Darwin's illness and systemic lupus erythematosus
11
doi: 10.1098/rsnr.1997.0007 , 77-86 51 1997 Notes Rec. R. Soc. Lond. D.A.B Young Darwin's illness and systemic lupus erythematosus Email alerting service here right-hand corner of the article or click Receive free email alerts when new articles cite this article - sign up in the box at the top http://rsnr.royalsocietypublishing.org/subscriptions go to: Notes Rec. R. Soc. Lond. To subscribe to This journal is © 1997 The Royal Society rsnr.royalsocietypublishing.org Downloaded from
Transcript of Darwin's illness and systemic lupus erythematosus

doi: 10.1098/rsnr.1997.0007, 77-8651 1997 Notes Rec. R. Soc. Lond.
D.A.B Young Darwin's illness and systemic lupus erythematosus
Email alerting service hereright-hand corner of the article or click
Receive free email alerts when new articles cite this article - sign up in the box at the top
http://rsnr.royalsocietypublishing.org/subscriptions go to: Notes Rec. R. Soc. Lond.To subscribe to
This journal is © 1997 The Royal Society
rsnr.royalsocietypublishing.orgDownloaded from

DARWIN’S ILLNESS AND SYSTEMIC LUPUS ERYTHEMATOSUS
by
D.A.B. YOUNG
23 Hillcrest, Downham Market, Norfolk PE38 9ND, UK
INTRODUCTION
For most of his adult life Charles Darwin, F.R.S. (1809–1882) suffered from a chronicindisposition, the nature of which has remained a mystery. Until Colp’s exhaustiveaccount of the illness,1 the principal symptoms cited were palpitation, dyspepsia,headache, weakness and exhaustion.2 Such symptoms suggested to many apsychosomatic disorder,1–4 although this has not gone uncriticized.5–7 The only physicaldiagnosis to have received attention was Chagas’ disease,8 an infection to whichDarwin might have been exposed to in Argentina. However, since Woodruff’s effectiveintervention,9 that diagnosis finds little support; and today the psychogenic hypothesisholds the field. But how reliable is this presumption in the light of the much fullermedical information available in Colp’s review, much of it derived from unpublishedletters, which subsequently have been or are being published?10
The important impression gained from Colp’s account is the severity of the repeatedattacks Darwin endured for over 35 years. He knew he was truly ill, as did his family,friends and at least some of his doctors. The desperation of his efforts on manyoccasions to pursue his scientific work despite prostration makes nonsense of thesuggestion, for example, that he induced vomiting attacks merely to avoid going todinner parties.2
THE ILLNESS
Although there were significant episodes of indisposition before and during theBeagle voyage, his mature illness began in September 1837; the attacks worsened in1839 and improved only in June 1842. Further series of serious attacks occurred in1848–49, 1863–64 and in 1865. Moreover, in the intervals he was rarely free fromsymptoms, albeit of lesser intensity; thus we know from his Diary of Health, kept forthe years 1849–55, that he was well on only 40 per cent of the days.11
Gastric symptoms
The first symptom of illness in 1837 was palpitation, but by May 1838 gastricsymptoms had become the major problem and palpitation was mentioned only once
77
Notes Rec. R. Soc. Lond. 51 (1), 77–86 (1997) © 1997 The Royal Society
rsnr.royalsocietypublishing.orgDownloaded from

more, in December 1860. The gastric symptoms were nausea, retching, vomiting, andflatulence with associated pain. Vomiting occurred daily in the first half of 1840 andin the attacks of 1863–64 and 1865. The significant feature of the vomiting was itstiming with relation to eating. As Darwin told Hooker (in February 1864)1: ‘it rarelycomes on till 2–3 hours after eating, so that I seldom throw up food ... otherwise I shdhave been dead, for during more than a month I vomited after every meal & severaltimes most nights’. This is borne out by his not complaining of weight loss during thefour major periods of vomiting, and by his wife’s testimony (in December 1863) thatdespite frequent vomiting, sometimes ‘after every meal’, he lost ‘no flesh & [had] agood appetite’.1 The timing is in marked contrast to that of psychogenic vomiting,which usually occurs during or immediately after a meal,12 and it suggests a motilitydisorder of the stomach.
Problems with gastric flatulence first became significant in the attack of 1848–49.But even after that, Darwin’s Diary of Health shows that he had flatulence and painof varying duration and frequency on most days, and that they could be especially badat night. Significantly, as Colp has noted, the Diary records many exacerbations ofillness without any apparent cause.1 This contradicts a major argument for psychogeniccausation, viz. that Darwin’s symptoms were brought on only by emotionally chargedsituations.1,2
In the 1848–49 exacerbation of his illness Darwin complained of a group ofsymptoms often associated with psychogenic illness, as they are frequently theconsequence of neurotic hyperventilation: swimming of the head, trembling of thehands, involuntary muscle twitching, fainting sensations and visual disturbances (e.g.black spots). However, these are symptoms common also to all anaemias.13 There areclear indications that during this and other exacerbations of his illness Darwin wasanaemic. Thus he often became very tired by the evening. He would complain ofweakness and being unable to walk more than a short distance, yet only a few weekslater when his health had returned he could accomplish walks of several miles. Thesesymptoms suggest moderate anaemia of rapid onset and recovery. In 1864 he reportedthat iron phosphate was doing him a lot of good; and his prescription book lists an ironcitrate tonic favoured by his doctor, William Brinton.1
Cutaneous symptoms
Darwin’s illness was characterized by a considerable variety of signs and symptoms.The second major group of these involved the skin and its blood supply. Erythemafrequently accompanied the gastric attacks, but it was also a prominent sign at othertimes. Darwin, in his Diary of Health, also referred to it as ‘rash’, ‘eczema’ and‘eruption’. Hooker noted that, during his visits to Down House (1844–47), morningdiscussions would sometimes induce in Darwin ‘an attack of violent eczema in thehead during which he [CD] was hardly recognizable’.14 Darwin would be well by noon.Erythema had an invigorating effect, as Darwin told Hooker in March 1863 andEmma Darwin endorsed in 1864.1 Although he had attacks of eczema in the 1850s,it was only in the 1860s that Darwin spoke of ‘fits of eczema’, and the site and
D.A.B. Young78
rsnr.royalsocietypublishing.orgDownloaded from

Darwin’s illness and systemic lupus erythematosus 79
FIGURE 1. A photograph of Charles Darwin by Julia Margaret Cameronheld in the Royal Society.
rsnr.royalsocietypublishing.orgDownloaded from

severity of some of these may have been the reason for his growing a beard in 1864.Throughout middle-age Darwin had a ruddy complexion;1,15 and that, said his
daughter, ‘deceived many to believe his ill health to be more imaginary than real’.16
Darwin himself said (in 1849): ‘Everyone tells me I look quite blooming ... and mostthink I am shamming’.15 Significantly, his complexion was described as ‘yellow’during his recovery from a sudden, very bad attack in June 1868.17 In his sixties,however, he saw himself as sallow.1
In October 1859, Darwin developed simultaneously ‘a badly swollen whole leg’resembling ‘elephantiasis’ and a swollen face with ‘eyes almost closed up’ (i.e. anasarcaand angioneurotic oedema), ‘much rash’ and a frightful succession of boils (four or fiveat once). He felt ‘quite ill’, as if he was ‘living in Hell’. The boils were not a new problem;in his Diary of Health they were the most common complaint after flatulence. Theyoccurred in varying numbers and sizes, but nothing is known of their distribution orwhether in fact they truly were furuncles. What is certain is that the boils were a significantcomponent of Darwin’s constitutional disorder and do not fit with a psychogenic aetiology.In June 1862 he experienced a ‘violent skin inflammation’ with his ‘hands burning as ifdipped in hell-fire’, presumably erythromelalgia. It has been asserted that Darwin had gumproblems, and possibly pyorrhoea, as his son Leonard recalled. Darwin, summarizing hismedical condition (in 1865), said that his tongue was ulcerated.1
It may not have been noted before, but Darwin complained of symptoms ofRaynaud’s phenomenon. Thus, in 1843 he spoke to his father about the ‘dreadfulnumbness in my finger ends’ that had been troubling him.1 In 1849 he reports that afterhydropathy ‘my feet are certainly less cold than formerly’. In 1865 he still reports ‘feetcoldish’.1 For many years, he wore large, loose, cloth boots lined with fur over hishouse shoes when he was indoors.15
Rheumatism and respiratory symptoms
Darwin had ‘rheumatism’ and lumbago at various times; and significantly, he notesin the synopsis of his medical condition (in 1865): ‘Eczema, now without lumbago,fiendish rash’. Clearly, they were a subsidiary condition; but Darwin’s statement ‘Alldoctors seem to think that I am a case of suppressed gout’ suggests that, even if arthritiswas not a major problem, arthralgia was probably often present. The term ‘suppressedgout’ was used when, despite the presence of the systemic symptoms of the disease,the joint inflammation was imperfectly developed.
Darwin complained of having many colds, but he did not describe what he meantby them. They caused him concern because they could upset him generally andexacerbate his vomiting; e.g. ‘a cold ... suddenly turned into my old vomiting’; ‘coldsand rheumatism nearly all the time’; ‘fell ill again with cold ... threw me back a wholemonth’.1 Some colds recorded in his Diary of Health would cause headache,depression and vomiting; and one cold was accompanied by mild fever and chestpains.1 In March 1860, during a prolonged recurrence of his stomach trouble, Darwinhad an attack of fever with pleurisy that ‘shattered me a good bit’. In his Diary ofHealth there are complaints of breathing difficulties and coughing.1
D.A.B. Young80
rsnr.royalsocietypublishing.orgDownloaded from

Nervous disorders
Just before his marriage in 1839 Darwin suffered a bad headache, ‘which continuedtwo days and two nights’. In his Diary of Health ‘headaches’ are a frequent symptom,both day and night, and some were accompanied by ‘dazzle’ or ‘dazzling’.1 In 1860he wrote to Hooker: ‘I have been very poorly with almost continuous bad headachefor 48 hrs’. At the end of May 1863 he was in bed ill with ‘devilish headaches’, thestart of yet another period of serious vomiting. There was also a new symptom: ‘mynervous system failed’, probably his first transient loss of memory; and an epilepticfit was feared. Similar episodes occurred in late 1872 and again in the summer of 1873;in the latter there was ‘much loss of memory and severe shock’.
Early symptoms
Advocates of the psychogenic hypothesis may cavil at the absence so far of any referenceto Darwin’s ills before 1837, for it is known that even in his youth, nausea and sicknesswere easily induced by unpleasant news. But whereas much is made of his triflingcomplaint of palpitation before the Beagle sailed, little mention is made of the embarrassinglip eruption he endured for at least eight months (December 1828–August 1829), whichin the July was accompanied by malaise for a few days; and that two years later hecomplained of his ‘hands being not quite well’, a problem he had had more than once.18
In Brazil in 1832 Darwin, several days after he had ‘pricked his knee’, walked fornine hours in strong sunlight and intense heat. The next day acute inflammation of theknee and malaise developed, which lasted a week and then rapidly disappeared.19 Amonth later, he felt ‘feverish, shivering and sickness’ the day after a ten hour rideacross ‘scorching plains ... glaring hot ... 96 °[F]’. He was ill for two days beforeabruptly recovering.20 In October 1833 in northern Argentina he became ‘unwell &feverish from having exerted myself too much in the sun’ and was confined to bed(‘very unwell’) for two days.19,20 In 1834 in Chile, Darwin became ill and was treatedashore by the ship’s doctor with rest and calomel. The illness began with anorexia,nausea and vomiting, and marked fatigue; and presumably continued with fever,malaise and prostration. It was an illness his physician father was later quite unableto account for.19 He recovered after four weeks only to have a relapse. Altogether hisillness covered seven weeks; and for the next four months he complained of increasedstomach weakness, additional to seasickness, to which, like Nelson, he was a martyr.Darwin believed this fever had a permanent effect on his health.1
Last years
It has been claimed that Darwin’s symptoms improved in the last years of his life andthat this makes an organic aetiology unlikely. However, although his gastric troubleshad lessened, he ‘continued to have chronic and acute illness in the last decade of hislife’.1 Moreover, some organic diseases do improve after many years, e.g. chronicbrucellosis.21 Finally, in June 1881, Darwin developed angina and he died of ischaemicheart disease on 19 April 1882.
Darwin’s illness and systemic lupus erythematosus 81
rsnr.royalsocietypublishing.orgDownloaded from

DIAGNOSIS
So much for a description of Darwin’s illness; but what was its cause? The principleof economy of hypothesis in clinical diagnosis is particularly pertinent here, as thewide variety of symptoms were so inextricably mixed. Is there any diagnosis,therefore, that can account for all the symptoms taken together?
The clue to such a diagnosis could be an occasion in January 1834, when Darwinand some of the Beagle’s crew went for a trek ashore in Patagonia. It was hot andsunny; and two of the men collapsed. Nevertheless, Darwin was very active andwhen they returned to the ship at nightfall, he reported he felt ‘not much tired’.However, for the next two days he was in bed very feverish, whereas the rest of theparty had fully recovered.19 As noted earlier, similar episodes, albeit not as clear cut,had occurred before. Such acute responses to strong sunlight and a hot environmentare typical of subjects suffering from systemic lupus erythematosus.
SYSTEMIC LUPUS ERYTHEMATOSUS
Systemic lupus erythematosus (SLE)22,23 is a chronic inflammatory disease of unknowncause, which may affect the skin, joints, kidneys, nervous system, heart, lungs andother organs. It is characterized particularly by autoimmune phenomena, involvingantibodies to the patient’s own cells and cellular constituents, especially nuclearmaterial (DNA, RNA, etc.). Deposition of antibody or immune complexes results,principally, in vasculitis in tissues and haemolysis and altered white cell response inblood.
The classic example of a patient with SLE is a young woman with a malar erythema,fever, arthralgia, pleural effusion and nephritis who, before the introduction of steroidtherapy, would have had only months to live. However, most patients exhibit a lessacute form with multiple remissions and exacerbations in one or more systems. Theexpression of the disease depends on several factors: genetic make-up, an earlyinfection, a triggering factor (adolescence, sun exposure or infection) and variationin the host barrier to the disease. If the ‘barrier’ is fully or largely maintained, thedisease is limited to the skin and is expressed respectively as either transient orchronic-scarring discoid LE. If the barrier is largely or fully overcome, the systemicform results, subacute or acute respectively.22 SLE is preponderantly a disease of thefemale sex (9:1), the host barrier apparently being much more resistant in the male.Among diseases, SLE is second only to syphilis as the great imitator,22 and the rangeand forms of its signs and symptoms are so great that consideration will have to belimited to those aspects relevant to Darwin’s case.
D.A.B. Young82
rsnr.royalsocietypublishing.orgDownloaded from

DARWIN AND SLE
If we assume that Darwin suffered from SLE, his disparate symptoms conform to anordered case history. His disease was never life-threatening, because the criticalorgans in this regard were apparently either unaffected (heart and kidneys) or onlyslightly affected (brain and respiratory systems).
The dominant aspect of Darwin’s illness was the gastrointestinal manifestations.These are common among patients with SLE and usually indicate a relapse of theunderlying disease. For Darwin the abdominal pain was gastric in origin and associatedwith flatulence; the latter probably resulting from impaired oesophageal function,something found in 25 per cent of SLE patients.23 Oesophageal dysfunction isdefinitely correlated with Raynaud’s phenomenon.23 Today’s treatment of oesophagealsymptoms involves frequent small meals, the use of antacid and the avoidance ofpostprandial recumbency. Darwin’s gastric problems improved under medicalsupervision when Jenner prescribed antacids and again later when Bence Jonesstipulated frequent small meals. Unfortunately, Darwin was a devotee of postprandialrecumbency. This practice probably came from his stratagem to counter the onset ofseasickness on the Beagle by lying on the cabin table.
The cutaneous manifestations of SLE, which occur in most patients, run the entiregamut from erythema to bullous lesions,22 so Darwin could have been quite consistentin describing his skin affections as erythema, rash, eczema and eruption. The erythemais mainly on exposed areas; the facial blush, either transitory or relatively permanent,is the commonest form and may be accompanied by oedema. After the attack subsidesthere may be a residual hyperpigmentation. As a consequence, the patient will oftenhave either a ruddy or a tanned complexion. The hands are the next most affected sitefor lesions of all types; and erythromelalgia is not uncommon. It seems probable thatthe ‘boils’ that troubled Darwin so much were painful nodules situated deep in thedermis. They are frequently present in patients with SLE and are found on the hands,arms and feet.24 The lip eruption of Darwin’s youth may well have been discoidlupus. Discoid lesions anticipate SLE in 11 per cent of SLE cases,22 or occur duringthe course of SLE (29 per cent); the earlier presence of gastric symptoms mightfavour the latter view.
Moderate anaemia occurs in 57 per cent of cases and is haemolytic in origin.22 Insevere attacks haemolysis may be great enough to produce jaundice. Neurological andpsychiatric disturbances are common manifestations (25 per cent) and includeepileptiform fits (14 per cent),22 ischaemic episodes and memory loss. Depression oftenoccurs. This was a frequent complaint of Darwin and has been discerned in hiscondition by other authors.1 Sudden episodes of SLE, whether photo-induced or not,often take the form of feverish colds with myalgia and arthralgia. The last is typicallytransitory, lasting up to a few days. Darwin’s illness in Chile (35°S) in September 1834began a week after he climbed a mountain over 6000 feet high.19 In view of hisearlier photosensitivity, the consequent increased exposure to ultraviolet light,especially if snow cover was present, could have induced an acute attack of SLE.
Darwin’s illness and systemic lupus erythematosus 83
rsnr.royalsocietypublishing.orgDownloaded from

D.A.B. Young84
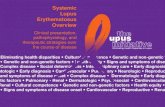
Table 1: Correspondence of Darwin’s symptoms with manifestations of systemic lupuserythematosus (SLE) and their frequency in patients.
Symptoms of Darwin’s illness Same symptoms in SLE patients22
Present Frequency(%)
A Gastrointestinal1 Anorexia ✓ 492 Nausea, retching and vomiting ✓ 533 Impaired oesophageal function
(cause of flatulence?) ✓ 25†
4 Gastric pain ✓ 19*
B Cutaneous ✓ 721 Facial erythema, etc.** ✓ 572 Facial and periorbital oedema ✓✓ 5, 53 Discoid lupus ✓ 294 Hyperpigmentation ✓ 85 Photosensitivity ✓ 336 Erythema, etc.** on the hands ✓ Common7 Cutaneous nodules (‘boils’) ✓
8 Anasarca, angioneuroticoedema and erythromelalgia ✓✓✓
9 Buccal lesions ✓ 9***
C Other1 Fever ✓ 842 Fatigue ✓ 81†
3 Raynaud’s phenomenon ✓ 184 Anaemia ✓ 575 Jaundice ✓ 46 Headache (migraine type) ✓(✓) 3 1† (15†)7 Temporary cerebral ischaemia,
memory loss and depression ✓✓✓
8 Pleurisy ✓ 459 Dyspnoea ✓
10 Arthralgia and myalgia ✓✓ 92, 48
* Abdominal pain.** Includes maculopapular lesions.*** Stomatitis, gingivitis and ulceration.† Per cent frequency, ref.23
rsnr.royalsocietypublishing.orgDownloaded from

Even from the limited information available (see table 1), the presence of threemajor manifestations (B1, 2; C3; C8), the possible significant presence of three others(B3; C5; C7) and the presence of six minor ones (A2, 4; B5; B7, 8; C1; C4; C10)would, according to the criteria of Dubois,22 make the diagnosis of SLE ‘probable’(two major and three minor), and perhaps ‘definite’ (three major and two minor).
Darwin attributed exacerbations of his illness to mental overwork. This wasparticularly exemplified by his ill health in 1863–64 when writing Variation ofAnimals and Plants under Domestication, a taxing assignment but not of contentiouscontent. Exacerbations of SLE would be expected from such overwork; and the valueof rest in both preventing and managing attacks of SLE is well attested to.22 Lastly,SLE has a familial occurrence,23 and two of Darwin’s children, George and Henrietta,showed pertinent symptoms.1
NOTES
1 R. Colp, To be an Invalid. The Illness of Charles Darwin. (University of Chicago Press,London, 1977).
2 G. Pickering, Creative Malady (Allen and Unwin, London, 1974).3 R. Good, Lancet 266, 106–107 (1954).4 D. Hubble, Lancet 244, 129–133 (1943); 265, 1351–1354 (1953).5 G. Himmelfarb, Darwin and the Darwinian Revolution. pp. 107–110 (Chatto and Windus,
London, 1959).6 L.A. Kohn, Bull. Hist. Med. 37, 239–256 (1963).7 P.B. Medawar, The Art of the Soluble. (Methuen, London, 1967). 8 S.W. Adler, Nature 184, 1102–1103 (1959).9 A.W. Woodruff, Br. med. J. 1, 745–750 (1965).10 The Correspondence of Charles Darwin, vols 1–7, 1821–59 (ed. F. Burkhardt and S. Smith);
vol. 8, 1860 (ed. F. Burkhardt, D.M. Porter, J. Browne and M. Richmond); vol. 9, 1861 (ed.F. Burkhardt, D.M. Porter, J. Harvey and M. Richmond) (Cambridge University Press,1985–94).
11 W.D. Foster, Bull. Hist. Med. 39, 476–478 (1965).12 M.H. Sleisenger, Vomiting. Cecil Textbook of Medicine, 16th edn (ed. J.B. Wyngaarden and
L.H. Smith), p. 601 (Saunders, Philadelphia, 1982).13 T.D. Savill, System of Clinical Medicine, 13th edn (ed. E.C. Warner), pp. 681–682 (Arnold,
London, 1950).14 J.D. Hooker, Nature 60, 187–188 (1899).15 F. Darwin, Life and Letters of Charles Darwin, chap. 3 (John Murray, London, 1887).16 H.E. Litchfield, Emma Darwin: A Century of Family Letters, vol. 2 (John Murray, London,
1915).17 W. Allingham, Diary, p. 184 (Centaur Press, Fontwell, 1967).18 ‘A skin eruption about Charles Darwin’s mouth and on his hands was a recurrent malady’,
ref. 10, vol. 1 (note 6, p. 75); also Susan Darwin (Shrewsbury, 22/7/1833) to her brother C.D.in South America: ‘I hope you keep quite well my dear Charles. Do your lips plague you now.’(ref. 10, vol. 1, p. 325).
Darwin’s illness and systemic lupus erythematosus 85
rsnr.royalsocietypublishing.orgDownloaded from

19 Charles Darwin’s Diary of the Voyage of HMS ‘Beagle’, ed. N. Barlow (CambridgeUniversity Press, 1933).
20 Charles Darwin and the Voyage of the ‘Beagle’, ed. N. Barlow (Pilot Press, London, 1945).21 D.A.B. Young, Br. med. J. 311, 1697–1700 (1995).22 E.L. Dubois, ed., Lupus Erythematosus, 2nd edn (McGraw-Hill, New York, 1966).23 Dubois’ Lupus Erythematosus, 4th edn, ed. D.J. Wallace and B.H. Hahn (Lea and Febiger,
Philadelphia, 1993).24 S.C. Gold and N.F.C. Gowling, Q. Jl Med. 22, 457–481 (1953).
D.A.B. Young86
rsnr.royalsocietypublishing.orgDownloaded from