
dataprocessing system adapted to special emergency...
9
J Clin Pathol 1983;36:847-855 A data processing system adapted to the special needs of the emergency laboratory D NEUMEIER,* H SATOR, GE RINDFLEISCH, M KNEDEL From the Institutfiir Klinische Chemie, Klinikum Groj3hadern, Ludwig-Maximilians-Universitat Miinchen, Munchen, West Germany SUMMARY A data processing system for the emergency laboratory was integrated in our clinical laboratory computer system, its prime objective being the service requirements of the laboratory. It included the possibility of simultaneous optical reading of request forms and on-line capturing, processing, and printing of laboratory test data. Priority request forms, which allow the clinician to specify the interval by which emergency test results must be available, are registered by an optical reader and arranged according to urgency by the computer. The production of worksheets is replaced by visual display of information required for accurate specimen analyses on a large colour TV screen. The individual processing status of all tests from as many as 30 request forms is displayed in a colour code. For process control the updated delay time for test performance is faded in. All reports are produced by direct machine transfer of verified test results. For security purposes all steps of sample processing (request, result, report) are recorded via line printers outside the emergency laboratory. The capacity of the computer for managing sample and data processing reduces the work load for technicians. This results in a reduction of the turn-round time of tests. 95% of all requested tests are performed and reported within the requested time period and in emergencies, test results are available within 5-10 min. There has been no major breakdown of the system in over one year of use. The number of emergency tests in clinical labora- tories has increased. Now, in some laboratories 25% of all routine analyses are requested as emergencies. ' In spite of the impact for patient care, workload and internal laboratory organisation, reports about this important facet are scanty. 1-8 Many factors contribute to excess use of the chemi- cal laboratory.9 In the case of emergency tests, requests arise from the proportion of high-intensity care beds in large university hospitals, the advent of new parameters, medicolegal considerations, inad- equate knowledge of test characteristics by the physician responsible for requesting, and intrinsic dif- ficulties of centralised laboratories in handling non- routine samples. Until recently, large capacity analysers have been inappropriate for processing single specimens with only a few tests. In addition the *Present address: Dr D Neumeier, Institut fir Klinische Chemie, Klinikum GroBhadern, PO Box 701 260, D-8000 Munchen 70, GFR. Accepted for publication 7 October 1982. procedure of blood sampling early in the day with reporting of results later the same day is not suitable in many clinical situations. This increasing demand as well as organisational problems led to the establish- ment of special emergency laboratories in many hospitals. This laboratory performs all tests which are collected outwith fixed admission hours for routine specimens. An advantage of centralising the emer- gency service in a single laboratory is that it provides a pool of specially trained technical staff, and that the greater work load reduces costs per single test. An important aspect of "emergency tests" is that not all the results are really needed within a few minutes or hours as long as they are available sometime during the day. ' The turn-round times desired by clinicians vary between minutes and a few hours. In a study of 53 laboratories in North America, Barnett et al " points out the problems in dealing with priority requests. Many institutions have a priority system, but a surprising number improvise, without a definite plan. For tests labelled as "soon", "instantly", "immediate", "stat", "urgent" or 847 on 23 May 2018 by guest. Protected by copyright. http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. Downloaded from
Transcript of dataprocessing system adapted to special emergency...

J Clin Pathol 1983;36:847-855
A data processing system adapted to the special needsof the emergency laboratoryD NEUMEIER,* H SATOR, GE RINDFLEISCH, M KNEDEL
From the Institutfiir Klinische Chemie, Klinikum Groj3hadern, Ludwig-Maximilians-Universitat Miinchen,Munchen, West Germany
SUMMARY A data processing system for the emergency laboratory was integrated in our clinicallaboratory computer system, its prime objective being the service requirements of the laboratory.It included the possibility of simultaneous optical reading of request forms and on-line capturing,processing, and printing of laboratory test data. Priority request forms, which allow the clinician tospecify the interval by which emergency test results must be available, are registered by an opticalreader and arranged according to urgency by the computer. The production of worksheets isreplaced by visual display of information required for accurate specimen analyses on a large colourTV screen. The individual processing status of all tests from as many as 30 request forms isdisplayed in a colour code. For process control the updated delay time for test performance is fadedin. All reports are produced by direct machine transfer of verified test results. For securitypurposes all steps of sample processing (request, result, report) are recorded via line printersoutside the emergency laboratory.The capacity of the computer for managing sample and data processing reduces the work load for
technicians. This results in a reduction of the turn-round time of tests. 95% of all requested tests areperformed and reported within the requested time period and in emergencies, test results areavailable within 5-10 min. There has been no major breakdown of the system in over one yearof use.
The number of emergency tests in clinical labora-tories has increased. Now, in some laboratories 25%of all routine analyses are requested as emergencies. 'In spite of the impact for patient care, workload andinternal laboratory organisation, reports about thisimportant facet are scanty. 1-8Many factors contribute to excess use of the chemi-
cal laboratory.9 In the case of emergency tests,requests arise from the proportion of high-intensitycare beds in large university hospitals, the advent ofnew parameters, medicolegal considerations, inad-equate knowledge of test characteristics by thephysician responsible for requesting, and intrinsic dif-ficulties of centralised laboratories in handling non-routine samples. Until recently, large capacityanalysers have been inappropriate for processingsingle specimens with only a few tests. In addition the
*Present address: Dr D Neumeier, Institut fir Klinische Chemie,Klinikum GroBhadern, PO Box 701 260, D-8000Munchen 70, GFR.
Accepted for publication 7 October 1982.
procedure of blood sampling early in the day withreporting of results later the same day is not suitablein many clinical situations. This increasing demand aswell as organisational problems led to the establish-ment of special emergency laboratories in manyhospitals. This laboratory performs all tests which arecollected outwith fixed admission hours for routinespecimens. An advantage of centralising the emer-gency service in a single laboratory is that it provides apool of specially trained technical staff, and that thegreater work load reduces costs per single test. Animportant aspect of "emergency tests" is that not allthe results are really needed within a few minutes orhours as long as they are available sometime duringthe day. ' The turn-round times desired by cliniciansvary between minutes and a few hours.
In a study of 53 laboratories in North America,Barnett et al" points out the problems in dealing withpriority requests. Many institutions have a prioritysystem, but a surprising number improvise, withouta definite plan. For tests labelled as "soon","instantly", "immediate", "stat", "urgent" or
847
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

848
"rush", the priorities are determined depending onthe patient's condition, in which hospital area therequest originated or by the type of test requested.Such inexact terminology prompted us in 1978 toprovide boxes on the request form to mark definitivedelay times, which inform the staff when the resultsare required at the clinical units. Simultaneously andindependently of us Henderson' developed a similarrequest form for emergency tests. Our experience,however, shows that it is very difficult to control theworkflow of specimens in a changing order of priorityby means of a conventional laboratory daybooksystem. This is particularly so when the work load isheavy and then the processing usually follows the"first-in/first-out" rule.
In response to the increasing work load and theproblem of request priorities we incorporated theemergency data handling into the computer system ofour clinical laboratory. The modification of oursystem was completed by June 1981. Since that time ithas been in constant routine use. We describe thepresent system and highlight the special requirementsof an emergency laboratory in system design.
Functions and workload ofthe Istitute of ClinicalChemistry
The Institute of Clinical Chemistry incorporated in anewly built university hospital is a centralised labora-tory for all routine pathology tests in haematologyincluding haemostasis, clinical chemistry, endo-crinology and protein chemistry. It provides facilitiesaround the clock for 14 clinical departments with 1348beds as well as outpatient services. One hundred andeighteen beds are intensive care beds.Each year over 530 000 specimens with approxi-
mately 2- 8 million requested tests and a workload ofnearly 4 0 million analyses are performed. Within theemergency laboratory the daily workload varies bet-ween 350 and 500 requests with 2000 tests performed.This includes all tests out of routine admission hours(0730-0900 h) but excludes all the specimens of out-patients and the routine monitoring of blood glucoselevel. All specimens are sent directly from the clinicalunits to the laboratory by a dedicated pneumatic tubesystem.
Since June 1980 a new central clinical laboratorycomputer system assists in specimen processing and inhandling of the data in all laboratories except theemergency laboratory. This new developed system isbased on the experiences with an older data pro-cessing system (Siemens 305/SILAB)'2 used from1974 to 1980.
Neumeier, Sator, Rdfleisch, Knedel
Design objectives of the emency bo ry dataprocessing system
The data processing system for the emergency labora-tory was designed as part of the central clinicallaboratory computer system but with the require-ments of the emergency service as its prime objective.It includes optical reading of request forms withsimultaneous capture, processing and printing oflaboratory test data. The system is designed to facili-tate smooth workflow and to reduce turnaroundtime. Emphasis is placed on the ability of thecomputer to manage sample processing in order ofpriority.A data processing system in operation for 24 h must
give maximum flexibility and protection fromcomputer breakdown to be accepted by the labora-tory technical staff. To provide this the emergencyversion of our clinical laboratory computer systemwas tailored to the needs of this laboratory and wasdesigned so that:(a) at any time the current status of sample proces-
sing is clearly obvious. Worksheets and result-listings are replaced by display of all requisiteinformation on a large colour TV monitor. Thestatus of all tests from as many as 30 separaterequest forms is displayed in a colour code.From top to bottom the request forms are up-dated by the computer in a decreasing orderof priority, not in the serial sequence ofacquisition;
(b) on-line capture of patient identification data(PID) and nearly all of test result data ispossible;
(c) specimens can be analysed in any sequence;(d) no restraints are imposed on the order in which
the work on each specimen is performed for theinput of PID and the various test results areindependent of each other;
(e) the laboratory technical staffcan correct any testresult;
(f) comments could, when necessary, replace orsupplement test results in the final reportdocument;
(g) all test results have to be validated by the labora-tory technical staff. As far as possible they areassisted by the computer- for example, it checksfor life-incompatible test results;
(h) each validated test result can be made availableto the physician at any time, if necessary, as anincomplete report; a visual display unit is usedto provide the laboratory technical staff all up-to-the-minute information and all requisite data(demographic and test related data, all orselected updated previous results). At any timeall relevant data up to the most recent, from all
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

A data processing system adapted to the special needs ofthe emergency laboratory
parts of the institute are available on this and allother VDUs in the system in order to answertelephone inquiries; the system is operatedthrough a "menu" structure organised by amaster program, which is executed automatical-ly when a VDU is logged to the system. Themaster program then displays a list of options atthe terminal. The speed of filing and retrieval isnot reduced to such an extent as to render thisimpractical since multiple copies of specifiedprograms can be active at the same time;
(i) in addition, worksheets are continuouslygenerated by request form and result-listingsgenerated by test result are produced near to butoutside the laboratory. They provide a safetyfactor to ensure that no data already in thesystem are lost if the laboratory computersystem breaks down. It should be emphasisedthat the worksheets are not used as a means oflaboratory specimen management and that theydo not impose any constraints on the laboratorytechnical staff. Indeed, the system allows pro-cessing and operation without any worksheetsbeing printed at all.
Hardware
The computers used are two Siemens R-30 with 256 Kwords each and adequate external storage on twodrums and four disc-drives. The peripheral unitsneeded for the system are one semigraphic colourdisplay unit, one VDU for communication with thesystem, one printer with 200 lines/min and fiveprinters with 140 characters per second in the labora-tory. In addition there are 22 printers distributed
Optical .1 VDU 13~~'
reader _u
Line status ofprinter scrrmVe
Lineprinters
throughout the hospital. As interfaces, which arenecessary to convert the output from analysers into aform suitable for input into the computer units of theSILAB system (Siemens AG, Munich) are used.'2
Software
The emergency computer system is integrated as partof the central laboratory computer system. For thepast two years this modular structured system servesall sections of the laboratory. 3 To reach a high levelof availability all application programs have beenwritten in assembler language by the staff of theinstitute. The software allows, that the two centralunits operate in a master-slave mode - that is, oneunit processes all data, while the other secures allimportant results and information.
Processing of data
The flow diagram (Fig. 1) demonstrates the mainsequence of events.
Request form
We developed a computer readable request form foremergency tests (Fig. 2), which is in keeping with allother routine request forms of the institute but withthe special requirements of the emergency laboratoryin mind. On the front of the request form from top tobottom there have to be marked: the patient identifi-cation number (hospital numberof the patient) whichis unique for the period of hospitalisation; the wardcode and the time the specimen was drawn; spacefollows for the clinical indication of the emergency
Fig. 1 Flow diagram delineatingcomputerised processing ofemergency
/DU laboratory data.control
849
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

Neumeier, Sator, Rindfleisch, Knedel
KLINIKUM GROSSHADERNDNOflUT FOR KLiNISC$E CREMiEftdkot: batt. Or. M1. K, d
def ;;;_ ................
Fig. 2 Request form for theemergency laboratory: Frontside (left) from top to bottom;Patient identification number,ward code, time when specimenwas drawn, indication fornon-routine investigations andadditional clinical information.Reverse side (right) from top tobottom; boxes for the specificdelay time, frequendy performedtests (i.e., leucocyte count) andtest code numbers of infre-quently performed tests.
investigation, for clinical information relevant to theanalysis itself and for the interpretation of the testresults. At the bottom of the form fields are providedfor the laboratory accession number.When a specimen arrives at the laboratory the con-
tainer or the containers and the accompanying testrequest form are given a five digit laboratory acces-sion number. Self-adhesive labels are pre-printed forthe identification of specimens. The first two digits ofthe accession number represent the day of the monthand the last three start daily at 001 and are increasedby one for each succeeding request form. This easilyunderstood number is unique in any month and linkspatient identification data, sample collection timeand test results. The computer is designed for up to
700 emergency request forms each day but could beexpanded if necessary.The back of the request form is reserved for
indicating tests to be performed on the specimens.Those frequently performed are tabled and arerequested by a single mark in the appropriate box;those infrequently requested are indicated by a fourdigit code number. The codes are specified in adirectory issued to all medical and nursing staff. Thislist is updated regularly with the addition of new testsor discarding those found inadequate. On the first lineof the back of the form, the requesting physicianindicates the specific delay by which he should havethe report of the emergency test results. This timeinterval, varying from one hour to sometime during
850
awmw
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

A data processing system adapted to the special needs ofthe emergency laboratory
the day, allows the clinician to discriminate betweensituations requiring immediate or delayed test per-formance. Single tests can be additionally flagged inan emergency or during a surgical operation, if testresults indicate the need for immediate treatment ofthe patient. The signal induces the interruption of allother emergency services and the immediate per-formance of the flagged test.
ENTRY OF THE DATA OF THE REQUEST FORMReal-time controlAll information on the request form is entered intothe laboratory computer by a compact optical readerdeveloped by our technical staff. 4 Data on both sidesof the request form are read simultaneously. In theevent that a request form has not been read properlythe readers display up to fifteen error codes. Thisallows real-time control of the data entry so that errorscan be corrected at once. When the identificationdata for a new patient are missing, these data arerecalled from the central hospital computer. In rareconditions of urgency, patient's name and forenamecan be entered into the computer via the VDU in theemergency laboratory.
Processing control on the TV screenAfter reading the request form all data relevant fortest performance are displayed on a large centralcolour TV screen. The request forms are continu-ously updated by the computer in a decreasing orderof urgency according to the physician-indicated delaytimes and displayed like the presentation of the flyingschedule at an airport. Each request form occupiesone horizontal line and the ten most frequentlyrequested tests are displayed in reserved columns.The information given on the screen for each requestform is: accession number, remaining delay time fortest performance and requested test symbolised byred rectangles in the respective columns. Tests per-formed infrequently are indicated by a red underlaidthree-character code in the remaining fields. Flashingtest symbols emphasise the highest priority of flaggedtests. For process control the remaining delay time oftest performance is updated by the computer everyfive minutes. This graphic presentation of all in-formation required for priority controlled specinenanalyses is generated continuously by each newrequest form. On the screen up to 30 acquisitionnumbers are displayed. In addition to these thenumber of request forms not outlined on the screen isfaded in on the bottom.The visual display allows the analytical procedure
to start after batching of samples without any delaycaused by worksheet printing. The samples can beanalysed immediately after entering the accessionnumber (see below) even before the information on
the request sheet is input. In the few cases when atest-oriented worksheet is required to make up anassay batch listing can easily be triggered via enteringthe test code number by the technician.
Additional information supplied by the computersystemProvision has been made to have access to all patientdata, which might be important for performing a test.By entering the laboratory accession number of thespecimen or the patient identification number on avisual display unit pertinent data are displayed on thescreen. This information includes name, sex, age,clinical unit, first day of hospitalisation, the clinicaldetails marked on the request sheet including indi-cation, diagnosis, therapeutic procedures influencingtest or interpretation and the result and date ofprevious tests if any are on file. This informationhelps technical staff to prepare the specimenadequately and to monitor test performance.By entering the patient identification number in a
"historical" data file the cumulative results of allprevious laboratory tests are obtained. Comprehen-sive computer-based cumulative filing according totest code number, date or the pathological characterof results is possible as well. These disc file searchesare not time consuming and do not retrench the "real-time" nature of the system.
Data protectionFor security purposes a paper worksheet is printedoutside the emergency laboratory. This worksheetgenerated continuously per laboratory accessionnumber includes all the above specified "worksheet-type" data. The list can be used when the centralcolour TV screen does not operate.
TEST DATA CAPTUREOn-line test dataThe basic devices currently in use in the emergencylaboratory include two Coulter Counters S, two flamephotometers, two photometers, one atomic absorp-tion photometer and two automated chemicalanalysers (ACA, DuPont) (Fig. 3). This nearly dupli-cated analytical equipment allows the immediateperformance of laboratory tests in situations when asingle analyser does not work. The laboratorycomputer receives on-line all the results generated bythese analysers together with the associated sampleaccession number, which is entered into the computervia keyboards at the analysers or via the patientidentification card (ACA, DuPont) before or con-current with the entry of results. At both CoulterCounters S the analytical results, the accessionnumber and the patient identification number aremerged and displayed together with the patient
851
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

852
Fig. 3 On-line analysers ofthe emergency laboratory.
identity data and information about the previous testresults on a small associated VDU screen. Values areflagged to highlight statistically abnormal and analy-tically invalid results that is, outside the measuringrange, whole blood control sample outside the presetrange. These methods, direct monitoring of resultsand computer-assisted quality control at the time ofanalysis, allow reduction of the sample processingtime and technical staff do not have to wait for a hardprint copy.The photometers linked on-line by microprocessor
interfaces have digital displays incorporated in thefront panel. Test data transfer is initiated, when the"data" key is pressed. The laboratory data processingsystem provides an immediate printout of analyticallydoubtful results outside given limits, for example,quality control range, diluting limit.
Manual test dataThe procedures for the miscellaneous manual testssuch as coagulation tests, microscopic urine examina-tion or cell counts in spinal fluid differs slightly fromthat of on-line tests. Here the results as well as theassociated accession number are entered through akeyboard. For microscopic urine examination thekeyboards used have keys coded for 16 various urineingredients. The results of the coagulation testsmeasured in seconds or as a percentage of normal areentered directly. In addition, the keyboards are usedfor the correction of a test result and for the input offour digit comment codes representing a variety ofreasons which may either exclude test performance oraffect the result of a given test. An example of the firstis the comment "clotted." This type of commentsubstitutes for a test result, whereas the comment"lipaemic" does not inhibit the input of a test result.
Newneier, Sator, Rindfleisch, Knedel
Processing control on the colour TV screenOn the colour TV screen the red rectangle symbo-lising the status of a requested test changes to yellowafter entry of a computer-controlled test result in theresult file. Thus every technologist within the rota hasan immediate and continuously updated informationof the processing status of all actual request forms.
Data protectionAll analytical results entered into the computer areprinted simultaneously with the associated accessionnumber in a condensed form by line-printers outsidethe emergency laboratory. These intralaboratoryresult copies ensure that in the cases of a major failurein the data processing equipment only the mostrecently transferred data will be lost.
DATA VALIDATIONThe computer controlled analytical data cannot beprinted on patient reports until they have been re-viewed and validated by the laboratory technicalstaff. The program used for preanalytical patientinformation provides also facilities to display the ana-lytical results merged with requisite patient detailson a VDU screen. Validated results are flagged byentering the single-character code F for "free."This comment allocates the test results to the reportprinting program. When the laboratory staff, how-ever, enters the comment S (Sperren), the data areretained only in the raw data file. Additionally pro-visions are made to override the computer checks.The option E (Entsperren) for "additionally con-trolled" enables the laboratory staff to verify a result,which has previously been blocked by the computer-for example, manually controlled results outside themeasuring range of the Coulter S. For normal use testdata validation is performed according to the acces-sion number. But all these options can also be used inthe result files of the single tests. When this way ischosen, the results of a single analytical method or agroup of tests are displayed in the order in which thesamples have been analysed. This type of data valida-tion is advantageous if a set of results after batching ofspecimens is available.
Process control on the TV screenAll patients with result data for all tests requested areidentified by a yellow underlaid accession number inthe first column of the TV graph. This functions as anadditional marker for the technical staff to validateresults of completed tests. On the colour TV screen avalidated test result is symbolised by a change of thecolour code to green.
REPORTSThe data reporting mechanisms of an emergency
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from
A data processing system adapted to the special needs ofthe emergency laboratory
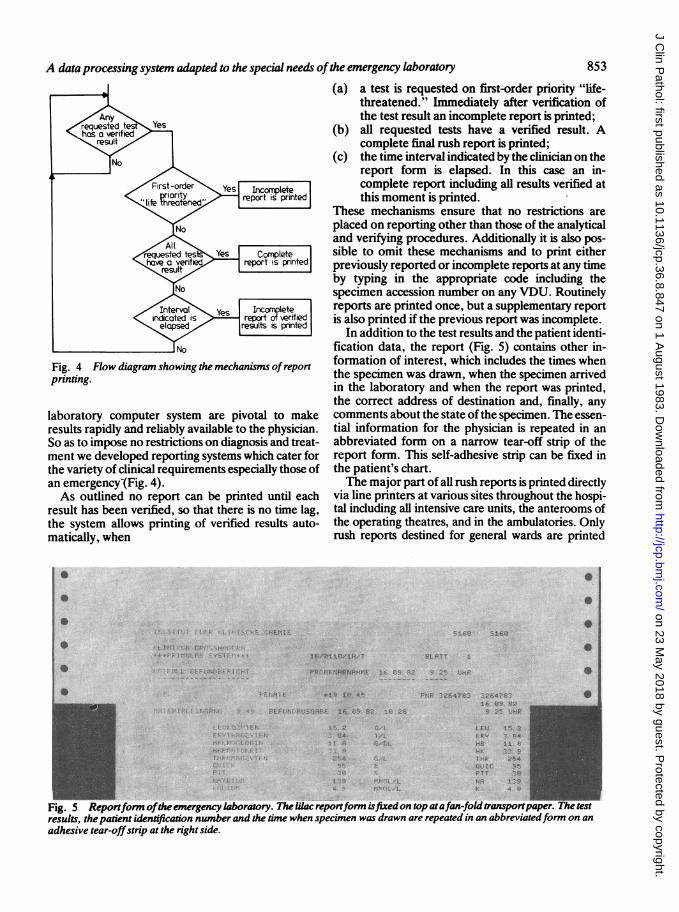
Fig. 4 Flow diagram showing the mechanisms ofreportprinting.
laboratory computer system are pivotal to makeresults rapidly and reliably available to the physician.So as to impose no restrictions on diagnosis and treat-ment we developed reporting systems which cater forthe variety of clinical requirements especially those ofan emergency (Fig. 4).As outlined no report can be printed until each
result has been verified, so that there is no time lag,the system allows printing of verified results auto-matically, when
(a) a test is requested on first-order priority "life-threatened." Immediately after verification ofthe test result an incomplete report is printed;
(b) all requested tests have a verified result. Acomplete final rush report is printed;
(c) the time interval indicated by the clinician on thereport form is elapsed. In this case an in-complete report including all results verified atthis moment is printed.
These mechanisms ensure that no restrictions areplaced on reporting other than those of the analyticaland verifying procedures. Additionally it is also pos-sible to omit these mechanisms and to print eitherpreviously reported or incomplete reports at any timeby typing in the appropriate code including thespecimen accession number on any VDU. Routinelyreports are printed once, but a supplementary reportis also printed if the previous report was incomplete.
In addition to the test results and the patient identi-fication data, the report (Fig. 5) contains other in-formation of interest, which includes the times whenthe specimen was drawn, when the specimen arrivedin the laboratory and when the report was printed,the correct address of destination and, finally, anycomments about the state of the specimen. The essen-tial information for the physician is repeated in anabbreviated form on a narrow tear-off strip of thereport form. This self-adhesive strip can be fixed inthe patient's chart.The major part of all rush reports is printed directly
via line printers at various sites throughout the hospi-tal including all intensive care units, the anterooms ofthe operating theatres, and in the ambulatories. Onlyrush reports destined for general wards are printed
*
* 0> i - 5 .1 3C, 31,< _ 69
0e s4, 4-4-- t .
t tL., !. -Z -, 'j I qr e I i iC/ 1 He'T R !. T' 1
FPTF9 3.ABNi +9h.Ft E : C9 -; j.:. 4tHP.
33913Al *19 Vl V~
31i~i 5q FF 6 . t ks .:,
1!'. 2
:.4
F-, 'e.- A, 4 7e_i.cn f.47P16. e.9 82
!R 2e- limP
LEIIERY
G, I..t
i,
15. 2Z 84
7- 94
*54
4 Ce
Fig. 5 Reportform ofthe emergency laboratory. The lilac reportform isfixedon top atafan-fold transportpaper. The testresults, the padent identification number and the time when specimen was drawn are repeated in an abbreviatedform on an
adhesive tear-offstrip at the right side.
0
853
$ t'. .. f. 1.". ':I t ;
,4 ." ,P
;-. , i. "
1 r. 1. .:
C.., ,-7. .,
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

854
within the laboratory and are despatched to the wardsvia a pneumatic tube system. When a printer on thewards breaks down, all corresponding printingoperations are performed in the laboratory until theprinter is in operation again. As a general principleresults previously not printed are never transmittedverbally because errors might be lethal and thereforeall rush reports are produced by direct machinetransfer.A 22 5 cm x 15 cm lilac paper sheet serves as report
form. These sheets are fixed only on top slightlyoverlapping on a 29- 15 cm wide fan-fold transportpaper. Single rush reports just printed can easily betorn off from the transport paper without handlingthe skipping device of the line printer, thus elimi-nating possible breakdowns caused by untrainedpersonnel on the wards. For security reasons a con-
densed replica of printed final reports is producedcontinuously within the laboratory.
Benefits ofthe system
The emergency laboratory computer system has beenin use for over two years. Except for occasional hard-ware problems affecting only parts of the system,there was no major breakdown. The laboratory stafffound it easy to use after a short training period. Thecodes used for program handling and verification ofresults are simple and easy to memorise. The systemhas changed the type of work in the emergency la-boratory considerably. The clerical tasks of enteringspecimen details into a reception book, transcribingresults on both the laboratory day-book and on reportforms, have all disappeared. The major benefit forthe staff lies in the continual awareness of the pro-cessing status of all specimens present.The actual workload is obvious at any time and the
greater control of work flow places less stress on theemergency laboratory. According to the indicateddelay times tests may be arranged in small batches.Further advantages result from the incorporation ofthe emergency laboratory in the central computersystem. For example, all test results, even the mostrecent ones, from all sections of the Institute areaccessible immediately and at any time.The response from the medical staff in the hospital
has been favourable. A major benefit for them is thereduction in the laboratory's turn-around time, whichis achieved by the reporting of results according to theindicated delay time (Fig. 6). In an emergency, theresults of test requested under this criterion arereported within 5-10 min after accession of thespecimen. Ninety-one per cent of tests with one hourdelay are reported within this interval. Thirty-fiveminutes after accession the final report of one half ofthese patients is printed or ready for despatch to the
Neumeier, Sator, Rindfleisch, Knedel
0 20 40 60 80 100 120 140(mriutes)
Fig. 6 Histograms ofprocessing intervals between theacceptance ofa specimen in the emergency laboratory andprint ofthefinal report. Above: indicated delay time"I hour" (n = 1583). For91% ofaUspecimens thefinalreport isprinted within the indicated delay time. After36mn50% ofallfinal reports areprinted. Below: indicated delaytime "2 hours" (n = 237). For allspecimensthefinalreport isprinted within the indicated delay time.
wards. Tests requested with two or more hours delayare always reported within the indicated interval.The time delay boxes on the request form, how-
ever, have created some problems for the laboratory
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from

A data processing system adapted to the special needs ofthe emergency laboratoryas the clinical unit's personnel sometimes lacksknowledge of how urgently a test result has to beavailable. Nearly two-thirds of all tests are requestedwith a one hour delay. It is in our own interest toreduce this percentage by continuous communicationwith the medical house-staff so there is best use of theemergency request forms. Another advantage fromthe user's point of view is the clear presentation ofresults, the better format of the printed reports andthe ease with which telephone enquiries aboutprevious results can be answered.Whether the basic concept of an emergency labora-
tory data processing system as described, is generallyapplicable to other hospitals may be debated. How-ever, the mechanisation of tests in the emergencylaboratory and computerised data handling, providebetter controlled reports more readily for the clini-cians and will improve care at the bedside of thecritically ill.
We would like to thank Dr Ch Pietrzyk for his helpduring the preparation of this paper and Miss SHoffmann and Mrs I Wolfium for typing this manu-script.
References
Henderson AR. The priority request form - A method forimproving communication between the physician and theEmergency Clinical Biochemistry Laboratory. J Clin Pathol1979;32:97-9.
2 Landon J, Sanders P, Peppiatt R, Clayton B, Jenkins P, CotgroveI. Emergency chemical pathology service in central London.Lancet 1971;ii:480-2.
Ferard PG, Klumpp T, Ragagnin M, Metzger G, Metais P.Description d'un systeme informatique dans un laboratoire
d'analyses biologiques d'urgence. J Clin Chem Clin Biochem1980;18:39-48.
4 Prellwitz W, Schuster HP, Suter P, Linderer Th, Schlichting K.Das Instrumentarium der Intensivstation - Stoffwechseluber-wachung (Basisprogramm, Lactatanalyse, Osmometrie,Onkometrie). Deutsch Med Wochenschr 1980;105:588-90.
Wiener K. Pathology measurements closer to the patient? J ClinPathol 1980;33:857-63.
6 Hannak D, Kattermann R. Notfall-Diagnostik - Notfall-LaborFolge 1: Kriterien des Notfall-Labors, Vorschlage fur ein inter-disziplinares Basisprogramm und fachbezogene Zusatz-programme. Fortschr Med 1981;99:57-61.Notfall-Diagnostik - Notfall-Labor Folge 2: Zuordnung desNotfall-Labors, Organisation, Methoden und Gerate. FortschrMed 1981;99:140-4.
Weil MH, Michaels S, Puri VK, Carlson RW. The Stat laboratory- facilitating blood gas and biochemical measurements for thecritically ill and injured. Am J Clin Pathol 1981;76:34-42.
8 Wiener F, Weil MH, Carlson RW. Computer systems for facili-tating management of the critically ill. Comput Biol Med 1982;12: 1-15.
Connely D, Steele B. Laboratory utilization - Problems andsolutions (Editorial). Arch Pathol Lab Med 1980;104:59-62.
Murphy JM, Penberthy LA, Fraser CG. The clinical view of turn-around times for stat tests. Am J Clin Pathol 1979;70:885.
Barnett RN, McIver DD, Gorton WL. The medical usefulnessof stat tests. Am J Clin Pathol 1978;69:520-4.
12 Knedel M. Datenverarbeitung im Klinisch-Chemischen Institutam Stadtischen Krankenhaus Munchen-Harlaching - EinSystem im Aufbau. Siemens Druckschrift NrMC 50/1016.
Knedel M, Neumeier D, Vogt W, eds. Datenverarbeitung in derKlinischen Chemie - 10 Jahre Erfahrungen. GIT-Verlag ErnstGiebler: Darmstadt, 1983.
14 Killian K. Verarbeitung von klinisch-chemischen MeBwerten inredundanten Systemen durch externe und interne Variation vonProgrammstruktur und Messvorgang. In: Wagner G, KohlerCO, eds. Interaktve Datenverarbeitung in der Medizin Stuttgart- New York: Schattauer-Verlag FK, 1976:178-87.
Requests for reprints to: Dr D Neumeier, Institut furKlinische Chemie, Klinikum BroBhadern, PO Box 701 260,D-8000 Munchen 70, GFR.
855
on 23 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.36.8.847 on 1 August 1983. D
ownloaded from


















