CYANOTIC SPELLS paroxysmal hyperpnea hypoxic spells anoxic spells blue spells.
22
-
Upload
philip-kennedy -
Category
Documents
-
view
383 -
download
11
Transcript of CYANOTIC SPELLS paroxysmal hyperpnea hypoxic spells anoxic spells blue spells.

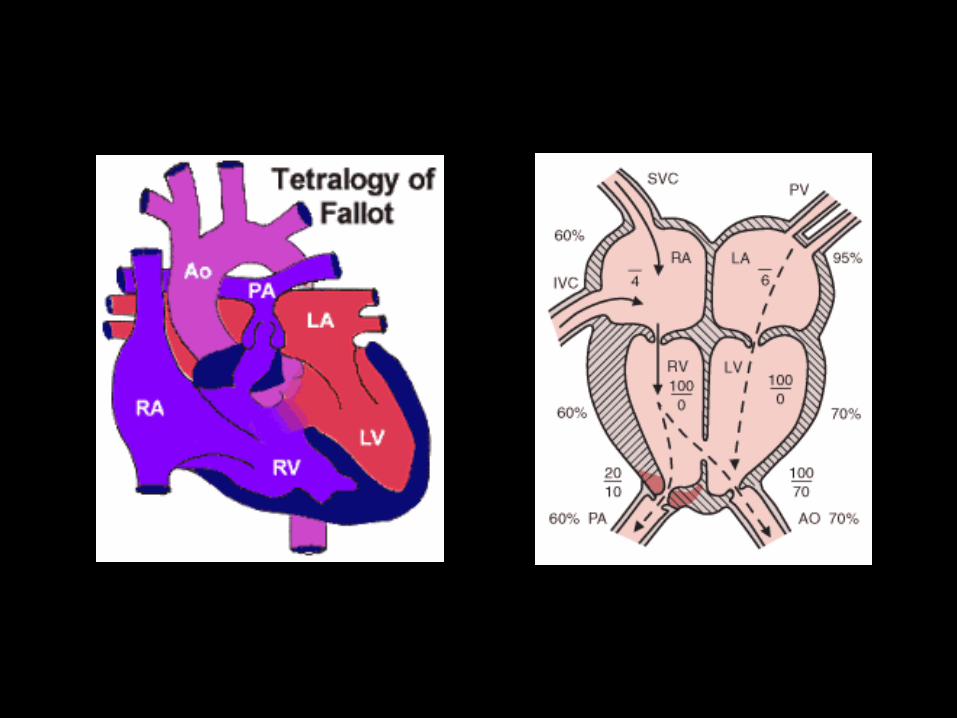
CYANOTIC SPELLS
• paroxysmal hyperpnea
• hypoxic spells
• anoxic spells
• blue spells
CYANOTIC SPELLS
rate & depth of respiration
increasing cyanosis
Limpness , syncope, -------- convulsions, CVA
------------------------------ DEATH
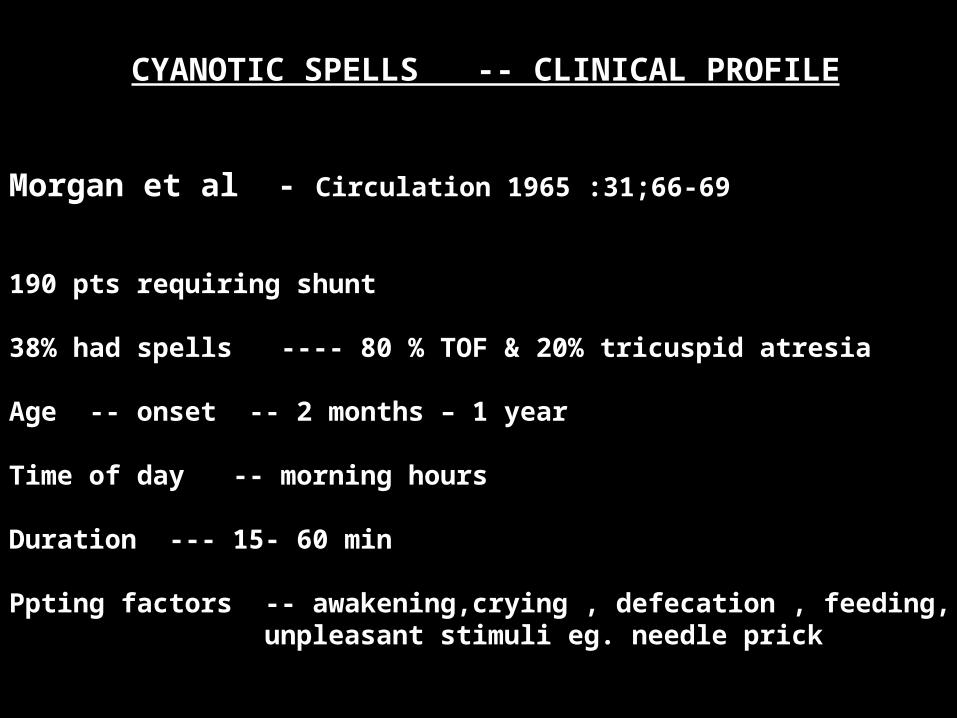
CYANOTIC SPELLS -- CLINICAL PROFILE
Morgan et al - Circulation 1965 :31;66-69
190 pts requiring shunt
38% had spells ---- 80 % TOF & 20% tricuspid atresia
Age -- onset -- 2 months – 1 year
Time of day -- morning hours
Duration --- 15- 60 min
Ppting factors -- awakening,crying , defecation , feeding, unpleasant stimuli eg. needle prick
CYANOTIC SPELLS -- CLINICAL PROFILE
• not always correlate with severity of TOF
• infrequent in high altitude natives
due to diminished sensitivity of respiratory centre to hypoxia
• frequency decreases after morning hours as respiratory centre gets adapted


CYANOTIC SPELLS -physiology
HYPERVENTILATION is the main factor
Normal – sleep is attended by reduction in ventilation
PaCO2 , PaO2,SaO2,pH
On waking up reverse occurs
CYANOTIC SPELLS -physiology
TOF
Sleep - reduced O2 demend --- better SaO2
Waking up --- ventilation, activity
PaCO2, SaO2, PaO2,pH
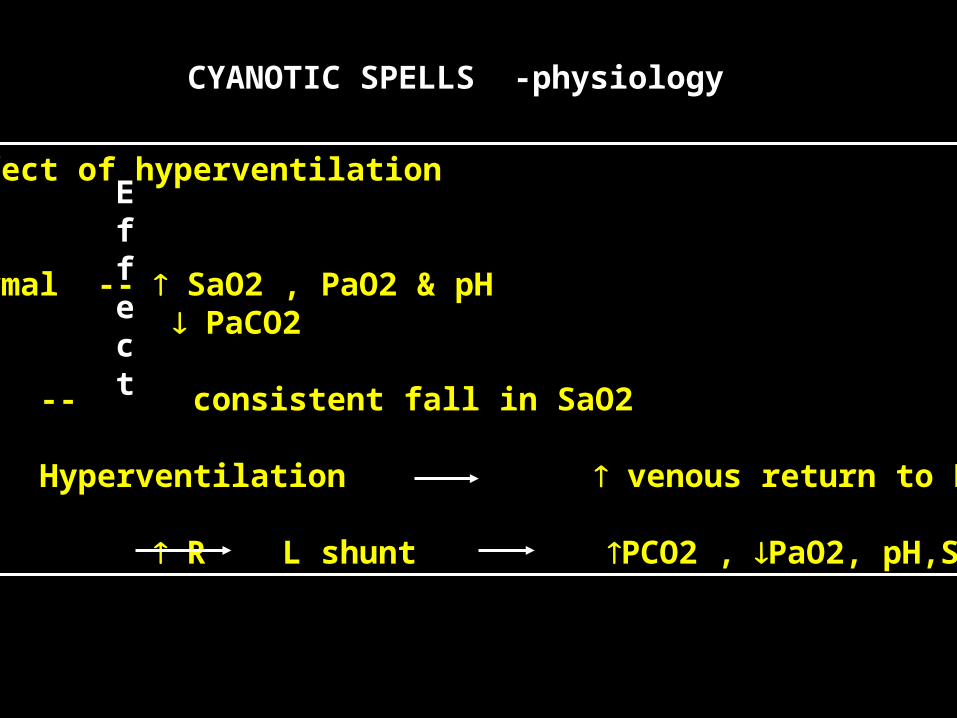
CYANOTIC SPELLS -physiology
Effect
Effect of hyperventilation
Normal -- SaO2 , PaO2 & pH PaCO2
TOF -- consistent fall in SaO2
Hyperventilation venous return to RV
R L shunt PCO2 , PaO2, pH,Sao2
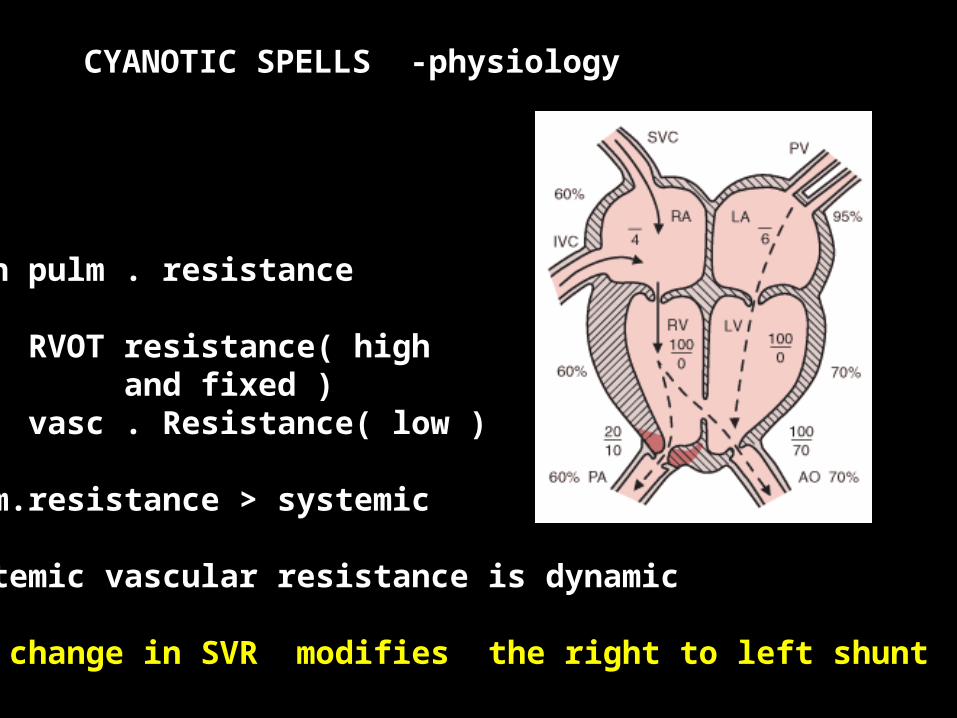
CYANOTIC SPELLS -physiology
TOF
High pulm . resistance
RVOT resistance( highand fixed )
vasc . Resistance( low )
Pulm.resistance > systemic
Systemic vascular resistance is dynamic
Any change in SVR modifies the right to left shunt
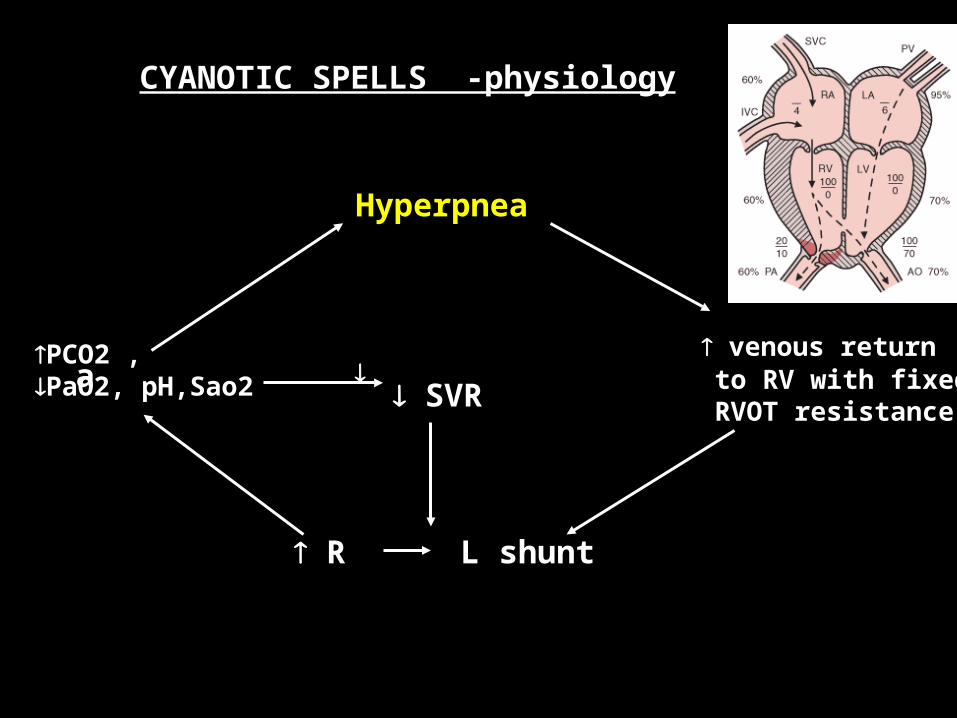
CYANOTIC SPELLS -physiology
Hyperpnea
venous return to RV with fixed RVOT resistance
R L shunt
aPCO2 , PaO2, pH,Sao2
SVR
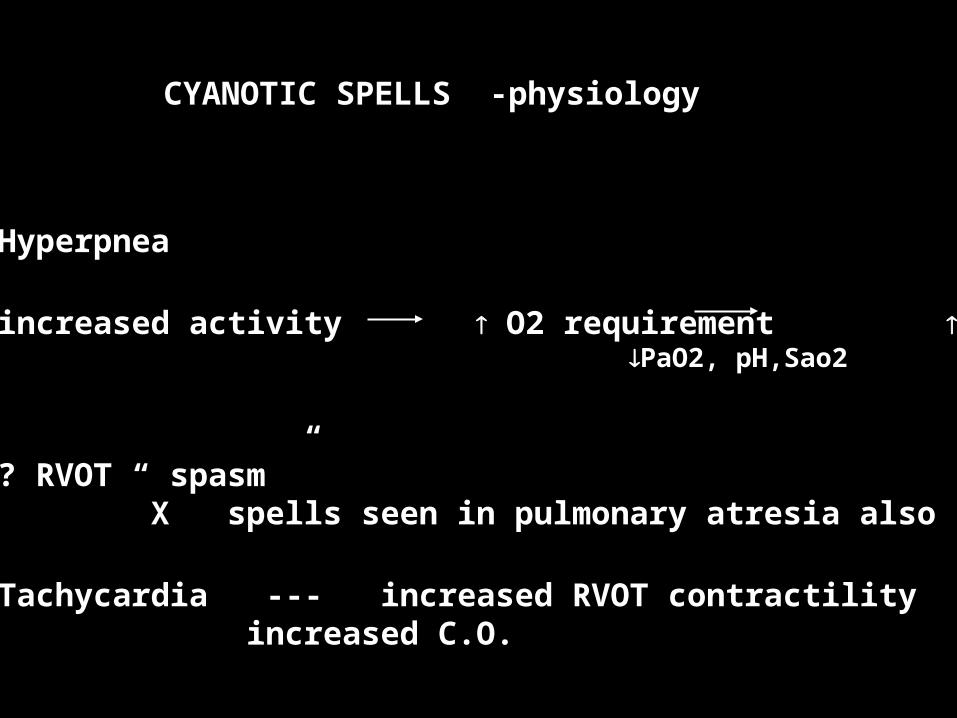
CYANOTIC SPELLS -physiology
• Hyperpnea
• increased activity O2 requirement PCO2 , PaO2, pH,Sao2
• ? RVOT “ spasm ”X spells seen in pulmonary atresia also
• Tachycardia --- increased RVOT contractilityincreased C.O.

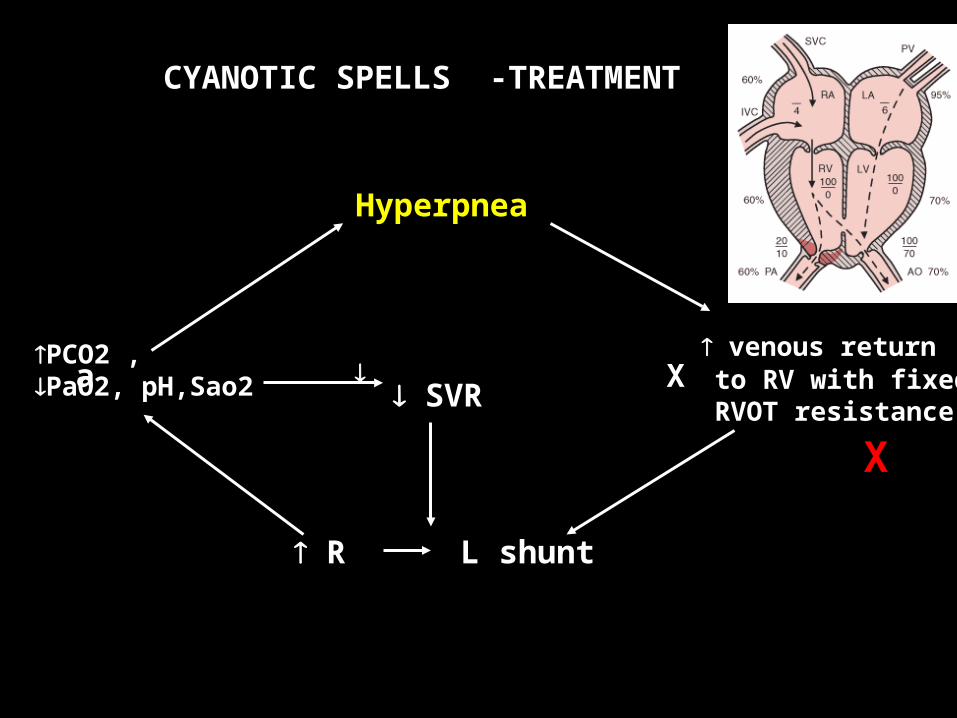
CYANOTIC SPELLS -TREATMENT
Hyperpnea
venous return to RV with fixed RVOT resistance
R L shunt
aPCO2 , PaO2, pH,Sao2
SVR
X -
CYANOTIC SPELLS -TREATMENT
Hyperpnea
venous return to RV with fixed RVOT resistance
R L shunt
aPCO2 , PaO2, pH,Sao2
SVRX
X

CYANOTIC SPELLS -TREATMENT
Hyperpnea
venous return to RV with fixed RVOT resistance
R L shunt
aPCO2 , PaO2, pH,Sao2
SVR x
CYANOTIC SPELLS -TREATMENT
• knee chest position
• O2 inhalation
• morphine
•propranolol
• alpha stimulants
• sodabicarb
• general anesthesia
• emergency shunt in recurrent spells
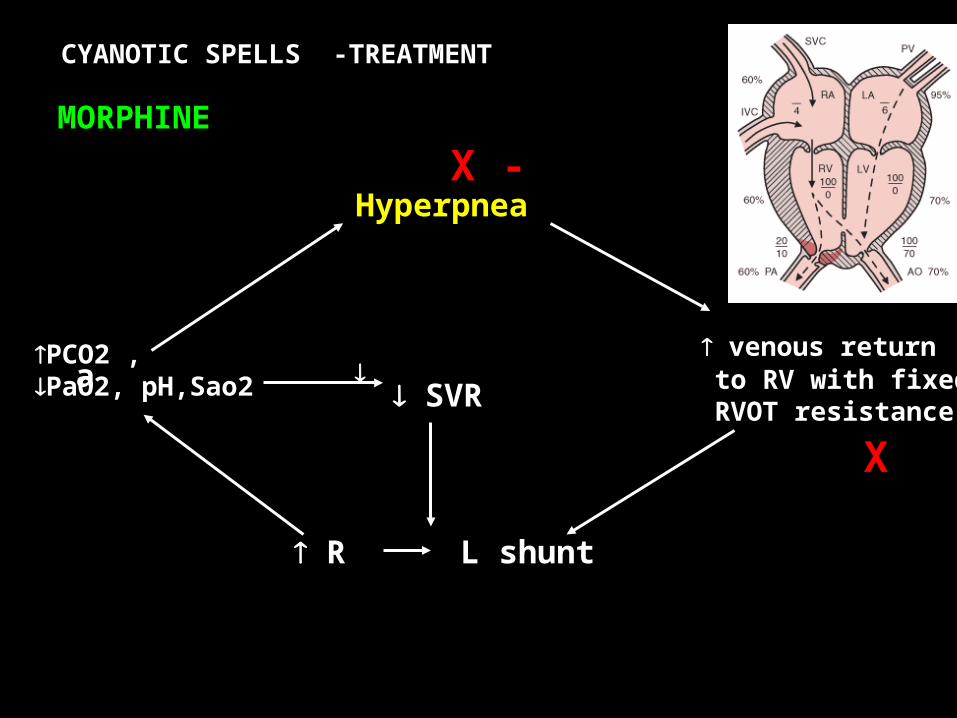
CYANOTIC SPELLS -TREATMENT
Hyperpnea
venous return to RV with fixed RVOT resistance
R L shunt
aPCO2 , PaO2, pH,Sao2
SVR
X - MORPHINE
X
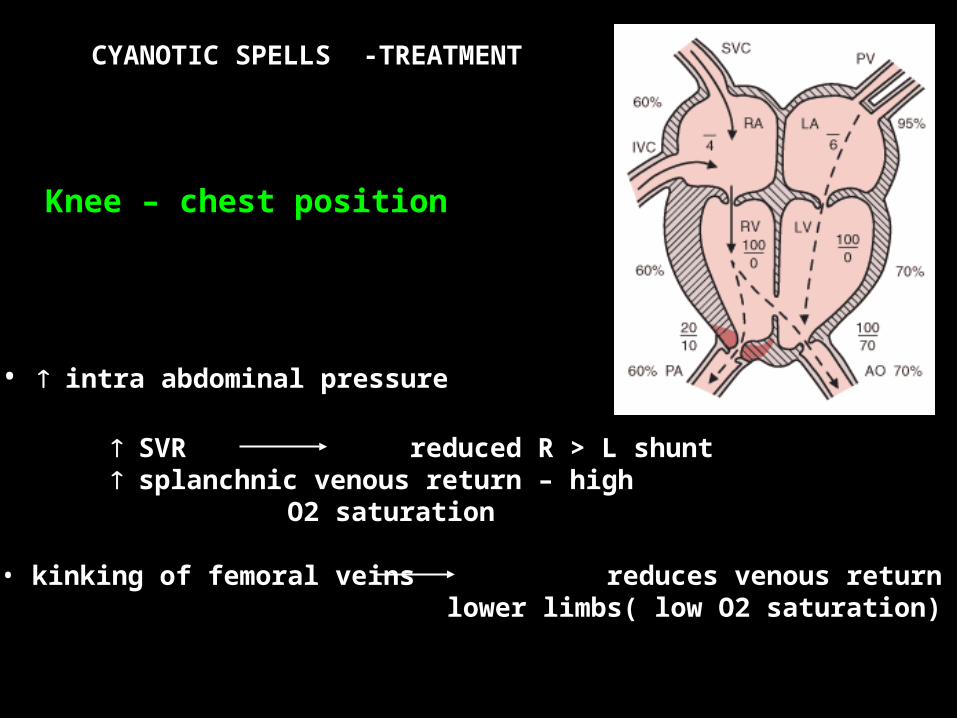
CYANOTIC SPELLS -TREATMENT
Knee – chest position
• intra abdominal pressure
SVR reduced R > L shunt splanchnic venous return – high
O2 saturation
• kinking of femoral veins reduces venous return lower limbs( low O2 saturation)
CYANOTIC SPELLS -TREATMENT
PROPRANOLOL
• 0.2 mg/kg IV
• reduces HR, RVOT contractility
• increases SVR
More useful in those with
• little cyanosis at rest• marked reduction in SaO2 with activity / hyperventilation
CYANOTIC SPELLS
RECURRENT SPELLS AT HOME –GET SPONTANEOUSLY ABORTED
SPELLS IN HOSPITALS — LAND UP IN ANESTHESIA
PARADOX