Adverse Vascular Risk is Related to Cognitive Decline in Older
Upload
erste-stiftungCategory
view
212download
1description

ERSTE FoundationFellowship for Social Research
Labour Market and Employment in Central and Eastern Europe
2013–2014
Decline in Physical Health of Older Workers and Retirees Predicted by Negative Psychosocial Working Conditions on the JobLucie KalousovaCarlos Mendes de Leon

1
Decline in Physical Health of Older Workers and Retirees Predicted by Negative Psychosocial Working Conditions on the Job
By Lucie Kalousova & Carlos Mendes de Leon University of Michigan ACKNOWLEDGMENTS This research project was developed within the ERSTE Foundation Fellowship for Social Research 2013. It benefited from the feedback provided by Sarah A. Burgard, Katherine Y. Lin and the European University Institute Inequality Working Group. This paper uses data from SHARE wave 4 release 1.1.1, as of March 28th 2013(DOI: 10.6103/SHARE.w4.111) or SHARE wave 1 and 2 release 2.6.0, as of November 29 2013 (DOI: 10.6103/SHARE.w1.260 and 10.6103/SHARE.w2.260) or SHARELIFE release 1, as of November 24th 2010 (DOI: 10.6103/SHARE.w3.100). The SHARE data collection has been primarily funded by the European Commission through the 5th Framework Programme (project QLK6-CT-2001-00360 in the thematic programme Quality of Life), through the 6th Framework Programme (projects SHARE-I3, RII-CT-2006-062193, COMPARE, CIT5- CT-2005-028857, and SHARELIFE, CIT4-CT-2006-028812) and through the 7th Framework Programme (SHARE-PREP, N° 211909, SHARE-LEAP, N° 227822 and SHARE M4, N° 261982). Additional funding from the U.S. National Institute on Aging (U01 AG09740-13S2, P01 AG005842, P01 AG08291, P30 AG12815, R21 AG025169, Y1-AG-4553-01, IAG BSR06-11 and OGHA 04-064) and the German Ministry of Education and Research as well as from various national sources is gratefully acknowledged (see www.share-project.org for a full list of funding institutions).

2
ABSTRACT Well-established evidence has shown that negative psychosocial working conditions adversely affect the health and well-being of workers. Yet little is known about their consequences on the health of older workers. Our article examines the associations between declines in physical health in later life, measured as frailty, and negative psychosocial working conditions. We use longitudinal cross-national data collected by SHARE I and SHARE IV and focus on respondents who were working at baseline. We find that low reward, high effort, effort to reward ratio, and effort to control ratio were all predictors of an increase in frailty. The association between low reward and change in frailty was modified by retirement status at follow-up, with nonretired respondents in low-reward jobs experiencing the largest increases in frailty at follow-up. These results suggest that the effect of psychosocial working conditions on physical health may extend well past the prime working age, and retirement may have a protective effect on the health of older workers in low reward jobs.

3
INTRODUCTION Retirees are a rapidly growing segment of the European population. Demographers project that by 2020 nearly 20% of all EU citizens will be 65 years old or older (European Commission, 2009). In response to these projections, European countries have gone to great lengths to prepare their healthcare systems and social services to serve this population and maintain the population’s health and well-being (Rechel et al., 2013). However, the success with which this population will age has already been to some extent determined by exposures in the earlier stages of life, as health is subject to cumulative processes over the course of life, a fact that has been well documented (Barker, 1998; Hamer et al., 2012; Johnson et al., 2012). We argue that a key set of exposures related to health in older age, which has been largely overlooked are psychosocial working conditions. It is especially important to advance our understanding of the connections between working conditions and health in later life because most of today’s older adults held a job for at least part of their lives and many for their entirety. A well-established body of literature has shown that psychosocial characteristics of our jobs have important consequences for health while in the labor force. For example, poor psychosocial working conditions have been associated with occupational injuries (Gillen et al., 2007) and absenteeism (Melchior et al., 2003). Other research suggests that poor psychosocial working conditions may pose an especially high risk for our cardiovascular systems, as evidenced by an elevated risk of developing coronary heart disease (Bosma et al., 1998). Workers, who face poor psychosocial working conditions, are also more likely to express their intention to leave the labor force early (Siegrist et al., 2006; Wahrendorf et al., 2012a). Most recently, scholars of working conditions have joined forces with gerontologists to begin conceptualizing psychosocial working conditions as an exposure with potential late-life effects. For example, Wahrendorf and colleagues found that, in a sample of former predominantly white-collar French employees, those who experienced less favorable working conditions reported worse physical and mental health after retirement (Wahrendorf et al., 2012b).
In this study, we expand on the emergent line of research by asking two research questions. First, we ask, are poor psychosocial working conditions associated with a greater rate of decline in physical health in later life? And second, does retirement buffer the effects of negative working conditions on health in later life? We examine these questions in a representative sample of older European workers and recent retirees. We also contribute to the literature on health in later life by constructing a multidimensional indicators of health, frailty, a marker for poor physical health in older age. We employ a robust analytical strategy that takes advantage of the longitudinal health data collected by two waves of Survey of Health, Ageing and Retirement in Europe, SHARE I and SHARE IV.

4
BACKGROUND A commission jointly assembled by the International Labor Office and the World Health Organization (ILO & WHO Committee on Occupational Health) defined psychosocial factors in the workplace as “interactions among job content, work organization and management, and other environmental and organizational conditions, on the one hand, and employees’ competencies and needs on the other (1986).” Research on poor psychosocial working conditions and health has found consistent associations between exposure and adverse health outcomes. Some of the strongest findings in this area pertain to the relationship among heart disease, negative health behaviors, and poor psychosocial working conditions (for detailed overviews see Kivimäki et al., 2006; Siegrist & Rödel, 2006). Although the exact mechanisms that led to these associations have been notoriously difficult to specify in nonexperimental settings, they are thought to be related to the adverse physiological consequences of the stress brought about by the misfit between a person and his/her work environment, including the perceived lack of ability to realize one’s potential in the available opportunity structure (Siegrist, 1996). The two most frequently posited explanatory frameworks of the abovementioned physiological consequences rest on the assumption that damage to the body is a by-product of a coping reaction, be it physiological or behavioral. Researchers have argued that negative psychosocial working conditions generate “active distress,” which is a form of stress arousal that leads to the activation of two bodily systems: the sympathetic-adrenal-medullary system (SAM) and the hypothalamic-pituitary-adrenal system (HPA). Frequent activation of these stress response systems without adequate opportunities for recovery is likely to cause chronic impairments (Geurts & Sonnentag, 2006). The behavioral pathway involves adopting behaviors considered “risky,” such as smoking, excessive alcohol consumption, and eating foods rich in saturated fats and calories. This mechanism has sometimes been labeled as “secondary” or “mediating.” Little consensus exists on how to unambiguously conceptualize or quantify the effects of the secondary pathway on health, as most health behaviors are thought to arise from a complex interplay of personal environmental contexts that are encountered in earlier parts of the life course, rather than from a reaction to a specific and acute stressor (Lamontagne, 2012; Siegrist & Rödel, 2006).
Despite convincing evidence that negative working conditions harm the health of workers, it is yet unclear whether the cessation of work-related stress due to retirement provides a respite from their further negative effects. This is because removing the psychosocial stressor may not necessarily slow down a process of decline already on its way. At the same time, it is plausible that, although retirement is not likely to heal the damage already done, it may provide much needed relief to workers in particularly poor psychosocial working conditions, and their health decline may become less steep after retirement as a result.

5
Frailty as a Health Outcome It is a challenge to provide a uniform definition of overall health status in later life, the period many associate with worsening health. Most common chronic conditions become clinically apparent during this time, and adults develop multiple morbidities that together result in a progressive decline in overall health and function as they age. The concept of successful aging is a widely accepted framework to capture the multiple aspects of declining health commonly observed in older adults. It was developed by Rowe and Kahn, who defined successful aging based on three dimensions: maintenance of high levels of physical and cognitive function; absence of disease and disability; and continued engagement in productive activities (Rowe & Kahn, 1987). This definition provides cohesive framework for distinguishing the effects of illness from the effects of old age on physical health status. Kaplan and others later identified predictors of successful aging, which included level of physical activity, not smoking, and sociability (Kaplan et al., 1987). Adults who display behaviors not associated with successful aging, such as seclusion, tend to have higher counts of morbidities and also a greater chance of death (Strawbridge et al., 1996). However, successful aging is not easy to measure in diverse populations and sometimes falls short of accounting for variability in quality of life (Strawbridge et al., 2002). In this paper, we build on the conceptual framework of successful aging and evaluate health by a calculating an individual’s frailty scores, a health measure we consider best suited to cross-national comparative research, such as ours.
The concept of frailty has been discussed in medical circles for several decades but is more of a newcomer to social scientific research (Ahmed et al., 2007). Frailty has many definitions. The most systematic attempt to establish the “frailty phenotype” was undertaken by Fried and colleagues in 2001. They identified five dimensions of frailty: shrinking, weakness, poor endurance and energy, slowness, and low physical activity level. Older adults placed in lower ranges for multiple indicators were shown to be at “a high-risk state predictive of a range of adverse health outcomes.” Frail older adults are thought to be especially vulnerable to adverse health outcomes because they have greater difficulty to recover from a health challenge, even if it constitutes an otherwise relatively minor medical event (Clegg et al., 2013). Frailty is constructed by taking advantage of biomarkers and self-reported physical-condition data that are relatively free of cultural biases (Romero-Ortuno et al., 2010). As a combined measure of multiple dimensions of physical health, it is not designed to represent a uniform, culturally dependent concept, as is, for instance, self-reported health, which may have multiple meanings and interpretations that become increasingly complex in older age groups (Schnittker, 2005). It is also superior to condition-specific morbidity, which only captures whether a respondent has been diagnosed with a particular disease. Although population-level evaluations of frailty prevalence remain relatively rare, prior studies conducted by medical researchers have linked frailty to a number of adverse health outcomes. These include increased incidence of falls as a result of impaired balance or gait, acute confusion, fluctuating disability, and mortality (Clegg et al., 2013; Fried et al., 2009; Mitnitski et al., 2002; Walston et al., 2006).

6
METHODS
Study Design Our study addresses the following two research questions: First, are negative psychosocial working conditions associated with steeper declines in physical health? Second, does retirement buffer the effects of negative psychosocial working conditions on health? In order to answer these question, we use two waves of data collected by the cross-national Survey of Health, Ageing and Retirement in Europe SHARE I in 2004 and SHARE IV in 2011. We construct an analytic sample of those who were still in the labor force at the baseline of the survey, and, controlling for frailty score at baseline and other relevant sociodemographic characteristics, we predict change in frailty score at follow-up by a set of psychosocial working condition measures, and respondent’s retirement status. Dataset SHARE is a cross-national, longitudinal dataset of noninstitutionalized adults 50 years or older and their partners. At baseline, SHARE collected data from 31,115 people residing in one of the following twelve countries: Austria, Belgium, Denmark, France, Germany, Greece, Italy, Netherlands, Spain, Sweden, and Israel. In its fourth wave, SHARE expanded the sample to a total of 58,489 respondents, now also with additional respondents from the Czech Republic, Estonia, Hungary, Poland, Portugal, and Slovenia, but Greek respondents were not re-contacted for their follow-up survey at that time. For a more detailed description of the survey sampling and data-collection procedures in the individual countries, see Börsch-Supan et al. (2013; 2008) or Abduladze and Börsch-Supan (2013).
We used the following criteria for the construction of our analytical sample. We restricted the analysis to respondents from the eleven European countries that were surveyed at SHARE I. (We exclude respondents from Israel because the first data collection in this country took place nearly two years later than in other countries.) Of these, 12,211 respondents participated in both SHARE I and SHARE IV data-collection waves. To test our hypotheses, we only included the subset of respondents who were employed or self-employed at baseline (N = 3,865). We only used data of the participants who provided complete information about their health status with the biomarker data necessary for the construction of the frailty score at both waves (N = 3,562), and who answered questions about their working conditions (N = 3,408). Furthermore, we limited our sample to those who provided valid answers to questions about all other key characteristics included as controls in our models (N = 3,378)I and for whom SHARE provided valid survey weights (N = 2,508). Finally, we excluded several respondents who reported being in the labor force at their first interview, but at follow-up reported they had retired ten or more years ago. Our final analytical sample consists of 2475 respondents. Descriptive characteristics of the analytical sample are displayed in Table 1.

7
Frailty Measure We created a frailty measure based on the five criteria of the phenotype developed by Fried and associates (2001) . We followed the guidelines described by Santos-Eggimann and colleagues (2009), who adapted the original criteria by Fried and colleagues for SHARE, and measured prevalence of frailty across Europe. Based on their strategy, we allocated one point for each dimension of the frailty phenotype for which the respondent met the frailty criteria. These dimensions included exhaustion, shrinking, weakness, slowness, and low activity. Exhaustion was identified by the question: “In the last month, have you had too little energy to do things you wanted to do?” (25% positive at SHARE I; 27% positive at SHARE IV). The shrinking dimension was considered fulfilled when the respondent said they were experiencing “a diminution in desire for food” when asked: “What has your appetite been like?” (3% positive at SHARE I; 5% positive at SHARE IV). We used biomarker measures of handgrip assessed by a dynamometer during the interview to determine level of weakness. Each respondent was measured four times, twice on each hand, and the highest measurement was used. We then used the gender and body mass-specific cut-off criteria recommended by Fried and colleagues to identify weakness (3% positive at SHARE I; 4% positive at SHARE IV). SHARE measured walking speed only at its first wave and only for some respondents. Based on their analysis, Santos-Eggimann and colleagues recommended using two mobility questions as highly reliable substitutes for slowness. These questions were: “Because of a health problem, do you have difficulty [expected to last more than 3 months] walking 100 meters?” or “…climbing one flight of stairs without resting?” (3% positive at SHARE I; 5% positive at SHARE IV). And finally, respondents were judged to fulfill the criteria for the low-activity dimension if they said they “engage in activities that require a low or moderate level of energy such as gardening, cleaning the car, or going for a walk” only “one to three times a month,” “hardly ever,” or “never (10% positive at SHARE I; 8% positive at SHARE IV). A respondent could earn a maximum number of five points. The average score was 0.45 and 0.49 at SHARE I and IV, respectively. Respondents with no points on any dimension of the phenotype are considered non-frail (63% at SHARE I and SHARE IV); those with one or two points pre-frail (36% at SHARE I and 35% at SHARE IV); and those with three to five points frail (1% at SHARE I and 2% at SHARE IV). Our outcome variable in all models was the change in frailty score between waves. The mean observed increase in frailty was 0.04 points on the scale, with -3 being the largest decrease and +5 the largest increase. Working Conditions Measures The SHARE questionnaire includes a set of psychosocial work-quality items derived from the conceptual frameworks put forth by Karasek (1979), updated by Karasek and Theorell (1990), and Siegrist (1996). We used these questions to construct scales of effort, reward, and control and, subsequently, five measures of negative psychosocial working conditions. The first three of these measures are dichotomized scales, indicating high score on the effort scale, low score on the reward scale, and low score on the control scale. The second two are ratio measures:

8
effort/reward ratio and effort/control ratio. The effort scale ranges from 2 to 8, with the mean of the analytical sample 5.16. The highest quartile of the responses, 6 or more points, were designated as exerting high effort. The reward scale ranges from 4 to 16, with the mean of the analytical sample 10.64. Those who reported 9 or fewer points, the lowest quarter of the responses, were designated as receiving low reward. The control scale ranges from 3 to 12, with the mean of the analytical sample 8.69. Respondents with 8 or fewer points, in the bottom quartile of all responses, were categorized as having low control.
After standardization, we used these same scales to construct ratio measures. The effort/reward ratio ranges from 0.25 to 4, with the mean of the analytical sample 1.02. The effort/control ratio ranges from 0.25 to 4, with the mean of the analytical sample 0.96. In both ratios, values greater than 1 indicated that respondents perceived that job effort exceeded the reward or control they received at their work place. For a more detailed theoretical discussion of these measures, see Siegrist et al. (2004) and Siegrist et al. (2006). The text of questions used for the construction of all measures is included in Appendix A.
Retirement Measure At follow-up, respondents were again asked about their labor force status. 42% of our analytical sample had retired by SHARE IV, and, when retired, had been, on average, 4.11 years out of the labor force. Other Predictor Variables Past research suggests important predictors of declining health in older age that need to be accounted for in our analysis. In multivariable regression models, we control for respondents’ age and gender (male versus not). Social status and financial resources are also important predictors of health status among the elderly. We therefore include a control for educational attainment based on the International Standard Classification of Education (ISCED-97). We categorized respondents as having low (pre-primary, primary, or lower secondary), medium (secondary or post-secondary), or high (first and second stage of tertiary) education (Hoffmeyer-Zlotnik, 2008). We control for income with a SHARE-provided variable designating the country-specific income decile for every respondent. As it is likely that working conditions and their effects on health are influenced by how long has one held a particular job; we also control for job tenure in all models.
Analytic Strategy We present descriptive characteristics of the analytical sample in Table 1. Then we estimate ordinary least-squares regression models predicting between-wave change in frailty by the first three dichotomized scales with country-fixed effects, controlling for frailty score at baseline and other relevant sociodemographic characteristics. These results are presented in Table 2. The following set of results, in Table 3, shows analogous models but with ratio measures used in place of the dichotomized scales. Table 4 presents interactions between working conditions
9
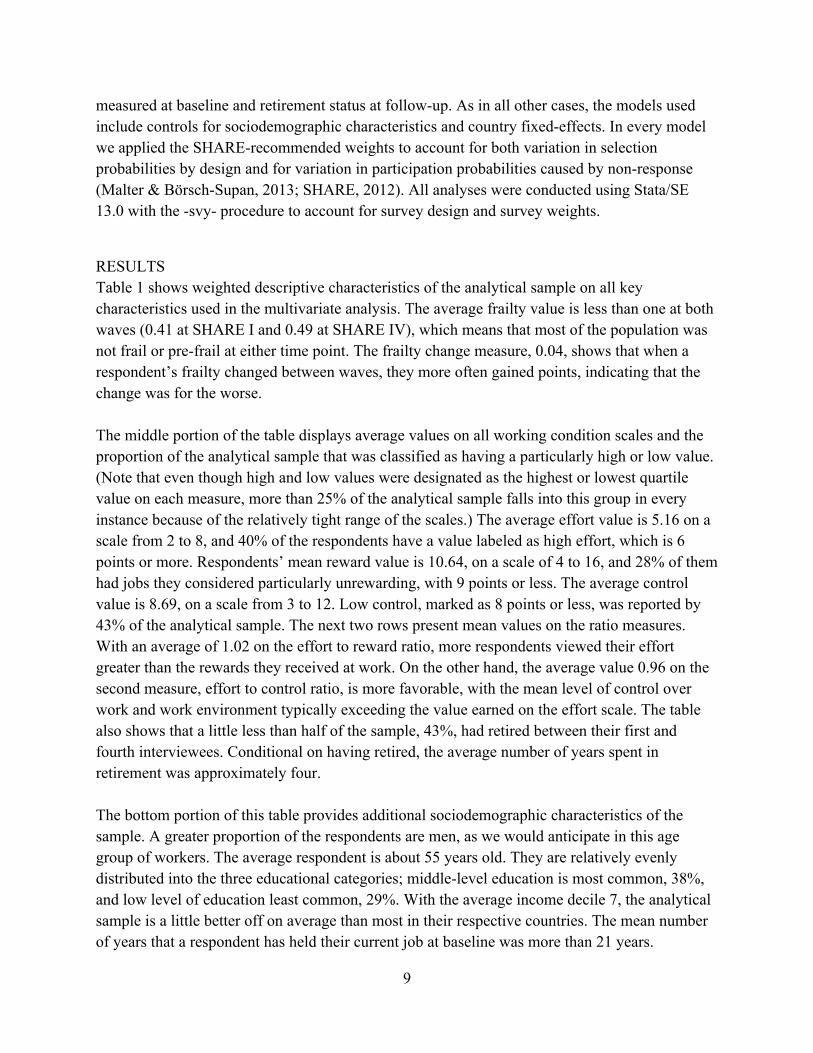
measured at baseline and retirement status at follow-up. As in all other cases, the models used include controls for sociodemographic characteristics and country fixed-effects. In every model we applied the SHARE-recommended weights to account for both variation in selection probabilities by design and for variation in participation probabilities caused by non-response (Malter & Börsch-Supan, 2013; SHARE, 2012). All analyses were conducted using Stata/SE 13.0 with the -svy- procedure to account for survey design and survey weights.
RESULTS Table 1 shows weighted descriptive characteristics of the analytical sample on all key characteristics used in the multivariate analysis. The average frailty value is less than one at both waves (0.41 at SHARE I and 0.49 at SHARE IV), which means that most of the population was not frail or pre-frail at either time point. The frailty change measure, 0.04, shows that when a respondent’s frailty changed between waves, they more often gained points, indicating that the change was for the worse. The middle portion of the table displays average values on all working condition scales and the proportion of the analytical sample that was classified as having a particularly high or low value. (Note that even though high and low values were designated as the highest or lowest quartile value on each measure, more than 25% of the analytical sample falls into this group in every instance because of the relatively tight range of the scales.) The average effort value is 5.16 on a scale from 2 to 8, and 40% of the respondents have a value labeled as high effort, which is 6 points or more. Respondents’ mean reward value is 10.64, on a scale of 4 to 16, and 28% of them had jobs they considered particularly unrewarding, with 9 points or less. The average control value is 8.69, on a scale from 3 to 12. Low control, marked as 8 points or less, was reported by 43% of the analytical sample. The next two rows present mean values on the ratio measures. With an average of 1.02 on the effort to reward ratio, more respondents viewed their effort greater than the rewards they received at work. On the other hand, the average value 0.96 on the second measure, effort to control ratio, is more favorable, with the mean level of control over work and work environment typically exceeding the value earned on the effort scale. The table also shows that a little less than half of the sample, 43%, had retired between their first and fourth interviewees. Conditional on having retired, the average number of years spent in retirement was approximately four. The bottom portion of this table provides additional sociodemographic characteristics of the sample. A greater proportion of the respondents are men, as we would anticipate in this age group of workers. The average respondent is about 55 years old. They are relatively evenly distributed into the three educational categories; middle-level education is most common, 38%, and low level of education least common, 29%. With the average income decile 7, the analytical sample is a little better off on average than most in their respective countries. The mean number of years that a respondent has held their current job at baseline was more than 21 years.

10
– TABLE 1 ABOUT HERE –
In Table 2 we show the results from multivariable ordinary least-squares regression models with country-level fixed effects predicting change in frailty at SHARE IV by each of the scales in turn, with and without a control for retirement status. Coefficients for country fixed-effects are omitted from the display. We find that high effort and low reward are both associated with an increase in frailty, irrespective of controlling for whether or not a respondent had retired by follow-up, but these coefficients are only marginally statistically significant, and they are not especially sizeable. High effort was associated with a 0.07 point increase in frailty and low reward with an 0.08 point increase in frailty. Other significant predictors in these models include being male, having a high level of education, and frailty score at the first wave. Men reported smaller increases in frailty in comparison to women and so did people with high levels of education in comparison to those with medium education. Frailty score at baseline had a negative association with a change in frailty value at follow-up. This means that people with a higher level of frailty at baseline were less likely to see their frailty score grow even higher by the fourth wave.
– TABLE 2 ABOUT HERE –
Table 3 shows models analogous to Table 2, this time with the ratio measures used as main predictors. We find that both ratios are significant predictors of an increase in frailty, although efforts to control ratio only marginally so. A 1 point increase in the to reward ratio measure was associated with a 0.15 point increase in frailty, and a 1 point increase in control to reward measure was associated with a 0.10 increase in frailty. Other significant predictors were similar to Table 2. Here again, being a man, having a high level of education, and frailty score at baseline were predictive of lesser increases in frailty by follow-up.
– TABLE 3 ABOUT HERE –
In Table 4 we display results of ordinary least-squares regression models with the same controls and country fixed-effects as in the previous sets of models; this time with interactions between all working condition measures and retirement status. As the coefficients for control variables are nearly identical with those seen in the last two tables, we only show the coefficients of interactions. We find that retirement does not modify the associations between change in frailty and working conditions with one exception: low reward. For ease of interpretation of this interaction, we include a chart where we visualize the estimated relationship between low reward and retirement. The image shows predicted change in frailty for a 60-year-old male with medium-level education, in fifth income decile, who worked in his current (last) job for twenty years, and who earned no points on the frailty scale at baseline. If this hypothetical male reported

11
high or average reward at work at baseline, and retired by follow-up, we predict an increase in frailty of 0.36. The predicted increase in frailty would be significantly smaller for this person if he had not retired, 0.28. The picture is reversed for those with who reported low reward at baseline. We predicted a between-wave increase of 0.27 for retirees and 0.48 increase for those who stayed in the labor force.
– FIGURE 1 ABOUT HERE –
DISCUSSION Understanding to the processes that influence how we age is high on the list of priorities for scientific researchers and policy makers. The range of exposures with documented consequences for health in older age includes events occurring as early as in-utero and spans across childhood through the end of midlife (for an overview see Kuh et al., 2003). In this article, we consider the influence of psychosocial working conditions on change in health in later life and the potential sheltering role of retirement.
The impact of working conditions on health has been studied primarily with respect to the health outcomes of those who are currently employed. In the short term, it has been shown that those who report negative psychosocial working conditions are more likely to experience an on-the-job injury (Gillen et al., 2007) or absenteeism (Melchior et al., 2003). In the medium term, it has been demonstrated that negative psychosocial working conditions are connected to, for example, weakened function of the cardiovascular system (Bosma et al., 1998) or poor mental health (Laaksonen et al., 2006). Considering how working conditions may be affecting people’s health in later life and even after retirement is a natural extension of the present theoretical framework, and our study provides some of the first empirical evidence in support of such a relationship.
We found that high effort and low reward predicted a greater decline in health, measured as frailty, both in their binary indicator forms and as ratios. It is thus likely that jobs with a combination of high effort and low reward are especially damaging to the health of people in this age group. We also found that a greater effort to control ratio predicted an increase in frailty; however, this finding could be primarily driven by the associations of low reward to change in health. Our findings corroborate the results of previous studies that focus on people who are still in the labor force and suggest that adverse working conditions might translate to more permanent or progressive damage to physical health.
In answering our second research question, exploring the potential buffering effect of retirement, we discovered that the relationship between low reward and change in frailty was indeed modified by respondents’ retirement status. Low reward had the most detrimental consequences for health when a respondent did not retire. On the other hand, respondents with low reward conditions at baseline, who retired by follow-up, experienced the least deterioration in their

12
physical health. Importantly, we predicted a greater frailty increase among those who retired from average or high reward positions compared with those who stayed employed. This finding adds an additional layer to the extant literature on the health effects of retirement that has thus far been inconclusive in its assessment of retirement’s consequences on health (Van Der Heide et al., 2013). However, it is important to qualify this result by adding that it is vulnerable to the threat of endogeneity. Although we controlled for frailty at baseline, it is possible that a worker retired in response to a sudden downturn in his or her health that took place between baseline and follow-up. If this was more often the case for workers in jobs with average or high reward, the resulting picture for this group would be similar, but the underlying mechanism is radically different. Our analysis is not able to distinguish between these two situations.
This study has several additional limitations that need to be considered. The psychosocial working condition measures we constructed are relatively crude in comparison with those used in surveys that mainly focus on the quality of working conditions. Further research would benefit from testing these questions with more nuanced indicators that would allow researchers to discuss what particular components of low reward and high effort could be especially damaging to later life health. Moreover, we do not have any information about how long have respondents been experiencing negative working conditions, and this affects the strength of the conclusions we can draw on the basis of our study. It could be the case that working conditions in later life are quite different from those in other parts of the life course, even in the same job. Moreover, while some respondents might be evaluating their working conditions during their entire job tenure, some may be speaking to how they have been experiencing their job lately. Therefore, our study cannot speak to the issue of cumulative working conditions over the life course. Furthermore, the results of our study are only valid if the constructs and measures we rely on are cross-nationally neutral and translatable across Europe. While it is unlikely that the more fact-focused questions—such as “How many years of education have you completed” or “Do you have difficulty climbing one flight of stairs without resting?”—would be affected by the social and cultural differences among the countries surveyed, some of the psychosocial working conditions measures, such as “My immediate work environment was uncomfortable,” may not be as directly comparable. Fortunately, most of the working conditions measures that were used in this study have been previously validated cross-nationally in several other studies (e.g. Choi et al., 2009; R. Karasek et al., 1998; Siegrist et al., 2004). Finally, our findings might be impacted by selection bias and non-random attrition. It is possible, even probable, that the subsections of the population that were most negatively affected by adverse work environments were also those most likely to be excluded from the sample by retiring early (Wahrendorf et al., 2012a) or due to their premature death or institutionalization. If this is the case, our results are biased toward zero. The matter is further complicated by the fact that SHARE has a relatively low response rate in some regions and a non-negligible attrition rate

13
between the first and fourth wave of the survey, which has led to the reduction of the sample size used in this study and limited our analytical possibilities. We rely on the provided ex-post calibrated weights to reduce the bias in our estimates (Börsch-Supan et al., 2013). The shortcomings of this study notwithstanding, it provides new and valuable insights into the connections between psychosocial working conditions and health in later life. In particular, we show evidence that high effort and low reward might play an important role in determining an individual’s physical aging, and that, for individuals who have jobs with little reward, retirement may help with tempering their consequences for physical health. This finding needs to be taken into account by policy makers of the many European nations that are re-evaluating their mandatory or recommended retirement ages at the moment, as it may come with unexpected health costs. The burdens of unfavorable working conditions are born both by individuals and societies. In 2007, the EU’s Occupational Safety and Health Administration released a report showing clear indications of an increase in negative psychosocial working conditions across European workplaces. The report calls for policies designed to ameliorate working conditions and reverse this trend because negative working conditions are associated with the loss of productivity and harm the health of workers (EU-OSHA, 2007). We would like to expand this declaration by arguing that workers with poor working conditions are not only less likely to be productive while labor force active, they may also eventually be in need of a greater amount of health care. Our study is yet another contribution to the rapidly expanding body of research that shows how social and economic policies influence and even shape population health (Schoeni, 2008). Policies and labor laws that strengthen the position of employees on the job would likely result in more rewarding work experiences. As past research demonstrated, this could translate to lasting improvements in the health of the working population. Our study contends that labor laws and policies have health effects greater than those that can be observed among workers and need to be considered in the framework of the lifecourse health trajectory.
ENDNOTES
I. Due to a large amount of missing data about respondents’ sources of income that would not allow for the construction of the aggregate gross household income indicator (63.11 %), we relied on the imputed income decile values generated and distributed by the SHARE survey research team.

14
REFERENCES
Abduladze, L.M.F., & Börsch-Supan, A. (2013). SHARE Wave 4 : Innovations & Methodology. München: Munich Center for the Economics of Aging.
Ahmed, N., Mandel, R., & Fain, M.J. (2007). Frailty: An Emerging Geriatric Syndrome. The American journal of medicine, 120, 748-753.
Barker, D.J.P. (1998). Mothers, babies, and health in later life. Edinburgh; New York: Churchill Livingstone.
Börsch-Supan, A., Brandt, M., Hunkler, C., Kneip, T., Korbmacher, J., Malter, F., et al. (2013). Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). International Journal of Epidemiology.
Börsch-Supan, A., Hank, K., Jürges, H., & Schröder, M. (2008). Longitudinal data collection in continental Europe : experiences from the Survey of Health, Ageing and Retirement in Europe (SHARE). Mannheim: Univ., Fak. für Volkswirtschaftslehre und Statistik.
Bosma, H., Peter, R., Siegrist, J., & Marmot, M. (1998). Two alternative job stress models and the risk of coronary heart disease. American Journal of Public Health, 88, 68-74.
Choi, B., Bjorner, J.B., Ostergren, P.O., Clays, E., Houtman, I., Punnett, L., et al. (2009). Cross-language differential item functioning of the job content questionnaire among European Countries: The JACE study. International Journal of Behavioral Medicine, 16, 136-147.
Clegg, A., Young, J., Iliffe, S., Rikkert, M.O., & Rockwood, K. (2013). Frailty in elderly people. The Lancet, 381, 752-762.
EU-OSHA (2007). Expert forecast on emerging psychosocial risks related to occupational safety and health. Luxembourg: Office for Official Publications of the European Communities.
European Commission. (2009). The 2009 Ageing Report : Economic and Budgetary Projections for the EU-27 Member States (2008-2060). Luxembourg: Office for Official Publications of the European Communities.
Fried, L.P., Tangen, C., Walston, J., Newman, A., Hirsch, C., Gottdiener, J., et al. (2001). Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci, 56, M146 - 156.
Fried, L.P., Xue, Q., Cappola, A., Ferrucci, L., Chaves, P., Varadhan, R., et al. (2009). Nonlinear multisystem physiological dysregulation associated with frailty in older women: implications for etiology and treatment. J Gerontol A Biol Sci Med Sci, 64, 1049 - 1057.
Geurts, S.A.E., & Sonnentag, S. (2006). Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scandinavian Journal of Work, Environment and Health, 32, 482-492.
Gillen, M., Yen, I.H., Trupin, L., Swig, L., Rugulies, R., Mullen, K., et al. (2007). The association of socioeconomic status and psychosocial and physical workplace factors with musculoskeletal injury in hospital workers. American Journal of Industrial Medicine, 50, 245-260.
Hamer, M., Kivimaki, M., & Steptoe, A. (2012). Longitudinal patterns in physical activity and sedentary behaviour from mid-life to early old age: A substudy of the Whitehall II cohort. Journal of Epidemiology and Community Health, 66, 1110-1115.
Hoffmeyer-Zlotnik, J.H.P. (2008). Harmonisation of Demographic and Socio-Economic Variables in Cross-National Survey Research. Bulletin de Méthodologie Sociologique, 98, 5-24.
ILO & WHO Committee on Occupational Health (1986). Psychosocial factors at work : recognition and control. Geneva: International Labour Office.

15
Johnson, R.C., Schoeni, R.F., & Rogowski, J.A. (2012). Health disparities in mid-to-late life: The role of earlier life family and neighborhood socioeconomic conditions. Social Science and Medicine, 74, 625-636.
Kaplan, G.A., Seeman, T.E., Cohen, R.D., Knudsen, L.P., & Guralnik, J. (1987). Mortality among the elderly in the Alameda County Study: behavioral and demographic risk factors. American journal of public health, 77, 307.
Karasek Jr, R.A. (1979). Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Administrative Science Quarterly, 24, 285-308.
Karasek, R., Brisson, C., Kawakami, N., Houtman, I., Bongers, P., & Amick, B. (1998). The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. Journal of occupational health psychology, 3, 322-355.
Karasek, R., & Theorell, T. (1990). Healthy work : stress, productivity, and the reconstruction of working life. New York: Basic Books.
Kivimäki, M., Virtanen, M., Elovainio, M., Kouvonen, A., Väänänen, A., & Vahtera, J. (2006). Work stress in the etiology of coronary heart disease - A meta-analysis. Scandinavian Journal of Work, Environment and Health, 32, 431-442.
Kuh, D., Ben-Shlomo, Y., Lynch, J., Hallqvist, J., & Power, C. (2003). Life course epidemiology. Journal of Epidemiology and Community Health, 57, 778-783.
Laaksonen, M., Rahkonen, O., Martikainen, P., & Lahelma, E. (2006). Associations of psychosocial working conditions with self-rated general health and mental health among municipal employees. International Archives of Occupational and Environmental Health, 79, 205-212.
Lamontagne, A.D. (2012). Invited commentary: Job strain and health behaviors-developing a bigger picture. American Journal of Epidemiology, 176, 1090-1094.
Malter, F., & Börsch-Supan, A. (2013). SHARE Compliance Profiles - Wave 4. Munich: Max Planck Institute for Social Law and Social Policy.
Melchior, M., Niedhammer, I., Berkman, L.F., & Goldberg, M. (2003). Do psychosocial work factors and social relations exert independent effects on sickness absence? A six year prospective study of the GAZEL cohort. Journal of Epidemiology and Community Health, 57, 285-293.
Mitnitski, A., Graham, J., Mogilner, A., & Rockwood, K. (2002). Frailty, fitness and late-life mortality in relation to chronological and biological age. BMC Geriatr, 2, 1.
Rechel, B., Grundy, E., Robine, J.-M., Cylus, J., Mackenbach, J.P., Knai, C., et al. (2013). Ageing in the European Union. The Lancet.
Romero-Ortuno, R., Walsh, C.D., Lawlor, B.A., & Kenny, R.A. (2010). A Frailty Instrument for primary care: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatrics, 10.
Rowe, J., & Kahn, R. (1987). Human aging: usual and successful. Science, 237, 143-149. Santos-Eggimann, B., Cuenoud, P., Spagnoli, J., & Junod, J. (2009). Prevalence of frailty in
middle-aged and older community-dwelling Europeans living in 10 countries. J Gerontol A Biol Sci Med Sci, 64, 675 - 681.
Schnittker, J. (2005). When mental health becomes health: Age and the shifting meaning of self-evaluations of general health. Milbank Quarterly, 83, 397-423.
Schoeni, R.F.R.S.F. (2008). Making Americans healthier : social and economic policy as health policy. New York: Russell Sage Foundation.

16
SHARE. (2012). SHARE IV Release Guide 1.1.1. Siegrist, J. (1996). Adverse health effects of high-effort/low-reward conditions. Journal of
occupational health psychology, 1, 27-41. Siegrist, J., & Rödel, A. (2006). Work stress and health risk behavior. Scandinavian Journal of
Work, Environment and Health, 32, 473-481. Siegrist, J., Starke, D., Chandola, T., Godin, I., Marmot, M., Niedhammer, I., et al. (2004). The
measurement of effort-reward imbalance at work: European comparisons. Social Science and Medicine, 58, 1483-1499.
Siegrist, J., Wahrendorf, M., von dem Knesebeck, O., Jürges, H., & Börsch-Supan, A. (2006). Quality of work, well-being, and intended early retirement of older employees—baseline results from the SHARE Study. The European Journal of Public Health, 17, 62-68.
Strawbridge, W.J., Cohen, R.D., Shema, S.J., & Kaplan, G.A. (1996). Successful Aging: Predictors and Associated Activities. American Journal of Epidemiology, 144, 135-141.
Strawbridge, W.J., Wallhagen, M.I., & Cohen, R.D. (2002). Successful Aging and Well-Being. The Gerontologist, 42, 727-733.
Van Der Heide, I., Van Rijn, R.M., Robroek, S.J.W., Burdorf, A., & Proper, K.I. (2013). Is retirement good for your health? A systematic review of longitudinal studies. BMC Public Health, 13.
Wahrendorf, M., Dragano, N., & Siegrist, J. (2012a). Social Position, Work Stress, and Retirement Intentions: A Study with Older Employees from 11 European Countries. European Sociological Review.
Wahrendorf, M., Sembajwe, G., Zins, M., Berkman, L., Goldberg, M., & Siegrist, J. (2012b). Long-term effects of psychosocial work stress in midlife on health functioning after labor market exit - Results from the GAZEL study. Journals of Gerontology - Series B Psychological Sciences and Social Sciences, 67 B, 471-480.
Walston, J., Hadley, E.C., Ferrucci, L., Guralnik, J.M., Newman, A.B., Studenski, S.A., et al. (2006). Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc., 54, 991-1001.

Mean or % Min MaxHealth Measures Frailty Score at W1 (mean) 0,45 0 4 Frailty Score at W4 (mean) 0,49 0 5 Frailty Score Change W1 to W4 (mean) 0,04 -3 5
Working Conditions Measures (all measured at W1) Effort Score (mean) 5,16 2 8 High Effort (%) 0,40 0 1 Reward Score (mean) 10,64 4 16 Low Reward (%) 0,28 0 1 Control Score (mean) 8,69 3 12 Low Control (%) 0,43 0 1 Effort/Reward Ratio at W1 (mean) 1,02 0,25 4 Effort/Control Ratio at W1 (mean) 0,96 0,25 4
Retirement Transitions Retired between W1 and W4 (%) 0,43 0 1 Years retired by W4 (conditional mean) 4,11 0 9
Other Sociodemographic Characteristics (all measured at W1) Male (%) 0,58 0 1 Age (mean) 55,14 50 80 Education Low (%) 0,29 Medium (%) 0,38 High (%) 0,33 Household Income Decile (mean) 7,07 1 10 Job Tenure (mean) 21,49 0 64N 2.475
Table 1. Weighted health, working conditions and sociodemographic characteristics of the analytic sample.
1 3