Cutaneous Lymphoid Hyperplasia, Cutaneous T-Cell Lymphoma, & Cutaneous B-Cell Lymphomas JoAnne M....
146
Cutaneous Lymphoid Hyperplasia, Cutaneous T- Cell Lymphoma, & Cutaneous B-Cell Lymphomas JoAnne M. LaRow, DO May 4, 2004
-
date post
22-Dec-2015 -
Category
Documents
-
view
223 -
download
1
Transcript of Cutaneous Lymphoid Hyperplasia, Cutaneous T-Cell Lymphoma, & Cutaneous B-Cell Lymphomas JoAnne M....

Cutaneous Lymphoid Hyperplasia, Cutaneous T-Cell Lymphoma, & Cutaneous B-Cell Lymphomas
JoAnne M. LaRow, DOMay 4, 2004

Cutaneous Lymphoid Hyperplasia• Collection of lymphocytes with other inflammatory cells in the skin• Aka: lyphocytoma cutis, lymphadenosis benigna cutis (LABC),
Spiegler-Fendt sarcoid• Not a single dx state• Rxn to a range of stimuli• Possibilities:
– medications, – infections– arthropod bites– UV light– Borrelia burgdorferi infection

Clinical features
• Seen most often in adults; more often in women• A firm, erythematous-violaceous papule on
head, neck, or upper extremity• Localized clusters of papules are often seen• Mostly there is no surface change-but some
slight scale & follicular accentuation has been described

• Erythematous nodules characteristic of this dx

• Coalescing erythematous follicular papules and raspberry-like nodules on the right shoulder.

Cutaneous lymphoid hyperplasia
• Low: in cutaneous lymphoid hyperplasia there are nodular aggregates of mononuclear cells within dermis that may extend into subcutaneous fat;infiltrate may be diffuse or as seen here nodular in architecture

• Cutaneous lymphoid hyperplasia: demonstrates germinal center formation, presence of tingible-body macrophages, & a mantle zone

Cutaneous lymphoid hyperplasia• High:germinal
center consists of central large mononuclear cells with vesicular nuclei-these are surrounded by a mantle of small lymphocytes

Pathology
• Superficial & deep nodular or diffuse infiltrate of lymphocytes admixed with histiocytes & occasional plasma cells & eos
• Dense dermal infiltrate-recapitulating nodal architecture• In florid cases, germinal centers with prominent tingible-
body macrophages are seen• A mantle zone may surround the lymphoid follicles• Diagnosis can usually be made on routine H&E, with
addition of immunostains if H & E non-diagnostic

Cutaneous Lymphoid Hyperplasia
• May progress to lymphoma• Immunosuppression may aggravate the infiltrate and may regress
with immunosuppression is removed• Differential dx: lymphoma cutis, lymphocytic infiltrate of Jessner, &
occasionally adnexal tumors• Can be differentiated from lymphoma by presence of reactive
germinal centers, a polymorphous infiltrate of lymphocytes & histiocytes & presence of eos &/or plasma cells
• Most CLH demonstrates brisk B lymphocytic infiltrate; Jessner’s generally T-cell predominant

Immunophenotyping
• Predominance of T cells, B cells localized to germinal centers
• Cells with both kappa & lambda expression are present• Predominance of CD4+ T helper lymphocytes, with a
significant minority population of CD8+ cytotoxic/suppressor T cells
• Positive CD68 demonstrates presence of abundant histiocytes

Cutaneous lymphoid hyperplasia
• The lack of acanthosis, "bottom-heavy" infiltrates, light-chain expression of monotypical B-cells, and immunoglobulin gene rearrangements (75%) provide strong evidence for the diagnosis of B-cell lymphoma
• A careful monitoring of these patients for the development of lymphoma is necessary


Cutaneous T Cell Lymphomas

Primary Cutaneous T-Cell Lymphomas
Dx:Obtain 4-5 mm punch bx/or excisional or incisional
bx from most representative skin lesionLymphoma vs benign condition?Atypical T-cell infiltrates are found also in lymphoid
drug rxns(pseudolymphoma)Immunohistochemical stains aid in dx(use
antibodies reactive with cell-surface or cytoplasmic molecules

Mycosis Fungoides• Most common type of CTCL• Accounts for 50% of all primary cutaneous lymphomas• Term reserved for classical ‘Alibert-Bazin’type-characterized by typical
evolution of patches, plaques,tumors or for clinicopathologic variants showing a simiilar cclinical course
• Malignancy of T-lymphocytes, almost always MEMORY T-CELL• Race: MF is more common in black than in white patients (incidence ratio 1.6). • Sex: MF occurs more frequently in men than in women (male-to-female ratio
of 2:1). • Age: The most common age at presentation is 50 years; however, MF also
can be diagnosed in children and adolescents with apparently similar outcomes.

Mycosis Fungoides
• Patch Stage – pre-mycotic, severe pruritis. • Plaque Stage – infiltrated plaque• Tumor Stage – when de novo, called d’ emblee
form• Erythroderma – Rare

MF Staging
• TNMB system on skin (T) node (N), viscera (M), and blood (B)
• T1 – Skin involvement <10%• T2 – Skin involvement >10%• T3 – Tumor• T4 – Erythroderma

MF Staging
• N0 – normal nodes• N1 – palpable but not pathologically MF• N2 – not palpable but pathologically MF• N3 – clinically and pathologically involved
• M0 B0 - Viscera and blood not involved• M1 B1 - Viscera and blood involved

MF Staging
• Stage IA – T1, N0, M0 – 8-9% progress• Stage IB – T2, N0, M0 – 11-16 years surv• Stage IIA – T1-2, N1, M0 – 7.7 years• Stage IIB – T3, N0-1, M0 – 3-8 years surv• Stage IIIA – T4, N0, M0 – 1.8-3.7 years• Stage IIIB – T4, N1, M0 – 1.8-3.7 years• Stage IVA – T1-4, N2-3, M0• Stage IVB – T1-4, N0-3, M1


Limited patch/plaque stage dx (1a)
• Patches on buttocks involving <10% of skin surface• Atypical lymphocytes in typical linear configuration along epidermal basal layer

Generalized patch/plaque stage
• Extensive patches & plaques involving >10% of skin surface; pronounced epidermotropism with formation of small nests of atypical cells (Pautrier’s microabscesses)

Tumor stage
• Multiple skin tumors in combination with typical patches & plaques; diffuse dermal infiltrates of medium-sized to large neoplastic T cells

Cutaneous T-cell lymphoma• Medium:
epidermotropic T cells (“Pautrier microabscesses”) which is a feature that helps differentiate this lesion from cutaneous B-cell lymphoma

Lymph nodes in MF
• Extracutaneous involvement is more clinically evident as the stage and extent of MF increases
• Peripheral lymphadenopathy is the most frequent site of extracutaneous involvement in MF
• Evaluate palpable lymphadenopathy by obtaining a biopsy because the result influences the patient’s stage, prognosis, and treatment.

MF Workup• CBC – to review the buffy coat smear for Lymph nodes• CMP• Liver Function to include LDH (aggressive) and
transaminase (liver involvement) values• CXR• If lymph nodes are palpable
– CT to access abdominal and pelvic nodes– Lymph node biopsy


Histologic Findings
The criteria for diagnosis include the following: • A bandlike upper dermal infiltrate of lymphocytes and other
inflammatory cells, with no grenz zone, is present. • Epidermotropism of mononuclear cells occurs. • When a clear halo surrounds an intraepidermal mononuclear cell
singly or in clumps, this is called a Pautrier microabscess. Its presence is suggestive of MF, but it is not necessary for diagnosis.
• Little spongiosis of the epidermis is found. • Lymphocytes have nuclei that are hyperchromatic and
convoluted or cerebriform.




tx• Pts with limited patch/plaque stage dx: topical corticosteroids• Topical mechlorethamine (nitrogen mustard) & carmustine
(BCNU) effective in early stage• Nitrogen mustard, either dissolved in complete water or used
as an ointment-based preparation results in complete remission in approx. 60-80% of pts with stage IA-B
• Tx with BCNU has similar remission rate• Total skin electron beam irradiation (TSEB) with energy of 4-
6 MeV is highly effective in pts with skin-limited MF• Total dose is 36 Gy administered in fractions over8-10 weeks

• TSEB is most effective in pts with stage IA-B with complete response rates of over 80%
• Most centers incorporate TSEB with PUVA or topical chemo• Local radiotherapy with X-ray or preferably electron beam for single tumors
in pts with plaque stage• Several types of phototherapy can be used: UVA irradiation following
photosensitization with 8-methoxypsoralen (PUVA), broad-band & narrow-band UVB & UVA-1 therapy(new therapies-unsure of how they compare with first 2)
• ECP may be effective in pts with SS• Systemic chem: used in pts with unequivocal lymph node or visceral
involvement or progressive skin tumors• CHOP;80-90% response-but response short

• Biologic response modifiers: aimed at potentiating the host’s immune response to neoplastic cells
• These are: cytokines, retinoids, immunotoxins & vaccination therapy• BRM are most effective when combined with (or preceded by)
traditional therapies• Interferon alpha (most common BRM) response rate 50% with 17%
experiencing complete remissions• Retinoids like isotretinoin, etretinate & acitretin A a novel RXR-
selective retinoid (bexarotene) used as single agents are roughly comparable to IFN-alpha
• Combination of retinoids + PUVA (RePUVA) shows a response similar to PUVA alone-but less tx & lower UVA dose cumulatively

• New immunomodulatory therapies in MF are: receptor targeted cytotoxic fusion proteins (DAB389IL2; denileukin difitox), cytokines (IL-12) & various vaccination stragegies
• DAB389IL12 is a fusion protein, in which diphtheria toxin is linked to IL-2
• It binds to the high affinity IL-2 receptor expressed by neoplastic T cells in MF
• Result is inhibition of protein synthesis & apoptosis• Overall & complete response rates are 30% & 10% respectively• Vaccination with peptides or peptide-loaded dendritic cell is
currently under investigation








Variants of MF
• Apart from classical Alibert-Bazin type of MF, many clinical variants reported
• Bullous & hyper-or hypopigmented MF have clinical behavior like MF
• In contrast follicular MF, pagetoid reticulosis & granulomatous slack skin have distinctive clinicopathologic features


Follicular MF• AKA:Mf-associated follicular mucinosis• Folliculocentric or pilotropic MF• Variant found in 10% of MF pts;mostly in adults;men>women• Pt presents with (grouped) follicular papules, acneiform
lesions, indurated plaques & sometimes tumors• Mostly on head & neck area• Skin lesions may be associated with alopecia• Infiltrated papules in eyebrow region are common • Pruritus more common then MF;secondary bacterial
infections may be present

Pagetoid Reticulosis
• AKA:Localized epidermotropic reticulosis• Woringer-Kolopp disease• Acral mycoses fungoides• Unilesional MF• Mycosis fungoides palmaris et plantaris

Pagetoid Reticulosis
• 0.6% of all MF cases• Woringer-Kolopp variant: localized type• Ketron-Goodman variant: disseminated• Long duration without progression to frank lymphoma is
the clinical hallmark of Woringer-Kolopp• Ketron-Goodman type is a manifestation of aggressive
CD-8+epidermotropic CTCL or of classical tumor stage MF
• TOC: local excision or radiation therapy maybe curative.

Clinical features
• Solitary psoriasiform or hyperkeratotic patch or plaque
• Usually localized to an extremity• Slowly progressive• Extra-cutaneous dissemination or disease-
related deaths have not been reported (in contrast to MF)

Pathology
• Hyperplastic epidermis with marked infiltration by large atypical pagetoid cells, singly or arranged in nests or clusters
• Atypical cells have medium-sized or large, sometimes hyperchromic & cerebriform nuclei and abundant, vacuolated cytoplasm
• Superficial dermis may have an infiltrate of mostly small lymphocytes, but rarely contains neoplastic T cells

• Pagetoid reticulosis: solitary plaque
• Purely intraepidermal proliferation

Scattered plaque-like lesions on both lower extremities.Ketron-Goodman disease

Band-like infiltration of lymphoid cells in lower epidermis and upper dermis. Intra-epidermal infiltrate were medium- to large-sized atypical cells. Lymphoid cells infiltrating upper dermis revealed no overt atypia

Granulomatous Slack Skin
• Extraordinarily rare type of CTCL• Characterized by slow development of folds of lax skin
& a granulomatous infiltrate• Affects adolescents & adults• Characterized by pendulous lax skin• Predilection for axillae & groin• 1/3 of reported pts had an association with Hodgkin’s dx• An association with classical MF has also been
described

• Pendulous fold of atrophic lax skin in the right inguinal area


Pathology & tx
• Dense granulomatous dermal infiltrates containing atypical T cells with cerebriform nuclei, macrophages & often many multinucleated giant cells
• Destruction of elastic tissue & elastophagocytosis by multinucleated cells
• Epidermis is infiltrated by small atypical T cells with cerebriform nuclei, as in classical MF
• Atypical T cells have a CD3+, CD4+, CD8+ phenotype• Radiotherapy may be effective; rapid recurrences after
surgical excision have been reported

Sezary Syndrome
• Leukemic phase of mycosis fungoides• Generalized erythroderma, superficial
lymphadenopathy, atypical cells in circulating blood
• Erythroderma from onset with leonine facies, eyelid edema, ectropion, alopecia, palm and sole hyperkeratosis
• Pruritis, burning, chill and profuse sweating

definition
• Historically traid defines it: erythroderma, generalized lymphadenopathy, & neoplastic T cells (Sezary cells) in skin, lymph nodes & peripheral blood
• No consensus on diagnositc criteria

• Electron photomicrograph of a skin a skin bx showing characteristic Sezary cells

Clinical features• Erythroderma, which may be associated with marked exfoliation,
edema, & lichenification• It is intensely pruritic• Lymphadenopathy, alopecia, onychodystrophy, & palmoplantar
hyperkeratosis are common• Overt clinical picture may be preceeded by by non-diagnostic
dermatits• Bone marrow may contain neoplastic cells, but real replacement of
bone marrow tissue is rare• Poor prognosis: 10-20% survival• Most pts die of opportunistic infections due to immunosuppression





tx• Being a systemic dx(leukemia) by definition systemic tx is
required• Prolonged tx with combination of low-dose chlorambucil &
prednisone, or with methotrexate is often effective in controlling dx• CHOP or CHOP-like regimens may produce higher response
rates, these responses are short-lived• ECP, either alone or in combination with other tx modalities has
been suggested as toc in SS & erythrodermic MF-response rate of 30-80%; complete response in 14-25%
• There are no controlled randomized trials showing ECP superiority over traditional low-dose chemo

Primary Cutaneous CD30-Positive Lymphoproliferative Disorders
• Second most common group of CTCL• Accounts for approx. 30% of CTCL• Includes primary cutaneous CD30-positive
large T-cell lymphoma, lymphomatoid papulosis (LyP), & borderline cases



Lymphomatoid Papulosis• LyP has a chronic indolent course in most patients; • estimates indicate that as many as 10-20% of LyP patients have
a history of associated malignant lymphoma (ALCL, HD, or mycosis fungoides [MF]) prior to, concurrent with, or subsequent to the diagnosis of LyP.
• Race: Black persons may be less affected than other racial groups.
• Sex: No consistent sex predominance is found in studies. • Age: LyP may develop at any age, usually in the third to fourth
decade
Lymphomatoid Papulosis
• Chronic, recurrent, self-healing papulonecrotic or papulonodular skin dx with histo features suggestive of a CD30+ malignant lymphoma
• Introduced by Macuaulay in 1968-still unclear whether maligant. Premalignant, or benign
• Should probably be regarded as a low-grade malignant CTCL• Etiology unknown; ?viral• Accounts for 185 approx of all CTCL• Youngest pt affected was 18 months-oldest 84; average age
35-45 yrs; male to female ratio: 1.5:1

LP• Typical lesions are red-brown papules & nodules that may develop
central hemorrhage, necrosis, & crusting & spontaneously disappear within 3-8 weeks
• Characteristically, skin lesions in different stages of evolution coexist• Papulonodules may leave transient hypopigmented or hyperpigmented
macules & superficial atrophic(varioliform) scars or disappear completely
• Predominant sites are trunk & limbs• In up to 20% of pts LyP may be preceded by, asssociated with , or
followed by another type of malignant lymphoma-generally MF or a CD30+ large cell or Hodgkin’s dx
• Usually prognosis is excellent

LyP-pathology
• Variable , extremely; 3 histologic types of LyP described:A,B, & C• Type A: Characterized by large (25-40 mm) CD30+ atypical cells with
polymorphic convoluted nuclei and a minimum of 1 prominent nucleolus. These large cells resemble Reed-Sternberg cells when binucleate. Type A LyP is the most common histologic variant.
• Type B: Characterized by smaller (8-15 mm) atypical cells with hyperchromatic cerebriform nuclei resembling the atypical lymphocytes in MF. CD30+ large cells are rare, but epidermotropism is more common in this variant.
• Type C: Characterized by monotonous population or large clusters of large CD30+large cell lymphomas
LyP-Tx
• Unsatisfactory• Topical or systemic corticosteroids or antibiotics are
ineffective• Aggressive txs like systemic chemo or total electron
beam irradiation may produce complete remissions but lesions reappear
• In pts with few lesions non-scarring-no tx• In cosmetically disturbing lesions:low-dose oral
methotrexate is most effective therapy for reducing lesion numbers
Lymphomatoid Papulosis
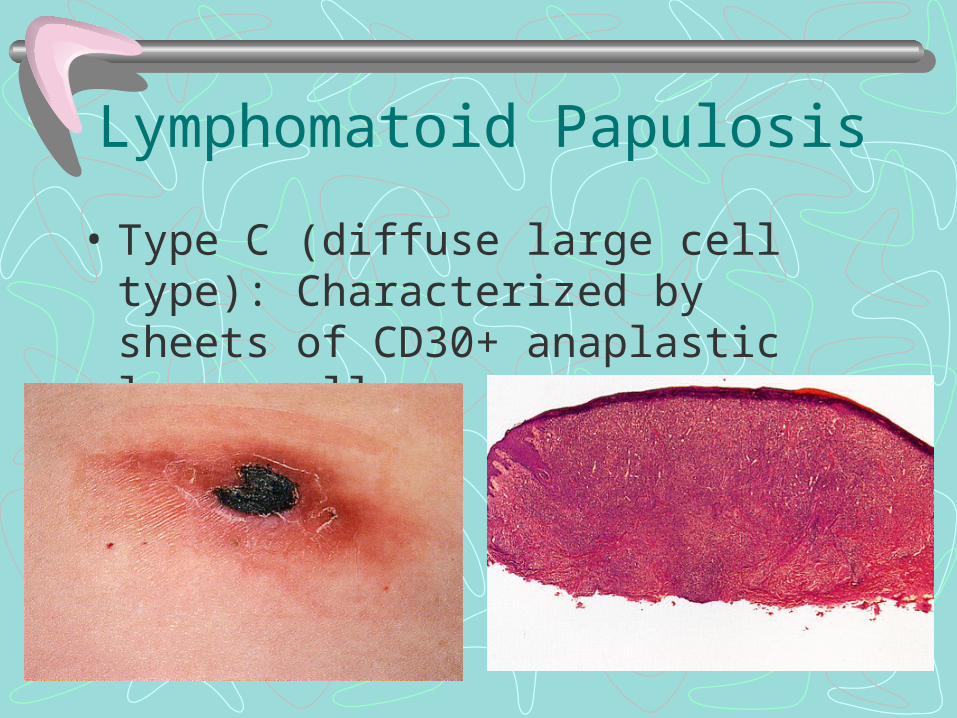
• Type C (diffuse large cell type): Characterized by sheets of CD30+ anaplastic large cells

• Clinical presentation with papulo-necrotic skin lesions at different stages of evolution
• Detail of dermal infiltrate showing mixed inflammatory infiltrate with scattered (CD30-pos) large anaplastic cells (LyP, type A)

• Lymphomatoid papulosis: high power-infiltrate is heterogeneous & includes neutrophils & eos & small lymphocytes & few large anaplastic cells

• Lymphomatoid papulosis:high. CD30 immunostain-few large neoplastic CD30+cells-in contrast to anaplastic large cell lymphoma do not form large sheets or nodular clusters
Treatment of LyP• Mid-to-high potency topical steroids to hasten resolution. • Low-dose weekly methotrexate is a safe and effective treatment
for suppressing LyP; however, the disease recurs within 1-2 weeks after ending medication.
• Oral psoralen plus UV-A phototherapy (PUVA) also effectively treats and suppresses the disease.
• carmustine, topical nitrogen mustard, intralesional interferon, low-dose cyclophosphamide, chlorambucil, and dapsone help disease suppression.


Primary CTCL other than Mycosis Fungoides
• CD30-positive cutaneous T-Cell Lymphoma • Secondary Cutaneous CD30 positive large-cell
lymphoma • Non-MF CD30-negative cutaneous large T-cell
lymphoma • Non-MF CD30-negative cutaneous pleomorphic small
or medium sized cell lymphoma • Subcutaneous (Panniculitis-Like) T-Cell Lymphoma• Nasal/Nasal Type T/NK Cell Lymphoma

CD30-positive cutaneous T-Cell Lymphoma
• Consist of large tumor cells, most expressing the CD30 antigen
• No history of LyP, MF, or CTCL’s• Present as solitary or localized skin lesions with tendency to
ulcerate and have spontaneous regression• Rare in children, occur more frequently in males• 5 year survival rate 90%• Highly responsive to radiotherapy• Lesions can be surgically excised
Primary Cutaneous CD30 + Large T-cell lymphoma
• Histologically show diffuse non-epidermotropic infiltrates with cohesive sheets of large CD30 + tumor cells
• Mostly having morphologically of anaplastic cells, with round, oval, or irregularly shaped nuclei, prominent (eosinophilic) nucleoli & abundant cytoplasm
• The t(2;5) translocation is predominantly found in children with systemic CD30+ anaplastic lymphoma is not found
• Tx:radiotherapy for few localized nodules or tumors• Debatable whether tx with doxorubicin & multi-agent chemo
agents should be done; skin relapses after CHOP are common & spontaneous regression may occur

Primary Cutaneous CD30+Lymphoma
• Best tx is radiation or low-dose methotrexate (few lesions)
• Multi-agent chemo (those with extracutaneous dx)

• Characteristic clinical presentation with a solitary ulcerating tumor; dermal infiltrate with cohesive clusters of large(CD30+) anaplastic cells with pronounced eosinophilic nucleoli & abundant cytoplasm

Non-MF CD 30 Negative Cutaneous Large T-Cell lymphoma
• CD30-neg large neoplastic cells without prior or concurrent MF
• Differentiation from small/medium sized pleomorphic CTCL is based on presence of >30% large pleomorphic T cells
• May present with solitary or localized nodules or tumors; more commonly present with generalized lesions
• Prognosis is poor: overall 15% 5- year survival• No difference in survival between cases of CD3+,
CD4+,, CD8- & cases of CD3+, CD4+, CD8 +phenotype

• Rapidly growing nodules & tumors. No patches present, rather deep plaques present for 2 weeks
CD30-neg Cutaneous Large Cell Lymphoma
• Pathology: nodular or diffuse infiltrates with variable numbers of medium-sized-large pleomorphic or immunoblasic-like T cells
• Cells represent at least 30% of total tumor cell population• Must be differentiated from CD30+ LTCL, CD56+ blastic
NK-cell lymphomas• Absence of prior or concurrent patches & plaques is a
decisive criterion• Tx:multi-agent chemo;only pts with localized or solitary dx
may radiotherapy considered as initial tx
Non-MF CD 30 Negative Cutaneous Small or Medium Size Cell T-Cell lymphoma
• Differentiate from large-cell type by having less than 30% large pleomorphic cell.
• Similar to large type clinically• Prognosis is better than large cell type. 50% 5 year
survival.• Radiation tx or surgical excision for solitary localized
skin lesions; interferon alfa, or cyclophosphamide are effective in more generalized dx

Large cell anaplastic lymphoma
• Cells are large with hyperchromic nuclei;bizzare forms & mitotic figures seen

Large cell anaplastic lymphoma
• Medium power: dense sheets of atypical cells admixed with inflammatory cells, freq. Eos
• A number of atypical cells show more than 1 nucleus

Cutaneous anaplastic large cell lymphoma
• Low power: dense infiltrate occupying entire dermis
• Associated ulceration of epidermis

Subcutaneous (Panniculitis-Like) T-Cell Lymphoma
• Clinically presents with subcutaneous nodules• Usually on lower extremities• Frequently diagnosed as having erythema nodosum or
other forms of panniculitis• Systemic symptoms like fever, fatigue, & wt. Loss may
occur• May be complicated by hemophagocytic syndrome-
rapidly progressive• Cases with TCRgamma/epsilon+phenotype have worse
prognosis than TCRalpha/beta+

A, Marked edema of right calf at time of presentation. B, Erythematous nodules with associated vascular ectasia on abdominal wall.

Subcutaneous Panniculitis-Like T-Cell Lymphoma
• Pathology: subcutaneous infiltrate simulate pannicultis-with mixture of neoplastic pleomorphic T cells of various sizes & often many macrophages
• Overlying epidermis & dermis are typically uninvolved• Rimming of individual fat cells by neoplastic T cells is a
diagnostic feature• Tx:early stage: systemic corticosteroids• However pts with a hemophagocytic syndrome
prognosis is poor despite aggressive multiagent chemo

Subcutaneous Panniculitis-Like T-Cell Lymphoma
• Subcutaneous infiltrate with characteristic rimming of individual fat cells by the neoplastic T cells

High-power view of infiltrate showing random atypical lymphocytes

Cutaneous B-Cell Lymphoma-types:
• Primary Cutaneous Follicular Center Cell Lymphoma
• Primary Cutaneous Immunocytoma/Marginal Zone Lymphoma
• Intravascluar Large B-Cell Lymphoma• Primary Cutaneous Plasmacytoma

B-cell lymphomas of the skin
• Aka Cutaneous B-cell lymphoma & SALT-related B-cell lymphoma
• Group of malignant lymphomas whose primary site is the skin
• Derived from B lymphocytes in different stages of differentiation
• Skin can be the site of secondary involvement by extracutaneous (usually nodal) B-cell lymphomas
• Most are low-grade malignancies, indolent behavior & good prognosis

• Immunohistochemical & molecular genetic techniques show that previously classified cases of B-cell pseudolymphomas represent low-grade malignant B-cell lymphomas of the skin
• Precise classification can be achieved after complete synthesis of clinical, histopathologic, immunophenotypic, & molecular features done
• Terminology is not uniform & varies depending on medical center
• Most cases tx consists of local radiotherapy; in case of 1-2 lesions sx excision is an option; systemic chemotherapy is needed in a small proportion of pts

Classification
• EORTC classification divides into 3 major types & 2 provisional categories
1. Follicle center cell lymphoma2. Immunocytoma/marginal zone lymphoma3. Large B-cell lymphoma of the legProvisional categories:1. Plasmacytoma2. Intravascular large cell B-cell lymphoma


Nomenclature
• In EORTC classification primary cutaneous lymphoma was defined as ‘presence of dx limited to the skin for at least 6 months after complete staging
• Bolognia believes definition should read:malignant lymphomas confined to skin at presentation, based on 2 arguments:
• A. aggressive lymphomas arising within skin may disseminate prior to 6 months
• B. pts need to be tx at time of presentation & therefore dx is needed then not 6 months later

Primary Cutaneous Follicular Center Cell Lymphoma
• AKA B-Cell lymphoma of follicular center cell origin• AKA Reticulohistiocytoma of the dorsum/Crosti’s lymphoma• Neoplastic proliferation of germinal center cells confined to skin• Common subtype• Multiple papules, plaques nodules in one anatomic region
surrounded by patches of erythema• Ulceration is common• Usually asymptomatic-LDH is normal• 2/3 of case on the trunk, 1/5 on the head and neck• 15% on the leg

Primary Cutaneous Follicular Center Cell Lymphoma
• M:F = 2:1• Prognosis: Head and neck 100% 5 yr surv.; Leg
lesion of people over 70, 50% 5 yr surv.• Recurrences seen in up to 50%, dissemination
to lymph nodes or internal organs is rare• Stains with B-Cell marker CD 20, monotypic for
immunoglobulin production of kappa or lambda chain, not both

Cutaneous follicle center cell lymphoma: large ulcerated tumors on the scalp surrounded by infiltrated erythematous nodules & plaques

• Cutaneous follicle center cell lymphoma:large ulcerated tumor on the back
• Note surrounding erythematous papules, patches & plaques

Cutaneous lymphoma
• 57-yr-old woman with B-cell lymphoma developed asymptomatic erythematous-lavender plaques & tumors on face & scalp




Cutaneous follicular B-cell lymphoma
• Low: multinodular pattern seen-lymphomatous infiltrate situated at dermal-subcutaneous junction-composed of small cleaved follicular center cells arranged as coalescing follicles

Cutaneous follicular B-cell lymphoma
• Medium: absence of tingible-body macrophages
Cutaneous B-cell lymphoma
• Studies should be performed are: CBC, CMP, BMBx, CT of chest, abdomen, & pelvis
• Flow cytometry of peripheral blood & bone marrow are optional-can be helpful in low-grade lymphomas
• Gallium scans are being replaced by PET scans

Cutaneous diffuse B-cell lymphoma
• High:cytologically atypical lymphoid cells admixed with nuclear fragments

Cutaneous diffuse B-cell lymphoma
• High: not all cells are large & atypical
• In this example cells are small, hyperchromic, & monotonous in appearance

• Cutaneous diffuse B-cell lymphoma(low): dense dermal infiltrate of basophilic cells not involving overlying epidermis
• Typically, B-cell lymphoma has a bottom heavy infiltrate-a significant portion of infiltrate involves lower dermis
• Medium: dermal infiltrate may be nodular & cells permeate between bundles of reticular dermis

• Cuatneous immunocytoma: domeshaped erythematous nodule with smooth surface
• Surrounding area shows features of acrodermatitis chronica atrophicans

Primary Cutaneous Immunocytoma
• Proliferation of small lymphocytes, lymphoplasmacytoid cells & plasma cells with monotypic intracytoplasmic immunoglobulins
• Primary cutaneous immunocytoma differs from nodal cutaneous immunocytoma b/c pts do not show features of Waldenstrom’s macroglobulinemia & have an excellent response to tx
• Some consider cutaneous immunocytoma & cutaneous MZL to be a single entity

• Pts present with solitary or grouped erythematous-red-brown plaques or dome-shaped tumors
• Favors lower extremity• Generalized lesions are rare & called miliary type of cutaneous
immunocytoma• Sometimes resolution of lesions causes secondary anetoderma due to
loss of elastic fibers• Can arise from areas of acrodermatitis chronica atrophicans & may be
linked to Borrelia spp.• More frequently linked to B-cell lymphoma• Skin lesions asymptomatic;& no B- symptoms;normal LDH• Excellent prognosis; although local recurrence may occur

Clinical features
• Present with solitary or grouped erythematous to red-brown plaques or dome-shaped tumors favoring lower extremities
• Generalized lesions are rare• Sometimes resolution results in secondary anetoderma-
due to loss of elastic fibers in area of tumor infiltrate• May arise in areas affected by acrodermatitis chronica
atrophicans-may be linked to infection by Borrelia spp.• Serum LDH levels are usually normal• Prognosis is excellent recurrences

Cutaneous Marginal Zone Lymphoma
• Variant of low-grade malignant primary cutaneous B-cell lymphoma
• Closely related to immunocytoma & MALT-lymphomas• Terminology is inconsistent in different centers• Lesions designated in past as cutaneous atypical
lymphoid hyperplasia with monotypic plasma cells probably represent examples of cutaneous marginal zone lymphoma

Cutaneous Marginal Zone Lymphoma
• Pts present with recurrent red-brown papules, plaques, & nodules
• Localized preferentially to upper extremities or trunk
• Generalized lesions may be seen rarely• Ulceration rarely, if ever occurs; usually
asymptomatic, & no B symptoms, normal LDH• Prognosis : excellent

• Solitary erythematous nodule on upper arm

• Multiple, erythematous papules on the arm


Intravascular Large Cell B-Cell Lymphoma of the Skin
• Malignant proliferation of large B-lymphocytes within blood vessels
• Formerly known as malignant angioendotheliomatosis• Renamed peculiar variant of non-Hodgkin’s lymphoma• Rare to have only skin involvement;usually systemic
dissemination including CNS at onset• Pts present with indurated, erythematous or violaceous patches
& plaques• Preferentially located on back & trunk & thighs• Clinical appearance not typical of lymphoma-more like purpura or
panniculitis

Large erythematous tumor on scalp of an 11-month-old child

B-Lymphoblastic Lymphoma• Malignant proliferations of precursor B lymphocytes• Rare to have skin as primary site• All pts should be classified with, tx for systemic dx-even in
absence of systemic dx at dx• In contrast to other B-cell lymphomas shows predilection for
children & young adults• Pts present with solitary large erythematous tumors • Commonly on head & neck• Pts with primary dx have asymptomatic skin lesions of a few
weeks duration• Those with secondary skin lesions are ill: B-symptoms


Large B-Cell Lymphoma of the Leg
• LBCLL has large cell morphology & intermediate prognosis• Occurs almost exclusively in elderly pts, predominantly
women• Pt presents with solitary or clustered erythematous or red-
brown nodules• Located on distal aspect of one leg, lesions may arise on
both legs too• Ulceration is common• Tumors with similar morphology & phenotypia can arise in
areas other than legs

Large B-Cell Lymphoma of the Leg• Prognosis is less favorable than other cutaneous B-cell
lymphomas• 5-yr survival is 50% approx.• 3 prognostic variables were independent predictors of
behavior:1.) morphology of infiltrate-predominantly large cells worse than
predominantly large cleaved cells2.) # of lesions at presentation-pts with more have worse
prognosis3.) location on legs-pts presenting with lesions on the legs have
worse prognosis

Cutaneous Plasmacytoma• Characterized by a clonal proliferation of plasma cells primarily affecting
the skin• No bone marrow involvement• Exceedingly rare• Its existence called into question ? Some cases may be MZL arising in
different organs• Occurs most commonly in elderly men• Pt presents with solitary, clusteredor rarely, generalized erythematous,
red-brown or violaceous cutaneous/subcutaneous plaques or tumors• Predilection for head & neck• Amyloid deposition is rare & serum & urine monoclonal protein neg

Cutaneous Plasmacytoma
• Prognosis is controversial• Prognosis is probably related to tumor burden & pts with
small solitary lesions have very good prognosis• Development of multiple myeloma & systemic soft-
tissue mets have been seen in some• As with other pts with non-cutaneous plasmacytomas
they should undergo an evalution for systemic dx : bone marrow bx/aspirate, protein electrophoresis, & serum & urine immunofixation



• Cutaneous marginal zone B-cell lymphoma:
• Top: small nodules of reactive lymphocytes(dark areas) surrounded by neoplastic marginal zone cells, lymphoplasmactoid cells, & plasma cells(clear areas)
• Bottom: monotypic expression






tx• Selected after exact classification found• After analysis of staging investigations• Overall condition of pt• Pts with secondary cutaneous lesions of extra-cutaneous B-
cell lymphoma should be tx by oncology –not dermatology• Many pts with low-grade malignant primary lymphoma can
be managed conservatively with watchful-waiting strategy• F/u for these pts should be q 6 months or at onset of new
lesions/or symptoms

• Most pts with low-grade B-cell lymphomas: FCCL,MZL, cutaneous immunocytoma- & who have solitary or few lesions can be tx with local radiotherapy, or sx excision followed by radiotherapy or surgical field
• Wide margins-10-20cm beyond clinically apparent lesions have fewer recurrences
• This is especially good for Crosti’s lymphoma• Surgical excision with narrow margins is valuable for pts with solitary well-
circumscribed lesions• Recently few reports have appeared tx low-grade primary cutaneous B-cell
lymphomas with antibiotics-achieving resolution in a percentage of pts• This type of tx is conceptually analogous to that of Helicobacter pylori-
associated MALT lymphomas of the stomach-which if caught early can be cured with antib’s

• Another tx for low-grade malignant primary cutaneous B-cell lymphoma is subcutaneous intralesional interferon-in particular interferon alfa-2a
• Complete resolution in 50% of pts• Good for pts with multiple lesions at different body sites-radiotherapy
difficult• Intralesional antiCD20 monclonal antibody (Rituximab) has been used
to induce tumor reduction in pts with indolent primary CBL-response rate was better with IV
• Next generation anti-CD20 monoclonal antibodies will be attached to 131 I or yttrium-being able to then tumor target & ‘radiotherapy’
• Pts with disseminated lesions of diffuse FCCL or large B-cell lymphoma need systemic chemo-CHOP

• Intravascular large B-cell lymphoma TOC is systemic chemo-regardless of staging
• Pts with B-cell lymphoblastic lymphoma should be tx by hematology, aggressive chemo needed & BMT discussed
• Cutaneous plasmocytomas can be tx with local radiotherapy
• Systemic chemo reserved for pts with advanced dx• Neg staging is mandatory before tx of pts with
cuatneous plasmocytomas