Current Best Practice in Interventional Cardiology€¦ · BLBK225-FM BLBK225-Meier October 14,...
24
Current Best Practice in Interventional Cardiology EDITED BY Bernhard Meier, MD, FACC, FESC Cardiology Swiss Cardiovascular Center Bern University Hospital Bern Bern Switzerland A John Wiley & Sons, Ltd., Publication
Transcript of Current Best Practice in Interventional Cardiology€¦ · BLBK225-FM BLBK225-Meier October 14,...

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
Current BestPractice inInterventionalCardiologyE D I T E D B Y
Bernhard Meier, MD, FACC, FESCCardiologySwiss Cardiovascular Center BernUniversity Hospital BernBernSwitzerland
A John Wiley & Sons, Ltd., Publication

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
Current Best Practice in Interventional Cardiology

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
Commissioning Editor: Thomas V. HartmanDevelopment Editor: Kate NewellProduction Editor: Cathryn GatesProduction Controller: Susan Shepherd

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
Current BestPractice inInterventionalCardiologyE D I T E D B Y
Bernhard Meier, MD, FACC, FESCCardiologySwiss Cardiovascular Center BernUniversity Hospital BernBernSwitzerland
A John Wiley & Sons, Ltd., Publication

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
This edition first published 2010 C© 2010 by Blackwell Publishing Ltd
Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishing program hasbeen merged with Wiley’s global Scientific, Technical and Medical business to form Wiley-Blackwell.
Registered office: John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to apply forpermission to reuse the copyright material in this book please see our website atwww.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance with theCopyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted,in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except aspermitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not beavailable in electronic books.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand namesand product names used in this book are trade names, service marks, trademarks or registered trademarks oftheir respective owners. The publisher is not associated with any product or vendor mentioned in this book.This publication is designed to provide accurate and authoritative information in regard to the subject mattercovered. It is sold on the understanding that the publisher is not engaged in rendering professional services. Ifprofessional advice or other expert assistance is required, the services of a competent professional should besought.
The contents of this work are intended to further general scientific research, understanding, and discussion onlyand are not intended and should not be relied upon as recommending or promoting a specific method,diagnosis, or treatment by physicians for any particular patient. The publisher and the author make norepresentations or warranties with respect to the accuracy or completeness of the contents of this work andspecifically disclaim all warranties, including without limitation any implied warranties of fitness for a particularpurpose. In view of ongoing research, equipment modifications, changes in governmental regulations, and theconstant flow of information relating to the use of medicines, equipment, and devices, the reader is urged toreview and evaluate the information provided in the package insert or instructions for each medicine,equipment, or device for, among other things, any changes in the instructions or indication of usage and foradded warnings and precautions. Readers should consult with a specialist where appropriate. The fact that anorganization or Website is referred to in this work as a citation and/or a potential source of further informationdoes not mean that the author or the publisher endorses the information the organization or Website mayprovide or recommendations it may make. Further, readers should be aware that Internet Websites listed in thiswork may have changed or disappeared between when this work was written and when it is read. No warrantymay be created or extended by any promotional statements for this work. Neither the publisher nor the authorshall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication DataCurrent best practice in interventional cardiology / edited by Bernhard Meier.
p. ; cm.Includes bibliographical references.ISBN 978-1-4051-8255-31. Heart–Surgery. 2. Heart–Diseases–Treatment. 3. Heart–Interventional radiology.
I. Meier, Bernhard, M.D.[DNLM: 1. Heart Diseases–surgery. 2. Cardiovascular Diseases–diagnosis. 3. Diagnostic Imaging–methods.
4. Vascular Diseases–surgery. WG 169 C97517 2009]RD598.C84 2009617.4’12–dc22
2009014017ISBN: 9781405182553
A catalogue record for this book is available from the British Library.
Set in 9/12pt Meridien by Aptara R© Inc., New Delhi, IndiaPrinted and bound in Malaysia
1 2010

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
Contents
List of Contributors, vii
Preface, ix
Part I Coronary Artery Disease
1 Acute Coronary Syndromes, 3Pierre-Frederic Keller and Marco Roffi
2 Modern Coronary Stenting, 23Stephane Cook
3 Chronic Total Occlusion, 40David Rosenmann, David Meerkin and Yaron Almagor
4 Nonrevascularization Therapy, 53Jean-Paul Schmid
Part II Noncoronary Interventions
5 Transcatheter Aortic Valve Implantation, 69Helene Eltchaninoff and Alain Cribier
6 Patent Foramen Ovale Closure, 81Bernhard Meier
7 Closure of Atrial and Ventricular Septal Defects in Adults, 93David Hildick-Smith
8 Carotid Artery Stenting, 103Paul Chiam, Sriram Iyer, Gary Roubin and Jiri Vitek
9 Alcohol Ablation of Hypertrophic Cardiomyopathy, 117Otto M. Hess and Sven Streit
Part III Treatment of Left Ventricular Failure
10 Biventricular Pacing, 129Haran Burri and Etienne Delacretaz
11 Percutaneous Left Ventricular Assist Devices, 145Georgios Sianos and Pim J. de Feyter
12 Treatment of Left Ventricular Failure, 152Roger Hullin
v

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
vi Contents
Part IV Cardiovascular Imaging
13 Computed Tomography for Screening and Follow-up, 163Stephan Achenbach
14 Magnetic Resonance for Functional Testing and Interventional Guidance, 178Simon Koestner
15 Optical Coherence Tomography for Coronary Imaging, 195Jean-Francois Surmely
16 Intravascular Ultrasound, 206Masao Yamasaki, Junya Ako, Yasuhiro Honda and Peter J. Fitzgerald
Index, 212

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
List of Contributors
Stephan Achenbach, MD, FACC, FESCDepartment of CardiologyUniversity of ErlangenErlangen, Germany
Junya Ako, MDCenter for Research in Cardiovascular InterventionsStanford University Medical CenterStanford, CA, USA
Yaron Almagor, MDInterventional CardiologyShaare Zedek Medical CenterJerusalem, Israel
Haran Burri, MDCardiology ServiceUniversity Hospital of GenevaGeneva, Switzerland
Paul Chiam, MBBS, MRCP, FACCDepartment of CardiologyNational Heart CenterSingapore
Stephane Cook, MDCardiologySwiss Cardiovascular Center BernUniversity Hospital BernBern, Switzerland
Alain Cribier, MDDepartment of CardiologyHospital Charles NicolleUniversity of RouenRouen, France
Pim J. de Feyter, MDDepartment of CardiologyErasmus UniversityRotterdam, The Netherlands
Etienne Delacretaz, MD, FACCCardiologySwiss Cardiovascular Center BernUniversity Hospital BernBern, Switzerland
Helene Eltchaninoff, MDDepartment of CardiologyHospital Charles NicolleUniversity of RouenRouen, France
Peter J. Fitzgerald, MD, PhDDivision of CardiologyStanford University Medical CenterStanford, CA, USA
Otto M. Hess, MDCardiologySwiss Cardiovascular CenterUniversity HospitalBern, Switzerland
David Hildick-Smith, MDSussex Cardiac CentreBrighton and Sussex University Hospital NHS TrustBrighton, UK
Yasuhiro Honda, MDDivision of CardiologyStanford University Medical CenterStanford, CA, USA
Roger Hullin, MDDepartment de Medecine InterneCentre Hospitalier Universitaire VaudoisLausanne, Switzerland
Sriram Iyer, MD, FACCDepartment of Cardiac and Vascular Interventional ServicesLenox Hill Heart and Vascular Institute of New YorkNew York, NY, USA
vii

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
viii Contributors
Pierre-Frederic Keller, MDDivision of CardiologyUniversity Hospital of GenevaGeneva, Switzerland
Simon Koestner, MDCardiologyCardiovascular DepartmentUniversity Hospital BernBern, Switzerland
David Meerkin, MBBSInterventional CardiologyShaare Zedek Medical CenterJerusalem, Israel
Bernhard Meier, MD, FACC, FESCCardiologySwiss Cardiovascular Center BernUniversity Hospital BernBern, Switzerland
Marco Roffi, MDDivision of CardiologyUniversity Hospital of GenevaGeneva, Switzerland
David Rosenmann, MDInterventional CardiologyShaare Zedek Medical CenterJerusalem, Israel
Gary Roubin, MD, PhD, FACCDepartment of Cardiac and Vascular Interventional ServicesLenox Hill Heart and Vascular Institute of New YorkNew York, NY, USA
Jean-Paul Schmid, MDCardiologySwiss Cardiovascular Center BernUniversity Hospital BernBern, Switzerland
Georgios Sianos, MD, PhD, FESC1st Department of CardiologyAHEPA University HospitalThessaloniki, Greece
Sven Streit, MDCardiologySwiss Cardiovascular CenterUniversity HospitalBern, Switzerland
Jean-Francois Surmely, MDCardiologyClinique de la SourceLausanne, Switzerland
Jiri Vitek, MD, PhDDepartment of Cardiac and Vascular Interventional ServicesLenox Hill Heart and Vascular Institute of New YorkNew York, NY, USA
Masao Yamasaki, MDDivision of CardiologyStanford University Medical CenterStanford, CA, USA

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
Preface
A comprehensive textbook on interventional car-diology requires 3 volumes or a DVD. What youhold in your hand is a glimpse at the current bestpractice of some selected aspects of interventionalcardiology.
The book is targeted at a wide spectrum of read-ers ranging from the accomplished interventionalcardiologist, desirous of looking over the fence orfilling in some of the few remaining dark spotsin his or her knowledge or armamentarium, tothe nurse, technician, or physician assistant activein interventional cardiology. A cardiologist refer-ring patients for catheter-based interventions mightwant to take a look at what is available, and a car-diovascular surgeon might want to find out what isoffered to patients before or instead of summoningsurgical help. Finally, industry representatives anddevice developers may use it to keep abreast of thestate of the art, remaining shortcomings, and needsthat may yet have to be identified.
Part I is the bread-and-butter section: percuta-neous interventions for coronary artery disease.Acute coronary syndromes account for more thanone-third of patients treated with percutaneouscoronary intervention (PCI, introduced under thename PTCA 32 years ago). Stents are an inte-gral part of the procedure, at least intentionally.Globally, 10% to 30% of lesions are still treatedwithout a stent, but this is usually imposed by cir-cumstances rather than the primary plan. Drug-eluting stents are about to supplant the tradi-tional bare metal stents. Their advantage is smallbut relevant enough to render bare metal stentsunattractive, irrespective of the fact that they havedone a superb job so far. As for indications, thedelineation between bypass surgery and PCI hasbeen concretized by randomized trials. Selecteddouble-vessel disease and triple-vessel disease in-
cluding the left main have been cleared for PCI,albeit only in selected cases. A remaining bas-tion is chronic total occlusion. The books are stillopen about how important it is to recanalize it,what the best stepwise approach is, and how muchtime, radiation, and material should be investedbefore giving up in favor of medical treatmentor bypass surgery. End-stage coronary artery dis-ease carries a stigma almost like end-stage cancer.The respective treatments discussed here are cor-rectly called palliative. So is revascularization, bythe way.
In Part II, a variety of noncoronary interventionsare discussed, a popular name for them being struc-tural interventions. The most intriguing example ispercutaneous replacement of the aortic valve. Thisis the current phoenix of interventional cardiologyand rightfully so. In a very common disease,onerous open heart surgery can be replaced by acatheter intervention, in some cases even underlocal anesthesia. In contrast to PCI, which startedto compete with surgery in the easy case, percu-taneous aortic valve replacement is starting withthe difficult one. The future looks bright, as percu-taneous aortic valve replacement appears to workeven in these patients. Closure of atrial shuntspreceded PCI by a couple of years. Moreover, it hasthe potential to become more common than PCI,as every fourth person carries a patent foramenovale. The medical community is carefully inves-tigating the true value of these procedures, andthe respective chapters help with that endeavor.Carotid angioplasty currently involves by defaulta stent and a protection device. In contrast to PCIthe differences between surgery and the percuta-neous procedure are small (no thoracotomy, noheart-lung machine). Hence a draw in outcome isnot accepted; the percutaneous approach has to be
ix

BLBK225-FM BLBK225-Meier October 14, 2009 20:47 Char Count=
x Preface
better and safer. We are not there yet, but we hopeto be on the right track. Alcohol ablation for hyper-trophic cardiomyopathy looks back on more than adecade of clinical use. It has been adopted as a firstapproach for most patients with this rather rareclinical need.
Part III is dedicated to interventional approachesto left ventricular failure. Biventricular pacing ap-pears to have gained an indelible place for chronictreatment, whereas percutaneous left ventricularassist devices usually serve for short periods of timeas bridges to recovery or more definitive treat-ments. Stem cell therapy is discussed as a glow onthe horizon, although it is not quite clear whetherthe sun is rising on it or has already set on it andwe just do not know yet.
Part IV deals with cardiovascular imaging,putting magnetic resonance in the forefront as therecognized technique of the future. Computed to-mography and intravascular imaging such as ultra-sound and optical coherence tomography are alsodiscussed.
Whether the book is read from cover to cover,used as a hard-copy thesaurus to thumb throughwhen a question comes up, or—why not?—utilizedas a picture book to browse through when somespare time is at hand, the authors truly hope thatthe contact with this book will be interesting, re-warding, and pleasurable.
Bernhard Meier

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
PART I
Coronary Artery Disease

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
CHAPTER 1
Acute Coronary SyndromesPierre-Frederic Keller and Marco RoffiDivision of Cardiology, University Hospital of Geneva, Geneva, Switzerland
Chapter Overview
� Acute coronary syndromes (ACS) are the acute manifestation of atherosclerotic coronary artery disease.
Based on different presentations and management, patients are classified into non–ST-segment elevation
ACS (NSTE-ACS) and ST-segment elevation myocardial infarction (STEMI).� In western countries, NSTE-ACS is more frequent than STEMI.� Even if the short-term prognosis (30 days) for NSTE-ACS is more favorable than for STEMI, the long-term
prognosis is similar or even worse.� Early invasive strategy is the management of choice in patients with NSTE-ACS, particularly in high-risk
subgroups.� Primary percutaneous coronary intervention (PCI) is the treatment of choice for STEMI. Facilitated PCI is of
no additional benefit.� The reduction of door-to-balloon time in primary PCI is critical for improved outcomes in STEMI patients.� If fibrinolytic therapy is administered in STEMI, then patients should be routinely transferred for immediate
coronary angiography, and if needed, percutaneous revascularization.� High-risk ACS patients (eg, elderly patients, those in cardiogenic shock) have the greatest benefit from PCI.� Antithrombotic therapy in ACS is getting more and more complex. The wide spectrum of antiplatelet agents
and anticoagulants requires a careful weighing of ischemic and bleeding risks in each individual patient.
ST-Segment ElevationMyocardial Infarction
The term acute coronary syndrome (ACS) hasemerged as useful tool to describe the clinical cor-relate of acute myocardial ischemia. ST-segment el-evation (STE) ACS includes patients with typicaland prolonged chest pain and persistent STE onthe ECG. In this setting, patients will almost in-variably develop a myocardial infarction (MI), cate-gorized as ST-segment elevation myocardial infarc-tion (STEMI). The term non–ST-segment (NSTE)ACS refers to patients with signs or symptoms sug-
gestive of myocardial ischemia in the absence of sig-nificant and persistent STE on ECG. According towhether the patient has at presentation, or will de-velop in the hours following admission, laboratoryevidence of myocardial necrosis or not, the work-ing diagnosis of NSTE-ACS will be further specifiedas NSTE-MI or unstable angina.
Recently, MI was redefined in a consensus doc-ument [1]. The 99th percentile of the upper refer-ence limit (URL) of troponin was designated as thecut-off for the diagnosis. By arbitrary convention, apercutaneous coronary intervention (PCI)-relatedMI and coronary artery bypass grafting (CABG)-related MI were defined by an increase in cardiacenzymes more than three and five times the 99thpercentile URL, respectively. The application of thisdefinition will undoubtedly increase the number of
Current Best Practice in Interventional Cardiology. Edited by
B Meier. © 2010 Blackwell Publishing,
3

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
4 Part I Coronary Artery Disease
events detected in the ACS and the revasculariza-tion setting. The impact on public health as well asat the clinical trial level of the new MI definitioncannot be fully foreseen.
The extent of cellular compromise in STEMI isproportional to the size of the territory supplied bythe affected vessel and to the ischemic length oftime. Therefore a quick and sustained restorationof normal blood flow in the infarct-related arteryis crucial to salvage myocardium and improvesurvival.
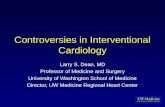
Primary PCI VersusThrombolytic TherapyPrimary percutaneous coronary intervention be-came increasingly popular in the early 1990s. Ev-idence favoring this strategy in comparison withthrombolytic therapy is substantiated by a meta-analysis of 23 randomized trials demonstrating that
Figure 1.1 Short-term clinical outcomes of patients in23 randomized trials of primary PCI versus thrombolysis.(Reproduced with permission from [2] Keeley EC, BouraJA, Grines CL. Primary angioplasty versus intravenous
thrombolytic therapy for acute myocardial infarction: aquantitative review of 23 randomised trials. Lancet.2003;361:13–20.)
PCI more efficaciously reduced mortality, nonfatalreinfarction, and stroke (Fig. 1.1) [2]. The advan-tage of primary PCI over thrombolysis was inde-pendent of the type of thrombolytic agent used,and was also present for patients who were trans-ferred from one institution to another for the per-formance of the procedure. Therefore, primary PCIis now considered the reperfusion therapy of choiceby all the guidelines [3,4]. With respect to bleed-ing complications, a recent meta-analysis demon-strated that the incidence of major bleeding compli-cations was lower in patients treated with primaryPCI than in those undergoing thrombolytic therapy[2]. In particular intracranial hemorrhage, the mostfeared bleeding complication, was encountered inup to 1% of patients treated with fibrinolytic ther-apy and in only 0.05% of primary PCI patients. Thealgorithm for treatment of patients admitted for aSTEMI is presented in Fig. 1.2 [5].

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
Chapter 1 Acute Coronary Syndromes 5
STEMIWithin 12 hours after onset of symptoms
Patient presenting in ahospital with PCI
Patient presenting in ahospital without PCI
> 3 hours ≤ 3 hours
*PCI ≤ 24 hours not available PCI ≤ 24 hours available
✝If thrombolysis is contraindicated or the patient is at high risk, immediate transfer should be considered*Even after successful thrombolysis, adjunctive PCI should be considered
Thrombolysis
Successful Failed
Immediatetransfert
Primary PCI
Predischarge ischemia
Ischemia guided PCI Post thrombolysis PCI Rescue PCI
Figure 1.2 Algorithm for revascularization in STEMIpatients with less than 12 hours from symptom onsetaccording to the 2005 ESC guideline for PCI.(Reproduced with permission [5] from Silber S,
Albertsson P, Aviles FF, et al. Guidelines forpercutaneous coronary interventions. The Task Force forPercutaneous Coronary Interventions of the EuropeanSociety of Cardiology. Eur Heart J. 2005;26:804–847.)
Advantages of Primary PCIMore than 90% of patients treated by primaryPCI achieve normal flow (thrombosis in myocar-dial infarction [TIMI] grade flow 3) at the endof the intervention, while only 65% of patientstreated by thrombolytic therapy benefit from thisdegree of reperfusion (Table 1.1) [6–8]. In addi-tion, thrombolyis is characterized by a rapidly de-creased efficacy after 2 hours of symptom onset(Fig. 1.3) [9]. There is a close relationship betweenthe quality of coronary flow obtained after reperfu-sion therapy and mortality, and the prognosis of pa-tients in whom flow normalization is not achievedis similar to that of patients with persistent ves-sel occlusion. The classification of TIMI myocar-dial blush grade allows an estimate of the tissue-level perfusion (Table 1.1). A critical link betweenlower TIMI myocardial blush grade, expression ofa microcirculatory compromise, and mortality has
been demonstrated in patients with normal epicar-dial flow following reperfusion therapy [10]. Theimprovement of clinical outcomes with primaryPCI versus thrombolysis is also the consequenceof a lower rate of reocclusion (0–6%). Accord-ingly, with thrombolytic therapy, reocclusion mayoccur in over 10% of cases even among patientspresenting within the first 2 hours of symptomonset.
Mechanical complications of STEMI, such asacute mitral regurgitation and ventricular septal de-fect, were reduced by 86% by primary PCI com-pared with thrombolytic therapy in a meta-analysisof the GUSTO-1 and PAMI trials [11]. Free wallrupture was also significantly reduced by primaryPCI [12]. Finally, primary PCI may allow earlierdischarge (2–3 days following PCI versus 7 daysfollowing fibrinolytic therapy for uncomplicatedcourses).

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
6 Part I Coronary Artery Disease
Table 1.1 TIMI Classification of Coronary Flow and Perfusion
Flow Grade Classification
TIMI Flow Grade Definition
0 No antegrade flow beyond the point of occlusion.1 Faint antegrade coronary flow beyond the occlusion, although filling of the distal coronary bed is
incomplete.2 Delayed or sluggish antegrade flow with complete filling of the distal territory.3 Normal flow that fills the distal coronary bed completely.
Perfusion Grade Classification
Perfusion Grade Definition
0 Minimal or no myocardial blush is seen.1 Dye stains the myocardium; this stain persists on the next injection.2 Dye enters the myocardium but washes out slowly so that the dye is strongly persistent at the end
of the injection.3 There is normal entrance and exit of the dye in the myocardium so that the dye is mildly persistent
at the end of the injection.
Adapted with permission from [7] Gibson CM, Schomig A. Coronary and myocardial angiography: angiographicassessment of both epicardial and myocardial perfusion. Circulation. 2004;109:3096–3105; and [8] Schomig A, Mehilli J,Antoniucci D, et al. Mechanical reperfusion in patients with acute myocardial infarction presenting more than 12 hoursfrom symptom onset: a randomized controlled trial. JAMA. 2005;293:2865–2872.
Figure 1.3 Time delays to thrombolysis in STEMI andthe absolute reduction in 35-day mortality. (Reproducedwith permission from [9] Boersma E, Maas AC, DeckersJW, Simoons ML. Early thrombolytic treatment in acutemyocardial infarction: reappraisal of the golden hour.Lancet. 1996;348:771–775.)
Decreasing the Time to Reperfusion inPrimary PCIThe survival benefit of reperfusion associated withthrombolytic therapy shrinks with increasing delay
in the administration of the agent. For stable pa-tients undergoing primary PCI, no association be-tween symptom-onset-to-balloon time and mortal-ity was observed in the U.S. NRMI registry [13].In contrast, a significant increase in mortality wasdetected for patients with a door-to-balloon-timegreater than 2 hours [14]. Therefore, the findingsof primary PCI trials may be only applicable to hos-pitals with established primary PCI programs, expe-rienced teams of operators, and a sufficient volumeof interventions. Indeed, an analysis of the NRMI-2registry demonstrated that hospitals with less than12 primary PCIs per year have a higher rate of mor-tality than those with more than 33 primary PCIsper year [13]. Useful tools to decrease the door-to-balloon time are described in Table 1.2 [15].
Challenging Groups of Patients
Concomitant High-Grade Non-Culprit LesionsThe timing of revascularization of severe non-culprit lesion treatment in patients with multivessel

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
Chapter 1 Acute Coronary Syndromes 7
Table 1.2 Strategies to Reduce theDoor-to-Balloon Time in Primary PCI
� Emergency medicine physicians activate the catheterizationlaboratory (mean reduction in door-to-balloon time, 8.2 minutes)
� Having a single call to a central page operator activate the laboratory(13.8 minutes)
� Having the emergency department activate the catheterizationlaboratory while the patient is en route to the hospital (15.4 minutes)
� Expecting staff to arrive in the catheterization laboratory within20 minutes after being paged (vs. >30 minutes) (19.3 minutes)
� Having an attending cardiologist always on site (14.6 minutes),� Having staff in the emergency department and the catheterization
laboratory use real-time data feedback (8.6 minutes).
From [15] Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing thedoor-to-balloon time in acute myocardial infarction. N Engl J Med.2006;355:2308–2320.
disease undergoing primary PCI has long been de-bated. Multivessel PCI in stable STEMI patientswas found to be an independent predictor ofmajor adverse cardiac events (MACE) at 1 year[16]. However, a recent study suggested that sys-tematic revascularization of multivessel disease atthe time of primary PCI in contrast to ischemia-driven revascularization may be of advantage be-cause incomplete revascularization was found tobe a strong and independent risk predictor fordeath and MACE [17]. Another study supportedthe notion that complete revascularization im-proved clinical outcomes in STEMI patients withmultivessel disease [18]. Accordingly, the studyshowed a significant lower rate of recurrent is-chemic events and acute heart failure during the in-dexed hospitalization. Nevertheless, current Amer-ican College of Cardiology/American Heart Associ-ation (ACC/AHA) guidelines recommend that PCIof the non-infarct artery should be avoided inthe acute setting in patients without hemodynamicinstability [19].
Cardiogenic ShockThe incidence of cardiogenic shock in acute MI pa-tients is in decline, accounting for approximately6% of all cases [20]. As the result of the increas-ing use of primary PCI, the shock-related mor-tality has decreased. Accordingly, a U.S. analysisshowed mortality rates in shock of 60% in 1995
and 48% in 2004, while the corresponding primaryPCI rates were 27% to 54% [21]. In the SHOCKtrial, early revascularization was associated with asignificant survival advantage [22]. In the study,approximately two-thirds of patients in the inva-sive arm were revascularized by PCI and one-thirdby CABG surgery. Thrombolysis was administeredin 63% of patients allocated to the medical sta-bilization arm. Early revascularization is stronglyrecommended for shock patients younger than75 years. In older patients, revascularization maybe considered in selected patients [23].
In the last two decades, hemodynamic sup-port devices have been developed to limit end-organ failure in the setting of cardiogenic shock.The intraaortic balloon pump (IABP) is the mostcommonly used mechanical support device. Per-cutaneous left atrial-to-femoral arterial bypass as-sistance, and more recently the Impella Recovermicroaxial left ventricular and/or right ventricularassist device, have been developed to increase car-diac output. However, no randomized clinical dataexist to support the benefit of this device. Percu-taneous cardiopulmonary bypass support using ex-tracorporeal membrane oxygenation (ECMO) canbe used in cardiogenic shock for a longer pe-riod of time than the other devices just described.However, while ECMO has excellent oxygenationproperties, it provides only limited cardiac outputsupport.

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
8 Part I Coronary Artery Disease
Elderly PatientsElderly patients present more frequently withnon–ST-segment elevation myocardial infarction(NSTEMI) than with STEMI. As many as 80% ofall deaths related to MI occur in persons older than75 years of age. With respect to STEMI, up to two-thirds may occur in patients older than 65 years ofage. Although, fibrinolytic therapy has been shownto be as effective in the elderly as in younger pa-tients for achieving TIMI-3 flow, the percentage ofpatients eligible for this therapy decreases with ad-vancing age due to comorbid conditions. The Se-nior PAMI trial randomized 483 patients ≥ 70 yearsold who were eligible for thrombolysis to primaryPCI versus thrombolytic therapy [24]. A substan-tial benefit of PCI was seen in patients aged 70 to80 with a 37% reduction in death, and a 55% re-duction in the composite end point of death, MI,or stroke. Among patients older than 80 years ofage, the prognosis was poor in both the PCI andthrombolytic arms. Based on these findings and onthe increased delay of reperfusion observed in thispopulation, primary PCI is the preferred revascu-larization approach.
Late PresentationFew studies have evaluated whether mechani-cal reperfusion is beneficial in patients presenting�12 hours from symptom onset. The OAT trialdemonstrated in patients randomized to conserva-tive medical therapy or late PCI that stable patientsdo not clinically benefit from late invasive strategyafter MI [25]. This was confirmed with the DECOPItrial [26]. However, in the latter trial at 6 months,left ventricular ejection fraction was 5% higherin the invasive compared with the medical group(p = 0.013), suggesting that mechanical revascu-larization may improve ventricular remodeling andfunction. The BRAVE-2 investigators randomized365 patients with STEMI (between 12 and 48 hoursfrom symptom onset) to PCI with abciximab ver-sus conservative care [28]. Infarct size measured bysestamibi was smaller in the invasive group, witha favorable trend with respect to composite clini-cal end points. These data suggest that the benefitof primary PCI may extend beyond the traditional12-hour window.
Rescue and Urgent PCI FollowingThrombolytic TherapyBecause of the high rate of primary failure of fib-rinolysis, in the absence of reperfusion rescue PCImust be considered 60 to 90 minutes after throm-bolytic therapy [27]. Suggestive of primary failureare persistent, severe, or worsening chest pain, dys-pnea, diaphoresis, persistent or worsening ST seg-ment elevation, and hemodynamic or rhythmic in-stability. According to the ACC/AHA guidelines, re-duction of � 50% of the initial ST segment eleva-tion on ECG at 60 to 90 minutes after thrombolytictherapy is suggestive of reperfusion, and � 70%reduction is considered as complete resolution [4].Among 1398 STEMI patients presenting within6 hours of symptom onset, the 35-day mortalityrate for complete, partial (30–70%), or no resolu-tion of ST segment elevation at 3 hours was 2.5%,4.3%, and 17.5%, respectively (p � 0.0001) [28].This relationship was observed in both anterior andinferior wall infarction. In the study, the degree ofST segment resolution was the most powerful clin-ical predictor of 35-day mortality. In the InTIME-IItrial, the prognostic impact of ST segment resolu-tion at 60 versus 90 minutes was compared among1797 patients [29]. Patients with ST segment res-olution at 60 minutes had a lower mortality rateat 30 days and 1 year compared to those withresolution at 90 minutes. These findings suggestthat ST segment should be routinely reassessed at60 minutes and, in the absence of reperfusion,patients should undergo rescue PCI.
Facilitated PCIFacilitated PCI refers to the administration ofan urgent pharmacologic therapy (ie, thrombol-ysis, GP IIb/IIIa inhibitor, or a combination) fol-lowed by systematic early PCI. Although the in-ternational European Society of Cardiology (ESC)and ACC/AHA guidelines recommended a door-to-balloon time for primary PCI of less than 90 min-utes, a survey of 4278 patients transferred for pri-mary PCI from the U.S. NRMI registry found thatonly 4% and 15% of them were treated within 90and 120 minutes, respectively [30]. In the CAPI-TAL AMI trial, 170 high-risk STEMI patients wererandomized to full-dose tenecteplase or full-dose

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
Chapter 1 Acute Coronary Syndromes 9
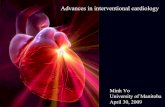
Figure 1.4 Thirty-day mortalityfollowing primary or facilitated PCI byusing tenecteplase [TNK] among the1663 patients involved in the ASSENT-4trial. (Data extracted with permissionfrom the ASSENT-4 investigators [32].)
tenecteplase followed by immediate transfer for PCI[31]. The composite primary end point of death, re-current MI, recurrent unstable ischemia, or strokeat 6 months was significantly decreased by facili-tated PCI (11.6% vs. 24.4 %, p = 0.04). The reduc-tion was driven by a decrease in recurrent ischemia.
The ASSENT-4 trial randomized 4000 patientswith STEMI of less than 6 hours from symptomonset to full dose tenecteplase or placebo prior toprimary PCI. The composite primary end point wasdeath, heart failure, or shock within 90 days. Thestudy was stopped prematurely because of a sig-nificant increase in mortality in the tenecteplasegroup (6% vs. 3%, p = 0.0105) (Fig. 1.4) [32]. Ameta-analysis of facilitated PCI trials showed thatGP IIb/IIIa inhibitor-facilitated PCI had no advan-tages in term of post-procedure TIMI 3 grade flowand clinical end points [33]. Similarly, no benefitin terms of ischemic event reduction but a greaterbleeding risk was observed in facilitated PCI withabciximab and half-dose reteplase compared withprimary PCI. Therefore, facilitated PCI should beavoided.
Adjunctive PCI AfterSuccessful ThrombolysisIn the CARESS-in-AMI trial, among 600 high-riskSTEMI patients treated with reteplase, randomiza-tion to immediate transfer for urgent PCI was as-sociated with a significant decrease in the compos-
ite end point of death, reinfarction, or refractory is-chemia at 30 days compared to a conservative ap-proach [34]. In the TRANSFER-AMI trial, high-riskSTEMI patients were randomized to tenecteplase ortenecteplase and transfer for PCI within 6 hoursof fibrinolysis [35]. The 30-day composite primaryend point of death, recurrent MI, congestive heartfailure, severe recurrent ischemia, or shock oc-curred in 16.6% of patients in the control groupand in 10.6% of patients in the invasive group (p =0.0013). No difference was noted in bleeding com-plications. The optimal timing of routine angiogra-phy and possible PCI after fibrinolytic therapy forSTEMI has not been determined. Evidence fromthe GRACIA-2 trial suggests that PCI within 3 to12 hours after fibrinolysis is both safe and effective[36]. Therefore following fibrinolytic therapy, pa-tients should be routinely transferred for immedi-ate coronary angiography.
Transfer for Primary PCIThe DANAMI-2 trial compared primary PCI andfibrinolysis, specifically addressing the impact of pa-tients transferred to primary PCI centers [37]. Theprimary composite end point of death, reinfarc-tion, or disabling stroke was significantly decreasedby primary PCI compared with fibrinolysis in theoverall study cohort (13.7% vs. 8%, p � 0.001)as well as among patients treated in centers with-out catheterization facilities. The greatest benefit

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
10 Part I Coronary Artery Disease
of primary PCI was found in patients with a de-lay of more than 4 hours from symptom onset toreperfusion. The mean duration of inter-hospitaltransportation by ambulance was short (32 min-utes). These benefits of primary PCI over throm-bolytic therapy persisted at 3 years [38]. Overall,primary PCI is to be considered superior to throm-bolytic therapy if it can be performed within 110minutes of admission to the first hospital.
Delayed PCIIt has been suggested that delayed reperfusioncompared to medical therapy prevents unfavor-able ventricular remodeling. However, the TOATstudy (N = 66) suggested that late recanalizationof occluded infarct-related arteries (1 month postSTEMI) in symptom-free patients had an adverseeffect on remodeling despite showing a trend to im-proved exercise tolerance and quality of life [39].The recent OAT study (N = 2166) demonstratedthat late PCI (3 to 28 days post STEMI) in stable pa-tients did not reduce the occurrence of death, rein-farction, or heart failure compared to medical man-agement, with a trend toward an excess of rein-farction in the intervention group at 4-year follow-up [25]. The BRAVE-2 trial including 365 asymp-tomatic patients found a significant smaller infarctsize by scintigraphy among individuals randomizedto PCI between 12 and 48 hours following a STEMIcompared to those treated optimal medical therapyalone (infarct size 8% vs. 13%, p � 0.001) [28]. Inconclusion, delayed PCI following a STEMI shouldbe considered in patients at high risk such as thosewith heart failure, left ventricular dysfunction, ormoderate to severe ischemia.
Techniques of Reperfusion andAdjunctive Pharmacologic Treatments
Bare-Metal and Drug-Eluting StentsThe CADILLAC trial compared balloon angioplastyand stenting in the setting of STEMI [40]. No differ-ence in mortality or reinfarction rates was noted,but a significant decrease in ischemic target ves-sel revascularization (TVR) at 6 months favoredstenting. The TYPHOON study randomized 712patients to sirolimus-eluting stents or bare-metal
stents (BMS) [41]. The composite primary endpoint defined as target vessel–related death, recur-rent MI, or TVR was significantly lower in the drug-eluting stent (DES) group than in the BMS groupat 1 year (7.3% vs. 14.3%, p = 0.004). There wasno significant difference between the two groupsin the rate of death, reinfarction, or stent throm-bosis. At 2 years, the benefit persisted. A similarbenefit was observed in the MULTISTRATEGY trialcomparing sirolimus-eluting stents and bare-metalstents among 672 STEMI patients. Therefore, drug-eluting stents appear to be beneficial also in theSTEMI setting [42].
Embolic Protection Devices andThrombus AspirationDistal embolization, a frequent phenomenon in thesetting of primary PCI, is associated with reducedepicardial and/or tissue-level perfusion and latemortality. Neverthelesss, a strategy based on dis-tal emboli protection did not reduce events in theSTEMI setting in two randomized trials (EMERALD[43] and PROMISE [44]). The use of thrombec-tomy with the AngioJet device was not beneficialin the AiMI trial but the strategy will be assessedagain in the JETSTENT trial in patients with largethrombotic burden [45]. The TAPAS study ran-domized 1701 STEMI patients prior to angiographyto thrombectomy with an aspiration catheter orconventional primary PCI [46]. The study demon-strated a significant increase in rate of completeresolution of ST-segment elevation with the useof aspiration catheters. While the use of distalprotection devices is not recommended, aspirationcatheter-based thrombectomy should be routinelyperformed in the presence of a sizable thrombus.
Antithrombotic TherapyA detailed description of antithrombotic agents willfollow in the NSTEMI section of the chapter. Withrespect to STEMI, an initial loading dose of 162to 325 mg of uncoated acetylsalicylic acid shouldbe given immediately and continued indefinitelyat a dose of 75 to 162 mg/day [3]. The recom-mendations for clopidogrel were extrapolated fromthe PCI and the NSTEMI setting because no ran-domized trial has been performed in the primary

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
Chapter 1 Acute Coronary Syndromes 11
PCI setting. Patients should be loaded with 300 to600 mg of clopidogrel prior to PCI, and the treat-ment should be continued for up to 1 year at75 mg/day. Prasugrel is discussed below.
Glycoprotein IIb/IIIa InhibitorsThe use of glycoprotein (GP) IIb/IIIa receptor in-hibitors is well established and supported by ameta-analysis demonstrating a MACE reduction at30 days and 6 months [47]. In addition, multipleregistries have shown a mortality reduction associ-ated with the use of this class of agents [48,49]. Al-though the most-studied compound in STEMI hasbeen abciximab, a high-bolus dose of tirofiban maybe equally effective [42]. Recently however, theBRAVE-3 study questioned the value of GP IIb/IIIainhibitors in STEMI patients pretreated with clopi-dogrel [50]. Among 800 patients there was no dif-ference in left ventricular infarct size assessed bynuclear imaging. The HORIZONS AMI trial studied3602 patients with STEMI randomized to either bi-valirudin with provisional use of a GP IIb/IIIa in-hibitor, or to unfractionated heparin (UFH) plusa GP IIb/IIIa inhibitor prior to primary PCI [51].There was a significant reduction in the primaryend point of net adverse clinical events in the groupreceiving bivalirudin at 30 days, and even a reduc-tion in 30-day mortality. Bivalirudin appears to bea valid alternative to UFH plus GP IIb/IIIa inhibitorsin selected patients.
Summary of GuidelinesPrimary PCI, if performed in a timely fashion, isthe reperfusion therapy of choice in patients withSTEMI. However, since not all hospitals have theability to perform primary PCI, the choice of reper-fusion strategy should take into account the delaybetween primary PCI in another institution and im-mediate thrombolysis. PCI should be considered asthe preferred strategy if it can be achieved within90 minutes from the first medical contact. The 2007ACC/AHA/SCAI PCI guidelines concluded that fa-cilitated PCI is harmful. However, facilitated PCI us-ing regimens other than full-dose fibrinolytic ther-apy might be considered in patients with a lowbleeding risk and if PCI is not available within90 minutes. The optimal timing of routine angiog-
raphy and possible PCI after fibrinolytic therapy forSTEMI has not been determined, though a proce-dure at 3 to 12 hours appears to be both safe andeffective. Mechanical thrombectomy using an aspi-ration catheter at the time of primary PCI is recom-mended.
Non–ST-Elevation AcuteCoronary Syndromes
Epidemiology and Risk StratificationIn western countries, the ratio between NSTE-ACSand STEMI has switched over time, and currentlyNSTE-ACS is more frequent than STEMI. Registriesand surveys have estimated that the annual inci-dence of hospital admissions for NSTE-ACS is inthe range of 3 per 1000 inhabitants. With respect togender, approximately 40% of ACS patients in theUnited States are women. Overall, the in-hospitalmortality is generally higher for STEMI than forNSTE-ACS (approximately 7% and 5%, respec-tively). However, while in STEMI most events oc-cur before or shortly after presentation, in NSTE-ACS adverse events continue over days and weeks.As a consequence, the mortality rates at 6 monthsof both conditions become comparable (approxi-mately 12% and 13%, respectively). At 4 years, atwo-fold higher rate in the NSTE-ACS populationcompared to STEMI has been reported. The differ-ence in mid- and long-term evolution may be dueto different patient profiles. NSTE-ACS patients aregenerally older, have more comorbidities such asdiabetes and renal failure, and may have a moreadvanced stage of CAD and vascular disease.
A variety of parameters have been shown tohave independent predictive power for long-termischemic events in patients with ACS. Clinical pa-rameters include age, heart rate, blood pressure,Killip class, diabetes, history of prior MI, history ofCAD, ECG changes such as ST-depression, labora-tory parameters such as troponin, measurementsof renal function, BNP or NT-proBNP, and high-sensitivity CRP. Some of them have been groupedto form multiple risk stratification scores. However,only a limited number of scores are simple enoughto be useful in everyday practice. The GRACErisk score, recommended by the ESC 2007 ACS

c01 BLBK225-Meier October 14, 2009 20:18 Char Count=
12 Part I Coronary Artery Disease
guidelines as the preferred risk stratification tool,is based upon a large unselected international pop-ulation of patients presenting with NSTE-ACS andSTEMI and has been validated in several registriesfor prediction of in-hospital deaths and postdis-charge deaths at 6 months [52,53]. However, scorecalculation is complex and hardly doable at thebedside. As alternative is the TIMI risk score, whichincludes 7 variables: age � 65 years; � 3 riskfactors for coronary artery disease; prior coronarystenosis � 50%; ST-segment deviation on ECG atpresentation; � 2 anginal events in the 24 hoursprior to admission; use of acetylsalicylic acid in the7 days prior to admission; and elevated serumcardiac biomarkers [54].
Anti-Ischemic MedicationsIndependently of the revascularization strategychosen, pharmacologic options in ACS includeantianginal medication, anticoagulants, and an-tiplatelet agents. The role of antianginal medica-tions in the acute setting of NSTE-ACS is lim-ited. No randomized data support the use ofnitrates for prognostic reasons. Two randomizedtrials have compared beta-blockers to placebo inunstable angina, showing a modest 13% reduc-tion in the risk of progression to STEMI. The valueof beta-blockade in the acute phase of ACS wasfurther shaken by the recent COMMIT study, amega-trial showing no benefit of an early and ag-gressive beta-blocker treatment in STEMI patients[55]. Only small randomized studies have testedcalcium channel blockers in NSTE-ACS, and ameta-analysis failed to document a reduction in theprogression to STEMI or mortality. Nicorandil andivabradine have not been tested in ACS.
AnticoagulantsA pooled analysis of six trials testing UFH or low-molecular-weight heparin (LMWH) versus placeboor untreated controls in the setting of NSTE-ACSdemonstrated a significant 33% risk reduction at7 days for death or MI. [56] A meta-analysis of thesix trials comparing UFH and enoxaparin includingalmost 22,000 patients found no difference in mor-tality but a modest, though statistically significantbased on the large sample size, 9% relative risk re-
duction in the combined end point of death or MIat 30 days in favor of enoxaparin [57]. No signif-icant differences in blood transfusions or in majorbleeding were observed.
Fondaparinux is the only selective factor Xa in-hibitor approved for ACS. In the OASIS-5 trial,among 20,078 patients with NSTE-ACS, fonda-parinux or enoxaparin conveyed similar reductionin ischemic events at 9 days [58]. However, fon-daparinux therapy was associated with halving inmajor bleeding episodes. As a result, the compos-ite outcome of death, MI, refractory ischemia, ormajor bleeding was significantly reduced with fon-daparinux (7.3% vs. 9.0%). In addition, the mor-tality was lower in the fondaparinux group both at30 days (2.9% vs. 3.5%, HR 0.83, p = 0.02) and at6 months (5.8% vs. 6.5%, HR 0.89, p = 0.05). Inthe study most of the patients were treated conser-vatively. However, also among the 6238 patientswho underwent PCI, fondaparinux halved majorbleeding compared to enoxaparin (2.4% vs. 5.1%,HR 0.46, p � 0.00001) [59]. In the presence of sim-ilar rates of ischemic events among the two arms,this resulted in a superior net clinical benefit forfondaparinux (death, MI, stroke, major bleeding:8.2% vs. 10.4%, HR 0.78, p = 0.004). A sourceof great concern was the observation that catheterthrombus formation was more common in patientsreceiving fondaparinux (0.9%) than enoxaparin(0.4%), despite an additional intravenous dose offondaparinux at the time of cardiac catheterization.
The direct thrombin inhibitor bivalirudin wasassessed in 13,819 patients with moderate- tohigh-risk NSTE-ACS undergoing early angiographywithin the ACUITY trial, a randomized, open-labelstudy [60]. Three primary 30-day end points in-cluded composite ischemia (death from any cause,MI, or unplanned revascularization for ischemia),major bleeding, and net clinical outcome (com-posite of ischemic events and major bleeding). Pa-tients were randomized to one of three treatmentgroups: UFH or LMWH with GP IIb/IIIa inhibitors;bivalirudin with GP IIb/IIIa inhibitor; or bivalirudinalone. In a subsequent randomization process, GPIIb/IIIa inhibitors were administered either up-stream or at the time of PCI. There was no sig-nificant difference between standard UFH/LMWH