Cutaneous Lupus Erythematosus - American Academy of ... F063... · ©2016 MFMER | 3507536-1...
73
©2016 MFMER | 3507536-1 Cutaneous Lupus Erythematosus Diagnosis, Classification, and Screening for Systemic Disease David A. Wetter, M.D. Professor of Dermatology, Mayo Clinic (Rochester, MN) Cutaneous Lupus and Dermatomyositis Management Pearls and Pitfalls for the General Dermatologist, Forum Session (F063) American Academy of Dermatology, Annual Meeting, Orlando, Florida, March 4, 2017
Transcript of Cutaneous Lupus Erythematosus - American Academy of ... F063... · ©2016 MFMER | 3507536-1...

©2016 MFMER | 3507536-1
Cutaneous Lupus Erythematosus Diagnosis, Classification, and Screening for Systemic Disease
David A. Wetter, M.D. Professor of Dermatology, Mayo Clinic (Rochester, MN)
Cutaneous Lupus and Dermatomyositis Management Pearls and Pitfalls for the General Dermatologist, Forum Session (F063)
American Academy of Dermatology, Annual Meeting,
Orlando, Florida, March 4, 2017

©2016 MFMER | 3507536-2
Disclosure
• I have no conflicts of interest
• Off-label use of systemic medications will be discussed

©2016 MFMER | 3507536-3
The scenario and
clinical conundrum…

©2016 MFMER | 3507536-4
A 36 year-old woman has this generalized eruption of the head, arms, and upper trunk. You are suspicious that this patient has discoid lupus.
1. What are the clinical and microscopic features that can help confirm the diagnosis of cutaneous lupus?
2. How should a patient be
• Initially evaluated for the presence of systemic involvement
• Monitored over time for the presence of systemic involvement

©2016 MFMER | 3507536-5
Overview
• How to diagnose cutaneous lupus
• How to classify the various subtypes of cutaneous lupus
• How to evaluate patients with cutaneous lupus for the possibility of systemic lupus (both at baseline and over time)

©2016 MFMER | 3507536-6
The Incidence of Cutaneous Lupus is
1. Greater than systemic lupus
2. The same as systemic lupus
3. Less than systemic lupus

©2016 MFMER | 3507536-7
Incidence Rate of Cutaneous Lupus is 4.30 per 100,000
Cutaneous lupus
is as common
as SLE

©2016 MFMER | 3507536-8
Incidence of Cutaneous Lupus is 3 Times Higher Than Systemic Lupus in Men

©2016 MFMER | 3507536-9
Which of the Following is an Example of Lupus Erythematosus-Specific Skin Disease?
1. Calcinosis cutis
2. Chilblain lupus
3. Leukocytoclastic vasculitis
4. Livedo reticularis
5. Periungual telangiectasia

©2016 MFMER | 3507536-10
Costner MI and Sontheimer RD
Do not show
characteristic
histopathology
of lupus and can
be seen in other
diseases Show characteristic histopathologic changes of lupus
erythematosus (e.g. interface dermatitis)

©2016 MFMER | 3507536-11
What are the typical clinical
findings of cutaneous lupus?

©2016 MFMER | 3507536-12
ACTIVITY: Erythema, scale/hypertrophy
DAMAGE: Dyspigmentation, scarring, atrophy
*Can help determine
1. How active disease is at time of evaluation (and thus influence your treatment approach)
2. Response to your treatment at follow-up
Arch Dermatol 147(2):203, 2011

©2016 MFMER | 3507536-13
• Note presence of both ACTIVITY (erythema, scale) and DAMAGE (dyspigmentation, scarring) in this patient with discoid lupus

©2016 MFMER | 3507536-14
A few examples of
lupus-specific skin disease…

©2016 MFMER | 3507536-15
Localized acute cutaneous lupus (“malar rash”)
Note:
1. Sparing of nasolabial fold
2. Involvement of malar cheeks extending over nasal dorsum (“butterfly rash”)

©2016 MFMER | 3507536-16
Patient had generalized DLE and
although had 4/11 ACR criteria
(discoid rash, oral ulcers,
photosensitivity, positive ANA), she
did not have clinically relevant SLE
(per rheumatologic evaluation)
Mucosal (oral)
discoid lupus (DLE)

©2016 MFMER | 3507536-17
Hypertrophic/verrucous DLE

©2016 MFMER | 3507536-18
Note violaceous
erythema and
swelling of 2nd toe
Chilblain lupus in setting of
systemic lupus (SLE)

©2016 MFMER | 3507536-19
Cutis 54(6):395, 1994
“Definite” chilblains lupus
requires fulfilling BOTH
major criteria and at least
one of the minor criteria

©2016 MFMER | 3507536-20
Proposed Diagnostic Criteria of Pernio
Major criteria
• Localized erythema and swelling
involving acral sites and persistent for
>24 h
Minor criteria
• Onset and/or worsening in cooler months
(between November and March)
• Histopathologic findings of skin biopsy
consistent with pernio (eg, dermal edema
with superficial and deep perivascular
lymphocytic infiltrate) and without findings
of lupus erythematosus
• Response to conservative treatments
(ie, warming and drying of affected areas)
Pernio (chilblains) – DIFFERENT entity
than chilblain lupus

©2016 MFMER | 3507536-21
Lupus panniculitis

©2016 MFMER | 3507536-22
Which of the following conditions can closely mimic lupus panniculitis both clinically and microscopically?
1. Deep morphea
2. Erythema nodosum
3. Lymphoma
4. Nodular vasculitis
5. Pancreatic panniculitis

©2016 MFMER | 3507536-23
Lupus panniculitis
and subcutaneous
panniculitis-like T-cell
lymphoma (SPTCL)
can present very
similarly both
clinically and
histopathologically

©2016 MFMER | 3507536-24
A few examples of
lupus-nonspecific skin disease...

©2016 MFMER | 3507536-25
Gutierrez Jr. and Wetter: Dermatologic Therapy 25:195, 2012
Ulcerations with focal extrusion of
chalky granules because of calcinosis
cutis in a patient with system lupus
erythematosus
Calcinosis cutis
(in a patient with SLE)

©2016 MFMER | 3507536-26

©2016 MFMER | 3507536-27
Underlying ACTD Female sex Male sex Total
Age at onset of calcinosis
cutis, mean (range), y
Time to onset of calcinosis cutis after
diagnosis of ACTD, mean (range), mo
Dermatomyositis 23 (77) 7 (23) 30 (38) 31 (4-75) 65 (3-216)
Classic 11 (73) 4 (27) 15 (19) 48 (21-75) 94 (12-216)
Amyopathic 1 (100) 0 1 (1) 52 72
Juvenile 11 (79) 3 (21) 14 (18) 10 (4-21) 35 (3-84)
Systemic sclerosis with limited
cutaneous scleroderma 21 (88) 3 (13) 24 (31) 54 (28-73) 90 (0-372)
Overlap CTD 5 (83) 1 (17) 6 (8) 39 (14-55) 128 (2-312)
Undifferentiated CTD 5 (83) 1 (17) 6 (8) 51 (31-67) 32 (0-84)
Lupus panniculitis 4 (100) 0 4 (5) 60 (39-74) 58 (5-108)
Mixed CTD 2 (50) 2 (50) 4 (5) 50 (39-62) 75 (12-92)
SLE 2 (100) 0 2 (3) 46 (35-57) 258 (228-288)
RA 1 (100) 0 1 (1) 29 24
Polymyositis 1 (100) 0 1 (1) 44 108
• Range of ACTD’s associated with calcinosis
• Dermatomyositis (38%)
• Systemic sclerosis with limited cutaneous scleroderma (31%)
• Lupus panniculitis (4 pts.), SLE (2 pts.)
Characteristics and Prevalence of ACTD Associated with Calcinosis Cutis Patients, No. (%) (n=78)

©2016 MFMER | 3507536-28
• Urticarial vasculitis
• Note “bruise-like” discoloration
• Can be associated with SLE –
particularly if associated with low
complement levels

©2016 MFMER | 3507536-29
Etiologies of Cutaneous Small Vessel Vasculitis
Chung et al: Dermatology, 2008, Ch. 25
Infection (15-20%)
Autoimmune connective tissue disease (15-20%)
Drug (10-15%)
Neoplasm (5%)
Idiopathic (45-55%)

©2016 MFMER | 3507536-30
What other conditions can
appear clinically similar to
cutaneous lupus?

©2016 MFMER | 3507536-31
Differential Diagnosis
Acute cutaneous lupus/malar rash
• Rosacea (including corticosteroid-induced)
• Seborrheic dermatitis (especially photosensitive form)
• Sunburn
• Drug induced photosensitivity (phototoxic and photoallergic)
• Dermatomyositis
• Erysipelas
• Pemphigus erythematosus
• Dermatitis, atopic, contact and photocontact
• Acne vulgaris (rarely)
Subacute cutaneous lupus
• Psoriasis
• Dermatophytosis, including tinea incognito
• Photolichenoid drug eruption
• Granuloma annulare
• Figurate erythemas (e.g. erythema annulare centrifugum)
• Dermatitis, atopic, contact and photocontact
• Permphigus foliaceus
Discoid lesions
• Facial discoid dermatosis
• Tinea faciei, tinea capitis, tinea corporis
• Lichen planus and lichen planopilaris
• Jessner’s lymphocytic infiltrate
• Polymorphous light eruption
• Sarcoidosis
• Lymphocytoma cutis
• Lymphoma cutis
• Granuloma faciale
• Dimorphic fungal infections, lupus vulgaris
• When single lesion, non-melanoma skin cancer
Tumid lupus lesions
• Jessner’s lymphocytic infiltrate
• Polymorphous light eruption
• Reticular erythematous mucinosis
Lupus panniculitis
• Other panniculitides
Lee and Werth: Dermatology, 2012, Ch. 41

©2016 MFMER | 3507536-32
What is the histopathology
of cutaneous lupus?

©2016 MFMER | 3507536-33
Low-Power Image Note Perivascular and Periadnexal Lymphocytic
Infiltrate as well as Follicular Plugging
Photo courtesy of Michael J. Camilleri, M.D. Mayo Clinic

©2016 MFMER | 3507536-34
Medium and High Power Images Note Interface Dermatitis With Basal Vacuolar Degeneration
Photo courtesy of Michael J. Camilleri, M.D. Mayo Clinic

©2016 MFMER | 3507536-35
Direct Immunofluorescence Microscopy (DIF)
• Photo highlights granular deposits of IgM along basement membrane zone
• “Lupus band” – continuous, strong, granular deposition of IgM, IgG, and complement (C3) along basement membrane zone
Photo courtesy of Michael J. Camilleri, M.D. Mayo Clinic

©2016 MFMER | 3507536-36
Which of the following is associated with worse disease in this patient with discoid lupus?
1. Alcohol use
2. Hepatitis C
3. Malignancy
4. Positive PPD
5. Smoking

©2016 MFMER | 3507536-37

©2016 MFMER | 3507536-38
Can medications be
associated with the onset
of cutaneous lupus?

©2016 MFMER | 3507536-39
Subacute Cutaneous Lupus Erythematosus (SCLE)

©2016 MFMER | 3507536-40
SCLE Note Photodistribution in Current and Previous Photo

©2016 MFMER | 3507536-41
Drug-Induced SCLE Drug-Induced SLE (Usually Does Not Have Skin Involvement)
Causes of Drug-Induced Lupus
Drug-induced SCLE
ACE inhibitors
Phenytoin
Hydroxychloroquine
Griseofulvin
Terbinafine
Tetracycline
Beta blockers
Calcium channel blockers
Tamoxifen
Docetaxel
Paclitaxel
Anastrozole
NSAIDS
Thiazide diuretics
Buproprion
Leflunomide
Proton Pump inhibitor
Anti-TNF biologics
Interferon-α
Drug-Induced SLE (typically without skin involvement)
Hydralazine
Isoniazid
Antihyperlipidemic agents
Minocycline
Procainamide
Anti-TNF biologics
Costner and Sontheimer: Dermatology in General Medicine, Ch. 155, 8th ed.

©2016 MFMER | 3507536-42
More than 1/3 of
SCLE cases could
be attributed to drug
exposure

©2016 MFMER | 3507536-43
What is already known about this topic?
• Eighteen cases of proton pump inhibitor (PPI)-induced cutaneous lupus erythematosus (CLE) have been reported in the literature since 2001
What does this study add?
• Nineteen new patients with 24 episodes of PPI-induced subacute CLE (SCLE) are reported
• Cross-reactivity between different PPIs is demonstrated
• Patients with previous CLE or other autoimmune diseases may be particularly prone to PPI-induced or exacerbated SCLE
• The diagnosis is challenged by the variation in time from prescription of the culprit drug to the appearance of SCLE
Sandholdt et al: British Journal of Dermatology 170:342, 2014

©2016 MFMER | 3507536-44

©2016 MFMER | 3507536-45
Antihypertensives 40 of 117 reported cases: 34.2%
Calcium channel blockers
Diltiazem 6 cases
Verapamil 5 cases
Nifedipine 3 cases
Nitrendipine 1 case
Diuretics
Hydrochorothiazide 10 cases
Hydrochlorothiazide + triamterene 3 cases
Chlorthiazide 2 cases
Beta blockers
Oxprenolol 4 cases
Acebutolol 1 case
Angiotensin-converting enzyme inhibitors
Enalapril 2 cases
Lisnopril 1 case
Captopril 1 case
Cilazapril 1 case
Antifungals 30 of 117 reported cases: 25.6%
Terbinafine 29 cases
Griseofulvin 1 case
Chemotherapeutics 10 of 117 reported cases: 8.5%
Docetaxel 3 cases
Paclitaxel 3 cases
Tamoxifen 2 cases
Capecitabine 2 cases
Antihistamines 9 of 117 reported cases: 7.7%
Ranitidine 7 cases
Brompheniramine 1 case
Cinnarizine + thiethylperazine 1 case
Immunomodulators 8 of 117 reported cases: 6.8%
Leflunomide 5 cases
Interferon α and β 3 cases
Antiepileptics 3 of 117 reported cases: 2.6%
Carbamazepine 2 cases
Phenytoin 1 case
Statins 3 of 117 reported cases: 2.6%
Simvastatin 2 cases
Pravastatin 1 case
Biologics 2 of 117 reported cases: 1.7%
Etanercept 2 cases
Efalizumab 1 case
Proton pump inhibitors 2 of 117 reported cases: 1.7%
Lansoprazole 2 cases
Nonsteroidal anti-inflammatory drugs 2 of 117 reported cases: 1.7%
Naproxen 1 case
Piroxicam 1 case
Hormone-altering drugs 2 of 117 reported cases: 1.7%
Leuprorelin 1 case
Anastrozole 1 case
Ultraviolet therapy 2 of 117 reported cases: 1.7%
PUVA 1 case
PUVA and UVB 1 case
Others 4 of 117 reported cases: 3.4%
Bupropion 1 case
Tiotropium 1 case
Ticlopidine 1 case
Hay with fertilizer 1 case
Answer: No (according to Lowe et al)

©2016 MFMER | 3507536-46
Approximately 80% of Patients With SCLE Will Have Positive Ro/SSA Antibodies (Does Not Differ Between Idiopathic and Drug-Induced Cases)
Ro/SS-A,
n/N (%)
La/SS-B
n/N (%)
Antinuclear
antibodies,
n/N (%)
Histone, n/N
(%)
Number reported
positive at
diagnosis
87/107 (81) 35/73 (48) 84/103 (82) 19/57 (33)
Number reported
positive after
resolution of rash
28/42 (67) 5/9 (56) 19/23 (83)
3/6 (50): in one
case antibody
appeared after
resolution
Autoantibodies in drug-induced subacute cutaneous lupus erythematosus
Ro/SS-A autoantibody rates were not significantly different between DI-SCLE and idiopathic SCLE

©2016 MFMER | 3507536-47

©2016 MFMER | 3507536-48
SLE criteria
ANA 14 (100) 57 (79)
Arthritis 13 (93) 22 (31)
Anti-dsDNA 10 (71) 52 (72)
Cutaneous features 4 (29) 48 (67)
Serositis 4 (29) 9 (12)
Hematologic disorder 4 (29) 16 (22)
Oral ulcers 4 (29) 3 (4)
Antiphospholipid antibodies 1 (7) 8 (11)
Renal disorder 0 (0) 5 (7)
Neurologic disorder 0 (0) 2 (3)
Anti-Smith antibodies 0 (0) 7 (10)
Other features
Hypocomplementemia 3 (21) 17%
Antihistone antibodies 3 (21) NA
Fever or general symptoms 11 (79) 23%
Number of SLE critieria fulfilled
≥4 9 (64) 37 (51)
3 3 (21) 17 (24)
1-2 2 (14) 18 (25)
Outcome
Improvement 13/13 (100) 71 (99)
Time to improvement (mo) 2.9 9.9
*High rate of arthritis and low rate of skin findings in our study
*Do not need to fulfill ACR criteria to have an important lupus-like syndrome (ACR criteria
developed more for clinical study classification, rather than establishing SLE diagnosis in
given patient [Cutaneous Manifestations of Rheumatic Diseases, 2nd ed.])

©2016 MFMER | 3507536-49
Which laboratory evaluations
should be performed in patients
with cutaneous lupus?

©2016 MFMER | 3507536-50
Clinically Relevant Information About Cutaneous Lupus Eythematosus
“The development of systemic disease in patients with what seems to be a strictly cutaneous disease at diagnosis has been highlighted in this issue of the Archives. What is needed is a clear statement of how to monitor patients for this possibility. Is there predictive value of obtaining immunoflurescence microscopic findings on patients at diagnosis? Should we be performing repeated serologic testing in our patients, or should we only follow patients with a careful clinical history along with complete blood cell counts and urinalyses?”
Callen: Arch Dermatol 145(3):316, 2009
How should patients with cutaneous lupus be monitored for
systemic disease at (1) time of diagnosis and (2) over time?
A CLEAR CONSENSUS DOES NOT YET EXIST

©2016 MFMER | 3507536-51
My Typical Workup for Cutaneous Lupus (CLE)
• Goal: confirm diagnosis and assess for systemic involvement
• Thorough review of systems (use ACR criteria as guide)
• Skin biopsy: H&E and lesional DIF (I personally find the H&E to be the most helpful)
• Basic labs: CBC, LFT’s, creatinine, inflammatory markers (ESR, CRP), urinalysis
• Autoimmune serologies, etc: ANA, ENA panel, dsDNA, complement (C3, C4, total), anti-phospholipid Abs (anti-cardiolipin, beta-2-glycoprotein-1, lupus anticoagulant)
• If considering systemic therapy: Eye exam (antimalarials), hepatitis serologies (methotrexate), thiopurine methyltransferase (TPMT; azathioprine)

©2016 MFMER | 3507536-52
Costner and Sontheimer

©2016 MFMER | 3507536-53
SLICC, 2012

©2016 MFMER | 3507536-54
SLICC (2012) criteria were
more sensitive than ACR
(1997) criteria in classifying
a patient as having SLE

©2016 MFMER | 3507536-55
How Do I Monitor Patients With (Clinically Quiescent/Stable) CLE Over Time?
• Chronic CLE (CCLE) [DLE most common subtype]
• Annual skin exam and review of systems
• Laboratory studies based on: skin findings, review of systems (and if any abnormal baseline labs at time of diagnosis that are more concerning for higher chance of progression to SLE)
• SCLE
• Annual skin exam and review of systems
• For first 1-2 years consider annual labs (CBC, Cr, ESR, urinalysis, ENA panel, dsDNA, complement levels); thereafter only if review of systems or skin exam concerning for SLE

©2016 MFMER | 3507536-56
In those with isolated discoid lupus, what is the risk of progression to systemic lupus over time?
1. 2%
2. 10%
3. 25%
4. 50%
5. 75%

©2016 MFMER | 3507536-57
• 13 of 129 patients (10.1%) with DLE progressed to SLE
• Mean time from cutaneous lupus diagnosis to progression to SLE was 8.2 years (this included all 19 [of 156 pts.] with cutaneous lupus that progressed to SLE)

©2016 MFMER | 3507536-58

©2016 MFMER | 3507536-59
Characteristic or Symptom CLE (n=64) SLE (n=13) P
Age, mean (SD), y 51.0 (14.3) 50.35 (14.80) 0.88
Time from CLE diagnosis to first visit, mean (SD), y 7.64 (8.52) 6.62 (6.10) 0.68
Follow-up time, mean (SD), y 2.33 (1.21) 2.81 (1.34) 0.20
No. of visits, median [range] 4 [2-12] 7 [2-13)
Female sex, No. (%) 44 (69) 12 (92) 0.10
White race/ethnicity, No. (%) 46 (72) 12 (92) 0.18
CCLE, No. (%) 45 (70) 8 (62) 0.53
Discoid localized 22 (34) 1 (8) 0.04
Discoid generalized 6 (9) 4 (31)
SCLE, No. (%) 19 (30) 5 (38) 0.53
Antibody test result, No. (%)
Negative baseline ANA titer 54 (84) 5 (38)
0.002 Baseline ANA titer, 1:80-1:160 3 (5) 4 (31)
Baseline ANA titer, 1:320-1:1280 7 (11) 4 (31)
Positive for anti-dsDNA 5 (8) 2 (15) 0.35
Positive for anti-Smith 0 1 (8) 0.17
Positive for anti-cardiolipin or lupus anticoagulant 3 2 (15) 0.20
Therapeutic agent, No. (%)
Topical or IL corticosteroid 18 (28) 2 (15) 0.50
Prednisone 6 (8) 1 (8) NA
Antimalarials or dapsone 49 (77) 7 (54) 0.17
Immunomodulators 4 (6) 1 (8) NA
Thalidomide 4 (6) 1 (8) NA
No. of ACR criteria at baseline, mean (SD) 1.62 (0.92) 2.38 (0.78) 0.007
Musculoskeletal, No. (%) 2 (3) 1 (8) 0.43
Renal, No. (%) 1 (2) 11 (8) 0.31
Hematologic, No. (%) 2 (3) 0 NA
Overall severity, No. (%)
None to mild 64 (100) 11 (85) 0.03
Moderate/severe 0 2 (15)
• 13 of 77 patients with cutaneous lupus (CLE) progressed to systemic disease (SLE): 16.8%
• 5/24 SCLE (20.8%)
• 8/53 DLE (15.1%)
• Those developing SLE were more likely to have
• ANA >1:80 at baseline (P=0.002)
• Mean time from CLE diagnosis to SLE diagnosis (n=13) was 8.03 years
Baseline Patient Characteristics and Symptoms
P<0.005 = statistically significant

©2016 MFMER | 3507536-60
Criteria SLE, No. (%) (n=13)
Photosensitivity 12 (92)
ANA 9 (69)
Discoid rash 8 (62)
Oral ulcers 7 (54)
Arthritis 6 (46)
Malar rash 4 (31)
Hematologic 4 (31)
Antibodies 3 (23)
Renal 2 (15)
Pleuritis 0
Neurologic 0
Mucocutaneous criteria only 1 (8)
Mucocutaneous criteria and antibodies 3 (23)
Criteria Met by Patients Who Transitioned to SLE
Severity of systemic
symptoms
SLE, No.
(%) (n=13)
SLE
(n=13) P
Musculoskeletal
Mild 1 (2) 0 0.004
Moderate/severe 0 3 (23)
Renal
Mild 0 2 (15) <0.001
Moderate/severe 0 2 (15)
Hematologic
Mild 5 (8) 4 (31) 0.04
Moderate/severe 0 0
Overall severity
Mild 64 (100) 8 (62) <0.001
Moderate/severe 0 5 (38)
Severity of Systemic Symptoms Developed During the Study
• Most patients that developed SLE did so via mucocutaneous ACR criteria (Table 2)
• Of the 13 that developed SLE, only 5 (38.5%) developed new moderate to severe
systemic disease (Table 3)

©2016 MFMER | 3507536-61
• Wieczorek et al. concluded:
• Few patients with newly diagnosed CLE will go on to develop SLE (17%)
• Those that progress to SLE are likely to have mild systemic symptoms/disease (62%)
Note: the 2 patients that developed renal involvement had the following baseline criteria (1 – photosensitivity, ANA, discoid lesions; 2 – photosensitivity, discoid lesions, and arthritis [patient 2 later developed positive ANA and other autoantibodies]) (Personal correspondence with Victoria Werth, M.D., 3/26/14)

©2016 MFMER | 3507536-62
• A new SLE diagnosis in CLE may not require rheumatologic referral if primarily skin disease
• 31% of SLE patients only had mucocutaneous +/- ANA and other autoantibody titers
• Proposed monitoring
1. CBC with differential and urinalysis annually
2. Complete review of systems at each visit
3. Additional serologic tests based on positive review of systems (eg, ANA, anti-dsDNA, anti-Sm)
Chong: JAMA Dermatology, 2014

©2016 MFMER | 3507536-63

©2016 MFMER | 3507536-64
• 20% (18 of 90) SCLE patients met ACR
criteria for SLE
• HOWEVER, only 1 with SLE had
lupus nephritis and none of the
others had renal, neurologic, or
notable hematologic sequelae
• 14% (13 of 90) SCLE patients also had
Sjögren syndrome
• 3 of 13 (23%) had systemic
manifestations of Sjögren syndrome:
pulmonary interstitial fibrosis,
peripheral neuropathy, and
inflammatory myopathy
• (1) Importance of evaluating SCLE patients
not only for SLE, but also for Sjögren
syndrome
• (2) Only rare serious systemic sequelae
in SCLE patients with SLE – may help
guide clinicians on how to monitor their
patients over time for SLE development
Mayo Clinic Proceedings, March 2017 (in press)

©2016 MFMER | 3507536-65
In a patient with lupus, which of the following cutaneous findings is associated with the highest risk of systemic involvement?
1. Generalized DLE
2. Leukocytoclastic vasculitis
3. Lupus panniculitis
4. SCLE
5. Tumid lupus

©2016 MFMER | 3507536-66
Lupus Erythematosus (LE)-Specific Skin Disease
Costner and Sontheimer, Dermatology in General Medicine, Ch. 155, 8th ed.
LE-non-specific
skin disease
Systemic disease Skin disease
only
SCLE
Generalized DLE
Localized DLE
Hypertrophic DLE
LE profundus
ACLE
Risk of systemic lupus:
ACLE, LE-non-specific disease >>> SCLE > DLE (generalized > localized)

©2016 MFMER | 3507536-67
Risk factors for both: (1) progression of DLE to SLE and (2) SLE patients with DLE
• Widespread DLE lesions
• Arthralgias/arthritis
• Nail changes (eg, periungual telangiectasia)
• Anemia
• Leukopenia
• High ESR (sedimentation rate)
• High-titer ANA
2012;166:29

©2016 MFMER | 3507536-68
Summary of Studies Comparing DLE-Only Patients and SLE Patients With DLE
Study, year Groups studied Clinical Laboratory
Cardinali et al., 2000 116 DLE only, 19 DLE with SLE • Generalized DLE
• Nail changes
(i.e. periungual telan
giectasias)
None mentioned
Ng et al., 2000 63 DLE only, 10 DLE with SLE • Generalized DLE • ANA (≥1:160)
• (+) C1q deposits
Scott and Rees, 1959 16 SLE without DLE, 14 DLE with SLE, 11 DLE
with systemic findings but no SLE, 77 DLE only
• Generalized DLE • (+) LE test
Callen, 1982, Callen, 1985 56 DLE only, 17 DLE with SLE • Generalized DLE
• Periungual telangiectasias
• Arthritis
• (+) Anti-nDNA
• Elevated ESR
• Hypocomplementemia
• (+) ANA
• Leucopenia
• Anemia
Vera-Recabarren et al., 2010 148 CCLE only, 10 CCLE with SLE • Generalized DLE
• Arthralgias/arthritis
• Nephropathy
• Xerophthalmia
• Leucopenia
• (+) ANA (≥1:80)
• (+) Anti-Ro
• Lymphopenia
• (+) Anti-dsDNA
Prystowsky and Gilliam, 1975 80 DLE without SLE, 15 DLE with systemic
involvement, 13 SLE with proliferative
glomerulonephritis
• None mentioned • (+) ANA
• Low CH50
• (+) LBT
Characteristics associated with systemic involvement

©2016 MFMER | 3507536-69
Summary of Studies Comparing DLE-Only Patients and Patients With DLE Who Progresses to SLE
Study, year Groups studied Clinical Laboratory
Callen et al., 1982 56 DLE only, 4 DLE → SLE • Widespread DLE
• Periungual telangiectasias
• Arthralgias/arthritis
• Anemia
• High ANA titres
• Leucopenia
• High ESR
Healy et al., 1995 26 localized DLE, 27 widespread DLE, 7
SLE, 3 DLE → SLE
• Progression of localized DLE to
generalized DLE
• Persistently anemia
• Persistently (+) ANA (≥1:80)
• Persistently abnormal ESR
• Persistently abnormal serum
immunoglobins
Insawang et al., 2010 71 DLE only, 59 DLE with SLE (including
27 DLE → SLE)
• Arthralgia/arthritis
• Generalized DLE
• Presence of ANA
• Abnormal urinalysis
Millard and Rowell, 1979 67 localized DLE, 19 disseminated DLE,
6 DLE → SLE
None mentioned • Persistently (+) ANF titre (>1:50)
• Persistently low hemoglobin
Risk factors for systemic spread

©2016 MFMER | 3507536-70
JAMA Dermatology, 2014
©2016 MFMER | 3507536-71

©2016 MFMER | 3507536-72
SLE manifestation
(n=positive finding of
1043)
SLE without
DLE (n=926),
n(%)
SLE with DLE
(n=117), n (%)
Unadjusted OR
(95% CI)
Adjusted OR
(95%)
Adjusted OR
(95%)
Anti-Smith 201(21.7) 45 (38.5) 2.25 (1.50-3.38) 2.27 (1.50-3.45) 2.41 (1.58-3.69)
Photosensitivity 374 (40.4) 60 (51.3) 1.55 (1.06-2.28) 1.71 (1.15-2.55) 1.63 (1.09-2.44)
Leukopenia 301 (32.5) 50 (42.7) 1.55 (1.05-2.29) 1.50 (1.01-2.24) 1.55 (1.03-2.32)
Pleuritis 349 (37.7) 31 (26.5) 0.59 (0.39-0.92) 0.56 (0.36-0.88) 0.56 (0.36-0.76)
Arthritis 738 (79.7) 79 (67.5) 0.53 (0.35-0.80) 0.51 (0.33-0.79) 0.49 (0.31-0.76)
Lupus nephritis 281 (30.3) 38 (32.5) 1.10 (0.73-1.66) 1.09 (0.71-1.68) 1.33 (0.83-2.14)
Pericarditis 112 (12.1) 10 (8.6) 0.68 (0.35-1.34) 0.68 (0.34-1.36) 0.68 (0.34-1.36)
Proteinuria 256 (27.7) 27 (23.1) 0.78 (0.50-1.23) 0.70 (0.43-1.13) 0.77 (0.47-1.27)
Casts 117 (12.6) 9 (77) 0.56 (0.28-1.17) 0.53 (0.26-1.09) 0.57 (0.27-1.20)
End-stage renal
disease 48 (5.1) 7 (6.0) 1.16 (0.51-2.64) 0.96 (0.41-2.22) 1.24 (0.50-3.05)
Oral ulcers 240 (25.9) 37 (31.6) 1.32 (0.87-2.00) 1.35 (0.88-2.07) 1.32 (0.86-2.03)
Malar rash 406 (43.8) 46 (39.3) 0.82 (0.56-1.23) 0.86 (0.57-1.30) 0.88 (0.58-1.32)
Seizure 100 (10.8) 14 (12) 1.12 (0.61-2.03) 1.14 (0.62-2.09) 1.20 (0.65-2.21)
Psychosis 16 (1.7) 3 (2.6) 1.50 (0.43-5.21) 1.45 (0.41-5.14) 1.50 (0.42-5.38)
Anemia 181 (19.5) 26 (22.2) 1.17 (0.74-1.87) 1.12 (0.69-1.80) 1.15 (0.71-1.86)
Lymphopenia 340 (36.7) 51 (43.6) 1.33 (0.90-1.96) 1.32 (0.88-1.97) 1.38 (0.91-2.08)
Thrombocytopenia 110 (11.9) 18 (15.4) 1.35 (0.79-2.31) 1.45 (0.83-2.54) 1.54 (0.87-2.71)
Anti-dsDNA 610 (65.9) 83 (70.9) 1.27 (0.83-1.93) 1.25 (0.81-1.93) 1.33 (0.86-2.07)
Antiphospholipid
antibodies 225 (24.3) 24 (20.5) 0.80 (0.50-1.29) 0.85 (0.52-1.37) 0.87 (0.54-1.43)
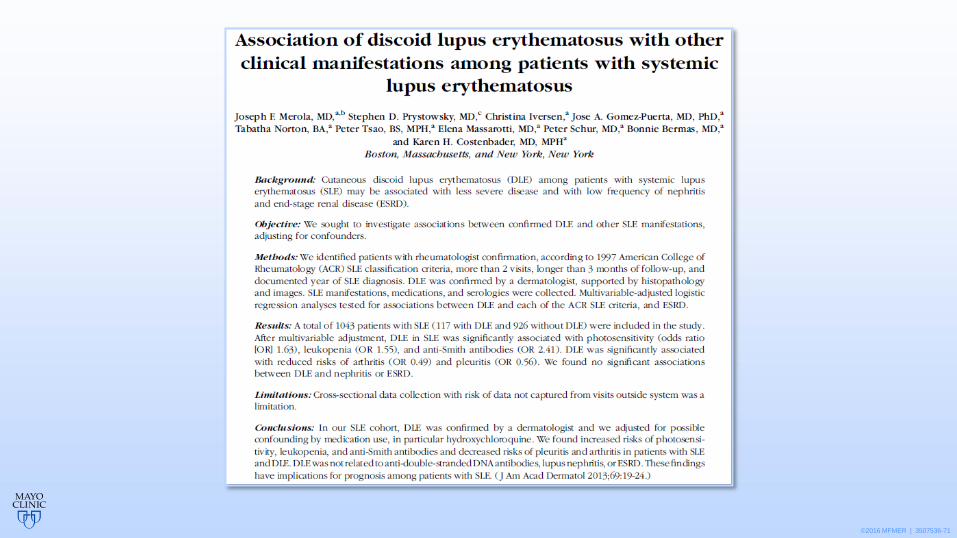
Capsule Summary
• Prior studies suggest that discoid lupus erythematosus among patients with systemic lupus erythematosus is a marker for less severe disease, often offered as reassurance
• We did not observe any associations (either positive or negative) with discoid lupus erythematosus and severe lupus manifestations (ie, renal or neurologic)
• These findings have important implications for counseling our patients with systemic lupus erythematosus and discoid lupus erythematosus regarding prognosis
DLE in SLE (compared to SLE without DLE):
• Increased risk of photosensitivity, leukopenia, and anti-Smith antibodies
• Decreased risk of pleuritis and arthritis
• No association (positive or negative) with nephritis or neurologic disease
Associations between discoid lupus erythematosus and other American College of
Rheumatology criteria for systemic lupus erythematosus and end-stage renal disease

©2016 MFMER | 3507536-73
Summary of Cutaneous Lupus (CLE)
• Diagnosis of CLE requires clinicopathologic correlation
• CLE classified as
• Lupus-specific skin disease (multiple subtypes)
• Lupus-nonspecific skin disease
• Risk of systemic disease varies according to the type of skin disease present
• Smoking is associated with worse CLE
• Medications can trigger CLE (particularly SCLE)
• Patients with CLE should be monitored for progression to systemic disease, but consensus guidelines lacking
• Risk factors for SLE in those with DLE include
• Widespread DLE, arthralgias/arthritis, periungual telangiectasias, anemia, leukopenia, high ESR, high-titer ANA