Cytogenetic follow-up by karyotyping and fluorescence in ... · with myelodysplastic syndrome and...
25
Cytogenetic follow-up by karyotyping and fluorescence in situ hybridization: implications for monitoring patients with myelodysplastic syndrome and deletion 5q treated with lenalidomide by Gudrun Göhring, Aristoteles Giagounidis, Guntram Büsche, Winfried Hofmann, Hans Heinrich Kreipe, Pierre Fenaux, Eva Hellström-Lindberg, and Brigitte Schlegelberger Haematologica 2010 [Epub ahead of print] Citation: by Göhring G, Giagounidis A, Büsche G, Hofmann W, Kreipe HH, Fenaux P, Hellström-Lindberg E, and Schlegelberger B. Cytogenetic follow-up by karyotyping and fluorescence in situ hybridization: implications for monitoring patients with myelodysplastic syndrome and deletion 5q treated with lenalidomide. Haematologica. 2010; 95:xxx doi:10.3324/haematol.2010.026658 Publisher's Disclaimer. E-publishing ahead of print is increasingly important for the rapid dissemination of science. Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts that have completed a regular peer review and have been accepted for publication. E-publishing of this PDF file has been approved by the authors. After having E-published Ahead of Print, manuscripts will then undergo technical and English editing, typesetting, proof correction and be presented for the authors' final approval; the final version of the manuscript will then appear in print on a regular issue of the journal. All legal disclaimers that apply to the journal also pertain to this production process. Haematologica (pISSN: 0390-6078, eISSN: 1592-8721, NLM ID: 0417435, www.haemato- logica.org) publishes peer-reviewed papers across all areas of experimental and clinical hematology. The journal is owned by the Ferrata Storti Foundation, a non-profit organiza- tion, and serves the scientific community with strict adherence to the principles of open access publishing (www.doaj.org). In addition, the journal makes every paper published immediately available in PubMed Central (PMC), the US National Institutes of Health (NIH) free digital archive of biomedical and life sciences journal literature. Official Organ of the European Hematology Association Published by the Ferrata Storti Foundation, Pavia, Italy www.haematologica.org Early Release Paper Support Haematologica and Open Access Publishing by becoming a member of the European Hematology Association (EHA) and enjoying the benefits of this membership, which include free participation in the online CME program Copyright 2010 Ferrata Storti Foundation. Published Ahead of Print on November 25, 2010, as doi:10.3324/haematol.2010.026658.
-
Upload
truongcong -
Category
Documents
-
view
224 -
download
4
Transcript of Cytogenetic follow-up by karyotyping and fluorescence in ... · with myelodysplastic syndrome and...

Cytogenetic follow-up by karyotyping and fluorescence in situ hybridization: implications for monitoring patients with myelodysplastic syndrome and deletion 5q treated with lenalidomide
by Gudrun Göhring, Aristoteles Giagounidis, Guntram Büsche, Winfried Hofmann,Hans Heinrich Kreipe, Pierre Fenaux, Eva Hellström-Lindberg,and Brigitte Schlegelberger
Haematologica 2010 [Epub ahead of print]
Citation: by Göhring G, Giagounidis A, Büsche G, Hofmann W, Kreipe HH, Fenaux P,Hellström-Lindberg E, and Schlegelberger B. Cytogenetic follow-up by karyotyping and fluorescence in situ hybridization: implications for monitoring patients with myelodysplastic syndrome and deletion 5q treated with lenalidomide. Haematologica. 2010; 95:xxx doi:10.3324/haematol.2010.026658
Publisher's Disclaimer. E-publishing ahead of print is increasingly important for the rapid dissemination of science.Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts thathave completed a regular peer review and have been accepted for publication. E-publishingof this PDF file has been approved by the authors. After having E-published Ahead of Print,manuscripts will then undergo technical and English editing, typesetting, proof correction andbe presented for the authors' final approval; the final version of the manuscript will thenappear in print on a regular issue of the journal. All legal disclaimers that apply to the journal also pertain to this production process.
Haematologica (pISSN: 0390-6078, eISSN: 1592-8721, NLM ID: 0417435, www.haemato-logica.org) publishes peer-reviewed papers across all areas of experimental and clinicalhematology. The journal is owned by the Ferrata Storti Foundation, a non-profit organiza-tion, and serves the scientific community with strict adherence to the principles of openaccess publishing (www.doaj.org). In addition, the journal makes every paper publishedimmediately available in PubMed Central (PMC), the US National Institutes of Health (NIH)free digital archive of biomedical and life sciences journal literature.
Official Organ of the European Hematology AssociationPublished by the Ferrata Storti Foundation, Pavia, Italy
www.haematologica.org
Early Release Paper
Support Haematologica and Open Access Publishing by becoming a member of the European Hematology Association (EHA)and enjoying the benefits of this membership, which include free participation in the online CME program
Copyright 2010 Ferrata Storti Foundation.Published Ahead of Print on November 25, 2010, as doi:10.3324/haematol.2010.026658.

Cytogenetic follow-up by karyotyping and fluorescence in situ hybridization:
implications for monitoring patients with myelodysplastic syndrome and
deletion 5q treated with lenalidomide
Gudrun Göhring,1 Aristoteles Giagounidis,2 Guntram Büsche,3 Winfried Hofmann,1
Hans Heinrich Kreipe,3 Pierre Fenaux,4 Eva Hellström-Lindberg,5
and Brigitte Schlegelberger1
1Institute of Cell and Molecular Pathology, Hannover Medical School, Germany; 2Department of Haematology, Oncology and Clinical Immunology, Johannes
Hospital, Duisburg, Germany; 3Institute of Pathology, Hannover Medical School,
Germany; 4Service d'Hématologie Clinique, Hôpital Avicenne, Assistance Publique
Hôpitaux de Paris, Paris, Bobigny, France; and 5Division of Haematology and Centre
of Experimental Haematology, Department of Medicine, Karolinska Institutet,
Karolinska University Hospital, Stockholm, Sweden
Correspondence Gudrun Göhring, Institute of Cell and Molecular Pathology, Hannover Medical
School, Carl-Neuberg-Str. 1, 30625 Hannover, Germany.
Phone: international +49.511.5324517. Fax: international +49.511.5324521.
E-Mail: [email protected]
Acknowledgments The authors would like to thank Gillian Teicke for her help in preparing the manuscript, Michael Morgan for critically reading the manuscript and Aspasia Stamatoullas, Odile Beyne-Rauzy, Ghulam Mufti, Petra Muus, Lars Nilsson, Guillermo F. Sanz and Dominik Selleslag for the recruitment of patients. Finally, we thank Dr. Robert Knight and Dr. Jay Backström, Celgene, for allowing us to use data obtained within the Celgene MDS-003 and MDS-004 clinical trials. Funding Supported by COST Action BM0801 (EuGESMA) and the Excellence cluster Rebirth.
DOI: 10.3324/haematol.2010.026658

Abstract
In patients with low and intermediate risk myelodysplastic syndrome and deletion 5q
(del(5q)) treated with lenalidomide, monitoring of cytogenetic response is mandatory,
since patients without cytogenetic response have a significantly increased risk of
progression. Therefore, we have reviewed cytogenetic data of 302 patients.
Patients were analyzed by karyotyping and fluorescence in situ hybridization.
In 85 patients, del(5q) was only detected by karyotyping. In 8 patients undergoing
karyotypic evolution, the del(5q) and additional chromosomal aberrations were only
detected by karyotyping. In 3 patients, del(5q) was only detected by fluorescence in
situ hybridization, but not by karyotyping due to a low number of metaphases.
Karyotyping was significantly more sensitive than fluorescence in situ hybridization in
detecting the del(5q) clone. In conclusion, to optimize therapy control of
myelodysplastic syndrome patients with del(5q) treated with lenalidomide and to
identify cytogenetic non-response or progression as early as possible, fluorescence
in situ hybridization alone is inadequate for evaluation. Karyotyping must be
performed to optimally evaluate response.
(clinicaltrials.gov identifier: NCT01099267 and NCT00179621)
DOI: 10.3324/haematol.2010.026658

Introduction
Myelodysplastic syndrome (MDS) associated with isolated del(5q) is a distinct entity
with a risk of evolution into acute myeloid leukemia (AML) of approximately 10% (1-
2). It is characterized by anemia with or without other cytopenias and/or
thrombocytosis. Myeloblasts comprise <5% of bone marrow and <1% of peripheral
blood (1). Lenalidomide is particularly active in MDS patients with del(5q), with over
two-thirds of low and intermediate risk MDS patients with 5q deletions achieving
transfusion independence (3). In this cohort with an a priori increased risk, about one
third of the patients underwent clonal evolution and AML progression (4-5). Patients
without hematologic or cytogenetic response had a significantly increased risk of
progression (5). Therefore, careful monitoring of the cytogenetic response may add
important prognostic information in MDS patients treated with lenalidomide.
Gold standard for the detection of aberrations is karyotyping (6-8). Aberrations are
detected in about half of MDS patients (9). Additional fluorescence in situ
hybridization (FISH) analyses are recommended to detect deletions 5q, 7q, 17p or
20q, monosomy 7 and trisomy 8 (6). Recently, it was suggested that FISH should be
performed in cases of a suspected ‘5q- syndrome’ and/or if karyotyping shows no
metaphases or an aberrant karyotype involving chromosome 5 (10).
In order to optimize therapeutic control of MDS patients treated with lenalidomide, we
have evaluated the cytogenetic data of 302 del(5q) patients treated with lenalidomide
and compared the results obtained by karyotyping and FISH.
Design and Methods
Patients
Our cohort included 302 patients with transfusion-dependent anemia due to low- or
intermediate-1-risk myelodysplastic syndrome (according to the International
DOI: 10.3324/haematol.2010.026658

Prognostic Scoring System (IPSS)) associated with a 5q deletion with or without
additional cytogenetic abnormalities. This cohort includes all European patients
enrolled in the CC-5013-MDS-003 (ClinicalTrials.gov Identifier: NCT01099267) and
all patients enrolled in the CC-5013-MDS-004 study (ClinicalTrials.gov Identifier:
NCT00179621) for MDS patients with del(5q) treated with lenalidomide. Cytological
and morphological diagnoses were made centrally at St. Johannes Hospital Duisburg
and Hannover Medical School. Patients were enrolled in the studies MDS-003 (n=42)
or MDS-004 (n=260) and treated with lenalidomide (starting dose, 10mg daily)
according to the study protocols (3). Written informed consent was provided
according to the Declaration of Helsinki and approval from the Ethics Committee of
Hannover Medical School (MHH) was obtained.
Lenalidomide therapy is still ongoing in responding patients. Dose adjustments were
performed in the majority of patients due to side effects such as neutropenia.
Regular follow-up investigations were performed every 6 months of treatment or
more frequently, depending upon clinical features. As many as 11 cytogenetic
analyses were performed for each patient. In total, we reviewed 1075 cytogenetic
analyses.
Standardized cytogenetic investigations: Karyotyping and FISH
Bone marrow was received from European study centers for central cytogenetic
review. Karyotyping was performed according to standard procedures (11).
Whenever possible, 25 metaphases were analyzed. Description of the karyotype, the
chromosomal aberrations, followed the recommendations of the International System
for Cytogenetic Nomenclature (12). In all patients, an interstitial del(5q) containing the
commonly deleted region 5q31 was present (Figure 1A-C). Fluorescence in situ
hybridization (FISH) for del(5q) was included in each investigation (probes supplied
by Abbott, Wiesbaden, Germany). FISH was performed on fixed cells from the
DOI: 10.3324/haematol.2010.026658

cytogenetic culture according to standard procedures (Figure 1D-F) (11). For each
FISH analysis, at least two hundred interphase nuclei were analyzed. In agreement
with the literature, mean cut-off levels were determined to be 8% (+/- 3SD) by
analysis of at least 1000 cells from 10 healthy donors (10).
Cytogenetic response
Cytogenetic response was applied to karyotyping only. Complete cytogenetic
response (CCyR) was defined as disappearance of the 5q deletion or any other
chromosomal aberration. Partial cytogenetic response (PCyR) was defined as a
reduction of aberrant metaphases of more than 50% compared to the previous
karyotyping (3). Cytogenetic relapse was defined as reappearance of a metaphase
with a deletion in 5q after reaching a complete cytogenetic response.
Statistical analyses
Analysis of del(5q) detection rates in metaphases and interphases was done by
Wilcoxon test (13). Values of p<0.05 were considered statistically significant.
Results and Discussion
We compare the sensitivity of detecting the del(5q) clone by karyotyping and FISH,
respectively, in a large cohort of MDS patients treated with lenalidomide (n=302). A
complete cytogenetic investigation based on at least 25 metaphases and FISH based
on the analyses of at least 200 interphase nuclei was performed in 835 (78%) of the
investigations. Here, we focus on discrepant results of karyotyping and FISH that
would have led to a different judgement of whether the patient is eligible for treatment
with lenalidomide, or to a different diagnosis of cytogenetic remission, relapse or
progression during follow-up.
DOI: 10.3324/haematol.2010.026658

Detection of del(5q) at study entry before treatment with lenalidomide
Twelve of 302 patients (4%) (patients 1-10, 23 and 86) showed discrepant
karyotyping and FISH results already in the first cytogenetic investigation at study
entry (Table 1). In patients 1-10, del(5q) was not detected by FISH but only by
karyotyping. In 5 of these 10 patients less than 10% of the metaphases showed a
deletion in 5q at study entry. In contrast, a deletion in 5q was detected in 72% and
100% of the metaphases in two of those patients (patients 6 and 10) (Supplement 1).
In patients 23 and 86, del(5q) was detected by FISH only. The del(5q) was detected
in 21% and 32% of the interphase nuclei, respectively. However, in both
investigations, less than 10 metaphases could be analyzed. 17 patients showed one
additional aberration and 12 patients an independent clone, e.g. +8 or t(2;11).
Follow-up after 6 months of treatment
Six months after treatment with lenalidomide, in 27 of 232 patients (12%) del(5q) was
detected only by karyotyping and not by FISH. In two of these patients, a clonal
evolution occurred. Neither the clonal evolution nor the del(5q) clone would have
been detected if only FISH had been used. At this time point, in no case was del(5q)
detected by FISH only (Table 1, Supplement 2).
Follow-up after 12 months of treatment
After 12 months of treatment, in 39 of 169 patients (23%) del(5q) was detected only
by karyotyping. In one patient, del(5q) was detected only by FISH. In three patients, a
clonal evolution occurred. In 6 patients, a cytogenetic relapse occurred at this time
point. This relapse would not have been detected if only FISH had been used (Table
1).
Third and later follow-up investigations after 18 months and later of treatment
In 85 of 267 patients (32%), a discrepancy was detected after at least 18 months of
treatment. In only one patient was del(5q) detected by FISH only. In the other cases,
DOI: 10.3324/haematol.2010.026658

del(5q) was detected by karyotyping only and not by FISH. In 31 of these patients, a
cytogenetic relapse occurred and would not have been detected if only FISH had
been used. In five of them, a progress with a clonal evolution was identified by
karyotyping. Neither the clonal evolution nor the del(5q) clone would have been
detected if only FISH had been used (Table 2). There was no difference regarding
the detection of the del(5q) comparing patients with a discrepancy at the first time
point of analysis and others.
Detection of a complete cytogenetic response
24 of 163 patients (15%) with a discrepancy between karyotyping and FISH reached
a CCyR. Eleven patients reached CCyR after 6 months of treatment with
lenalidomide. Three patients reached CCyR after 12 months, 9 patients after 18 and
one patient after 24 months (median of 15 months). Nine of these 24 patients (37%)
reached a partial response and 15 patients (63%) did not reach a partial response
beforehand. The partial response occurred once after 6 months, 7 times after 12
months and once after 18 months of treatment. Patient 35, for example, showed a
CCyR after 12 months without reaching a partial remission beforehand (Supplement
2). On the other hand, patient 15 reached a partial remission after 6 and a CCyR
after 12 months of treatment (Supplement 1).
In 19 of 302 patients (6%), independent clones were detected by karyotyping. The
independent clones contained trisomy 8 in 12 patients, loss of the Y chromosome in
4 patients, monosomy 7 in 3 patients, del(20q) in 2 patients, and del(11q), trisomy 14
and der(1;7) in one patient each. In four of these patients, two or three independent
clones were found. In 8 of 16 patients undergoing a karyotypic evolution, at 17 time
points, neither the del(5q) nor the additional chromosomal aberrations were detected
by FISH – in contrast to karyotyping. In patients 34, 35 and 36, karyotypic evolution
occurred after they had reached a complete cytogenetic response.
DOI: 10.3324/haematol.2010.026658

Clinical consequences
This study has three major implications for monitoring MDS patients with del(5q)
treated by lenalidomide. Firstly, the del(5q) clone was detected significantly more
sensitively by karyotyping than by FISH, thus making the diagnosis of non-remission
and cytogenetic relapse possible only by karyotyping in a significant number of
patients. Secondly, without prior knowledge of the additional chromosome
aberrations, clonal evolution can be identified only by karyotyping. At the time point of
clonal evolution, even del(5q) was detected only by karyotyping in a significant
number of patients. Thirdly, detection of the del(5q) clone was sometimes only
possible by FISH, making the diagnosis of non-remission and cytogenetic relapse in
these patients only possible by FISH analysis. Thus, all cytogenetic follow-up
investigations must include karyotyping. An additional FISH analysis should at least
be performed, if karyotyping does not give sufficient results, e.g. due to poor
chromosome morphology or due to a low number of metaphases (< 25 metaphases).
Karyotyping was significantly more sensitive than FISH for detection of del(5q)
(p<2.2e-16). This was true for the time point of study entry as well as during follow-
up. In contrast, a deletion in 5q was only detected by FISH in three patients. In these
cases, less than 10 metaphases were available for analysis. As recommended by the
European LeukemiaNet, at least 25 metaphases are necessary for a reliable
karyotyping (6). In the literature, several studies described discrepant results of
karyotype and FISH analyses (10,14-17). In most instances, the cases with a
discrepant result (positive by FISH only) had an insufficient number of metaphases or
the chromosome morphology was poor. Pitchford et al. recommended FISH in MDS
patients only if an adequate karyotyping with at least 20 metaphases was not
possible, since they were unable to demonstrate a benefit of FISH in the setting of an
optimal banding analysis (7). FISH is a valuable method to quantify the clone size
DOI: 10.3324/haematol.2010.026658

with cytogenetic aberrations known from diagnosis. It may be discussed whether it is
sufficient only to perform FISH during follow-up analyses. FISH may be used to
monitor for the presence of a specific chromosomal abnormality that was present
before treatment (18). Obviously, this approach has positive aspects, such as being
cost- and time-effective as no culturing is needed since only interphase nuclei are
analyzed. However, our findings question the proposal that FISH analysis alone is
sufficient for follow-up analysis. Using this approach in our study, cytogenetic non-
response or relapse and even clonal evolution would not have been detected in a
significant number of patients.
One reason for the higher sensitivity of karyotyping in detecting the del(5q) clone
might be that a small clone with proliferative advantage over normal cells may be
more easily identified by karyotyping than by FISH. FISH is a quantitative method
counting interphase nuclei with a normal signal constellation and with a signal
constellation indicative of a del(5q). A small clone with a del(5q) might be missed if it
is below the cut-off level for the detection of a deletion, which is typically between 3
and 10 % and was 8% in our study (7,9,19). In contrast, karyotyping is based on
metaphases, i.e. cells undergoing spontaneous cell division in vitro. Therefore, the
amount of metaphases with a del(5q) identified by karyotyping does not necessarily
represent the proportion of these cells within the bone marrow. To monitor
cytogenetic response in chronic myeloid leukemia (CML), Fugazza et al. did not find
an advantage of karyotyping or FISH. As in our study, one or the other method was
superior in some patients (20). In contrast, the GIMENA group recently showed that
FISH is more sensitive than banding analysis in CML and should be used for
monitoring (21). However, due to the FISH probe designed to detect the Philadelphia
translocation, the cut-off level was below 1%.
DOI: 10.3324/haematol.2010.026658

A very important advantage of karyotyping is the possibility to identify additional
aberrations. Only previously selected loci can be analyzed by FISH. Moreover, an
additional multicolor FISH can be applied to detect cryptic aberrations not seen by
karyotyping. In our study, clonal evolution was identified in 8 patients. In most
patients, clonal evolution was associated with leukemic progression as described
before (5,22,23). In these patients, chromosomal instability leading to clonal evolution
seems to be the driving force behind the expansion of tumor cell populations (24).
In conclusion, to optimize monitoring of MDS patients with del(5q) treated with
lenalidomide and to detect cytogenetic non-response, cytogenetic relapse or clonal
evolution as early as possible, FISH alone is inadequate for evaluation. Karyotyping
must be performed to optimally evaluate response.
Authorship and Disclosures
GG and BS were the principal investigators and take primary responsibility for the
paper. AG, PF and EHL recruited the patients. GG, GB, and HHK performed the
laboratory work for this study. WH participated in the statistical analysis. GG and BS
wrote the paper. The authors reported no potential conflicts of interest.
DOI: 10.3324/haematol.2010.026658

References
1. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Fourth
Edition. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J,
Vardiman JW (Eds). IARC, Lyon 2008.
2. Giagounidis AA, Germing U, Haase S, Hildebrandt B, Schlegelberger B, Schoch
C, et al. Clinical, morphological, cytogenetic, and prognostic features of patients
with myelodysplastic syndromes and del(5q) including band q31. Leukemia. 2004;
18(1):113-9.
3. List A, Dewald G, Bennett J, Giagounidis A, Raza A, Feldman E, et al.
Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N
Engl J Med. 2006; 355(14):1456-65.
4. Malcovati L, Germing U, Kuendgen A, Della Porta MG, Pascutto C, Invernizzi R,
et al. Time-dependent prognostic scoring system for predicting survival and
leukemic evolution in myelodysplastic syndromes. J Clin Oncol. 2007;
25(23):3503-10.
5. Göhring G, Giagounidis A, Büsche G, Kreipe H, Zimmermann M, Hellström-
Lindberg E, et al. Patients with del(5q) MDS who fail to achieve sustained
erythroid or cytogenetic remission after treatment with lenalidomide have an
increased risk for clonal evolution and AML progression. Ann Hematol. 2010;
89(4):365-74.
6. Haferlach C, Rieder H, Lillington DM, Dastugue N, Hagemeijer A, Harbott J, et al.
Proposals for standardized protocols for cytogenetic analyses of acute leukemias,
chronic lymphocytic leukemia, chronic myeloid leukemia, chronic
myeloproliferative disorders, and myelodysplastic syndromes. Genes
Chromosomes Cancer. 2007; 46(5):494-9.
DOI: 10.3324/haematol.2010.026658

7. Pitchford CW, Hettinga AC, Reichard KK. Fluorescence in situ hybridization
testing for -5/5q, -7/7q, +8, and del(20q) in primary myelodysplastic syndrome
correlates with conventional cytogenetics in the setting of an adequate study. Am
J Clin Pathol. 2010; 133(2):260-4.
8. Slovak ML, Dewald GW. International Working Group on MDS cytogenetics:
October 2007 meeting report. Leuk Res. 2008; 32(9):1329-32.
9. Haase D, Germing U, Schanz J, Pfeilstocker M, Nosslinger T, Hildebrandt B, et al.
New insights into the prognostic impact of the karyotype in MDS and correlation
with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;
110(13):4385-95.
10. Mallo M, Arenillas L, Espinet B, Salido M, Hernández JM, Lumbreras E, et al.
Fluorescence in situ hybridization improves the detection of 5q31 deletion in
myelodysplastic syndromes without cytogenetic evidence of 5q-. Haematologica.
2008; 93(7):1001-8.
11. Göhring G, Hanke C, Kratz C, Kontny U, Steinemann D, Niemeyer C, et al.
Fluorescence in situ hybridization using the subtelomeric 11q probe as a
diagnostic tool for congenital thrombocytopenia. Ann Hematol. 2006; 85(12):883-
5.
12. ISCN (1995): Guidelines for cancer cytogenetics, supplement to an international
system for human cytogenetic nomenclature. Mitelman F (Ed). S. Karger, Basel,
Switzerland 1995.
13. Team RDC. R: A language and environment for statistical computing [Internet].
Vienna, Austria: 2009. Available from: http://www.R-project.org
14. Cherry AM, Brockman SR, Paternoster SF, Hicks GA, Neuberg D, Higgins RR, et
al. Comparison of interphase FISH and metaphase cytogenetics to study
myelodysplastic syndrome: an Eastern Cooperative Oncology Group (ECOG)
DOI: 10.3324/haematol.2010.026658

study. Leuk Res. 2003; 27(12):1085-90.
15. Bernasconi P, Cavigliano PM, Boni M, Calatroni S, Klersy C, Giardini I, et al. Is
FISH a relevant prognostic tool in myelodysplastic syndromes with a normal
chromosome pattern on conventional cytogenetics? A study on 57 patients.
Leukemia. 2003; 17(11):2107-12.
16. Beyer V, Castagné C, Mühlematter D, Parlier V, Gmür J, Hess U, et al.
Systematic screening at diagnosis of -5/del(5)(q31), -7, or chromosome 8
aneuploidy by interphase fluorescence in situ hybridization in 110 acute
myelocytic leukemia and high-risk myelodysplastic syndrome patients:
concordances and discrepancies with conventional cytogenetics. Cancer Genet
Cytogenet. 2004; 152(1):29-41.
17. Yilmaz Z, Sahin FI, Kizilkilic E, Karakus S, Boga C, Ozdogu H. Conventional and
molecular cytogenetic findings of myelodysplastic syndrome patients. Clin Exp
Med. 2005; 5(2):55-9.
18. Olney HJ, Le Beau MM. Evaluation of recurring cytogenetic abnormalities in the
treatment of myelodysplastic syndromes. Leuk Res. 2007; 31(4):427-34.
19. Ketterling RP, Wyatt WA, VanWier SA, Law M, Hodnefield JM, Hanson CA, et al.
Primary myelodysplastic syndrome with normal cytogenetics: utility of 'FISH panel
testing' and M-FISH. Leuk Res. 2002; 26(3):235-40.
20. Fugazza G, Miglino M, Bruzzone R, Quintino S, Gatti AM, Grasso R, et al.
Cytogenetic and fluorescence in situ hybridization monitoring in Ph+ chronic
myeloid leukemia patients treated with imatinib mesylate. J Exp Clin Cancer Res.
2004; 23(2):295-9.
21. Testoni N, Marzocchi G, Luatti S, Amabile M, Baldazzi C, Stacchini M, et al.
Chronic myeloid leukemia: a prospective comparison of interphase fluorescence
in situ hybridization and chromosome banding analysis for the definition of
DOI: 10.3324/haematol.2010.026658

complete cytogenetic response: a study of the GIMEMA CML WP. Blood. 2009;
114(24):4939-43.
22. Duell T, Poleck-Dehlin B, Schmid C, Wunderlich B, Ledderose G, Mittermuller J,
et al. Clonal karyotype evolution involving ring chromosome 1 with
myelodysplastic syndrome subtype RAEB-t progressing into acute leukemia. Acta
Haematol. 2006; 116(2):131-6.
23. Wang H, Wang X, Xu X, Lin G. Cytogenetic evolution correlates with poor
prognosis in myelodysplastic syndrome. Cancer Genet Cytogenet. 2010;
196(2):159-66.
24. Gao C, Furge K, Koeman J, Dykema K, Su Y, Cutler ML, et al. Chromosome
instability, chromosome transcriptome, and clonal evolution of tumor cell
populations. Proc Natl Acad Sci U S A. 2007; 104(21):8995-9000.
DOI: 10.3324/haematol.2010.026658

Table 1. Discrepancy in detecting del(5q) by karyotyping and FISH in patients with MDS and del(5q) at study entry before treatment with lenalidomide (time point 0) and after 6 and 12 months of treatment (time point 1 and 2).
Time point Patient No FAB ISCN-Karyotyp ISCN FISH % MP 5q- % IP 5q- Response*0 1 RARS 46,XY,del(5)(q?14q34)[1]/46,XY[24] 5q31(EGR1x2) 4 1 n.e.0 2 RA 46,XX,del(5)(q22q34)[4]/46,XX[21] 5q31(EGR1x2) 16 3 n.e.0 3 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 4 n.e.0 4 RA 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 6 n.e.0 5 punctio sicca 47,XX,+8[4]/45,XX,del(5)(q1?q34),-7[3]/46,XX[48] 5q31(EGR1x2) 5 4 n.e.0 6 punctio sicca 46,XX,del(5)(q13q34)[1]/46,idem,add(20)(q13)[2] 5q31(EGR1x2) 100 2 n.e.0 7 RA 46,XX,del(5)(q23q34)[4]/46,XX[7] 5q31(EGR1x2) 36 6 n.e.0 8 RARS 46,XY,del(5)(q?21q?34)[2]/46,XY[23] 5q31(EGR1x2) 8 5 n.e.0 9 RA 46,XY,del(5)(q21q34)[1]/46,XY[24] 5q31(EGR1x2) 4 6 n.e.0 10 RA 46,XY,del(5)(q14q34),inv(11)(p13 p14q22 q23)[18]/46,XY[7] 5q31(EGR1x2) 72 0 n.e.0 23 RAEB 46,XX[2] 5q31(EGR1x1) 0 21 n.e.0 86 punctio sicca 46,XX[3] 5q31(EGR1x1) 0 32 n.e.1 8 RARS 46,XY,del(5)(q21q34)[1]/46,XY[19] 5q31(EGR1x2) 5 4 no CyR1 11 RA 46,XY,del(5)(q21q34)[3]/46,XY[22] 5q31(EGR1x2) 12 4 no CyR1 12 RA 46,XX,t(X;16)(p11;q23),del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 4 no CyR1 14 RA 46,XX,del(5)(q21q34)[2]/46,XX[23] 5q31(EGR1x2) 8 5 no CyR1 15 RARS 46,XX,del(5)(q14q34)[1]/46,XX[19] 5q31(EGR1x2) 5 0 no CyR
1 30 RA47,XX,+8[7]/46,XX,del(20)(q12q13)[4]/46,XX,del(5)(q14q34)[2]/ 46,XX,del(5)(q14q34),del(20)(q12q13)[1]/46,XX[11] 5q31(EGR1x2) 12 2
progress
1 31 RA 47,XX,+8[2]/46,XX,del(5)(q14q34)[1]/46,XX[22] 5q31(EGR1x2) 12 2 progress1 32 RARS 46,XX,del(5)(q13q34)[2]/46,idem,dup(1)(q21q32)[4]/47,XX,+8[5]/46,XX[14] 5q31(EGR1x2) 24 7 progress
1 37 RA46,XX,t(2;11)(p16;q23)[11]/46,idem,-11,+der(11)t(2;11) (p16;q23)[13]/46,idem,del(5)(q14q34)[1] 5q31(EGR1x2) 4 7
no CyR
1 39 RA 46,XX,del(5)(q14q34)[1]/46,XX,del(20)(q12q13)[2]/ 46,XX[22] 5q31(EGR1x2) 4 0 no CyR1 41 RARS 46,XX,del(5)(q14q34)[4]/46,XX[21] 5q31(EGR1x2) 16 5 no CyR1 46 RA 46,XY,del(5)(q22q34)[1]/46,XY[10] 5q31(EGR1x2) 9 0 no CyR1 51 RA 46,XX,del(5)(q14q34)[4]/46,XX[12] 5q31(EGR1x2) 25 4 no CyR1 60 RA 46,XX,del(5)(q14q34)[8]/46,XX[17] 5q31(EGR1x2) 32 5 no CyR1 61 RA 46,XX,del(5)(q14q34)[8]/46,XX[5] 5q31(EGR1x2) 62 6 no CyR1 66 RA 46,XX,del(5)(q21q34)[2]/46,XX[23] 5q31(EGR1x2) 8 2 no CyR1 68 RA 46,XX,del(5)(q21q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3 no CyR1 69 RA 46,XX,del(5)(q14q34)[6]/47,XX,+8[14]/46,XX[5] 5q31(EGR1x2) 24 7 no CyR1 70 RA 47,XX,+8[25]/45,XX,-7[2]/46,XX,del(5)(q14q34)[1] 5q31(EGR1x2) 4 6 no CyR1 73 RA 46,XX,del(5)(q21q34),del(11)(q21)[3]/47,XX+8[7]/46,XX[17] 5q31(EGR1x2) 11 2 no CyR1 75 RARS 46,XX,del(5)(q21q34),t(6;13)(p?23;q?13)[1]/47,XX,+8[21]/46,XX[9] 5q31(EGR1x2) 3 1 no CyR1 76 RA 46,XX,del(5)(q?14q?34)[1]/46,XX[11] 5q31(EGR1x2) 8 7 no CyR1 77 RA 46,XX,del(5)(q13q34)[5]/47,XX,+8[2]/46,XX[18] 5q31(EGR1x2) 20 6 no CyR1 80 RA 46,XX,del(5)(q14q34)[6]/46,XX[19] 5q31(EGR1x2) 24 2 no CyR1 83 RARS 46,XY,del(5)(q14q34)[1]/46,XY[19] 5q31(EGR1x2) 5 0 no CyR1 84 RA 46,XY,del(5)(q14q34)[2]/46,XY[23] 5q31(EGR1x2) 8 6 no CyR1 85 RARS 46,XY,del(5)(q14q34)[1]/46,XY[19] 5q31(EGR1x2) 5 0 no CyR2 9 RA 46,XY,del(5)(q14q34)[1]/46,XY[24] 5q31(EGR1x2) 4 2 no CyR2 10 RA 46,XY,del(5)(q14q34),inv(11)(p13 p14q22 q23)[2]/ 46,XY[23] 5q31(EGR1x2) 8 4 relapse2 13 RA 46,XX,del(5)(q14q34)[1]/46,XX[25] 5q31(EGR1x2) 4 4 no CyR2 23 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 1 relapse2 24 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 0 relapse2 26 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3 relapse2 27 RARS 46,XX,del(5)(q21q34)[1]/46,XX[24] 5q31(EGR1x2) 4 1 relapse
2 29RA
46,XX,del(5)(q14q34)[1]/48-50,idem,+21,+21,+idic(21)(q21~q22), +mar[cp4]/46,XX[20] 5q31(EGR1x2) 20 6
progress
2 30 RA 46,XX,del(20)(q12q13)[6]/46,XX,del(5)(q14q34)[1]/47,XX,+8[1]/46,XX[14] 5q31(EGR1x2) 5 4 progress2 31 RA 46,XX,del(5)(q14q34)[1]/46,idem,del(11)(q21)[2]/46,XX[22] 5q31(EGR1x2) 12 3 progress2 33 RA 46,XX,del(5)(q14q34)[3]/46,XX[3] 5q31(EGR1x2) 50 4 no CyR2 36 RA 45,X,-Y[13]/46,XY,del(5)(q14q34)[5]/ 46,idem,del(13)(q14q31)[4]/ 46,XY[3] 5q31(EGR1x2) 36 2 relapse, progress2 38 RA 46,XY,del(5)(q14q34)[3]/46,XY[22] 5q31(EGR1x2) 12 5 no CyR2 39 RA 46,XX,del(20)(q12q13)[13]/46,XX,del(5)(q14q34)[1]/46,XX[11] 5q31(EGR1x2) 4 3 no CyR2 43 RA 45,XX,-7[3]/46,XX,del(5)(q14q34)[2]/46,XX[20] 5q31(EGR1x2) 8 3 no CyR2 45 RA 46,XY,del(5)(q14q34)[1]/46,XY[24] 5q31(EGR1x2) 4 0 no CyR2 46 RA 46,XY,del(5)(q22q34)[1]/46,XY[11] 5q31(EGR1x2) 9 0 no CyR2 47 RA 46,XY,del(5)(q21q34)[4]/46,XY[21] 5q31(EGR1x2) 16 3 no CyR2 49 RA 47,XX,+8[6]/46,XX,del(5)(q14q34)[4]/46,XX[15] 5q31(EGR1x2) 16 6 no CyR2 50 RA 46,XX,del(5)(q14q34)[1]/46,XX[6] 5q31(EGR1x2) 14 2 no CyR2 53 RA 46,XY,t(2;11)(q16;q24)[23]/46,idem,del(5)(q14q34)[2] 5q31(EGR1x2) 8 4 no CyR2 56 RA 46,XY,del(5)(q14q34)[4]/46,XY[21] 5q31(EGR1x2) 16 6 no CyR2 57 RA 46,XX,del(11)(q14)[3]/46,XX,del(5)(q13q34)[2]/46,XX[20] 5q31(EGR1x2) 8 0 no CyR2 59 RA 46,XX,add(1)(q31),del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 96 3 no CyR2 60 RA 46,XX,del(5)(q14q34)[2]/46,XX[24] 5q31(EGR1x2) 8 6 no CyR2 63 punctio sicca 46,XX,del(5)(q14q34)[4]/46,XX[13] 5q31(EGR1x2) 24 3 no CyR2 64 RA 46,XX,del(5)(q21q34)[3]/46,XX[22] 5q31(EGR1x2) 12 4 no CyR2 66 RA 46,XX,del(5)(q14q34)[3]/46,XX[23] 5q31(EGR1x2) 12 5 no CyR2 67 RA 46,XX,add(5)(q14)[1]/46,XX[13] 5q31(EGR1x2) 7 3 no CyR2 68 punctio sicca 46,XX,del(5)(q21q34)[1]/46,XX[24] 5q31(EGR1x2) 4 1 no CyR2 69 RA 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 6 no CyR2 71 RA 46,XX,del(5)(q22q34)[4]/46,XX[21] 5q31(EGR1x2) 16 4 no CyR2 72 RARS 46,XX,del(5)(q21q34)[2]/46,XX[23] 5q31(EGR1x2) 8 7 no CyR2 74 RA 46,XX,del(5)(q14q34),del(13)(q12q14[1]/46,XX[24] 5q31(EGR1x2) 4 1 no CyR2 79 RA 46,XY,del(5)(q13q34)[4]/46,XY[14] 5q31(EGR1x2) 22 4 no CyR2 80 RA 46,XX,del(5)(q14q34)[2]/46,XX[18] 5q31(EGR1x2) 10 5 no CyR2 81 RA 46,XX,del(5)(q14q34)[14]/46,XX[11] 5q31(EGR1x2) 56 3 no CyR2 82 RA 46,XX,del(5)(q14q34)[8]/46,XX[7] 5q31(EGR1x2) 53 0 no CyR2 85 RARS 46,XY,del(5)(q14q34)[1]/46,XY[25] 5q31(EGR1x2) 4 0 no CyR2 87 RA 46,XX[3] 5q31(EGR1x1) 0 17 no CyR
MP: metaphases. IP: interphases. ISCN: International System for Human Cytogenetic Nomenclature. FISH: fluorescence in situ hybridization. RA: refractory anemia. RARS: RA with ring sideroblasts. n.e.:not evaluable. no CyR: no cytogenetic response. Bold: all discrepancies between karyotyping and FISH, including discrepancies in the detection of independent clones and clonal evolution. *Cytogenetic response was applied to karyotyping only. Complete cytogenetic response (CCyR) was defined as disappearance of the 5q deletion or any other chromosomal aberration. Partial cytogenetic response (PCyR) was defined as a reduction of aberrant metaphases of more than 50% compared to the previous karyotyping. Cytogenetic relapse was defined as reappearance of a metaphase with a deletion in 5q after reaching a complete cytogenetic response. At study entry, in 10 patients, del(5q) was detected only by karyotyping and not by FISH. Therefore, patients 1-10 would not have been eligible for treatment with lenalidomide, if only FISH had been used. In 2 patients, del(5q) was detected only by FISH and not by karyotyping. After 6 months of treatment, in 27 patients del(5q) was detected only by karyotyping and not by FISH. In three of
DOI: 10.3324/haematol.2010.026658

these patients, a clonal evolution occurred. Neither the clonal evolution nor the del(5q) clone would have been detected, if only FISH had been used. After 12 months of treatment, in 39 patients del(5q) was detected only by karyotyping. In one patient, del(5q) was detected only by FISH. In four patients, a clonal evolution occurred. In 6 patients, a cytogenetic relapse occurred at this time point. This relapse would not have been detected, if only FISH had been used.
DOI: 10.3324/haematol.2010.026658

Table 2. Discrepancy in detecting del(5q) by karyotyping and FISH in patients with MDS and del(5q) under at least 18 months (time point 3) of treatment with lenalidomide.
Time point Patient No FAB ISCN-Karyotyp ISCN FISH % MP 5q- % IP 5q- Response*3 14 RA 46,XX,del(5)(q21q34)[3]/46,XX[23] 5q31(EGR1x2) 12 7 relapse3 15 RARS 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 0 relapse3 17 RA 46,XX,del(5)(q14q34)[1]/46,XX,[24] 5q31(EGR1x2) 4 4 relapse3 19 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3 relapse3 21 RA 46,XX,del(5)(q21q34)[10]/46,idem,del(13)(q12q14)[16] 5q31(EGR1x2) 100 1 relapse3 23 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 0 relapse3 24 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3 relapse3 25 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3 relapse3 26 RA 46,XX,del(5)(q14q34)[3]/46,XX[29] 5q31(EGR1x2) 9 6 relapse3 30 RA 46,XX,del(20)(q12q13)[3]/46,XX,del(5)(q14q34)[2]/ 46,XX[20] 5q31(EGR1x2) 8 2 progress
3 31RA
46,XX,del(5)(q14q34),del(11)(q21)[8]/46,idem,?t(X;1)(q11;q36)[2]/47,idem, ?t(X;1)(q11;q36),+8[2]/46,XX[13] 5q31(EGR1x2) 48 4
progress
3 33 RA 46,XX,del(5)(q14q34)[2]/46,idem,del(13)(q13q21)[2]/ 46,XX[21] 5q31(EGR1x2) 8 6 progress3 34 RA 46,XY,del(5)(q14q34)[4]/46,XY,del(11)(q14)[2]/46,XY[19] 5q31(EGR1x2) 16 4 relapse, progress
3 37 RA46,XX,t(2;11)(p16;q23)[21]/46,idem,del(5)(q14q34)[2]/46,idem,der(18)t(9;18) (p10;q10)[2] 5q31(EGR1x2) 8 4
no CyR
3 38 RA 46,XY,del(5)(q14q34)[1]/46,XY[15] 5q31(EGR1x2) 6 8 no CyR3 40 RA 46,XX,del(5)(q14q34)[9]/46,XX[16] 5q31(EGR1x2) 36 4 no CyR3 44 RA 46,XX,inv(9)(p11q12)c[24]/46,idem,del(5)(q14q34)[1] 5q31(EGR1x2) 4 5 no CyR3 46 RA 46,XY,del(5)(q14q34)[3]/46,XY[22] 5q31(EGR1x2) 12 4 no CyR3 47 RA 46,XY,del(5)(q21q34)[10]/46,XY[15] 5q31(EGR1x2) 40 1 no CyR3 48 RA 45,X,-Y[4]/46,XY,del(5)(q21q34)[2]/46,XY[19] 5q31(EGR1x2) 8 5 no CyR3 50 RA 46,XX,del(5)(q14q34)[1]/46,XX[4] 5q31(EGR1x2) 20 3 no CyR3 52 RA 46,XX,del(5)(q14q34)[1]/46,XX[6] 5q31(EGR1x2) 14 3 no CyR3 53 RA 46,XY,t(2;11)(p16;q24)[24]/46,idem,del(5)(q14q34)[2] 5q31(EGR1x2) 8 6 no CyR3 54 RA 47,XX,del(5)(q13q34),+21[9]/46,XX[1] 5q31(EGR1x2) 90 2 no CyR3 55 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3 no CyR3 60 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 0 no CyR3 63 punctio sicca 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 4 no CyR3 66 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 1 no CyR3 67 RA 46,XX,del(5)(q14q34)[2]/46,XX[12] 5q31(EGR1x2) 14 2 no CyR3 68 punctio sicca 46,XX,del(5)(q21q34)[2]/46,XX[23] 5q31(EGR1x2) 8 3 no CyR3 71 RA 46,XX,del(5)(q22q34)[2]/46,XX[5] 5q31(EGR1x2) 29 3 no CyR3 72 RARS 46,XX,del(5)(q21q34)[4]/46,XX[21] 5q31(EGR1x2) 16 6 no CyR3 74 RA 46,XX,del(5)(q14q34),del(13)(q12q14)[3]/46,XX[22] 5q31(EGR1x2) 12 2 no CyR3 79 RA 46,XY,del(5)(q13q34)[1]/46,XY[25] 5q31(EGR1x2) 4 2 no CyR4 11 RA 46,XY,del(5)(q21q34)[2]/46,XY[23] 5q31(EGR1x2) 8 4 relapse4 12 RA 46,X,t(X;16)(p11;q23),del(5)(q21q34)[3]/46,XX[23] 5q31(EGR1x2) 12 4 relapse4 13 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 5 relapse4 18 RA 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 5 relapse4 20 RA 46,XX,del(5)(q15q34)[5]/46,XX[20] 5q31(EGR1x2) 20 7 relapse4 22 RARS 45,X,-Y[5]/46,XY,del(5)(q14q34)[2]/46,XY[20] 5q31(EGR1x2) 7 1 relapse4 23 RA 46,XX,del(5)(q14q34)[1]/46,idem,del(1)(p32p35)[1]/ 46,XX[23] 5q31(EGR1x2) 8 1 relapse4 24 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 4 relapse4 25 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 1 relapse4 28 RARS 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 2 relapse
4 30 RA46,XX,del(1)(p32p36),del(5)(q14q34)[11]/46,XX,del(20)(q12q13)[4]/46,XX[10] 5q31(EGR1x2) 44 3
progress
4 34 RA 46,XY,del(11)(q14)[5]/46,XY,del(5)(q14q34)[3]/46,XY[17] 5q31(EGR1x2) 12 6 relapse, progress4 38 RA 46,XY,del(5)(q21q34)[2]/46,XY[3] 5q31(EGR1x2) 40 6 no CyR4 42 RA 46,XX,del(5)(q21q34)[10]/46,XX[19] 5q31(EGR1x2) 34 2 no CyR4 47 RA 46,XY,del(5)(q14q34)[1]/46,XY[5] 5q31(EGR1x2) 17 5 no CyR4 48 RA 46,XY,del(5)(q21q34)[11]/45,X,-Y[2]/46,XY[12] 5q31(EGR1x2) 44 7 no CyR4 50 RA 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 2 no CyR4 52 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 2 no CyR4 60 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 2 no CyR4 65 RA 46,XX,del(5)(q14q34)[10]/47,idem,+21[1]/46,XX[10] 5q31(EGR1x2) 52 6 no CyR4 66 RA 46,XX,del(5)(q14q34)[1]/46,XX[28] 5q31(EGR1x2) 3 4 no CyR4 67 RA 46,XX,del(5)(q14q34)[3]/46,XX[14] 5q31(EGR1x2) 18 0 no CyR4 68 punctio sicca 46,XX,del(5)(q21q34)[1]/46,XX[24] 5q31(EGR1x2) 4 4 no CyR4 78 RA 47,XX,+X[24]/47,idem,del(5)(q14q34)[1] 5q31(EGR1x2) 4 2 no CyR4 79 RA 92,XXYY,del(5)(q13q34)x2[1]/46,XY[4] 5q31(EGR1x2) 20 4 no CyR5 11 RA 46,XY,del(5)(q21q34)[2]/46,XY[23] 5q31(EGR1x2) 8 2 relapse5 12 RA 46,XX,t(X;16)(p11;q23),del(5)(q21q34)[5]/46,XX[20] 5q31(EGR1x2) 20 4 relapse5 13 RA 46,XX,del(5)(q14q34) [3]/46,XX[22] 5q31(EGR1x2) 12 4 relapse5 16 RA 46,XX,del(5)(q23q34)[20]/46,XX[5] 5q31(EGR1x2) 80 0 relapse5 24 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 5 relapse5 25 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 1 relapse
5 30 RA46,XX,del(1)(p32p36),del(5)(q14q34)[7]/46,idem,del (20)(q12q13)[1]/ 46,XX,del(20)(q12q13)[8]/46,XX[9] 5q31(EGR1x2) 32 1
progress
5 35 RA 46,XX,del(5)(q14q34),-7,-17,+mar[2]/ 46,XX[24] 5q31(EGR1x2) 8 0 relapse, progress
5 37 RA46,XX,t(2;11)(p16;q23)[3]/46,idem,-11,+der(11)t(2;11) (p16;q23)[20]/ 46,idem,del(5)(q14q34)[2] 5q31(EGR1x2) 8 6
no CyR
5 40 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 5 no CyR5 47 RA 46,XY,del(5)(q21q34)[10]/46,XY[12] 5q31(EGR1x2) 45 0 no CyR5 53 RA 46,XY,t(2;11)(p16;q24)[24]/46,idem,del(5)(q14q34)[1] 5q31(EGR1x2) 4 1 no CyR5 66 RA 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 1 no CyR5 67 RA 46,XX,del(5)(q14q34)[6]/46,XX[19] 5q31(EGR1x2) 24 5 no CyR5 68 punctio sicca 46,XX,del(5)(q21q34)[1]/46,XX[26] 5q31(EGR1x2) 4 1 no CyR5 87 RA 46,XX[3] 5q31(EGR1x1) 0 56 no response6 11 RA 46,XY,del(5)(q21q34)[2]/46,XY[24] 5q31(EGR1x2) 8 2 relapse6 16 RA 46,XX,del(5)(q23q34)[1]/46,XX[24] 5q31(EGR1x2) 4 2 relapse6 33 RA 46,XX,del(5)(q14q34)[2]/46,idem,del(13)(q13q21)[6]/ 46,XX[17] 5q31(EGR1x2) 8 3 progress
6 37 RA46,XX,t(2;11)(p16;q23)[3]/46,idem,-11,+der(11)t(2;11 (p16;q23)[20]/46,idem,del(5)(q14q34)[3] 5q31(EGR1x2) 12 2
no CyR
6 58 punctio sicca 46,XX,del(5)(q14q34)[5]/46,XX[20] 5q31(EGR1x2) 20 4 no CyR6 60 RA 46,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 2 no CyR7 11 RA 46,XY,del(5)(q21q34)[4]/46,XY[21] 5q31(EGR1x2) 16 5 relapse
7 37 RA46,XX,t(2;11)(p16;q23),der(11)t(2;11)(p16;q23)[23]/ 46,idem,del(5)(q14q34), -der(11)t(2;11)(p16;q23)[2] 5q31(EGR1x2) 8 2
no CyR
8 62 RA 68 - 178,3 - 8n ,del(5)(q14q34),+21[cp2]/46,XX[9] 5q31(EGR1x2) 18 1 no CyR9 62 RA 47,XX,del(5)(q21q34),+21[1]/46,XX[24] 5q31(EGR1x2) 4 2 no CyR
MP: metaphases. IP: interphases. ISCN: International System for Human Cytogenetic Nomenclature. FISH: fluorescence in situ hybridization. RA: refractory anemia. RARS: RA with ring sideroblasts. n.e.: not evaluable. No CyR: no cytogenetic response. Bold: all discrepancies between karyotyping and FISH, including discrepancies in the detection of independent clones and clonal evolution.*Cytogenetic response was applied to karyotyping only. Complete cytogenetic response (CCyR) was defined as disappearance of the 5q deletion or any other chromosomal aberration. Partial cytogenetic response (PCyR) was defined as a reduction of aberrant metaphases of more than 50% compared to the previous karyotyping. Cytogenetic relapse was defined as reappearance of a metaphase with a deletion in 5q after reaching a complete cytogenetic response. In 85 cases, a discrepancy was detected. In only one patient was del(5q) detected by FISH only. In the other cases, del(5q) was detected by karyotyping only and not by FISH. In 31 cases, a cytogenetic relapse occurred and would not have been detected, if only FISH had been used. In 9 cases, a progress with a clonal evolution could be detected by karyotyping. Neither the clonal evolution nor the del(5q) clone would have been detected, if only FISH had been used.
DOI: 10.3324/haematol.2010.026658

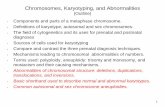
Figure 1 (A) Karyogram of a patient with myelodysplastic syndrome and a deletion in
the long arm of chromosome 5 (fluorescence R-banding). (B) More detailed analysis
identified the deletion as an interstitial deletion. (C) Comparison with the ideogram of
chromosome 5 shows that the breakpoints are located in 5q14 and 5q34.
(D) Scheme of fluorescence in situ hybridization to detect a deletion in 5q. The probe
localized to the short arm of chromosome 5 (5p21) generates a green control signal.
The probe binding to the commonly deleted region 5q31 gives an orange signal.
(E) Interphase nucleus with a normal signal constellation, i.e. two green and two
orange signals. (F) Interphase nuclei with a signal constellation indicative of a
deletion in 5q, i.e. two green signals and one orange signal.
DOI: 10.3324/haematol.2010.026658

Figure 1
A
C c
D
F
B
E
A
C c
D
F
B
E
DOI: 10.3324/haematol.2010.026658

Supplementary Table 1
Patient No ISCN Karyotype ISCN FISH % MP 5q- % IP 5q-
1 46,XY,del(5)(q?14q34)[1]/46,XY[24] 5q31(EGR1x2) 4 146,XY[25] 5q31(EGR1x2) 0 346,XY[28] 5q31(EGR1x2) 0 2
2 46,XX,del(5)(q22q34)[4]/46,XX[21] 5q31(EGR1x2) 16 33 46,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 44 46,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 6
46,XX,del(5)(q14q34)[24]/46,XX[1] 5q31(EGR1x1) 96 3446,XX,del(5)(q14q34)[11]/46,XX[14] 5q31(EGR1x2) 44 546,XX,del(5)(q14q34)[15]/46,XX[10] 5q31(EGR1x1) 60 1746,XX,del(5)(q14q34)[15]/46,XX[10] 5q31(EGR1x1) 60 2446,XX,del(5)(q14q34)[16]/46,XX[9] 5q31(EGR1x1) 64 3746,XX,del(5)(q14q34)[15]/46,idem,der(1)t(1;10)(p11;?),der(9)t(1;9)(?;?),der(10)t(9;10)(?;q21) [2]/46,XX[8] 5q31(EGR1x1) 68 3746,XX,del(5)(q14q34)[12]/46,idem,der(1)t(1;10)(p11;?),der(9)t(1;9)(?;?),der(10)t(9;10)(?;q21)/47,idem,der(1)t(1;10)(p11;?),+9,der(9)t(1;9)(?;?)x2,der(10)t(9;10)(?;q21)[2]/45,idem,der(1) t(1;10)(p11;?),-7,der(9),t(1;9)(?;?),der(10)t(9;10)(q;q21)[3]/46,idem,der(1)t(1;10)(p11;?),-7, der(9)t(1;9)(?;?),der(10)t(9;10)(?;q21),+mar[2]/46,XX[5] 5q31(EGR1x1) 80 4546,XX,del(5)(q14q34)[2]/46,idem,der(1)t(1;10)(p11;?),der(2)t(2;4)(p25;q26),inv(6)(p12q15), der(9)t(1;9)(?,?),der(10)t(9;10)(?;q21)[12]/44,idem,-7,dic(12;15)(p11;p11),-17,+mar[5]/ 46,XX[1] 5q31(EGR1x1) 95 35
5 47,XX,+8[4]/45,XX,del(5)(q1?4q34),-7[3]/46,XX[48] 5q31(EGR1x2) 5 46 46,XX,del(5)(q13q34)[1]/46,idem,add(20)(q13)[2] 5q31(EGR1x2) 100 2
46,XX,del(5)(q14q34)[21]/46,XX[4] 5q31(EGR1x1) 84 297 46,XX,del(5)(q23q34)[4]/46,XX[7] 5q31(EGR1x2) 36 6
46,XX,del(5)(q23q34)[20]/46,XX[5] 5q31(EGR1x1) 80 5846,XX,del(5)(q23q34)[1]/46,XX[2] 5q31(EGR1x1) 33 26no metaphases 5q31(EGR1x1) - 35
8 46,XY,del(5)(q?21q?34)[2]/46,XY[23] 5q31(EGR1x2) 8 546,XY,del(5)(q21q34)[1]/46,XY[19] 5q31(EGR1x2) 5 4
9 46,XY,del(5)(q21q34)[1]/46,XY[24] 5q31(EGR1x2) 4 646,XY,del(5)(q14q34)[15]/46,XY[9] 5q31(EGR1x1) 63 2646,XY,del(5)(q14q34)[1]/46,XY[24] 5q31(EGR1x2) 4 246,XY[25] 5q31(EGR1x2) 0 446,XY[14] 5q31(EGR1x2) 0 546,XY,del(5)(q21q34)[9]/46,idem,inv(1)(p12p35),t (1;4)(p36;q32)[3]/ 46,XY[15] 5q31(EGR1x1) 44 1846,XY,del(5)(q21q34)[3]/46,idem,inv(1)(p12p35),t (1;4)(p36;q32)[7]/ 46,XY[5] 5q31(EGR1x1) 67 1646,XY,del(5)(q21q34)[10]/46,idem,inv(1)(p12p35),t(1;4)(p36;q32)[12]/46,XY[3] 5q31(EGR1x1) 88 46
10 46,XY,del(5)(q14q34),inv(11)(p13~p14q22 q23)[18]/46,XY[7] 5q31(EGR1x2) 72 045,X,-Y[11]/46,XY[14] 5q31(EGR1x2) 0 046,XY,del(5)(q14q34),inv(11)(p13~p14q22 q23)[2]/ 46,XY[23] 5q31(EGR1x2) 8 445,X,-Y[11]/46,XY[14] 5q31(EGR1x2) 0 346,XY[25] 5q31(EGR1x2) 0 046,XY[25] 5q31(EGR1x2) 0 0
11 47,XY,del(5)(q21q34),+8[3]/46,XY[2] 5q31(EGR1x1) 60 7346,XY,del(5)(q21q34)[3]/46,XY[22] 5q31(EGR1x2) 12 446,XY,del(5)(q21q34)[3]/46,XY[22] 5q31(EGR1x1) 12 346,XY[20] 5q31(EGR1x2) 0 446,XY,del(5)(q21q34)[2]/46,XY[23] 5q31(EGR1x2) 8 446,XY,del(5)(q21q34)[2]/46,XY[23] 5q31(EGR1x2) 8 2
DOI: 10.3324/haematol.2010.026658

Supplementary Table 1
46,XY,del(5)(q21q34)[2]/46,XY[24] 5q31(EGR1x2) 8 246,XY,del(5)(q21q34)[4]/46,XY[21] 5q31(EGR1x2) 16 5
12 46,XX,t(X;16)(p11;q23),del(5)(q14q34)[23]/46,XX[2] 5q31(EGR1x1) 92 7346,XX,t(X;16)(p11;q23),del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 446,XX[25] 5q31(EGR1x2) 0 246,XX[25] 5q31(EGR1x2) 0 546,XX,t(X;16)(p11;q23),del(5)(q21q34)[3]/46,XX[23] 5q31(EGR1x2) 12 446,XX,t(X;16)(p11;q23),del(5)(q21q34)[5]/46,XX[20] 5q31(EGR1x2) 20 446,XX,t(X;16)(p11;q23),del(5)(q21q34)[10]/46,XX[15] 5q31(EGR1x1) 40 9
13 46,XX,del(5)(q14q34)[19]/46,XX[6] 5q31(EGR1x1) 76 71
46,XX,del(5)(q14q34)[1]/46.XX[14]no interphase nuclei 7 -
46,XX,del(5)(q14q34)[1]/46,XX[25] 5q31(EGR1x2) 4 446,XX[24] 5q31(EGR1x2) 0 346,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 546,XX,del(5)(q14q34) [3]/46,XX[22] 5q31(EGR1x2) 12 446,XX,del(5)(q14q34)[12]/46,XX[13] 5q31(EGR1x1) 48 18
14 46,XX,del(5)(q21q34)[11]/46,XX[5] 5q31(EGR1x1) 69 1246,XX,del(5)(q21q34)[2]/46,XX[23] 5q31(EGR1x2) 8 546,XX[26] 5q31(EGR1x2) 0 246,XX,del(5)(q21q34)[3]/46,XX[23] 5q31(EGR1x2) 12 746,XX,del(5)(q21q34)[9]/46,XX[16] 5q31(EGR1x1) 36 3846,XX,del(5)(q21q34)[19]/47,idem,+21[1]/46,XX[5] 5q31(EGR1x1) 80 36
15 46,XX,del(5)(q14q34)[15]/46,XX[6] 5q31(EGR1x1). 71 5946,XX,del(5)(q14q34)[1]/46,XX[19] 5q31(EGR1x2) 5 046,XX[20] 5q31(EGR1x2) 0 046,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 0
16 46,XX,del(5)(q14q34)[20]/46,XX[5] 5q31(EGR1x1) 80 5947,XX,+14[2]/46,XX[23] 5q31(EGR1x2) 0 346,XX,del(5)(q23q34)[22]/46,XX[3] 5q31(EGR1x1) 8 7447,XX,+8[5]/46,XX,del(5)(q14q34)[2]/46,XX[18] 5q31(EGR1x1) 8 1146,XX[25] 5q31(EGR1x2) 0 146,XX,del(5)(q23q34)[20]/46,XX[5] 5q31(EGR1x2) 80 046,XX,del(5)(q23q34)[1]/46,XX[24] 5q31(EGR1x2) 4 2
17 46,XX,del(5)(q14q34)[20] 5q31(EGR1x1) 100 3745,XX,-7[16]/47,XX,+8[4]/46,XX,del(5)(q14q34)[3]/46,XX[2] 5q31(EGR1x1) 12 347,XX,+8[1]/46,XX[24] 5q31(EGR1x2) 0 046,XX,del(5)(q14q34)[1]/46,XX,[24] 5q31(EGR1x2) 4 446,XX,+1,der(1;7)(q10;p10)[5]/46,XX[20] 5q31(EGR1x2) 0 246,XX,+1,der(1;7)(q10;p10)[9]/46,XX[16] 5q31(EGR1x2) 0 346,XX,+1,der(1;7)(q10;p10)[12]/46,XX[13] 5q31(EGR1x2) 0 146,XX,+1,der(1;7)(q10;p10)[9]/46,XX[16] 5q31(EGR1x2) 0 2
18 no metaphasesno interphase nuclei - -
no metaphases 5q31(EGR1x2) - 546,XX[25] 5q31(EGR1x2) 0 346,XX[28] 5q31(EGR1x1) 0 446,XX,del(5)(q14q34)[3]/46,XX[22] 5q31(EGR1x2) 12 546,XX,del(5)(q14q34)[1]/46,XX[2] 5q31(EGR1x1) 33 25
19 46,XX,del(5)(q14q34)[14]/46,idem,del(12)(p12p13)[5]/ 46,XX[6] 5q31(EGR1x1) 76 62
DOI: 10.3324/haematol.2010.026658

Supplementary Table 1
46,XX,del(5)(q14q34)[6]/46,XX[19] 5q31(EGR1x1) 24 846,XX[25] 5q31(EGR1x2) 0 546,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 346,XX,del(5)(q14q34)[14]/46,idem,del(12)(p12p13)[5]/ 46,XX[6] 5q31(EGR1x1) 76 8
20 46,XX,del(5)(q15q34)[25] 5q31(EGR1x1) 100 8146,XX,del(5)(q15q34)[18]/46,XX[7] 5q31(EGR1x1) 72 4446,XX,del(5)(q15q34)[3]/46,XX[17] 5q31(EGR1x1) 15 1046,XX[25] 5q31(EGR1x2) 0 246,XX,del(5)(q15q34)[5]/46,XX[20] 5q31(EGR1x2) 20 746,XX,del(5)(q15q34)[13]/46,idem,del(17)(p12)[6]/ 46,XX[6] 5q31(EGR1x1) 76 2746,XX,del(5)(q15q34)[24]/46,idem,del(17)(p12)[1] 5q31(EGR1x1) 100 5846,XX,del(5)(q15q34)[25]/46,XX[1] 5q31(EGR1x1) 96 5246,XX,del(5)(q15q34)[23]/46,idem,del(17)(p12)[2]/ 46,XX[1] 5q31(EGR1x1) 96 4146,XX,del(5)(q15q34)[23]/46,XX[2] 5q31(EGR1x1) 92 64
21 46,XX,del(5)(q21q34)[10]/46,idem,del(13)(q12q14)[16] 5q31(EGR1x1) 100 8146,XX[7] 5q31(EGR1x2) 0 446,XX[23] 5q31(EGR1x2) 0 246,XX,del(5)(q21q34)[10]/46,idem,del(13)(q12q14)[16] 5q31(EGR1x2) 100 146,XX[7] 5q31(EGR1x2) 0 146,XX[25] 5q31(EGR1x2) 0 346,XX[25] 5q31(EGR1x2) 0 246,XX,del(5)(q21q34),del(13)(q12q14)[2]/46,XX[25] 5q31(EGR1x1) 7 8
22 46,XX,del(5)(q14q34)[8]/46,XX[17] 5q31(EGR1x1) 32 2245,X,-Y[5]/46,XY[23] 5q31(EGR1x2) 0 245,X,-Y[10]/46,XY[16] 5q31(EGR1x2) 0 145,X,-Y[5]/46,XY[21] 5q31(EGR1x2) 0 145,X,-Y[5]/46,XY,del(5)(q14q34)[2]/46,XY[20] 5q31(EGR1x2) 7 1
23 46,XX[2] 5q31(EGR1x1) 0 2146,XX[25] 5q31(EGR1x2) 0 146,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 146,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 046,XX,del(5)(q14q34)[1]/46,idem,del(1)(p32p35)[1]/ 46,XX[23] 5q31(EGR1x2) 8 146,XX[26] 5q31(EGR1x2) 0 246,XX[25] 5q31(EGR1x2) 0 2
24 46,XX,del(5)(q14q34)[20]/46,XX[6] 5q31(EGR1x1) 77 6346,XX[25] 5q31(EGR1x2) 0 446,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 046,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 346,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 446,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 5
25 46,XX,del(5)(q14q34)[23]/46,XX[2] 5q31(EGR1x1) 92 5146,XX[3] 5q31(EGR1x2) 0 646,XX[25] 5q31(EGR1x2) 0 346,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 346,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 146,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 146,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x1) 4 8
26 46,XX,del(5)(q14q34)[25] 5q31(EGR1x1) 100 6346,XX[25] 5q31(EGR1x2) 0 446,XX,del(5)(q14q34)[1]/46,XX[24] 5q31(EGR1x2) 4 3
DOI: 10.3324/haematol.2010.026658

Supplementary Table 1
46,XX,del(5)(q14q34)[3]/46,XX[29] 5q31(EGR1x2) 9 627 46,XX,del(5)(q21q34)[7] 5q31(EGR1x1) 100 64
46,XX[6] 5q31(EGR1x2) 0 246,XX,del(5)(q21q34)[1]/46,XX[24] 5q31(EGR1x2) 4 1
no metaphasesno interphase nuclei - -
46,XX[25] 5q31(EGR1x2) 0 246,XX[27] 5q31(EGR1x2) 0 546,XX[14] 5q31(EGR1x2) 0 1
28 46,XX,del(5)(q14q34)[3]/46,XX[23] 5q31(EGR1x1) 12 846,XX[25] 5q31(EGR1x2) 0 046,XX[9] 5q31(EGR1x2) 0 246,XX[24] 5q31(EGR1x2) 0 446,XX,del(5)(q14q34)[2]/46,XX[23] 5q31(EGR1x2) 8 2
DOI: 10.3324/haematol.2010.026658

Supplementary Table 2
Patient No ISCN Karyotype ISCN FISH % MP 5q- % IP 5q-29 46,XX,del(5)(q14q34)[10]/47,idem,+21[4] 5q31(EGR1x1) 100 42
46,XX,del(5)(q14q34)[11]/50,idem,+idic(21)(q22)x5[1]/ 46,XX[13] 5q31(EGR1x1) 48 12
46,XX,del(5)(q14q34)[1]/48-50,idem,+21,+21,+idic(21)(q21q22), +mar[cp4]/46,XX[20] 5q31(EGR1x2) 20 6
30 46,XX,del(5)(q14q34)[24]/46,XX[1] 5q31(EGR1x1) 96 7247,XX,+8[7]/46,XX,del(20)(q12q13)[4]/46,XX,del(5)(q14q34)[2]/ 46,XX,idem,del(20)(q12q13)[1]/46,XX[11] 5q31(EGR1x2) 12 246,XX,del(20)(q12q13)[6]/46,XX,del(5)(q14q34)[1]/ 47,XX,+8[1]/ 46,XX[14] 5q31(EGR1x2) 5 446,XX,del(20)(q12q13)[3]/46,XX,del(5)(q14q34)[2]/ 46,XX[20] 5q31(EGR1x2) 8 246,XX,del(1)(p32p36),del(5)(q14q34)[11]/46,XX,del(20)(q12q13) [4]/ 46,XX[10] 5q31(EGR1x2) 44 346,XX,del(1)(p32p36),del(5)(q14q34)[7]/46,idem,del (20)(q12q13)[1]/ 46,XX,del(20)(q12q13)[8]/46,XX[9] 5q31(EGR1x2) 32 1
31 46,XX,del(5)(q14q34)[21]/46,XX[4] 5q31(EGR1x1) 84 4547,XX,+8[2]/46,XX,del(5)(q14q34)[1]/46,XX[22] 5q31(EGR1x2) 12 2
46,XX,del(5)(q14q34)[1]/46,idem,del(11)(q21)[2]/46,XX[22] 5q31(EGR1x2) 12 346,XX,del(5)(q14q34),del(11)(q21)[8]/46,idem,?t(X;1)(q11;q36)[2]/47,idem,?t(X;1)(q11;q36),+8[2]/46,XX[13] 5q31(EGR1x2) 48 446,XX,del(5)(q14q34),del(11)(q21)[6]/47,idem,t(X;1)(q11;q36), +8[16]/46,idem,del(12)(p12p13)[1]/46,XX[2] 5q31(EGR1x1) 92 82
32 46,XX,del(5)(q1?3q34)[22] 5q31(EGR1x1) 100 6046,XX,del(5)(q13q34)[2]/46,idem,dup(1)(q21q32)[4]/ 47,XX,+8[5]/ 46,XX[14] 5q31(EGR1x2) 24 7
33 no metaphasesno interphase nuclei - -
46,XX,del(5)(q?14q34)[1] 5q31(EGR1x1) 100 2746,XX,del(5)(q14q34)[3]/46,XX[3] 5q31(EGR1x2) 50 446,XX,del(5)(q14q34)[2]/46,idem,del(13)(q13q21)[2]/ 46,XX[21] 5q31(EGR1x2) 8 646,XX[27] 5q31(EGR1x2) 0 346,XX,del(5)(q14q34)[6]/46,idem,del(13)(q13q21)[4]/ 46,XX[15] 5q31(EGR1x1) 40 1246,XX,del(5)(q14q34)[2]/46,idem,del(13)(q13q21)[6]/ 46,XX[17] 5q31(EGR1x2) 8 3
34 46,XY,del(5)(q14q34)[23]/46,XY[2] 5q31(EGR1x1) 92 8146,XY,del(5)(q14q34)[25] 5q31(EGR1x1) 100 8946,XY[25] 5q31(EGR1x2) 0 546,XY,del(5)(q14q34)[4]/46,XY,del(11)(q14)[2]/46,XY[19] 5q31(EGR1x2) 16 446,XY,del(11)(q14)[5]/46,XY,del(5)(q14q34)[3]/46,XY[17] 5q31(EGR1x2) 12 6
35 46,XX,del(5)(q21q34)[6] 5q31(EGR1x1) 100 6846,XX,del(5)(q21q34)[21] 5q31(EGR1x1) 100 5946,XX[25] 5q31(EGR1x2) 0 146,XX[25] 5q31(EGR1x2) 0 046,XX[25] 5q31(EGR1x2) 0 245,XX,del(5)(q),-7,-17,+mar[2]/ 46,XX[24] 5q31(EGR1x2) 8 044,XX,del(5)(q21q34),-7,idic(8;?17)(p11;p11),del(12)(p12p13), 18[24]/46,XX[1] 5q31(EGR1x1) 96 31
36 46,XY,del(5)(q14q34)[8]/46,XY[5] 5q31(EGR1x1) 62 1345,X,-Y[19]/ 46,XY[7] 5q31(EGR1x2) 0 545,X,-Y[13]/46,XY,del(5)(q14q34)[5]/ 46,idem,del(13)(q14q31)[4]/ 46,XY[3] 5q31(EGR1x2)
36 2
DOI: 10.3324/haematol.2010.026658