
Cystic fibrosis* brosis 6 Shalethorax.bmj.com/content/thoraxjnl/46/4/261.full.pdfDistal intestinal...
7
Thorax 1991;46:261-267 Cystic fibrosis* 6 Series editor: D J Shale Gastrointestinal and nutritional aspects Hinda Kopelman Cystic fibrosis is the most frequent cause of pancreatic insufficiency and chronic lung disease with progressive pulmonary failure in childhood. Though most cases are diagnosed in childhood, because affected individuals now live beyond their 20th birthday' cystic fibrosis is encountered more often by physicians deal- ing with adults. It has become a major cause of refractory malnutrition and new man- agement approaches to nutrition are impor- tant in the care of these patients. This article will review the pancreatic, intestinal, hepatobiliary, and nutritional disturbances characteristic of cystic fibrosis and some current developments in our understanding of their pathogenesis, and in our approaches to management. Pathogenesis The primary defect in cystic fibrosis is un- known. The gene locus has been identified on the long arm of chromosome 7, cloned, and sequenced, but the function of the protein product remains unknown at the time of writ- ing. The gene is consistently expressed in epithelial cells and abnormal regulation of epithelial ion transport can account for the experimental findings in several tissues classi- cally affected in the disease (fig 1). Chloride impermeability in the sweat duct gives rise to the well known finding of a raised sweat chloride concentration in cystic fibrosis. Exocrine glands that depend on the epithelial transport of anions to move water across membranes and into secretions may develop obstructive plugging because of increased concentrations of macromolecules and the consequent failure to clear secretions. Studies using pancreatic secretions from patients with their pancreatic dysfunction well controlled strongly support this hypothesis.2 Pancreatic manifestations The earliest characteristic morphological feature of the pancreas in cystic fibrosis is the accumulation of secretory material within ducts and ductal obstruction. Subsequent tissue damage, presumably from acinar release of lytic enzymes, leads to the progressive loss of functioning acinar tissue, fibrosis, and fatty replacement, the hallmarks of pancreatic disease in cystic fibrosis (fig 2). The degree of pancreatic destruction is highly variable, accounting for the differences in clinical Secretory defect |- Abnormally viscous secretions (a) macromolecular hyperconcentration (b) low volumes Division of Gastroenterology, Department of Pediatrics, and McGill University-Montreal Children's Hospital Research Institute, Montreal H3H 1P3, Canada H Kopelman Reprint requests to: Dr Kopelman, Division of Gastroenterology, 2300 Tupper Room D596, Montreal Children's Hospital, Montreal H3H 1P3, Canada. High sweat chloride concentrations Hyponatraemic Hypochloraemic Metabolic alkalosis Obstructive plugging ...obiiary _ Z eens Exocrine pancreatic insufficiency Pancreatitis Glucose intolerance Adult onset diabetes mellitus Meconium ileus Distal intestinal obstruction syndrome Focal biliary fibrosis Multilobular cirrhosis Cholelithiasis Recurrent pneumonia Chronic lung disease Male infertility Figure 1 Pathogenesis and clinical manifestations of cystic fibrosis. Reproduced by courtesy of Medicine (North America). 261 Cystic brosis - 6 Series editor: D J Shale on 25 May 2018 by guest. Protected by copyright. http://thorax.bmj.com/ Thorax: first published as 10.1136/thx.46.4.261 on 1 April 1991. Downloaded from
Transcript of Cystic fibrosis* brosis 6 Shalethorax.bmj.com/content/thoraxjnl/46/4/261.full.pdfDistal intestinal...
Thorax 1991;46:261-267
Cysticfibrosis* 6 Series editor: D J Shale
Gastrointestinal and nutritional aspects
Hinda Kopelman
Cystic fibrosis is the most frequent cause ofpancreatic insufficiency and chronic lungdisease with progressive pulmonary failure inchildhood. Though most cases are diagnosedin childhood, because affected individuals nowlive beyond their 20th birthday' cystic fibrosisis encountered more often by physicians deal-ing with adults. It has become a major causeof refractory malnutrition and new man-agement approaches to nutrition are impor-tant in the care of these patients. This articlewill review the pancreatic, intestinal,hepatobiliary, and nutritional disturbancescharacteristic of cystic fibrosis and somecurrent developments in our understanding oftheir pathogenesis, and in our approaches tomanagement.
PathogenesisThe primary defect in cystic fibrosis is un-known. The gene locus has been identified onthe long arm of chromosome 7, cloned, andsequenced, but the function of the proteinproduct remains unknown at the time of writ-ing. The gene is consistently expressed inepithelial cells and abnormal regulation ofepithelial ion transport can account for the
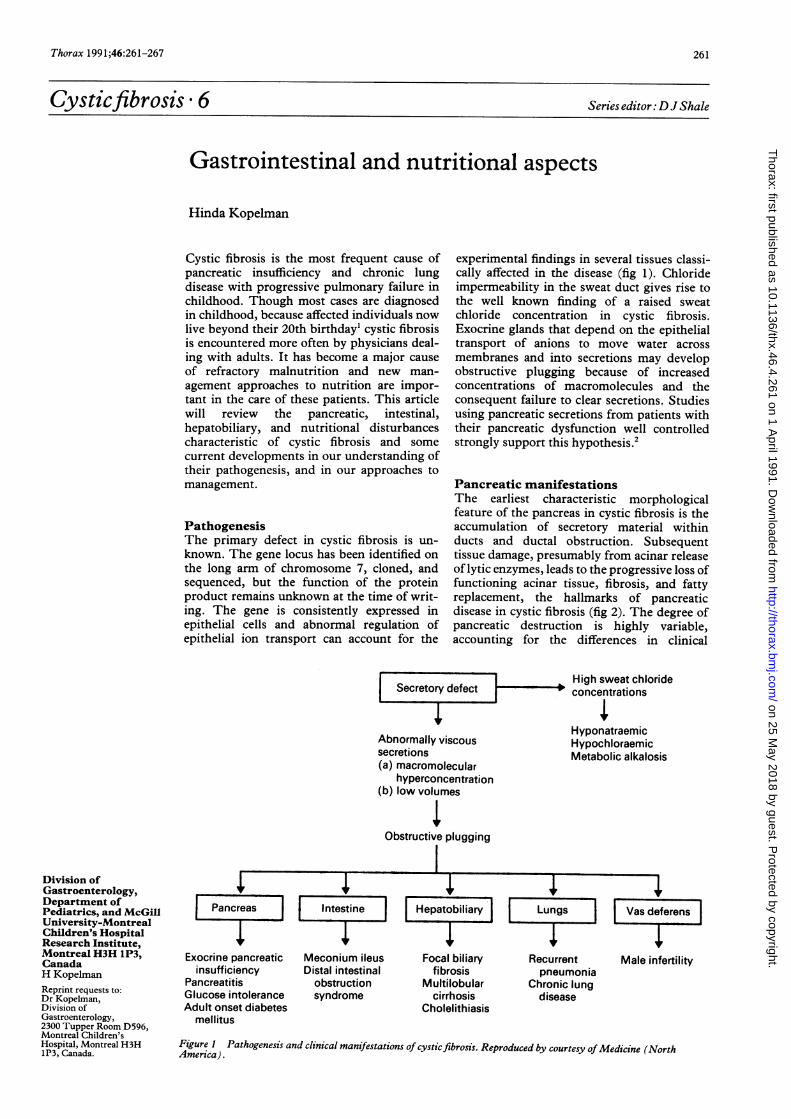
experimental findings in several tissues classi-cally affected in the disease (fig 1). Chlorideimpermeability in the sweat duct gives rise tothe well known finding of a raised sweatchloride concentration in cystic fibrosis.Exocrine glands that depend on the epithelialtransport of anions to move water acrossmembranes and into secretions may developobstructive plugging because of increasedconcentrations of macromolecules and theconsequent failure to clear secretions. Studiesusing pancreatic secretions from patients withtheir pancreatic dysfunction well controlledstrongly support this hypothesis.2
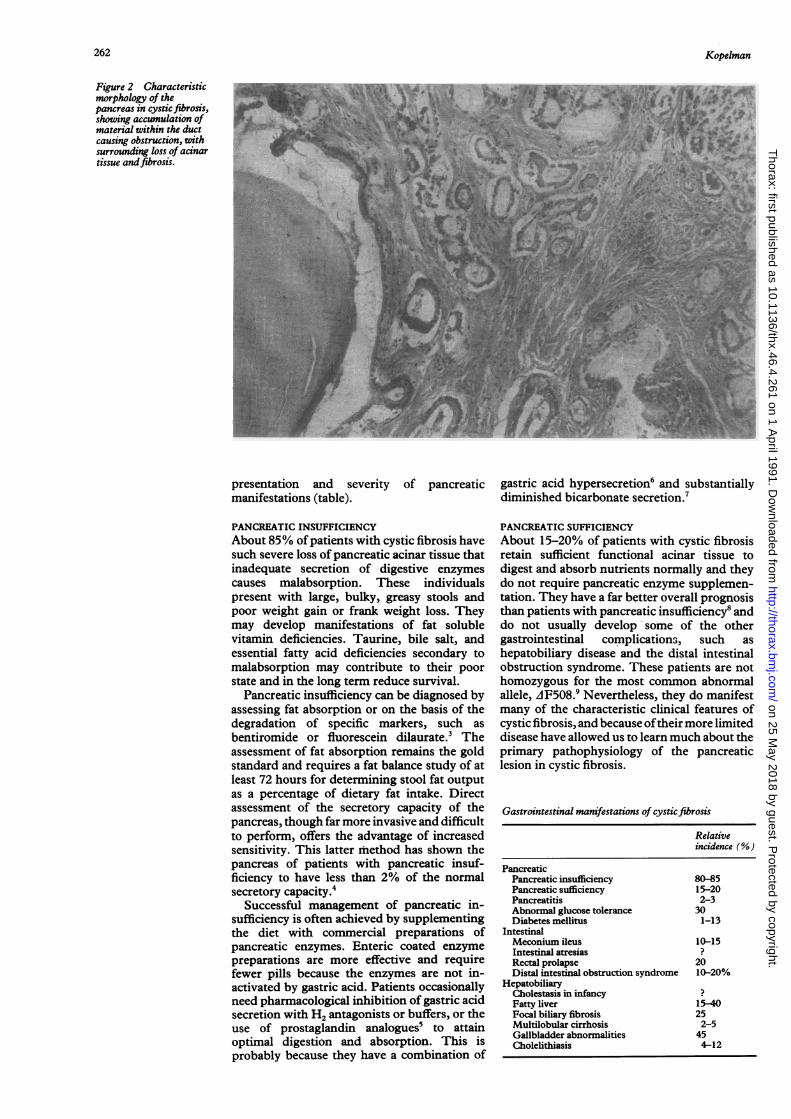
Pancreatic manifestationsThe earliest characteristic morphologicalfeature of the pancreas in cystic fibrosis is theaccumulation of secretory material withinducts and ductal obstruction. Subsequenttissue damage, presumably from acinar releaseof lytic enzymes, leads to the progressive loss offunctioning acinar tissue, fibrosis, and fattyreplacement, the hallmarks of pancreaticdisease in cystic fibrosis (fig 2). The degree ofpancreatic destruction is highly variable,accounting for the differences in clinical
Secretory defect |-
Abnormally viscoussecretions(a) macromolecular
hyperconcentration(b) low volumes
Division ofGastroenterology,Department ofPediatrics, and McGillUniversity-MontrealChildren's HospitalResearch Institute,Montreal H3H 1P3,CanadaH KopelmanReprint requests to:Dr Kopelman,Division ofGastroenterology,2300 Tupper Room D596,Montreal Children'sHospital, Montreal H3H1P3, Canada.
High sweat chlorideconcentrations
HyponatraemicHypochloraemicMetabolic alkalosis
Obstructive plugging
...obiiary_ Z eens
Exocrine pancreaticinsufficiency
PancreatitisGlucose intoleranceAdult onset diabetes
mellitus
Meconium ileusDistal intestinal
obstructionsyndrome
Focal biliaryfibrosis
Multilobularcirrhosis
Cholelithiasis
Recurrentpneumonia
Chronic lungdisease
Male infertility
Figure 1 Pathogenesis and clinical manifestations of cystic fibrosis. Reproduced by courtesy ofMedicine (NorthAmerica).
261
Cystic brosis - 6 Series editor:DJ Shale
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from
Kopelman
Figure 2 Characteristicmorphology of thepancreas in cysticfibrosis,showing accumulation ofmaterial within the ductcausing obstruction, withsurrounding loss of acinartissue andfibrosis.
presentation and severitymanifestations (table).
of pancreatic gastric acid hypersecretion6 and substantiallydiminished bicarbonate secretion.7
PANCREATIC INSUFFICIENCYAbout 85% of patients with cystic fibrosis havesuch severe loss of pancreatic acinar tissue thatinadequate secretion of digestive enzymescauses malabsorption. These individualspresent with large, bulky, greasy stools andpoor weight gain or frank weight loss. Theymay develop manifestations of fat solublevitamin deficiencies. Taurine, bile salt, andessential fatty acid deficiencies secondary tomalabsorption may contribute to their poorstate and in the long term reduce survival.
Pancreatic insufficiency can be diagnosed byassessing fat absorption or on the basis of thedegradation of specific markers, such asbentiromide or fluorescein dilaurate.3 Theassessment of fat absorption remains the goldstandard and requires a fat balance study of atleast 72 hours for determining stool fat outputas a percentage of dietary fat intake. Directassessment of the secretory capacity of thepancreas, though far more invasive and difficultto perform, offers the advantage of increasedsensitivity. This latter method has shown thepancreas of patients with pancreatic insuf-ficiency to have less than 2% of the normalsecretory capacity.4
Successful management of pancreatic in-sufficiency is often achieved by supplementingthe diet with commercial preparations ofpancreatic enzymes. Enteric coated enzymepreparations are more effective and requirefewer pills because the enzymes are not in-activated by gastric acid. Patients occasionallyneed pharmacological inhibition of gastric acidsecretion with H2 antagonists or buffers, or theuse of prostaglandin analogues5 to attainoptimal digestion and absorption. This isprobably because they have a combination of
PANCREATIC SUFFICIENCYAbout 15-20% of patients with cystic fibrosisretain sufficient functional acinar tissue todigest and absorb nutrients normally and theydo not require pancreatic enzyme supplemen-tation. They have a far better overall prognosisthan patients with pancreatic insufficiency8 anddo not usually develop some of the othergastrointestinal complicationS, such ashepatobiliary disease and the distal intestinalobstruction syndrome. These patients are nothomozygous for the most common abnormalallele, AF508.9 Nevertheless, they do manifestmany of the characteristic clinical features ofcystic fibrosis, and because oftheir more limiteddisease have allowed us to learn much about theprimary pathophysiology of the pancreaticlesion in cystic fibrosis.
Gastrointestinal manifestations of cystic fibrosis
Relativeincidence (%)
PancreaticPancreatic insufficiencyPancreatic sufficiencyPancreatitisAbnormal glucose toleranceDiabetes mellitus
IntestinalMeconium ileusIntestinal atresiasRectal prolapseDistal intestinal obstruction syndrome
HepatobiliaryCholestasis in infancyFatty liverFocal biliary fibrosisMultilobular cirrhosisGallbladder abnormalitiesCholelithiasis
80-8515-202-3301-13
10-15
2010-20%
15-40252-5454-12
262
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from
Gastrointestinal and nutritional aspects
PANCREATIC STIMULATION TEST
CONTINUOUSGASTRIC ASPIRATION
A
STOMACH AMPULLA OF
AiLIl j VATER
A
S
A
S
A
0
A
- lt ** tl;U t t 1;* n't IJh1II t ts1A1*t'lII1ulzllTI JII] I I fllII II I II I l
PI PIDUODENALASPIRATION
because of duct obstruction and acinar releaseof enzymes. They often have a milder clinicalcourse without all the features of cystic fibrosisand indeed the disease may not be diagnosed.Recurrent pancreatitis should be therefore anindication for sweat testing. About 15% ofpatients with cystic fibrosis who have pancreatic
LT sufficiency may suffer from clinical pancreatitis.
DIABETES MELLITUSProgressive pancreatic fibrosis ultimately dis-rupts pancreatic islet cell function. At least30% of patients with pancreatic insufficiencywill have an abnormal tolerance to glucoseloads. Frank (. .abetes mellitus is less frequentand tends to occur later in the course of thedisease. Its clinical presentation, diagnosis, andmanagement are similar to the idiopathic adultonset form of diabetes mellitus.
BSP INFUSION
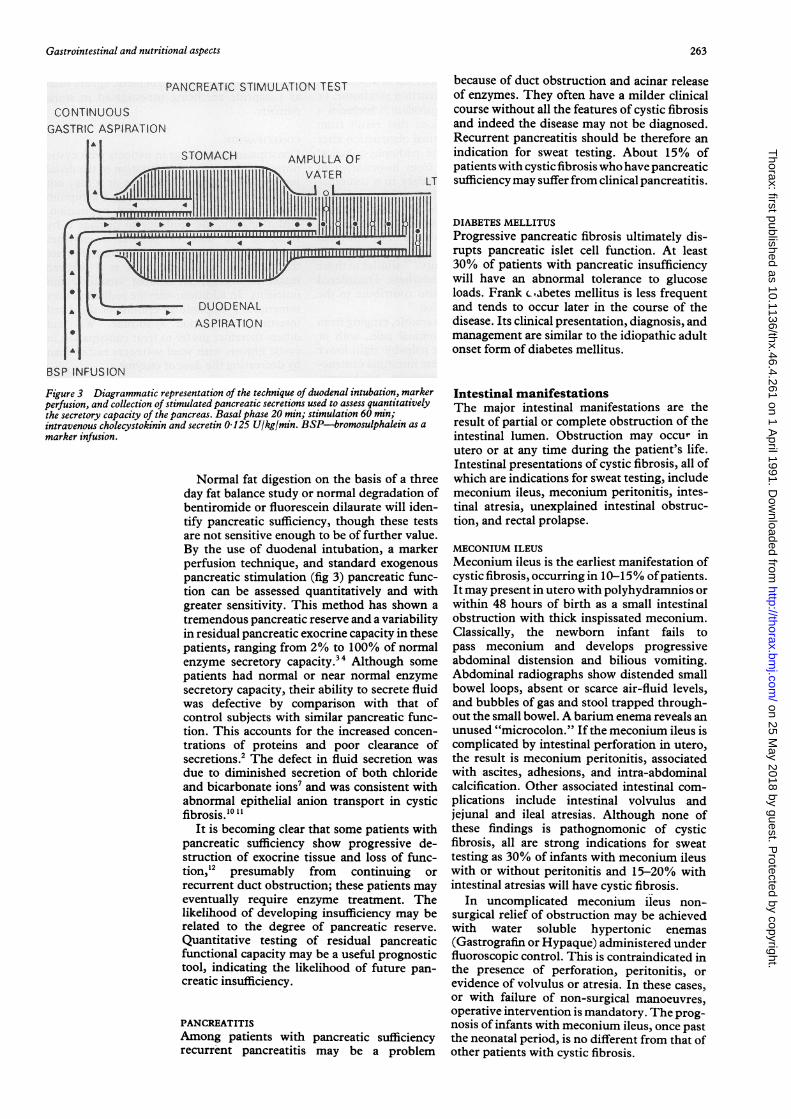
Figure 3 Diagrammatic representation of the technique of duodenal intubation, markerperfusion, and collection of stimulated pancreatic secretions used to assess quantitativelythe secretory capacity of the pancreas. Basal phase 20 min; stimulation 60 min;intravenous cholecystokinin and secretin 0 125 U/kg/min. BSP-bromosulphalein as amarker infusion.
Normal fat digestion on the basis of a threeday fat balance study or normal degradation ofbentiromide or fluorescein dilaurate will iden-tify pancreatic sufficiency, though these testsare not sensitive enough to be of further value.By the use of duodenal intubation, a markerperfusion technique, and standard exogenouspancreatic stimulation (fig 3) pancreatic func-tion can be assessed quantitatively and withgreater sensitivity. This method has shown atremendous pancreatic reserve and a variabilityin residual pancreatic exocrine capacity in thesepatients, ranging from 2% to 100% of normalenzyme secretory capacity.34 Although somepatients had normal or near normal enzymesecretory capacity, their ability to secrete fluidwas defective by comparison with that ofcontrol subjects with similar pancreatic func-tion. This accounts for the increased concen-trations of proteins and poor clearance ofsecretions.2 The defect in fluid secretion wasdue to diminished secretion of both chlorideand bicarbonate ions7 and was consistent withabnormal epithelial anion transport in cysticfibrosis.'0 11
It is becoming clear that some patients withpancreatic sufficiency show progressive de-struction of exocrine tissue and loss of func-tion,12 presumably from continuing orrecurrent duct obstruction; these patients mayeventually require enzyme treatment. Thelikelihood of developing insufficiency may berelated to the degree of pancreatic reserve.Quantitative testing of residual pancreaticfunctional capacity may be a useful prognostictool, indicating the likelihood of future pan-creatic insufficiency.
PANCREATITISAmong patients with pancreatic sufficiencyrecurrent pancreatitis may be a problem
Intestinal manifestationsThe major intestinal manifestations are theresult of partial or complete obstruction of theintestinal lumen. Obstruction may occur inutero or at any time during the patient's life.Intestinal presentations of cystic fibrosis, all ofwhich are indications for sweat testing, includemeconium ileus, meconium peritonitis, intes-tinal atresia, unexplained intestinal obstruc-tion, and rectal prolapse.
MECONIUM ILEUSMeconium ileus is the earliest manifestation ofcystic fibrosis, occurring in 10-15°% ofpatients.It may present in utero with polyhydramnios orwithin 48 hours of birth as a small intestinalobstruction with thick inspissated meconium.Classically, the newborn infant fails topass meconium and develops progressiveabdominal distension and bilious vomiting.Abdominal radiographs show distended smallbowel loops, absent or scarce air-fluid levels,and bubbles of gas and stool trapped through-out the small bowel. A barium enema reveals anunused "microcolon." If the meconium ileus iscomplicated by intestinal perforation in utero,the result is meconium peritonitis, associatedwith ascites, adhesions, and intra-abdominalcalcification. Other associated intestinal com-plications include intestinal volvulus andjejunal and ileal atresias. Although none ofthese findings is pathognomonic of cysticfibrosis, all are strong indications for sweattesting as 30% of infants with meconium ileuswith or without peritonitis and 15-20% withintestinal atresias will have cystic fibrosis.
In uncomplicated meconium ileus non-surgical relief of obstruction may be achievedwith water soluble hypertonic enemas(Gastrografin or Hypaque) administered underfluoroscopic control. This is contraindicated inthe presence of perforation, peritonitis, orevidence of volvulus or atresia. In these cases,or with failure of non-surgical manoeuvres,operative intervention is mandatory. The prog-nosis of infants with meconium ileus, once pastthe neonatal period, is no different from that ofother patients with cystic fibrosis.
I I I I I I t I I I I -9-1 1-1-1 1-1 I 1-1-1 I I I I I I I I I I I I I I i I I I I I I I I i I I I01- .1ullollm ilim illillullill
263
r }. * t * t *I.0- * I-illl.EUI-IW 1
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from

Kopelman
DISTAL INTESTINAL OBSTRUCTION SYNDROMEThe distal intestinal obstruction syndrome, orthe "meconium ileus equivalent," includes arange of clinical conditions that result frompartial or complete intestinal obstruction afterthe neonatal period. The pathophysiologicalfeatures probably arise from inspissation ofintestinal secretions secondary to a combina-tion ofpancreatic insufficiency with diminishedproteolytic degradation of mucoproteinaceoussecretions and poor clearance of concentrated,dehydrated intestinal contents. The intestinalmucosal epithelial cell possesses defects inchloride and fluid transport"'6 similar to thoseseen in epithelial cells elsewhere. Disorderedintestinal motility may also contribute to theoccurrence of this condition.'7
Presentation is highly variable, ranging fromrecurrent cramping abdominal pain, with orwithout an asymptomatic palpable right lowerquadrant mass, to complete intestinal obstruc-tion with abdominal distension, tenderness,and vomiting. It is often difficult to differentiatefrom the far less common conditions requiringsurgical intervention, such as appendicitis,appendiceal abscess, intussusception andcaecal neoplasm. The detection of largeamounts of faecal material in the right lowerquadrant by abdominal radiography orGastrograffin enema, abdominal ultrasound, orcomputed tomography and resolution withtreatment for the distal intestinal obstructionsyndrome may help diagnostically.
Surgical intervention is rarely required.Medical management consists of increasedamounts of pancreatic enzyme replacement;stool softeners such as mineral oil, psylliumhydrophilic mucilloid, and fibre; Gastrograffinand other enemas; and, in the past, oral or rectalN-acetylcysteine. In the absence of completeintestinal obstruction, balanced isotonic elec-trolyte solutions for gastrointestinal lavage areadministered orally or by nasogastric infusion
Figure 4 Characteristicmorphology of the liver incysticfibrosis, showingfocal bile ductproliferation andaccumulation of materialwithin ductules.
with excellent results."8 Prokinetic agents suchas Cisapride are being investigated in somepatients.
CONSTIPATIONConstipation may occur in patients with cysticfibrosis. It may be a manifestation of the distalintestinal obstruction syndrome or it may notbe related to cystic fibrosis, being a symptomseen commonly in the general population.Unfortunately, the tendency to manage it byreducing the dose of pancreatic enzymesinduces fat malabsorption. This may alleviatethe constipation but the price is a reducedintake of energy, fat soluble vitamins, andnutrients. In addition, enzyme reduction maysometimes precipitate an episode of the distalintestinal obstruction syndrome. We andothers therefore prefer to treat constipation incystic fibrosis with stool softeners rather thanby decreasing the dose of enzyme.
RECTAL PROLAPSERectal prolapse occurs in about 20% ofpatientsand may be the first manifestation ofthe disease.It is usually recurrent in the first few years oflife, spontaneously resolves by 5 years of age,and often improves once treatment for pan-creatic insufficiency is initiated. It rarelyrequires surgical intervention. Rectal prolapsemay also occur in the absence of pancreaticinsufficiency. In these circumstances attemptsto diminish constipation or straining duringbowel movements, or both, may be of benefit.
OTHER GASTROINTESTINAL PROBLEMSPatients with cystic fibrosis may have othergastrointestinal problems, which may or maynot be related to cystic fibrosis. Gastro-oesophageal reflux is extremely common andoesophagitis and peptic ulcer disease occur.There have also been reports of coeliac diseaseand Crohn's disease.
*/ *# .s ,.. ,
;oo'
4's* } t F! n
ss .. Ss ..IM
.¶;..:
. .4
In4:j
264
Ift V
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from
Gastrointestinal and nutritional aspects
PATHOLOGICAL, RADIOLOGICAL, ANDFUNCTIONAL ABNORMALITIESFeatures of the intestinal mucosa sufficientlycharacteristic to be diagnostic of cystic fibrosisinclude increased numbers of mucin filledgoblet cells, dilated mucin filled crypts, andeosinophilic casts. Common radiological find-ings include thickened duodenal folds, nodularfilling defects, and variable dilatation of intes-tinal loops. These findings probably have littleclinical importance and should not be inter-preted as signs of "duodenitis," ulceration, orinflammatory or infiltrative disease without fur-ther confirmation.
Selective intestinal absorptive defects inamino acids and bile acids have been reported,but remain to be confirmed; clinicallyimportant defects in the structure and functionofthe intestinal mucosa are not evident. Villousstructure is intact, D-xylose absorption isnormal, and intestinal lactase activity is normalor even increased. Lactose intolerance mayoccur, but its frequency reflects the normalethnic and age related frequency in the popula-tion and it is unrelated to cystic fibrosis.
Hepatobiliary manifestationsThe incidence of hepatobiliary problems incystic fibrosis are listed in the table. The morefrequent abnormalities have little effect onoverall health and wellbeing. They include (1)obstructive jaundice in infancy, probablysecondary to biliary plugging, which oftenresolves and is not necessarily associated withliver disease later in life; (2) hepatomegaly dueto fatty change, which may be present evenwithout appreciable malnutrition; (3) a non-
functioning or "micro" gall bladder, unas-
sociated with clinical symptoms.The characteristic histological lesion in the
liver in cystic fibrosis is focal biliary fibrosis,which is often present in symptomless patientswith no biochemical evidence of liver disease.It is characterised by inspissated eosinophilicmaterial in dilated ductules, bile duct prolifera-tion, and variable fibrosis (fig 4). This probably
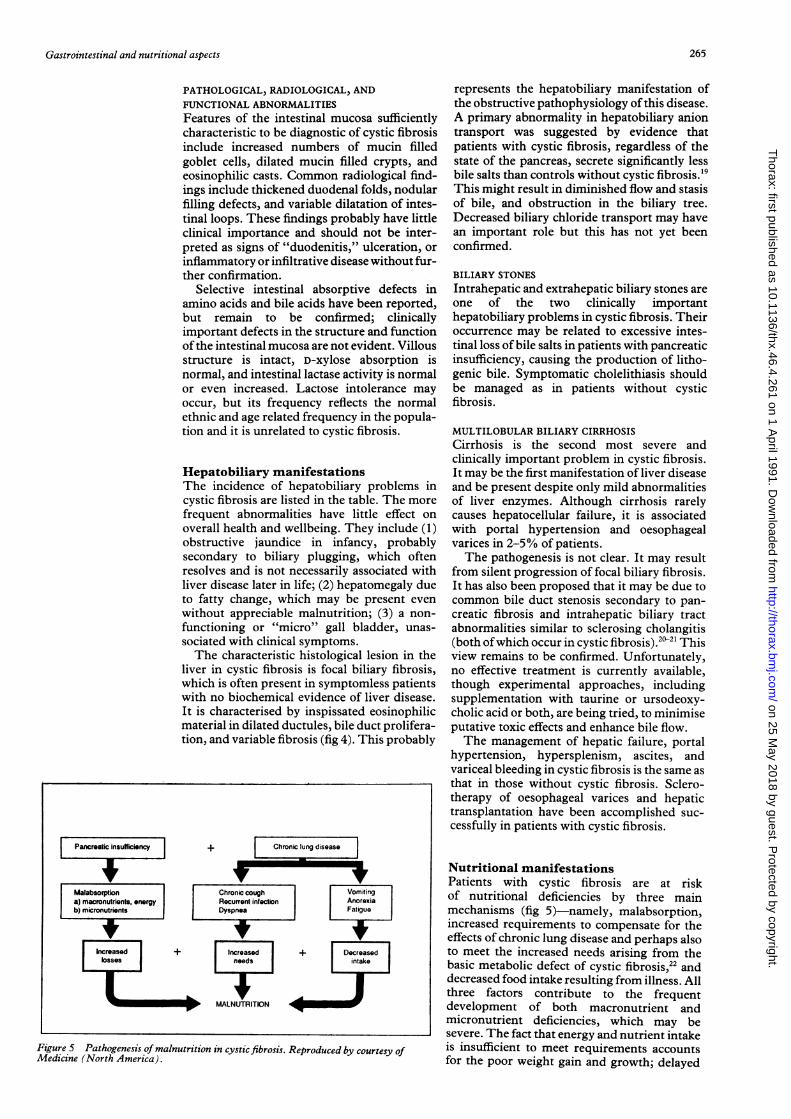
Figure 5 Pathogenesis of malnutrition in cystic fibrosis. Reproduced by courtesy ofMedicine (North America).
represents the hepatobiliary manifestation ofthe obstructive pathophysiology ofthis disease.A primary abnormality in hepatobiliary aniontransport was suggested by evidence thatpatients with cystic fibrosis, regardless of thestate of the pancreas, secrete significantly lessbile salts than controls without cystic fibrosis.'9This might result in diminished flow and stasisof bile, and obstruction in the biliary tree.Decreased biliary chloride transport may havean important role but this has not yet beenconfirmed.
BILIARY STONESIntrahepatic and extrahepatic biliary stones areone of the two clinically importanthepatobiliary problems in cystic fibrosis. Theiroccurrence may be related to excessive intes-tinal loss of bile salts in patients with pancreaticinsufficiency, causing the production of litho-genic bile. Symptomatic cholelithiasis shouldbe managed as in patients without cysticfibrosis.
MULTILOBULAR BILIARY CIRRHOSISCirrhosis is the second most severe andclinically important problem in cystic fibrosis.It may be the first manifestation of liver diseaseand be present despite only mild abnormalitiesof liver enzymes. Although cirrhosis rarelycauses hepatocellular failure, it is associatedwith portal hypertension and oesophagealvarices in 2-5% of patients.The pathogenesis is not clear. It may result
from silent progression of focal biliary fibrosis.It has also been proposed that it may be due tocommon bile duct stenosis secondary to pan-creatic fibrosis and intrahepatic biliary tractabnormalities similar to sclerosing cholangitis(both ofwhich occur in cystic fibrosis).2"" Thisview remains to be confirmed. Unfortunately,no effective treatment is currently available,though experimental approaches, includingsupplementation with taurine or ursodeoxy-cholic acid or both, are being tried, to minimiseputative toxic effects and enhance bile flow.The management of hepatic failure, portal
hypertension, hypersplenism, ascites, andvariceal bleeding in cystic fibrosis is the same asthat in those without cystic fibrosis. Sclero-therapy of oesophageal varices and hepatictransplantation have been accomplished suc-cessfully in patients with cystic fibrosis.
Nutritional manifestationsPatients with cystic fibrosis are at riskof nutritional deficiencies by three mainmechanisms (fig 5)-namely, malabsorption,increased requirements to compensate for theeffects of chronic lung disease and perhaps alsoto meet the increased needs arising from thebasic metabolic defect of cystic fibrosis,22 anddecreased food intake resulting from illness. Allthree factors contribute to the frequentdevelopment of both macronutrient andmicronutrient deficiencies, which may besevere. The fact that energy and nutrient intakeis insufficient to meet requirements accountsfor the poor weight gain and growth; delayed
265
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from
Kopelman
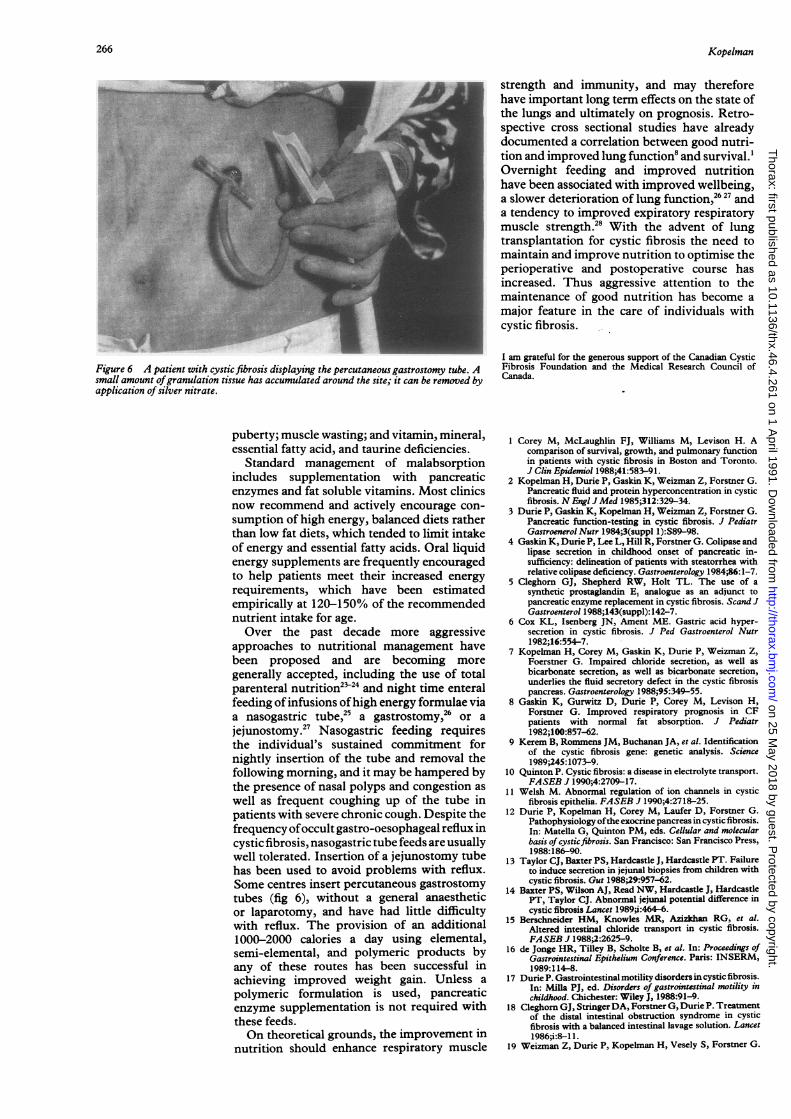
Figure 6 A patient with cysticfibrosis displaying the percutaneous gastrostomy tube. Asmall amount ofgranulation tissue has accumulated around the site; it can be removed byapplication of silver nitrate.
puberty; muscle wasting; and vitamin, mineral,essential fatty acid, and taurine deficiencies.
Standard management of malabsorptionincludes supplementation with pancreaticenzymes and fat soluble vitamins. Most clinicsnow recommend and actively encourage con-
sumption of high energy, balanced diets ratherthan low fat diets, which tended to limit intakeof energy and essential fatty acids. Oral liquidenergy supplements are frequently encouragedto help patients meet their increased energy
requirements, which have been estimatedempirically at 120-150% of the recommendednutrient intake for age.
Over the past decade more aggressiveapproaches to nutritional management havebeen proposed and are becoming more
generally accepted, including the use of totalparenteral nutrition2524 and night time enteralfeeding of infusions ofhigh energy formulae viaa nasogastric tube,25 a gastrostomy,26 or a
jejunostomy.2' Nasogastric feeding requiresthe individual's sustained commitment fornightly insertion of the tube and removal thefollowing morning, and it may be hampered bythe presence of nasal polyps and congestion as
well as frequent coughing up of the tube inpatients with severe chronic cough. Despite thefrequency ofoccult gastro-oesophageal reflux incystic fibrosis, nasogastric tube feeds are usuallywell tolerated. Insertion of a jejunostomy tubehas been used to avoid problems with reflux.Some centres insert percutaneous gastrostomytubes (fig 6), without a general anaestheticor laparotomy, and have had little difficultywith reflux. The provision of an additional1000-2000 calories a day using elemental,semi-elemental, and polymeric products byany of these routes has been successful inachieving improved weight gain. Unless a
polymeric formulation is used, pancreaticenzyme supplementation is not required withthese feeds.On theoretical grounds, the improvement in
nutrition should enhance respiratory muscle
strength and immunity, and may thereforehave important long term effects on the state ofthe lungs and ultimately on prognosis. Retro-spective cross sectional studies have alreadydocumented a correlation between good nutri-tion and improved lung function8 and survival.'Overnight feeding and improved nutritionhave been associated with improved wellbeing,a slower deterioration of lung function,26 27 anda tendency to improved expiratory respiratorymuscle strength.28 With the advent of lungtransplantation for cystic fibrosis the need tomaintain and improve nutrition to optimise theperioperative and postoperative course hasincreased. Thus aggressive attention to themaintenance of good nutrition has become amajor feature in the care of individuals withcystic fibrosis.
I am grateful for the generous support of the Canadian CysticFibrosis Foundation and the Medical Research Council ofCanada.
1 Corey M, McLaughlin FJ, Williams M, Levison H. Acomparison of survival, growth, and pulmonary functionin patients with cystic fibrosis in Boston and Toronto.J Clin Epidemiol 1988;41:583-91.
2 Kopelman H, Durie P, Gaskin K, Weizman Z, Forstner G.Pancreatic fluid and protein hyperconcentration in cysticfibrosis. N Engi J Med 1985;312:329-34.
3 Durie P, Gaskin K, Kopelman H, Weizman Z, Forsmer G.Pancreatic function-testing in cystic fibrosis. J PediatrGastroenerol Nutr 1984;3(suppl 1):S89-98.
4 Gaskin K, Durie P, Lee L, Hill R, Forstner G. Colipase andlipase secretion in childhood onset of pancreatic in-sufficiency: delineation of patients with steatorrhea withrelative colipase deficiency. Gastroenterology 1984;86:1-7.
5 Cleghom GJ, Shepherd RW, Holt TL. The use of asynthetic prostaglandin E, analogue as an adjunct topancreatic enzyme replacement in cystic fibrosis. Scand JGastroenterol 1988;143(suppl): 142-7.
6 Cox KL, Isenberg JN, Ament ME. Gastric acid hyper-secretion in cystic fibrosis. J Ped Gastroenterol Nutr1982;16:554-7.
7 Kopelman H, Corey M, Gaskin K, Durie P, Weizman Z,Foerstner G. Impaired chloride secretion, as well asbicarbonate secretion, as well as bicarbonate secretion,underlies the fluid secretory defect in the cystic fibrosispancreas. Gastroenterology 1988;95:349-55.
8 Gaskin K, Gurwitz D, Durie P, Corey M, Levison H,Forstner G. Improved respiratory prognosis in CFpatients with normal fat absorption. J Pediatr1982;100:857-62.
9 Kerem B, Rommens JM, Buchanan JA, et al. Identificationof the cystic fibrosis gene: genetic analysis. Science1989;245: 1073-9.
10 Quinton P. Cystic fibrosis: a disease in electrolyte transport.FASEB J 1990;4:2709-17.
11 Welsh M. Abnormal regulation of ion channels in cysticfibrosis epithelia. FASEB J 1990;4:2718-25.
12 Durie P, Kopelman H, Corey M, Laufer D, Forstner G.Pathophysiology ofthe exocrine pancreas in cystic fibrosis.In: Matella G, Quinton PM, eds. Cellular and molecularbasis of cysticfibrosis. San Francisco: San Francisco Press,1988:186-90.
13 Taylor CJ, Baxter PS, Hardcastle J, Hardcastle PT. Failureto induce secretion in jejunal biopsies from children withcystic fibrosis. Gut 1988;29:957-62.
14 Baxter PS, Wilson AJ, Read NW, Hardcastle J, HardcastlePT, Taylor CJ. Abnormal jejural potential difference incystic fibrosis Lancet 1989;i:464-6.
15 Berschneider HM, Knowles MR, Azizkhan RG, et al.Altered intestinal chloride transport in cystic fibrosis.FASEB J 1988;2:2625-9.
16 de Jonge HR, Tilley B, Scholte B, et al. In: Proceedings ofGastrointestinal Epithelium Conference. Paris: INSERM,1989:114-8.
17 Durie P. Gastrointestinal motility disorders in cystic fibrosis.In: Milla PJ, ed. Disorders of gastrointestinal motility inchildhood. Chichester: Wiley J, 1988:91-9.
18 Cleghorn GJ, StringerDA, Forstner G, Durie P. Treatmentof the distal intestinal obstruction syndrome in cysticfibrosis with a balanced intestinal lavage solution. Lancet1986;i:8-1 1.
19 Weizman Z, Durie P, Kopelman H, Vesely S, Forstner G.
266
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from
Gastrointestinal and nutritional aspects
Bile acid secretion in cystic fibrosis-evidence for a primarydefect. Gut 1986;27:1362-8.
20 Gaskin KJ, Waters DLM, Howman-Giles R, et al. Liverdisease and common bile duct stenosis in cystic fibrosis. NEnglJ Med 1988;318:340-6.
21 Strandvik B, Hjelte L, Gabrielsson N, Glaumann H.Sclerosing cholangitis in cystic fibrosis. Scand J Gastro-enterol 1988;23(suppl 143):121-4.
22 Shepherd RW, Holt TL, Vasques-Velasquez L, et al.Increased energy expenditure in young children withcystic fibrosis. Lancet 1988;i: 1300-3.
23 Shepherd R, Cooksley WGE, Cook WDD. Improvedgrowth and clinical nutritional therapy in cystic fibrosis.J Pediatr 1980;97:351-6.
24 Mansell AL, Andersen JC, Muttart CR, et al. Short-termpulmonary effects of total parenteral nutrition in children
with cystic fibrosis. JPediatr 1984;104:700-5.25 Scott RB, O'Laughlin EV, Gall DG. Gastroesophageal
reflux in patients with cystic fibrosis. J Pediatr1985;106:223-7.
26 Levy LD, Durie PR, Pencharz PB, Corey ML. Effects oflong-term nutritional rehabilitation on body compositionand clinical status in malnourished children and adoles-cents with cystic fibrosis. JPediatr 1985;107:225-30.
27 Boland MP, Stoski DS, MacDonald NE, Soucy P, Patrick J.Chronic jejunostomy feeding with a non-elemental for-mula in undernourished patients with cystic fibrosis.Lancet 1986:232-4.
28 Drury D, Pianosi P, Kopelman H, Charge D, Coates A. Theeffect of nutritional status on respiratory muscle strengthand work capacity in cystic fibrosis [abstract]. Pediatr Res1990:104A.
267
on 25 May 2018 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.46.4.261 on 1 A
pril 1991. Dow
nloaded from


















