascular dementia is not a
single disease; it is a group of syndromes that are caused by vascular
pathologies, such as:
Cerebral infarct
Cerebral hemorrhage
Embolic and/or thrombotic obstructions (i.e., stroke)
Various types of lesions like lacunar lesions

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 16
There are many causes of vascular dementia, and athersclerosis,
diabetes, hypercholesterolemia, hypertension, and smoking are
significant risk factors for the development of this pathology.
Delirium: Definition, Diagnostic Criteria And Etiology
Delirium is an acute change in mental status characterized by
confusion and disturbances in cognition.9 Delirium is a sudden change
in cognition. It develops over a short period, it fluctuates in severity,
and the most prominent features of delirium are the abnormal changes
that occur in attention and awareness. As with dementia, delirium is a
syndrome, there are a multitude of causes, and the clinical
presentation can vary. Delirium is usually transient and reversible, but
delirium can persist for hours or days (acute) or weeks or months
(persistent), and it is associated with high rates of morbidity and
mortality. The DSM-5 criteria for delirium are:9
Delirium: DSM-5 Diagnostic Criteria
1. A disturbance in attention (i.e., reduced ability to direct, focus,
sustain, and shift attention) and awareness (reduced orientation
to the environment).
2. The disturbance develops over a short period of time (usually
hours to a few days), represents a change from baseline
attention and awareness, and tends to fluctuate in severity
during the course of a day.
3. An additional disturbance in cognition (i.e., memory deficit,
disorientation, language, visuospatial ability, or perception).

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 17
4. The disturbances in Criteria A and C are not better explained by
another preexisting, established, or evolving neurocognitive
disorder and do not occur in the context of a severely reduced
level of arousal, such as coma.
5. There is evidence from the history, physical examination, or
laboratory findings that the disturbance is a direct
physiological consequence of another medical condition,
substance intoxication or withdrawal (i.e., due to a drug of abuse
or to a medication), or exposure to a toxin, or is due to multiple
etiologies.
When making the diagnosis of delirium it must be specified if the
delirium is hyperactive, hypoactive, or involves a mixed level of
activity, and associated with the following symptoms.
Hyperactive:
The individual has a hyperactive level of psychomotor activity
that may be accompanied by mood lability, agitation, and/or
refusal to cooperate with medical care.
Hypoactive:
The individual has a hypoactive level of psychomotor activity
that may be accompanied by sluggishness and lethargy that
approaches stupor.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 18
Mixed level of activity:
The individual has a normal level of psychomotor activity even
though attention and awareness are disturbed. Also includes
individuals whose activity level rapidly fluctuates.
A hyperactive level of psychomotor activity characterizes hyperactive
delirium, and is it seen in patients who are intoxicated or in withdrawal
from drugs such as amphetamine or phencyclidine. A decreased level
of psychomotor activity characterizes hypoactive delirium, and the
patient is lethargic and sluggish. Mixed state delirium is characterized
by alternating periods of agitation and sedation.
As with dementia, there are many causes of delirium. Drugs and
medications are an important and common cause of delirium.
Dementia is also a very common cause of delirium. Delirium can
happen to any patient, but it is more prevalent in the elderly.
It is not clear if advanced age itself is a risk factor for delirium.
However, the elderly patient population often has greater exposure to
identified risk factors for delirium; bladder catheterization, decreased
ability to metabolize and eliminate medications, dementia, fracture,
hearing impairment, immobility, inadequate or excessive use of
analgesics or sedatives, malnutrition, multiple medications, pre-
existing dementia, sensory deprivation, status-post anesthesia and
surgery, underlying medical or neurologic illnesses, use of physical
restraints, and visual impairment.1,5,9 Common causes of delirium are
listed in Table 4 below.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 19
Table 4: Common Causes of Delirium1,8
Acute blood loss
Acute myocardial infarction
Acute psychoses
Azotemia
Congestive heart failure
Decreased cardiac output
Decreased sensory input
Dehydration
Dementia
Drugs
Drug overdose
Drug withdrawal
Dehydration
Fecal impaction
Fracture
Intoxication
Hypercarbia
Hypo- or hyperglycemia
Hyponatremia
Hypo- or hyperthermia
Hypoxia
Immobility
Infections
Malnutrition
Metabolic disorders
Post-Operative State
Parkinson’s disease
Stroke (small cortical)
Urinary retention
Visual impairment

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 20
Delirium is often misdiagnosed and it may be mistaken for dementia,
depression, another psychiatric disorder, or attributed to old age.9 This
underrecognition can delay treatment, and it can also prolong the
duration of delirium and expose the patient to permanent neurological
damage.5
Mild Cognitive Impairment And Pseudo-dementia
Mild cognitive impairment (MCI) and pseudo-dementia should also be
mentioned when discussing dementia. Individuals who have MCI or
pseudo-dementia can often develop dementia. MCI is often
overlooked, and pseudo-dementia is often misdiagnosed as dementia.
Mild cognitive impairment is a term used to describe cognitive deficits
that are not considered to be a normal part of aging but do not fit the
diagnostic criteria for dementia.10,11 There are differences in the
diagnostic criteria for MCI and these criteria are not precise, but MCI is
generally considered to be an intermediate state between normal
cognitive functioning and dementia. In their 2014 review, Langa, et
al., used these criteria for the diagnosis of MCI.10
Concern regarding a change in cognition from the patient,
knowledgeable informant, or from a skilled clinician
observing the patient.
Objective evidence of impairment (from cognitive testing)
in 1 or more cognitive domains including memory,
executive function, attention, language, or visuospatial
skills.
Preservation of independence in functional abilities
(although individuals may be less efficient and make more

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 21
errors at performing activities of daily living and
instrumental activities of daily living than in the past).
No evidence of a significant impairment in social or
occupational functioning (i.e., not demented).
Patients who have MCI have memory deficits and occasionally they
have subtle defects in other cognitive abilities, but they have normal
executive functioning and they do not have difficulties performing
activities of daily living.10,11 The patient who has MCI is aware of the
change in his/her memory, unlike the person who has dementia. Mild
cognitive impairment may be temporary and a reversion to normal
mental status is possible12 but approximately 5%-20% of people who
have MCI will develop dementia.10
Pseudo-dementia is a descriptive term for a clinical presentation that
closely mimics dementia, but is usually caused by depression and
occasionally by other psychiatric disorders.13,14 Depression in the
elderly can cause many of the cognitive defects that are common to
dementia.
Dementia can produce depressive signs and symptoms14 so a
misdiagnosis is relatively common. Some key differences between
dementia and depression are:6
Depression has a relatively abrupt onset but the onset of
dementia is slow.
Dementia progresses while depression plateaus.
Patients who are depressed often know they are depressed and
will complain of their problem. Patients who have dementia are
seldom aware of their condition.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 22
The affect and emotions of people who have dementia are
variable. People who are depressed have a depressed affect and
mood.
Imaging tests, laboratory tests, and the neurological exam of a
patient who has dementia will often be abnormal; this is not the
case for patients who are depressed.
Assessment Of Dementia
Assessment and the diagnosing of
dementia can be quite challenging.
One of the primary problems in the
assessment is that the patient is
often an unreliable source of
information. Confirmation of the
diagnosis of dementia using imaging
studies, laboratory tests, and/or
specific physical findings may not be
possible. Also, some patients may
have more than one cause of
dementia. The diagnostic process is time consuming and it is not
uncommon for dementia to be mis-diagnosed.4 The incidence of a
missed diagnosis of dementia has been reported to be as high as 50%-
80%, depending on the severity of the case and who is doing the
assessment.15
The specific diagnostic approach, i.e., what tests should be ordered,
will differ depending on the suspected cause of dementia. But the
assessment process outlined below can be applied to any situation in
which dementia may be present.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 23
Vital Signs
Assessment of the airway, breathing, and circulation (ABCs) and body
temperature is always the first step of a patient assessment.
Abnormalities of blood pressure, pulse, and temperature can provide
valuable indicators about the source of dementia. For example,
hypothermia can indicate the presence of hypothyroidism and
hypertension can indicate the possible presence of vascular dementia.
History
The events in the patient’s life prior to the assessment should be
reviewed, either by speaking to the patient, family members, friends,
or caretakers. The reviewer should ask specific questions about
behavior, changes in social circumstances, daily activities, elimination
patterns, food and fluid intake, and mood. It is important to learn
whether there have been any recent events such as an accident,
illness, trauma, or surgery that could be a cause of delirium. The
reviewer should also determine if the neuropsychological changes have
been slow or sudden in onset and how quickly they have progressed as
this information can provide valuable clues about the etiology of
dementia.16,17
Family/Significant Other Interview
A careful interview of family members/significant others and
caretakers is a necessary part of patient evaluation because the
patient who has dementia will seldom be aware of the changes in
cognition and memory. The interviewer should ask specific questions
about the patient’s day-to-day life:

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 24
Has the patient been agitated, disruptive, or verbally aggressive?
Has there been wandering behavior or dangerous driving?
Has the patient had difficulty sleeping?
Has the patient’s personal hygiene deteriorated or has he/she
been incontinent?
Galvin, et al., found that the following eight question interview was
sensitive and specific for detecting dementia and cognitive
impairment.18 Has the patient shown any of the following deficits or
behaviors?
Problems with judgment
Reduced interest in activities or hobbies
Repeating questions, stories, or statements
Trouble learning how to use an appliance or tool
Forgetting what month or year it is
Unable to handle simple financial affairs
Forgetting appointments
Consistent problems with memory and/or thinking
Medical and Surgical History
The patient’s medical and surgical history should be be carefully
reviewed. This review should include the medical history of the
patient’s immediate family, i.e., parents and siblings. Asking about
alcohol or drug abuse can be uncomfortable but it should be done;
and, it is often helpful to review the patient’s history of alcohol or drug
abuse with someone other than the patient.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 25
Medication History
When reviewing the patient’s health history a current list of the
prescription medications the patient is taking should be obtained and
verified to know whether new medications have recently been
prescribed or doses have been changed. An inquiry should be made
about the use of over-the-counter and/or herbal medications. It should
also be determined if the patient has been taking his/her medications
as prescribed. There may have been an inadvertent or intentional
overdose, the patient may have been skipping doses, or he/she may
have simply stopped taking a prescribed medication.
Physical Assessment
A comprehensive physical examination should be performed. The
findings may be equivocal and/or non-specific, but the presence of
some physical findings and the absence of others can help the
clinician decide which diagnostic tests should be done and suggest the
cause of the dementia. For example, bradykinesia and gait
disturbances are characteristic of Parkinson’s disease, the presence of
papilledema suggests that the patient may a brain tumor or a subdural
hematoma, and myoclonus can indicate the presence of human
immunodeficiency virus (HIV)-related dementia.7
Laboratory Tests, Imaging Studies, Other Diagnostic Tools
There are no laboratory tests, imaging studies, or other diagnostic
tools that should be routinely performed for every patient who is
suspected of having dementia.4,16 The physical examination and
history taking should determine what is needed, and it is important to

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 26
focus diagnostic efforts in order to avoid unnecessary procedures and
delays in making the diagnosis.
Laboratory tests that are helpful when determining the cause or
presence of dementia include complete blood count (CBC), blood urea
nitrogen (BUN) and creatinine, serum calcium and phosphorus, pulse
oximetry, serum glucose, serum electrolytes, liver function tests,
thyroid studies, vitamin B12 level, 12-lead ECG, and (possibly) testing
for HIV antibodies.16 The American Academy of neurology suggests
that at a minimum laboratory tests for determining the cause of
dementia should include CBC, electrolytes, renal and thyroid function
studies, a vitamin B12 level, and a neuro-imaging study such as a
computerized tomography (CT) scan or a magnetic resonance imaging
(MRI) scan.16
The use of neuro-imaging studies such as CT or MRI - especially MRI -
can be used to determine the specific type of dementia, to evaluate
the progress of neurological damage, and possibly predict who will
develop dementia.16,19,20 For example, medial temporal lobe atrophy is
common in patients with dementia, but it is usually more pronounced,
and the pattern of injury different, in patients who have Alzheimer’s
disease; and, cerebral infarcts may be seen in patients who have
vascular dementia.19
Neurologic and Psychiatric Assessment
A careful assessment of the patient’s neurological and psychiatric
status is the crucial part of the evaluation for the presence of
dementia. There is much information that can be acquired by simple
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 27
observation. When the clinician is examining or interviewing the
patient, it is important to pay special attention to:7,16,17
Alertness/level of consciousness:
Whether the patient is paying attention and responding to their
surroundings
Aphasia:
Inability to express or understand language, spoken or written
Apraxia:
Inability to perform physical tasks that the patient has the
capability of doing
Behavior:
Erratic or inappropriate behavior in the patient, observed or
reported
General appearance
Memory:
How well the patient retains and recalls information
Mood:
Unexplained mood swings in the patient, observed or reported
Orientation:
Whether the patient knows the date and time
Thought process:
Organized or disorganized thinking
The clinician should also carefully observe the patient for:1
Executive functioning, i.e., planning, weighing alternatives,
coordination of mental faculties for accomplishing tasks
Insight and judgment
Memory, short-term and long-term
Use of language

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 28
Level of consciousness
Visuospatial functions, i.e., how well the patient analyzes and
understands space in several dimensions
Neurological and psychiatric functioning can also be assessed by using
neuropsychological testing and standardized screening tests.
Neuropsychological testing is a broad term that refers to tests that are
designed to assess a single neurological function such as memory,
intelligence, or visuospatial ability. For example, memory can be
tested using the Constructional Praxis Test and using the clock test can
assess visuospatial ability. Neuropsychological tests are lengthy and
complex and they can be helpful when the initial assessment shows a
cognitive deficit but the specific problem causing the cognitive deficit is
not obvious. These tests are considered to have a relatively high
sensitivity and specificity for detecting dementia,4 and can be useful in
differentiating dementia from depression.1
Standardized screening tests can be helpful to assess for the presence
and severity of dementia, but it should be remembered that these are
used for screening; they are not diagnostic nor are they a substitute
for a comprehensive mental status examination; they may not detect
early stage dementia, and; they cannot differentiate between different
types of dementia.16,17 Nonetheless, these screening tests are widely
used and a familiarity with them is important.
Five screening tests that are commonly used are the Mini-Mental State
Examination (MMSE), the Mini-Cog, The Clinical Dementia Rating
(CDR) scale, Addenbrooke’s Cognitive Examination - revised (ACE-r),

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 29
and the Montreal Cognitive Assessment (MOCA). There are many other
assessment tests/tools and a full discussion of each one and their
limits, strengths, and how and when they should be used is beyond
the scope of this module but several will be reviewed here. In depth
information on dementia screening tests is available in the 2015
review by Tsoi, et al. (2015),21 the 2014 review by Yokomizo, et al.,15
and a 2013 review by Lin, et al.22
Mini-Mental Status Exam
The Mini-Mental Status Exam (MMSE) is commonly used. It can be
done relatively quickly, and it is the most widely studied of the
cognitive screening tests.4 The test is not considered to be sensitive
for mild dementia and performance may be affected by age and level
of education.4
The MMSE involves performance of the following tasks:
What is the date: (year)(season)(date)(day)(month) - 5 points
Where are we: (state)(county)(town)(hospital)(floor) - 5 points
Name three objects:
Name three objects and then ask the patient to repeat them.
Give one point for each correct answer. Repeat them until
he/she learns all three. Count and record the number of trials.
The first repetition determines the score, but if the patient
cannot learn the words after six trials then recall cannot be
meaningfully tested: Maximum score is 3 points.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 30
Serial 7s:
Ask the patient to count backwards in increments of 7, starting
with the number 100. One point for each correct answer; stop
after five answers. Alternatively, spell WORLD backwards, one
point for each letter in correct order: Maximum score is 5 points.
Ask for the three objects repeated above - one point for each
correct: Maximum score is 3 points.
Show and ask patient to name a pencil and wristwatch - 2
points.
Repeat the following: "No ifs, ands, or buts." Allow only one trial
- 1 point.
Follow a three stage command, "Take a paper in your right hand,
fold it in half, and put it on the floor." Score one point for each
task executed: Maximum score is 3 points.
On a blank piece of paper write "close your eyes." Then ask the
patient to read and do what it says - 1 point.
Give the patient a blank piece of paper and ask him/her to write
a sentence. The sentence must contain a noun and verb and be
sensible - 1 point.
Ask the patient to copy a design (i.e., intersecting pentagons).
All 10 angles must be present and two must intersect – 1 point.
The maximum score on the MMSE is 30 points. A score of less than 24
points is usually considered to be suggestive of dementia or delirium.4

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 31
Mini-Cog
The Mini-Cog test requires the patient to: 1) Draw a clock with the
numbers in correct sequence and the clock hands correctly indicating
the current time; and, 2) Perform an uncued recall of three objects.
The names of the three objects (i.e., banana, car, dog) are given to
the patient and he/she is then asked to repeat them. After that, the
patient is asked to draw the clock and when that task has been
completed, he/she is asked to tell the interviewer the names of the
three objects. Each correctly recalled word is worth one point and the
clock is considered normal if the time is correct and the clock is grossly
normal.
Dementia is present if the score is 0 or if the patient recalls 1-2 words
and the clock is abnormal. If the patient recalls 1-2 words and the
clock is normal or if the patient recalls all 3 words, there is no
dementia. The Mini-Cog is very quick to administer. It takes
approximately three minutes to complete and it is considered to be
very sensitive for detecting dementia.4
Clinical Dementia Rating
The Clinical Dementia Rating (CDR) was designed to assess the
severity of Alzheimer’s disease. It is rather lengthy to administer and it
depends to a degree on the subjective observations of the test
administrator, but it has been shown to be valid and sensitive.4
The patient’s abilities in the following areas are assessed when using
the CDR.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 32
Community affairs
Home and hobbies
Judgment
Memory
Orientation
Problem solving
The patient is judged on his/her abilities and performances in these
areas as follows:
0 = None
0.5 = Very mild
1 = Mild
2 = Moderate
3 = Severe
The ratings and interpretations are:
0 = Normal
0.5 to 4 = Questionable cognitive impairment
4.5 to 9 = Mild dementia
9.5 to 15.5 = Moderate dementia
≥ 16 = Severe dementia
Montreal Cognitive Assessment (MOCA)
The Montreal Cognitive Assessment (MOCA) has been shown to be a
useful screening tool for detecting MCI and detecting MCI in patients
who have Alzheimer’s disease,23,24 for identifying people with cognitive
impairment who are at risk for developing dementia,25 and identifying
patients who have dementia.26,27 The patient is assessed in 10 areas of
cognitive ability, i.e., attention, memory, and sentence repetition and

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 33
the test takes approximately 10 minutes to administer. A complete
example of the MOCA will not be presented here, as it is quite lengthy;
and, the reader is recommended to pursue additional information
online at the mocatest.org website.
Assessment Of Delirium
In many cases delirium is a clinical diagnosis that cannot be confirmed
by imaging studies, laboratory tests, or specific physical findings and
determining whether the patient does, or does not have delirium will
depend on thorough history taking and patient assessment. The
assessment process outlined below can be applied to any situation in
which delirium may be present.
Vital Signs
Assessment of the airway, breathing, and circulation (ABCs), and body
temperature is always the first step of a patient assessment. Hypo-
and hyperthermia, hypoxia, hyper- and hypotension, bradycardia,
tachycardia, respiratory depression and tachypnea can be signs of
causes of delirium. Some causes of delirium include blood loss,
congestive heart failure, dehydration, drug overdose, infection, and
myocardial infarction.
History
The events in the patient’s life prior to the onset of delirium should be
reviewed, either by speaking to the patient, family members, friends,
or caretakers. The clinician should ask specific questions about
behavior, changes in social circumstances, daily activities, elimination
patterns, food and fluid intake, and mood. It is important to learn

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 34
whether there have been any recent events such as an accident,
illness, trauma, or surgery that could be a cause of delirium.
Medical and Surgical History
The patient’s medical and surgical history should be carefully
reviewed. This review should include the medical history of the
patient’s immediate family, i.e., parents and siblings. Similar to the
history taking with dementia, the history should include a thorough
investigation into the patient’s use or abuse of substances. Since
she/he may not be forthcoming or unable to inform the interviewer
about the history of substance abuse, it may be necessary to ask
someone other than the patient about the patient’s use of alcohol
and/or illicit drugs.
Medication History
A current list of the prescription medications the patient is taking and
verification of new medications recently prescribed or changes in
dosing is important. The clinician should inquire about the use of over-
the-counter and/or herbal medications. It is important to determine if
the patient has been taking his or her medications as prescribed.
There may have been an inadvertent or intentional overdose, the
patient may have been skipping doses, or he or she may have simply
stopped taking a prescribed medication.
Physical Assessment
A physical examination can be difficult or impossible to perform if the
patient is agitated, confused, or uncooperative. If it is not possible to
do a complete physical examination then the clinician should do a

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 35
partial examination in stages and gather as much information as
possible by observing the patient.
Findings from a physical examination in situations where the patient
may be unable to cooperate may be equivocal. However, the presence
of some physical findings and the absence of others can help the
clinician decide which diagnostic tests should be done and can suggest
the cause of the delirium. For example, the patient who has had a
stroke may have hemiparesis or a patient who is dehydrated will have
dry mucous membranes and decreased skin turgor.
Laboratory Testing, Imaging Studies, Other Diagnostic Tools
There are no laboratory tests, imaging studies, or other diagnostic
tools that should be routinely performed for every patient who is
suspected of having delirium. The physical examination and history
taking should determine what is needed, and it is important to focus
diagnostic efforts in order to avoid unnecessary procedures and delays
in making the diagnosis.
Basic tests that are helpful when assessing for the presence of delirium
are the CBC, creatinine, serum calcium, electrolytes, and glucose,
arterial blood gas, 12-lead ECG, and urinalysis and urine culture. Drug
levels of medications such as digoxin and lithium should be done if
appropriate. Neuro-imaging should be done if there is no obvious
cause of delirium.8

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 36
Neurological and Psychiatric Assessment
As with the physical examination, a complete neurological and
psychiatric evaluation may not be possible if the patient is agitated,
confused, or uncooperative. When evaluating a patient for the
presence of delirium, carefully observe these areas of cognition and
behavior:1,8
Executive functioning, i.e., planning, weighing alternatives
General appearance and behavior
Insight and judgment
Memory, short-term and long-term
Language
Level of consciousness
Orientation
Language
Mood and affect
Thought content
Visuospatial functions, i.e., how well the patient analyzes and
understands space in several dimensions
The signs and symptoms of delirium include:1,8
Agitation
Anxiety
Apathy
Delusions
Difficulty with language and speech
Disorientation
Distractibility
Drowsiness

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 37
Dysarthria
Dysphasia
Emotional lability
Flight of ideas
Fluctuating level of consciousness
Hallucinations
Illusions
Inability to concentrate or focus
Memory loss
Perceptual disturbances
Restlessness
Sleep disturbances
Tremor
Standardized screening tests can be used to detect delirium. One of
the oldest and most commonly used in the Confusion Assessment
Method (CAM).8 The CAM has been shown to be accurate and
reliable.8,28 It is easy to administer and it can be used in a wide variety
of clinical situations but it does require considerable training to use
correctly.28
The CAM compares well to other delirium screening tests, but it should
be remembered that no screening test is perfect for detecting
delirium.29,30
The CAM has two parts: the first is an assessment tool that is used to
detect cognitive impairment and the second is a short screening test
that is used to distinguish delirium from dementia. Part two is

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 38
presented here, in Table 5. The diagnosis of delirium by CAM requires
the presence of features 1 and 2 and either 3 or 4.31
Table 5: The CAM Screening Test Part 2
1. Acute onset and fluctuating course
Is there evidence of an acute change in mental status from the
patient’s baseline?
Did the abnormal behavior fluctuate during the day, i.e., tend to come
and go, or increase and decrease in severity)?
2. Inattention
Did the patient have difficulty focusing attention (i.e., being easily
distractible) or have difficulty keeping track of what was being said?
3. Disorganized thinking
Was the patient’s thinking disorganized or incoherent? Did he/she have
rambling or irrelevant conversation, unclear or illogical flow of ideas, or
unpredictable switching from subject to subject?
4. Altered level of consciousness
How would you rate this patient’s level of consciousness? Alert
(normal), vigilant (hyper-alert), lethargic (drowsy, easily aroused),
stuporous (difficult to arouse), or coma (unarousable). If the patient’s
level of consciousness is anything other than alert, that should be
considered a positive score.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 39
Nursing Care Of The Patient With Dementia
Nursing care and treatment of the patient who has dementia should
focus on:
Communication
Neuropsychiatric behavioral issues
Safety and comfort
Pain Control
Medication used to treat dementia
Communication
The patient who has Alzheimer’s disease, vascular dementia, or any
pathology that causes dementia will have problems in using and
understanding language. The patient may have difficulty
understanding what is said, expressing ideas and emotions, and
responding appropriately.32 Hearing and speech impairments may be
present and depression may negatively influence the patient’s desire
to communicate.
Limitations of the patient with
dementia do not mean the patient
needs to be isolated or that the
nurse cannot have clear and
meaningful communication with
the patient. The keys to
overcoming limitations are
assessment and adjustment.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 40
The nurse caring for the dementia patient needs to assess the patient’s
communication abilities and needs and then adjust to his or her
communication style. If the nurse can do this, the interactions
between the nurse and the patient will be effective and satisfying. This
is done on an individual basis but there are some simple principles the
nurse should always keep in mind when communicating with a patient
who has dementia.
Communication problems associated with dementia do not
correspond to a loss of self-identity and studies show that the
personality endures despite these communication difficulties.33,34
When a caregiver acknowledges a patient’s self-identity, the
patient’s disruptive and combative behavior is often dissipated.
The challenge for caregivers is to discover the patient’s self-
identity.
Families and caregivers develop effective personalized
communication patterns with patients35 and it can be very
helpful to ask them how they communicate with the patient.
Reality orientation is a helpful communication strategy. It
involves constant, repetitive verbal and visual clues to keep the
patient oriented. This technique can improve functional abilities
in patients who have dementia.36,37 Potential scenarios would be
that the nurse introduces themself each time they talk to the
patient, points to calendars and clocks frequently in
conversation, and talks about current events and the plans for
the day.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 41
Speaking clearly and slowly is important in the facilitation of
meaningful and successful conversation with the patient who has
dementia. Remember to make eye contact and use short
sentences. Waiting for responses and not answering for the
patient is another helpful strategy; avoid finishing sentences for
the patient or interrupting the patient.
If the patient cannot answer or respond correctly at first, the
nurse should try again. Being aware of one’s tone and volume of
voice and of body language is important. Minimizing distractions
when communicating with the patient with dementia and
avoiding several conversations at the same time will help the
patient’s effort to communicate.
The Alzheimer’s Association publishes a guideline on
communicating with patients who have dementia that outlines
some of these strategies (accessible at alzheimers.org).
Neuropsychiatric Behavioral Problems
Neuropsychiatric behavior problems are a common and serious
complication of dementia.38-40 Agitation, aggression, anxiety, apathy,
delusions, depression, disinhibition, hallucinations, inappropriate
behavior, sleep disturbances, and wandering occur quite often and
they are disturbing for patients and caregivers. They are also
potentially dangerous and if not properly managed, they can increase
the incidence of morbidity and mortality and increase length of
hospital stay.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 42
It is often assumed that these problems are simply part of dementia
and dementia does contribute to their development, their intensity and
how and when they occur. However, the cause of and initiating factors
for agitation, aggression, inappropriate actions and speech, and other
neuropsychiatric behavioral problems is almost always internal and/or
external stimuli that are not obvious to family members, caregivers,
and health care professionals.41
The patient who has dementia frequently has cognitive deficits that
affect his or her ability to cope, communicate, and provide self-care,
and neuropsychiatric behavior problems are simply a response to
stress. It is important for the caregiver or clinician to evaluate
stressors and the patient’s response to stressors. Considering
neuropsychiatric behavior problems as “normal” for a patient who has
dementia is in one sense treating the patient as less than whole.
It is recommended that behavioral and environmental approaches
should be used to treat neuropsychiatric behavior problems before
pharmacological intervention.38,42,43 Medications should only be used in
these situations if:
Non-pharmacologic interventions have failed.
The patient has major depression with or without suicidal
ideation.
The patient has a psychosis that is causing great harm or has
the potential to do so.
The patient is very aggressive and may harm himself/herself or
others.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 43
DICE Method
The optimal approach to neuropsychiatric behavior problems can be
summarized as making every effort to understand the situation from
the patient’s point of view. A recommended method is the DICE
approach: Describe, Investigate, Create and Evaluate.44 This is a
systematic way of identifying and treating neuropsychiatric behavior
problems that operates with the assumption that such behavior
problems are caused by a stressor that can be identified and
corrected and that these issues can be solved with creativity and
patience.
Describe
In the first step of the DICE method the clinician is exploring such
questions as:
When is the patient agitated and where is he or she when this
behavior is happening?
Who was the patient interacting with or near to when the
agitation occurred?
What are the environmental conditions, the time of day?
What was the patient doing immediately before the agitation
began?
Is the patient complaining and if so, about what?
Investigate
In this step the clinician is looking for cause, by investigating such
questions as:
Was the patient recently given a medication or is he or she
scheduled for a dose?

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 44
Was the patient recently started on a medication?
Has the patient been incontinent or could he or she be in pain?
Has the patient’s daily activity schedule been changed or his or
her sleep pattern been disrupted?
What are the patient’s vital signs?
When performing this investigation it is important to remember that
many people who have dementia are elderly and have chronic medical
problems. Neuropsychiatric behavioral problems are often caused by
emotional or psychological stress, but the possibility of an acute illness
or exacerbation of an existing one should always be considered.
Create
Creating a treatment plan should be a collaborative effort between
nurses, other healthcare professionals and if they are involved in day-
to-day care, the family members. The clinician needs to focus on the
behavior that is problematic at the time, but also on root cause and
prevention. Strategies for the two can be different. The patient who is
agitated may need to be in a place that is quiet and away from others
- an immediate solution - but underlying causes such as over-
stimulation and pain need to be addressed.
Evaluate
In this final step, the clinician is evaluating the strategy in terms of
negative and positive consequences and how easy it was to apply.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 45
Safety And Comfort Of The Patient With Dementia
Safety and comfort are very important areas of care. The patient who
has dementia has a decreased capacity for decision making and may
also have limited physical capabilities. Those factors increase the risk
for accidents, errors in judgment, falls, and other forms of harm.
Discomfort is a common source of behavioral problems for the patient
who has dementia. He or she may be unable to communicate about
discomfort or take actions to relieve discomfort and this can lead to
behavioral problems such as agitation or wandering. Assessment and
re-assessment of the patient and his or her environment must be done
frequently, and the clinician should always be evaluating whether the
patient is safe and comfortable.
Pain Control
Pain is very common in patients who have dementia and it is often
under-recognized and under treated.45-47 Patients who have dementia
do not experience any less pain than older adults without dementia,
but assessment for pain in this patient population is challenging.
Patients who have dementia may not interpret sensations as painful,
have difficulty recalling pain in the recent past, and may be unable to
tell someone about their pain. In addition, the patient who has
dementia may be prescribed analgesics, antipsychotics, or other
medications that can blunt their response to pain. Untreated pain can
cause behavioral problems and psychological distress,45 and untreated
pain in any patient is unacceptable.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 46
In many patient care situations assessment for the presence of pain
and evaluating the success of treatments for pain depends in large
part on self-reporting: the patient will tell us how much pain he or she
is having and if the interventions provided relief. But for the patient
who has dementia this is often not an option. Nurses and other
healthcare professionals will need to use professional judgment and an
assessment tool.
There are many pain assessment tools available, but it is not clear
which ones are best for this clinical application. Recent reviews by
Corbett, et al. (2014) and Husebo, et al. (2016; 2014; 2010) of pain
assessment tools utilized when assessing patients with dementia noted
that the Mobilization-Observation-Behavior-Intensity-Dementia-2
(MOBID-2) pain assessment tool is useful and reliable45,47-49 and the
MOBID-2 has “... high-to-excellent reliability and aspects of
validity”.45
The MOBID-2 is very reliable for detecting the presence of pain in
patients who have dementia and could also be used to assess the
response to pain treatments.45 The MOBID-2 uses the patient’s
observed responses (facial expression, aversive/defensive behavior,
and noises indicating the presence of pain) to five simple physical
tasks, i.e., stretching both arms towards the head; and, observations
by the nurse or other caregiver of patient behavior during normal daily
activities that may indicate the presence of pain.49
The choice of pain medication should be guided by the clinical
situation. There are few controlled studies that have assessed the use
of analgesics for this patient population. Husebo, et al. (2016)

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 47
reviewed the available literature and found the evidence was strongest
for the use of acetaminophen; there was very little data on the use of
opioids; and, there are no controlled studies on the use of codeine,
non-steroidal anti-inflammatories, or tramadol.47
Medications Used to Treat Dementia
Non-pharmacologic treatments should be the first line therapies for
treating patients who have dementia and have behavioral issues such
as agitation and anxiety but these may not always be effective. The
primary drugs that are used to treat problematic behaviors in this
patient population are the cholinesterase inhibitors and memantine.
The drugs most commonly used to treat dementia are the
cholinesterase inhibitors.50,51 The three cholinesterase inhibitors
currently available in the U.S., that have a labeled use for the
treatment of dementia of Alzheimer’s disease are donepezil,
galantamine, and rivastigmine. Cholinesterase inhibitors inhibit the
activity of cholinesterase at the synaptic cleft and increase cholinergic
transmission. Patients who have Alzheimer’s disease have a decreased
cerebral synthesis of acetylcholine, but the cholinesterase inhibitors
are also used to treat vascular dementia, Lewy body disease,
frontotemporal dementia, and other forms of dementia.
The cholinesterase inhibitors can produce a mild improvement in
cognition and increase the ability to perform activities of daily living,
and they may delay progression of cognitive defects.50 The long-term
benefits of the use of cholinesterase inhibitors for patients who have
dementia is still being determined, and it is not known which patients
who have dementia should be prescribed these drugs and what the

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 48
optimum duration of therapy is.50 Regardless, most sources
recommend a trial period of cholinesterase inhibitors and donepezil,
galantamine, or rivastigmine can be used; they appear to be equally
effective.50 The dose should be slowly titrated and at the end of eight
weeks of the maximum dose the patient should be reassessed. If there
is no improvement, the drug should be stopped.50
Donepezil, galantamine, and rivastigmine are available as oral tablets,
solution, sustained-release capsules, and transdermal patch. Because
of their mechanism of action, gastrointestinal effects such as diarrhea,
nausea, and vomiting are very common. Agitation, ataxia, dizziness,
headache are also common adverse effects.
Memantine is an N-methyl-D-aspartate (NMDA) receptor antagonist. N-
methyl-D-aspartate is a neurotransmitter that mimics the action of
glutamate, one of the major excitatory neurotransmitters. Memantine
has a labeled use for the treatment of moderate to severe dementia
associated with Alzheimer’s disease and an unlabeled use for the
treatment of mild to moderate vascular dementia. Used alone or with
cholinesterase inhibitors, memantine helps improve cognition and
performance of activities of daily living, and it may slow progression of
the disease.52 Common adverse reactions effects of memantine include
confusion, dizziness, and headache. The drug is available as oral
tablets, solution, and extended-release capsules.
The use of antipsychotics for treating behavioral problems associated
with dementia is somewhat controversial. Brasure, et al., in their 2016
review write that the antipsychotic medications “... have limited
efficacy and significantly increase the risk of stroke and mortality. For

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 49
some individuals with dementia, side effects of antipsychotic
medications can lower quality of life.”38 Greenblatt, et al. (2016)
however note that the conventional and atypical antipsychotics
“... appear to have modest to moderate clnical efficacy in the
treatment of these symptoms.”53 Both of these authors acknowledge
the increased risk of mortality associated with the use of
antipsychotics in this patient population but the opinion of the risk by
Greenblatt, et al., appears tempered: “... the observed risk increase
may be partially confounded by illness severity and/or preexisting
health determinants”.53 However, Greenblatt, et al., do caution that
the dose and duration of therapy of these drugs should be minimized
and that patients shhould be continuously monitored for adverse
effects.
Press and Alexander (2016) point out that the antipsychotics do not
have a labeled use for treating behavioral disorders in patients with
dementia, and their preference is to administer these drugs only if the
patient is having severe behavioral problems and other approaches or
medications are not effective.54
The benzodiazepines may seem to be a logical choice for treating
behavioral problems associated with dementia, but they should not be
routinely used in these clinical situations.55 There is limited evidence
for their benefit and the adverse effects and risks of their use are
considerable.54,55
Depression is best treated with a selective serotonin reuptake
inhibitor.54 These drugs should be used cautiously for patients who
have dementia however, and there is little evidence of their efficacy
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 50
for treating depression in patients who have dementia.56-58 Other
medications that have been used to treat patients who have dementia,
either for symptomatic relief or as preventative measures include:
estrogen, folic acid, gabapentin, gingko biloba, lamotrigine, melatonin,
metylphenidate non-steroidal anti-inflammatories, selegiline, statins,
trazodone, valproate, vitamin B6, vitamin B12, and vitamin E.1,54 At this
time, there is either no evidence or very limited evidence that any of
these drugs, supplements, or vitamins are effective.1,54
Other Therapies and Interventions
Cognitive rehabilitation, formalized exercise programs, and
occupational therapy are relatively risk-free interventions that have
been shown to be of benefit for patients who have dementia.42
Delirium: A Medical Emergency
Delirium is considered to be a medical emergency. Therapies and
interventions that would be appropriate when treating most patients
who have delirium would be:59,60
Hydration
Assess the level of stimulation. Under- and over-stimulation can
be a problem for patients who have delirium.
Re-orientation techniques
Bedside sitter
If possible and if it helps, close contact with a family member or
someone familiar to the patient is encouraged.
Make sure the patient has his or her corrective lenses and/or
hearing aid if they use these.
Maintain normal sleep patterns.
Assess for and treat pain.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 51
Non-pharmacologic interventions should always be the first-line choice
for patients who have delirium.59 Physical restraints should not be
used unless other interventions have failed and there is risk to the
patient or others.59 Antipsychotics can be used to treat severe
agitation in patients who have delirium, but they do have significant
side effects and there is little data that supports their use for the
treatment of delirium.59
The standard pharmacological therapy for treating patients who have
delirium and who do not respond to non-pharmacological interventions
is haloperidol.59 Haloperdiol and the atypical antipsychotics olanzapine,
quetiapine, risperidone ziprasidone have all been shown to be effective
in treating delirium.59-61 Drowsiness, hypotension, and extrapyramidal
effects are common adverse effects of the antipsychotics.
Benzodiazepines are useful if the delirium is caused by alcohol or drug
withdrawal,59 but in other types of delirium they may worsen the
patient’s confusion and cause sedation.
Summary
Dementia and delirium are neurological disorders that cause signficant
cognitive impairment and increase the risk of morbidity and mortality.
These diseases can be difficult to detect and diagnose. Some cases of
dementia and many cases of delirium are reversible, but dementia is
most often chronic, progressive, and cannot be cured; and, the
dementias and deliriums that are considered reversible may result in
serious complications. The most common cause of dementia is
Alzheimer’s disease. Medications and dementia appear to be the most
common causes of delirium.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 52
Advanced age itself is not a cause of either disease, but the elderly do
have a high risk for developing dementia and delirium and as the U.S.,
population continues to get older, the incidences of dementia and
delirium are likley to increase. Treatment of dementia and delirium is
primarily symptomatic and supportive unless there is a clearly
identified etiology. Primary concerns when providing nursing care for
the patient who has either dementia or delirium are: monitoring of
vitals signs, behavioral and environmental interventions, safety and
comfort, pain control, and safe administration of medications.
Please take time to help NurseCe4Less.com course planners evaluate the nursing knowledge needs met by completing the self-assessment
of Knowledge Questions after reading the article, and providing feedback in the online course evaluation.
Completing the study questions is optional and is NOT a course requirement.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 53
1. One of the defining characteristics of dementia is
a. inability to perform activities of daily living.
b. severe agitation. c. reversible cognitive impairment.
d. occurrence before age 50.
2. Most cases of dementia are caused by
a. trauma and heavy metal poisoning. b. infections and hemorrhage.
c. Alzheimer’s disease and vascular pathologies. d. hypoxia and Parkinson’s disease.
3. Defining characteristics of delirium include
a. movement disorders and a progressive cognitive decline. b. attention deficits and confusion.
c. expressive aphasia and hypotension. d. hyperthermia and depression.
4. The onset of delirium is
a. acute.
b. slow. c. chronic.
d. fluctuating.
5. Common causes of delirium include
a. Parkinson’s disease and advanced age.
b. drug withdrawal and Lewy body dementia. c. acute blood loss and frontotemporal dementia.
d. drugs and dementia.
6. True or False: Dementia is an inevitable consequence of aging.
a. True
b. False

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 54
7. The onset of neurologic changes of dementia are usually
a. acute.
b. slow and progressive. c. chronic.
d. fluctuating and regressive.
8. Use physical restraints with patients who have dementia
a. if the patient is agitated or confused. b. when there is a significant risk for a fall.
c. if all other interventions fail and there is a serious risk of harm.
d. if the patient is likely to wander.
9. Neuropsychiatric behavior problems in patients who have
dementia
a. are caused by an external or internal stimulus. b. typically occur randomly and without cause.
c. only occur if patients are over-medicated. d. happen primarily at night.
10. The use of antipsychotics for treating patients who have
dementia
a. is considered first-line therapy. b. is most effective when used in conjunction with cholinesterase
inhibitors. c. can reverse the progress of dementia.
d. is questionably effective and potentially dangerous.
11. The drug most commonly used to treat agitation in patients
who have delirium is
a. diazepam. b. haloperidol.
c. galantmine. d. bupropion.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 55
12. True or False: Physical restraints are the first-choice
therapy for treating patients who have delirium.
a. True b. False
13. Benzodiazepines are
a. the first-line treatment for dementia or delirium.
b. absolutely contraindicated for dementia or delirium. c. seldom useful and may worsen dementia or delirium.
d. only useful if used together with antipsychotics.
14. Which of the following is commonly used to treat dementia?
a. Fluvoxamine. b. Lithium.
c. Methylphenidate. d. Rivastigmine.
15. Which of the following is commonly used to treat
dementia?
a. Memantine. b. Nortriptyline.
c. Carbamazepine. d. Diphenhydramine.
16. Dementia is a syndrome because the signs and symptoms
of dementia
a. are specific to a single age group.
b. cannot be eliminated or cured. c. can have many different causes.
d. is a major cognitive disorder.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 56
17. The Diagnostic and Statistical Manual of Mental Disorders,
fifth edition, (DSM-5) has replaced the term dementia with the term
a. major/mild cognitive disorder.
b. major/minor cognitive deficit. c. dementia syndrome.
d. neurocognitive syndrome.
18. Cognitive deficits do not occur exclusively in the context of delirium with respect to which of the following syndromes?
a. Only with major cognitive disorder
b. With major or mild cognitive disorder c. When mental illness (e.g., schizophrenia) is not present
d. Only with minor cognitive disorder
19. Dementia can be usefully divided into two categories:
a. dementia syndrome and senior dementia.
b. unspecified and specified. c. cognitive disorder and cognitive deficit.
d. reversible and irreversible.
20. True or False: Most cases of dementia are irreversible.
a. True b. False
21. Which of the following is NOT able to cause irreversible
dementia?
a. Degenerative diseases of the nervous system
b. Trauma c. Vascular disorders
d. None of the above
22. In most cases, dementia caused by _______________ is reversible but not always.
a. carbon monoxide poisoning
b. aging c. a drug
d. hypoxia

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 57
23. Drugs that can cause dementia and delirium include:
a. alcohol.
b. anti-arrhythmics. c. skeletal muscle relaxers.
d. All of the above
24. Alzheimer’s disease is seen in the characteristic ___________________ in the parietal and temporal lobes.
a. lesions
b. protein deposits c. destruction of dopamine-producing cells
d. thrombotic obstructions
25. Frontotemporal lobe dementia is a neurodegenerative
disease caused by _____________ the frontal and temporal lobe.
a. thrombotic obstructions of
b. atrophy of c. protein deposits in
d. All of the above
26. ____________________ is a chronic, progressive neurodegenerative disease that is characterized by the
presence of abnormal deposits of protein that accumulate in neurons in specific areas of the brain.
a. Lewy body dementia
b. Frontotemporal lobe dementia
c. Parkinson’s disease d. Vascular dementia
27. Patients who have dementia often suffer from
neuropsychiatric problems such as
a. language impairment. b. arrhythmias.
c. agitation. d. hypoxia.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 58
28. True or False: In dementia patients, there is typically no
disturbance of consciousness: the patient is awake, alert, and responsive.
a. True
b. False
29. In Alzheimer’s disease, lesions in the parietal and temporal lobes
a. interrupt the normal metabolism of neurons.
b. interrupt self-repair of neurons. c. disrupt communication between different areas of the brain.
d. All of the above
30. When making the diagnosis of ____________ it must be
specified if it is hyperactive, hypoactive, or involves a mixed level of activity.
a. Parkinson’s disease
b. vasculitis c. dementia
d. delirium
31. ___________ is an acute change in mental status characterized by confusion and disturbances in cognition.
a. Hypoxia
b. Vasculitis c. Dementia
d. Delirium
32. Parkinson’s disease’s characteristic motor symptoms are
similarly found with __________________ patients.
a. Lewy body dementia b. Alzheimer’s disease
c. frontotemporal dementia d. vascular dementia
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 59
33. Lewy body dementia is distinguished from other types of
dementia by
a. thrombotic obstructions. b. behavioral and speech defects.
c. visual hallucinations. d. expressive and fluent aphasia.
34. The hallmark signs of frontotemporal dementia are
a. visual hallucinations.
b. Parkinsonian motor signs. c. behavioral and speech defects.
d. bradykinesia and tremors.
35. With Alzheimer’s disease, the time from diagnosis to death
can be as little as
a. seven years. b. 10 years.
c. five years. d. three years.
36. True or False: Smoking is a significant risk factor for the
development of vascular dementia.
a. True b. False
37. ______________________ (a 10-minute test to
administer) has been shown to be a useful screening tool
for detecting mild cognitive impairment (MCI) and detecting MCI in patients who have Alzheimer’s disease,
and dementia, and who are at risk for developing dementia.
a. The Montreal Cognitive Assessment (MOCA)
b. The Mini-Cog test c. The Clinical Dementia Rating (CDR)
d. The ABC test
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 60
38. Depression in the elderly can cause many of the cognitive
defects that are common to
a. delirium. b. dementia.
c. Parkinsonian motor signs. d. normal aging.
39. Mild cognitive impairment is a term used to describe
cognitive deficits that are
a. a normal part of aging. b. fit into the diagnostic criteria for dementia.
c. in an intermediate state between normal cognitive functioning and dementia.
d. All of the above
40. True or False: It is well established that advanced age
itself is a risk factor for delirium.
a. True b. False
41. In many cases, delirium is
a. confirmed by laboratory tests.
b. confirmed by imaging studies. c. confirmed through specific physical findings.
d. a clinical diagnosis.
42. When delirium is suspected, the first step of a patient
assessment includes
a. neuro-imaging to confirm whether delirium is present. b. urinalysis and urine culture.
c. a 12-lead ECG. d. assessment of the airway, breathing, and circulation (ABCs).

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 61
43. One of the oldest and most commonly used standardized
screening tests used to detect delirium is
a. the Confusion Assessment Method (CAM). b. the Mini-Cog test
c. the Clinical Dementia Rating (CDR) d. the ABC test
44. The CAM has two parts: the first is an assessment tool that
is used to detect cognitive impairment and the second is a short screening test that is used
a. to distinguish delirium from drug usage.
b. to distinguish delirium from dementia. c. to identify Parkinsonian motor signs.
d. to diagnose Alzheimer’s disease.
45. In addition to assessing a patient’s airway, breathing, and
circulation (ABCs), the first step of a patient assessment for delirium includes
a. a complete blood test (CBC).
b. a urinalysis and urine culture. c. taking the patient’s body temperature.
d. neuro-imaging to confirm whether delirium is present.
46. True or False: When communicating with a patient who has dementia, a nurse should avoid finishing sentences for the
patient or interrupting the patient.
a. True
b. False
47. When a caregiver acknowledges a patient’s ___________ the patient’s disruptive and combative behavior is often
dissipated.
a. self-identity b. condition
c. limitations d. inability to communicate

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 62
48. A nurse introduces herself to the patient each time she
talks to the patient, points to calendars and clocks frequently in conversation, and talks about current events:
this is an example of a. acknowledging the patient’s self-identity.
b. recognizing limitations.
c. an inability to communicate.
d. reality orientation.
49. Successful conversation with the patient who has dementia involves
a. making eye contact.
b. using short sentences. c. speaking clearly and slowly.
d. All of the above
50. It is recommended that dementia patients with neuropsychiatric behavior problems be treated
a. only if the patient is a danger to himself or others. b. first using pharmacological intervention.
c. first using behavioral and environmental approaches. d. if the patient has concomitant delirium.
51. True or False: Neuropsychiatric behavior problems are
normal for a patient who has dementia and a nurse should accept it as part of the patient experience.
a. True
b. False
52. A recommended method for identifying and treating neuropsychiatric behavior problems in dementia patients is
known as
a. the DICE Method.
b. the Confusion Assessment Method (CAM). c. the Montreal Cognitive Assessment (MOCA).
d. the Mini-Cog.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 63
53. The ____________________________________ is very
reliable for detecting the presence of pain in patients who have dementia and could also be used to assess the
response to pain treatments.
a. DICE Method b. Confusion Assessment Method (CAM)
c. Montreal Cognitive Assessment (MOCA) d. Mobilization-Observation-Behavior-Intensity-Dementia-2
(MOBID-2).
54. The drugs most commonly used to treat dementia are
a. antipsychotics. b. cholinesterase inhibitors.
c. benzodiazepines.
d. All of the above
55. The DICE Method operates with the assumption that neuropsychiatric behavior problems in dementia patients
are caused by
a. reality disorientation. b. dementia.
c. a stressor. d. delirium.
56. When treating dementia, the dose of cholinesterase
inhibitors should be slowly titrated and at the end of ___________ of the maximum dose the patient should be
reassessed.
a. one month
b. eight weeks c. one week
d. six months
57. If there is no improvement for the dementia patient at the end of the trial of doing with cholinesterase inhibitors,
a. the drug should be stopped.
b. drug dosing should be increased. c. drug treatment should be continued until improvement is seen.
d. None of the above

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 64
58. True or False: The benzodiazepines may seem to be a
logical choice for treating behavioral problems associated with dementia, but they should not be routinely used in
these clinical situations.
a. True b. False
CORRECT ANSWERS:
1. One of the defining characteristics of dementia is
a. inability to perform activities of daily living.
2. Most cases of dementia are caused by
b. Alzheimer’s disease and vascular pathologies.
3. Defining characteristics of delirium include
b. attention deficits and confusion.
4. The onset of delirium is
a. acute.
5. Common causes of delirium include
c. drugs and dementia.
6. True or False: Dementia is an inevitable consequence of aging.
b. False
7. The onset of neurologic changes of dementia are usually
b. slow and progressive.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 65
8. Use physical restraints with patients who have dementia
c. if all other interventions fail and there is a serious risk of
harm.
9. Neuropsychiatric behavior problems in patients who have dementia
a. are caused by an external or internal stimulus.
10. The use of antipsychotics for treating patients who have
dementia
d. is questionably effective and potentially dangerous.
11. The drug most commonly used to treat agitation in patients
who have delirium is
b. haloperidol.
12. True or False: Physical restraints are the first-choice therapy for treating patients who have delirium.
b. False
13. Benzodiazepines are
c. seldom useful and may worsen dementia or delirium.
14. Which of the following is commonly used to treat
dementia?
d. Rivastigmine.
15. Which of the following is commonly used to treat
dementia?
a. Memantine.
16. Dementia is a syndrome because the signs and symptoms of dementia
c. can have many different causes.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 66
17. The Diagnostic and Statistical Manual of Mental Disorders,
fifth edition, (DSM-5) has replaced the term dementia with the term
a. major/mild cognitive disorder.
18. Cognitive deficits do not occur exclusively in the context of
delirium with respect to which of the following syndromes?
b. With major or mild cognitive disorder
19. Dementia can be usefully divided into two categories:
d. reversible and irreversible.
20. True or False: Most cases of dementia are irreversible.
a. True
21. Which of the following is NOT able to cause irreversible
dementia?
d. None of the above
22. In most cases, dementia caused by _______________ is reversible but not always.
c. a drug
23. Drugs that can cause dementia and delirium include:
d. All of the above
24. Alzheimer’s disease is seen in the characteristic ___________________ in the parietal and temporal lobes.
a. lesions
25. Frontotemporal lobe dementia is a neurodegenerative
disease caused by _____________ the frontal and temporal lobe.
b. atrophy of

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 67
26. ____________________ is a chronic, progressive
neurodegenerative disease that is characterized by the presence of abnormal deposits of protein that accumulate
in neurons in specific areas of the brain.
a. Lewy body dementia
27. Patients who have dementia often suffer from neuropsychiatric problems such as
c. agitation.
28. True or False: In dementia patients, there is typically no
disturbance of consciousness: the patient is awake, alert, and responsive.
a. True
29. In Alzheimer’s disease, lesions in the parietal and temporal lobes
d. All of the above
30. When making the diagnosis of ____________ it must be
specified if it is hyperactive, hypoactive, or involves a mixed level of activity.
d. delirium
31. ___________ is an acute change in mental status
characterized by confusion and disturbances in cognition.
d. Delirium
32. Parkinson’s disease’s characteristic motor symptoms are
similarly found with __________________ patients.
a. Lewy body dementia
33. Lewy body dementia is distinguished from other types of dementia by
c. visual hallucinations.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 68
34. The hallmark signs of frontotemporal dementia are
c. behavioral and speech defects.
35. With Alzheimer’s disease, the time from diagnosis to death
can be as little as
d. three years.
36. True or False: Smoking is a significant risk factor for the development of vascular dementia.
a. True
37. ______________________ (a 10-minute test to
administer) has been shown to be a useful screening tool
for detecting mild cognitive impairment (MCI) and detecting MCI in patients who have Alzheimer’s disease,
and dementia, and who are at risk for developing dementia.
a. The Montreal Cognitive Assessment (MOCA)
38. Depression in the elderly can cause many of the cognitive
defects that are common to
b. dementia.
39. Mild cognitive impairment is a term used to describe cognitive deficits that are
c. in an intermediate state between normal cognitive functioning and dementia.
40. True or False: It is well established that advanced age
itself is a risk factor for delirium.
b. False
41. In many cases, delirium is
d. a clinical diagnosis.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 69
42. When delirium is suspected, the first step of a patient
assessment includes
d. assessment of the airway, breathing, and circulation (ABCs).
43. One of the oldest and most commonly used standardized screening tests used to detect delirium is
a. the Confusion Assessment Method (CAM).
44. The CAM has two parts: the first is an assessment tool that
is used to detect cognitive impairment and the second is a short screening test that is used
b. to distinguish delirium from dementia.
45. In addition to assessing a patient’s airway, breathing, and circulation (ABCs), the first step of a patient assessment
for delirium includes
c. taking the patient’s body temperature.
46. True or False: When communicating with a patient who has dementia, a nurse should avoid finishing sentences for the
patient or interrupting the patient.
a. True
47. When a caregiver acknowledges a patient’s ___________ the patient’s disruptive and combative behavior is often
dissipated.
a. self-identity
48. A nurse introduces herself to the patient each time she
talks to the patient, points to calendars and clocks frequently in conversation, and talks about current events:
this is an example of
d. reality orientation.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 70
49. Successful conversation with the patient who has dementia
involves
d. All of the above
50. It is recommended that dementia patients with neuropsychiatric behavior problems be treated
c. first using behavioral and environmental approaches.
51. True or False: Neuropsychiatric behavior problems are
normal for a patient who has dementia and a nurse should accept it as part of the patient experience.
b. False
52. A recommended method for identifying and treating neuropsychiatric behavior problems in dementia patients is
known as
a. the DICE Method.
53. The ____________________________________ is very reliable for detecting the presence of pain in patients who
have dementia and could also be used to assess the response to pain treatments.
d. Mobilization-Observation-Behavior-Intensity-Dementia-2
(MOBID-2).
54. The drugs most commonly used to treat dementia are
b. cholinesterase inhibitors.
55. The DICE Method operates with the assumption that
neuropsychiatric behavior problems in dementia patients are caused by
c. a stressor.
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 71
56. When treating dementia, the dose of cholinesterase
inhibitors should be slowly titrated and at the end of ___________ of the maximum dose the patient should be
reassessed.
b. eight weeks
57. If there is no improvement for the dementia patient at the end of the trial of doing with cholinesterase inhibitors,
a. the drug should be stopped.
58. True or False: The benzodiazepines may seem to be a
logical choice for treating behavioral problems associated with dementia, but they should not be routinely used in
these clinical situations.
a. True
References Section
The reference section of in-text citations include published works
intended as helpful material for further reading. Unpublished works
and personal communications are not included in this section, although
may appear within the study text.
1. Kane RL, Ouslander JG, Abrass IB, Resnick B. Dementia and
delirium. Essentials of Clinical Geriatrics. 7th ed. New York, NY:
McGraw-Hill; 2013. Online edition. Accessed September 25, 2014
from www.UCHC.edu.
2. Fiest KM, Roberts JI, Maxwell CJ, et al. The prevalence and
incidence of dementia due to Alzheimer's disease: a systematic
review and meta-analysis. Can J Neurol Sci. 2016;43(Suppl
1):S51-S82.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 72
3. Centers for Disease Control and Prevention. Alzheimer’s Disease.
July 25, 2104.
http://www.cdc.gov/aging/aginginfo/alzheimers.htm. Accessed
August 8. 2016.
4. Larson EB. Evaluation of cognitive impairment and dementia.
UpToDate. October 28, 2015. From
http://www.uptodate.com/contents/evaluation-of-cognitive-
impairment-and-
dementia?source=search_result&search=dementia&selectedTitle=
1%7E150. Accessed August 7, 2016.
5. Cole MG, Mccusker J. Delirium in older adults: a chronic cognitive
disorder? Int Psychogeriatr. 2016;28(8):1229-1233.
6. American Psychiatric Association. Major and mild neurocognitive
disorders. In: Diagnostic and Statistical Manual of Mental
Disorders, Fifth ed. Alexandria, VA: American Psychiatric
Association; 2013.
7. Greenberg DA, Aminoff MJ, Simon RP. Dementia & Amnestic
Disorders. Clinical Neurology, 8th ed. New York, NY: McGraw-
Hill;2012. Accessed September 25, 2014 from www. UCHC.edu.
8. Francis J, Young, GB. Diagnosis of delirium and acute confusional
states. UpToDate. August 22, 2014.
http://www.uptodate.com/contents/diagnosis-of-delirium-and-
confusional-
states?source=search_result&search=Delirium+and+acute&select
edTitle=2%7E150. Accessed August 8, 2016.
9. American Psychiatric Association. Delirium. Diagnostic and
Statistical Manual of Mental Disorders, 5th ed. Arlington, VA:
American Psychiatric Publishing; 2013.
10. Langa KM, Levine DA. The diagnosis and management of mild
cognitive impairment: a clinical review. JAMA. 2014;
312(23):2551-2561
11. McDade EN, Petersen RN. Mild cognitive impairment:
epidemiology, pathology, and clinical assessment. UpToDate,
October 30, 2015. http://www.uptodate.com/contents/mild-
cognitive-impairment-epidemiology-pathology-and-clinical-
assessment?source=search_result&search=mild+cognitive+impai
rment&selectedTitle=1%7E56. Accessed August 8, 2016.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 73
12. Sachdev PS, Lipnicki DM, Crawford J, et al. Factors predicting
reversion from mild cognitive impairment to normal cognitive
functioning: a population-based study. PLoS One.
2013;(3):e59649. doi: 10.1371/journal.pone.0059649. Epub
2013 Mar 27.
13. Fisman M. Pseudo-dementia. Prog Neuropsychopharmaco Bio
Psychiatry. 1985;9(5-6):481-484
14. Kang H, Zhao F, You L, et al. Pseudo-dementia: A
neuropsychological review. Ann Indian Acad Neurol.
2014;17(2):147-154.
15. Yokomizo JE, Simon SS, de Campos Bottino CM. Cognitive
screening for dementia in primary care: a systematic review. Intl
Psychogeriatr. 2014;26(11):1783-1804.
16. Seeley WW, Miller BL. Dementia. In: Longo DL, Fauci AS, Kasper
DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison’s Principles
of Internal Medicine, 19th ed. New York, NY: McGraw-Hill; 2015.
On line edition. Accessed August 8, 2016 from www.UCHC.edu.
17. Grossman M, Irwin DJ. The mental status examination in patients
with suspected dementia. Continuum (Minneap Minn)
2016;22(2):385--403.
18. Galvin JE, Roe CM, Xiong X, Morris JC. Validity and reliability of
the ADB informant interview in dementia. Neurology.
2006;67(11):1942-1948.
19. Mortimer M, Likeman M, Lewis TT. Neuroimaging in dementia: a
practical guide. Practl Neurol. 2013;13(2):92-103.
20. Kanev T, Sablosky M, Vento J, O’Hanlon D. Structural and
functional neuro-imaging methods in the diagnosis of dementia: A
retrospective chart and brain imaging review. Neurocase.
2012;18(3):224-234.
21. Tsoi KK, Chan JY, Hirai HW, Wong SY, Kwok TC. Cognitive tests to
detect dementia: A systematic review and meta-analysis. JAMA
Intern Med. 2015;175(9):1450-1458.
22. Lin JS, O'Connor E, Rossom RC, Perdue LA, Eckstrom E. Screening
for cognitive impairment in older adults: A systematic review for
the US Preventive Services Task Force. Ann Intern Med.
2013;159(9):601-612.
23. Freitas S, Simões MR, Alves L, Santana I. Montreal cognitive
assessment: validation study for mild cognitive impairment and

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 74
Alzheimer disease. Alzheimer Dis Assoc Disord. 2013; 27(1):37-
43.
24. O'Caoimh R, Timmons S, Molloy DW. Screening for mild cognitive
impairment: Comparison of "MCI Specific" screening instruments.
J Alzheimers Dis. 2016;51(2):619-629.
25. Lam B, Middleton LE, Masellis M, Stuss DT, Harry RD, Kiss A.
Criterion and convergent validity of the Montreal Cognitive
Assessment with screening and standardized neuropsychological
testing. J Amer Geriatr Soc. 2013;61(12):2181-2185.
26. Dong Y, Lee WY, Basri NA, et al. The Montreal Cognitive
Assessment is superior to the Mini-Mental State Examination in
detecting patients at higher risk of dementia. Int Psychogeriatr.
2012; 24(11):1749-1755.
27. Wang CS, Pai MC, Chen PL, Hou NT, Chien PF, Huang YC.
Montreal Cognitive Assessment and Mini-Mental State
Examination performance in patients with mild-to-moderate
dementia with Lewy bodies, Alzheimer's disease, and normal
participants in Taiwan. Int Psychogeriatr. 2013;25(11):1839-
1845.
28. Han JH, Wilson A, Graves AJ, Shintani A, Schnelle JF, Ely EW. A
quick and easy delirium assessment for nonphysician research
personnel. Am J Emerg Med. 2016;34(6):1031-1036.
29. Wong CL, Holroyd-Leduc J, Simel DL, Straus SE. Does this patient
have delirium?: value of bedside instruments. JAMA 2010;
304(7):779-786.
30. Hendry K, Quinn TJ, Evans J, et al. Evaluation of delirium
screening tools in geriatric medical inpatients: a diagnostic test
accuracy study. Age Ageing. 2016 Aug 8. [Epub ahead of print]
31. Waszynski CM. Confusion Assessment Method (CAM). Try This:
Best Practices in Nursing Care to Older Adults. The Hartford
Institute for Geriatric Nursing. 2001;November, Issue 13.
32. Veselinova C. Influencing communication and interaction in
dementia. Nursing & Residential Care. 2014;16(3):162-166.
33. Skaalvik MW, Fjelltun AM, Normann HK, Norberg A. Expressions
of sense of self among individuals With Alzheimer's disease. Res
Theory Nurs Pract. 2016;30(2):161-175.
34. O’Connell B, Gardner A, Takase M, et al. Clinical usefulness and
feasibility of using reality orientation with patients who have

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 75
dementia in acute care settings. Int J Nurs Pract.
2007;13(3):182-192.
35. Miller C. Communication difficulties in hospitalized older adults
with dementia. Am J Nurs. 2008;108(3):59-66.
36. Dourado MC, Laks J. Psychological interventions for
neuropsychiatric disturbances in mild and moderate Alzheimer's
disease: Current evidences and future directions. Curr Alzheimer
Res. 2016 Jul 28. [Epub ahead of print]
37. Camargo CH, Justus FF, Retzlaff G. The effectiveness of reality
orientation in the treatment of Alzheimer's disease. Am J
Alzheimers Dis Other Demen. 2015;30(5):527-532.
38. Brasure M, Jutkowitz E, Fuchs E, Nelson VA, Kane RA, Shippee T,
Fink HA, Sylvanus T, Ouellette J, Butler M, Kane RL.
Nonpharmacologic Interventions for Agitation and Aggression in
Dementia. Comparative Effectiveness Review No. 177. (Prepared
by the Minnesota Evidence-based Practice Center under Contract
No. 290-2012-00016-I.) AHRQ Publication No.16-EHC019-EF.
Rockville, MD: Agency for Healthcare Research and Quality; March
2016. www.effectivehealthcare.ahrq.gov/reports/final.cfm.
Accessed August 1, 2016.
39. Dourado MC, Laks J. Psychological interventions for
neuropsychiatric disturbances in mild and moderate Alzheimer's
disease: Current evidences and future directions. Curr Alzheimer
Res. 2016 Jul 28. [Epub ahead of print]
40. Mitoku K, Shimanouchi S. The decision-making and
communication capacities of older adults with dementia: A
population-based study. The Open Nurs J: 2014;8:17-24.
41. Rabins, PV, Blass DM. In the clinic: Dementia. Ann Int Med. 2014;
161(3):ITC1. doi:10.7326/0003-4819-161-3-201408050-01002.
42. Kales HC. Common sense: Addressed to geriatric psychiatrists on
the subject of behavioral and psychological symptoms of
dementia. Am J Geriatr Psychiatry. 2015;23(12):1209-1213.
43. Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of
behavioral and psychological symptoms of dementia. BMJ. 2015
Mar 2;350:h369. doi: 10.1136/bmj.h369.
44. Kales HC, Gitlin LN, Lyketsos CG; Detroit Expert Panel on
Assessment and Management of Neuropsychiatric Symptoms of
Dementia. Management of neuropsychiatric symptoms of
nursece4less.com nursece4less.com nursece4less.com nursece4less.com 76
dementia in clinical settings: recommendations from a
multidisciplinary expert panel. J Am Geriatr Soc. 2014;
62(4):762-769.
45. Corbett A, Husebo BS, Achterberg WP, Aarsland D, Erdal A, Flo E.
The importance of pain management in older people with
dementia. Br Med Bull. 2014;111(1):139-148.
46. Chandler RC, Zwakhalen SM, Docking R, Bruneau B, Schofield P.
Attitudinal & knowledge barriers towards effective pain
assessment & management in dementia: A narrative synthesis.
Curr Alzheimer Res. 2016 Jun 2. [Epub ahead of print]
47. Husebo BS, Achterberg W, Flo E. Identifying and managing pain in
people with Alzheimer's disease and other types of dementia: A
systematic review. CNS Drugs. 2016;30(6):481-497.
48. Husebo BS, Ostelo R, Strand LI. The MOBID-2 pain scale:
reliability and responsiveness to pain in patients with dementia.
Eur J Pain. 2014;18(10):1419-1430.
49. Husebo BS, Strand LI, Moe-Nilssen R, Husebo SB, Ljunggren AE.
Pain in older persons with severe dementia. Psychometric
properties of the Mobilization-Observation-Behaviour-Intensity-
Dementia (MOBID-2) Pain Scale in a clinical setting. Scan J Caring
Sci. 2010;24(2):380-391.
50. Press D, Alexander M. Cholinesterase inhibitors in the treatment
of dementia. UpToDate. December 11, 2015.
https://remote.uchc.edu/Citrix/UConnHealthWeb/clients/HTML5Cli
ent/src/SessionWindow.html?launchid=1471023199589. Accessed
August 12, 2016.
51. Campos C, Rocha NB, Vieira RT, et al. Treatment of cognitive
deficits in Alzheimer's disease: A psychopharmacological review.
Psychiatr Danub. 2016;28(1):2-12.
52. Deardorff WJ, Grossberg GT. Pharmacotherapeutic strategies in
the treatment of severe Alzheimer's disease. Expert Opin
Pharmacother. 2016; 29:1-12.
53. Greenblatt HK, Greenblatt DJ. Use of antipsychotics for the
treatment of behavioral symptoms of dementia. J Clin Pharmacol.
2016 Mar 7. doi: 10.1002/jcph.731. [Epub ahead of print]
54. 55. Press D, Alexander M. Management of neuropsychiatric
symptoms of dementia. UpToDate. June 6, 2016.
https://www.uptodate.com/contents/management-of-

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 77
neuropsychiatric-symptoms-of-dementia. Accessed August 13,
2016.
55. Defrancesco M, Marksteiner J, Fleischhacker WW, Blasko I. Use of
benzodiazepines in Alzheimer's disease: A systematic review of
literature. Int J Neuropsychopharmacol. 2015 May
19;18(10):pyv055. doi: 10.1093/ijnp/pyv055.
56. Puranen A, Taipale H, Koponen M, et al. Incidence of
antidepressant use in community-dwelling persons with and
without Alzheimer's disease: 13-year follow-up. Int J Geriatr
Psychiatry. 2016 Feb 28. doi: 10.1002/gps.4450. [Epub ahead of
print]
57. Laitinen ML, Lönnroos E, Bell JS, Lavikainen P, Sulkava R,
Hartikainen S. Use of antidepressants among community-dwelling
persons with Alzheimer's disease: a nationwide register-based
study. Int Psychogeriatr. 2015;27(4):669-672.
58. Sepehry AA, Lee PE, Hsiung GY, Beattie BL, Jacova C. Effect of
selective serotonin reuptake inhibitors in Alzheimer's disease with
comorbid depression: a meta-analysis of depression and cognitive
outcomes. Drugs Aging. 2012;29(10):793-806.
59. Francis J. Delirium and acute confusional states: Prevention,
treatment, and prognosis. UpToDate. August 13, 2014.
http://www.uptodate.com/contents/delirium-and-acute-
confusional-states-prevention-treatment-and-prognosis. Accessed
August 8, 2016.
60. Balas MC, Rice M, Chaperon C, Smith H, Disbot M, Fuchs B.
Management of delirium in critically ill older adults. Critl Care
Nurse. 2012;32(4):15-26.
61. Yoon HJ, Park KM, Choi WJ, et al. Efficacy and safety of
haloperidol versus atypical antipsychotic medications in the
treatment of delirium. BMC Psychiatry. 2013 Sep 30;13:240. doi:
10.1186/1471-244X-13-240.

nursece4less.com nursece4less.com nursece4less.com nursece4less.com 78
The information presented in this course is intended solely for the use of healthcare
professionals taking this course, for credit, from NurseCe4Less.com.
The information is designed to assist healthcare professionals, including nurses, in
addressing issues associated with healthcare.
The information provided in this course is general in nature, and is not designed to
address any specific situation. This publication in no way absolves facilities of their
responsibility for the appropriate orientation of healthcare professionals.
Hospitals or other organizations using this publication as a part of their own
orientation processes should review the contents of this publication to ensure
accuracy and compliance before using this publication.
Hospitals and facilities that use this publication agree to defend and indemnify, and
shall hold NurseCe4Less.com, including its parent(s), subsidiaries, affiliates,
officers/directors, and employees from liability resulting from the use of this
publication.
The contents of this publication may not be reproduced without written permission
from NurseCe4Less.com.


















