Delirium - an overview
43
DELIRIUM
-
Upload
sriram-periasamy -
Category
Health & Medicine
-
view
25 -
download
1
Transcript of Delirium - an overview
DELIRIUM
WHAT IS IN THIS PRESENTATION:
Why do we need to know about delirium?
What is delirium?
D/D with respect to psychiatry
How to prevent delirium?
Diagnosis and assessment
Treatment
WHY DO WE NEED TO KNOW ABOUT DELIRIUM?
WHY DO WE NEED TO KNOW ABOUT DELIRIUM?
Delirium is common
Delirium is associated with increased complications
Delirium is often unrecognized
Delirium is preventable
WHAT IS DELIRIUM?

WHAT IS DELIRIUM?
• Acute confusional state
• Constellation of symptoms
• Widespread disruption of higher cortical function
• Acute onset and fluctuating course
• Three core domains:
- cognitive with disproportionate impairment of attention
- circadian disturbance (sleep wake cycle, motor alterations)
- disturbances of higher level of thinking(comprehension, language, thinking process)

CORE FEATURES & ASSOCIATED FEATURES
Core features:• Features that are almost invariably present• Disturbances of - attention - memory - orientation - language - thought process - sleep-wake cycle
Meagher et
al 2007 BJP
CORE FEATURES & ASSOCIATED FEATURES
Associated features:
• Features that are more variable in presentation
• Psychotic symptoms• Affective disturbances• Different motoric profiles
Meagher et al 2007 BJP
IMPAIRMENT OF CONSCIOUSNESS Universal, fluctuating
Barely perceptible dulling of awareness to profound coma
Worsen at night, with fatigue, decreased environmental stimuli
Failure to be selective -----------distractible
Failure to mobilize & sustain attention -------impaired attention
Inability to shift attention------------perseveration
Minor degree---vague malaise, feelings of uncertainity, difficulties in judging passage of time, focusing attention, neglect of appearance, episode of incontinence
Severe degree----too slow in responding, loses thread in conversation, attention to outside events hard to arouse and sustain, drowsy
RECENT WORKS
• Disorder of global cognition
• Prominent disturbance of attention
• Disorientation is least frequent core symptom
• Cognition & language are not as fluctuant as previously described
• Subsyndromal , resolving , persisting delirium
Meagher et al BJP 2012 & BJP 2007
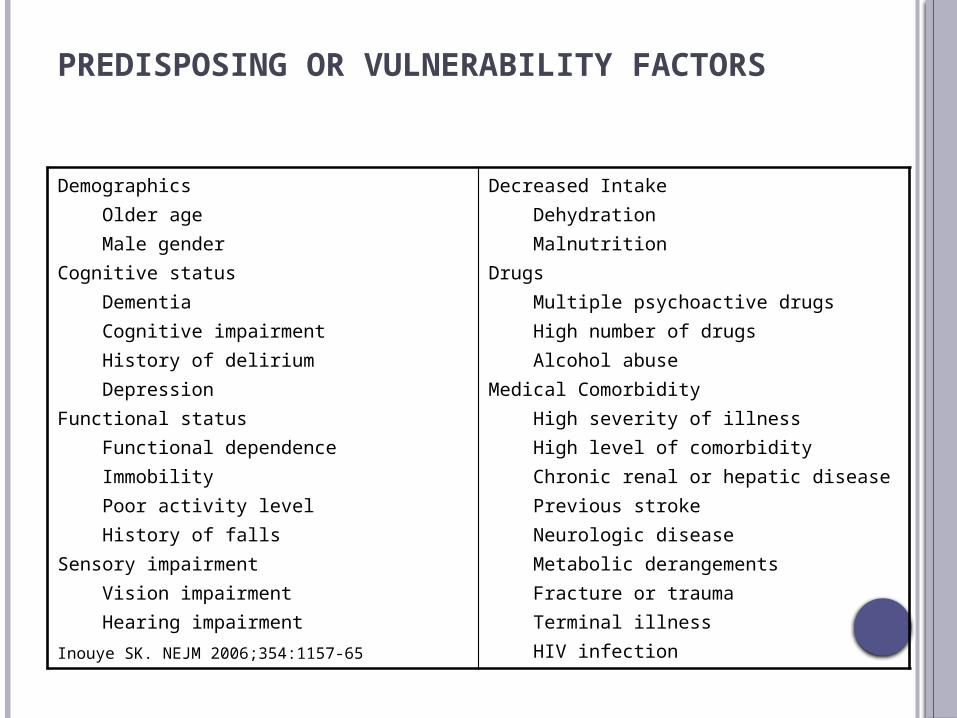
PREDISPOSING OR VULNERABILITY FACTORS
Demographics Older age Male genderCognitive status Dementia Cognitive impairment History of delirium DepressionFunctional status Functional dependence Immobility Poor activity level History of fallsSensory impairment Vision impairment Hearing impairment
Decreased Intake Dehydration MalnutritionDrugs Multiple psychoactive drugs High number of drugs Alcohol abuseMedical Comorbidity High severity of illness High level of comorbidity Chronic renal or hepatic disease Previous stroke Neurologic disease Metabolic derangements Fracture or trauma Terminal illness HIV infection
Inouye SK. NEJM 2006;354:1157-65

PRECIPITATING FACTORS OR INSULTS
Drugs Sedative hypnotics Narcotics Anticholinergic drugs Polypharmacy Alcohol or drug withdrawalPrimary neurological diseases Stroke, particularly nondominant hemispheric Intracranial bleed Meningitis/encephalitisEnvironmental Intensive care unit admission
Physical restraint useBladder catheter useHigh number of proceduresPainEmotional stress
Prolonged sleep deprivation
Intercurrent illnesses Infections Iatrogenic complications Severe acute illness Hypoxia Shock Fever/hypothermia Anemia Dehydration Poor nutritional status Low serum albumin Metabolic derangements (e.g., electrolytes, glucose, acid-base)Surgery Orthopedic surgery
Cardiac surgeryDuration of cardiopulmonary bypassNon-cardiac surgery
Inouye SK. NEJM 2006;354:1157-65
URGENT RECOGNITION: Wernicke’s Hypoxia Hypoglycemia Hypertensive encephalopathy Intracerebral hemorrhage Meningitis/encephalitis Poisoning/medications

ETIOLOGIES -“ I WATCH DEATH “
• I = Infection
• W = Withdrawal• A = Acute Metabolic• T = Trauma• C = CNS Pathology• H = Hypoxia
• D = Deficiencies (especially vitamin)
• E = Endocrinopathies• A = Acute Vascular• T = Toxins• H = Heavy metals
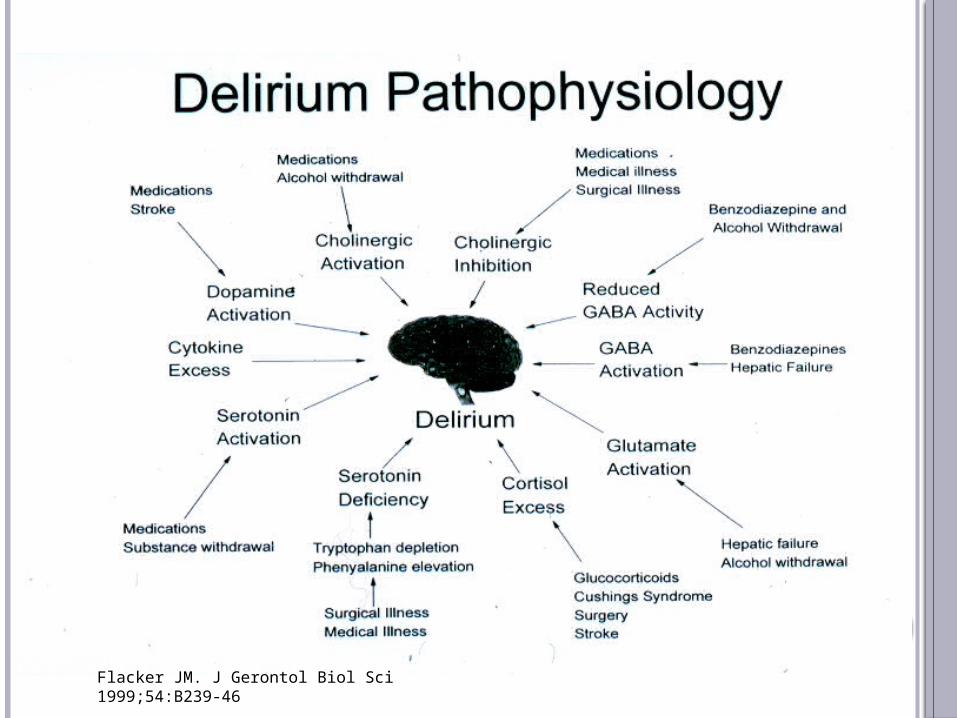
Flacker JM. J Gerontol Biol Sci 1999;54:B239-46

DIFFERENTIAL DIAGNOSIS IN PSYCHIATRY

DIFF DELIRIUM & PSYCHIATRIC DISORDER
• Clouded consciousness or decreased level of alertness
• Disorientation
• Acuity of onset and course- serial mental status exams can help demonstrate this
• Age >40 without prior psych history
• Presence of risk factors for delirium, recent medical illness or treatment
DELIRIUM V/S SCHIZOPHRENIA
• Onset of schizophrenia is rarely after 50.
• Auditory hallucinations are much more common than visual hallucinations
• Memory is grossly intact and disorientation is rare
• Speech is not dysarthric
• No wide fluctuations over the course of a day
• Thought content and abnormal perceptions are related
• In delirium, thought and perception are influenced by immediate environment
MOOD DISORDER V/S DELIRIUM
• Mood disorders manifest persistent rather than labile mood with more gradual onset
• In mania the patient can be very agitated however cognitive performance is not usually as impaired
• Flight of ideas usually have some thread of coherence unlike simple distractibility
• Disorientation is unusual in mania

DELIRIUM V/S DEMENTIA
Delirium Dementia
Impaired memory +++ +++
Impaired thinking +++ +++
Clouding of consciousness +++ -
Major attention deficit +++ +
Fluctuation of course/day +++ +
Disorientation +++ ++
Vivid perceptual dbn ++ +
Incoherent speech ++ +
Disrupt sleep/wake cycle ++ +
Nocturnal exacerbation ++ +
Acute/subacute onset ++ -
Impaired judgement ++ +++

DELIRIUM IS PREVENTABLE
PREVENTING DELIRIUM
• Yale delirium prevention trial
• Designed to counteract iatrogenic influences leading to delirium in the hospital
• Multicomponent intervention strategy targeted at 6 delirium risk factors
SIGNIFICANCE OF DELIRIUM PREVENTION TRIAL
• First demonstration of delirium as a preventable medical condition
• Targeted multicomponent strategy works• Significant reduction in risk of delirium and total
delirium days, without significant effect on delirium severity or recurrence
• Primary prevention of delirium likely to be most effective treatment strategy
• Effectiveness and cost-effectiveness of the program has been demonstrated in multiple studies
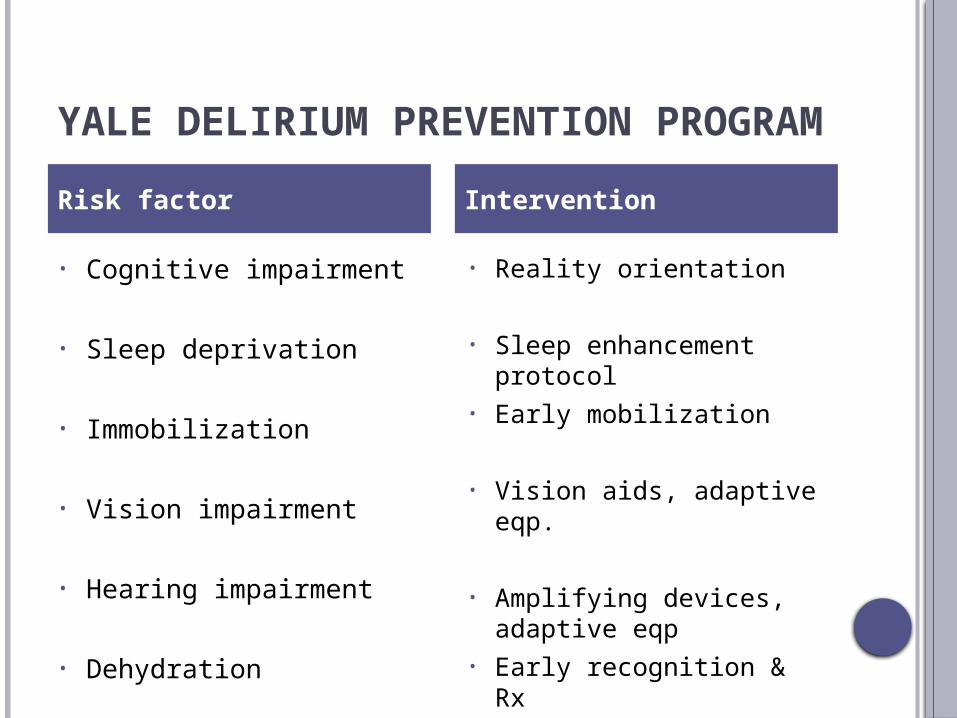
YALE DELIRIUM PREVENTION PROGRAM
• Cognitive impairment
• Sleep deprivation
• Immobilization
• Vision impairment
• Hearing impairment
• Dehydration
• Reality orientation
• Sleep enhancement protocol
• Early mobilization
• Vision aids, adaptive eqp.
• Amplifying devices, adaptive eqp
• Early recognition & Rx
Risk factor Intervention
DIAGNOSIS AND ASSESSMENT

DIAGNOSIS AND ASSESSMENT
• Delirium is a clinical diagnosis
• History and physical examination
• Mental Status Exam
• Rating Scales-consider on admission

ASSESSMENT INSTRUMENTS
To identify delirium:• Delirium rating scale – revised 98 ( DRS – R98)• Confusion assessment method (CAM)• Delirium symptom interview (DSI)• Confusion assessment method for ICU (CAM-ICU)• Intensive care delirium screening checklist (ICDSC)
To assess symptom severity:• Delirium detection scale (DDS)• Memorial delirium assessment scale (MDAS)
To test neuropsychological function:• Cognitive test for delirium (CTD)
DIAGNOSIS AND ASSESSMENT
Lab tests cannot diagnose delirium but may support dx CBC, CMP, UA, urine tox, TSH, B12, ammonia CXR, EKG, LP if indicated Neuroimaging
EEG Generalized slowing in delirium, nonspecific Triphasic waves in hepatic encephalopathy Low voltage fast activity in EtOH or BZD w/d

TREATMENT
TREATING PATIENTS WITH DELIRIUM
Treat underlying causes Don’t stop looking after finding one potential
cause
• Anticipate in high risk states
• Diagnosis & treatment should occur concurrently
• Regular evaluation of progress is important
• Best managed in hospital setting
TREATING PATIENTS WITH DELIRIUM
• Supportive and environmental measures - support and orientation
- unambiguous environment
- maintaining competence
• Drug treatment - antipsychotics
- benzodiazepines
- emerging therapies
• Managing patients after discharge
PROVIDING SUPPORT AND ORIENTATION Communicate clearly and concisely; give repeated
verbal reminders of the day, time, location, and identity of key individuals, such as members of the treatment team and relatives
Provide clear signposts to patient's location including a clock, calendar, chart with the day's schedule
Have familiar objects consistency in staff Use television or radio for relaxation and to help the
patient maintain contact with the outside world Involve family and caregivers to encourage feelings of
security and orientation

PROVIDING AN UNAMBIGUOUS ENVIRONMENT
Simplify care area by removing unnecessary objects; allow adequate space
between beds Consider using single rooms to aid rest and avoid
extremes of sensory experience Avoid using medical jargon in patient's presence
because it may encourage paranoia Ensure that lighting is adequate; provide a 40 60 W
night light to reduce misperceptions Control sources of excess noise (such as staff,
equipment, visitors); aim for < 45 decibels in the day and < 20 decibels at night
Keep room temperature between 21.1°C to 23.8°C
MAINTAINING COMPETENCE Identify and correct sensory impairments
Encourage self care and participation in treatment
Treatments to allow maximum periods of uninterrupted sleep
Maintain activity levels:
-ambulatory patients should walk three times each day;
-non ambulatory patients should undergo a full range of movements for 15 minutes three times each day

DRUG TREATMENT
• Benefits v/s adverse effects
• Use of psychotropic drugs: - complicates ongoing assesment of MSE
- impair patient’s ability to understand or co-operate
- greater incidence of falls
• Prescribing often influenced by: - pressure from relatives
- time constraints
-diff in coomunication between medical & nursing staff

ANTIPSYCHOTICS
• Hyperactive and hypoactive delirium
• Improve cognition
• Rapid onset
• Improvement evident in hours or days
• Superior to benzodiazepines

ANTIPSYCHOTICS
• Chlorpromazine , Haloperidol, Droperidol – similar efficacy
• Atypicals – further research needed
• Haloperidol is preferred:
- fewer active metabolites
- limited anticholinergic side effects
- less sedative & hypotensive effects
- administered by different routes
- EPS *reported incidence is low
*iv administration – EPS less likely

BENZODIAZEPINES
• Can protect or pose risk
• Delirium associated with seizure, withdrawal from alcohol or sedatives
• Adjunct if antipsychotics are not tolerated
• Lorazepam is preferred
- rapid onset
- short duration of action
- low risk of accumulation
- no major active metabolites
- predictable bioavailability if given i.m.
EMERGING THERAPIES
• Physostigmine – anticholinergic delirium
(hypoxia, hypoglycaemia, drug related, trauma)
• Nicotine replacement treatment – protective?
• Pimozide –potent calcium antagonist
- delirium ass with hypercalcemia
• Trazadone & Mianserin ( 5HT 2 antagonist)
• Light therapy

OUTCOME OF DELIRIUM
40%
25%
35%
Recovery Permanent Cognitive Impairment Mortality
MANAGING AFTER DISCHARGE• Many patients dicharged before full resolution
• Delirium may persists for weeks or even months
• Risk of new diagnosis of dementia increased at least threefold
• Problems in attention may persist
• Prevent further episodes
- address risk factors
- correct sensory impairments
• Look for psychological sequalae
- depression
- PTSD
• Follow up - must
THANK YOU
“Knowing is not enough;we must apply.
Willing is not enough;we must do.”
- Goethe