CUTTING EDGEdbcms.s3.amazonaws.com/media/files/1dc27be8-52d6-42c7...by Cynthia Yoshida, MD, AGAF,...
32
Topics covered in this issue include: • A basic review of anatomy and physiology of the gastrointestinal tract (GI) • Gastroparesis • Diet intervention for the patient with gastroparesis • Celiac disease • Small bowel bacterial overgrowth • Constipation • Narcotic bowel syndrome Each article provides background information on the topic, signs and symptoms to aid in the identification and diagnosis, as well as the most current evidence to guide treatment interventions. Providing strategies to help patients with DM who present with GI complications to maximize their overall quality of life is at the heart of this OTCE issue. We were very fortunate to obtain an outstanding slate of authors. The article series begins with a tour of the GI tract by Cynthia Yoshida, MD, AGAF, entitled “How Well Do You Know Your Gut? Gastrointestinal Anatomy and Physiology.” This article reviews key structures and their functions. Each major segment of the GI tract is reviewed individually, beginning with the pancreas, then moving to the luminal GI tract, progressing from mouth to colon. Doing so allows you to easily cross-reference specific anatomical areas as you read the accompanying articles on diabetes complications. A Peer-Reviewed Publication Winter 2011 | Volume 32 | Number 6 GASTroINTESTINAl ISSuES ENCouNTErED IN DIAbETES MEllITuS oN THE Diabetes Care and Education CUTTING EDGE Message from the Theme Editor: Carol rees Parrish, MS, rD Nutrition Support Specialist university of Virginia Health System Digestive Health Center of Excellence Charlottesville, VA The patient with diabetes mellitus (DM) must devote constant attention to glycemic control or risk untoward inflammatory, neuropathic and myopathic effects from hyperglycemia (1,2) or, the scarier converse, a hypoglycemic episode. Attention must also be given to the amount of carbohydrates consumed. He or she might require daily oral medications, insulin injections or an insulin pump to achieve near euglycemia. As if management of these issues were not enough for an individual, additional complications of DM may ensue. one of the more vexing complications involves the gastrointestinal tract — the theme of this OTCE issue. 4 How Well Do You Know Your Gut? Gastrointestinal Anatomy and Physiology: A review 8 Gastroparesis Part I: Diagnosis and Treatment 12 Gastroparesis Part II: Nutritional Care 15 Celiac Disease and Diabetes Mellitus 18 Small bowel bacterial overgrowth in Diabetes Mellitus 22 Constipation in Patients with Diabetes Mellitus 26 Narcotic bowel Syndrome 31 2011-2012 DCE Officer Directory a dietetic practice group of the Diabetes Care and Education
-
Upload
trinhtuyen -
Category
Documents
-
view
216 -
download
0
Transcript of CUTTING EDGEdbcms.s3.amazonaws.com/media/files/1dc27be8-52d6-42c7...by Cynthia Yoshida, MD, AGAF,...

Topics covered in this issue include:• A basic review of anatomy and
physiology of the gastrointestinal tract (GI)
• Gastroparesis • Diet intervention for the patient
with gastroparesis • Celiac disease• Small bowel bacterial overgrowth• Constipation• Narcotic bowel syndrome
Each article provides background information on the topic, signs and symptoms to aid in the identification and diagnosis, as well as the most current evidence to guide treatment interventions. Providing strategies to help patients with DM who present with GI complications to
maximize their overall quality of life is at the heart of this OTCE issue.
We were very fortunate to obtain an outstanding slate of authors. The article series begins with a tour of the GI tract by Cynthia Yoshida, MD, AGAF, entitled “How Well Do You Know Your Gut? Gastrointestinal Anatomy and Physiology.”
This article reviews key structures and their functions. Each major segment of the GI tract is reviewed individually, beginning with the pancreas, then moving to the luminal GI tract, progressing from mouth to colon. Doing so allows you to easily cross-reference specific anatomical areas as you read the accompanying articles on diabetes complications.
A Peer-Reviewed Publication
Winter 2011 | Volume 32 | Number 6
GASTroINTESTINAl ISSuES ENCouNTErED IN DIAbETES MEllITuS
oN THE
Diabetes Care and EducationCUTTING EDGE
Message from the Theme Editor: Carol rees Parrish, MS, rDNutrition Support Specialistuniversity of Virginia Health System Digestive Health Center of Excellence Charlottesville, VA
The patient with diabetes mellitus (DM) must devote constant attention to glycemic control or risk untoward inflammatory, neuropathic and myopathic effects from hyperglycemia (1,2) or, the scarier converse, a hypoglycemic episode. Attention must also be given to the amount of carbohydrates consumed. He or she might require daily oral medications, insulin injections or an insulin pump to achieve near euglycemia. As if management of these issues were not enough for an individual, additional complications of DM may ensue. one of the more vexing complications involves the gastrointestinal tract — the theme of this OTCE issue.
4 How Well Do You Know Your Gut? Gastrointestinal Anatomy and Physiology: A review
8 Gastroparesis Part I: Diagnosis and Treatment
12 Gastroparesis Part II: Nutritional Care
15 Celiac Disease and Diabetes Mellitus
18 Small bowel bacterial overgrowth in Diabetes Mellitus
22 Constipation in Patients with Diabetes Mellitus
26 Narcotic bowel Syndrome
31 2011-2012 DCE Officer Directory
a dietetic practice group of the
Diabetes Care and Education

NewsFlASH and On the Cutting Edge are bi-monthly publications of the Diabetes Care and Education (DCE) Dietetic Practice Group of the Academy of Nutrition and Dietetics (the Academy).
Print Communications Coordinator:liz Quintana, EdD, rD, lD, CDE
Newsflash Editor:lorena Drago, MS, rD, CDN, CDE
On the Cutting Edge Editor:Alyce Thomas, rD
On the Cutting Edge associate Editor:Diane reader, rD, CDE
Publication in this DCE newsletter does not imply a statement of policy or endorsement by the DCE. The opinions expressed represent those of the authors and do not reflect official policy of the Academy.
Mention of product names in this publication does not constitute endorsement by DCE or the Academy.
All material appearing in the NewsFlASH and On the Cutting Edge is covered by copyright and may be photocopied or otherwise reproduced for noncommercial scientific or educational purposes only, provided the source is acknowledged. Special arrangements for permission are required from the Print Communications Coordinator for any other purpose.
Subscriptions are available for people who are ineligible for the Academy membership for $30 (domestic), $35 (international) by sending a check to:
linda flanagan Vahl DCE administrative Manageracademy of Nutrition and Dietetics120 south Riverside Plaza, suite 2000Chicago, Il 60606-6995
Payable to Academy of Nutrition and Dietetics/DCE noting preferred mailing address.
©2011 Diabetes Care and EducationDietetic Practice Group/Academy of Nutrition and Dietetics.All rights reserved.library of Congress National Serials Data Program ISSN #1070-5945, issued 7/93.
MIssIONDCE members are the most valued authorities on nutrition and diabetes prevention, education, and management.
VIsIONDCE members lead the future of nutrition and diabetes prevention, education, and management.
oN THE
Diabetes Care and EducationCUTTING EDGE Henry P. Parkman, MD, enlightens us
with his cutting-edge review on, “Gastroparesis Part I: Diagnosis and Treatment.” Gastroparesis, a gastric motility disorder characterized by gastric stasis in the absence of mechanical obstruction, is classically described in type 1 DM, but can also be seen in patients with type 2 DM. Evaluation consists of an assessment of delayed gastric emptying in a patient with appropriate symptoms. Treatment for gastroparesis requires several components, including dietary management, maximizing glucose control, antiemetic medications and prokinetic agents. This article prepares clinicians for evaluation and management of patients with diabetic gastroparesis. Complementing Dr. Parkman’s review of gastroparesis is an article I authored on a comprehensive approach to nutrition in those patients who suffer from this complication in, “Gastroparesis Part II: Nutritional Care.” Nutritional assessment, and oral diet suggestions are discussed, as well as when to employ enteral or parenteral nutrition support as primary or adjunctive therapy.
Celiac disease, an immune-mediated process, occurs in 1% to 16% of individuals with DM. Individuals with both DM and celiac disease may be at risk for other autoimmune
diseases, and should be evaluated by an endocrinologist and screened if appropriate. laurie A. Higgins, MS, rD, lDN, CDE provides a clear overview of transitioning from a diabetes meal planning lifestyle to one that incorporates celiac principles in a practical way.
John K. Dibaise, MD, introduces small intestinal bacterial overgrowth (SIbo) and its potential role in the patient with DM. SIbo is an excess number of bacteria (greater than 105 colony-forming units (cfu)/ml) in the proximal small intestine. SIbo may complicate the course of DM and result in a variety of gastrointestinal symptoms. The clinical features, nutritional complications and factors predisposing the patient with DM to SIbo are described, as are its diagnosis and treatment.
one very important aspect of care that is often not adequately discussed is constipation. In “Constipation in Patients with Diabetes Mellitus,” lawrence r. Schiller, MD, informs us that constipation affects many patients with long-standing DM and is a common GI complaint in this population. Patients with DM may have any of the causes of constipation found in the general population, but are more likely to have medication side effects, dietary
GOal 1: Sustain and grow a high level of satisfaction and retention among members.
use electronic technology to engage new and existing members.
Promote and support member professional development.
Maintain a high value of membership.
GOal 2: Advance DCE’s unique position as the authority in nutrition and diabetes prevention, education and management.
Promote and maintain new DCE image.
Develop domestic and global alliance and stakeholder relationships.
Promote and support evidence-based practice and research.
sTRaTEGIC PRIORITY aREas

3
OTCE Winter 2011 Acknowledgments
ThaNK YOU!To the following people for assisting with the development
of this issue of On the Cutting Edge:
ThEME TEaMCarol rees Parrish, MS, rD
liz Quintana, EdD, rD, lD, CDEAlyce Thomas, rD
REVIEwERs
Sally brozek, MS, rD, lD, CDEleila bruno, MS, rD, CDE
Johanna burani, MS, rD, CDEKim Campbell, rD, lDN, CDE
Nedra K. Christensen, PhD, rDrenee Davis, rD, CDE
Karen Ferrantella, rD, lDJane Giordano-Trosten, MS, rD
Heidi Gunderson, MS, rD, lD, CDE, ClTCarolyn Harrington, rD, CD, CDEAndrea Herbert, MS, rD, lD, CDE
Art Kress, MS, rD, lDNPaula K. leibovitz, MS, rD, CDN, CDE
lois Moss-barnwell, MS, rD, lDN, CDEKathryn Mount, MS, rD, lDN
Virginia o’Kelly, rD, CDEJennifer okemah, MS, rD, CDE, bC ADM
Dalia Perelman, MS, rD, CDEliz Quintana, EdD, rD, lD, CDE
Diane reader, rD, lD, CDElaura russell, rD, lrD, CDE
Florence Schermer, MS, rD, lD, CDECarol Sherman, MPH, rD, lD/N, CDE
Martie Slaughter, MHA, MS, MA, rD, lD, FACHE, FADA Kathi Taylor, MS, rD, lMNT, CDE
Alyce Thomas, rDlinda Flanagan Vahl
Sarah Williams, rD, lD, CDE
changes, and neuropathy as etiologic factors. Clinical management first and foremost depends on understanding what the patient means by constipation. Although fiber is often thought to be the cure for all constipation, in some patients, it may be detrimental. understanding the etiology behind each patient’s constipation is imperative to developing an appropriate treatment plan.
Nora Decher, MS, rD, CNSC, completes this issue by educating us on narcotic bowel syndrome, a newly recognized and underappreciated GI condition. Diabetic neuropathy occurs in over 30% to 50% of those with DM; 20% of whom experience pain associated with it. Despite a variety of pain medications available, only 40% to 60% of patients with neuropathic pain experience even partial relief, making its management a complex clinical issue. As such, those with refractory pain may require opioids. Narcotic bowel syndrome, a type of bowel dysfunction, is a serious problem that affects patients with chronic pain requiring narcotics, including neuropathic pain related to DM.
Much appreciation goes to Alyce Thomas, rD, Editor, and Diane reader, rD, CDE, Associate Editor, for their time, varied expertise and commitment to making this issue of OTCE both educational and practical. I also want to thank liz Quintana, EdD, rD, lD, CDE for her assistance in the planning stages of this issue.
references 1. Jensen Gl. Inflammation: an
expanding universe. Nutr Clin Pract. 2008;23:1–2.
2. Krenitsky J. Glucose control in the intensive care unit: a nutrition support perspective. Nutr Clin Pract. 2011;26:31–43.

4
AbstractSome of the most devastating complications of diabetes mellitus (DM) affect the luminal gastrointestinal (GI) tract and liver. These include: gastroparesis, small bowel bacterial overgrowth, diabetic diarrhea, constipation and non-alcoholic fatty liver disease. This article will review GI anatomy and physiology to aid the reader in understanding the complications discussed in the succeeding articles.
PancreasThe pancreas is divided into the head/uncinate process (situated within the C loop of the duodenum) and the body and the tail (located directly behind the stomach). The endocrine pancreas secretes hormones (e.g., insulin, glucagon, somatostatin and amylin) directly into the blood whereas the exocrine pancreas secretes digestive enzymes and alkaline pancreatic juice into the small intestine (SI) via the main pancreatic duct.
Endocrine PancreasThe endocrine pancreas is comprised of over a million islet cells with four distinct cell types: alpha cells (20%) produce glucagon, beta cells (68%) produce insulin and amylin, delta cells (10%) produce somatostatin, and PP cells (2%) produce pancreatic polypeptide.
Glucose homeostasis requires an intricate balance of pancreatic (e.g., insulin, glucagon, amylin) and gut modulators (e.g., glucagon-like peptide (GlP-1), glucose-dependent insulinotropic peptide (GIP), epinephrine, cortisol and growth hormone) that influence multiple target tissues (e.g., muscle, liver, brain, adipose). Circulating glucose derives from: 1) intestinal absorption following a meal; 2) hepatic glycogenolysis; and 3) hepatic/renal gluconeogenesis during fasting. blood glucose levels peak about 1.5 hours after a meal and after ~4 hours slowly return to fasting levels. Immediately after eating, a rapid release of pre-formed insulin (first-phase insulin) is initiated, increasing insulin levels before a rise in blood glucose. This phase of insulin secretion lasts ~10 minutes. Second phase, newly synthesized insulin is released to maintain blood glucose levels. Plasma half-life averages ~6 minutes; most circulating insulin is cleared rapidly within 10 to 15 minutes by insulinase enzymes in the liver, kidney and muscles.
Glucagon maintains basal glucose concentrations during fasting and exercise by glycogenolysis (during the first 12 hours of fasting) and by gluconeogenesis (with prolonged fasting or exercise). Amylin is secreted simultaneously with insulin after a meal by beta cells. Amylin
How Well Do You Know Your Gut?Gastrointestinal Anatomy and Physiology: A review
Cynthia Yoshida, MD, AGAFGastroenterologistCharlottesville, VA
works with insulin to manage blood glucose via three mechanisms: 1) suppresses postprandial glucagon secretion via centrally mediated vagal efferents, 2) slows gastric emptying to decrease nutrient transport from the stomach to the SI and 3) dose-dependently decreases food intake and body weight. Amylin exerts its actions through central nervous system receptors in the area postrema, which lacks a blood-brain barrier and allows exposure to rapid changes in plasma glucose levels.
Exocrine PancreasThe pancreas secretes ~1.5 liters of pancreatic juice (bicarbonate, water and digestive enzymes) daily into the duodenum via the pancreatic duct. Pancreatic exocrine secretion is regulated by vagal stimulation, secretin and cholecystokinin (CCK). The latter two gut hormones are produced by duodenal cells when gastric acid, peptides and luminal fatty acids reach the SI. Secretin stimulates pancreatic bicarbonate and hepatic bile secretion. CCK stimulates pancreatic digestive enzyme secretion and bile release from the gallbladder. Pancreatic enzymes include proteases, pancreatic lipase and amylase.
luminal GI Tractluminal GI tract functions include digestion, absorption and defecation. The adult human GI tract is ~ 8 meters long and includes:

5
• Mouth / oropharynx / cricopharyngeus
• Esophagus, gastroesophageal junction
• Stomach, pylorus• Small Intestine (duodenum,
jejunum, ileum) / ileocecal valve• large Intestine (colon) / rectum
Gastrointestinal MotilityGI motility mixes and propagates the food bolus from mouth to rectum. GI contraction involves peristalsis, segmentation and the migrating motor complex. Segmentation mixes food with enzymes and allows for maximal epithelial contact for efficient absorption. Migrating motor complex (between meals) peristaltic wave cycles last 5 to 15 minutes and repeat every 1 to 2 hours to remove excess food and bacteria. Motility is controlled by the vagus nerve. Contractile activity varies by location. It takes 8 to 20 seconds for peristalsis to proceed down the length of the esophagus. Gastric slow waves occur at three cycles per minute and originate from a pacemaker in the body of the stomach. Duodenal contractions occur ~12 cycles/minute. In the colon, non-propagating, mixing contractions occur at 2 to 4 cycles per minute. Mass motor movements (high amplitude propagating contractions usually resulting in defection) are infrequent and occur ~ one to two times a day.
Mouth, oropharynx, CricopharyngeusChewing increases food surface area and lubricates the bolus with saliva (water, mucins and bicarbonate to maintain pH 6.5-7.5). Salivary amylase initiates the digestion of starch to maltose.
Swallowing is a complex coordination of nerves and muscles that occurs in two phases:
1) oral phase (one second) — lip closure and anterior to posterior tongue movement pushing food to the oropharynx and
2) Pharyngeal phase (one second) — velum elevation, velopharyngeal port closure (to prevent food from entering the nasal cavity), and initiation of pharyngeal peristalsis
once the larynx is elevated and closed and the cricopharyngeus (upper esophageal sphincter) relaxes, the bolus passes from the pharynx to esophagus.
EsophagusThe esophagus is a 25-30 cm muscular tube that propagates food from pharynx to stomach. It is lined with non-keratinized stratified squamous epithelium, and submucosal glands secrete mucin, bicarbonate, epidermal growth factor and prostaglandin E2, which protect the mucosa from gastric acid. The gastroesophageal junction is made up of the lower esophageal sphincter (lES) and the skeletal muscle right diaphragmatic crus. remaining closed at rest and after swallowing, the lES relaxes to allow food to pass into the stomach.
StomachThe stomach accommodates and stores the meal, triturates food into smaller particles, and controls emptying into the duodenum. When empty, gastric volume is ~50 ml but can expand to ~4 liters. Gastric parietal cells produce 1.5 to 2 liters of acid daily resulting in a pH between 1 to 2; peak basal secretion occurs in the evening. Acid secretion is regulated by neural, paracrine and endocrine factors. receptors that relay information stimulating gastric antral G cells to secrete gastrin into the bloodstream are stretched by
gastric distension with food stimulates. Gastrin stimulates parietal cell secretion of hydrochloric acid, and is inhibited by gastric pH less than 4 and by somatostatin. There are three phases of gastric acid secretion:
1) cephalic phase (30% of gastric acid produced) when food is smelled/tasted
2) gastric phase (60%) after stomach distension and protein digestion
3) intestinal phase (10%) following SI distension.
Vasoactive inhibitory peptide (VIP), CCK and secretin inhibit acid production. Gastric mucosal cells are protected from acid by a mucus gel layer. Patients with frequent vomiting lose excess chloride and acid resulting in profound metabolic alkalosis.
Gastric chief cells secrete pepsinogen which breaks down to active pepsin in acidic conditions. Food-bound vitamin b-12 is released by gastric acid and is bound to r protein (haptocorrin). Pancreatic enzymes cleave b-12-r protein complex in the SI. After cleavage, intrinsic factor (secreted by gastric parietal cells) binds with vitamin b-12. Intrinsic factor is required for absorption of food-bound vitamin b-12 (but not synthetic b-12) in the terminal ileum.
Gastric emptying is controlled by the calorie content of the meal; the stomach delivers ~150 kilocalories per hour to the duodenum. Increased size/energy density of a meal results in increased rates of gastric emptying. Duodenal mucosal receptors for fatty acids (FA), amino acids (AA) and carbohydrates (CHo) regulate neural/humoral feedback mechanisms. GIP, CCK, secretin and enteroglucagon decrease gastric motility. Within the ileum and colon,
6
chyme delays gastric transit (“ileal brake”) allowing more time for digestion and absorption. Chyme is delivered to the duodenum at a controlled rate to allow adequate mixing with pancreaticobiliary secretions. Consistency, viscosity, pH, osmolality, lipid and caloric content determine the rate of stomach-emptying. The pylorus controls gastric emptying by selectively allowing rapid passage of liquids and retention of solid particles greater than 2 millimeters in size.
Small IntestineThe small intestine (SI) is ~600 cm long and is comprised of the duodenum (26 cm), jejunum (250 cm) and ileum (350 cm). The term “small” intestine refers to the smaller diameter (3 cm) as compared to the large intestine (7 cm).
With a majority of digestion occurring in the SI, trypsin and chymotrypsin – proteolytic pancreatic enzymes – are secreted into the duodenum to cleave proteins into smaller peptides. Intestinal brush border peptidases (carboxypeptidase, aminopeptidase, dipeptidase) break down di- and tri-peptides into individual AA. lipid metabolism also occurs in the proximal SI. Pancreatic lipase is secreted into the duodenum and breaks down triglycerides into free fatty acids and monoglycerides. CHo digestion begins in the mouth with salivary amylase; in the SI, pancreatic amylase cleaves CHo into oligosaccharides. brush border enzymes dextrinase, glucoamylase, maltase, sucrase and lactase further break down oligosaccharides.
Nutrient absorption occurs through finger-like SI mucosal villi. Each villus is covered in microvilli to increase SI surface area (equivalent to a doubles tennis court). Glucose and AA are
transported via active transport into the intestinal cells and then into the capillaries. Glycerol and FA enter villi by passive diffusion and are reassembled into triglycerides. They combine with proteins, expelled by exocytosis, then move into the lacteals for transport via the lymphatic system. Most nutrients are absorbed in the jejunum with the following exceptions: 1) iron absorbed in the duodenum, and 2) bile salts and food-bound vitamin b-12 absorbed in the ileum.
The majority of chemical digestion occurs in the duodenum, the shortest SI segment. Secretin, released in the duodenum in response to acid gastric chyme, stimulates pancreatic bicarbonate and enzymes (e.g., trypsin, lipase and amylase) secretion. CCK, released by duodenal epithelial cells following fatty stimuli, stimulates the liver and gallbladder to bile release to aid in lipid digestion. Mucus is secreted by brunner’s glands. The majority of nutrient absorption occurs in the jejunum whose longer villi and plicae circulares maximize surface area. Jejunal pH remains ~7 to 8. The ileum — the most distal portion of the SI — absorbs residual nutrients that are not absorbed by the jejunum including food-bound vitamin b-12; bile salts are absorbed in the terminal ileum. by regulating the flow of liquid chyme into the colon, the ileocecal valve functions as a one-way valve.
Fluid Secretion in the GI tract between 6 to 7 liters of fluid are secreted into the GI tract every day. This includes: saliva (1to 1.5 liters), stomach (1.5 to 2.5 liters), bile (0.5 to 1 liter), pancreas (1 to 1.5 liters), SI (1 to 1.8 liters). Electrolytes and water make up most of the volume of secreted fluids. Ions (hydrogen,
potassium, chloride, sodium, bicarbonate) are initially secreted then reabsorbed along the GI tract. bicarbonate secretion neutralizes gastric acid and prevents degradation of digestive enzymes. Digestive enzymes are secreted by the mouth, stomach, intestines and pancreas. Some (e.g., lactase) are embedded in the SI epithelium. Gastric chief cells secrete pepsinogen which is activated by gastric acid to active pepsin. bile is made up of bile salts, bilirubin and cholesterol. It is produced in the liver, stored in the gallbladder and released into the duodenum via the common bile duct after a meal. bile salts facilitate fat absorption by forming hydrophilic emulsion (micelles). bile salts are reabsorbed in the terminal ileum, returned via the portal vein to the liver, and reused. This enterohepatic circulation handles ~30 grams of bile acids daily. A small amount escapes and is lost in the feces. Mucus is secreted in the stomach, small and large intestine to lubricate and protect the intestinal epithelium.
ColonThe colon is 150 cm in length. The main function of the colon is to absorb the remaining water and electrolytes and to compact and store fecal matter prior to defecation. When chyme enters the colon, greater than 80% of dietary liquid and GI secretions have been absorbed. If water is not absorbed, diarrhea can result, causing dehydration and ion loss. Colonic transit time is ~20 to 25 hours. The colon also absorbs vitamin K which is produced by colonic bacteria.
Dietary fiber is comprised of: 1) soluble (functional/prebiotic) fiber that is fermented by colonic bacteria to form gases and short-chain fatty acids, and 2) insoluble (non-

7
functional) fiber that bulks/softens stool, absorbs water and shortens transit time. Short-chain fatty acids (acetate, proprionate and butyrate) lower colonic pH and enhance the colonic mucosal barrier. butyrate nourishes colonocytes.
Fecal matter is composed of 75% water and 25% solids. one-third of the solids are intestinal bacteria, the other two-thirds are undigested materials. between 300 to 1000 different species of bacteria reside within the colon to make up the intestinal microbiota or “flora.” bacterial fermentation of undigested carbohydrate results in the formation of several gases: nitrogen, carbon dioxide, hydrogen, methane and hydrogen sulfide.
liverThe liver, the largest solid organ, weighs 1.5 kilograms. Hepatocytes perform over 500 functions and produce over 1000 essential enzymes. The liver’s major functions include:
• bile synthesis — hemoglobin is broken down to bilirubin/biliverdin, which are then combined with bile salts/cholesterol to make bile. The bile then drains from the bile canaliculi into the common bile duct to be temporarily stored in the gallbladder or secreted into the duodenum to aid in fat emulsification.
• Carbohydrate metabolism — gluconeogenesis, glycogenolysis, glycogenesis and the breakdown of many hormones (e.g., insulin, glucagon).
• lipid metabolism — cholesterol synthesis and lipogenesis.
• Protein synthesis/metabolism — produces albumin, a major
blood osmotic protein. The liver also produces blood clotting factors, proteins C and S and antithrombin; and converts lactate to alanine and ammonia to urea.
• Detoxification — metabolizes many toxic substances/drugs (e.g., acetaminophen).
• Storage — glucose (as glycogen), vitamin b-12, iron, copper and vitamin A.
• Immunologic effects — hepatic reticuloendothelial cells clear antigens from the portal circulation so they do not reach the systemic circulation.
Summaryunderstanding GI anatomy/physiology is paramount to the management of disease. While this article cannot be all-inclusive, hopefully, it will aid the registered dietitian in understanding the following articles that discuss the GI complications of DM.
resource list• Feldman M, Friedman lS, brandt lJ.
Sleisenger and Fordtran’s Gastrointestinal and Liver Disease, Ninth Edition. Philadelphia, PA: Wb Saunders; 2010.
• Yamada T, Alpers DH, Kalloo AN, Kaplowitz N, owyang C, Powell DW. Textbook of Gastroenterology, 5th Edition. Hoboken, NJ: Wiley-blackwell; 2009.
• bowen rA, Austgen l, rouge M. Pathophysiology of the Digestive System. Available at http:// www.vivo.colostate.edu/hbooks/pathphys/digestion/. Accessed February 2, 2011.
CPE CrEDITANSWER KEY
See the CPE credit self-assessment questionnaire on page 30.
1. b
2. c
3. d
4. d
5. c
6. a
7. b
8. e
9. d
10. c

8
AbstractGastroparesis is a gastric motility disorder characterized by symptoms and evidence of gastric stasis in the absence of mechanical obstruction. Classically described in type 1 diabetes mellitus, gastroparesis can also be seen in patients with type 2 diabetes. Evaluation consists of demonstrating delayed gastric emptying with the absence of obstruction or mucosal disorders in a patient with appropriate symptoms. Treatment for gastroparesis primarily involves dietary management; improving glucose control; and taking antiemetic and prokinetic agents.
IntroductionA gastric motility disorder characterized by symptoms of, and evidence for, gastric retention in the absence of mechanical obstruction, gastroparesis can occur in many clinical settings with varied symptoms and severity of those symptoms (1). This article will cover the evaluation and management of patients with gastroparesis, particularly diabetic gastroparesis.
overviewGastroparesis is a well-recognized complication of diabetes mellitus (DM) that has a significant impact on quality of life. Those with type I diabetes mellitus (T1DM) have a higher prevalence of gastroparesis (30% to 50%) than those with type 2
diabetes mellitus (T2DM) (15% to 30%). A similar number of patients present with gastroparesis of an idiopathic, or unknown, nature (2). Post-surgical gastroparesis, often with vagotomy, represents the third most common etiology of gastroparesis.
Classically, gastroparesis occurs in patients with long-standing T1DM with associated complications of DM, such as retinopathy, nephropathy and peripheral neuropathy (3). Many patients may have other signs of autonomic dysfunction, including postural hypotension. Gastroparesis may also occur in patients with T2DM. Patients who have had DM for a relatively short time may experience accelerated emptying from impairment of fundic relaxation caused by vagal dysfunction.
In patients with DM, delayed gastric emptying contributes to erratic glycemic control because of unpredictable delivery of food into the duodenum. Delayed gastric emptying of nutrients, in conjunction with insulin administration, may produce hypoglycemia. Conversely, acceleration of the emptying of nutrients with prokinetic agents has been reported to cause early postprandial hyperglycemia. Difficulty in the control of blood glucose levels may be an early indication that a patient with diabetes is developing gastric motor
Gastroparesis Part I: Diagnosis and Treatment
Henry P. Parkman, MDProfessor of MedicineTemple university School of MedicinePhiladelphia, PA
dysfunction. Hyperglycemia itself can further delay gastric emptying (4).
Evaluation of Patients With Suspected GastroparesisA careful history and physical examination is important in patient evaluation (1). Symptom onset and progression of the disease with understanding of exacerbation periods are particularly important. reviewing the patient’s medications will help identify and eliminate medications that can aggravate symptoms. Physical examination may reveal signs of dehydration or malnutrition.
laboratory studies may help identify electrolyte abnormalities, renal insufficiency, anemia, pancreatitis, or thyroid dysfunction. In females with the recent onset of symptoms, a pregnancy test should be obtained. An abdominal obstruction series evaluates for mechanical gastric outlet or small bowel obstruction. Most patients need an upper endoscopy to exclude mechanical obstruction or ulcer disease. The presence of retained food in the stomach after overnight fasting is suggestive of gastroparesis. bezoars may be found in severe cases.
The classic test for measurement of gastric emptying is scintigraphy (4). Gastric emptying scintigraphy of a

9
solid-phase meal is often used for diagnosis. Patients should discontinue medications that may affect gastric emptying (See Table). For most medications, this will be 48 to 72 hours. opiate analgesics and anticholinergic agents delay gastric emptying. Prokinetic agents that accelerate emptying may give a falsely normal gastric emptying result. Serotonin receptor antagonists such as ondansetron, which have little effect on gastric emptying, may be given for severe symptoms before performance of gastric scintigraphy. Hyperglycemia (glucose level greater than 270 mg/dl) delays gastric emptying in those with DM (1). If hyperglycemia is present on the morning of the test, it is reasonable to defer gastric emptying testing until relative euglycemia is achieved to obtain a reliable determination of emptying parameters.
A wireless motility capsule (SmartPill) can assess gastric emptying by the acidic gastric residence time of the capsule (5). In addition, this capsule can assess whole gut transit including small bowel and colonic transit. A 13C-ocanoate breath test is being investigated for the measurement of gastric emptying (6).
Treatment of GastroparesisThe general principles for treating symptomatic gastroparesis are: 1) to correct and prevent fluid, electrolyte and nutritional deficiencies; 2) to control symptoms; and 3) to identify and rectify the underlying cause of gastroparesis, if possible (1,7). Management of patients with gastroparesis can be particularly challenging. Care of patients generally relies on dietary modification, medications that stimulate gastric motor activity and
antiemetic drug therapy. For patients with severe gastroparesis, treatment may include enteral nutritional support through a jejunostomy tube and/or use of gastric electric stimulation.
Dietary TreatmentSee the following article by Parrish on gastroparesis nutritional care.
Metabolic ControlIncreasing glucose control helps reduce symptoms, improves gastric emptying and enhances efficacy of prokinetic agents. Diabetes patients with gastroparesis frequently exhibit labile blood glucose concentrations with prolonged periods of significant hyperglycemia. Hyperglycemia greater than 270 mg/dl can delay gastric emptying.
Prokinetic AgentsCurrent prokinetic agents enhance gastric emptying and are used to treat gastroparesis. Metoclopramide (Reglan)Metoclopramide, with its antinausea and prokinetic actions, is widely used
for the treatment of gastroparesis. This medication serves as a dopamine receptor antagonist both in the CNS and in the stomach. Metoclopramide provides symptomatic relief and accelerates gastric emptying. It is effective for short-term treatment of gastroparesis for up to six to eight weeks. Symptomatic improvement does not necessarily accompany improvement in gastric emptying. The usual dosage is 10 mg four times a day.
unfortunately, side effects are relatively common with metoclopramide; it can cause both acute and chronic CNS side effects in some patients. Although rare, acute dystonic reactions can occur. Treatment over several weeks may produce depression or anxiety. rare cases of tardive dyskinesia have been reported with long-term treatment. Consequently, the FDA issued a “black box” warning against long-term treatment (defined as greater than 3 months). (www.fda.gov/newsevents/newsroom/pressannouncements/ucm149533.htm).
Erythromycin The antibiotic erythromycin exerts prokinetic effects via action on gastroduodenal receptors for motilin, an endogenous peptide responsible for initiation of the phase III migrating motor complex in the stomach. Erythromycin has been shown to stimulate gastric emptying in gastroparesis. In studies on oral erythromycin with symptom assessment as a clinical end point, improvement was noted in 43% of patients. oral administration of erythromycin should be initiated at low doses (e.g., 125 mg prior to meals). liquid suspension erythromycin may be preferred because it is rapidly and more reliably absorbed. Side effects of
Delay Gastric Emptying• opiate narcotic opioid analgesics• Anticholingergic agents• Calcium channel blockers• Anti-diabetes agents o Pramlintide, an amylin-like
compound o Exenatide, a GlP-1 receptor
agonist
accelerate Gastric Emptying• Prokinetic agents o Metoclopramide o Domperidone o Erythromycin o Azithromycin
Table. Medications That May Affect Gastric Emptying
Adapted from: Parkman HP, Hasler Wl, Fisher rS. Gastroenterology. 2004;127:1592-1622.
10
erythromycin at higher doses include nausea, vomiting and abdominal pain. Erythromycin should be used with caution along with other agents that inhibit cytochrome P450, such as calcium channel blockers.
Domperidone (Motilium)Domperidone’s effect on the upper gut is similar to those of metoclopramide, including stimulation of antral contractions, promotion of antroduodenal coordination and enhancement of gastric emptying. Domperidone does not readily cross the blood-brain barrier; therefore, it is much less likely than metoclopramide to cause extrapyramidal side effects. In addition to prokinetic actions in the stomach, domperidone exhibits antiemetic properties via action on the area postrema, a brainstem region with a porous blood-brain barrier. Side effects of domperidone include galactorrhea and amenorrhea. Even though it is not approved in the u.S., the FDA has developed a program for physicians who would like to prescribe domperidone for their patients with severe upper GI motility disorders. The program encompasses refractory to standard therapy (http://www.fda.gov/Drugs/DrugSafety/Informationby DrugClass/ucm073070.htm).
Antiemetic MedicationsAntiemetic agents are given acutely for symptomatic nausea and vomiting (1,7,8). Principal classes of medications used for these symptoms are phenothiazines, antihistamines, anticholinergics, dopamine receptor antagonists and serotonin receptor antagonists. The antiemetic action of phenothiazine compounds appear to be mediated primarily through a central antidopaminergic mechanism in the
area postrema of the brain. Commonly used agents include: prochlorperazine (Compazine), trimethobenzamide (Tigan), and promethazine (Phenergan). Serotonin (5-HT3) receptor antagonists, such as ondansetron (Zofran) and granisetron (Kytril), have been shown to be helpful in treating or preventing chemotherapy-induced nausea and vomiting. Since there is a high density of 5-HT3
receptors in the area postrema, the primary site of action for these compounds is probably the chemoreceptor trigger zone.
Psychotropic Medications as Symptom ModulatorsTricyclic antidepressants may have significant benefits in suppressing symptoms in some patients with nausea and vomiting as well as patients with abdominal pain (9). The dosage of tricyclic antidepressants used is lower than that used to treat depression. A reasonable starting dose for these agents is 10 to 25 mg at bedtime. If benefit is not observed in several weeks, doses are increased by 10- to 25-mg increments, up to 50 to 75 mg. Side effects can interfere with management and lead to a change in medication in 25% of patients who use tricyclic antidepressants. Secondary amines, such as nortriptyline and desipramine, may have fewer side effects. There are limited data on the use of selective serotonin reuptake inhibitors in gastroparesis.
Pyloric botulinum Toxin InjectionGastric emptying is a highly regulated process reflecting the integration of the propulsive forces of proximal fundic tone and distal antral contractions with the functional resistance provided by the pylorus. Several open-label studies
have tested the effects of pyloric injection of botulinum toxin in small numbers of patients with diabetic and idiopathic gastroparesis. During these studies, mild improvements in gastric emptying and modest reductions in symptoms for several months were observed. Two double-blind, placebo-controlled studies reported an improvement in gastric emptying, but no improvement in symptoms compared to placebo (10,11). Thus, botulinum toxin injection into the pylorus is not a long-term treatment option for gastroparesis.
Gastric Electric StimulationGastric electric stimulation (GES) is a treatment for refractory gastroparesis (12). Currently, it involves stimulating wires sutured into the gastric antrum with placement of a subcutaneous pulse generator that delivers a high-frequency (12 cpm), low-energy signal with short pulses. based on the initial studies that have shown symptom benefit, especially in patients with diabetic gastroparesis, the gastric electric neurostimulator was granted humanitarian approval from the FDA for the treatment of chronic, refractory nausea and vomiting secondary to idiopathic or diabetic gastroparesis.
The main complications of GES have been infection and intestinal obstruction, which has necessitated device removal in approximately 5% to 10% of cases. A small minority of patients can have temporary shocking sensations. Symptoms of nausea and vomiting can improve with stimulation; however abdominal pain often does not (13). Patients who have a favorable response to GES generally:
• have primary symptoms of nausea and/or vomiting
• are not taking narcotic pain

11
medications that do not have an adequate response to antiemetic and prokinetic medications.
SummaryThe gastrointestinal symptoms prevalent in patients with diabetes contribute a negative impact on the quality of life. Gastroparesis can affect patients with either T1DM or T2DM. Poor glycemic control is associated with an increased prevalence of GI symptoms. Careful patient evaluation to ensure the proper diagnosis and appropriate management can improve symptoms and quality of life in patients with diabetic gastroparesis.
references 1. Parkman HP, Hasler Wl, Fisher rS.
American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology. 2004;127:1592–1622.
2. Soykan I, Sivri b, Sarosiek I, Kiernan b, McCallum bW. Demography, clinical characteristics, psychological profiles, treatment and long-term follow-up of patients with gastroparesis. Dig Dis Sci. 1998;43:2398–2404.
3. Camilleri M. Clinical Practice — Diabetic gastroparesis. N Engl J Med. 2007;356:820–829.
4. Abell Tl, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy. a joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am J Gastroenterol. 2008;103:753–763.
5. Kuo b, McCallum rW, Koch K, et al. Comparison of gastric emptying of a non-digestible capsule to a radiolabeled meal in healthy and gastroparetic subjects. Aliment Pharmacol Ther. 2008;27:186–189.
6. bromer MQ, Kantor SN, Wagner DA, Knight MD, Maurer AH, Parkman HP. Simultaneous measurement of gastric emptying with a simple muffin meal using [13C]octanocate breath test and scintigraphy in normal subjects and patients with in dyspeptic symptoms. Dig Dis Sci. 2002;47:1657–1663.
7. Abell Tl, bernstein rK, Cutts T, et al. Treatment of gastroparesis: a multidisciplinary review. Neurogastroenterol Motil. 2006;18:263–283.
8. Quigley EMM, Hasler W, Parkman HP. AGA Technical review on nausea and vomiting. Gastroenterology. 2001;120: 263–286.
9. Prakash C, lustman PJ, Freedland KE, Clouse rD. Tricyclic antidepressants for functional nausea and vomiting: clinical outcome in 37 patients. Dig Dis Sci. 1998; 43:1951–1956.
10. Friedenberg FK, Palit A, Parkman HP, et al. botulinum toxin A for the treatment of delayed gastric emptying. Am J Gastroenterol. 2008;103:416–423.
11. Arts J, Holvoet l, Caenepeel P, et al. Clinical trial: a randomized-controlled crossover study of intrapyloric injection of botulinum toxin in gastroparesis. Aliment Pharmacol Ther. 2007;26:1251–1258.
12. Abell T, McCallum r, Hocking M, et al. Gastric electrical stimulation for medically refractory gastroparesis. Gastroenterology. 2003;125: 421–428.
13. Maranki Jl, lytes V, Meilahn JE, et al. Predictive factors for clinical improvement with Enterra gastric electric stimulation treatment for refractory gastroparesis. Dig Dis Sci. 2008;53:2072–2078.

12
IntroductionIn part I of the discussion on gastroparesis, Dr. Parkman discussed the diagnosis and treatment. The discussion continues in part II with a review of the nutritional assessment and intervention in the patient with gastroparesis as a result of diabetes mellitus (DM).
Nutritional AssessmentPatients with gastroparesis are at risk for fluid, electrolyte and nutrient deficits; and in those with DM, erratic glycemic control. Medications are important in the treatment of gastroparesis (see preceding article). At the initial clinic visit, it is important to establish nutrition goals with the gastroparetic patient, including:
• Stabilize weight loss• Improve glycemic control• replete nutritional deficiencies• Manage symptoms • Maintain hydration status• Avoid hospitalization • Improve overall quality of life
Weight lossThe most clinically apparent marker of nutritional depletion is unintentional weight loss. losing 5% to 10% of one’s usual body weight over 3 to 6 months is indicative of severe malnutrition (1). Significant weight loss requires close monitoring on the part of the clinician to identify those in need of nutrition support sooner vs. later while the GI work-up continues. Assessing
hydration status first is always important in patients with gastroparesis. In experiencing diabetic ketoacidosis or ongoing nausea and vomiting, weight loss can appear greater than it truly is. When using weight loss as an assessment tool, it is essential to compare a patient’s usual body weight with his or her current actual weight. Comparing a patient’s actual weight to an ideal body weight can either mask the seriousness of their weight loss (if overweight to begin with), or overestimate the loss (if underweight to begin with).
Hemodialysis patients are at high risk for gastroparesis (2), which may go unappreciated as nausea is frequently attributed to dialysis itself, or perhaps other co-morbidities (1). Monitoring these patients for serial weight loss below their target weight over time is essential. It is also important to investigate the possibility of gastroparesis in those patients who complain of fullness, especially in the morning, upon waking. Discuss a weight goal with the patient and physician. Decide on how much weight loss (if any), or lack of weight gain, is acceptable for that individual patient. The team should also discuss the possibility of more aggressive inter-vention if the weight goal is not met.
Diet HistoryAn initial 3 to 5 day record of all food and fluids ingested can help identify those patients in need of earlier
Gastroparesis Part II: Nutritional Care
Carol rees Parrish, MS, rDNutrition Support SpecialistDepartment of Nutrition Servicesuniversity of Virginia Health SystemCharlottesville, VA
nutrition support. Specifically, look for food groups avoided such as red meats, milk products or very high-fiber, greasy or fatty foods. Patients who consume large meals one to three times a day may do well on a regimen of smaller, frequent meals. replacing solid foods with more nutritious liquids may allow some patients to meet their nutritional requirements (1).
laboratory DataIt has long been established that albumin and prealbumin are reflections of the severity of illness and not a marker of nutritional status (3). Periodic glycemic monitoring, through the use of glycosylated hemoglobin, provides insight into overall glucose control. It is well-established that hyperglycemia cannot only aggravate gastroparesis and attenuate the prokinetic action of erythromycin, but also may accelerate the catabolic process and weight loss (1). Avoid wide swings in serum glucose in particular (4).
bowel Habitsone aspect of care that is often overlooked is a patient’s normal bowel routine. Constipation, in particular, can exacerbate symptoms in a patient with gastroparesis and be indicative of a motility disturbance that extends beyond the stomach. In the hospital setting, it is not uncommon for clinicians to expect daily bowel movements in all patients, when that

13
may not be their baseline. Some patients may have been using a prescribed (or non-prescribed) bowel regimen at home which was not continued after admission to the hospital. bulk-forming agents used to treat constipation may not empty well from the stomach; in those patients who have presented with a gastric bezoar it is especially important that they avoid a high fiber diet (1).
Specific Vitamin and Mineral IssuesAttention should be given to the monitoring of certain nutrients in patients with gastroparesis due to limited oral intake, or anatomical changes from surgery (partial gastrectomy, roux-en-Y, status post Whipple, etc.) (5). More common deficiencies include iron, and vitamins D and b-12. Measurement of serum folate is helpful in those with suspected dysmotility below the stomach, as it can be indicative (but not diagnostic) for small bowel bacterial overgrowth. bacteria synthesize folate in the GI tract, which is then absorbed resulting in above-normal folate levels.
Any patient who has experienced a considerable, unintentional weight loss at presentation is at risk for total nutrient deficiency. unfortunately, there are no large comparative trials evaluating vitamin and mineral status in the gastroparesis population. However, a recent survey of patients with gastroparesis demonstrated that intakes of many nutrients were suboptimal (6). Consider empirical treatment in suspected vitamin- or mineral-deprived patients, and provide a therapeutic vitamin or mineral supplement for two to four weeks. Following the treatment period, reevaluate the need for continued supplementation, instead of obtaining serum levels on all
nutrients due to the poor validity of many. A chewable or liquid supplement may be better tolerated than the tablet form in some patients.
Nutrition InterventionMany clinicians who work with patients with gastroparesis will advise the use of smaller, frequent meals and a restriction on fat and
fiber. This practice is widespread, yet no prospective, randomized controlled trials comparing dietary treatments in patients with gastroparesis exist. In those patients who are nutritionally compromised, restricting fat may set an unattainable expectation for the patient: to make up for the fat-calorie deficit by eating more food. It may be
Table 1. Summary of Oral Nutrition Intervention in the Patient with Gastroparesis
1) Decrease the volume of meals • Advise patients to eat smaller, more frequent meals.
2) Use more liquid calories • If symptoms increase over the course of the day, try solid food meals in the
morning, switching to more liquid meals late in the day. • If solid foods cause increased symptoms, try a liquid/pureed diet to enhance
gastric emptying. • Chew foods well. • Suggest that the patient sit up during and for 1 to 2 hours after meals.
3) Glucose control • If gastroparesis is a result of DM, achieve and maintain blood glucose control. • Monitor the need to change the timing of, or the overall requirements for
insulin in order to have consistent delivery of nutrients with optimal total calories ingested.
• Expect an increase in insulin requirements as improved symptom control will likely result in an increase in total calories ingested.
• In general, dietary restrictions (i.e., DM or heart-healthy diets) should be lifted until the patient is eating well again.
4) Medications • Prokinetics and antiemetics should be given in regular scheduled doses
(rather than “as-needed” doses) and may be best tolerated in liquid form. • If possible, avoid use of medications that affect gastric motility. • review and delete any “unnecessary” medications (may always be added
back later).
5) fat • Fat in liquids should be tolerated; implement intervention options No. 1 to 4
above before restricting.
6) fiber • Fiber can be fermented in a “slow” gut by bacteria potentially causing gas,
cramping and bloating, and can ultimately aggravate gastroparesis. • If bezoar formation is a concern, the patient should avoid high-fiber foods and
certain medications.
7) Treat bacterial overgrowth if suspected/symptomatic—see article on small bowel bacterial overgrowth in this issue.
8) Monitor and replace as needed: iron, vitamin B-12, vitamin D and calcium • If the patient is significantly malnourished, a daily standard vitamin/mineral
elixir can be used for one month or longer — or until stores are repleted. • If patient has gastric intolerance to iron, try smaller doses; some is better than
none. liquid iron may be a better choice in some patients. Consider giving iron in conjunction with vitamin C.
Adapted from: Parrish Cr, Yoshida C. Practical Gastroenterology. 2005;XXI(8):29.

14
the solid food that accompanies the fat that is the rate-limiting factor in these patients, due to loss of the grinding action of the stomach. High-calorie liquids (e.g., those with fat), are often well-tolerated. (This is drawn from the author’s personal experience).
Evidence to DateThus far, the only experimental trials in patients with gastroparesis include small diet-record surveys, or the assessment of GI symptoms; tolerance of a single meal, fluid, or particle size (mashed potatoes, oral glucose, mixed meals, addition of 300 ml water), with calories ranging from 120 to 580 (5). unfortunately, these observational studies are too small to make recommendations for this patient population. Additionally, they include such a heterogeneous group of patients (asymptomatic, symptomatic, long-standing DM, fasting vs. non-fasting, type 1 or type 2 diabetes, and mixed gastroparesis etiologies) that it is impossible to draw conclusions.
oral Diet Suggestions See Table 1 for a summary of diet interventions. Extensive dietary guidelines can be accessed at the university of Virginia Health System website: www.ginutrition.virginia.edu (see Table 2 for available diets).
Enteral vs. Parenteral NutritionSome patients will require nutritional support due to unrelenting, refractory gastroparesis. Enteral nutrition is safer, less expensive and less labor-intensive for patients and caregivers than parenteral nutrition. Experts in the field of motility, however, are not in agreement regarding the best access to use in these patients and little evidence exists for the best route. Enteral
access should be considered in those patients who:
• Fail to achieve nutritional goals• Experience unintentional weight
loss greater than 5% to 10% over 3 to 6 months
• Exhibit persistent vomiting and the potential need for gastric decompression, or repeated hospitalizations for diabetic ketoacidosis, hydration, nutrition or medication delivery
• Fail to thrive, and whose overall quality of life is at risk
For an in-depth discussion of enteral feeding in this patient population, see reference 1, (available online).
ConclusionCaring for patients with gastroparesis can be quite challenging. Chronic nausea and vomiting can not only precipitate dehydration, electrolyte disturbances, hyperglycemia, malnutrition, and inadequate medication delivery, but seriously impact overall quality of life. Early identification of patients who are at nutrition risk will help clinicians decide who might benefit from early nutrition support to replenish nutrition and hydration status. In the patient with DM, glycemic control is paramount, not only to decrease gastroparesis symptoms, but to allow full utilization of ingested nutrients. A multidisciplinary approach is necessary to address the medical, nutritional and pharmacological aspects of this debilitating complication
in order to maximize the quality of life for patients living with gastroparesis. Table 2 provides a list of resources for professionals and patients.
references 1. Parrish Cr, Yoshida C. Nutrition
Intervention for the patient with gastroparesis: an update. Practical Gastroenterolgy. 2005;XXIX(8):29.
2. American Diabetes Association. Diabetes Statistics. American Diabetes Association Web site. www.diabetes.org. Accessed March 4, 2011.
3. banh, l. Serum proteins as markers of nutrition: what are we treating? Practical Gastroenterology. 2006; XXX(10):46.
4. Chang J, rayner CK, Jones Kl, Horowitz M. Diabetic gastroparesis and its impact on glycemia. Endocrinol Metab Clin North Am. 2010;39(4):754-762.
5. Parrish Cr, McCray S. Gastroparesis and nutrition: the art. Practical Gastroenterology. 2011;XXXV(9):26.
6. Parkman HP, Yates KP, Hasler Wl, et al. Dietary Intake and nutritional deficiencies in patients with diabetic or idiopathic gastroparesis. Gastroenterology. 2011;141(2):486–498.
Table 2. Resources for Clinicians and Patients with Gastroparesis
university of Virginia Health System GI Nutrition Webpage www.ginutrition.virginia.edu
Nutrition articles in Practical Gastroenterology
GI Motility Websites• Gastroparesis and Dysmotilities Association – www.digestivedistress.com • American Motility Society – www.motilitysociety.org

15
AbstractDietary management of type 1 diabetes and celiac disease (CD) can be challenging and sometimes overwhelming for those who are newly diagnosed. Working closely with an experienced registered dietitian (rD) who is knowledgeable in both diabetes and CD can help patients manage both diseases. The rD provides patients with the education and information needed, including: carbohydrate-counting, label-reading, understanding the gluten-free diet and ensuring a diet that is nutritionally complete.
IntroductionThe prevalence of CD in type 1 diabetes (T1DM) is well-defined in the literature as an immune-mediated disease that occurs in 1% to 16% of individuals with T1DM and approximately 1% of the general population (1). It is also estimated that approximately 1% of persons with type 2 diabetes will have CD and could also be at risk for other autoimmune diseases. Therefore, they should be evaluated by an endocrinologist and screened for those diseases, if appropriate.
CD can be classified as a classic, silent or latent disease. Classic CD often presents with gastrointestinal (GI) symptoms such as gas, diarrhea, bloating, malabsorption and weight loss, although symptoms can be varied among individuals, and even missed when they have poorly
controlled diabetes or gastroparesis. Individuals with T1DM recently diagnosed with CD, or were not following a gluten-free (GF) diet may have only symptoms of erratic blood glucose (bG). These erratic bGs can be a result of malabsorption caused by damage to the intestine, which alters the rate of food absorption and makes it extremely difficult to manage bG with insulin.
Diagnosing Celiac DiseaseThe American Diabetes Association recommends screening for CD in adults based on signs and symptoms, but recommends that children be screened soon after the diagnosis of diabetes is made, with a plan to rescreen in the future if symptoms present (1). The most common serology tests used to screen for CD are tissue transglutaminase-IgA (tTG-IgA) or the endomysial antigliadin antibodies IgA (EMA-IgA) with a total IgA titer. It is recommended to check the IgA titer because approximately 2% to 10% of individuals with CD are deficient in IgA. If deficient in IgA, a false negative for the tTG-IgA will result, and will require measurement of tTG-IgG antibodies (2). CD can be triggered at any age, so it is especially important that individuals at high risk for CD be screened and rescreened if symptoms develop at a later date. rubio-Tapia et al. suggests that CD has increased four-fold in the past 50 years in the united States alone (3). In serology-
Celiac Disease and Diabetes Mellitus
laurie A. Higgins, MS, rD, lDN, CDECoordinator of Pediatric Nutrition Education & researchJoslin Clinicboston, MA
positive individuals, a referral should be made to a gastroenterologist for further evaluation and to confirm the diagnosis with a small bowel biopsy.
once the diagnosis has been confirmed, it is important that the individual follow up with the diabetes healthcare team and an rD who is experienced in both CD and diabetes mellitus (DM) management. Additionally, individuals may become overwhelmed with the diagnosis of a second chronic disease, and mental health support may be beneficial.
Managing Diabetes with Celiac DiseaseDiabetes is managed with a combination of oral agents, insulin (with varied dosing and number of injections) or insulin pumps, and flexible-to-consistent meal plans. Every patient’s diabetes self- management plan is designed with his or her diabetes healthcare team based on individual needs or capabilities. It is important to reinforce diabetes self-management skills.
The gluten-free (GF) foods will be different than the gluten-containing foods the individual might have eaten on a regular basis. These foods are made from a variety of refined flours and starches (arrowroot, corn starch, potato, rice and tapioca) that are much lower in fiber and protein. However, in recent years, more GF whole grain products are coming to the marketplace.

16
When transitioning to the GF diet, many of the old rules of thumb may not apply. For instance, a typical slice of whole grain bread contains 14 to 19 or more grams of carbohydrates, while a slice of GF bread can be 15 to 24 grams or more per slice. In addition to having more carbohydrates, many of the GF foods made from refined flours have higher glycemic indices (GI) and may raise bG levels more than gluten-containing whole grain products with lower GIs. If on insulin, a patient might benefit from taking their rapid insulin 15 to 20 minutes before they eat, and even earlier if their bG is out of target. Additionally, many GF products have added fat to enhance the texture and provide some moisture. The fat will add extra calories and decrease the rate of absorption of the food as compared to the non-GF counterparts.
The GF diet can be low in fiber. Encourage the person to choose whole grain GF diet flours and products, add fresh fruit to all meals, encourage 2 to 3 cups vegetables daily, as well as a serving of nuts, and adding ground flax seed to baked products. This will enable them to meet their fiber goals. See Table 1 for a sample menu.
To assist the diabetes team in managing the diabetes, it is helpful to have the patient keep a detailed log book with their bGs, insulin and/or medication doses, total carbohydrates for all meals and snacks, and physical activity. This will help to identify a pattern in the glucose readings and to guide appropriate recommendations for insulin and/or medication adjustments. If patients are still struggling with their bG control, many diabetes treatment centers have diagnostic continuous glucose monitoring (CGM) available. This is a glucose sensor that is placed under the skin and measures the glucose levels every 5 minutes for 3 to 5 days. blood glucose levels will continued to be monitored by finger stick two to
four times a day depending on the device used, as well as recording carbohydrates, insulin and physical activity. Information captured by the device is then downloaded and reviewed with the detailed log book for education and medication adjustments.
Transitioning to a Gluten-Free DietWhen transitioning to the GF diet, diabetes medications may have to be adjusted as the GI tract heals and absorption improves. Transitioning to the GF diet can be accomplished gradually over a few weeks, especially if the individual is overwhelmed, or has difficulty finding GF foods. An individual would benefit from a few visits with the rD to help with the transition. This usually involves starting with the present diabetes meal plan and modifying it to become GF. once the patient has a basic understanding of the GF diet, there can be more of a
focus on making changes or recommendations to improve the nutritional quality. Many GF foods are not fortified or enriched, and the GF diet can inherently lack b-vitamins, iron, calcium, vitamin D and fiber (4,5). Nutritional supplementation might also be warranted.
Addressing the basics with the patient and providing guidelines is the first step in transitioning to a GF diet. review the foods consumed on a typical day to identify simple substitutions and appropriate meal ideas. Exploring hidden sources of gluten and discussing portion sizes and carbohydrate content using real-life examples can make the transition seem a little less daunting. Consider all foods that can be included in the GF diet, such as fresh fruits and vegetables. Substitute wheat products for whole grain GF counterparts (Table 2), and include starchy vegetables at meals and snacks.
Table 1. Gluten Free Sample Menu
Breakfast Calories fiber (g)1 cup GF oatmeal 166 41 cup low-fat milk 120 01 tbsp ground flax seed 37 1.9raisins (0.5 oz small box) 42 0.5
Morning snackMedium apple (3” diameter) 95 4.4
lunch2 slices GF bread with fiber 180 43 oz turkey 83 01 tsp mustard 3 0lettuce leaf & 2 slices tomato 36 0.4Corn chips (1oz) 141 1.51 kiwi 42 2.11 cup low-fat milk 120 0
afternoon snack 1 serving lentil crackers (5) 110 11 cup vegetables sticks (carrots & celery) 13 1.1½ cup hummus 100 3.6
Dinner 1 cup cooked quinoa 205 41/3 cup tomato sauce 74 2.2½ cup broccoli 27 2.64 oz baked salmon 206 01½ cups salad (lettuce, tomato, carrots) 30 1.8balsamic vinaigrette (2 tbsp) 20 0.1
1850 35.2

17
Patients who are malabsorbing or experiencing difficulty with weight loss or erratic bG could gain weight once the GF diet is initiated and the GI tract begins to heal. Weight gain also increases insulin resistance. It is important to review portion sizes with the patient to make sure their average daily intake is within their estimated energy needs. Monitoring bG levels pre- and post-meals and/or snacks will help the diabetes team make appropriate adjustments to the diabetes medications. Additionally, other oral non-diabetes medications may need to be adjusted as absorption improves.
If the GI symptoms persist or recur, the patient should follow up with the rD to identify any hidden gluten or possible cross-contamination of foods in the diet. Cross-contamination sources in the home can include toasters, condiments, countertops, sponges and colanders. For example, oats are inherently GF, but were excluded from the GF diet for years. A study by Thompson (6) suggested that many of the oats commercially available in the united States were actually contaminated with gluten. Most of the GF communities have incorrectly assumed that many inherently GF products are GF. Thompson et al. analyzed a variety of inherently GF grains for gluten
content. Thirty-two percent of the convenience samples were above the Food and Drug Administration’s proposed level of 20 ppm of gluten (7). An individual experiencing persistent symptoms should purchase products exclusively from a company that voluntarily analyzes their products to ensure that they are GF. See Table 3 for resources.
ConclusionManagement of CD with diabetes can be very overwhelming and daunting. The comprehensive plan for managing both diseases should be individualized and based on the patient’s needs and abilities. Working together with the patient and his/her diabetes team is essential to provide a consistent message. When making adjustments to meal planning while coordinating diabetes management based on self-monitoring of blood glucose, frequent follow-up, physical activity and medications are essential. This is particularly important in the early stages after the diagnosis of CD in patients with DM.
references 1. American Diabetes Association.
Standards of medical care in diabetes — 2011. Diabetes Care. 2011;34 Suppl 1:S11–S61.
2. NIH Consens State Sci Statements. NIH Consensus Development Conference on Celiac Disease. 2004;21(1):1-23.
3. rubio-Tapia A, Kyle rA, Kaplan El, et al. Increased prevalence and mortality in undiagnosed celiac disease. Gastroenterology. 2009;137(1):88–93.
4. Thompson T, Dennis M, Higgins lA, lee Ar, Sharrett MK. Gluten-free diet survey: are Americans with coeliac disease consuming recommended amounts of fibre, iron, calcium and grain foods? J Hum Nutr. Diet 2005;18(3): 163–169.
5. Kupper C. Dietary guidelines and implementation for celiac disease. Gastroenterology. 2005; 128(4 Suppl 1):S121–S127.
6. Thompson T. Gluten contamination of commercial oat products in the united States. N Engl J Med. 2004; 351(19):2021–2022.
7. Thompson T, lee Ar, Grace T. Gluten contamination of grains, seeds, and flours in the united States: a pilot study. J Am Diet Assoc. 2010;110(6):937–940.
8. Kupper C, Higgins lA. Combining diabetes and gluten-free dietary management guidelines. Practical Gastroenterology. 2007;31:68–83.
Amaranth bean floursbuckwheatCornMilletMontina® (Indian rice grass)Nut flours (almond, peanut, brazilian, etc.)oats (certified gluten free)Quinoarice (brown, wild)SorghumSoyTeff
Table 2. Gluten-Free Whole Grains
Table 3. Celiac Resources for the Professional
Organizations• Dietitians in Gluten Intolerance Disease (DGID) A dietetic practice group (DPG) subunit of the Medical Nutrition Practice Group
DPG of the Academy of Nutrition and Dietetics. www.eatright.org• Gluten Intolerance Group – http://www.gluten.net • Celiac Disease foundation – www.celiac.org • Canadian Celiac association – www.celiac.ca • Celiac Diet series at UVahs: www.ginutrition.virginia.edu• The Gluten-free Dietitian – http://www.glutenfreedietitian.com
Books • Case S. Gluten-Free Diet: A Comprehensive Resource Guide – Expanded and Revised
Edition. Case Consulting Inc., 2010. http://www.glutenfreediet.ca. • Dennis M, leffler D. Real Life with Celiac Disease: Troubleshooting and Thriving
Gluten Free. bethesda, MD: AGA Press; 2010.• blumer I, Crowe S. Celiac for Dummies. Hoboken, NJ: Wiley Publishing Inc.; 2010 • Thompson T, brown M. American Dietetic Association Easy Gluten-Free. Hoboken,
NJ: John Wiley & Sons, Inc.; 2010.
Kupper C, Higgins lA. Practical Gastroenterology. 2007;31:68-83.

18
AbstractSmall bowel bacterial overgrowth may complicate the course of diabetes, and result in a variety of gastrointestinal symptoms. Disturbances in gastrointestinal motility and gastric acid secretion are the principal predisposing factors. Although simple, noninvasive breath tests are commonly used to diagnose small bowel bacterial overgrowth, the gold standard test remains the culture of a small intestinal aspirate, which can be collected during routine endoscopy. Treatment is aimed at reducing intestinal microbial density, generally with a broad-spectrum oral antibiotic; and correction of associated nutritional deficiencies when present.
IntroductionSmall bowel bacterial overgrowth (Sbbo) commonly complicates the course of the patient with diabetes. Sbbo is characterized by a variety of signs and symptoms that result primarily from competition between the atypical and excessive bacteria present in the proximal small bowel and the human host for ingested nutrients. Injury to the intestinal epithelium caused by these bacteria may also contribute. Sbbo implies a quantitative assessment of bacteria present in the small intestine (SI) and is classically defined as the presence of greater than 105 colony forming units/ml of bacteria in the proximal
SI; however, it is unclear whether the pathologic consequences of Sbbo are due to an increased overall number of bacteria, the type of bacteria or a combination of both. Herein, the clinical features, nutritional complications and factors predisposing the patient with diabetes to Sbbo are described, as are its diagnosis and treatment.
Clinical Features and Nutritional ConsequencesTraditionally, Sbbo has been considered in the context of a malabsorptive syndrome; however, Sbbo may be asymptomatic or manifest with generally non-specific symptoms. Not infrequently, symptoms of Sbbo are incorrectly ascribed to the underlying disease which predisposes to Sbbo. The spectrum of severity of Sbbo symptoms varies considerably. The negative effects of Sbbo on nutrient digestion and absorption are largely responsible for the clinical features that occur. Symptoms of disturbed gastrointestinal motility may also occur in Sbbo as a consequence of alterations in gut peptide secretion due to differences in nutrient presentation to the respective segments of the gut.
Fat maldigestion and malabsorption occur mainly due to the deconjugation of bile acids by intraluminal bacteria,
Small bowel bacterial overgrowth in Diabetes Mellitus
John K. Dibaise, MDProfessor of MedicineDivision of GastroenterologyMayo ClinicScottsdale, AZ
allowing their absorption by the jejunum and leading to insufficient concentrations for micelle formation and fat absorption. Fat malabsorption may lead to steatorrhea, oxalate kidney stones, and fat-soluble vitamin deficiencies with their associated symptoms. bacterial deconjugation may also result in the production of substances, such as lithocholic acid, which may exert toxic effects on the intestinal epithelium and result in impaired absorption of fat, carbohydrate and protein. Furthermore, secretory diarrhea may occur because of the presence of hydroxylated fatty acids and deconjugated bile acids due to the caustic nature of these substances on the intestinal mucosa. because of the fat maldigestion and malabsorption that occurs in the setting of Sbbo, deficiencies of the fat-soluble vitamins A, D and E can occur. Vitamin K deficiency is rarely seen in Sbbo due to the ability of some gut microbes to synthesize this micronutrient. Carbohydrate malabsorption may also result from the intraluminal degradation of sugars by enteric bacteria and from bacteria-related decreases in enterocyte disaccharidase and brush-border hydrolase activity and impaired monosaccharide absorption. Importantly, while carbohydrate malabsorption often results in gas-related symptoms and sometimes, diarrhea, it rarely results

19
in clinically significant effects on postprandial blood glucose levels. Protein malnutrition is rare in Sbbo. Vitamin b-12 deficiency is caused by bacterial consumption involving predominantly anaerobic organisms within the intestinal lumen before it can be absorbed. Vitamin b-12 malabsorption may result in megaloblastic anemia and neurological symptoms related to degeneration of the dorsal and lateral white matter of the spinal cord. Deficiencies of thiamine and nicotinamide have also been reported. In contrast, folate levels may be elevated in Sbbo as a result of bacterial synthesis and its subsequent absorption providing a clue to the possible presence of Sbbo.
Factors Protecting Against the Development of SbboThe most important factors preventing excessive small bowel colonization are normal small bowel motility, which prevents attachment of ingested organisms; and gastric acid, which destroys many organisms before they reach the SI. Further enzymatic digestion by pancreaticobiliary secretions and the presence of adequate mucosal immunity including immunoglobulins within the intestinal secretions also help to control the bacterial populations in the small bowel. The intestinal mucus contributes by trapping bacteria intraluminally (1).
risk Factors for Developing Sbbo in DiabetesTaking the above into consideration, conditions that are associated with the presence of Sbbo can be divided primarily into those where stasis/stagnation occurs within the SI and those where diminished gastric acid secretion is present. In many chronic
conditions such as diabetes, a multifactorial cause may be present. Eradication of Sbbo has been demonstrated to normalize orocecal transit in persons with diabetes (2). using antisecretory (e.g., proton pump inhibitors and somatostatin analogs) and/or antimotility/antidiarrheal (e.g., loperamide, diphenoxylate and opioid analgesics) medications may further predispose some persons with diabetes to develop excess bacterial colonization of the SI.
Prevalence of Sbbo in DiabetesGastrointestinal (GI) symptoms occur commonly in both type 1 and type 2 diabetes and seem to be associated with the presence of diabetes complications and duration of disease (3,4). Early satiety, nausea, vomiting, weight loss, constipation, diarrhea and epigastric pain are often reported and may result from Sbbo. The prevalence of Sbbo in diabetes is poorly understood, but clearly varies depending upon a variety of clinical factors and the method used to diagnose the condition. using hydrogen breath testing as the diagnostic method, the prevalence has ranged from 28% to 60% (2,5,6). Sbbo occurs more commonly in persons with diabetes who have chronic diarrhea (5) and gastroparetic symptoms (6), which underscores the need to address both clinical issues when determining the optimal management strategy for these challenging patients.
Disorders Associated with Diabetes that May Predispose to SbboDiabetes is associated with a number of conditions such as celiac disease; chronic kidney disease — end-stage renal disease in particular; and acute and chronic pancreatic diseases. Poor
or absent response to a gluten-free diet may be seen in up to 30% of patients with celiac disease. A limited number of conditions including Sbbo seem to be responsible (7). In this scenario, Sbbo may be differentiated from other potential causes by its association with the presence of diarrhea and abdominal pain. Although the mechanism is unclear, intestinal dysmotility is suspected. GI symptoms are common in patients with chronic renal failure. Sbbo also appears to be common in those with chronic kidney disease, particularly those who require dialysis (8). Hemodialysis has been shown to improve gastric motility; however, a reduction in Sbbo has yet to be demonstrated (9). Finally, Sbbo may complicate the course of both acute and chronic pancreatitis and may be particularly prevalent, with reports of up to 40% in those with associated pancreatic exocrine insufficiency (10-12). The mechanism is likely multifactorial including disease-related and treatment-related (e.g., opioid analgesics) intestinal dysmotility, hypochlorhydria and alterations in pancreaticobiliary secretions.
DiagnosisThe culture of aspirated small bowel fluid remains the “gold standard” in the diagnosis of Sbbo upon, which other methods are compared (13,14). This is despite its limitations, including invasiveness, expense, potential for not detecting Sbbo occurring in the more distal SI, and inability to culture the majority of enteric microbes.
A small bowel aspirate can be readily obtained during endoscopy by passing a sterile aspiration catheter through the endoscope. Nevertheless, because of the limitations noted above, indirect methods of detecting Sbbo have been advocated and, in

20
clinical practice, appear to be more commonly used. Hydrogen breath testing is the most commonly used alternative method to diagnose Sbbo in clinical practice, and is based on the fact that gut microbes are the sole source of hydrogen in the gut. Hydrogen breath testing utilizes an orally ingested carbohydrate (e.g., glucose or lactulose, most commonly) as a substrate that — in the presence of excessive bacteria in the small bowel — is metabolized. Hydrogen is thereby released, subsequently absorbed and finally released into expired air. A rise in hydrogen (usually greater than 20 parts per million), generally within 90 minutes, in the breath sample after the oral administration of the substrate indicates Sbbo. While inexpensive and simple to perform, several factors may influence the results of this test including diet, exercise, tobacco smoking, recent use of antibiotics and rapid orocecal transit. The diagnostic criteria used may also lead to wide variations in sensitivity and specificity, and disappointing reliability for prediction of results of small bowel culture (13,15). The hydrogen breath test is also limited by the fact that up to a quarter of the population produces little or no hydrogen, a limitation that may be partly overcome by the simultaneous measurement of expired methane. because of the limitations of the diagnostic tests for Sbbo, it appears to be common clinical practice to provide empiric antibiotic treatment for individuals suspected of having Sbbo. However, caution is advised when using the response to an empirical antibiotic therapy as a means of “diagnosing” Sbbo, as the response may be difficult to interpret. Consequently, the diagnosis of Sbbo can set in motion a process of frequent antibiotic use and the performance of numerous tests if
symptoms do not respond or if symptoms return.
Treatmentonce pathologic Sbbo has been identified in a person with diabetes, whenever possible, the underlying anatomic or functional disturbance should be corrected. A reassessment of the need for continued use of antimotility and antisecretory medications, when applicable, should be undertaken. using prokinetic agents in the setting of gastro-intestinal dysmotility should be initiated; however, little evidence exists to support their long-term efficacy in humans (16,17). Medical nutrition therapy remains an important part of the management of Sbbo. The initiation of a lactose-restricted diet may result in a decrease in the development of gas-related symptoms and osmotic diarrhea in some individuals. Fat restriction may be useful to reduce steatorrhea, but is uncommonly needed in the absence of a coexisting cause of fat malabsorption. The correction of micronutrient deficiencies may also be necessary. In this regard, the periodic monitoring of micronutrient levels (e.g., fat-soluble vitamins, iron and vitamin b-12 in particular) in Sbbo patients
should be considered. In the rare patient who has experienced significant weight loss and has had difficulty regaining, supplemental nutrition support may prove beneficial.
The primary goal when treating Sbbo is to reduce the numbers of microbes present. As the culture of small intestinal contents will not necessarily identify the specific microbe(s) responsible, a trial-and-error approach to antibiotic therapy is often used with success being judged on improvement symptoms. Given the diversity of organisms present in Sbbo, broad-spectrum antimicrobial therapy is advised (Table). little objective evidence exists to favor one agent over another. In one of the few randomized, controlled trials of antibiotic therapy in Sbbo, both amoxicillin-clavulanate and norfloxacin were shown to provide a modest reduction in stool frequency and lead to improvements in hydrogen breath testing (18). In the person with diabetes, both amoxicillin-clavulanate and the poorly absorbed antibiotic, rifaximin, have been shown to both normalize the results of hydrogen breath testing and improve symptoms (2,5).
agent Dose
Amoxicillin-clavulanate 500 mg Po 3 times/day
Cephalexin 250 mg Po 2 times/day
Ciprofloxacin 500 mg Po 2 times/day
Doxycycline 100 mg Po 2 times/day
Metronidazole 250 mg Po 3 times/day
Neomycin 500 mg Po 2 times/day
Norfloxacin 400 mg Po 2 times/day
rifaximin 550 mg Po 3 times/day
Trimethoprim-sulfamethoxazole 1 double-strength tablet Po 2 times/day
Table. Examples of Antibiotic Options to Treat SBBO
Po = per os (by mouth) Adapted from: Attar A et al. Gastroenterology. 1999;117:794-797.
21
A single 7 to14-day course of therapy will usually lead to an improvement in symptoms. However, the duration of symptom improvement is highly variable. because the underlying mechanism(s) responsible for causing Sbbo are unlikely to change in the person with diabetes, periodic (e.g., 7 to 14 days per month) use may be necessary. In this circumstance, rotation of three or four different antibiotics is advised to reduce the risk of antibiotic resistance.
There is increasing interest in the use of probiotics in the management of Sbbo. This is due to the concern over the development of antimicrobial resistance, antibiotic-associated allergic reactions, Clostridium difficile diarrhea and the expense associated with prolonged use of antibiotics. At present, only anecdotal reports have suggested efficacy of probiotics in the management of Sbbo and further study of their use in this condition is needed.
ConclusionIn summary, Sbbo is characterized by a variety of clinical features and commonly complicates the course of treatment in the person with diabetes. Although the optimal diagnostic approach remains uncertain, available testing combined with clinical suspicion rather than empirical treatment is recommended. Finally, while antibiotics continue to be the mainstay of Sbbo treatment, attention to medical nutrition therapy is an important part of the management.
references 1. Collins MD, Gibson Gr. Probiotics,
prebiotics, and synbiotics: approaches for modulating the microbial ecology of the gut. Am J Clin Nutr 1999;69:1052S–1057S.
2. Cuoco l, Montalto M, Jorizzo rA, et al. Eradication of small intestinal bacterial overgrowth and oro-cecal transit in diabetics. Hepato-Gastroenterology. 2002;49:1582–1586.
3. oh JH, Choi MG, Kang MI, et al. The prevalence of gastro-intestinal symptoms in patients with non-insulin dependent diabetes mellitus. Korean J Intern Med. 2009;24:309–317.
4. Maleki D, locke Gr 3rd, Camilleri M, et al. Gastrointestinal tract symptoms among persons with diabetes mellitus in the community. Arch Intern Med. 2000;160:2808–2816.
5. Virally-Monod M, Tielmans D, Kevorkian JP, et al. Chronic diarrhea and diabetes mellitus: prevalence of small intestinal bacterial overgrowth. Diabetes Metab. 1998;24:530-536.
6. reddymasu SC, McCallum rW. Small intestinal bacterial overgrowth in gastroparesis: are there any predictors? J Clin Gastroenterol. 2010;44:e8–e13.
7. leffler DA, Dennis M, Hyett b, Kelly E, Schuppan D, Kelly CP. Etiologies and predictors in nonresponsive celiac disease. Clin Gastroenterol Hepatol. 2007;5:445–450.
8. Strid H, Simren M, Stotzer Po, ringstrorm G, Abrahamsson H, bjornsson ES. Patients with chronic renal failure have abnormal small intestinal motility and a high prevalence of small intestinal bacterial overgrowth. Digestion. 2003;67:129–137.
9. Adachi H, Kamiya T, Hirako M, et al. Improvement of gastric motility by hemodialysis in patients with chronic renal failure. J Smooth Muscle Res. 2007;43:179–189.
10. Trespi E, Ferrieri A. Intestinal bacterial overgrowth during chronic pancreatitis. Curr Med Res Opin. 1999;15:47–52.
11. Van Felius ID, Akkermans lM, bosscha K, et al. Interdigestive small bowel motility and duodenal bacterial overgrowth in experimental acute pancreatitis. Neurogastroenterol Motil. 2003;15:267–276.
12. Casellas F, Guarner l, Vaquero E, Antolin M, de Gracia X, Malagelada r. Hydrogen breath test with glucose in exocrine pancreatic insufficiency. Pancreas. 1998; 16:481–486.
13. Corazza Gr, Menozzi MG, Strocchi A, et al. The diagnosis of small bowel bacterial overgrowth. reliability of jejunal culture and inadequacy of breath hydrogen testing. Gastroenterology. 1990;98:302–309.
14. riordan SM, McIver CJ, Walker bM, Duncombe VM, bolin TD, Thomas MC. The lactulose breath hydrogen test and small intestinal bacterial overgrowth. Am J Gastroenterol. 1996;91: 1795–1803.
15. Abu-Shanab A, Quigley EM. Diagnosis of small intestinal bacterial overgrowth: the challenges persist! Expert Rev Gastroenterol Hepatol. 2009;3: 77–87.
16. Pardo A, baroli r, lorenzo-Zuniga V, et al. Effect of cisapride on intestinal bacterial overgrowth and bacterial translocation in cirrhosis. Hepatology. 2000; 31:858–863.
17. Soudah HC, Hasler Wl, owyang C. Effect of octreotide on intestinal motility and bacterial overgrowth in scleroderma. N Engl J Med. 1991;325:1461–1467.
18. Attar A, Flourie b, rambaud JC, Franchisseur C, ruszniewski P, bouhnik Y. Antibiotic efficacy in small intestinal bacterial overgrowth-related chronic diarrhea: a crossover, randomized trial. Gastroenterology. 1999;117:794–797.

22
Abstract Constipation affects many patients with longstanding diabetes, and is a common gastrointestinal complaint in this population. Persons living with diabetes may have any of the causes of constipation found in the general population, but are particularly likely to have medications, dietary changes, and neuropathy as etiologic factors. The treatment for constipation mirrors what is provided to persons without diabetes and usually can provide effective relief of this condition.
Definition and Pathophysiology Constipation means different things to different people. For most physicians and some patients, it is synonymous with infrequent defecation (fewer than three bowel movements per week). For most patients, constipation encompasses a broader spectrum of symptoms, centering on difficulty with the process of defecation (Table 1) (1,2). This variation in definition makes it imperative that caregivers understand exactly what the patient means by the term, “constipation.”
Constipation is due to altered physiology in the colon (3). In healthy people, each day approximately 1 to 1.5 liters of fluid is delivered to the colon. This represents the residue remaining from roughly 9 to 10 liters of ingested material and digestive secretions that daily enter the small
intestine. by the time the intestinal contents reach the colon they include water, salt and undigested solids, mainly composed of fiber that is consumed but undigested. Movement of this material through the colon is slow, taking roughly 24 hours to reach the rectum. During this time, the lining of the colon absorbs most of the water and salt, and the bacteria in the colon ferments the fiber into short-chain fatty acids and gas, some of which can be absorbed. only about 100 ml — or 1% — of the volume that enters the small intestine proceeds to the rectum. This volume is the average amount that triggers an urge to defecate, thus the average person consuming a typical diet has about one bowel movement per day. Frequency and amount of bowel movements are sensitive to diet
Constipation in Patients with Diabetes Mellitus
lawrence r. Schiller, MDDigestive Health Associates of TexasProgram Director, Gastroenterology Fellowshipbaylor university Medical CenterDallas, TX
composition and personality factors (4). Slower transit through the colon allows more time for mucosal absorption and bacterial fermentation to occur, thus less material gets to the rectum and it takes longer to collect enough material in the rectum to stimulate defecation. Infrequency of defecation is the cardinal symptom of slow-transit constipation, and stools are typically small, compact and pebble-like.
Constipation can also be caused by difficulty with the defecation process (5). These patients usually have problems removing those barriers to defecation which ordinarily preserve continence. The rectum can be envisioned as a reservoir that is capable of accommodating the storage of 100-200 ml of stool. In infants, stool entering the rectum from the sigmoid colon is propelled rapidly through the anus in an automatic process that involves reflex relaxation of the internal anal sphincter when the rectum is distended. In adults, internal anal sphincter relaxation still occurs when stool enters the rectum. However, learned contraction of the external anal sphincter and pelvic floor prevent defecation, while the rectum relaxes to accommodate the increase in volume if defecation is not appropriate at that time. When appropriate, relaxing the external anal sphincter and pelvic floor allows increased abdominal and intrarectal
Straining
Hard stools, knobby stool form
Incomplete evacuation
Abdominal bloating
Inability to evacuate
Need for manual assistance with defecation
Infrequency of defecation (<3 bowel movements per week)
Abdominal discomfort
Table 1. Symptoms of Constipation
Adapted from: Paré P et al. Am J Gastroenterol. 2001;96:3130–3137.

23
pressure to eject stool into and out from the anal canal. This process can be perverted in a number of ways producing outlet-obstruction constipation (Table 2).
Diabetes may produce several changes that may make persons with diabetes more likely to develop constipation than persons without diabetes (6,7). Hyperglycemia (blood glucose greater than 200 mg/dl) by itself affects smooth muscle function and motility, but this has been better demonstrated in the upper gastrointestinal tract than in the colon (8). The enteric nervous system of the colon may be disturbed by loss of inhibitory nerves and the interstitial cells of Cajal due to oxidative stress and inflammation (9,10). This might slow transit as motility becomes more inefficient. Disturbances in the enteroendocrine system have also been described in diabetes (11).
outlet-obstruction constipation in persons living with diabetes may be related more to the presence of neuropathy that affects the skeletal muscle of the pelvic floor and the external anal sphincter than to direct effects on skeletal muscle (7). Neuropathy also may inhibit sensation from the rectum, thus
weakening the “call to stool” ordinarily experienced as stool enters the rectum (5).
Evaluation and Fiber Supplementation Patients with constipation can often be managed initially without an extensive diagnostic evaluation (1). only those with warning symptoms or signs (so called “red flags”) need a more thorough evaluation (Table 3).
It is important to understand what the patient means by constipation (Table 1) in order to recommend effective therapy. A detailed history of symptoms, including onset, variation over time, and previous evaluation and therapy, should be obtained. Most patients will have
tried some dietary manipulations and these should be investigated in as much detail as possible. A recollection of trying “more fiber” is not as valuable; quantify an estimate of how much and what kind of fiber was actually consumed. Associated symptoms, such as bloating, distention, nausea and abdominal pain, should be identified. These may be as important or more important to the patient than the actual alteration of bowel habit.
While medical nutrition therapy (MNT) remains the foundation of diabetes management for persons with diabetes who suffer from constipation, it is particularly
complex. In some patients MNT alone can control blood glucose adequately. However, in most, it facilitates medical management by limiting blood glucose excursions, thereby making medications such as oral hypoglycemics or insulin more effective. Since many persons with diabetes are overweight, diets also must be designed to facilitate weight loss. Finally, diets have direct impact on bowel habits and associated symptoms, and therapeutic diets for persons with diabetes with constipation need to address those issues as well.
Insufficient fiber intake has been postulated as a cause for constipation and supplementation of fiber as a cure for over 120 years (12).
Fiber is defined as plant wall constituents that resist digestion in the human small intestine (13). Cellulose, hemicellulose, pectins, fructooligosaccharides, and resistant starches are the major carbohydrate components. lignin is the main non-carbohydrate constituent of fiber. Fiber experts distinguish “soluble” and “insoluble” fiber, which have different abilities to form gels and be fermented, but this has not been distinguished in most epidemiological studies. Each food contains a different spectrum of substances categorized as “fiber,” in addition to any differences in the total amount of fiber present. Thus, fiber sources are not necessarily
Paradoxical puborectalis muscle contraction (dyssynergia)
Perineal descent
Intrarectal intussusception
Anterior wall rectal ulcer syndrome
rectal prolapse
Sigmoidocele
Anal stenosis
Painful anorectal disorders
Table 2. Causes of Outlet — Obstruction Constipation
Adapted from: rao SS. Clin Gastroenterol Hepatol. 2010;8:910–919.
onset of symptoms in patients more than 50 years of age
Incomplete response to therapy for constipation
Gastrointestinal bleeding (blood in stools, iron-deficiency anemia)
unintentional weight loss
Personal or family history of structural gastrointestinal disease
Table 3. Red Flags That Signal Prompt and Thorough Evaluation
Adapted from: lembo A & Camilleri M. N Engl J Med. 2003;349(14):1360–1368.

24
interchangeable in terms of potential biological effects. The polymers that constitute dietary fiber in the stool solids complex are about four to five times their weight of water and thus are a major determinant of stool weight and consistency (14). In addition, the fermentation of fiber in the colon produces many smaller molecules that can exert osmotic activity, enhancing water retention intraluminally and perhaps stimulating motility in the colon (12). Short-term increases in fiber intake are associated with increased stool output in normal subjects. Stool frequency and weight could be altered by a factor of two by variations in diet (4). Another study suggested that wheat bran is most effective at increasing stool weight, followed by fruits and vegetables, oats, corn and soya (15). Mucilages, cellulose and pectin were less effective than wheat bran. Studies such as this clearly show that fiber intake can drive stool output in normal individuals.
There is less evidence that dietary fiber intake can alter stool output in patients with constipation (16). While some studies have suggested that dietary fiber is beneficial (17,18), more recent work has emphasized the ineffectiveness of dietary fiber in most patients with constipation (19). Nevertheless, some patients may respond to fiber supplementation; and most patients with constipation should be tried on fiber before pursuing advanced diagnostic testing or other therapies (1). Fiber is most likely to be helpful in patients with relatively normal colonic transit and those who might benefit from production of softer stools. It is unlikely to help those who have severe colonic inertia; in that
circumstance it would only result in more material to transport through the colon. Patients who have evacuation problems due to pelvic floor disorders also may not benefit from fiber supplementation; it may only result in bulkier stools to evacuate with straining.
To use fiber successfully, one must first assess dietary fiber intake before making recommendations for fiber supplementation. If a patient is already taking 25 to 30 g of dietary fiber daily, further supplementation is unlikely to be helpful (1). If less than this amount is being consumed, fiber should be added slowly in graduated doses to eventually reach 25 to 30 g per day. If the entire supplemental amount is added at once, it is likely that the patient will develop intolerable side effects, such as bloating or excessive flatus. There is no clear consensus as to the ideal dietary fiber supplement for patients with constipation — let alone patients with constipation living with diabetes. While studies in normal individuals would favor wheat bran, there appears to be little clinical difference when different products are used in patients — even those that performed poorly in studies in normal subjects seem to be effective in some patients.
Fiber should not be viewed as a cure-all for constipation, and there may be downsides to an arbitrary increase in dietary fiber. The fermentation of fiber can produce large amounts of hydrogen or methane gas. It has been estimated that fermentation of 10 g of carbohydrate by colonic bacteria can yield one liter of gas (20). This may aggravate bloating or distention in addition to increasing flatus.
Persons with diabetes may have other sources of fermentable carbohydrates and sugar alcohols in their diets. Fructose and sugar alcohols (such as sorbitol) may be used preferentially by persons with diabetes as sweeteners to reduce glucose consumption. These substances are incompletely absorbed in the small intestine and can be fermented by the bacteria in the colon. These and other poorly absorbed substances may aggravate bloating and distention in many patients. The so-called “FoDMAP™ (Fermentable oligo-, Di-, and Mono-saccharides and Polyols) diet” reduces foods that are rich in poorly absorbed carbohydrates and may mitigate gas-induced symptoms (21).
Conclusion Constipation is a common problem in the general population, but especially in patients with diabetes, probably because of the effects of hyperglycemia and neuropathy over time. Additionally, drugs and dietary changes affect the frequency of constipation in those with diabetes. Clinical management first and foremost depends on understanding what the patient means by “constipation.” Increasing fiber intake is the simplest means to improve constipation symptoms and should be the first therapeutic step in most patients. Should this approach fail, or symptoms worsen, further evaluation and management is warranted.
25
references 1. brandt lJ, Prather CM, Quigley
EM, Schiller lr, Schoenfield P, Talley NJ. Systematic review on the management of chronic constipation in North America. Am J Gastroenterol. 2005; 100(Supple 1):S5–S21.
2. longstreth GF, Grant Thompson W, Chey WD, Houghton lA, Mearin F, Spiller rD. Functional bowel disorders. Gastroenterology. 2006;130:1480–1491.
3. Dinning PG, Smith TK, Scott SM. Pathophysiology of colonic causes of constipation. Neurogastroenterol Motil. 2009;21 (Suppl 2):20–30.
4. Tucker DM, Sandstead HH, logan GM Jr, et al. Dietary fiber and personality factors as determinants of stool output. Gastroenterology. 1981;81:879–883.
5. rao SS. Advances in diagnostic assessment of fecal incontinence and dyssynergic defecation. Clin Gastroenterol Hepatol. 2010;8:910–919.
6. bytzer P, Talley NJ, leemon M, Young lJ, Jones MP, Horowitz M. Prevalence of gastrointestinal symptoms associated with diabetes mellitus: a population-based survey of 15,000 adults. Arch Intern Med. 2001;161: 1989–1996.
7. Sellin JH, Chang Eb. Therapy insight: gastrointestinal complications of diabetes — pathophysiology and management. Nat Clin Pract Gastroenterol Hepatol. 2008;5:162–171.
8. Abid S, rizvi A, Jahan F, et al. Poor glycaemic control is the major factor associated with increased frequency of gastrointestinal symptoms in patients with diabetes mellitus. J Pak Med Assoc. 2007;57:345–349.
9. He Cl, Soffer EE, Ferris CD, Walsh rM, Szurszewski Jh, Farrugia G. loss of interstitial cells of Cajal and inhibitory innervation in insulin-dependent diabetes. Gastroenterology. 2001;121: 427–434.
10. Chandrasekharan b, Anitha M, blatt r, et al. Colonic motor dysfunction in human diabetes is associated with enteric neuronal loss and increased oxidative stress. Neurogastroenterol Motil. 2011;23:131–138.
11. el-Salhy M. The possible role of the gut neuroendocrine system in diabetes gastroenteropathy. Histol Histopathol. 2002;17: 1153–1161.
12. Cummings JH. Dietary fibre. Gut. 1973;14:69–81.
13. Spiller rC. Pharmacology of dietary fibre. Pharmacol Ther. 1994;62:407–427.
14. Wenzl HH, Fine KD, Schiller lr, Fordstran JS. Determinants of decreased fecal consistency in patients with diarrhea. Gastroenterology. 1995;108:1729–1738.
15. Jenkins DJA, Peterson rD, Thorne MJ, Ferguson PW. Wheat fiber and laxation: dose response an equilibration time. Am J Gastroenterol. 1987;82:1259–1263.
16. Muller-lissner SA, Kamm MA, Scarpignato C, Wald A. Myths and misconceptions about chronic constipation. Am J Gastroenterol. 2005;100:232–242.
17. Graham DY, Moser SE, Estes MK. The effect of bran on bowel function in constipation. Am J Gastroenterol. 1982;77:599–603.
18. badiali D, Corazziari E, Habib FI, et al. Effect of wheat bran in treatment of chronic nonorganic constipation: a double-blind controlled trial. Dig Dis Sci. 1995;40:349–356.
19. Voderholzer WA, Schatke W, Muhldorfer bE, Klauser AG, birkner b, Miller-lissner SA. Clinical response to dietary fiber treatment of chronic constipation. Am J Gastroenterol. 1997;92:95–98.
20. Hammer HF, Fine KD, Santa Ana CA, Porter Jl, Schiller lr, Fordtran JS. Carbohydrate malabsorption: its measurement and its contribution to diarrhea. J Clin Invest. 1990;86:1936–1944.
21. Gibson Pr, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: the FoDMAP approach. J Gastroenterol Hepatol. 2010; 25:252–258.

26
Abstract Narcotic bowel syndrome (NbS), a type of bowel dysfunction, is a serious problem that affects patients with chronic pain requiring narcotics, including neuropathic pain related to diabetes. The syndrome causes numerous gastrointestinal symptoms that may impair nutritional status. NbS is complex to treat, and is often overlooked. This article discusses the impact of NbS on overall nutritional status and glycemic control, and offers practical strategies for clinicians.
IntroductionDiabetic neuropathy is a common complication of diabetes. Population studies of patients with diabetes estimate the incidence of neuropathy at over 30% to 50% (1,2) and the incidence of pain associated with neuropathies at 20%. This type of pain is thought to be caused by injury to small and large sensory fibers. Improved glycemic control reduces pain intensity and is a primary treatment for neuropathic pain (3). However, many patients require a combination of therapies to achieve adequate pain control. Despite a variety of pain medications available, only 40% to 60% of patients with neuropathic pain experience even partial relief, making management a complex clinical issue (4).
First-line drug therapy for neuropathic pain includes tricyclic
antidepressants, gabapentinoids (e.g., Gabapentin, pregabalin), selective noradrenergic reuptake inhibitors (e.g., Duloxetine, venlafaxine), and topical lidocaine. Patients with refractory pain will often benefit from adjunctive therapies such as opioids (e.g., oxycodone, codeine, fentanyl, morphine, tramadol) (5).
NbS is characterized by chronic or recurrent abdominal pain that worsens as the analgesic effects of opioids wear off. The incidence of NbS in patients with diabetes is unknown, but is thought to be significant. Chronic narcotic use often results in tachyphylaxis, which leads to a continued or escalating need for pain control. The result is worsening abdominal pain and initiation of the vicious NbS cycle. The syndrome occurs in patients with chronic diabetes-related pain, is complex to treat, and is often overlooked. This article addresses the impact of NbS on nutritional status and glycemic control, and offers practical management strategies for clinicians.
literature reviewOpioid Effects on the GI Tractused for centuries as the mainstay for chronic pain management, the term “opioid” refers to a class of drugs that interact with one of the three opioid receptors (mu, kappa and delta) (6). opioids are used as front-line agents for acute and chronic cancer-related
Narcotic bowel Syndrome
Nora Decher, MS, rD, CNSCNutrition Support Dietitianuniversity of Virginia Health SystemCharlottesville, VA
pain, and are commonly used as adjunctive treatment for chronic and neuropathic pain.
opioids act primarily on the mu receptors which are located throughout the central and peripheral nervous system, including the myenteric plexus (the largest collection of neurons outside of the brain). In the GI tract, stimulation of mu receptors induces a variety of physiological effects and symptoms (see Table 1), the most common of which is constipation (7). Adverse clinical GI symptoms of opioids are collectively referred to as opioid bowel dysfunction (obD). opioid use is associated with bowel dysfunction in 40% of patients who take opioids for chronic non-cancer related pain (8). The side effects of opioids can be as severe and debilitating as the pain itself.
Pathophysiology of Narcotic Bowel SyndromeWhile central opioid receptors desensitize over time, the peripheral receptors generally remain highly sensitive. Many clinicians are not aware that narcotics may heighten a patient’s sensitivity to pain, and instead of stopping them or providing alternative therapies, prescribe increased doses of narcotics. This perpetuates the vicious cycle (escalating narcotic doses, persistent or worsening pain and GI symptoms, more pain medication required, etc.) known as NbS (9).

27
Table 1. Effects of Opioids on the Gastrointestinal Tract
Gastrointestinal location Physiological Effect symptom
lower esophageal sphincter Inhibition of relaxation Abdominal discomfort
Gallbladder Contraction, reduced secretion upper abdominal discomfort, pain, delayed gastric emptying
Stomach Delayed gastric emptying, increased pyloric Nausea, vomiting, abdominal discomfort contraction and acid release
Small intestine Increased tonic and segmental contraction, Constipation, delayed gastric emptying, increased overall transit time of food, bloating, cramps decreased secretion
Colon Increased segmentation, decreased frequency Constipation, hard and dry stools, bloating of contraction and secretion and distension, spasm, cramps, pain
Anus/rectum Decreased rectal sensitivity, increased internal Straining, constipation sphincter tone
reprinted with permission from Chan lN. opioid analgesic and the gastrointestinal tract. Pract Gastroenterol. 2008:24(64):37–50. Available at: www.ginutrition.virginia.edu.
Although little data is available, NbS is likely becoming increasingly prevalent as opioid use for chronic pain management becomes more common. More reports are appearing in the literature as clinicians are becoming increasingly aware of this problem. Pletcher et al. reported that opioid prescriptions for pain-related emergency department visits increased from 27% in 1993 to 37% in 2005 as a result of national quality initiatives (10). However, Choung et al. attempted to identify the prevalence of obD among 117 patients taking narcotics, and were only able to identify five patients with “probable NbS” (11). NbS is difficult to recognize (making prevalence rates difficult to capture) because symptoms can be nonspecific; treatment may focus on an underlying GI disorder; and patient response to opioids varies greatly.
NbS is particularly difficult to treat because of the complexity of the clinician’s relationship with the patient, and sometimes clinicians’ attitudes towards narcotic-seeking behavior. A variety of complications may arise, particularly in the outpatient setting, such as patients
attempting to negotiate to restart narcotics, stopping narcotics too abruptly, or patients leaving to seek drugs from clinicians elsewhere. Grunkenmeier and colleagues have published NbS treatment guidelines based on their center’s extensive experience (12). Treatment is based on 1) weaning the patient off narcotic medications, 2) adding adjunctive therapies for pain management and 3) management of GI symptoms.
Clinical ApplicationNutritional ConsiderationsConstipation is a potentially serious condition that is often overlooked by clinicians and caretakers. Various methods such as the rome criteria and the bristol Stool Scale are used to define constipation; however palliative experts stress that constipation, like pain, should be defined by the patient. Complications associated with poorly managed constipation can be devastating. These include fecal impaction and seepage diarrhea; pseudo-obstruction of the bowel, resulting in abdominal pain, nausea and vomiting; and interference with drug administration and absorption. In addition to the physical and
emotional toll, constipation is responsible for significant cost to patients and the health care system.
Patients with NbS often experience symptoms that may contribute to malnutrition or inconsistent nutrition intake. In addition to the GI symptoms above, patients are at risk for dehydration, metabolic disturbances, poor glycemic control, psychological factors, anorexia and sitophobia (fear of eating).
Nutritional ManagementTreatment of diabetes-related NbS is difficult because of the multifaceted etiology, and requires communication among multidisciplinary team members. Nutritional management of diabetes-related NbS should center on the management of 1) constipation, 2) gastroparesis and 3) glycemic control (See Table 2). Guidelines for nutritional management of opioid bowel dysfunction have been previously published (9).
ConstipationThe clinician should first evaluate all possible sources of constipation before developing a systematic
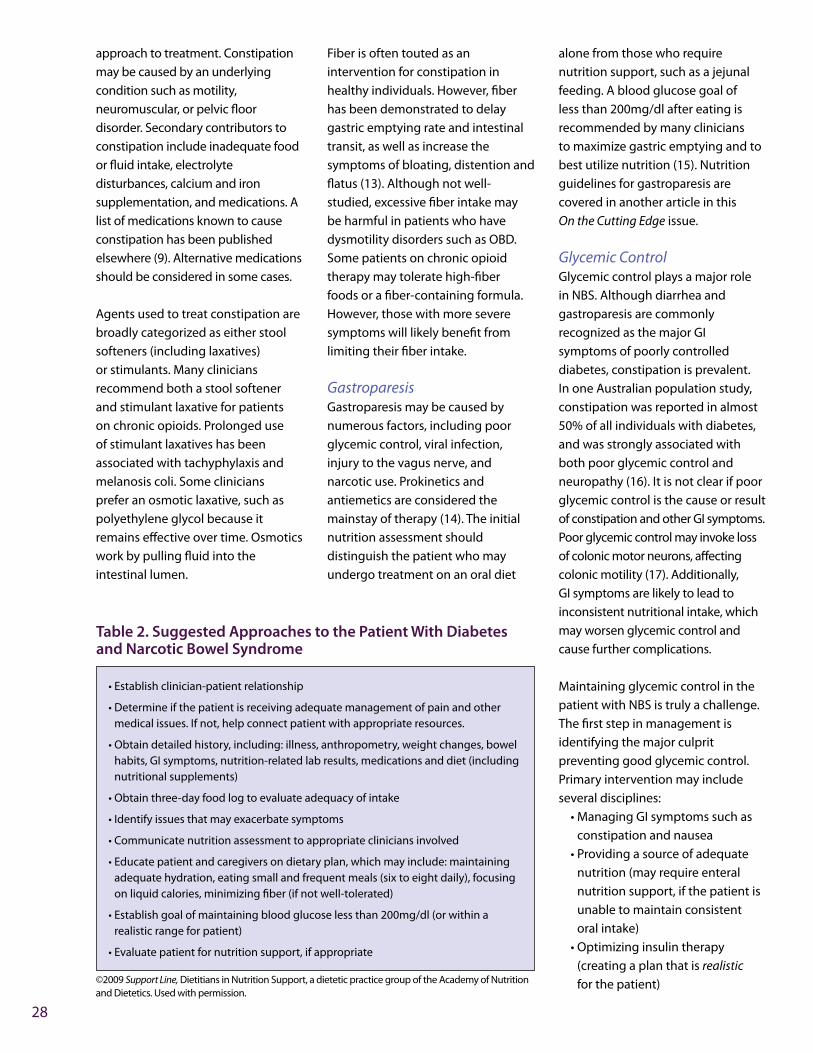
28
approach to treatment. Constipation may be caused by an underlying condition such as motility, neuromuscular, or pelvic floor disorder. Secondary contributors to constipation include inadequate food or fluid intake, electrolyte disturbances, calcium and iron supplementation, and medications. A list of medications known to cause constipation has been published elsewhere (9). Alternative medications should be considered in some cases.
Agents used to treat constipation are broadly categorized as either stool softeners (including laxatives) or stimulants. Many clinicians recommend both a stool softener and stimulant laxative for patients on chronic opioids. Prolonged use of stimulant laxatives has been associated with tachyphylaxis and melanosis coli. Some clinicians prefer an osmotic laxative, such as polyethylene glycol because it remains effective over time. osmotics work by pulling fluid into the intestinal lumen.
Fiber is often touted as an intervention for constipation in healthy individuals. However, fiber has been demonstrated to delay gastric emptying rate and intestinal transit, as well as increase the symptoms of bloating, distention and flatus (13). Although not well-studied, excessive fiber intake may be harmful in patients who have dysmotility disorders such as obD. Some patients on chronic opioid therapy may tolerate high-fiber foods or a fiber-containing formula. However, those with more severe symptoms will likely benefit from limiting their fiber intake.
GastroparesisGastroparesis may be caused by numerous factors, including poor glycemic control, viral infection, injury to the vagus nerve, and narcotic use. Prokinetics and antiemetics are considered the mainstay of therapy (14). The initial nutrition assessment should distinguish the patient who may undergo treatment on an oral diet
alone from those who require nutrition support, such as a jejunal feeding. A blood glucose goal of less than 200mg/dl after eating is recommended by many clinicians to maximize gastric emptying and to best utilize nutrition (15). Nutrition guidelines for gastroparesis are covered in another article in this On the Cutting Edge issue.
Glycemic ControlGlycemic control plays a major role in NbS. Although diarrhea and gastroparesis are commonly recognized as the major GI symptoms of poorly controlled diabetes, constipation is prevalent. In one Australian population study, constipation was reported in almost 50% of all individuals with diabetes, and was strongly associated with both poor glycemic control and neuropathy (16). It is not clear if poor glycemic control is the cause or result of constipation and other GI symptoms. Poor glycemic control may invoke loss of colonic motor neurons, affecting colonic motility (17). Additionally, GI symptoms are likely to lead to inconsistent nutritional intake, which may worsen glycemic control and cause further complications.
Maintaining glycemic control in the patient with NbS is truly a challenge. The first step in management is identifying the major culprit preventing good glycemic control. Primary intervention may include several disciplines:
• Managing GI symptoms such as constipation and nausea
• Providing a source of adequate nutrition (may require enteral nutrition support, if the patient is unable to maintain consistent oral intake)
• optimizing insulin therapy (creating a plan that is realistic for the patient)
• Establish clinician-patient relationship
• Determine if the patient is receiving adequate management of pain and other medical issues. If not, help connect patient with appropriate resources.
• obtain detailed history, including: illness, anthropometry, weight changes, bowel habits, GI symptoms, nutrition-related lab results, medications and diet (including nutritional supplements)
• obtain three-day food log to evaluate adequacy of intake
• Identify issues that may exacerbate symptoms
• Communicate nutrition assessment to appropriate clinicians involved
• Educate patient and caregivers on dietary plan, which may include: maintaining adequate hydration, eating small and frequent meals (six to eight daily), focusing on liquid calories, minimizing fiber (if not well-tolerated)
• Establish goal of maintaining blood glucose less than 200mg/dl (or within a realistic range for patient)
• Evaluate patient for nutrition support, if appropriate
Table 2. Suggested Approaches to the Patient With Diabetes and Narcotic Bowel Syndrome
©2009 Support Line, Dietitians in Nutrition Support, a dietetic practice group of the Academy of Nutrition and Dietetics. used with permission.

29
Mosapride citrate, a 5HT-4 receptor antagonist and prokinetic, has been shown to improve constipation, as well as lower blood glucose and is under investigation for use in diabetes-related constipation (18).
SummaryNbS is a complex condition. Management is challenging and involves coordination of numerous disciplines. Treatment of constipation, gastroparesis (if present), and glycemic control are the core of nutrition management for the patient with NbS.
references 1. Davies M, brophy S, Williams r,
Taylor A. The prevalence, severity, and impact of painful diabetic peripheral neuropathy in type 2 diabetes. Diabetes Care. 2006; 29(7):1518–1522.
2. daCosta Dibonaventura M, Cappelleri JC, Joshi AV. A longitudinal assessment of painful diabetic peripheral neuropathy on health status, productivity, and health care utilization and cost. Pain Med. 2011;12(1):118–126.
3. Albers JW, Herman WH, Pop-busui r, et al. Effect of prior intensive insulin treatment during the Diabetes Control and Complications Trial (DCCT) on peripheral neuropathy in type 1 diabetes during the Epidemiology of Diabetes Interventions and Complications (EDIC) Study. Diabetes Care. 2010;33(5):1090–1096.
4. Wong MC, Chung JWY, Wong TKS. Effects of treatments for symptoms of painful diabetic neuropathy: systematic review. BMJ. 2007;335(7610):87.
5. Haanpää Ml, Gourlay GK, Kent Jl, et al. Treatment considerations for patients with neuropathic pain and other medical comorbidities. Mayo Clin. Proc. 2010;85(Suppl 3):S15–S25.
6. Noto C, Pappagallo M. Current and emerging pharmacologic therapies for pain and challenges which still lay ahead. Methods Mol Biol. 2010;617:539–554.
7. Thomas J. opioid-induced bowel dysfunction. J Pain Symptom Manage. 2008;35(1):103–113.
8. Pappagallo M. Incidence, prevalence, and management of opioid bowel dysfunction. Am J Surg. 2001;182(Suppl 5A):11S–18S.
9. Decher N. Nutritional implications of opioid-induced bowel dysfunction in chronic pain management. Support Line. 2009;31(6):19–27.
10. Pletcher MJ, Kertesz SG, Kohn MA, Gonzales r. Trends in opioid prescribing by race/ethnicity for patients seeking care in u.S. emergency departments. JAMA. 2008;299(1):70–78.
11. Choung rS, locke Gr, Zinsmeister Ar, Schleck CD, Talley NJ. opioid bowel dysfunction and narcotic bowel syndrome: a population-based study. Am J Gastroenterol. 2009;104(5):1199–1204.
12. Grunkemeier DMS, Cassara JE, Dalton Cb, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol. Hepatol. 2007;5(10):1126–1139.
13. bianchi M., Capurso l. Effects of guar gum, ispaghula and microcrystalline cellulose on abdominal symptoms, gastric emptying, orocaecal transit time and gas production in healthy volunteers. Dig Liver Dis. 2002; 34 (Suppl 2):S129–S133.
14. Parkman H, Hasler Wl, Fisher rS; American Gastrointestinal Association. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology. 2004; 127(5):1592–1622.
15. Parrish Cr, Yoshida CM. Nutrition intervention for the patient with gastroparesis: an update. Practical Gastroenterology. 2005;XXIX(8):29.
16. bytzer P, Talley NJ, Hammer J, Young lJ, Jones MP, Horowitz M. GI symptoms in diabetes mellitus are associated with both poor glycemic control and diabetic complications. Am J Gastroenterol. 2002;97(3):604–611.
17. Chandrasekharan b, Anitha M, blatt r, et al. Colonic motor dysfunction in human diabetes is associated with enteric neuronal loss and increased oxidative stress. Neurogastroenterol Motil. 2011;23(2):131–138.
18. ueno N, Inui A, Satoh Y. The effect of mosapride citrate on constipation in patients with diabetes. Diabetes Res Clin Pract. 2010;87(1):27–32.

CPE Credit Self-Assessment QuestionnaireAfter reading this issue of On the Cutting Edge, “Gastrointestinal Issues Encountered in Diabetes Mellitus,” DCE members can earn 3.0 hours of free continuing professional education units (CPEus level II) approved by the Commission on Dietetic registration (CDr). CPE eligibility is based on active DCE membership status from June 1, 2011 to May 31, 2012.
DCE members must complete the post-test on the CPEus page on the DCE website: http://ww.dce.org/resources/cpeus by December 31, 2012. For each question, select the one best response. After passing the quiz, to view/print your certificate, access your CPEu credit history or view the learning objectives, go to: http://www.dce.org/account/history.
Please record 3.0 hours on your learning Activities log and retain the certificate of completion in the event you are audited by CDr. The certificate of completion is valid when the CPE questionnaire is successfully completed, submitted to, and recorded by DCE/Academy of Nutrition and Dietetics .
1) A key principle to remember when managing a person with diabetes and celiac disease is:
a. Many gluten-free products are whole grain which has a positive impact on blood glucose levels.
b. Encourage the use of fresh fruits, more vegetables and nuts to enhance fiber consumption.
c. If on insulin, the person may benefit from taking a rapid-acting insulin immediately before eating.
d. Generally transitioning to a gluten-free diet can be accomplished within one or two weeks.
2) Fiber is most likely to be helpful in patients:
a. With severe colonic inertia b. Who are producing soft stool c. With relatively normal colonic
transport d. none of the above
3) Amylin works with insulin to manage blood glucose by which mechanism?
a. Dose-dependently decreases food intake and body weight
b. Slows gastric emptying to decrease nutrient transport from the stomach to the small intestine
c. Suppresses postprandial glucagon secretion via centrally mediated vagal efferents
d. All of the above
4) Small bowel bacterial overgrowth in diabetes rarely results in deficiency of which of the following?
a. Vitamin A b. Vitamin D c. Vitamin E d. Vitamin K
5) For persons with diabetes who suffer from constipation, it is important to:
a. Distinguish between soluble and insoluble fiber sources
b. Continue to encourage an increase in fiber for all patients as there is no “downside”
c. Assess dietary fiber intake and make recommendations based on the assessment
d. Increase fiber intake slowly to eventually reach an intake of at least 35 grams of fiber per day
6) Symptoms of small bowel bacterial overgrowth in diabetes may include
a. Early satiety, nausea and vomiting b. Folate deficiency c. Protein malnutrition d. Weight gain
7) Attention should be given to the monitoring of certain nutrients in patients with gastroparesis due to limited oral intake or anatomical changes from surgery. More common deficiencies include:
a. Magnesium, calcium, folate b. Iron, vitamin D, vitamin b-12 c. Chromium, vitamin C, vitamin E d. Zinc, copper, vitamin A
8) Patients with narcotic bowel syndrome are at risk for GI symptoms including:
a. Dehydration, metabolic disturbances
b. Poor glycemic control, fear of eating c. Psychological factors, anorexia d. b & C e. All of the above
9) Hyperglycemia greater than ________ mg/dl can delay gastric emptying in those with diabetes.
a. 150 b. 180 c. 200 d. 270
10) How much fluid is secreted in the GI tract every day?
a. 4 to 5 liters b. 5 to 6 liters c. 6 to 7 liters d. 7 to 8 liters
30

2011-2012 DCE oFFICEr DIrECTorYEXECuTIVE CoMMITTEE
ChairAmy Hess, MS, rD, lD, bC-ADM, [email protected]
Chair-ElectAndrea Dunn, rD, lD, CDE440-871-1421 [email protected]
Past Chair/Industry Relations ChairMolly Gee, MEd, rD, [email protected]
secretaryCarolyn Harrington, rD, CD, CDE715-675-2003 [email protected] [email protected]
TreasurerAmber Wamhoff, MA, rD, lD, CDE314-583-4525 [email protected]
Membership CoordinatorJudy Giusti, MS, rD, lDN, [email protected] [email protected]
Print Communications Coordinatorliz Quintana, EdD, rD, lD, [email protected]
Electronic Communications CoordinatorSusie Wang, MS, rD, CD, [email protected]
Professional Development Coordinatorlisa brown, rD, lD, [email protected]
Public PolicySusan Yake, rD, CD, CDE, [email protected] [email protected]
Research CoordinatorMaggie Powers, PhD, rD, [email protected]
Dietetic Practice Group DelegateMaryann Meade, MS, rD, CDN, [email protected]
NEWSlETTEr CoMMITTEE
Newsflash Editorlorena Drago, MS, rD, CDN, CDE718- [email protected]
OTCE EditorAlyce Thomas, [email protected]
OTCE associate EditorDiane reader, rD, [email protected]
ElECTroNICS CoMMITTEE
e-Update Editorlinda ro, MS, rD, lD, [email protected]
website Editorraquel Pereira, MS, rD, [email protected]
listserv ModeratorMarylou Anderson, [email protected]
CoMMITTEE CHAIrS
alliance/InternationalMolly Gee, MEd, rD, lDAmy Hess, MS, rD, lD, bC-ADM, CDE Andrea Dunn, rD, lD, CDE
awards Committee ChairSusan rizzo, rD, lDN, [email protected]
awards Committee assistant ChairNell Stuart, MS, rD, lD, [email protected]
Publications Committee ChairNaomi Wedel, MS, rD, CD, CDE, [email protected]
Mentor Program ChairPat Severson-Wager, MS, rD, CDN, [email protected]
Reimbursement Committee ChairMarla Solomon, rD, lD/N, [email protected]
Nominating Committee ChairPatti urbanski, MEd, rD, lD, [email protected]
SPECIAl ProJECT HEADS
National Diabetes Education Program/ NDEP liaisonSandra Parker, rD, [email protected]
Technology Task force ChairKaren Poenisch, rD, CD, [email protected]
MEMbErSHIP CoMMITTEE
Membership RepresentativesPatti Geil, MS, rD, FADA, [email protected]
rosalyn Haase, MPH, rD, CD, CDE, [email protected]
Peggy o’Neil, rD, [email protected]
social Media ChairConstance brown-riggs, MSEd, rD, CDN, CDE [email protected]
ADA/DCE STAFF
administrative Managerlinda Flanagan Vahl312-899-4725800-877-1600 ext 4725Fax: [email protected]
DCE SuPPorT SErVICES
DCE webmasterAurimas [email protected]
DCE web address www.dce.org
DCE Copy Editor Donna [email protected]
31

PrINTED oN rECYClED PAPEr
lETTErS To
The EditorHave you ever wanted to ask an OTCE author a question after reading an article? Did you ever disagree with an author? or maybe you just wanted to comment on something you read. The letters to the Editor column is a forum to ask questions or comment about any of the OTCE articles that interest you. Please send your questions or comments to the OTCE editor at the following address:
Alyce Thomas, rD OTCE Editor [email protected]
Let us hear from you!
a dietetic practice group of the
Diabetes Care and Education