DANISH trial (Cardiology)
32
Presenter Dr Praveen Gupta Moderator Dr Raja Selvaraj MD(Ped) DNB(Card) Fellowship in Cardiac EP(Toronto) Cardiac Electrophysiologist Associate Professor of Cardiology Jawaharlal Institute of Postgraduate Medical Education and Research Pondicherry | India 605006 Date 19/12/2016 1
-
Upload
praveen-gupta -
Category
Education
-
view
41 -
download
0
Transcript of DANISH trial (Cardiology)

1
Presenter Dr Praveen Gupta
Moderator Dr Raja Selvaraj
MD(Ped) DNB(Card) Fellowship in Cardiac EP(Toronto)
Cardiac Electrophysiologist
Associate Professor of Cardiology
Jawaharlal Institute of Postgraduate Medical Education and Research
Pondicherry | India 605006
Date 19/12/2016

2

3

4
• The trial was supported by unrestricted grants from Medtronic, St. Jude
Medical, TrygFonden, and the Danish Heart Foundation
• Kober disclosed relevant relationships with Sanofi and Novartis.
• McMurray disclosed relevant relationships with Cardiorentis, Amgen,
Novartis, Oxford University/Bayer, GlaxoSmithKline, Theracos, AbbVie,
AstraZeneca, Vifor-Fresnius Pharma, DalCor, Pfizer, Merck, and Bristol-
Myers Squibb.

5
Introduction
Background
ICD benefit well documented in ischemic heart diseases
No trial showed a significant effect of ICD with non-ischemic HF
Positive effect of ICD confined to New York Heart Association (NYHA) class II,
and no patients received concomitant CRT
Large proportion of these patients now receive CRT, and the impact of ICD
implantation in this setting is not well known
ICD implantation confers a risk of device-related complications

6
Introduction
Objective
DANISH study to investigate the effect of ICD implantation in patients with HF
and reduced ejection fraction not caused by coronary artery disease who receive
contemporary HF therapy including CRT
DANISH study will add insight into the rate of complications in a cohort where a
large proportion of patients will require implantation of multiple leads

7
Methods
Trial design
Multicenter
Randomized
Unblinded
Controlled
Parallel
2-group trial

8
Inclusion criteria
Clinical HF
Non-ischemic etiology
Optimal medical treatment
NYHA functional class II or III (patients in NYHA class IV could be
included if planned for CRT)
LVEF ≤35%
NT-proBNP N200 pg/mL (23.6 pmol/L)

9
Exclusion criteria
Dysregulated permanent atrial fibrillation (resting heart rate N100
beats/min)
Uncorrected congenital heart disease or valve obstruction
Obstructive cardiomyopathy, active myocarditis, constrictive pericarditis,
untreated hypothyroidism or hyperthyroidism, adrenal insufficiency, and
active vasculitis due to collagen vascular disease
On the urgent waiting list for a heart transplant (UNOS category 1A or 1B,
or equivalent)

10
Exclusion criteria (Contd)
Recipient of
Major organ transplant
Receiving or received cytotoxic or cytostatic chemotherapy and/or
radiation therapy for malignancy within 6 m before randomization or
clinical evidence of current malignancy, with the following exceptions:
basal or squamous cell carcinoma of the skin, cervical intraepithelial
neoplasia, prostate cancer (if stable localized disease, with a life
expectancy of N2.5 y in the opinion of the investigator)
Known to be HIV positive, with an expected survival of b5 y due to HIV
Renal failure treated with dialysis

11
Exclusion criteria (Contd)
Recent (within 3 m) history of alcohol or illicit drug abuse disorder, based
on self-report
Any condition (eg, psychiatric illness) or situation that, in the investigator's
opinion, could put the participant at significant risk, confound the study
results, or interfere significantly with the participant's participation in the
study
Lack of informed consent

12
Intervention
Randomization performed on web-based system, using permuted-block
Non-ischemic etiology was determined by coronary angiogram, although a
normal computed tomography angiogram or nuclear myocardial perfusion
imaging study was acceptable
Patients could be included despite having 1 or 2 coronary artery stenoses,
if the extent of coronary artery disease did not explain the reduced left
ventricular systolic function
Decision to implant a CRT device made before randomization
Single or dual chamber ICD was implanted

13
Methods (Contd.)
Follow-up –
2 months
Every 6 months
Patients who receive ICD undergo regular follow-up by implantation
center

14
Primary analysis
Time to death from any cause

15
Secondary outcomes
Time to sudden cardiac death
Time to cardiovascular death
Time to resuscitated cardiac arrest or sustained ventricular tachycardia
Change in quality of life from baseline (Quality of life is assessed by the
Minnesota Living with Heart Failure Questionnaire)

16
Statistical Analysis
Study designed to have 80% power to detect a 25% difference in total mortality between the
treatment groups.
At least 246 primary outcome events were required for the study to be conclusive, and we planned to
include 1000 patients.
Because the event rate and enrollment rate were lower than expected, the steering committee decided
to prolong enrollment until June 30, 2014, or until 1200 patients were included (whichever came first)
and to follow the last randomly assigned patient for at least 2 years.
Baseline characteristics compared between the groups with the use of chi-square and Wilcoxon tests
Outcomes analyzed with the use of time-to-event methods
Kaplan–Meier plots were calculated for total mortality, and cumulative incidence curves were
calculated for events with competing risk (sudden cardiac death and cardiovascular death)

17
Statistical Analysis
The analysis of the primary outcome was performed with a log-rank model
The proportional-hazard assumption was assessed with Schoenfeld residuals
Post hoc annual event rate ratios were derived from a Poisson regression
Prespecified subgroup analyses of the primary outcome were performed for the
variables
All analyses were performed in the intention-to-treat population
Two sided P values of 0.05 or less were considered to indicate statistical significance.
Analyses were performed with SAS software, version 9.4 (SAS Institute), and R
software, version 3.3.1 (R Project for Statistical Computing)

18

19
Result
From February 7, 2008, to June 30, 2014,
Total of 1116 patients were enrolled at five centers; 556 patients were
randomly assigned to the ICD group, and 560 patients were assigned to the
control group
Follow-up data for all outcomes were available through June 30, 2016
The median follow-up period was 67.6 months (interquartile range, 49 to
85), and no patients were lost to follow-up for the primary outcome

20
Cohort and baseline characteristics

21

22
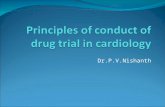
Result
• Primary outcome, death from
any cause, occurred in 120
patients (21.6%) in the ICD
group (4.4 events per 100
person-years) and in 131
patients (23.4%) in the
control group (5.0 events per
100 person-years)
• The hazard ratio for death
from any cause in the ICD
group, as compared with the
control group, was 0.87 (95%
confidence interval [CI] 0.68
to 1.12; P = 0.28)
Time-to-Event Curves for Death from Any Cause

23
Result
• Cardiovascular death
occurred in 77 patients
(13.8%) in the ICD
group and in 95
patients (17.0%) in the
control group (hazard
ratio, 0.77; 95% CI,
0.57 to 1.05; P = 0.10)
Time-to-Event Curves for Cardiovascular death

24
Result
Sudden cardiac
death occurred in 24
patients (4.3%) in
the ICD group and
in 46 patients
(8.2%) in the control
(hazard ratio, 0.50;
95% CI, 0.31 to
0.82; P = 0.005)
Time-to-Event Curves for Sudden Cardiac Death

25
Result
The clinical outcome of resuscitated
cardiac arrest or sustained ventricular
tachycardia occurred with similar
frequency in the two groups
Device infections in 4.9% in the ICD
and in 3.6% in the control (P = 0.29)
Patients not receiving CRT, the risk of
device infection was higher in the ICD
group than it was in the control group
(5.1% vs 0.8%) ( hazard ratio, 6.35;
95% CI, 1.38 to 58.87; P = 0.006).
Inappropriate shocks in 5.9% in the
ICD group

26
Result
With age there was a significant
treatment-by-subgroup
interaction (P = 0.009 )
The rate of death from any
cause was significantly lower
among patients younger than 68
years of age than among patients
68 years of age or older (hazard
ratio, 0.64; 95% CI, 0.45 to
0.90; = 0.01).
The effect of ICD implantation
was independent of CRT status
(P = 0.73 for the interaction)

27

28
Discussion
Implantation of an ICD in heart failure not caused by ischemic heart
disease did not provide an overall survival benefit, although the risk of
sudden cardiac death was halved with an ICD
No difference of ICD between patients with CRT and without CRT
Time-to-event curves diverge during initial 5 years and then converge
Rationale for long-term studies

29
Discussion
31% of deaths were due to noncardiovascular causes
Important interaction with age
Younger patients have a survival benefit with ICD
This is not surprising in an elderly population, but it highlights the
importance of selecting patients for ICD implantation carefully
Patients at higher risk more likely to benefit from ICD

30
Discussion
Lower likelihood of benefit in older patients might be used as an argument
for not implanting ICDs in frail patients
Long-term data from the Multicenter Automatic Defibrillator Implantation
Trial (MADIT) II indicate that clinical risk scores may make it possible to
identify the patients with ischemic heart disease who will benefit most
from ICD implantation
Such a method for identifying patients with nonischemic heart failure who
are at high risk for death from arrhythmia would be very useful

31
Discussion
The side effects associated with device implantation in our trial not trivial
Device related infections were not infrequent, but we did have a high
proportion of patients in both groups who were receiving CRT (which
requires implantation of an additional lead in the coronary sinus).
In addition, 10% of our patients already had a pacemaker and were
randomly assigned either to receive or not to receive an ICD upgrade; this
is a patient group that has not been included in most of the previous trials

32
Thank you