Treatment of Hepatitis B in Children (-) - NASPGHAN Homepage
1
2 3 4
5
6
7
The North American Society for Pediatric Gastroenterology, Hepatology and 8
Nutrition 9
Guideline for the Diagnosis and Management of Cyclic Vomiting Syndrome 10
11 12 13 14
Task Force: 15 16
B U.K. Li, Frank Lefevre, Gisela G. Chelimsky, Richard G. Boles, Suzanne P. Nelson, Donald 17 W. Lewis, Steve L.Linder, Robert M. Issenman, Colin 18
D. Rudolph 19 20
Coordinator: 21 22
Kathleen A. Adams B.S.N., R.N., President, Cyclic Vomiting Syndrome Association 23 24
NASPGHAN CVS Guidelines - 2
INTRODUCTION AND BACKGROUND 24
25
Cyclic vomiting syndrome (CVS) is a disorder characterized by recurrent, discrete, self-26
limited episodes of vomiting (1-3). Affected children usually experience a stereotypical pattern 27
of vomiting typified by a consistent time of onset, duration, and symptoms. The vomiting is 28
intense (six times/hour at the peak) often bilious (83% in some series), and accompanied by 29
disabling nausea (4). The resulting dehydration often necessitates a high rate of IV 30
replenishment. Associated symptoms of pallor, listlessness, anorexia, nausea, retching, 31
abdominal pain, headache and photophobia may make it difficult to distinguish episodes of CVS 32
from other causes of acute abdomen and altered consciousness. Episodes are often triggered by 33
psychological (e.g. birthdays, holidays) and physical stress (infections, lack of sleep, menstrual 34
periods). CVS commonly starts in early childhood and the vomiting symptoms may abate with 35
the onset of classical migraine headaches during adolescence. Less commonly the condition 36
persists into adulthood or starts in adulthood (5-7). 37
38
The etiology and pathogenesis remain unknown but there appears to be a strong link 39
between CVS and migraine, based upon similarities in symptoms, common coexistence of both 40
conditions in the same individual, a high family prevalence of migraine in CVS patients, and the 41
effectiveness of anti-migraine therapy (8-13). Postulated mechanisms include episodic 42
dysautonomia, mitochondrial DNA mutations that cause deficits in cellular energy production 43
and/or heightened hypothalamic stress response that activates the emetic response (13-15). CVS 44
presents with vomiting and a variety of associated symptoms that could represent either differing 45
levels of severity or even distinct pathophysiologic mechanisms. These presentations include 46
subgroups such as migraine-associated, menses-associated and Sato subtype (16, 17) with 47
episode-associated hypertension and elevated adrenocorticotropin hormone. 48
49
The North American Society for Pediatric Gastroenterology, Hepatology and Nutrition 50
(NASPGHAN) appointed a task force to develop consensus management guidelines for CVS in 51
2003 to improve the recognition and treatment of a disorder that lacks any standard medical 52
approaches. An absence of controlled trials in this disorder necessitated that these 53
recommendations be based primarily upon small clinical trials and expert opinion. Despite these 54
NASPGHAN CVS Guidelines - 3
limitations, the committee attempted to provide useful guidelines for patient management based 55
upon the currently available literature and clinical experience. These guidelines are intended for 56
use by pediatricians, family physicians, pediatric gastroenterologists, pediatric neurologists and 57
emergency department physicians. While there appear to be an increasing number of adults 58
diagnosed with this disorder, it was beyond the purview of this task force to develop 59
management guidelines for adult patients. 60
61
62
METHODS & LITERATURE SEARCH 63
64
The NASPGHAN convened an expert panel in order to review the evidence and propose 65
guidelines for the evaluation and treatment of CVS. The panel consisted of nine experts drawn 66
from the fields of pediatric gastroenterology, pediatric neurology, genetics, and epidemiology. 67
Guidelines were developed by consensus of the CVS panel, using a modified Delphi technique 68
for algorithm development. 69
70
A systematic review of the literature was performed to identify all published articles that 71
contained primary data on the epidemiology, clinical features, natural history, and/or treatment 72
of CVS. Particular attention was directed toward articles that addressed the efficacy of treatment 73
modalities for CVS as part of the guideline development process. 74
75
Specific questions 76
77
The panel addressed four primary questions. 78
1) How is CVS defined? 79
The panel considered the most appropriate clinical and laboratory data to be used in 80
diagnosing CVS. Recognizing the lack of definitive laboratory markers, the heterogeneous 81
nature of the disorder, and the variability of diagnostic criteria currently in the literature, the 82
panel developed an operational definition of CVS by nominal group technique. 83
84
NASPGHAN CVS Guidelines - 4
2) What is the appropriate laboratory, radiographic and endoscopic evaluation in children with 85
a pattern of cyclic vomiting? 86
After discussion that addressed the known differences amongst international pediatric 87
gastroenterologists as to the extent of laboratory evaluation that is performed in patients with 88
suspected CVS, the panel focused on: 1) the initial screening evaluation in an undifferentiated 89
patient with episodic pattern of vomiting meeting the cyclic vomiting criteria; 2) the sensitivity 90
of the various tests for serious surgical and metabolic disorders; and 3) alarm symptoms that 91
should instigate a more thorough laboratory evaluation. The panel considered but did not focus 92
on the issues of subdividing patients by age, sex, race, ethnicity and clinical subgroups (e.g. 93
neurologically impaired). 94
95
3) In patients with CVS, does prophylactic treatment improve long-term outcomes, as compared 96
to no treatment or alternative treatment options? 97
The panel evaluated the efficacy of prophylactic treatment including lifestyle changes 98
such as avoidance of triggers, reassurance, education and family support, and anti-migraine and 99
anti-convulsant medications. The outcomes of prophylactic treatment included frequency of 100
subsequent episodes, duration and severity of episodes including number of emeses, nausea and 101
other constitutional symptoms. The panel did divide treatment groups by age above and below 102
five years, but did not focus on other subgroups. 103
104
4) During an acute attack of CVS, does treatment improve outcomes, as compared to no 105
treatment or alternate treatment options ? 106
The task force evaluated the efficacy of abortive and supportive treatment including 107
intravenous fluid(s) containing dextrose, as well medication including anti-emetics, anti-108
migraine triptans (serotonin agonists), sedatives and nonsteroidal anti-inflammatory drugs 109
(NSAID). The outcomes of the acute attack included length of episode, number of emeses, 110
severity of nausea and other constitutional symptoms. The panel did consider but did not focus 111
on issues of treatment of various subgroups and criteria for successful treatment. 112
113
NASPGHAN CVS Guidelines - 5
Literature search strategy 114
115
MEDLINE was searched via PubMed using the following terms: ("cyclic vomiting" OR 116
"cyclic vomiting syndrome" OR “cyclical vomiting” OR "CVS" OR "abdominal migraine" OR 117
“periodic syndrome” OR “biliary attacks” OR “recurrent vomiting”) AND (pediatrics OR 118
children OR infants) NOT Review [Publication Type] during the years 1980-present. The 119
electronic search was supplemented with the ‘related articles’ function in PubMed; with hand-120
search of recent bibliographies; and by consultation with experts. Using this strategy, 236 121
citations were identified. The abstracts of all citations were reviewed, and potentially relevant 122
articles were identified that: 1) included patients with CVS, and 2) reported primary data, other 123
than in case report(s) format. Using these criteria, a total of 67 full-length articles were retrieved 124
for full review. 125
126
Studies were selected for final inclusion in the evidence base, if they met the following 127
criteria: 1) full-length article published in the peer-reviewed literature between the years of 128
1980-2003; 2) included patients with CVS, using parameters of: a) periodicity of attacks, 129
including healthy intervals between attacks, b) characteristic pattern of symptoms during attack, 130
and c) lack of other explanation(s) for nausea/vomiting; and 3) evaluated one or more of the 131
specified treatments for either abortive therapy or prophylactic therapy and reports on one or 132
more relevant outcomes. Following application of these selection criteria, a total of 12 articles 133
met the criteria for inclusion in review of evidence. 134
135
The study qualities were assessed as follows. Levels of evidence (ranging from I – 136
randomized control trial to III – expert opinion) were assigned according to the system originally 137
developed by the Canadian Task Force on the Periodic Health Examination (18) and refined by 138
the United States Preventative Services Task Force (19). For single-arm studies, four quality 139
indicators (relevant, representative patient population; uniform, unbiased treatment delivery; 140
most important outcomes measures represented; appropriate statistical analysis) were used to 141
assign an overall quality of GOOD (meets all criteria), FAIR (does not meet all criteria but no 142
fatal flaws), or POOR (study has ‘fatal flaws’ for one or more indicators). From these levels, 143
NASPGHAN CVS Guidelines - 6
grades of recommendations were derived (A – level I evidence to D – expert opinion only). In 144
all studies, the grades of recommendation were D. 145
146
THE CONSENSUS DIAGNOSTIC CRITERIA 147
148
Recognizing the lack of definitive criteria, the heterogeneous nature of the disorder, and 149
the variability of diagnostic criteria in the literature, the panel developed an operational 150
definition of CVS. Using a combination of expert opinion, definitions used in the literature, and 151
the clinical and research experience of the panel, nominal group technique was used to achieve 152
the consensus diagnostic criteria shown in Table 1. The committee considered adoption of the 153
Rome III criteria for CVS (two periods of intense nausea and vomiting and return to normal 154
health). However, the lack of specificity raised concerns about the utility of that definition in 155
these guidelines (20-22). 156
157
158
DIAGNOSTIC APPROACH TO RECURRENT, EPISODIC VOMITING 159
160
A pattern of recurrent, episodic vomiting in children that fulfills the revised historical 161
criteria listed in Table 1 is likely (about 90%) to be ultimately diagnosed as idiopathic cyclic 162
vomiting syndrome (23). The challenge to the practitioner is to differentiate those with specific 163
and serious underlying causes of vomiting ( about 10 %) for which prompt treatment may alter 164
outcomes (24). Testing to exclude all possible diagnoses would subject many children to 165
unnecessary and costly radiographic and endoscopic procedures (25). Therefore, the diagnostic 166
guidelines below are intended to help identify those children with a cyclic vomiting pattern 167
between the ages of 2 and 18 years at greatest risk of having an organic cause. Although 168
children less than two years may have CVS , serious underlying metabolic and surgical disorders 169
are more frequent and more difficult to diagnose in this age range. 170
171
There are no specific laboratory markers to diagnose CVS. The diagnostic criteria were 172
modified by nominal group technique from previously published consensus criteria (22) and 173
those established by the Headache Classification Subcommittee of the International Headache 174
NASPGHAN CVS Guidelines - 7
Society (26) (Table 1). The diagnosis of CVS is thus based upon the fulfillment of these criteria 175
in the absence of another explanation for the symptoms. Clinicians experienced in evaluating 176
CVS may treat without performing an extensive evaluation, but expert opinion supported 177
performing screening tests in all children with a cyclic vomiting pattern just prior to 178
administration of intravenous fluids to include electrolytes (Na+, K+, Cl-, HCO3-), glucose, and 179
upper gastrointestinal radiographs to exclude malrotation (27-29). An abdominal ultrasound to 180
rule out transient hydronephrosis, preferentially during a crisis, could also be considered in 181
refractory cases (30, 31). If a patient has hyponatremia or hypoglycemia further evaluation 182
should be performed to exclude Addison disease (32, 33) and disorders of fatty acid oxidation 183
(34). A thorough history and physical examination at presentation helps identify those children in 184
whom further diagnostic testing is prudent. Suspicious “alarm” symptoms and physical findings 185
include: 186
1. Bilious vomiting, abdominal tenderness and/or severe abdominal pain 187
2. Attacks precipitated by intercurrent illness, fasting and/or high protein meal 188
3. Abnormalities on neurologic exam including severe alteration of mental status, abnormal 189
eye movements, papilledema, motor asymmetry and/or gait abnormality (ataxia). 190
4. Progressively worsening episodes or conversion to a continuous or chronic pattern 191
192
Depending upon the presenting symptoms and signs other than vomiting, different diagnostic 193
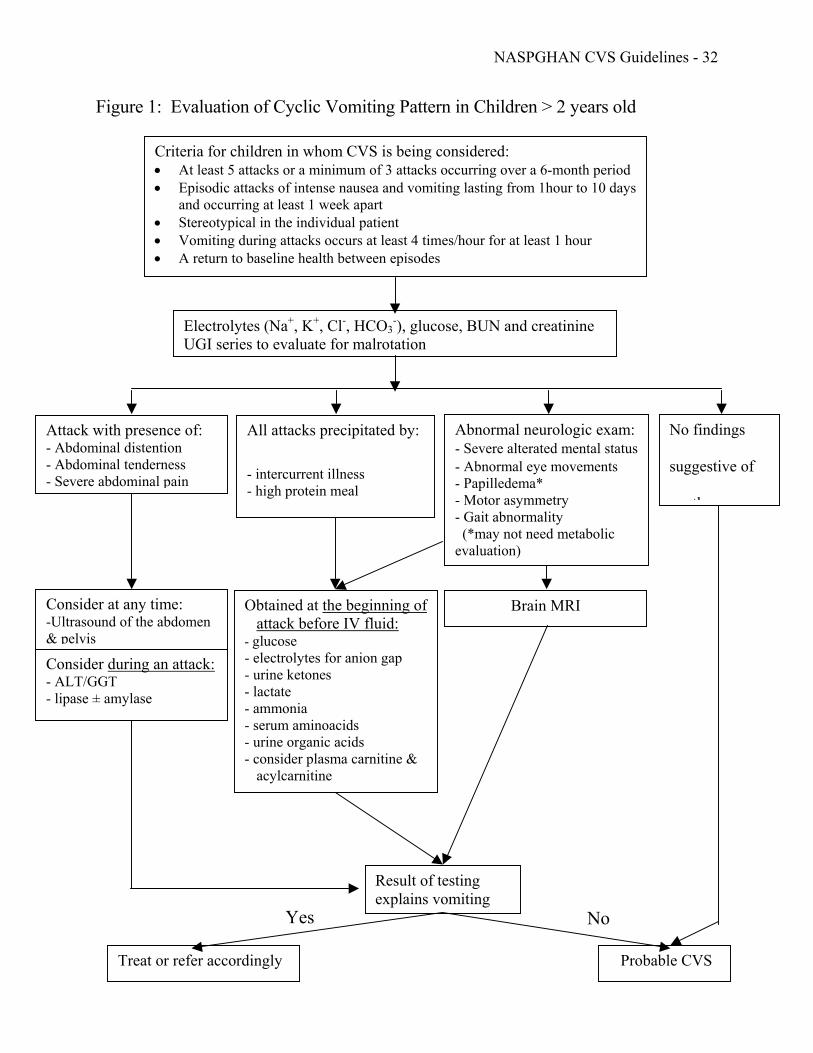
approaches are recommended as illustrated in Figure 1. 194
195
Evaluation of children with cyclic vomiting pattern and alarm symptoms or signs: 196
197
Bilious emeses, severe abdominal pain and/or hematemesis: Although children with CVS 198
frequently have bilious emesis (83%) and/or severe abdominal pain (80%) (4), serious surgical 199
and non-surgical disorders can present similarly. These disorders include intermittent bowel 200
obstruction from malrotation with volvulus (27, 28, 35) and post-operative adhesions/strictures, 201
gallbladder disease (36), choledochal cyst (37), hepatitis, pancreatitis, or uretero-pelvic junction 202
obstruction (31). When bile-stained vomitus or severe discomfort (e.g. writhing) are present, the 203
panel further recommends, in addition to an upper GI radiograph, obtaining amylase (38) and 204
lipase (39) to detect pancreatitis, ALT and GGT to screen for hepatitis and gallbladder disease, 205
NASPGHAN CVS Guidelines - 8
and an abdominal ultrasound and/or abdominal CT scan to evaluate the biliary (40) and urinary 206
tracts (41). Abnormal results would warrant further testing. If test results do not suggest an 207
alternate diagnosis, empirical treatment of CVS is recommended. 208
209
Recurrent episodes vomiting accompanied frequently by small amounts of hematemesis 210
raises the question about the role of esophagogastroduodenoscopy in the evaluation of these 211
children. Because the endoscopic biopsies usually do not reveal an etiologic cause of the 212
vomiting and typically demonstrate mild esophagitis or prolapse gastropathy as a cause of the 213
acute bleeding, the panel did not recommend a routine endoscopy unless there are chronic 214
symptoms in between episodes suggestive of a specific disorder (peptic/bacterial, allergic, 215
inflammatory or celiac), or, large amounts of hematemesis warrant endoscopic intervention (24) 216
217
Acute intermittent porphyria occurs infrequently and generally does not present before 218
puberty (42). It can present with recurrent vomiting and abdominal pain, mimicking CVS, but 219
usually has one or more of anxiety, depression, hallucination, seizures, cranial nerve weakness 220
and paresis of the extremeties. The diagnosis can be confirmed by finding an increased urinary 221
δ-aminolevulinic acid and porphobilinogen in a spot urine during the episode (43). 222
223
Attacks precipitated by intercurrent illness, fasting and/or a high protein meal. 224
225
Vomiting induced by metabolic disorders, including disorders of fatty acid oxidation 226
(FAO), the urea cycle, organic and amino acid metabolism, and mitochondrial energy 227
metabolism often follow a catabolic state induced by acute illness, fasting or a high protein meal. 228
Fasting can result from the anorexia and vomiting that accompanies mild viral upper respiratory 229
or GI infections, dieting or pre-surgical preparation. Although severe enzymatic deficiencies 230
generally present immediately after birth, partial enzymatic defects tend to affect toddlers. 231
232
A symptomatic metabolic disorder constitutes a medical emergency with substantial 233
risks for morbidity and mortality if appropriate treatment is not instituted promptly. If a 234
metabolic disorder is suspected, immediately obtain blood and urine for testing (Figure 1), 235
NASPGHAN CVS Guidelines - 9
deliver 10% dextrose-containing IV fluid at a rate of 1.5 times maintenance (simultaneously with 236
fluid boluses as necessary) and contact a metabolic specialist. 237
238
In partial urea cycle enzyme deficiencies, ammonia accumulation may present following 239
the ingestion of a high protein meal or with fasting. Although both sexes can be affected, most 240
are heterozygote girls with partial ornithine transcarbamylase (OTC) deficiency because the gene 241
is located on the X-chromosome. A urea cycle disorder is suggested by a plasma ammonia level 242
of ≥ 150 μm/L when symptomatic. Amino and organic acidemias often present in the first days 243
of life, but a subset with partial enzymatic deficiencies are silent until an illness-related fast 244
precipitates symptoms that can include episodes of vomiting. Altered mental status (see next 245
section), severe anion gap metabolic acidosis, substantial ketosis, and/or an unusual odor are 246
possible clues to the presence of the underlying condition. Developmental and growth delay are 247
present in many, but not all cases and can be subtle. Fatty acid oxidation disorders can present 248
with a cyclic vomiting pattern including medium-chain acyl-CoA dehydrogenase deficiency 249
(MCAD). 250
251
The diagnosis of these disorders is established with plasma amino acid and urine organic 252
acid analyses. The sensitivity of metabolic testing, both screening and sophisticated analyses, is 253
improved when performed early in an acute episode before dextrose containing IV fluid is given 254
(34). Analyses of plasma acylcarnitines and urine acylglycines are more sensitive than urine 255
organic acids in FAO disorders (44), and may be diagnostic even when asymptomatic (34). If 256
any of the screening tests are abnormal, the patient should be referred to a metabolic specialist 257
for further evaluation. 258
259
Biochemical, enzymatic and pedigree (maternal inheritance) data suggests that some 260
degree of mitochondrial dysfunction is present in many cases of CVS, and, although not the sole 261
cause, may contribute via insufficient cellular energy production (13, 45, 46). It is typical to find 262
mild-to-moderate degrees of an anion gap metabolic acidosis (calculated serum Na+ minus Cl- 263
minus HCO3- is often 15-20 mg/dl), lactic acidosis, urinary ketosis (early in an episode and thus 264
not a direct result of fasting) and/or hypoglycemia during vomiting episodes. These findings are 265
consistent with CVS and by themselves do not necessitate a comprehensive metabolic work-up. 266
NASPGHAN CVS Guidelines - 10
However, when encountered, quantitative urine organic acids and plasma amino acid analyses 267
obtained early in an episode can confirm mild mitochondrial dysfunction (elevated urine ketones, 268
Krebs cycle intermediates and/or dicarboxylic acids), and exclude other metabolic disorders. If 269
obtained either while asymptomatic or after several hours of IV dextrose, urine organic acids are 270
typically normal. 271
272
In some cases, episodic vomiting may be one manifestation of frank mitochondrial 273
disease; vomiting episodes can then be associated with a severe anion gap metabolic acidosis (> 274
20 mg/dl), insulin-resistance, and/or multi-system failure (e.g. cardiomyopathy, seizures etc.). 275
276
Abnormalities on neurological exam 277
278
Progressive or focal neurological findings, as well as new-onset ataxia, abnormal eye 279
movements, papilledema, motor asymmetry, gait abnormality, developmental regression or 280
stagnation, or recent personality changes, are not typical of CVS and should alert the clinician to 281
evaluate for increased intracranial pressure or a metabolic disorder. Intracranial pressure can be 282
due to underlying posterior fossa or hypothalamic tumor, Chiari malformation, hydrocephalus, or 283
subdural hematoma. Although one-quarter of children with brain tumors initially present with 284
vomiting, the majority will have other symptoms such as headache (often occipital), seizures or 285
behavioral changes, and demonstrable neurological signs of papilledema, abnormal eye 286
movements, motor asymmetry, gait ataxia or abnormal deep tendon reflexes (47). In 287
medulloblastoma, the most common brain tumor in childhood, about three-quarters present with 288
chronic vomiting, rarely cyclical, usually along with other signs such as papilledema, abnormal 289
eye movements, or ataxia (48). 290
291
If the vomiting is associated with progressive focal or diffuse neurological symptoms or 292
signs, neuroimaging with MRI is warranted. MRI is superior to CT scanning for visualization of 293
the posterior fossa. Skull X-rays have no value in this clinical setting. 294
295
Rarely, certain forms of complex partial seizures (e.g. temporal lobe or benign occipital 296
epilepsy) may be associated with episodic vomiting. Some degree of transient alteration of 297
NASPGHAN CVS Guidelines - 11
mental status, post-ictal confusion, and abnormal involuntary movements will likely be present. 298
If seizures are suspected, electroencephalography during awake, drowsy and sleep states is 299
indicated (49,50). 300
301
The most difficult sign to clarify is alteration of mental status. Children with CVS often 302
have altered consciousness during episodes that parents describe as a “conscious coma” in which 303
the child is lethargic, listless, withdrawn, disoriented and/or difficult to arouse. Since acute or 304
episodic neurological or metabolic diseases commonly produce distortions of mental status, it is 305
important to distinguish true encephalopathy from the listlessness typical of CVS. In CVS, the 306
child is usually oriented and able to respond appropriately to commands, but prefers not to 307
because of incapacitating nausea. In metabolic encephalopathy, the patient is frequently 308
disoriented, confused, excessively irritable, and/or difficult to arouse. With hyperammonemic 309
states, a rapidly shifting mental status and/or psychosis can also be observed. 310
311
Static non-focal neurological findings, including global developmental delay, generalized 312
seizures and/or hypotonia are found in some series upwards of 25% of CVS cases. When these 313
findings are present, the term “CVS+” has been applied (13, 45, 51), which predicts an earlier 314
age of onset for vomiting episodes, and a 3 to 8-fold increased prevalence for certain 315
dysautonomic-related (migraine, chronic fatigue, regional pain syndromes) and constitutional 316
(growth retardation and birth defects) disorders. Because these static non-focal neurological 317
findings are also present in many metabolic disorders associated with episodic vomiting, the 318
expert panel recommended that a screening metabolic evaluation be performed to include 319
quantitative plasma amino acids and quantitative urine organic acids obtained early in an episode 320
(Figure 1). 321
322
Suggested work-up in cases at higher risk for neurometabolic disease: The panel recommends 323
that children with cyclic vomiting be evaluated for a possible metabolic or neurologic disorder if 324
any of the following conditions are met (Figure 1): 325
Presentation under age 2 years (with cyclic vomiting or co-morbidities below) 326
Vomiting episodes associated with: intercurrent illnesses, prior fasting, increased protein intake 327
Any neurological finding: ataxia, dystonia, or another gait disturbance, mental retardation, 328
NASPGHAN CVS Guidelines - 12
seizure disorder or acute encephalopathy (including true lethargy, severe irritability, confusion, 329
psychosis or rapidly changing/unstable mental status) 330
Laboratory metabolic findings: hypoglycemia, substantial anion gap metabolic acidosis, 331
respiratory alkalosis or hyperammonemia 332
A referral to a specialist in metabolic disorders and/or a neurologist is suggested in patients with 333
any of the above findings. 334
335
No finding suggestive of another disorder 336
In children with a cyclic pattern of vomiting and no alarm findings in the history and 337
physical examination, an initial trial of empiric therapy can be considered (Figure 1). If the 338
patient responds to therapy with at least a 50% reduction in episode frequency and/or severity of 339
vomiting during attacks, then further evaluation is not required. If the patient does not improve 340
with initial therapy over a two month period, further evaluation is recommended. 341
342
Although uncommon as a cause of episodic vomiting, Munchausen-by-proxy may mimic 343
CVS. The perpetrator may describe vomiting episodes in a dehydrated child that has had 344
feedings withheld or may give the victim ipecac to induce vomiting (52). However, patients 345
have been inappropriately diagnosed with Munchausen-by-proxy when in fact CVS was causing 346
recurrent vomiting. 347
348
349
TREATMENT OF CYCLIC VOMITING SYNDROME 350
351
OVERALL APPROACH 352
353
The clinical course of CVS can be divided simply into the episode phase and the well 354
phase, during which the child returns to their normal or baseline state of health (4). The episode 355
phase is further divided into the prodrome as the child becomes ill up to the point when vomiting 356
begins, the vomiting phase and the recovery phase during which the vomiting ceases and the 357
child returns to baseline health. Each phase has therapeutic implications (53). During the well 358
phase, the avoidance of identified triggers can lead to fewer episodes. Treatment with abortive 359
NASPGHAN CVS Guidelines - 13
therapy as early as possible in the prodrome or vomiting phase may terminate the attack. If the 360
vomiting phase becomes full blown, supportive therapy at home or in hospital is focused on 361
providing relief from nausea, vomiting and abdominal pain. If abortive therapy fails consistently 362
or if episodes are frequent and/or severe, daily prophylactic therapy to prevent subsequent 363
episodes is recommended. 364
365
The management of CVS requires an individually tailored regimen that takes into 366
consideration the clinical course, the frequency and severity of attacks, and resultant disability 367
balanced with the potential side effects of treatment. The two key treatment arms are 368
prophylactic (or preventive) measures and medications administered between attacks, and acute 369
and supportive interventions given during attacks. Despite the absence of FDA approved 370
medications for use in children with CVS, the panel recommendations below include off-label 371
uses. In the larger context of pediatric medication use, over 70% of prescribed medications lack 372
pediatric approval (54). 373
374
Families should be strongly encouraged to contact the Cyclic Vomiting Syndrome 375
Association [cvsaonline.org] for information and ongoing support. 376
377
PROPHYLACTIC MEASURES 378
There is a paucity of controlled data on the prophylactic treatment of CVS – mostly case 379
series (level II evidence) (Table 2). The existing evidence consists of small, retrospective 380
clinical series that evaluate symptomatic responses to medications. The treatment 381
recommendations are based upon limited evidence (level II) and consensus opinion (level III, 382
Grade D) of an expert panel of clinicians with broad experience with CVS. 383
During the well phase, lifestyle changes such as avoidance of excessive excitement, 384
energy-depleted states (e.g. fasting, illness), sleep deprivation, triggering foods (e.g. chocolate, 385
cheese), menses, and motion sickness may reduce episode frequency. If episodes occur 386
frequently (e.g. more than every 1-2 months), are severe enough to cause repeated hospitalization 387
and school absences, and/or fail to respond to abortive therapy, preventative prophylactic 388
pharmacotherapy is recommended. 389
390
NASPGHAN CVS Guidelines - 14
Because fear and anticipation of future episodes can trigger episodes of CVS , the use of 391
reassurance and anticipatory guidance may help reduce the frequency of attacks. This includes 392
confirming that the attacks are not self-induced and that the child will typically improve with 393
age, as well as providing an individualized management protocol. 394
395
Lifestyle changes 396
Although there are no published trials that evaluate the impact of life style alterations on 397
CVS attacks, the panel’s consensus experience is that life style changes reduce episode 398
frequency in children with CVS (Table 3). Fleisher reported that 70% of patients initially 399
respond to consultation alone without drug therapy by reduced episode frequency (55). This 400
response may result from alleviation of known precipitating factors and/or from reductions in 401
stress (commonly a trigger of episodes) due to a positive diagnosis, knowledge that effective 402
therapies are available, and interaction with a caring physician. Because of common parental 403
concerns about potential side effects of preventative medications, lifestyle changes may be 404
recommended first, and, may delay or occasionally circumvent the use of daily medications. A 405
time-limited trial to assess the impact of lifestyle changes for one or two months or through one 406
or two typical cycles may be instituted concurrent with the testing to exclude organic causes of 407
vomiting (see Diagnostic Approach). 408
409
- Avoidance of triggers 410
A careful history and/or detailed “vomiting diary” that records intervals between episodes, 411
time of onset and ending, contents of preceding meals, and aggravating life events can help identify 412
potentially avoidable triggers in three-quarters of children (4). It is important that families 413
recognize that episodes can be precipitated by common infections, exciting occasions such as 414
birthdays and holidays, and lack of sleep and/or overexertion. 415
Avoidance of migraine triggering foods (e.g. chocolate and cheese) or food allergens can 416
reduce episode frequency in CVS. In one small study, seven of eight children with documented 417
food sensitivities to cow, soy or egg white protein, improved following specific dietary elimination 418
(56). Although total elimination of potential allergenic foods is not recommended by the panel, 419
it may be prudent to introduce a trial elimination of particular foods or chemical substances that 420
are consistently aggravating factors. Marijuana has been used for treatment of chronic nausea 421
NASPGHAN CVS Guidelines - 15
and vomiting of chemotherapy and also by adolescents to self-treat CVS. However in one series 422
of adult patients with CVS, marijuana use was found to worsen the cyclic hyperemesis and 423
cessation decreased episodes of vomiting (57). 424
425
- Supplemental carbohydrate 426
The use of supplemental carbohydrate can provide additional energy during times of high 427
energy demands. Published observations have noted that fasting induces some episodes and, 428
conversely, frequent feedings prevent others, even in the absence of documented hypoglycemia 429
(13). Furthermore, a rapid response to IV dextrose infusion can be seen during acute attacks (4). 430
When the history suggests fasting-induced attacks, high-carbohydrate snacks may be given 431
between meals, before physical exertion, and at bedtime. 432
433
- Migraine lifestyle interventions 434
Given that CVS is considered to be within the migraine spectrum as a “childhood 435
precursor to migraine”, it is appropriate to mention lifestyle changes commonly incorporated into 436
pediatric migraine management strategies. These include good sleep hygiene (e.g. regular sleep 437
schedules, avoiding sleepovers), regular aerobic exercise, regular meal schedules (i.e. avoid 438
skipping meals), maintenance of good hydration, and moderation (30 mg/day) or avoidance of 439
caffeine (58-60). 440
441
Prophylactic or preventive medications – general approach 442
Published clinical trials consist of uncontrolled or retrospective reports (i.e. level II 443
evidence) (Table 2). The literature does not permit the panel to provide evidence-based guidelines. 444
The recommendations which follow are based upon expert opinion (i.e. level II and III evidence, 445
grade D recommendations) (Table 4). 446
447
NASPGHAN CVS Guidelines - 16
Before initiating daily prophylactic pharmacotherapy, clinicians must consider the age of 448
the child, medical and psychological co-morbidities, dosage format, and side effect profiles of 449
the medications. We recommend beginning a low initial dose, and then increasing it 450
incrementally, “titrating to effect”. The rationale is that the lower doses may be therapeutic in 451
some cases and may limit side effects that emerge at higher doses. 452
453
Medications 454
Cyproheptadine, propranolol (61, 62), amitriptyline (5, 11, 13, 63), phenobarbital (64) and 455
pizotifen (65, 66) were five medications in which high response rates were observed in at least 10 456
patients (Class II evidence). However, these studies were prone to bias because they did not 457
account for the non-specific treatment effects, e.g. placebo response and recall (i.e. retrospective 458
reporting) effects. The differing inclusion criteria and qualitative outcomes used in these studies 459
does not allow comparison of relative efficacies. 460
461
The antihistamine and serotonin receptor antagonist cyproheptadine has a moderate 462
response rate in young children and is the first choice of the expert panel in children less than five 463
years of age (Table 4) (11, 13, 63). Increased weight due to enhanced appetite may be an 464
unacceptable side effect in school-aged girls, although cyproheptadine may be the appropriate first 465
choice in an underweight patient. Because the pharmacokinetics do not allow once-a-day dosing, 466
tiredness after the morning dose can interfere with school performance. Pizotifen was shown to be 467
highly efficacious in a case series of six CVS subjects (67) and one randomized placebo-controlled 468
trial in 16 abdominal migraine patients (66). However, pizotifen is only available in Canada and 469
the U.K. but not in the U.S. 470
471
The tricyclic antidepressant amitriptyline has a moderate-to-high response rate and is the 472
preferred first choice in the older child more than five years of age (Table 4) (5, 11, 13, 63). 473
Clinical experience indicates a higher response rate if given at an adequate dosage (1.0 mg/kg/day, 474
occasionally 1.5-2.0 mg)) for at least four weeks. To minimize side effects, dosing is commonly 475
initiated at a single night-time dose of 0.25-0.5 mg/kg/day (likely subtherapeutic) and increased 476
incrementally by 5-10 mg. The risk of ventricular arrhythmia is reduced by monitoring the QTc 477
interval (to maintain ≤ 460 msec) before and after establishing targeted dose (68). If a tricyclic 478
NASPGHAN CVS Guidelines - 17
medication is effective, but the child cannot tolerate tablets, amitriptyline can be solubilized by a 479
compounding pharmacist or at home. Although anecdotal experience has shown potential 480
efficacy in younger ages the panel has not recommended use in younger children because of 481
frequent side effects and a risk of overdose. 482
483
The β-blocker propranolol has moderate efficacy and is recommended as the second 484
choice in children of all ages (Table 4) (11, 13, 61, 62). The resting heart rate should be 485
monitored for potential bradycardia (< 60 beats/min) and, if propranolol is discontinued, it 486
should be tapered over 1-2 weeks. Alternatives, atenolol and nadalol, have fewer side effects, 487
but may be less effective because of inability to cross the blood-brain barrier. 488
489
The anti-convulsant, phenobarbital demonstrated efficacy in one study at a low single 490
nighttime dose of 2 mg/kg/day (64). Potential cognitive impairment limits the panel’s 491
enthusiasm for recommending this drug as first line therapy. In migraine there is an evolving 492
literature supporting the efficacy of other anticonvulsants (e.g. topiramate) but the side effects 493
and necessary titration of each of these medications require that an individual experienced in the 494
use of these agents in children (e.g. pediatric neurologist) should guide use of these agents in 495
patients with CVS (60, 69). 496
497
RECOMMENDATIONS ON PROPHYLAXIS 498
The panel recommends cyproheptadine or propranolol prophylaxis for children ≤ 5 years 499
of age. In the older child (> 5 years of age), amitriptyline or propranolol are recommended as 500
shown in Table 4. The dose can be titrated to effect by increasing it every 1-4 weeks to achieve 501
at least an average therapeutic dose for two CVS cycles (e.g. if monthly, then for two months). 502
If the medication causes intolerable side effects and/or proves to be ineffective, it is appropriate 503
to switch to another medication. The common side effects tend to be dose-related and may be 504
addressed by reducing the dosage. 505
506
In the panel’s experience, most CVS patients will respond to amitriptyline, cyproheptadine and/or 507
propranolol . If a patient does not respond, consider: 508
1) alternative diagnoses other than CVS and need of additional diagnostic testing; 509
NASPGHAN CVS Guidelines - 18
2) whether an adequate trial was administered, e.g. a high-end dose given for at least a two-510
cycle trial period, or lack of adherence; 511
3) combination therapy of two medications (e.g especially amitriptyline with one of the 512
other main drugs); 513
4) adding an alternative therapy from the list below 514
515
Alternate approaches for prophylaxis 516
Carnitine (commonly prescribed dose of 50-100 mg/kg/d, adults = 1.0 g TID), a nutrient 517
that serves as a transport cofactor for long-chain fatty acids into mitochondria, may help cases with 518
suspected mitochondrial or metabolic dysfunction, and has a benign side effect profile (70). 519
Another mitochondrial co-factor, coenzyme Q (commonly prescribed dose of 5-10 mg/kg/d, adults 520
= 100 mg TID) is receiving interest, but there is no data regarding efficacy. Although there are no 521
published data, low estrogen oral contraceptives have been used to treat girls with catemenial 522
(menstrual-related) CVS (71). Anecdotal experience suggests that acupuncture at the P6 523
(pericardial) point may attenuate the severity of CVS attacks (72). Psychotherapy, especially 524
stress reduction, may help as adjunctive therapy (73). 525 526 527 ACUTE INTERVENTION – SUPPORTIVE CARE AND ABORTIVE THERAPY 528
529
There are no controlled or open trials of supportive measures (e.g. nonstimulating 530
environment), pharmacologic (e.g. anti-migraine, anti-emetic) agents, or complementary 531
approaches (e.g. acupuncture) in managing acute CVS (Table 5). Based on small case series 532
(level II evidence), anecdotal experience and expert opinion (level III), the panel recommends 533
supportive and symptomatic care during acute episodes (grade D recommendation) (Table 6). 534
535
Expert opinion supports the efficacy of early intervention within the first several hours of 536
the onset. Some experts advocate an approach similar to that employed for migraine headache in 537
which nonsteroidal analgesics (e.g. ibuprofen) are administered orally during the early prodrome 538
before the vomiting begins. Once the vomiting starts, evaluation in an emergency department or 539
direct admission to the hospital ward before dehydration ensues is appropriate in some patients 540
for protocolized treatment specifying intravenous fluids, medications and admission criteria. 541
NASPGHAN CVS Guidelines - 19
Providing the patient with a letter that explains CVS and specifies an individualized management 542
protocol can facilitate prompt institution of therapy. A template of such a letter is provided at 543
(CVSA Website) and a sample protocol is shown in Table 7. 544
545
Some behaviors during episodes may appear to be odd but are in fact quite common in 546
CVS episodes. Many children become noncommunicative and curl into a fetal position because, 547
in their hypersensitive state, any further stimulation heightens their nausea and can trigger more 548
vomiting (74). At best, the child should not be unnecessarily disturbed. There are other children 549
who drink obsessively to induce vomiting. Reductions in these behavioral responses generally 550
are observed when patients receive adequate symptom relief with anti-emetics and sedation. 551
552
Most CVS patients will respond partially to one of the regimens discussed below. If a child 553
does not respond, or the episode differs substantially from previous ones by greater severity, longer 554
duration, or, new or different symptoms, reconsider the possibility of an underlying surgical lesion 555
and the need of new or repeated diagnostic testing, e.g. abdominal ultrasound or brain MRI. 556
557
Supportive care 558
Supportive care during acute episodes includes providing a less stimulating (dark, quiet) 559
environment, replacement of fluid, electrolyte and energy, use of anti-emetics with or without 560
sedation to lessen the nausea and vomiting, and provision of analgesia for pain (53). 561
562
Some experts recommend higher amounts of IV dextrose-containing fluids (D10 0.45 563
normal saline) (Table 6). If the child is evaluated in the later phases and substantial fluid and/or 564
electrolyte deficits are found, the panel recommends infusing 0.9% NaCl replacement fluid 565
through a “Y” connecter parallel to the D10. An increased anion gap (> 18-20 meq/L), may reflect 566
either severe dehydration or signal metabolic decompensation, and the need for hospital admission. 567
The ensuing catabolism following two to three days of minimal energy and/or protein intake can 568
prolong the illness, and can be reversed with parental nutrition to provide an adequate caloric 569
intake and 1.5 grams of protein/kg/day. 570
571
NASPGHAN CVS Guidelines - 20
Episodic vomiting can occasionally result from metabolic decompensation in frank 572
mitochondrial disease and be associated with metabolic acidosis with an anion gap (i.e. lactic 573
acidosis), hyperglycemia (insulin resistance) and/or multi-system failure. In such seriously ill 574
patients, administering higher amounts of glucose (e.g. 8-12 mg glucose/kg/min) with or without 575
concomitant insulin, closely monitoring the acidosis, and obtaining a metabolic consultation are 576
critical to management. 577
578
Abortive (triptans) and supportive (5HT3 receptor antagonist anti-emetic, sedative & 579
analgesic) medications 580
There are no controlled and no open trials of pharmacologic (e.g. anti-migraine, anti-581
emetic) agents in greater than 10 patients. Panel recommendations are made below for their off-582
label use (Table 6). 583
584
Triptans, 5HT1B/1D agonists, are not approved for use in children under age 18 years. 585
However, the panel recommend a trial as abortive agents in children aged ≥ 12 years who have 586
infrequent and/or mild episodes (e.g. < 1/month). One open label report and expert experience 587
indicate that triptans can terminate an episode (75) if administered early. The transient burning 588
sensation in the neck and upper chest appears to be uncommon with nasal form. Zolmitriptan 589
also comes in a nasal form. 590
591
5HT3 receptor antagonists are supportive rather than abortive anti-emetic agents 592
available in oral (liquid, tablet or dissolving tablet), rectal (reconstituted by pharmacy) and 593
intravenous forms (13, 23, 61). Because they are well tolerated and more effective at higher 594
doses, expert experience recommends ondansetron doses of 0.3-0.4 mg/kg with a usual upper 595
limit of 20 mg/dose. Safe use of doses up to 32 mg have been reported in children (76). 596
Granisetron is also available in IV form but there is little experience in CVS. Widely used 597
phenothiazine (D2 antagonists) anti-emetics, promethazine and prochlorperazine, are ineffective 598
when compared to ondansetron (22% vs. 58%, p < .05) (4). 599
600
When anti-emetics fail to control unrelenting nausea and vomiting, expert opinion 601
recommends adding sedatives. Parallel to the experience in severe migraines, sleep may be the 602
NASPGHAN CVS Guidelines - 21
only mode that provides symptomatic relief, and may occasionally shorten the episode. The 603
most effective combination therapy is ondansetron and lorazepam. Alternatively, 604
chlorpromazine and diphenhydramine can be used together but provides less anti-emetic and 605
more sedative effect (4, 53). 606
607
- Treatment of pain, hypertension and complications 608
Midline abdominal pain can be severe and treated empirically with analgesics. On 609
physical exam, even when the child is writhing in pain, the abdominal wall is typically soft to 610
palpation. To manage pain, the expert panel recommends the use of IV H2RAs e.g. ranitidine, 611
and the use of ketorolac, then morphine or fentanyl (77,78). If the pain has an epigastric location 612
and dyspeptic quality, IV administration of a H2 receptor antagonist or proton pump inhibitor 613
may be necessary to lessen the distress (53). The transient hypertension found in the Sato subset 614
of CVS should be treated, if needed, with short-acting ACE inhibitors during the episode only, 615
because it resolves promptly when the episode ends. 616
617
The main complications of an acute episode include dehydration (covered above), 618
electrolyte derangement including inappropriate secretion of anti-diuretic hormone (SIADH), 619
metabolic acidosis, hematemesis from prolapse gastropathy or Mallory-Weiss tear, chronic 620
esophagitis and weight loss (53). If SIADH with hyponatremia, low serum osmolality and high 621
urine specific gravity (despite adequate hydration) occurs, one restricts water intake until values 622
normalize. Because metabolic acidosis can have several potential causes including hypovolemia, 623
sepsis, lactic acidosis and ketosis from mitochondrial dysfunction, and hyperventilation 624
(respiratory alkalosis with renal compensation), obtaining serum electrolytes, urine pH and 625
ketones, and an arterial blood gas may clarify the situation. Hematemesis most commonly 626
results from prolapse gastropathy in which the vomiting bruises the stomach fundus by forcing it 627
retrograde through the GE junction and usually resolves without therapy (79). If the bleeding 628
persists and/or vital signs are affected, fluid replacement and endoscopic management may be 629
necessary. Moderate esophagitis may require ongoing acid suppression. Growth failure can 630
result from prolonged episodes without oral intake or other causes and may require dietary 631
counseling as well as nasogastric or parenteral nutrition between episodes to provide restorative 632
calories. 633
NASPGHAN CVS Guidelines - 22
634
Alternative abortive approaches 635
For those who have panic anxiety-triggered episodes or anticipatory attacks (i.e. akin to 636
anticipatory vomiting pre-chemotherapy), the use of either anxiolytic medications or stress 637
relaxation techniques (e.g. deep breathing and relaxation imagery) has been reported anecdotally 638
to abort episodes (53, 80). 639
640
Recovery and refeeding 641
The recovery phase from the last emesis to the point of being able to retain foods 642
typically lasts a few hours. Once children state that they are hungry and want to eat food, they 643
can generally resume a normal diet without gradual progression. However, this should be 644
individualized because some children require stepwise reintroduction of foods to prevent the 645
recurrence of nausea. 646
647
RECOMMENDATIONS – SUPPORTIVE AND ABORTIVE INTERVENTION 648
During the acute episode of vomiting, the panel recommends supportive measures 649
including placing children in less stimulating environs, replenishing fluids, electrolytes and 650
energy , treating symptomatic nausea, vomiting and severe abdominal pain. Early intervention 651
within the first two to four hours of onset either at home or at a hospital may be more effective 652
than that later on. At all ages, use of IV D10 and high dose 5HT3 antagonist anti-emetics (e.g. 653
ondansetron 0.3-0.4 mg/kg/dose) off label rather than D2 anti-emetics (e.g. phenothiazine-type) 654
is recommended to treat the energy deficits and vomiting respectively. If ineffective, 655
concomitant sedation is recommended. Severe abdominal pains are treated with parenteral acid 656
suppression and/or NSAID or narcotics. As an abortive approach, intranasal triptans may be 657
used off label in children age 12 and over with infrequent (< 1/month) or milder episodes (≤ 24 658
hours). 659
660
Alternative abortive approaches 661
For those who have panic anxiety-triggered episodes or anticipatory attacks (i.e. akin to 662
anticipatory vomiting pre-chemotherapy), the use of either anxiolytic medications or stress 663
NASPGHAN CVS Guidelines - 23
relaxation techniques (e.g. deep breathing and relaxation imagery) has been reported anecdotally 664
to abort episodes (53, 80).665
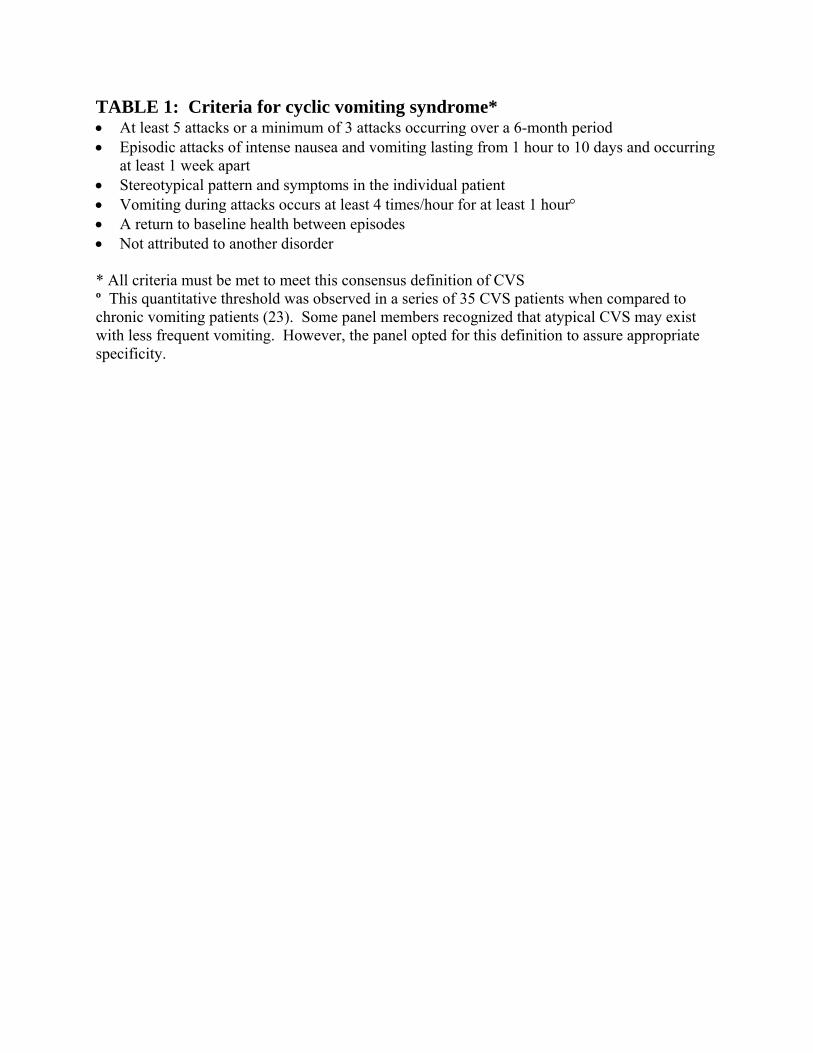
TABLE 1: Criteria for cyclic vomiting syndrome* • At least 5 attacks or a minimum of 3 attacks occurring over a 6-month period • Episodic attacks of intense nausea and vomiting lasting from 1 hour to 10 days and occurring
at least 1 week apart • Stereotypical pattern and symptoms in the individual patient • Vomiting during attacks occurs at least 4 times/hour for at least 1 hour° • A return to baseline health between episodes • Not attributed to another disorder * All criteria must be met to meet this consensus definition of CVS º This quantitative threshold was observed in a series of 35 CVS patients when compared to chronic vomiting patients (23). Some panel members recognized that atypical CVS may exist with less frequent vomiting. However, the panel opted for this definition to assure appropriate specificity.
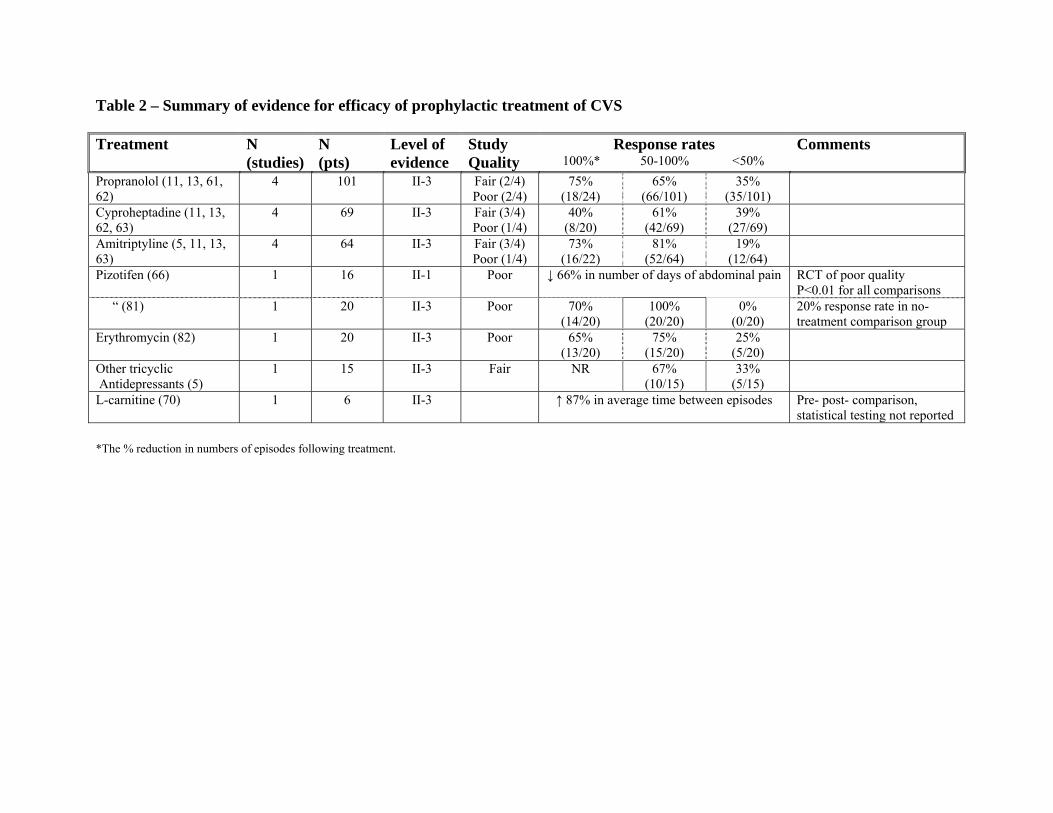
Table 2 – Summary of evidence for efficacy of prophylactic treatment of CVS Treatment N
(studies) N (pts)
Level of evidence
Study Quality
Response rates 100%* 50-100% <50%
Comments
Propranolol (11, 13, 61, 62)
4 101 II-3 Fair (2/4) Poor (2/4)
75% (18/24)
65% (66/101)
35% (35/101)
Cyproheptadine (11, 13, 62, 63)
4 69 II-3 Fair (3/4) Poor (1/4)
40% (8/20)
61% (42/69)
39% (27/69)
Amitriptyline (5, 11, 13, 63)
4 64 II-3 Fair (3/4) Poor (1/4)
73% (16/22)
81% (52/64)
19% (12/64)
Pizotifen (66) 1 16 II-1 Poor ↓ 66% in number of days of abdominal pain RCT of poor quality P<0.01 for all comparisons
“ (81) 1 20 II-3 Poor 70% (14/20)
100% (20/20)
0% (0/20)
20% response rate in no-treatment comparison group
Erythromycin (82) 1 20 II-3 Poor 65% (13/20)
75% (15/20)
25% (5/20)
Other tricyclic
Antidepressants (5) 1 15 II-3 Fair NR 67%
(10/15) 33%
(5/15)
L-carnitine (70) 1 6 II-3 ↑ 87% in average time between episodes Pre- post- comparison, statistical testing not reported
*The % reduction in numbers of episodes following treatment.
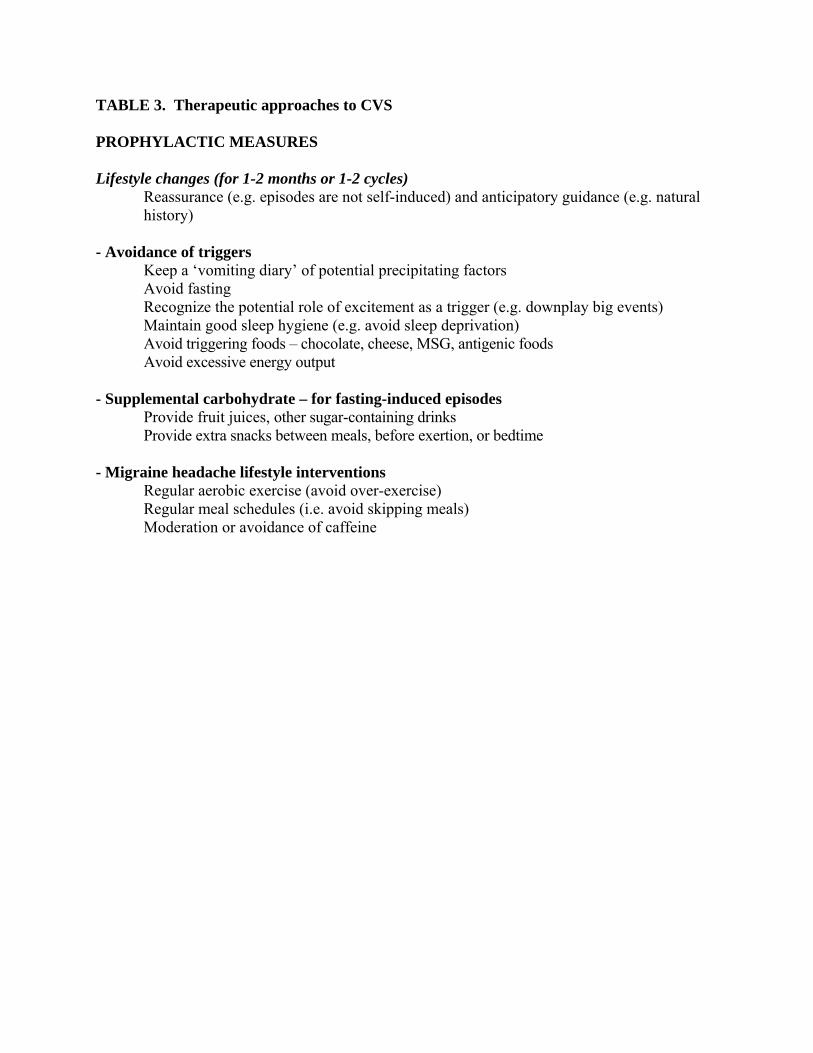
TABLE 3. Therapeutic approaches to CVS PROPHYLACTIC MEASURES Lifestyle changes (for 1-2 months or 1-2 cycles)
Reassurance (e.g. episodes are not self-induced) and anticipatory guidance (e.g. natural history)
- Avoidance of triggers Keep a ‘vomiting diary’ of potential precipitating factors Avoid fasting Recognize the potential role of excitement as a trigger (e.g. downplay big events) Maintain good sleep hygiene (e.g. avoid sleep deprivation) Avoid triggering foods – chocolate, cheese, MSG, antigenic foods Avoid excessive energy output
- Supplemental carbohydrate – for fasting-induced episodes
Provide fruit juices, other sugar-containing drinks Provide extra snacks between meals, before exertion, or bedtime
- Migraine headache lifestyle interventions Regular aerobic exercise (avoid over-exercise)
Regular meal schedules (i.e. avoid skipping meals) Moderation or avoidance of caffeine
NASPGHAN CVS Guidelines - 27
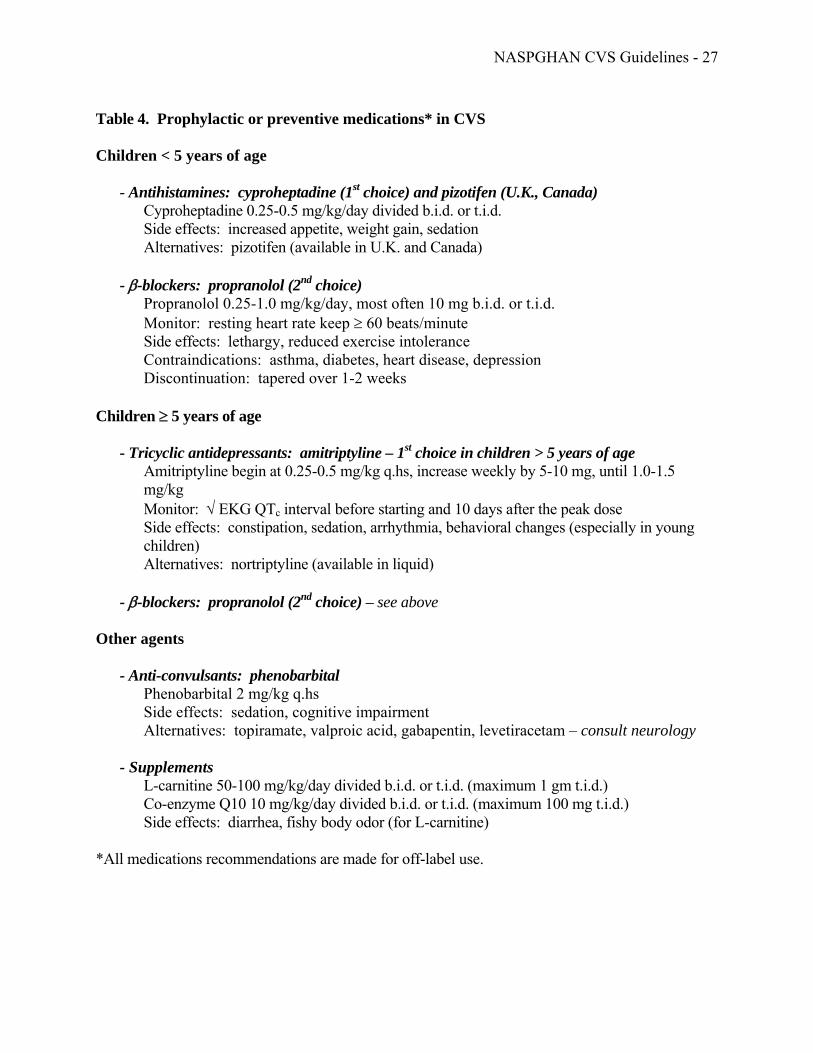
Table 4. Prophylactic or preventive medications* in CVS Children < 5 years of age
- Antihistamines: cyproheptadine (1st choice) and pizotifen (U.K., Canada) Cyproheptadine 0.25-0.5 mg/kg/day divided b.i.d. or t.i.d. Side effects: increased appetite, weight gain, sedation Alternatives: pizotifen (available in U.K. and Canada)
- β-blockers: propranolol (2nd choice)
Propranolol 0.25-1.0 mg/kg/day, most often 10 mg b.i.d. or t.i.d. Monitor: resting heart rate keep ≥ 60 beats/minute Side effects: lethargy, reduced exercise intolerance Contraindications: asthma, diabetes, heart disease, depression Discontinuation: tapered over 1-2 weeks
Children ≥ 5 years of age
- Tricyclic antidepressants: amitriptyline – 1st choice in children > 5 years of age Amitriptyline begin at 0.25-0.5 mg/kg q.hs, increase weekly by 5-10 mg, until 1.0-1.5 mg/kg Monitor: √ EKG QTc interval before starting and 10 days after the peak dose Side effects: constipation, sedation, arrhythmia, behavioral changes (especially in young children) Alternatives: nortriptyline (available in liquid)
- β-blockers: propranolol (2nd choice) – see above
Other agents
- Anti-convulsants: phenobarbital Phenobarbital 2 mg/kg q.hs Side effects: sedation, cognitive impairment Alternatives: topiramate, valproic acid, gabapentin, levetiracetam – consult neurology
- Supplements
L-carnitine 50-100 mg/kg/day divided b.i.d. or t.i.d. (maximum 1 gm t.i.d.) Co-enzyme Q10 10 mg/kg/day divided b.i.d. or t.i.d. (maximum 100 mg t.i.d.) Side effects: diarrhea, fishy body odor (for L-carnitine)
*All medications recommendations are made for off-label use.
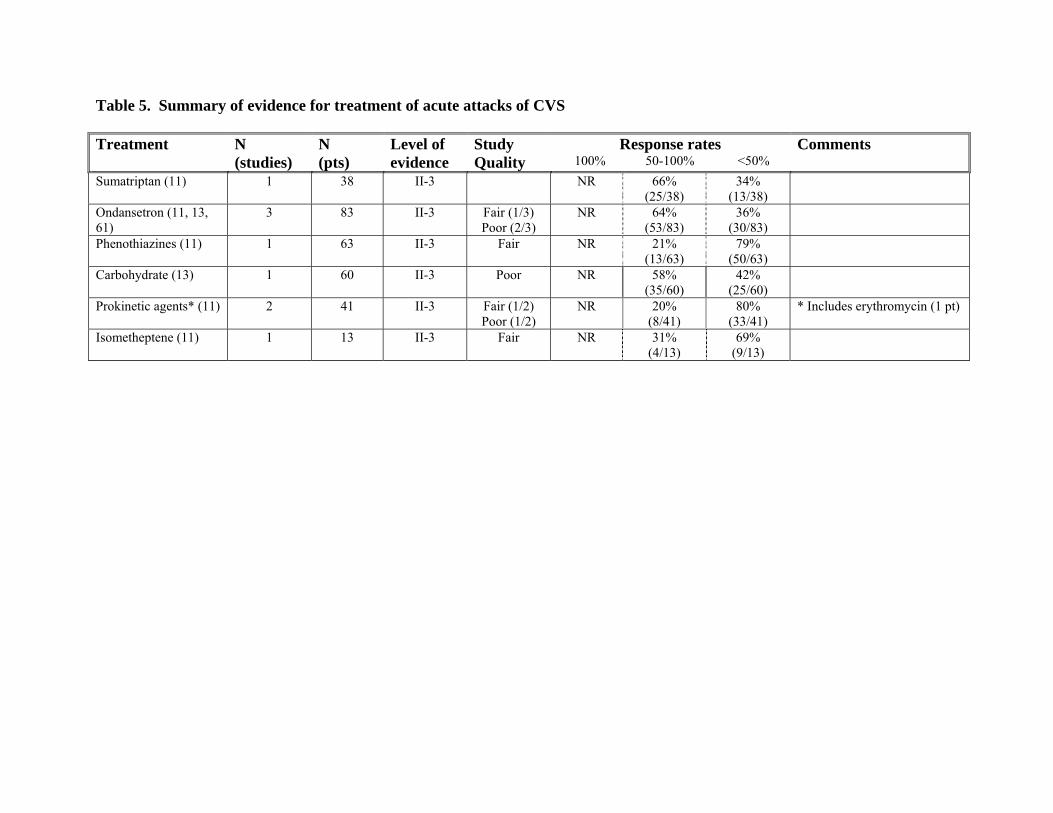
Table 5. Summary of evidence for treatment of acute attacks of CVS Treatment N
(studies) N (pts)
Level of evidence
Study Quality
Response rates 100% 50-100% <50%
Comments
Sumatriptan (11) 1 38 II-3 NR 66% (25/38)
34% (13/38)
Ondansetron (11, 13, 61)
3 83 II-3 Fair (1/3) Poor (2/3)
NR 64% (53/83)
36% (30/83)
Phenothiazines (11) 1 63 II-3 Fair NR 21% (13/63)
79% (50/63)
Carbohydrate (13) 1 60 II-3 Poor NR 58% (35/60)
42% (25/60)
Prokinetic agents* (11) 2 41 II-3 Fair (1/2) Poor (1/2)
NR 20% (8/41)
80% (33/41)
* Includes erythromycin (1 pt)
Isometheptene (11) 1 13 II-3 Fair NR 31% (4/13)
69% (9/13)
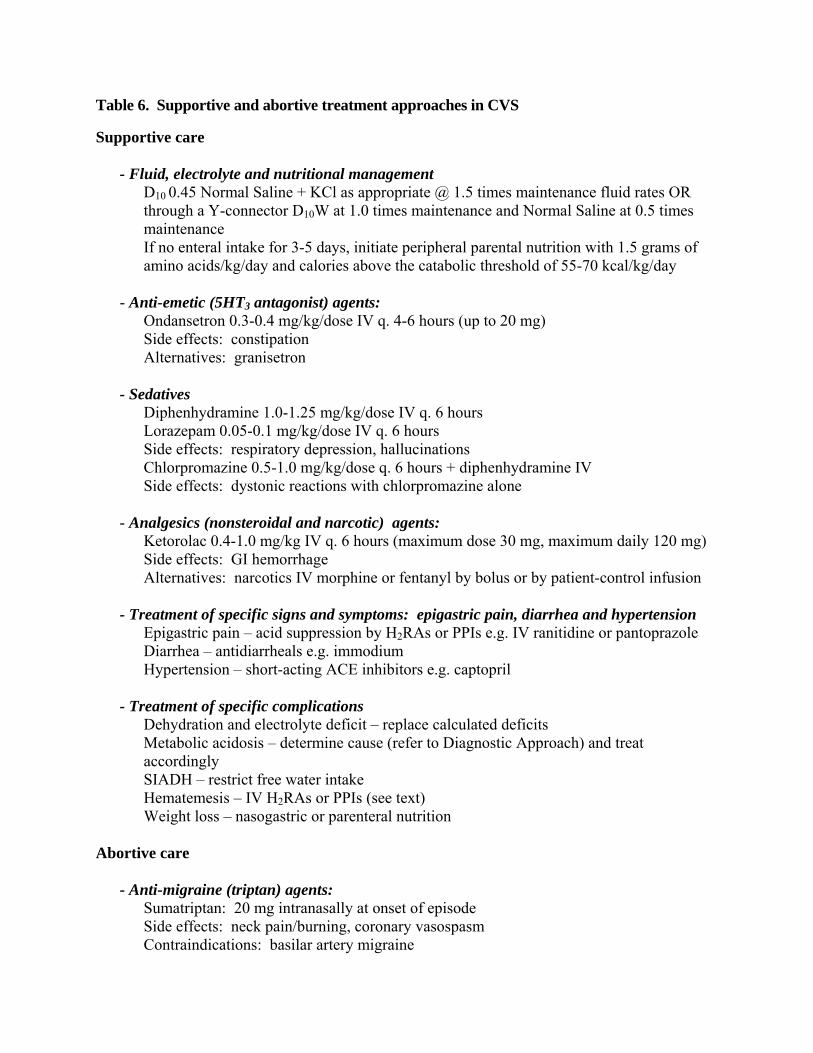
Table 6. Supportive and abortive treatment approaches in CVS Supportive care
- Fluid, electrolyte and nutritional management
D10 0.45 Normal Saline + KCl as appropriate @ 1.5 times maintenance fluid rates OR through a Y-connector D10W at 1.0 times maintenance and Normal Saline at 0.5 times maintenance If no enteral intake for 3-5 days, initiate peripheral parental nutrition with 1.5 grams of amino acids/kg/day and calories above the catabolic threshold of 55-70 kcal/kg/day
- Anti-emetic (5HT3 antagonist) agents:
Ondansetron 0.3-0.4 mg/kg/dose IV q. 4-6 hours (up to 20 mg) Side effects: constipation Alternatives: granisetron
- Sedatives
Diphenhydramine 1.0-1.25 mg/kg/dose IV q. 6 hours Lorazepam 0.05-0.1 mg/kg/dose IV q. 6 hours Side effects: respiratory depression, hallucinations Chlorpromazine 0.5-1.0 mg/kg/dose q. 6 hours + diphenhydramine IV Side effects: dystonic reactions with chlorpromazine alone
- Analgesics (nonsteroidal and narcotic) agents:
Ketorolac 0.4-1.0 mg/kg IV q. 6 hours (maximum dose 30 mg, maximum daily 120 mg) Side effects: GI hemorrhage Alternatives: narcotics IV morphine or fentanyl by bolus or by patient-control infusion
- Treatment of specific signs and symptoms: epigastric pain, diarrhea and hypertension
Epigastric pain – acid suppression by H2RAs or PPIs e.g. IV ranitidine or pantoprazole Diarrhea – antidiarrheals e.g. immodium Hypertension – short-acting ACE inhibitors e.g. captopril
- Treatment of specific complications
Dehydration and electrolyte deficit – replace calculated deficits Metabolic acidosis – determine cause (refer to Diagnostic Approach) and treat accordingly SIADH – restrict free water intake Hematemesis – IV H2RAs or PPIs (see text) Weight loss – nasogastric or parenteral nutrition
Abortive care
- Anti-migraine (triptan) agents: Sumatriptan: 20 mg intranasally at onset of episode Side effects: neck pain/burning, coronary vasospasm Contraindications: basilar artery migraine
NASPGHAN CVS Guidelines - 30
- Recovery and refeeding
Feed ad lib when child declares episode over
NASPGHAN CVS Guidelines - 31
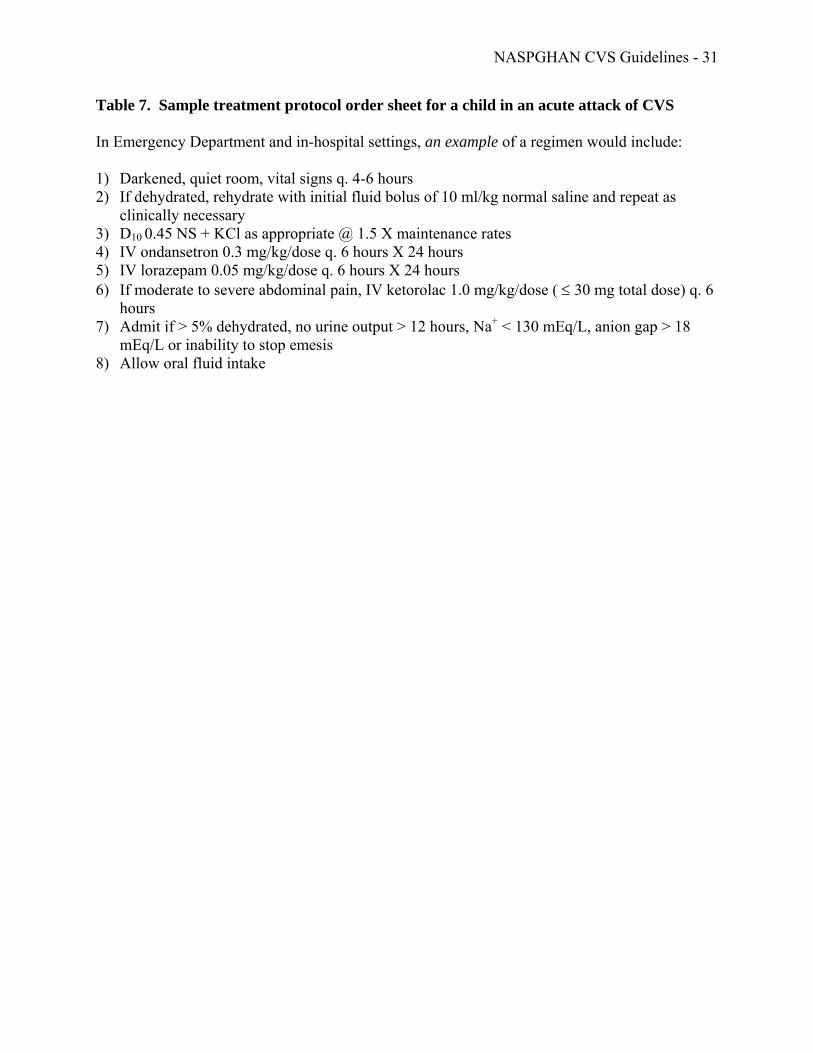
Table 7. Sample treatment protocol order sheet for a child in an acute attack of CVS In Emergency Department and in-hospital settings, an example of a regimen would include:
1) Darkened, quiet room, vital signs q. 4-6 hours 2) If dehydrated, rehydrate with initial fluid bolus of 10 ml/kg normal saline and repeat as
clinically necessary 3) D10 0.45 NS + KCl as appropriate @ 1.5 X maintenance rates 4) IV ondansetron 0.3 mg/kg/dose q. 6 hours X 24 hours 5) IV lorazepam 0.05 mg/kg/dose q. 6 hours X 24 hours 6) If moderate to severe abdominal pain, IV ketorolac 1.0 mg/kg/dose ( ≤ 30 mg total dose) q. 6
hours 7) Admit if > 5% dehydrated, no urine output > 12 hours, Na+ < 130 mEq/L, anion gap > 18
mEq/L or inability to stop emesis 8) Allow oral fluid intake
NASPGHAN CVS Guidelines - 32
Figure 1: Evaluation of Cyclic Vomiting Pattern in Children > 2 years old
Criteria for children in whom CVS is being considered: • At least 5 attacks or a minimum of 3 attacks occurring over a 6-month period • Episodic attacks of intense nausea and vomiting lasting from 1hour to 10 days
and occurring at least 1 week apart • Stereotypical in the individual patient • Vomiting during attacks occurs at least 4 times/hour for at least 1 hour • A return to baseline health between episodes
Attack with presence of: - Abdominal distention - Abdominal tenderness - Severe abdominal pain
All attacks precipitated by:
- intercurrent illness - high protein meal
Abnormal neurologic exam: - Severe alterated mental status - Abnormal eye movements - Papilledema* - Motor asymmetry - Gait abnormality (*may not need metabolic evaluation)
Consider at any time: -Ultrasound of the abdomen & pelvis
Obtained at the beginning of attack before IV fluid:
- glucose - electrolytes for anion gap - urine ketones - lactate - ammonia - serum aminoacids - urine organic acids - consider plasma carnitine &
acylcarnitine
Brain MRI
No findings
suggestive of
th
Electrolytes (Na+, K+, Cl-, HCO3-), glucose, BUN and creatinine
UGI series to evaluate for malrotation
Consider during an attack: - ALT/GGT - lipase ± amylase
Result of testing explains vomiting
Probable CVS Treat or refer accordingly
Yes No
NASPGHAN CVS Guidelines - 33
Bibliography
1. Gee S. On fitful or recurrent vomiting; 1882 1882. Report No.: 18. 2. Fleisher D, Matar M. The cyclic vomiting syndrome: a report of 71 cases and literature
review. JPGN 1993;17(4):361-9. 3. Hoyt CS, Stickler GB. A study of 44 children with the syndrome of recurrent vomiting.
Pediatrics 1960;25:775-80. 4. Li BU, Balint J. Cyclic vomiting syndrome: evolution in our understanding of a brain-gut
disorder. Adv Pediatr 2000;47:117-60. 5. Prakash C, Clouse R. Cyclic vomiting syndrome in adults: clinical features and response
to tricyclic antidepressents. Am J Gastroenterol 1999;94(10):2856-60. 6. Prakash C, Staiano A, Rothbaum RJ, Clouse RE. Similarities in cyclic vomiting
syndrome across age groups. Gastroenterology 2001;96(3):684-8. 7. Fleisher DR, Gornowicz B, Adams K, Burch R, Feldman EJ. Cyclic Vomiting Syndrome
in 41 adults: the illness, the patients, and problems of management. BMC Med 2005;3:20.
8. Whitney HB. Cyclic vomiting. A brief review of this affection as illustrated by a typical case. Arch Pediatr 1898;15:839-45.
9. Stickler GB. Relationship between cyclic vomiting syndrome and migraine. Clin Pediatr (Phila) 2005;44(6):505-8.
10. Withers GD, Silburn SR, Forbes DA. Precipitants and aetiology of cyclic vomiting syndrome. Acta Paediatr 1998;87(3):272-7.
11. Li BU, Murray RD, Heitlinger LA, Robbins J, Hayes J. Is cyclic vomiting syndrome related to migraine? J Pediatr 1999;134(5):567-72.
12. Wang Q, Ito M, Adams K, Li BU, Klopstock T, Maslim A, et al. Mitochondrial DNA control region sequence variation in migraine headache and cyclic vomiting syndrome. Am J Med Genet A 2004;131(1):50-8.
13. Boles RG, Adams K, Ito M, Li BU. Maternal inheritance in cyclic vomiting syndrome with neuromuscular disease. Am J Med Genet A 2003;120(4):474-82.
14. Boles RG, Le S, Maslim A, Adams K, Li BU, Higashimoto T, et al. Mitochondrial DNA control region sequence variations in cyclic vomiting syndrome with neuromuscular disease. unknown 2002.
15. Tache Y. Cyclic vomiting syndrome: the corticotropin-releasing-factor hypothesis. Dig Dis Sci 1999;44(8 Suppl.):79S-86S.
16. Sato T, Igarashi M, Minami S, Okabe T, Hashimoto H, Hasui M, et al. Recurrent attacks of vomiting, hypertension, and psychotic depression: a syndrome of periodic catecholamine and prostaglandin discharge. Acta Endocrinol (Copenh) 1988;117(2):189-97.
17. Sato T, Uchigata Y, Uwadana N, Kita K. A syndrome of periodic adrenocorticotropin and vasopressin discharge. J Clin Endocrinol Metab 1982;54(3):517-22.
18. Hayward RS, Steinberg EP, Ford DE, Roizen MF, Roach KW. Preventive care guidelines: 1991. American College of Physicians. Canadian Task Force on the Periodic Health Examination. United States Preventive Services Task Force. Ann Intern Med 1991;114(9):758-83.
19. Harris RP, Helfand M., Woolf, S.H. et al. Current methods of the U.S. Preventative Services Task Force: a review of the process. Am J Prev Med 2001;20(3 Suppl.):21-35.

NASPGHAN CVS Guidelines - 34
20. Hyman PE, Milla PJ, Benninga MA, Davidson GP, Fleisher DF, Taminiau J. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology 2006;130(5):1519-26.
21. Rasquin A, Di Lorenzo C, Forbes D, Guiraldes E, Hyams JS, Staiano A, et al. Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology 2006;130(5):1527-37.
22. Diagnostic criteria for cyclic vomiting syndrome. In: Li BU, editor. Cyclic vomiting syndrome: Proceedings of the International Scientific Symposium. J Pediatr Gastroenterol Nutr 1995;21(Suppl.).p. vi.
23. Pfau BT, Li BU, Murray RD, Heitlinger LA, McClung HJ, Hayes JR. Differentiating cyclic from chronic vomiting patterns in children: quantitative criteria and diagnostic implications. Pediatrics 1996;97(3):364-8.
24. Li BU, Murray RD, Heitlinger LA, Robbins J, Hayes JR. Heterogeneity of diagnosis presenting as cyclic vomiting. Pediatrics 1998;102((3 Pt. 1)):583-7.
25. Olson AD, Li BU. The diagnostic evaluation of children with cyclic vomiting: a cost-effectiveness assessment. J Pediatr 2002;141(5):724-8.
26. Heikkinen J, Vaheri R, Timonen U. Long-term safety and tolerability of continuous-combined hormone therapy in postmenopausal women: results from a seven-year randomised comparison of low and standard doses. J Br Menopause Soc 2004;10(3):95-102.
27. Torres AM, Ziegler MM. Malrotation of the intestine. World J Surg 1993;17(3):326-31. 28. Powell DM, Othersen HB, Smith CD. Malrotation of the intestines in children: the effect
of age on presentation and therapy. J Pediatr Surg 1989;24(8):777-80. 29. Long FR, Kramer SS, Markowitz RI, Taylor GE. Radiographic patterns of intestinal
malrotation in children. Radiographics 1996;16(3):547-56. 30. Schulte-Bockholt A, Kugathasan S, Mesrobian HG, Werlin SL. Ureteropelvic junction
obstruction: an overlooked cause of cyclic vomiting. Am J Gastroenterol 2002;97(4):1043-5.
31. Tsai JD, Huang FY, Lin CC, Tsai TC, Lee HC, Sheu JC, et al. Intermittent hydronephrosis secondary to ureteropelvic junction obstruction: clinical and imaging features. Pediatrics 2006;117(1):139-46.
32. Tobin MV, Aldridge SA, Morris AI, Belchetz PE, Gilmore IT. Gastrointestinal manifestations of Addison's disease. Am J Gastroenterol 1989;84(10):1302-5.
33. Woods M, Greenes D. An 11-year-old boy with vomiting, dehydration, and a tan complexion. Curr Opin Pediatr 1995;7(4):472-6.
34. Rinaldo P. Mitochondrial fatty acid oxidation disorders and cyclic vomiting syndrome. Dig Dis Sci 1999;44(8 Suppl.):97S-102S.
35. Lin JN. Intestinal malrotation and midgut volvulus: a 15-year review. J Formos Med Assoc 1995;94(4):178-81.
36. Friesen CA, Roberts CC. Cholelithiasis. Clinical characteristics in children. Case analysis and literature review. Clin Pediatr (Phila) 1989;28(7):294-8.
37. Buyukyavuz I, Ekinci S, Ciftci AO, Karnak I, Senocak ME, Tanyel FC, et al. A retrospective study of choledochal cyst: clinical presentation, diagnosis and treatment. Turk J Pediatr 2003;45(4):321-5.
38. Pieper-Bigelow C, Strocchi A, Levitt MD. Where does serum amylase come from and where does it go? Gastroenterol Clin North Am 1990;19(4):793-810.

NASPGHAN CVS Guidelines - 35
39. Agarwal N, Pitchumoni CS, Sivaprasad AV. Evaluating tests for acute pancreatitis. Am J Gastroenterol 1990;85(4):356-66.
40. Wesdorp I, Bosman D, de Graaff A, Aronson D, van der Blij F, Taminiau J. Clinical presentations and predisposing factors of cholelithiasis and sludge in children. J Pediatr Gastroenterol Nutr 2000;31(4):411-7.
41. Reinberg Y, Gonzalez R. Upper urinary tract obstruction in children: current controversies in diagnosis. Pediatr Clin North Am 1987;34(5):1291-304.
42. Stein JA, Tschudy DP. Acute intermittent porphyria. A clinical and biochemical study of 46 patients. Medecine (Baltimore) 1970;49(1):1-16.
43. Anderson KE, Bloomer JR, Bonkovsky HL, Kushner JP, Pierach CA, Pimstone NR, et al. Recommendations for the diagnosis and treatment of the acute porphyrias. Ann Intern Med 2005;142(6):439-50.
44. Costa CG, Guerand WS, Struys EA, Holwerda U, ten Brink HJ, Tavares de Almeida I, et al. Quantitative analysis of urinary acylglycines for the diagnosis of beta-oxidation defects using GC-NCI-MS. J Pharm Biomed Anal 2000;21(6):1215-24.
45. Boles RG, Adams K, Li BU. Maternal inheritance in cyclic vomiting syndrome. Am J Med Genet A 2005;133(1):71-7.
46. Boles RG, Williams JC. Mitochondrial disease and cyclic vomiting syndrome. Dig Dis Sci 1999;44(8 Suppl.):103S-7S.
47. Dobrovoljac M, Hengartner H, Boltshauser E, Grotzer MA. Delay in the diagnosis of paediatric brain tumours. Eur J Pediatr 2002;161(12):663-7.
48. Alston RD, Newton R, Kelsey A, Newbould MJ, Birch JM, Lawson B, et al. Childhood medulloblastoma in northwest England 1954 to 1997: incidence and survival. Dev Med Child Neurol 2003;45(5):308-14.
49. Kotagal P. The relationship between sleep and epilepsy. Semin Pediatr Neurol 2001;8(4):241-50.
50. Schauble B, Britton JW, Mullan BP, Watson J, Sharbrough FW, Marsh WR. Ictal vomiting in association with left temporal lobe seizures in a left hemisphere language-dominant patient. Epilepsia 2002;43(11):1432-5.
51. Boles RG, Burnett BB, Gleditsch K, Wong S, Guedalia A, Kaariainen A, et al. A high predisposition to depression and anxiety in mothers and other matrilineal relatives of children with presumed maternally inherited mitochondrial disorders. Am J Med Genet B Neuropsychiatr Genet 2005;137(1):20-4.
52. McClung HJ, Murray RD, Braden NJ, Fyda J, Myers RP, Gutches L. Intentional Ipecac poisoning of children. Am J Dis Child 1988;142(6):637-9.
53. Fleisher D. Management of cyclic vomiting syndrome. JPGN 1995;21(Suppl. 1):S52-S6. 54. Blumer JL. Off-label uses of drugs in children. Pediatrics 1999;104(3 Pt 2):598-602. 55. Fleisher D. Cyclic vomiting syndrome. In: Hyman P DC, editor. Pediatric
Gastroenterology Motility Disorders. New York, NY: Academy Professional Information Services; 1994. p. 89-104.
56. Lucarelli S, Corrado G, Pelliccia A, D'Ambrini G, Cavaliere M, Barbato M, et al. Cyclic vomiting syndrome and food allergy/intolerance in seven children: a possible association. Eur J Pediatr 2000;159(5):360-3.
57. Allen JH, de Moore GM, Heddle R, Twartz JC. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004;53(11):1566-70.
NASPGHAN CVS Guidelines - 36
58. Hoodin F, Brines BJ, Lake AE, 3rd, Wilson J, Saper JR. Behavioral self-management in an inpatient headache treatment unit: increasing adherence and relationship to changes in affective distress. Headache 2000;40(5):377-83.
59. Rasmussen BK. Migraine and tension-type headache in a general population: precipitating factors, female hormones, sleep pattern and relation to lifestyle. Pain 1993;53(1):65-72.
60. Lewis DW, Yonker M, Winner P, Sowell M. The treatment of pediatric migraine. Pediatr Ann 2005;34(6):448-60.
61. Lee WS, Kaur P, Boey CC, Chan KC. Cyclic vomiting syndrome in South-East Asian children. J Paediatr Child Health 1998;34(6):568-70.
62. Worawattanakul M, Rhoads J, Lichtman S, Ulshen M. Abdominal migraine: prophylactic treatment and follow-up. JPGN 1999;28(1):37-40.
63. Anderson JM, Sugerman KS, Lockhart JR, Weinberg WA. Effective prophylactic therapy for cyclic vomiting syndrome in children using amitriptyline or cyproheptadine. Pediatrics 1997;100(6):977-81.
64. Gokhale R, Huttenlocher P, Brady L, Kirschner BS. Use of barbituates in the treatment of cyclic vomiting during childhood. JPGN 1997;25(1):64-7.
65. Symon D. Pizotifen. In: Gallai V GV, editor. Juvenile Headache. Amsterday: Elsevier Science Publishers; 1991. p. 405-8.
66. Symon D, Russell G. Double blind placebo controlled trial of pizotifen syrup in the treatment of abdominal migraine. Arch Dis Child 1995;72(1):48-50.
67. Salmon MA, Walters DD. Pizotifen in the prophylaxis of cyclical vomiting. Lancet 1985;1(8436):1036-7.
68. Gutgesell H, Atkins D, Barst R, Buck M, Franklin W, Humes R, et al. Cardiovascular monitoring of children and adolescents receiving psychotropic drugs: A statement for healthcare professionals from the Committee on Congenital Cardiac Defects, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 1999;99(7):979-82.
69. Clouse RE, Sayuk GS, Lustman PJ, Prakash C. Zonisamide or levetiracetam for adults with cyclic vomiting syndrome: a case series. Clin Gastroenterol Hepatol 2007;5(1):44-8.
70. Van Calcar S, Harding C, Wolff J. L-carnitine administration reduces number of episodes in cyclic vomiting syndrome. Clinical Pediatrics 2002;41(3):171-4.
71. Welch KM, Darnley D, Simkins RT. The role of estrogen in migraine: a review and hypothesis. Cephalalgia 1984;4(4):227-36.
72. Johnston W. Acupuncture may treat cyclic vomiting syndrome. Anesth News 2000 5/2000.
73. Magagna J. Psychophysiologic treatment of cyclic vomiting. JPGN 1995;21(Suppl. 1):S31-S6.
74. Fleisher D. The cyclic vomiting syndrome described. JPGN 1995;21(Suppl. 1):S1-S5. 75. Benson J, Zorn S, Book L. Sumitriptan [Imitrex] in the treatment of cyclic vomiting. Ann
Pharm 1995;29(10):997-8. 76. Sandoval C, Corbi D, Strobino B, Fevzi Ozkaynak M, Tugal O, Jayabose S. Randomized
double-blind comparison of single high-dose ondansetron and multiple standard-dose ondansetron in chemotherapy-naive pediatric oncology patients. Cancer Invest 1999;17(5):309-13.
NASPGHAN CVS Guidelines - 37
77. Pasricha P, Schuster M, Saudek C, Wand G, Ravich W. Cyclic vomiting: association with multiple homeostatic abnormalities and response to ketorlac. Am J Gastroenterol 1996;91(10):2228-32.
78. Li BU, Misiewicz L. Cyclic vomiting syndrome: a brain-gut disorder. Gastroenterol Clin North Am 2003;32(3):997-1019.
79. Pohl JF, Melin-Aldana H, Rudolph C. Prolapse gastropathy in the pediatric patient. J Pediatr Gastroenterol Nutr 2000;30(4):458-60.
80. McRonald FE, Fleisher DR. Anticipatory nausea in cyclical vomiting. BMC Pediatr 2005;5(1):3.
81. Symon D, Russell G. Abdominal migraine: a childhood syndrome defined. Cephalalgia 1986;6(4):223-8.
82. Vanderhoof JA, Young R, Kaufmann SS, Ernst L. Treatment of cyclic vomiting syndrome in childhood with erythromycin. JPGN 1993;17(4):387-91.