CUTANEOUS PETECHIAE CORONARY ARTERY DISEASE · CUTANEOUS PETECHIAE IN FATAL CORONARY ARTERY DISEASE...
5
J. clin. Path. (1958), 11, 391. CUTANEOUS PETECHIAE IN FATAL CORONARY ARTERY DISEASE BY L. M. GERLIS From the Department of Pathology, Grimsby General Hospital (RECEIVED FOR PUBLICATION FEBRUARY 6, 1958) In the clinical recognition of myocardial ischaemia, the nature and distribution of the referred pain which frequently accompanies it are of considerable diagnostic importance. Unfor- tunately in cases of sudden death there may be no such history and not always is an unequivocal fatal cardiac lesion found, such as a recent or ruptured infarct, or an acute occluding lesion of a coronary artery. In some there is little to indicate why or how the patient actually died, as the only cardiac lesions found are of long standing. The fatal disturbance is often of function rather than of structure and in such cases the post-mortem diagnosis of acute coronary insufficiency is made by implication rather than observation. In seven necropsies on cases of acute coronary death cutaneous petechiae were observed at sites commonly associated with referred pain of cardiac origin (Fig. 1). No such lesions were observed in any deaths not of coronary origin. These petechiae were all outside the area of cutaneous post-mortem hypostasis and in no case w as there any evidence of generalized haemor- rhagic disease. It is suggested that this sign may be of diagnostic significance in the post-mortem diagnosis of coronary insufficiency. There appears to be no previous description of similar observations in cases of coronary heart disease either before or after death. Case Reports Case 1.-A housewife aged 72 years died two days after admission to hospital in a collapsed state with dyspnoea and pain in the left shoulder. Three weeks previously she had experienced an attack of gripping pain in the retrosternal region. There was no previous history of any other illness. At necropsy fine recent petechiae were seen over the left deltoid region and in the left submammary region. The heart showed extensive recent infarction involving the whole of the anterior wall of the left ventricle and most of the ventricular septum. The coronary arteries were severely atheromatous, and the first part of the anterior descending branch of the left coronary artery was occluded by a mass of degenerate atheroma. Case 2.-A man of 64 years who had led a healthy and active life as a pedlar was found dead in bed the day after he experienced a sensation of being unwell, accompanied by pain in the chest and abdomen, although these did not restrict his usual activities. There was a localized area of fine recent petechiae on the right side of the chest extending as a horizontal band 71 cm. long and 5 cm. wide just below the right nipple and fading out over the right border of the sternum. The lungs showed acute oedema. The heart was not enlarged. A solitary subepicardial petechia was present in the atrioventricular groove near the right cardiac border. The right coronary artery showed a region of atheromatous stenosis at a point 1 cm. from the origin. Distal to this there was a segment of complete occlusion by a thrombus extending for 2 cm., and histological examination showed acute haemorrhagic extravasation into the adventitia overlying this occluded portion. The myocardium showed no evidence of acute infarction. Case 3.-This 37-year-old blacksmith was found to have an enlarged heart and an atypical bundle-branch block at the age of 29. In the subsequent two years he had several attacks of "blackout " which were preceded by pain in the tips of the fingers of the left hand which spread up into the left arm, and terminated in unconsciousness. There was no history of convulsive fits. During the last two years of his life he suffered from palpitations. Three days before death in April, 1953, he had increasing dyspnoea and epigastric pain radiating to the back between the shoulder blades, upwards into both sides of the neck, and down the inner sides of both arms. Clinical examination showed severe shock with cardiomegaly and venous congestion. At necropsy numerous small recent petechiae were seen over both shoulders and between the shoulder blades. The heart was enormously enlarged, weigh- ing 33 oz. (935 g.), this being due to massive hyper- trophy and dilatation of the left ventricle. The atria were of normal size. Several superficial recent sub- epicardial petechiae were present in the atrioventricu- copyright. on January 29, 2021 by guest. Protected by http://jcp.bmj.com/ J Clin Pathol: first published as 10.1136/jcp.11.5.391 on 1 September 1958. Downloaded from
Transcript of CUTANEOUS PETECHIAE CORONARY ARTERY DISEASE · CUTANEOUS PETECHIAE IN FATAL CORONARY ARTERY DISEASE...

J. clin. Path. (1958), 11, 391.
CUTANEOUS PETECHIAE IN FATAL CORONARYARTERY DISEASE
BY
L. M. GERLISFrom the Department of Pathology, Grimsby General Hospital
(RECEIVED FOR PUBLICATION FEBRUARY 6, 1958)
In the clinical recognition of myocardialischaemia, the nature and distribution of thereferred pain which frequently accompanies it areof considerable diagnostic importance. Unfor-tunately in cases of sudden death there may beno such history and not always is an unequivocalfatal cardiac lesion found, such as a recent or
ruptured infarct, or an acute occluding lesion of a
coronary artery. In some there is little to indicatewhy or how the patient actually died, as the onlycardiac lesions found are of long standing. Thefatal disturbance is often of function rather thanof structure and in such cases the post-mortemdiagnosis of acute coronary insufficiency is madeby implication rather than observation.
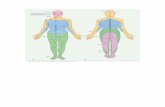
In seven necropsies on cases of acute coronarydeath cutaneous petechiae were observed at sitescommonly associated with referred pain ofcardiac origin (Fig. 1). No such lesions were
observed in any deaths not of coronary origin.These petechiae were all outside the area ofcutaneous post-mortem hypostasis and in no casew as there any evidence of generalized haemor-rhagic disease. It is suggested that this sign may
be of diagnostic significance in the post-mortemdiagnosis of coronary insufficiency. Thereappears to be no previous description of similarobservations in cases of coronary heart diseaseeither before or after death.
Case ReportsCase 1.-A housewife aged 72 years died two days
after admission to hospital in a collapsed state withdyspnoea and pain in the left shoulder. Three weekspreviously she had experienced an attack of grippingpain in the retrosternal region. There was no
previous history of any other illness.At necropsy fine recent petechiae were seen over
the left deltoid region and in the left submammaryregion. The heart showed extensive recent infarctioninvolving the whole of the anterior wall of the leftventricle and most of the ventricular septum. Thecoronary arteries were severely atheromatous, and the
first part of the anterior descending branch of the leftcoronary artery was occluded by a mass of degenerateatheroma.
Case 2.-A man of 64 years who had led a healthyand active life as a pedlar was found dead in bedthe day after he experienced a sensation of beingunwell, accompanied by pain in the chest andabdomen, although these did not restrict his usualactivities.There was a localized area of fine recent petechiae
on the right side of the chest extending as a horizontalband 71 cm. long and 5 cm. wide just below the rightnipple and fading out over the right border of thesternum. The lungs showed acute oedema. Theheart was not enlarged. A solitary subepicardialpetechia was present in the atrioventricular groovenear the right cardiac border. The right coronaryartery showed a region of atheromatous stenosis ata point 1 cm. from the origin. Distal to this therewas a segment of complete occlusion by a thrombusextending for 2 cm., and histological examinationshowed acute haemorrhagic extravasation into theadventitia overlying this occluded portion. Themyocardium showed no evidence of acute infarction.
Case 3.-This 37-year-old blacksmith was found tohave an enlarged heart and an atypical bundle-branchblock at the age of 29. In the subsequent two yearshe had several attacks of "blackout " which werepreceded by pain in the tips of the fingers of the lefthand which spread up into the left arm, andterminated in unconsciousness. There was no historyof convulsive fits. During the last two years of hislife he suffered from palpitations.Three days before death in April, 1953, he had
increasing dyspnoea and epigastric pain radiating tothe back between the shoulder blades, upwards intoboth sides of the neck, and down the inner sides ofboth arms. Clinical examination showed severe shockwith cardiomegaly and venous congestion.At necropsy numerous small recent petechiae were
seen over both shoulders and between the shoulderblades. The heart was enormously enlarged, weigh-ing 33 oz. (935 g.), this being due to massive hyper-trophy and dilatation of the left ventricle. The atriawere of normal size. Several superficial recent sub-epicardial petechiae were present in the atrioventricu-
copyright. on January 29, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.5.391 on 1 Septem
ber 1958. Dow
nloaded from

FIG. 1.-Diagram showing dis-tribution of the cutaneouspetechiae in the casesdescribed in the text.
/95
% I
I1)
2I
IANT. pOst
% I
/
7I
6
/
I
bwl j./'
F$
1.
copyright. on January 29, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.5.391 on 1 Septem
ber 1958. Dow
nloaded from

CUTANEOUS PETECHIAE IN FATAL CORONARY ARTERY DISEASE
lar groove. There were no septal defects or valvularmalformation and no stenosis at the aortic outlet.The aorta showed a moderate generalized hypoplasia.The coronary arteries shared in this hypoplasia; theinternal diameters of first parts of both main vesselsmeasured only 2 mm., displaying a marked dis-proportion to the enormously increased mass of themyocardium.
Case 4.--A woman aged 87 years was found deadin bed having always enjoyed good health until twoto three days previously, when she had complainedof slight pain in the chest. This caused little distress,and she refused medical attention.At necropsy six small recent petechiae were seen
on the left side of the precordium. Internal examina-tion showed terminal pulmonary oedema and moder-ate enlargement of the left ventricle. There wasgeneralized coronary atheroma with a zone of recentocclusion in the first part of the right main artery.The myocardium was soft, but there was no actualinfarct. Sections of the affected coronary arteryshowed old organized thrombus in the lumen andrecent haemorrhage in the wall.
Case 5.-An 86-year-old man was found dead.There was no previous medical history. There werefine recent petechiae over the left side of the pre-cordium, and over the anterior aspect of the rightshoulder. Internal examination showed terminalpulmonary oedema and a moderately enlarged heart.The myocardium was soft and there were patches ofinterstitial fibrosis. The coronary arteries showedwidespread stenosis by calcified atheroma, and therewas recent occlusion of the right main artery bythrombus.
Case 6.-For several months this 68-year-oldwoman had suffered transient attacks of dyspnoeaand a sensation of constriction in the chest which hadcaused very little inconvenience and responded torest, aspirin, and hot-water bottles. Her final attackbegan in the usual way, but the sense of constrictionbecame progressively worse and was accompanied bypain. She died before the doctor arrived.At post-mortem examination there was a transverse,
slightly oblique area of erythema over the upperportion of the right side of the precordium whichstopped abruptly at the midline. Numerous petechiaewere present in this area and there were afew up to 1.5 cm. beyond its well-defined margin(Fig. 2). Internal examination showed extensivecalcified atheroma and stenosis of the main coronaryarteries with complete occlusion of the anteriordescending branch of the left artery from within1 cm. of its origin. The myocardium was soft, but noinfarct was found. Sections of the skin showed thatthe erythema was due to dilatation of the capillariesof the dermis, and that the petechiae were minuteareas of recent haemorrhage.
Case 7.-A seaman aged 64 years was found deadin his bed. There was no available history ofprevious illnesses. There was a group of about 2020
s....Ar#..
..., ,
FIG. 2.-Post-mortem photograph of Case 6 showing the well-definedarea of precordial erythema and petechiae.
petechiae occupying a circular area approximately5 cm. in diameter in the skin overlying the centralportion of the left clavicle.Internal examination showed acute terminal con-
gestion and slight oedema of both lungs, thesechanges being most severe at the bases. Both cardiacventricles showed slight hypertrophy and there was asmall number of subepicardial petechiae in the wallof the left atrium and along the inferior margin ofthe right ventricle. Both coronary arteries showedmarked atherosclerosis with almost complete occlu-sion of the left coronary artery just proximal to itsbifurcation, and of its anterior descending branch.There was an area of haemorrhagic extravasation intothe adventitia of the circumflex branch beginningabout 3 cm. from its origin and extending for I cm.This was confirmed by histological examination(Figs. 3 and 4). No massive myocardial infarctionor fibrosis was present.
DiscussionTwo of these patients (Cases 1 and 3) had been
subjected to frequent clinical examinations beforedeath, but in neither case had cutaneous petechiaebeen noticed, nor have similar lesions beenrecorded amongst the clinical manifestations ofcoronary disease.Although fatal coronary disease is common,
these petechiae are rare. Five of the seven caseswere from a personally studied series of 360deaths due to coronary insufficiency in which asearch for petechiae was specifically made, givingan incidence of 1.7%.
It is considered that these cutaneous petechiaemay be caused by intense efferent stimuli alonga sympathetic nerve pathway similar to thatinvolved in referred pain, possibly by agonalrelaxation of blood vessels which had been
393
copyright. on January 29, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.5.391 on 1 Septem
ber 1958. Dow
nloaded from

L. M. GERLIS
FIG. 3.-Section of the circumflex branch of the left coronary arteryfrom Case 7 showing the adventitial haemorrhage. Involvednerves are indicated at A and B. ( x 12.)
damaged by prolonged spasm. Peripheral vaso-constriction has been held to be responsible forreferred cardiac pain by Roberts (1945) and hasbeen demonstrated by variations of cutaneoustemperature (Doret and Ferrero, 1951). Ananalogous mechanism is known to be responsiblefor the trophic lesions in the upper limb which arewell-recognized clinical sequelae of acute cardiacpain and myocardial infarction (Askey, 1941;Kehl, 1943; Johnson, 1943; Steinbrocker, Spitzer,and Friedman, 1948; Hilker, 1949; Chitwood,1950; Swan and Henderson, 1951).Apart from possibly initiating reflexes, which
may cause spasm of the peripheral vessels, thecoronary arteries themselves are subject to vaso-spastic stimuli from various organs of the body(von Bergmann, 1932; Greene, 1935; Gilbert,Fenn, and LeRoy, 1940; Freedberg, Spiegi, andRiseman, 1944). It is possible that in the casesdescribed in the present series the violent cutane-ous reflexes were accompanied by equally violentspasm of the coronary arteries. This may explainwhy the petechiae have been found only at post-
FIG. 4.-The area indicated by arrow A in Fig. 3 x 150, showing twoadventitial nerves in the area of haemorrhagic extravasation.
morten. examinations, and not in patients whohave survived an acute coronary episode.
In four of the seven cases there were haemor-rhages directly related to the coronary arteriesthemselves. In three of these there were haemor-rhages in the coronary adventitia and direct in-volvement of the nerve elements may have playedsome part in the production of vasospastic reflexesto the skin and coronary arteries (Figs. 3 and 4).However, such haemorrhages are not common infatal coronary insufficiency. In 100 cases withoutcutaneous petechiae, only three examples of ad-ventitial haemorrhage were found and the adven-titial lesions in the " petechiae " cases were prob-ably an effect rather than a cause, occurring to-gether with the cutaneous lesions by a similarreflex mechanism.
In Case 4 there was subintimal haemorrhage inthe wall of the coronary artery, and, if it is con-sidered that this condition may also be caused bynervous reflexes, this may have a bearing on amajor mechanism of acute coronary insufficiency.Paterson (1936) first showed the importance of
394
4. .-i' X..
copyright. on January 29, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.5.391 on 1 Septem
ber 1958. Dow
nloaded from

CUTANEOUS PETECHIAE IN FATAL CORONARY ARTERY DISEASE
subintimal haemorrhage in the pathogenesis ofcoronary disease, and Wartman (1938) consideredit to be the second most-common cause of coro-nary artery occlusion, thrombosis being the first.Expanding subintimal or mural haematomata areheld to be responsible for about 10% of cases ofacute coronary occlusion (Lowe, 1950), but inmany more cases a small haemorrhage in the wallmay play an important role by initiating throm-bosis in the arterial lumen. Wartman (1950)found significant haemorrhage in 62% of a seriesof 365 cases of fatal coronary occlusion, andDrury (1954) found it in 37 of 58 cases (68%).In a personal series of 100 deaths due to coro-nary disease mural haemorrhage was found in58 cases.
It is an interesting speculation that, if suchhaemorrhages can be produced by nervousstimuli, it is possible that anginal pain, notassociated with organic coronary occlusion,might in fact cause such occlusion.
SummarySeven cases are described in which cutaneous
petechiae were found at necropsy on patients whohad died of acute coronary insufficiency. Thesepetechiae occurred in areas commonly associatedwith referred cardiac pain.
It is suggested that the presence of such local-ized petechiae is supporting evidence of acutecoronary insufficiency, particularly in those caseswhere the coronary arteries themselves show norecent culpable organic lesion. In four of thecases haemorrhagic lesions were found in directrelationship to the coronary arteries. Themechanism is discussed and the possible role ofreflex activity in the aetiology of subintimal coro-nary haemorrhages is considered.
I wish to thank Dr. J. D. H. Millar and Dr. M.Steel for permission to publish clinical details of theircases, and also Dr. J. M. Johnstone for the post-
mortem findings on Case 7 and for his advice on thepreparation of this paper.
AddendumSince writing this paper the following additional
case has been encountered.A heavily built man aged 67 years was sitting
quietly in his home watching television; he bentforward to place some wood on the fire, sat back inhis chair and died suddenly and quietly.At necropsy there was a small group of minute
recent petechiae up to 0.5 cm. in diameter over thefront of the left shoulder in an ill-defined horizontalband 5 cm. long and 1 cm. wide.The heart was moderately enlarged (450 g.) and
there was an extensive area of recent myocardial in-farction involving the distal half of the anterior wallof the left ventricle and the adjacent portion of theinterventricular septum.The coronary arteries showed only moderate
atheroma, except for an area of localized occlusion ofthe anterior descending branch of the left artery at apoint of 3.5 cm. from its origin. Sections of thisregion showed considerable stenosis by a lipoidplaque in which there was recent haemorrhage whichcommunicated with a recent thrombus that occludedthe lumen of the vessel.
REFERENCESAskey, J. M. (1941). Amer. Heart J., 22, 1.Bergmann, G. von (1932). Dtsch. med. Wschr., 58, 605.Chitwood, W. R. (1950). New Engl. J. Med., 243, 813.Doret, J. P., and Ferrero, R. (1951). Cardiologia (Basel), 19, 80.Drury, R. A. B. (1954). J. Path. Bact., 67, 207.Freedberg, A. S., Spiegl, E. D., and Risernan, J. E. F. (1944). Amer
Heart J., 27, 611.Gilbert, N. C., Fenn, G. K., and LeRoy, G. V. (1940). J. Amer. med.
Ass., 115, 1926.Greene, C. W. (1935). Amer. J. Physiol., 113, 399.Hilker, A. W. (1949). Ann. intern. Med., 31, 303.Johnson, A. C. (1943). Ibid., 19, 433.Kehl, K. C. (1943). Ibid., 19, 213.Lowe, T. E. (1950). Studies in Pathology, p. 81. Cambridge University
Press, London.Paterson, J. C. (1936). Arch. Path. (Chicago), 22, 313.Roberts, J. T. (1945). Med. Ann. D.C., 14, 483.Steinbrocker, O., Spitzer, N., and Friedman, H. H. (1948). Ann.
intern. Med., 29, 22.Swan, W. G. A., and Henderson, C. B. (1951). Brit. Heart J., 13, 68.Wartman, W. B. (1938). Amer. Heart J., 15, 459.-(1950). Studies in Pathology, p. 95. Cambridge University
Press, London.
395
copyright. on January 29, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.5.391 on 1 Septem
ber 1958. Dow
nloaded from