Current aspects of renal diseases in HIV infection · Current aspects of renal diseases in HIV...
53
Current aspects of renal diseases in HIV infection Eric DAUGAS Service de Néphrologie Hôpital Bichat – Paris France
Transcript of Current aspects of renal diseases in HIV infection · Current aspects of renal diseases in HIV...

Current aspects of renal diseases in HIV infection
Eric DAUGASService de NéphrologieHôpital Bichat – Paris
France
1996 = HAART highly active antiretroviral therapy
combination of three antiretroviral agents two RTI + one PI orthree RTIs
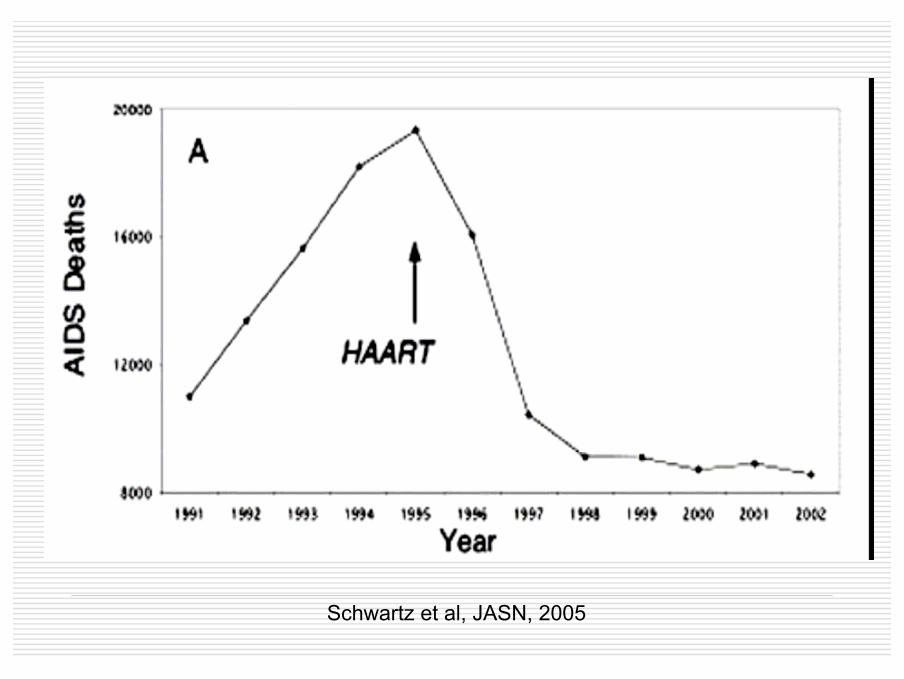
Schwartz et al, JASN, 2005

EPIDEMIOLOGYof
renal diseases in HIV infected patients
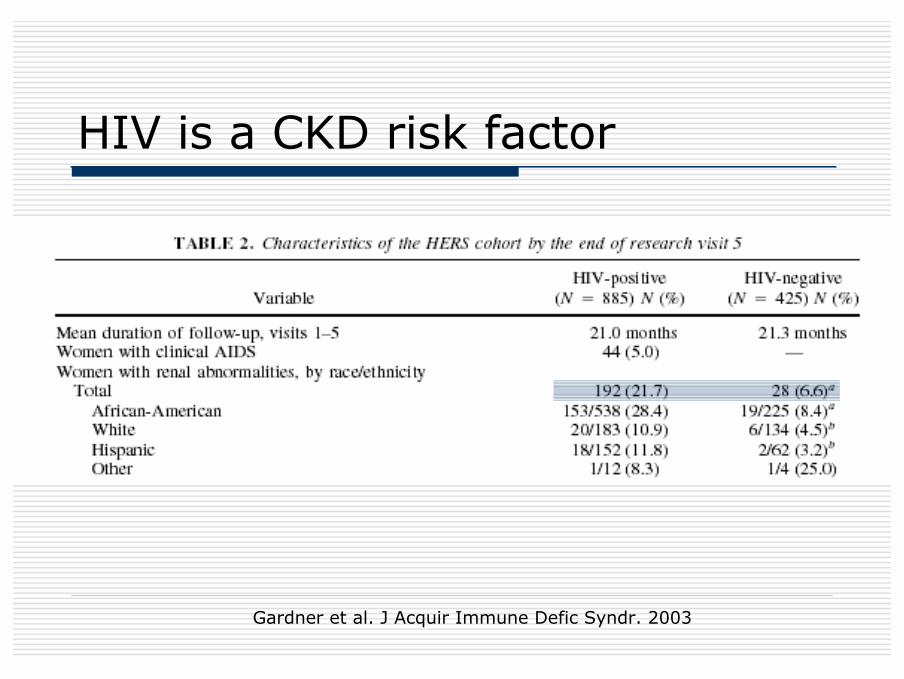
HIV is a CKD risk factor
Gardner et al. J Acquir Immune Defic Syndr. 2003

10%400Fernando SK, Am J Med Sci 2008
4%
Stage 3-5 CKD
29847Overton E, CROI 2007
29487Gupta SK, Clin Nephrol, 2004
32
Proteinuria%
n
2057 (w)Szczech LA, Kidney Int, 2002
High prevalence of CKD

CKD is associated with uncontrolledHIV
Proteinuria• Viral load• CD4 ≤ 200 mm3
• Afro-american • HCV
Renal failure• CD4 ≤ 200 mm3
• Viral load• Hypertension• Hypoalbuminemia
Szczech LA, Kidney Int, 2002

CKD = 3rd death risk factor in thisstudy
Gardner et al. J Acquir Immune Defic Syndr. 2003
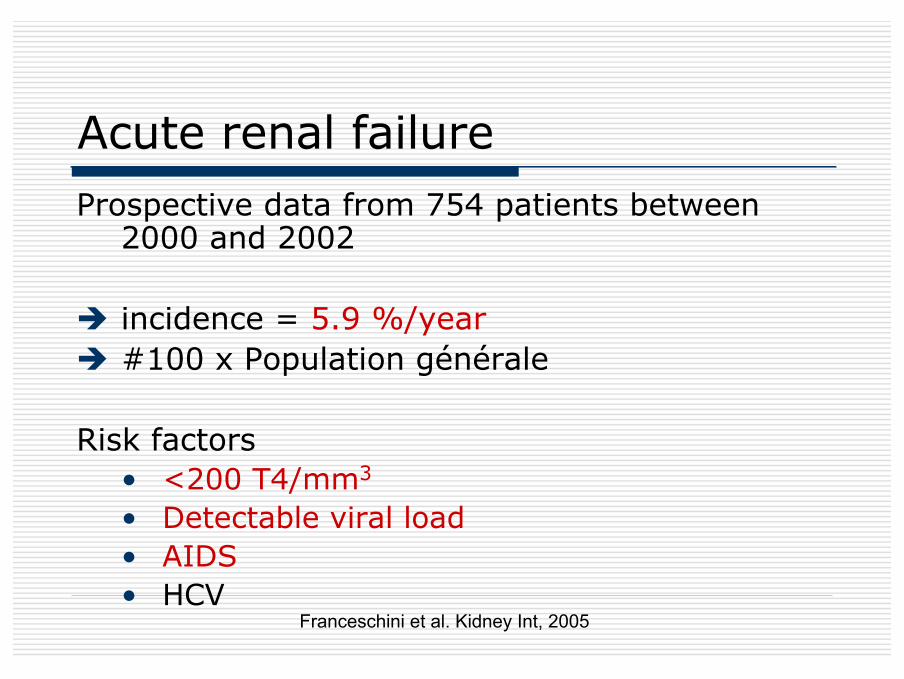
Acute renal failureProspective data from 754 patients between
2000 and 2002
incidence = 5.9 %/year#100 x Population générale
Risk factors• <200 T4/mm3
• Detectable viral load• AIDS• HCV
Franceschini et al. Kidney Int, 2005
Modifications of renal diseasesprofile in HAART era
New profile of kidney diseases in HAART era
• Improved control of HIV• Control of HIV-related renal diseases• Prolonged life with a continuous
exposure to HIV and to therapies• Immune reconstitution
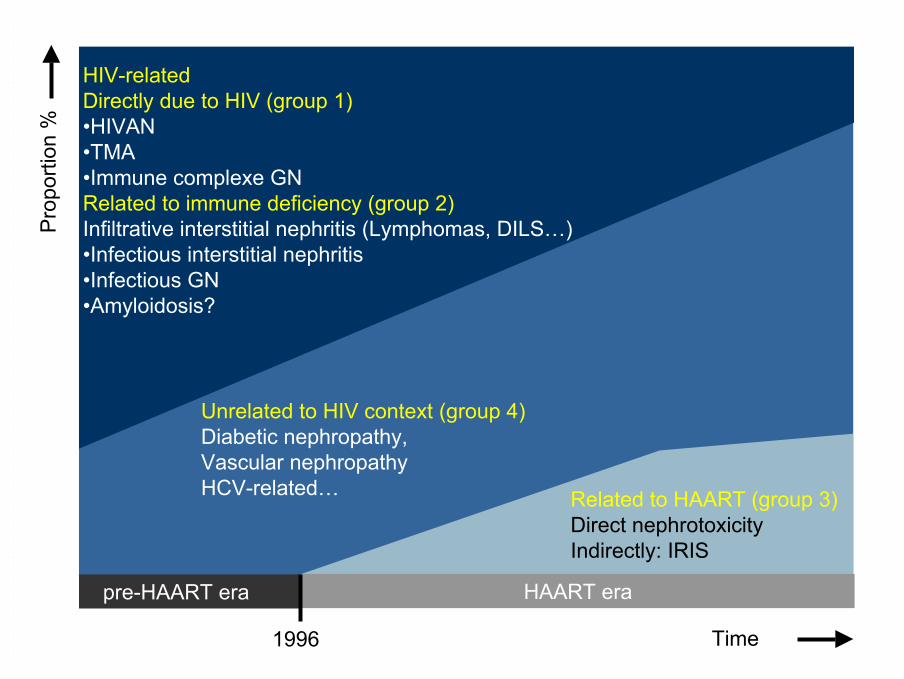
pre-HAART era
Pro
porti
on %
Time1996
HIV-related Directly due to HIV (group 1) •HIVAN•TMA•Immune complexe GNRelated to immune deficiency (group 2)Infiltrative interstitial nephritis (Lymphomas, DILS…)•Infectious interstitial nephritis•Infectious GN•Amyloidosis?
Related to HAART (group 3)Direct nephrotoxicityIndirectly: IRIS
Unrelated to HIV context (group 4)Diabetic nephropathy,Vascular nephropathyHCV-related…
HAART era
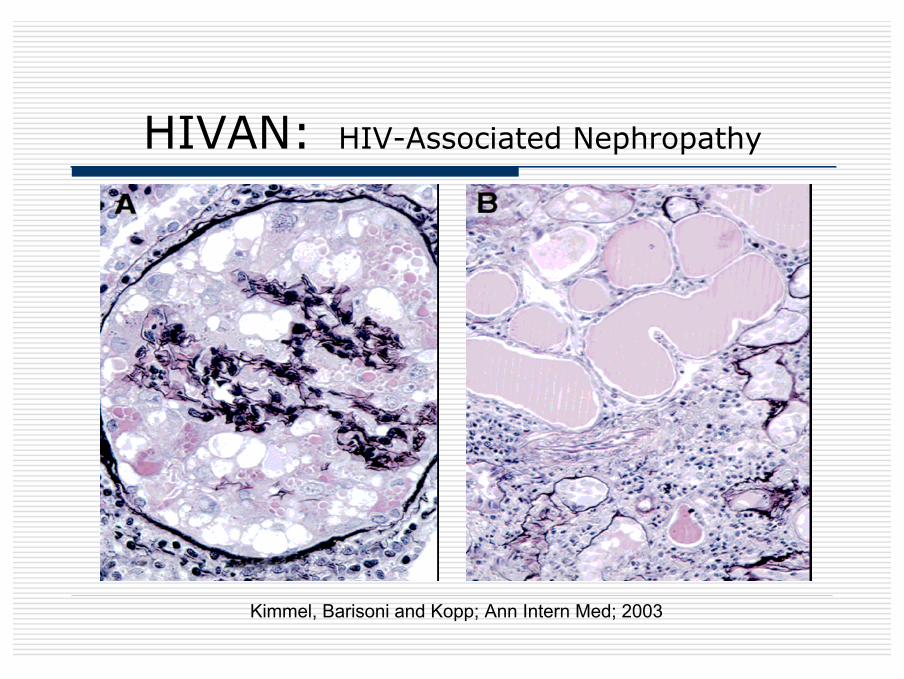
HIVAN: HIV-Associated Nephropathy
Kimmel, Barisoni and Kopp; Ann Intern Med; 2003

Beneficial effect of Zidovudine on HIVAN course in pre-HAART era
• Cook P.P, J Am Soc Nephrol 1990• Michel C., Nephron 1992• Ifudu O., Am J Nephrol 1995• Kimmel P.L, Am J Kidney Dis 1996
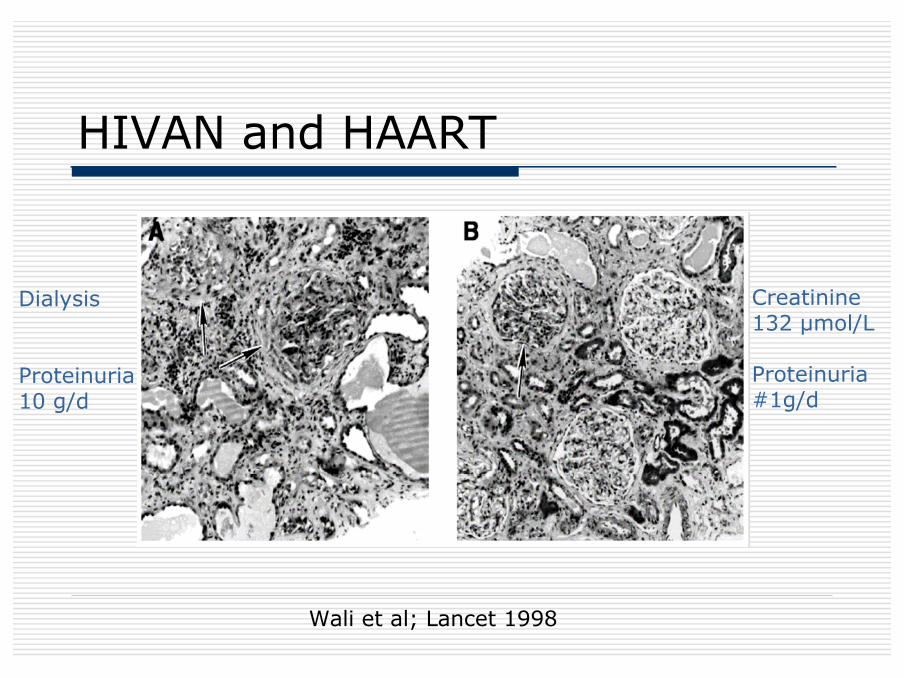
HIVAN and HAART
Wali et al; Lancet 1998
Dialysis
Proteinuria10 g/d
Creatinine132 µmol/L
Proteinuria#1g/d
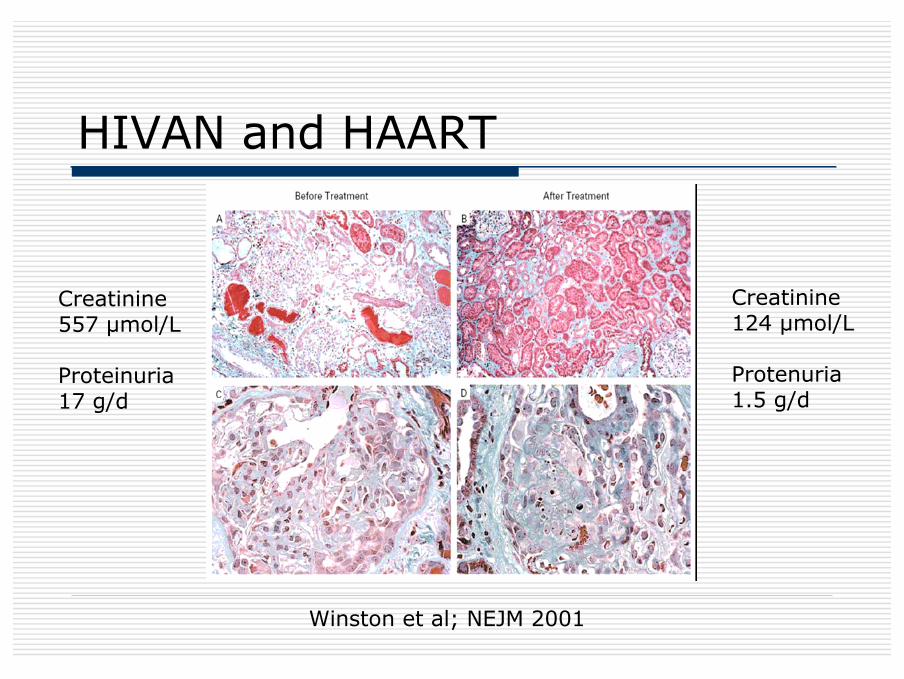
HIVAN and HAART
Winston et al; NEJM 2001
Creatinine557 µmol/L
Proteinuria17 g/d
Creatinine124 µmol/L
Protenuria1.5 g/d

HIVAN/HAART in African American
Lucas et al, AIDS, 2004
NRT a
lone
No A
RT
HAART
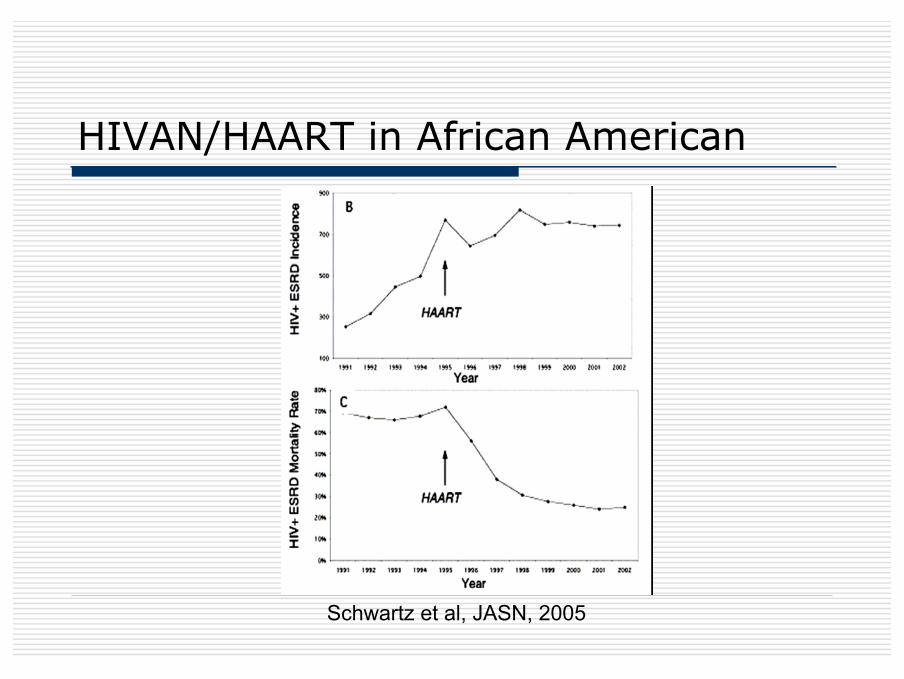
Schwartz et al, JASN, 2005
HIVAN/HAART in African American

HIVAN / HAART in Paris
HIVAN on histology
126 patients in pre-HAART eraMean creatinine 496µmol/L
versus33 patients HAARTMean creatinine 592µmol/L
Laradi et al, JASN 1998 and Burckle et al; Am Soc Nephrol; 2002
0102030405060708090
100
0,5 1 3
follow-up (year)
ren
al s
urv
ival
rat
e
1984-1996 1996-2000
Guidelines for HIVAN treatment
Gupta SK et al. Clin Infect Dis 2005
Immune glomerulonephritis
• Caucasians• Numerous nosologic entities
• IgA nephritis: 8% prevalence in Beaufilset al NDT 1995Eluted immune complex including IgAanti-HIV: Kimmel et al, NEJM 1992Treatment with HAART????
Thrombotic microangiopathy
Decreased incidence in HAART era
Gervasoni et al, Clin Infect Dis, 2002Becker et al, Clin Infect Dis, 2004
Direct and indirect effect of HIV containment by HAART
Renal toxicity of HAART
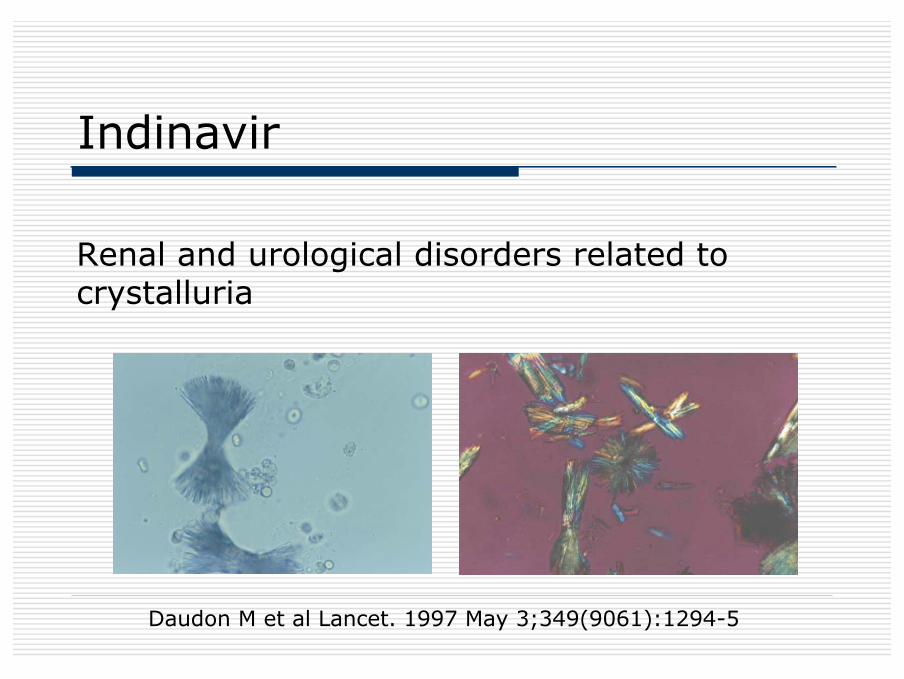
Indinavir
Renal and urological disorders related to crystalluria
Daudon M et al Lancet. 1997 May 3;349(9061):1294-5
Indinavir (Crixivan°)•Clinical manifestations
Renal colic /Flank pain / Dysuria/ Gross hematuriaUrolithiasis / radiolucent calculiRenal parenchymal defect / Papillary necrosis
Crystalluria / Leukocyturia / Microhematuria / Mild proteinuriaAcute renal failure / Chronic renal failureHypertension
•Histological findingsTubulointerstitial nephritis with indinavir crystals in tubules
Discontinuation in 33% of patients

Recommendations of the HIV MedicineAssociation of the Infectious DiseasesSociety of America
• Patients receiving indinavir should drink at least 1.5 L of water daily to prevent stone formation.
• Periodic monitoring of renal function and pyuria should be performed during the first 6 months of indinavir therapy and biannually thereafter,
• although routine screening for crystalluria is not warranted unless there is a suspicion of nephrolithiasis.
• Indinavir need not be withheld from patients with reduced renal function.
• In patients who develop indinavir nephrolithiasis, it would be reasonable to restart indinavir therapy once rehydration is achieved.
• Patients who develop indinavir-induced hypertension, pyuria, rhabdomyolysis, or renal insufficiency (acute or chronic) should permanently discontinue use of this drug.
Gupta SK et al. Clin Infect Dis 2005 Jun 1;40(11):1559-85.

AKIRitonavir (Norvir®)
Urolithiasis, renal colic Nelfinavir(Viracept®)
Cristalluria, renal colic, AKI and CKD Indinavir(Crixivan®)
Interstitial nephritis, urolithiasisAtazanavir(Reyataz®)
Renal toxicity of antiproteases
Daugas E et al., Kidney International, 2005 Izzedine H et al. AIDS, 2007
Nucleotide reverse transcriptase inhibitors: tenofovir
Dose dependent nephrotoxicityExacerbated by
advanced HIV disease, reduced GFR, no dosage adaptation to
reduced GFRconcurrent ritonavir or ddi, other nephrotoxic
5 to 12 months after starting tenofovir
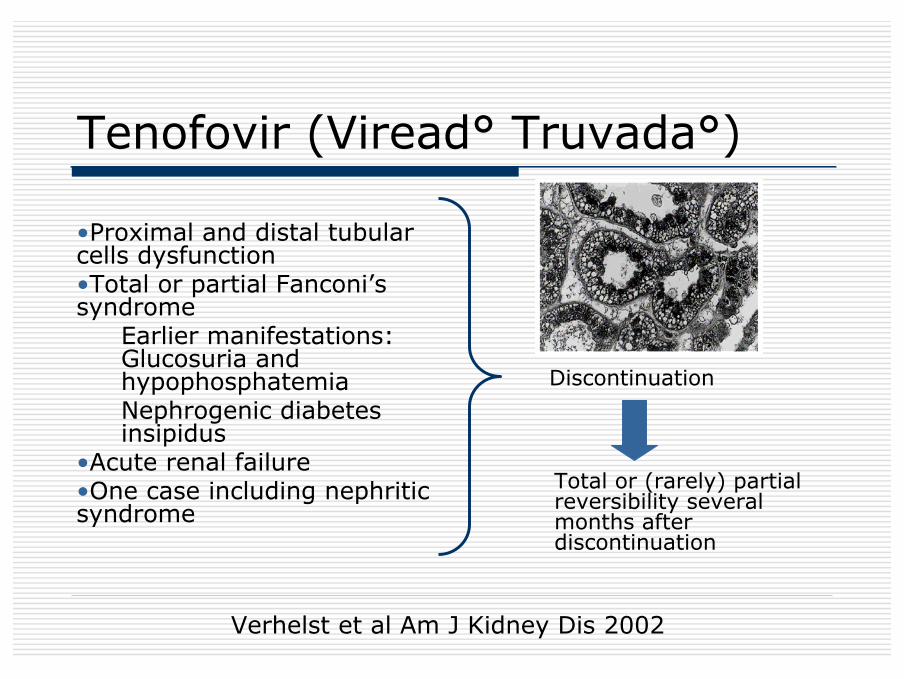
Tenofovir (Viread° Truvada°)
•Proximal and distal tubular cells dysfunction•Total or partial Fanconi’s syndrome
Earlier manifestations: Glucosuria and hypophosphatemiaNephrogenic diabetes insipidus
•Acute renal failure •One case including nephritic syndrome
Total or (rarely) partial reversibility several months after discontinuation
Discontinuation
Verhelst et al Am J Kidney Dis 2002
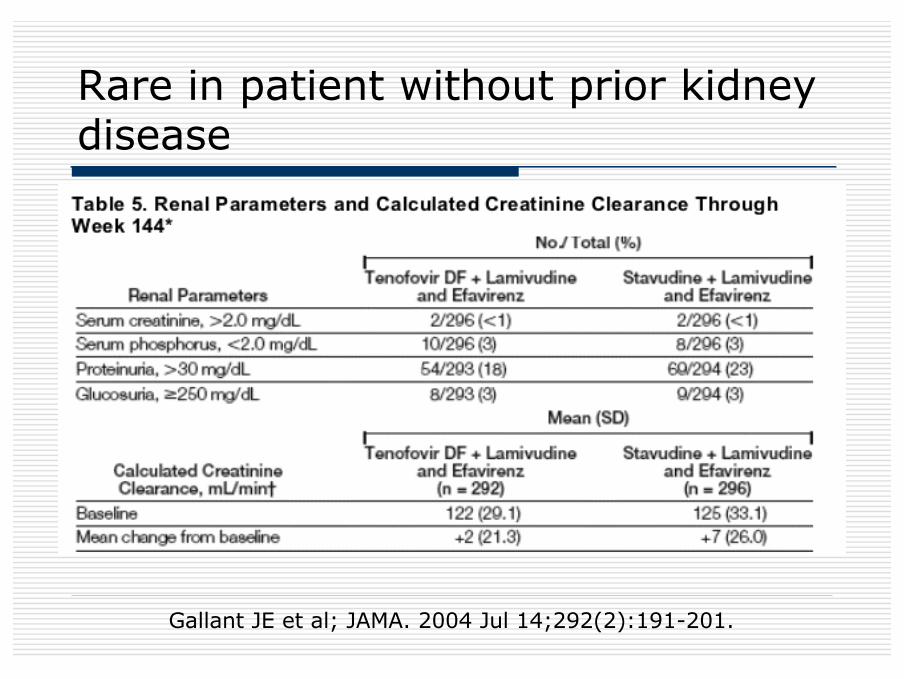
Rare in patient without prior kidneydisease
Gallant JE et al; JAMA. 2004 Jul 14;292(2):191-201.
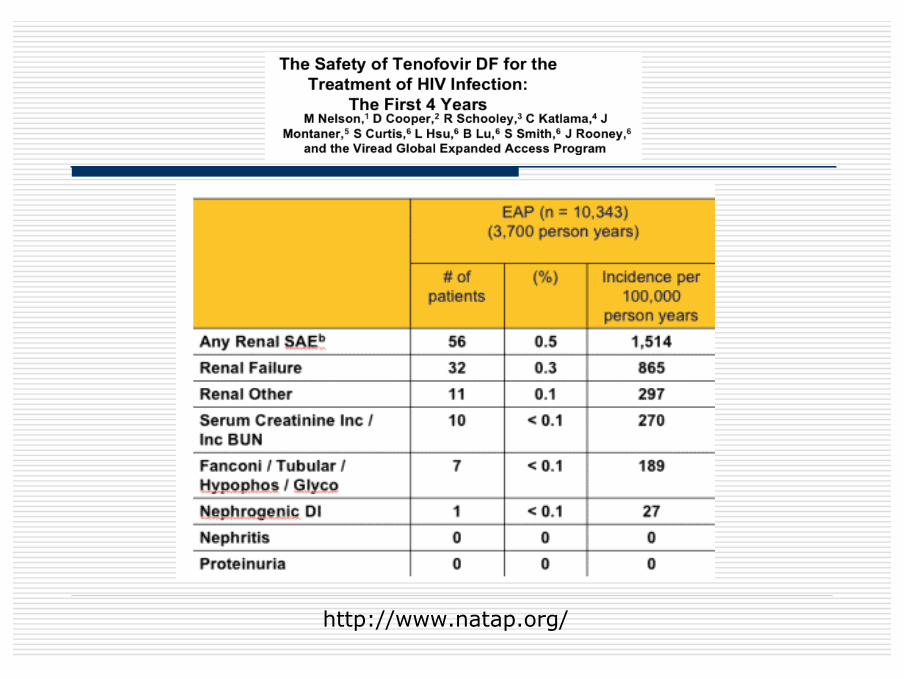
http://www.natap.org/
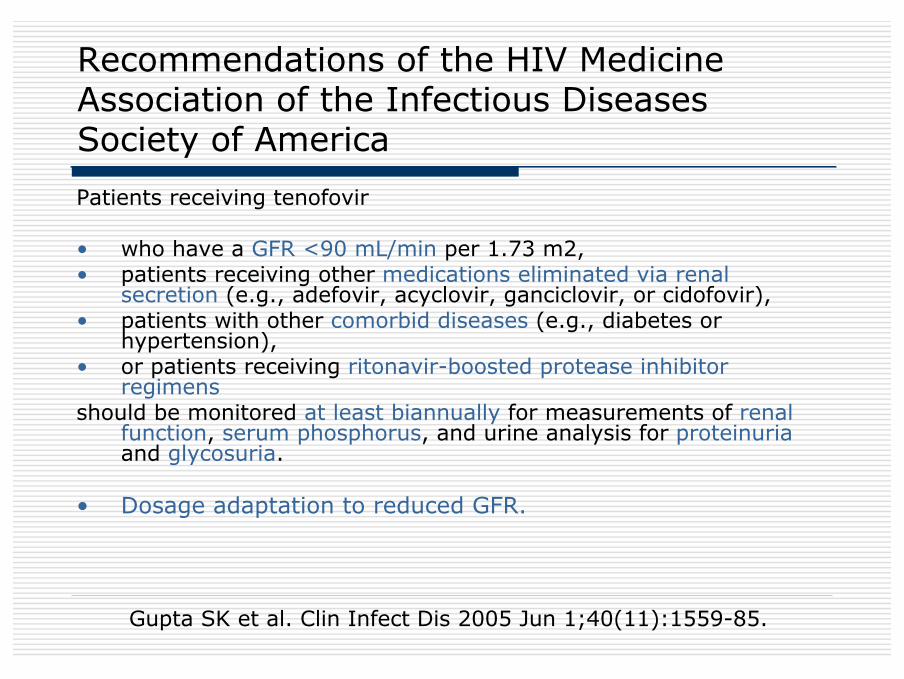
Recommendations of the HIV MedicineAssociation of the Infectious DiseasesSociety of America
Patients receiving tenofovir
• who have a GFR <90 mL/min per 1.73 m2, • patients receiving other medications eliminated via renal
secretion (e.g., adefovir, acyclovir, ganciclovir, or cidofovir), • patients with other comorbid diseases (e.g., diabetes or
hypertension), • or patients receiving ritonavir-boosted protease inhibitor
regimensshould be monitored at least biannually for measurements of renal
function, serum phosphorus, and urine analysis for proteinuriaand glycosuria.
• Dosage adaptation to reduced GFR.
Gupta SK et al. Clin Infect Dis 2005 Jun 1;40(11):1559-85.
Renal IRIS
Differential diagnosis of HAART renal toxicity
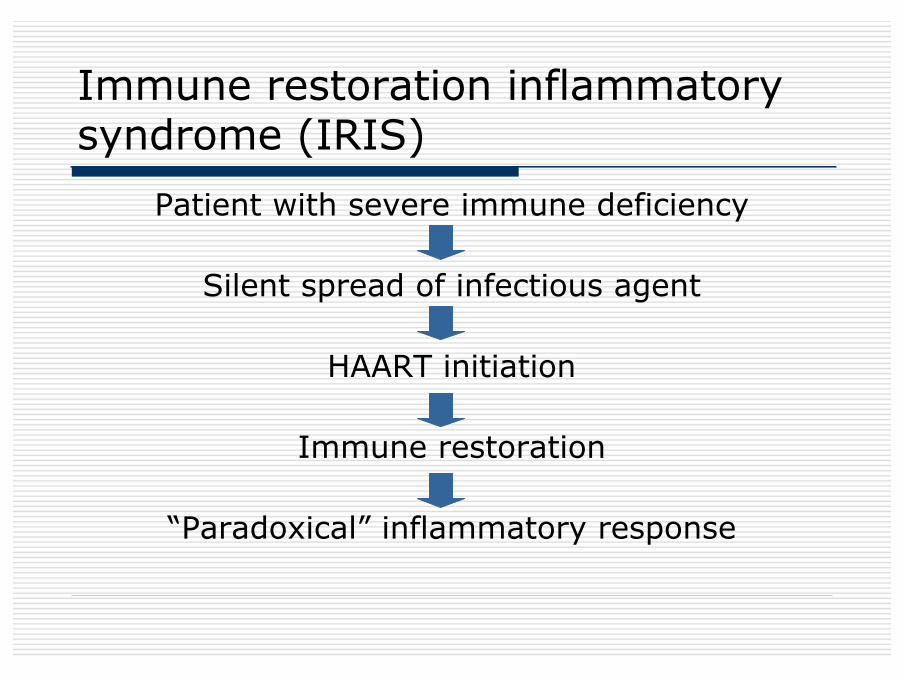
Immune restoration inflammatorysyndrome (IRIS)
Patient with severe immune deficiency
Silent spread of infectious agent
HAART initiation
Immune restoration
“Paradoxical” inflammatory response
IRISUp to 1/3 of patients coinfected with Mycobacterium
tuberculosis, MAC or Cryptococcus neoformans
Time between HAART and IRIS: #6-7 weeks
Risk factors• male gender• long duration and deep immunodeficiency• first introduction of HAART• short delay between treatment of opportunistic
infection and HAART• marked increase of CD4 T cell count and reduction of
HIV RNA level
Shelburne SA et al ; AIDS, 2005;19:399
IRIS: infectious agents and clinicalmanifestations
• Wide spectrum of pathogens• General manifestations• Visceral manifestations (hepatitis,
pneumonitis, encephalitis, lymphadenopathies, splenomegaly..)
• Life threatening in most severe cases• Management: continuation of HAART and
antiinfectious treatment, addition of antiinflammatory therapy: steroid therapy
Hirsch HH et al, Clin Infect Dis 2004;38:1159-
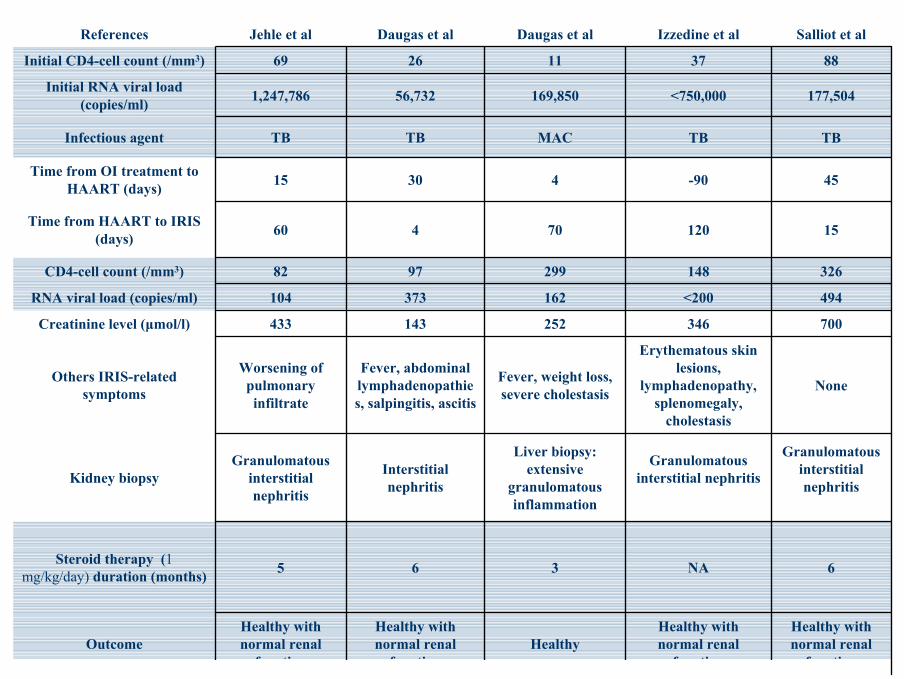
Healthy with normal renal
f ti
Healthy with normal renal
f tiHealthy
Healthy with normal renal
f ti
Healthy with normal renal
f tiOutcome
6NA365Steroid therapy (1 mg/kg/day) duration (months)
Granulomatous interstitial nephritis
Granulomatous interstitial nephritis
Liver biopsy: extensive
granulomatous inflammation
Interstitial nephritis
Granulomatous interstitial nephritis
Kidney biopsy
None
Erythematous skin lesions,
lymphadenopathy, splenomegaly,
cholestasis
Fever, weight loss, severe cholestasis
Fever, abdominal lymphadenopathies, salpingitis, ascitis
Worsening of pulmonary infiltrate
Others IRIS-related symptoms
700346252143 433Creatinine level (µmol/l)
494<200162373104RNA viral load (copies/ml)
3261482999782CD4-cell count (/mm3)
1512070460Time from HAART to IRIS (days)
45-90 43015Time from OI treatment to HAART (days)
TB TB MAC TB TB Infectious agent
177,504<750,000169,85056,7321,247,786Initial RNA viral load (copies/ml)
8837112669Initial CD4-cell count (/mm3)
Salliot et alIzzedine et alDaugas et alDaugas et alJehle et alReferences
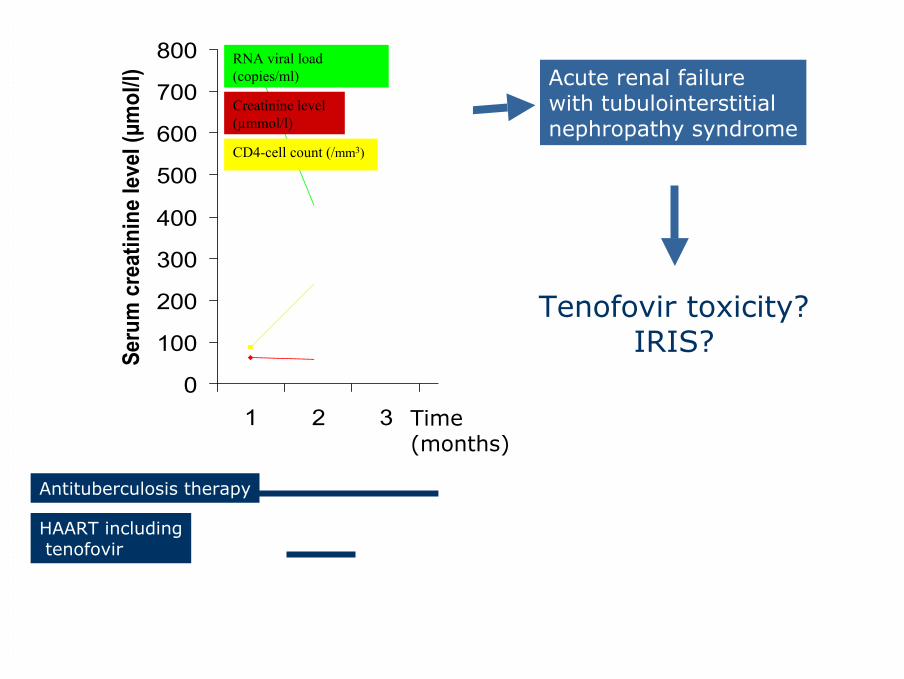
Case report
51-year-old Chinese manNo previous medical history
Disseminated tuberculosis revealed HIV-1CD4 cell 80/mm3 RNA viral load 177,504 copies/ml GFR 92 mL/min/ 1.73 m2 (creatinine: 62 µmol/L)
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7Time (months)
Seru
m c
reat
inin
e le
vel (
µmol
/l)
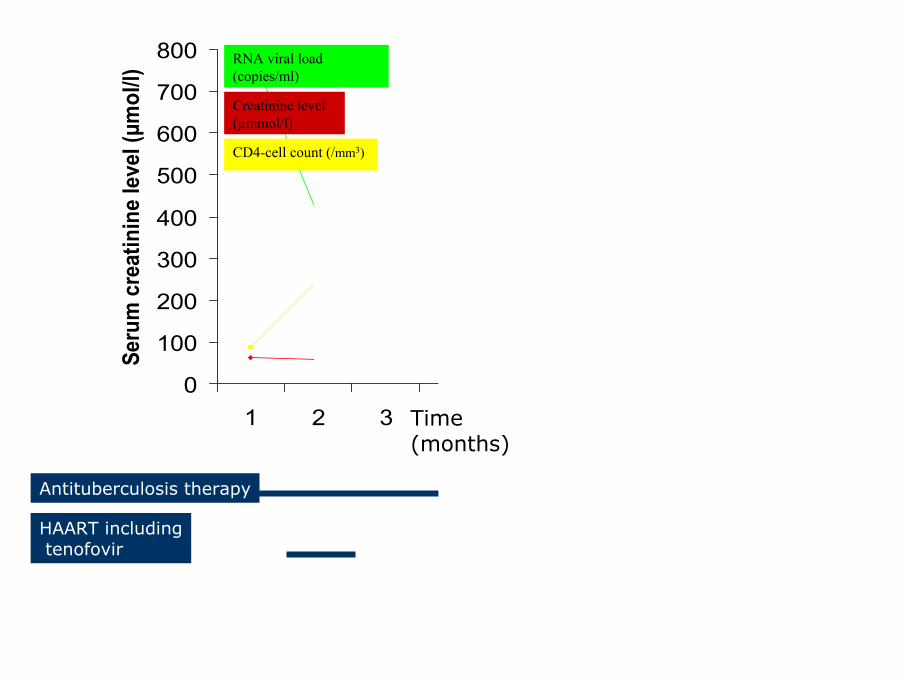
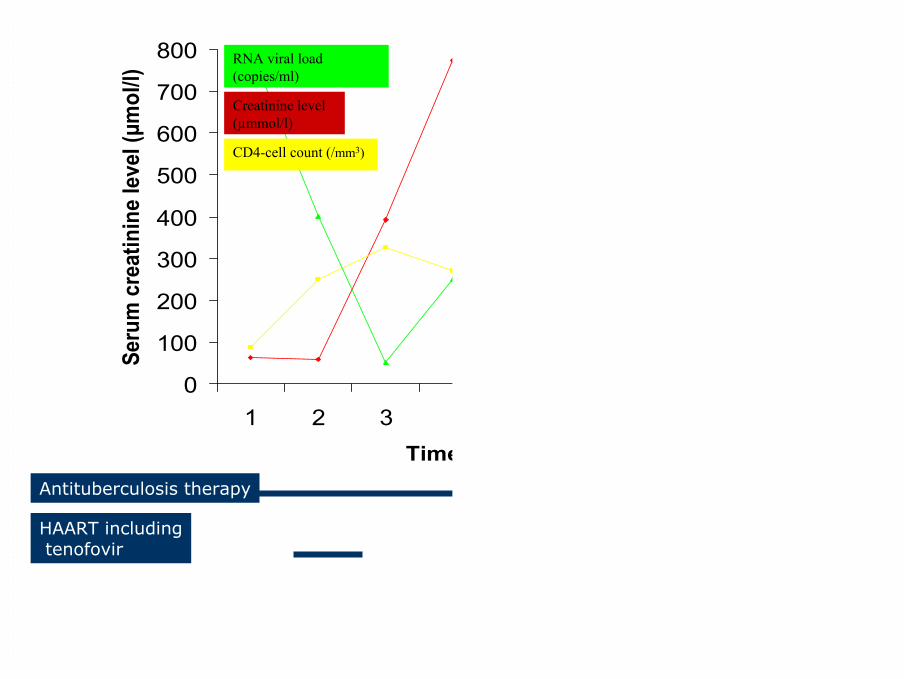
Antituberculosis therapy
HAART includingtenofovir
Time(months)
Creatinine level(µmmol/l)
RNA viral load(copies/ml)
CD4-cell count (/mm3)
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7Time (months)
Seru
m c
reat
inin
e le
vel (
µmol
/l)
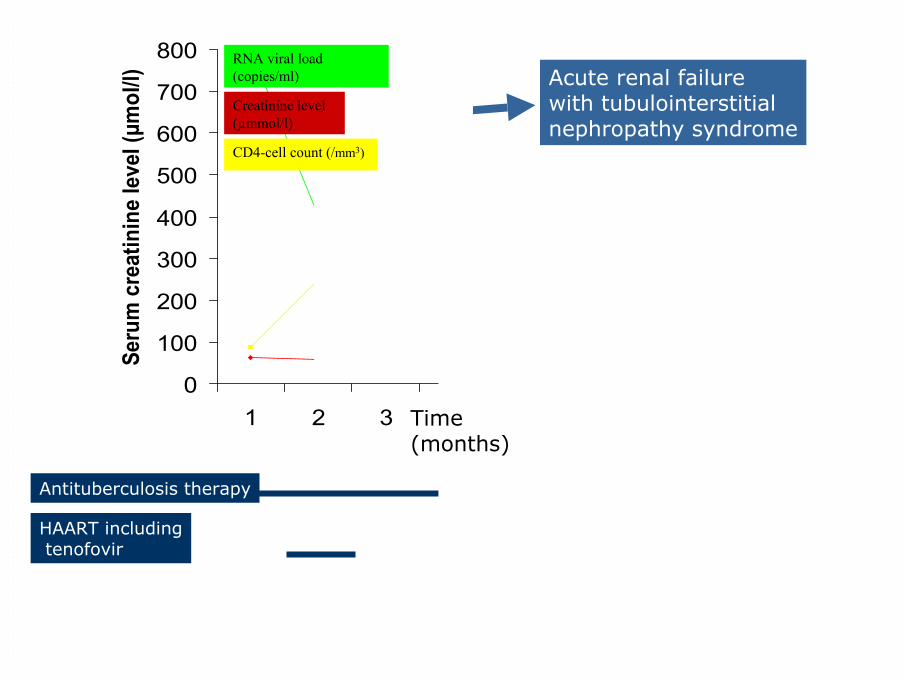
Antituberculosis therapy
HAART includingtenofovir
Time(months)
Creatinine level(µmmol/l)
RNA viral load(copies/ml)
CD4-cell count (/mm3)
Acute renal failurewith tubulointerstitial nephropathy syndrome
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7Time (months)
Seru
m c
reat
inin
e le
vel (
µmol
/l)
Antituberculosis therapy
HAART includingtenofovir
Time(months)
Creatinine level(µmmol/l)
RNA viral load(copies/ml)
CD4-cell count (/mm3)
Acute renal failurewith tubulointerstitial nephropathy syndrome
Tenofovir toxicity?IRIS?

0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7Time (months)
Seru
m c
reat
inin
e le
vel (
µmol
/l)
Antituberculosis therapy
HAART includingtenofovir
Time(months)
Creatinine level(µmmol/l)
RNA viral load(copies/ml)
CD4-cell count (/mm3)
Acute renal failurewith tubulointerstitial nephropathy syndrome
Tenofovir toxicity?IRIS?
Renal biopsy

J Vérine, Hôpital Saint-Louis, Paris
0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7Time (months)
Seru
m c
reat
inin
e le
vel (
µmol
/l)CD4-cell count (/mm3)
Creatinine level(µmmol/l)
RNA viral load(copies/ml)
Antituberculosis therapy
HAART includingtenofovir

0
100
200
300
400
500
600
700
800
1 2 3 4 5 6 7Time (months)
Seru
m c
reat
inin
e le
vel (
µmol
/l)CD4-cell count (/mm3)
Creatinine level(µmmol/l)
RNA viral load(copies/ml)
Antituberculosis therapy
HAART includingtenofovir
Prednisone
However HAART is beneficial
The Strategies for Management of Antiretroviral Therapy (SMART) trial
5472 patients, HIV, >350 CD4+/mm3
Open randomized controlled trial
• Continuous HAART« viral suppression group »
• Episodic HAARTif CD4<250/mm3 until > 350/mm3
« drug conservation group »
SMART study group, NEJM, 2006

After a mean followup of 16 months…
SMART study group, NEJM, 2006
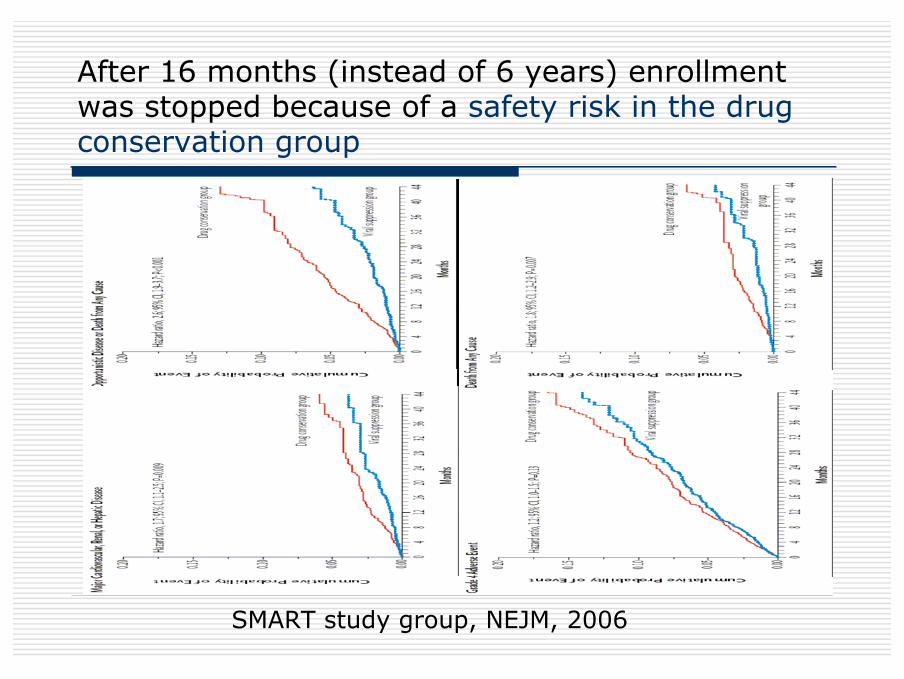
After 16 months (instead of 6 years) enrollmentwas stopped because of a safety risk in the drugconservation group
SMART study group, NEJM, 2006
Conclusion
Main treatment strategy for CKDis HAART
HAART at all stages including stage 5
HAART as early as possible
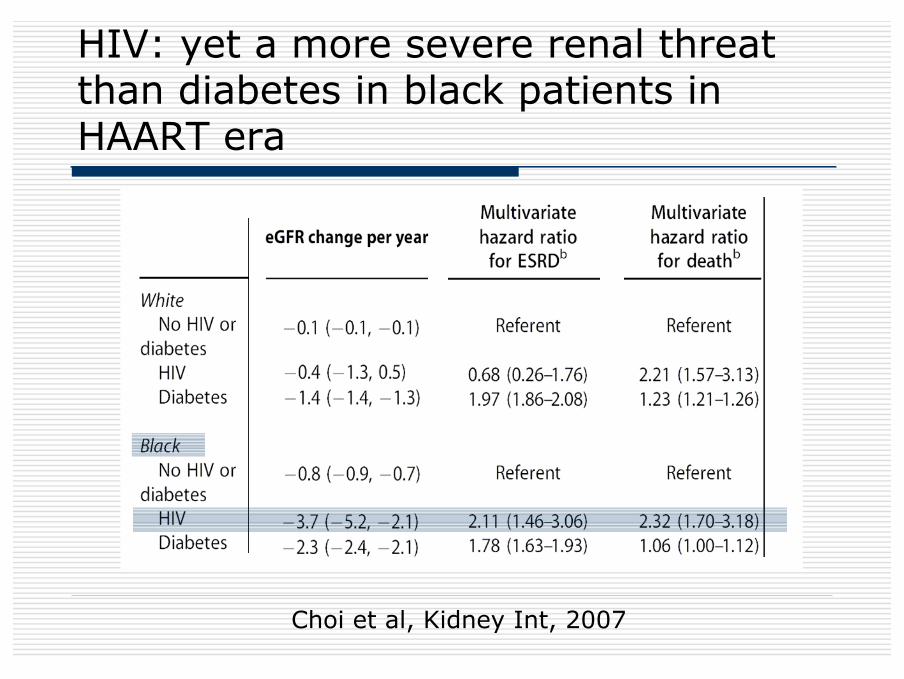
Choi et al, Kidney Int, 2007
HIV: yet a more severe renal threatthan diabetes in black patients in HAART era
Thank you