Delhi Scenario of HIV/AIDS Dr. A. K. Gupta MD (Pediatrics) Additional Project Director Delhi State...
39
Delhi Scenario of HIV/AIDS Dr. A. K. Gupta MD (Pediatrics) Additional Project Director Delhi State AIDS Control Society
-
Upload
jasmin-flynn -
Category
Documents
-
view
218 -
download
2
Transcript of Delhi Scenario of HIV/AIDS Dr. A. K. Gupta MD (Pediatrics) Additional Project Director Delhi State...

Delhi Scenario of HIV/AIDS
Dr. A. K. Gupta MD (Pediatrics)Additional Project Director
Delhi State AIDS Control Society

• Total population - 18 million, First case- 1988• Estimated PLHAs (2011)- 36,000 • Low prevalence state (Prevalence in Gen. population- 0.2%)• Highly vulnerable state- (Migrant labour- 0.88 million, Truckers stationed/day-35000)• Total high risk population ->1.00 Lakh • HIV +VE Regd. In HIV Care At ART Centers : 36452• Eligible patients actually started on ART- 17997• No. Currently Alive & on ART- 10822• LFU (7%), Died (8%) or Transferred out to other states(21%)
DELHI SCENARIO (March 2012)
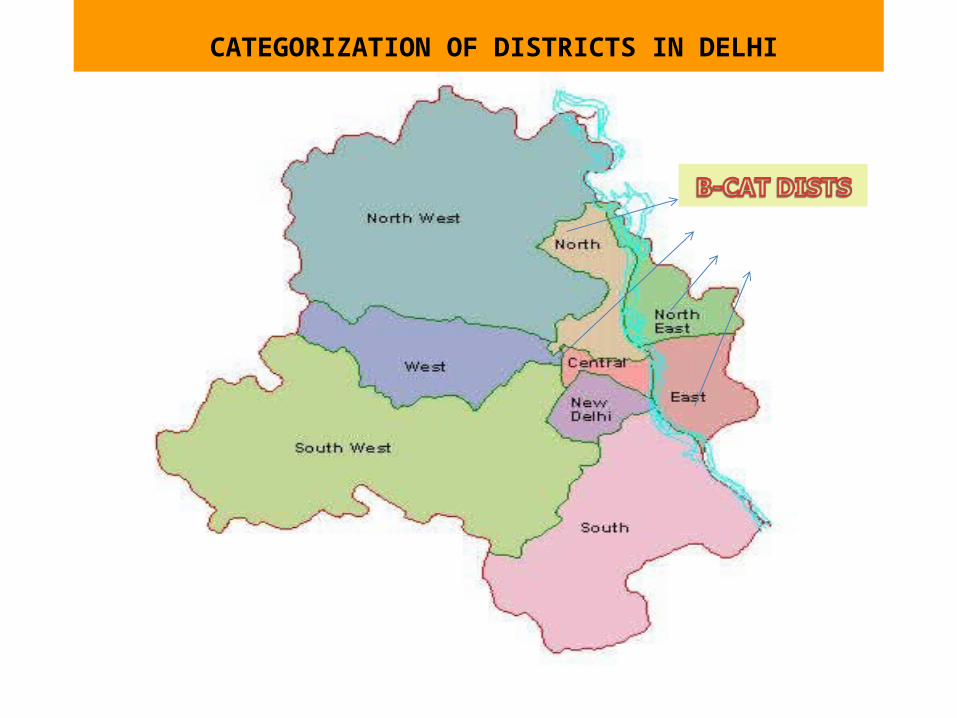
CATEGORIZATION OF DISTRICTS IN DELHI
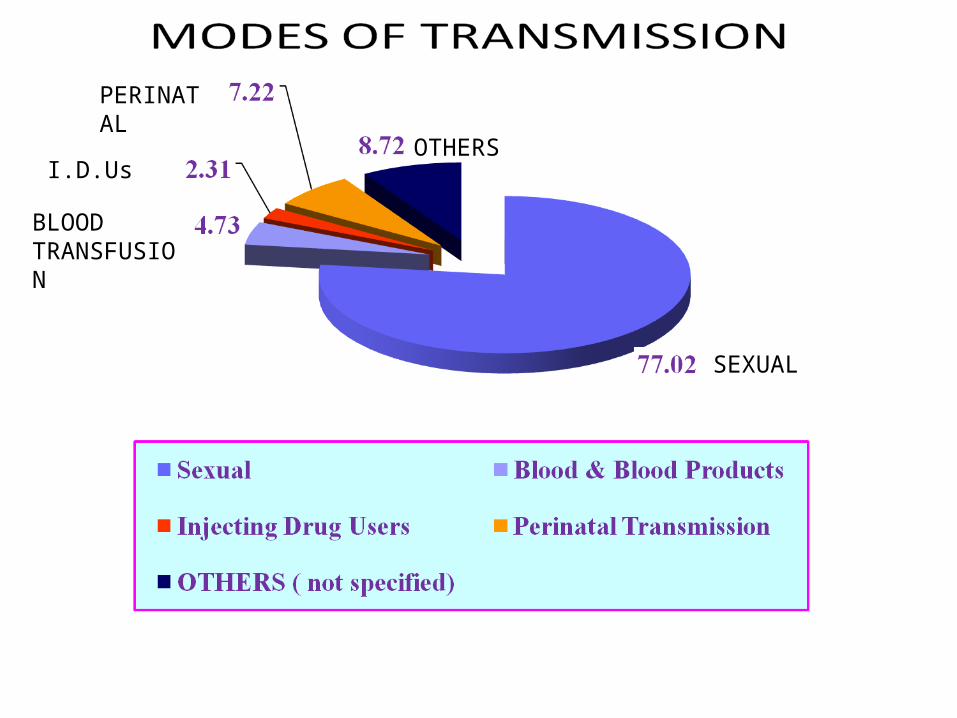
OTHERS
PERINATAL
I.D.Us
BLOOD TRANSFUSION
SEXUAL

HIV Trend Among Ante Natal Cases, Delhi
2004 2005 2006 2007 20080
0.05
0.1
0.15
0.2
0.25
0.3
0.350.31000000
00000010.31000000
0000001
0.1
0.2 0.2
ANC
ANC
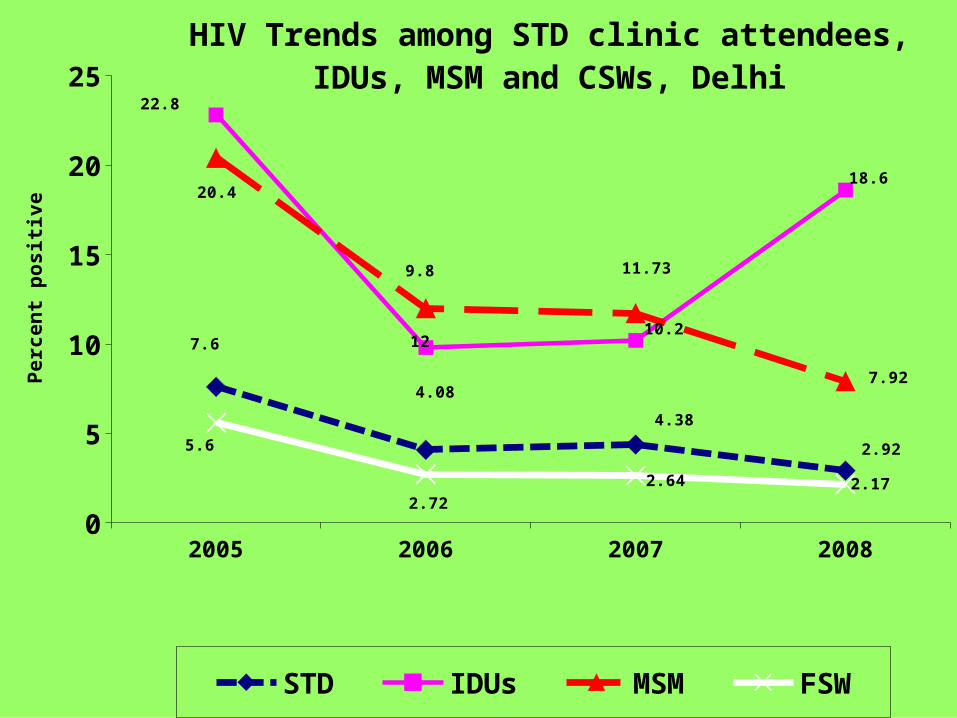
2005 2006 2007 20080
5
10
15
20
25
7.6
4.08
4.38
2.92
22.8
9.8
10.2
18.620.4
12
11.73
7.92
5.6
2.72
2.64 2.17
HIV Trends among STD clinic attendees, IDUs, MSM and CSWs, Delhi
STD IDUs MSM FSW
Per
cen
t p
osi
tiv
e
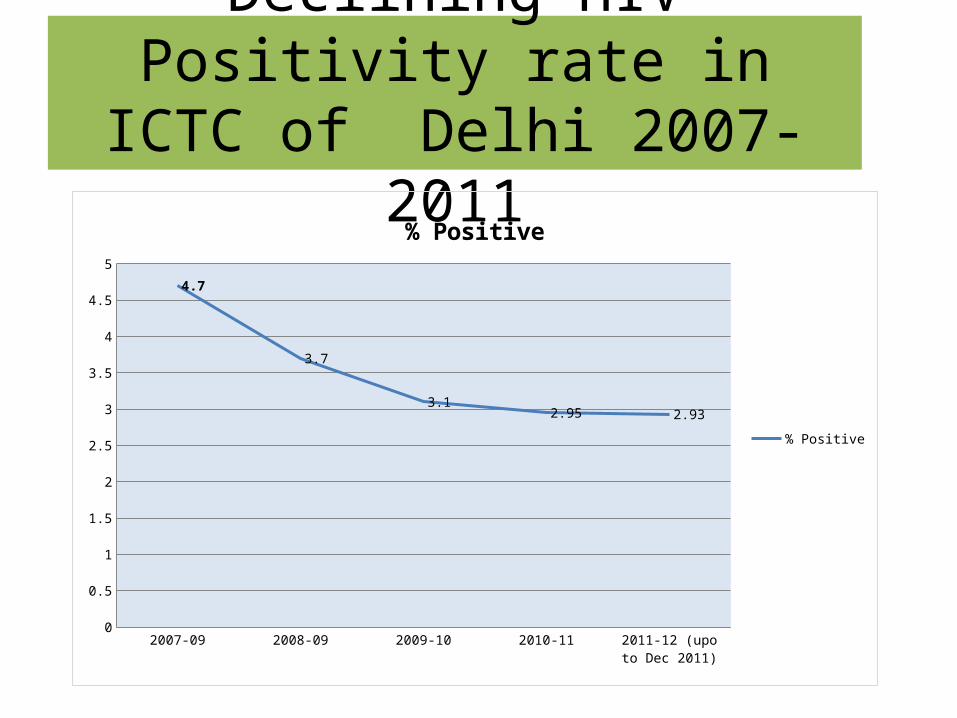
Declining HIV Positivity rate in ICTC of Delhi 2007-2011
2007-09 2008-09 2009-10 2010-11 2011-12 (upo to Dec 2011)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
4.7
3.7
3.12.95 2.93
% Positive
% Positive

Goal: To halt and reverse the epidemic in India over the next five years
Objectives:– Prevent new infections by saturating coverage of HRG
through TI and scaled up interventions in the general population.
– Provide greater care, support and treatment to larger numbers of PLHIV
– Strengthen the infrastructure, systems and human resources in prevention, care, support and treatment programme at district, state and national levels
– Strengthen the nationwide SIMS
NACP-III (2007-12) : Goal & Objectives

•Targeted interventions
•STI care
• Condom promotion
•Enabling environment
•Blood safety
•Integrated Counselling and testing including PPTCT
•STI Care
•IEC and social mobilisation
•Mainstreaming
•ART
•HIV-TB Co-ordination
•Treatment of Opportunistic Infections
•Community Care Centres
•Post-Exposure Prophylaxis
•HIV Sentinel Surveillance
•Behavioural Surveillance
•Monitoring and evaluation
•Operational research
• DAPCU
• Technical Resource Groups
•Enhanced HR at NACO, SACS and districts
•Enhanced training activities
Prevention
High risk populations
Low risk populations
Care & support
Monitoring and
Evaluation
Institutional Strengthening
Care, Support &
Treatment
Strategic Information
Management
Capacity Building


Status Of Targeted Intervention (TI) Projects 2011-12Sub Type (Registered)
No. of TIs
Target No. screened for Syphilis
No. found RPR reactive
No. tested at ICTC
No. detected HIV +ve (%)
No. linked to HIV care (%)
FSW (30982)
40 44350 15682 93 22286 97(0.43) 59 (60.8)
MSM+TG (15624)
17+2 18650 7436 40 8477 116(1.4) 82 (70.7)
IDUs (10124)
19 9600 3498 58 4245 125(2.9) 62(49.6)
Truckers (11602)
4 50000 0 0 930 15(1.6) 11(73.3)
Migrants (43200)
8
80000 0 0 1019 33(3.2) 19(57.6)
Total (111532)
90 202600 26616 191 (0.7%)
36957 386(1.0%)
233 (60.3%)

Integrated Counseling & Testing (I.C.T.C) (93 centres)S. No NEW PHYSICAL TARGETS TARGET(April-
DC 11)Achievement (April- DEC 11)
1 TESTING OF GENERAL PATIENT (ICTC) – annual target 3,00,000
250000 228550(91.5%)
2 No. OF GEN CLIENTS DETECTED HIV +VE 7344(3.21%)
3 TESTING OF ANC (PPTCT)- annual target 2,50.000
225000 204241 (91%)
4 No. OF ANC CLIENTS DETECTED HIV +VE- annual estimate 500 cases
356
5 No. ANC delivered and Mother Baby pair given NVP prophylaxis
356 224 (62.9 %)
6 HIV-TB CROSS REFERRALS- annual target 37000
40000 39038
7 No. OF PEOPLE WITH HIV-TB CO-INFECTION- annual estimate 1000 cases
1000 614
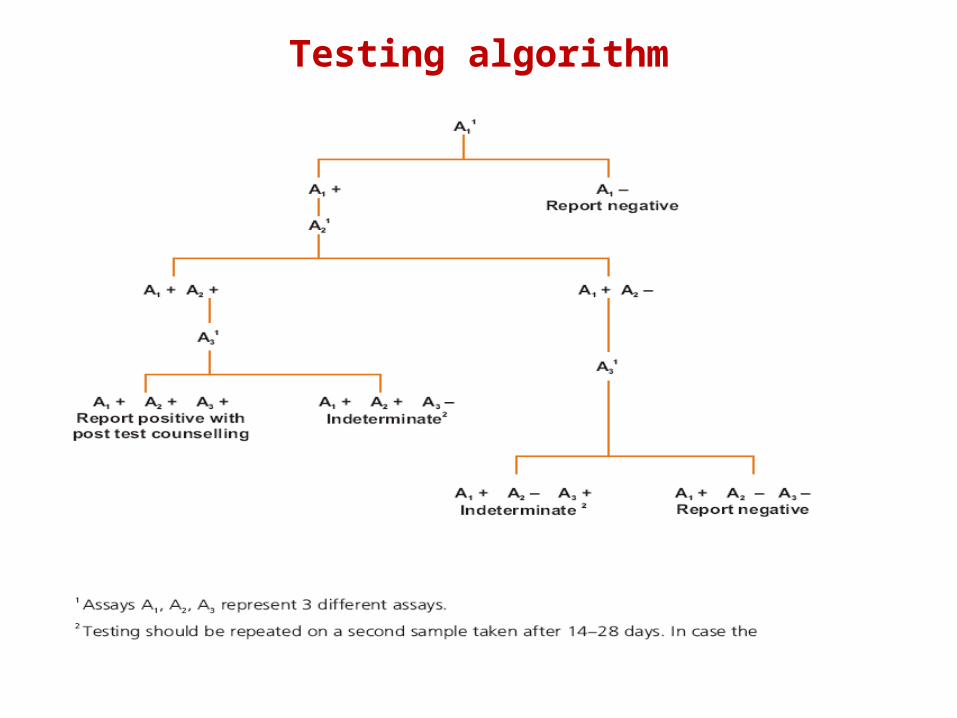
Testing algorithm

Rationale For PPTCT Services in Delhi
• Annual pregnancies - 2.5 lakh
• HIV infected pregnancies - 500
35% Transmission rate *
• Infected newborns - 175
*Risk of transmission without PMTCT intervention (WHO 2010)

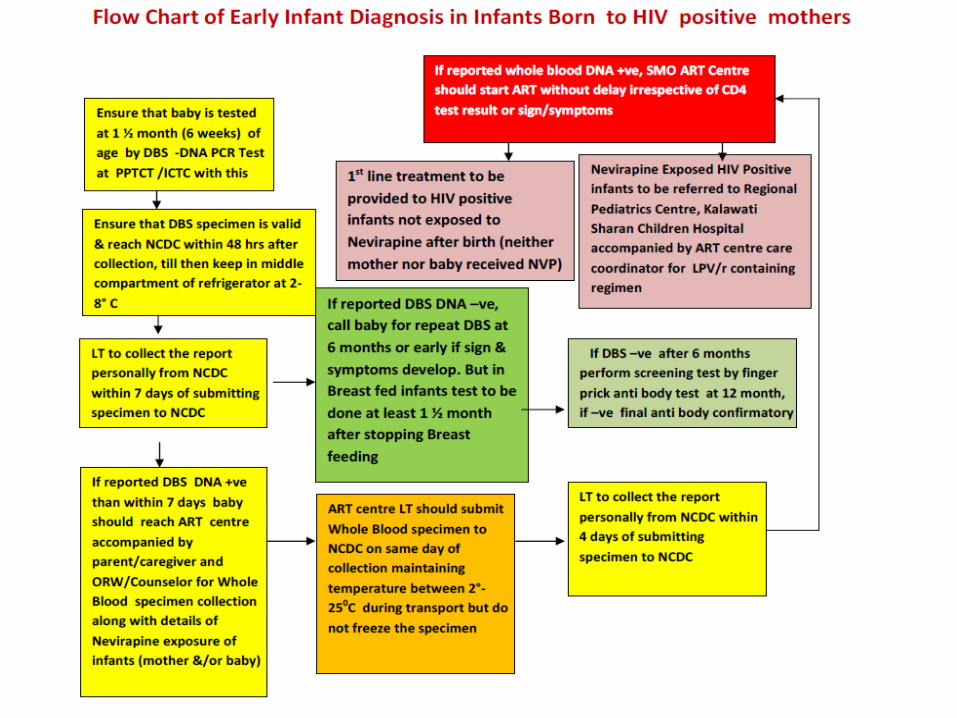
Early Infant Diagnosis• Launched in Dec 2010•EID Test Lab for DNA-PCR testing-1 (NCDC, New Delhi)• EID sample collection sites- 19 ICTCs• Whole Blood Collection for DNA-PCR sites (ART centers)- 7

Procedure for heel prick1. Warm the area2. Wash hands, put on gloves3. Position baby with foot down4. Clean area, dry 30 sec5. Press lancet into foot, prick skin6. Wipe away first drop7. Allow large drop to collect8. Touch blood drop to card9. Fill entire circle with drop10. Fill at least 3 circles11. Clean foot, no bandage
<5kg infants
5-10kg infants
Overhead 4-5

Valid DBS specimen
Overhead 4-34

Status of PMTCT ARV Prophylaxis in 234 MB pair (Feb 11-Jan12)Category (Number) HIV Positive
infant MTCT rate (%)Category I- MB pair received ARV Prophylaxis (n=161)
9 5.6
Category IA Maternal HAART (CD4≤350) in pregnancy & Baby received SdNVP (n=42)
0 0
Category IB- MB pair short course AZT+3TC to mother & AZT to baby (n=19)
0 0
Category IC- MB pair Sd NVP (n=100) 9 9
Category II- Only Mother received ARV prophylaxis (n-9)
1 11.1
Category III- Only baby received ARV prophylaxis (n=26)
3 11.5
Category IV- No. ARV prophylaxis (n=38) 11 28.9
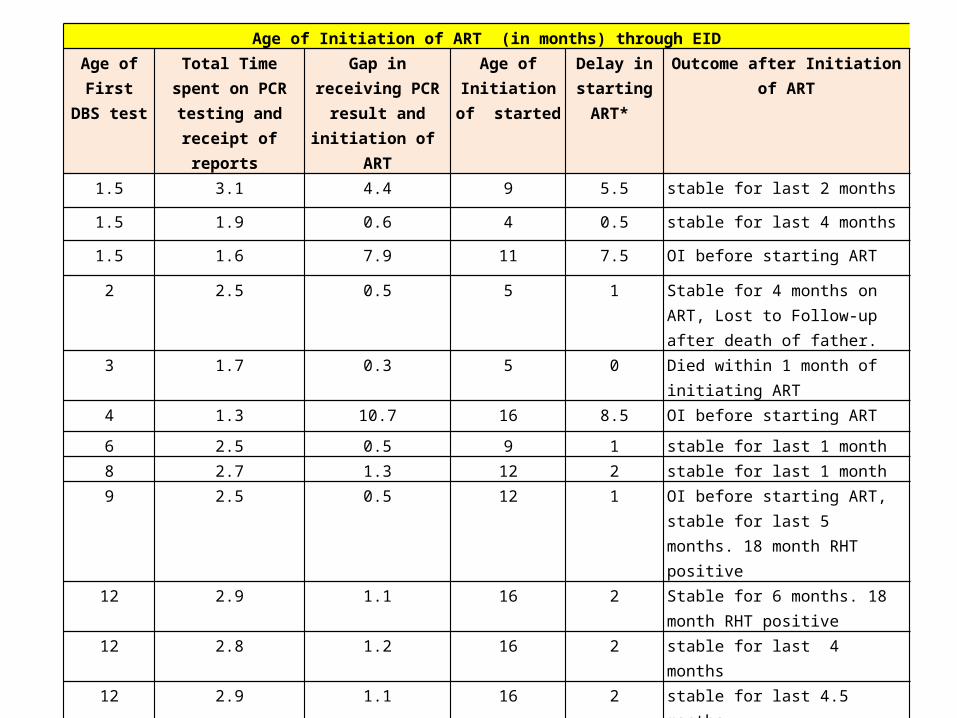
Age of Initiation of ART (in months) through EIDAge of First DBS test
Total Time spent on PCR testing and
receipt of reports
Gap in receiving PCR result and initiation
of ART
Age of Initiation of started
Delay in starting ART*
Outcome after Initiation of ART
1.5 3.1 4.4 9 5.5 stable for last 2 months
1.5 1.9 0.6 4 0.5 stable for last 4 months
1.5 1.6 7.9 11 7.5 OI before starting ART
2 2.5 0.5 5 1 Stable for 4 months on ART, Lost to Follow-up after death of father.
3 1.7 0.3 5 0 Died within 1 month of initiating ART
4 1.3 10.7 16 8.5 OI before starting ART
6 2.5 0.5 9 1 stable for last 1 month
8 2.7 1.3 12 2 stable for last 1 month 9 2.5 0.5 12 1 OI before starting ART, stable for last
5 months. 18 month RHT positive
12 2.9 1.1 16 2 Stable for 6 months. 18 month RHT positive
12 2.8 1.2 16 2 stable for last 4 months
12 2.9 1.1 16 2 stable for last 4.5 months
15 2.4 0.1 17.5 0.5 OI before starting ART, stable for last 6 months. 18 month RHT positive
15 2.4 0.1 17.5 0.5 OI before starting ART, stable for last 5 months. 18 month RHT positive
15 1.7 0.8 17.5 0.5 OI before starting ART, stable for last 2 months. 18 month RHT positive

TB-HIV Collaborative Activities

TB and HIV in India
• Highest TB burden in the world– 1.8 million TB cases per year
• 3rd highest HIV burden– 2.3 million PLHA (2007)– Prevalence 0.34% (adult population)
• Estimated HIV-TB co-infected: 55,000-65,000

Risk of TB in HIV Patients
HIV patients are at an increased risk of:• Acquiring latent TB• Developing active TB once infected with M.
tuberculosis• Becoming re-infected with a second strain of TB• Relapsing after stopping treatment
10%
60%
0%10%20%30%40%50%60%70%
PPD+/HIV-negative PPD+/HIV+
Source: NACO
Lifetime Risk of TB
Revised guidelines for starting ART for HIV TB co-infected patients
• All HIV infected TB patients need to be started on ART – with CD4 count <350 (in case of pulmonary TB)
and – irrespective of CD4 count in case of
extrapulmonary TB – within 2 weeks of starting ATT
• NACO, November 2008


Anti Retroviral Treatment

Goals of ART 1. Clinical goal
To prolong life & improve quality of life
2. Virological goal
Greatest possible reduction in viral load for as long as possible to halt disease progression and to prevent or delay resistance
3. Immunological goal
Immune reconstitution - CD4 within normal range

WHEN TO START? - Initiation of ART in Adults and Adolescents
National GuidelineRevised National Guideline (April 2009)
WHOClinical Staging
CD4 (cells/cu.mm)
I and II Treat if CD4 Count < 350
IIITreat irrespective of CD4 Count
IV
National ART regimen
• First-line ART:• First-line ART is the initial regimen prescribed for an ART naïve patient when the
patient fulfils national clinical and laboratory criteria to start ART. (Current NACO treatment guidelines for first-line ART recommends two classes of
drugs for initial treatment ie 2 NRTI + 1 NNRTI.)Zidovudine / Lamivudine / Nevirapine
Or Stavudine / Lamivudine / Nevirapine
( Efavirenz in place of Nevarapine if coinfected with TB or side effects with NVP,
Tenofovir for special situations only)
Initiating ART: Patient Education
• It is not curative, but prolongs life• Treatment is lifelong, expensive• High level of adherence is critical (>95%)• Short and long term adverse events• Drug interactions• Safer sex still essential• Do not share drugs with friends , family members
Start ART when patient is ready

SUCCESSFUL HIV THERAPY REQUIRES RIGOROUS ADHERENCE
• >95% adherence necessary to achieve viral load <400 copies/mL in 81% of HIV patients
• A 10% reduction in adherence was associated with a doubling of HIV RNA level
• 80% adherence may be sufficient to achieve therapeutic goals in other chronic disease states (e.g., hypertension)

Mar-05 Mar-06 Mar-07 Mar-08 Mar-09 march.-10 march.-11 Mar-05 Mar-06 Mar-07 Mar-08 Mar-09 march.-10 march.-11
Ever Reg-is-tered
NaN NaN 194607 428056 686913 933540 1253498
No. of pa-tient on 1st line
6845 37368 69016 140654 223223 315640 404882
No. of ART cen-tre
25 54 107 147 211 269 300
100000
300000
500000
700000
900000
1100000
1300000
25
75
125
175
225
275
325
Ever Registered No. of patient on 1st line No. of ART centre

Mar-05 Mar-06 Mar-07 Mar-08 Mar-09 Mar-10 Mar-11 Mar-05 Mar-06 Mar-07 Mar-08 Mar-09 Mar-10 Mar-11
Ever Reg-is-tered
NaN NaN 22462 32900 48721 64661 84987
No. of pa-tient
269 2335 6365 9495 14303 19203 23854
No. of ART cen-tre
25 54 107 147 211 269 300
5000
15000
25000
35000
45000
55000
65000
75000
85000
25
75
125
175
225
275
325
ART SCALE UP IN INDIA (CLHA)
Ever Registered No. of patient No. of ART centre

Cumulative Treatment Outcome
Cumulative Outcome of PLHAs on ART, India
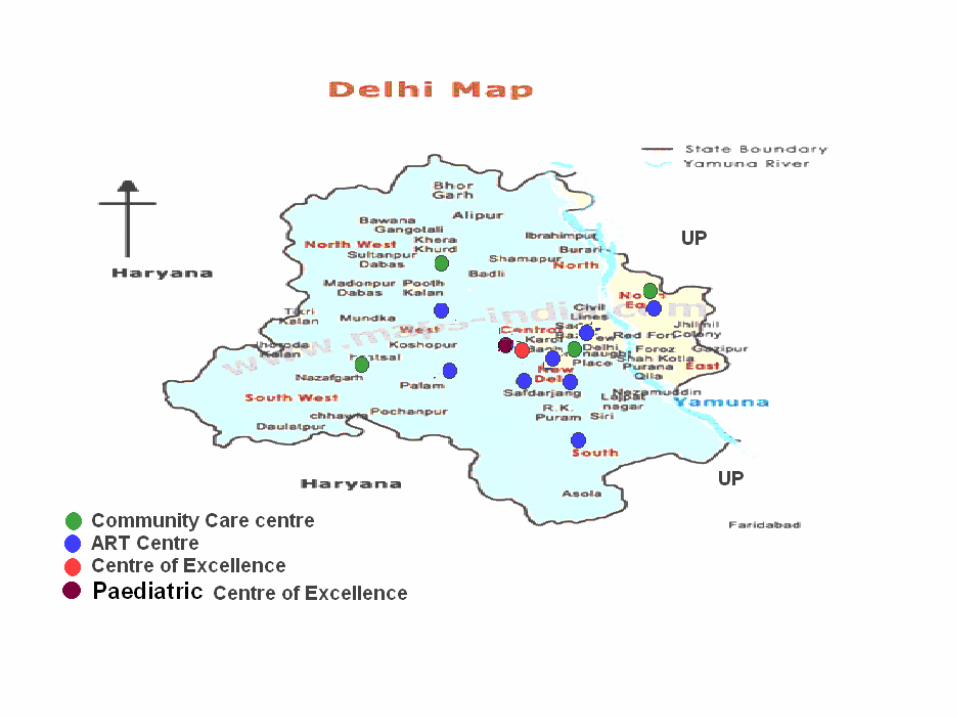

ALL 9 ART CENTRES of Delhi SINCE BEGINNING (2004) TO DECEMBER 2011
S. NO INDICATOR CUMULATIVE
1 REGISTRATION 36452
2 EVER STARTED ON ART 17997
3 ALIVE ON ART 10822
4 DEATH 2000
5 TRANSFERRED OUT 2240
6 STOPPED TREATMENT 135
7 LOST TO FOLLOW UP 2340
8 MISS 453

Special Achievements of DSACS under NACP III
•Financial Assistance to Poor PLHAs and Orphan children by Delhi Govt •Free Investigations including CT Scan, MRI, blood and other tests of PLHAs in HIV care at ART centers of Delhi•Free Blood / Blood products for PLHAs without processing fees and without replacement donations•Launch of First Post Exposure Prophylaxis toll free interactive voice response helpline in the country (dial 1097 and select option 6) for prevention of HIV, HBV & HCV in Health care Workers during occupational exposure. •Setting up of First Youth Friendly health Centre in Delhi in collaboration with DSHM/NRHM at Jamia Milia Islamia in August 2010.•Mapping of massage parlors for the first time in the country- in New Delhi, Central, North, North- West and South Delhi districts with aim to assess the Knowledge, Behavior, Attitude and practices of the workers, clients and owners of 1050 massage parlours and categorize them by assessment of vulnerability. 18% massage parlours observed to be having risky behavior activities. •Training of NRHM Grass-root level functionaries –ASHAs, ANMs etc