Cultural Awareness Issues in Chiropractic Faculty Development Day July 15, 2002 Cheryl Hawk, DC, PhD...
24
Cultural Awareness Cultural Awareness Issues in Chiropractic Issues in Chiropractic Faculty Faculty Development Day Development Day July 15, 2002 July 15, 2002 Cheryl Hawk, DC, PhD Cheryl Hawk, DC, PhD Director of Chiropractic Sciences Director of Chiropractic Sciences Dept. of Graduate Studies Dept. of Graduate Studies
-
Upload
teresa-cory-fletcher -
Category
Documents
-
view
214 -
download
0
Transcript of Cultural Awareness Issues in Chiropractic Faculty Development Day July 15, 2002 Cheryl Hawk, DC, PhD...
Cultural AwarenessCultural AwarenessIssues in ChiropracticIssues in Chiropractic
Faculty Faculty Development Day Development Day
July 15, 2002July 15, 2002Cheryl Hawk, DC, PhD Cheryl Hawk, DC, PhD
Director of Chiropractic SciencesDirector of Chiropractic SciencesDept. of Graduate StudiesDept. of Graduate Studies

DefinitionsDefinitions
• Culture:Culture: shared beliefs & values shared beliefs & values affecting affecting social interactionssocial interactions interpretation of experienceinterpretation of experience
• Race: Race: biological concept biological concept• EthnicityEthnicity : : self definedself defined group identity in group identity in
religionreligion nationality nationality cultureculture
Examples of different Examples of different cultures of chiropractic cultures of chiropractic
patientspatients• SexSex
male/female male/female sexual sexual
orientationorientation• AgeAge
childrenchildren adolescentsadolescents elderlyelderly
• Income/educationIncome/education• Race/ethnicityRace/ethnicity• ReligionReligion

What is “cultural competency”?What is “cultural competency”?
Set of skills, knowledge & attitudes Set of skills, knowledge & attitudes related to a clinician’srelated to a clinician’s understanding and respect for patients’ understanding and respect for patients’
values, beliefs, expectationsvalues, beliefs, expectations awareness of his/her own assumptions and awareness of his/her own assumptions and
value systemvalue system ability to adapt care to be congruent with ability to adapt care to be congruent with
patients’ expectations and preferences.patients’ expectations and preferences.

WHY should DCs be WHY should DCs be “culturally competent”?“culturally competent”?
• US population is increasingly US population is increasingly culturally diverseculturally diverse
• Different cultures have different Different cultures have different health behavior and health riskshealth behavior and health risks
• Doctor-patient communication and Doctor-patient communication and rapport are affected by cultural rapport are affected by cultural differencesdifferencesThis affects outcomes!This affects outcomes!

US population is US population is increasingly culturally increasingly culturally
diversediverse

Racial Racial Distribution of Distribution of US Population US Population
20002000
White White (72%)(72%)
HispaniHispanicc
Afr-AmAfr-Am
AsianAsian
Am. Am. IndianIndian

Are we keeping pace with Are we keeping pace with these changes?these changes?

US population vs chiropractic US population vs chiropractic patientspatients
% non-white/Hispanic% non-white/Hispanic
General population (1998)General population (1998) 28%28%
DC patients (1974-82)DC patients (1974-82) 4% 4%
DC patients (1997-98)DC patients (1997-98) 5%5%
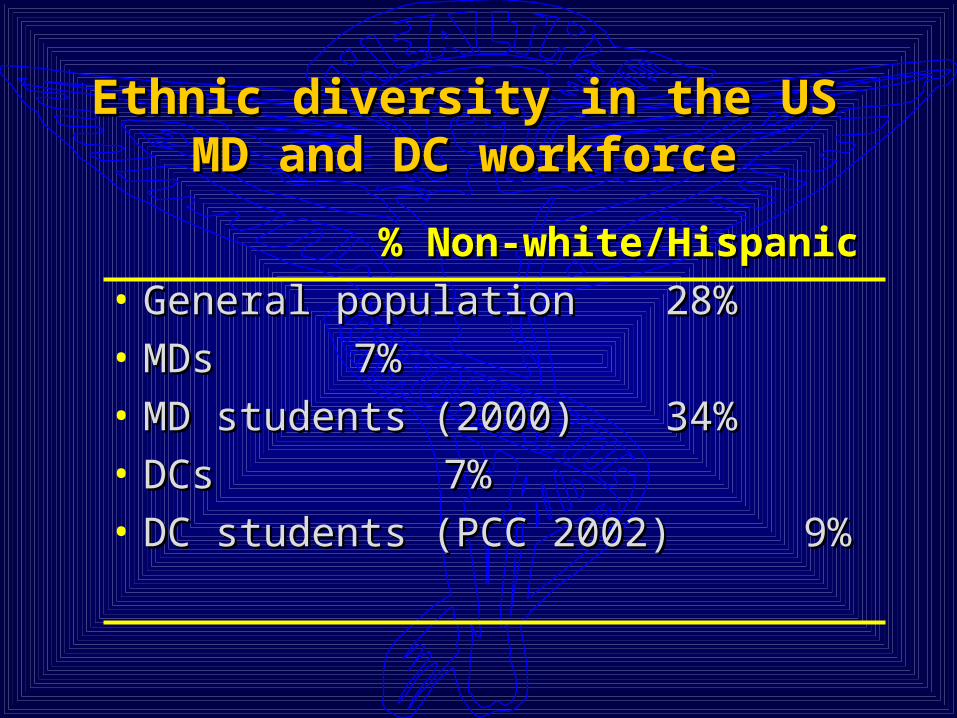
Ethnic diversity in the US Ethnic diversity in the US MD and DC workforceMD and DC workforce
% Non-white/Hispanic% Non-white/Hispanic• General populationGeneral population 28% 28%• MDsMDs 7% 7%• MD students (2000)MD students (2000) 34% 34%• DCsDCs 7% 7%• DC students (PCC 2002)DC students (PCC 2002) 9% 9%

US DCsUS DCs
19911991 1998 1998
FemaleFemale 13.3% 19.2% 13.3% 19.2% 51%51%
AsiaAsia nn 0.8 0.8 1.81.8 4 4
HispanicHispanic 1.6 1.6 1.71.7 1313
African AmericanAfrican American 0.5 0.5 0.60.6 1212
American IndianAmerican Indian 0.2 0.2 0.80.8 1 1
GenGen. . poppop..

and… and… why should we care?why should we care?
• Only Only 11%11% of all Americans see a of all Americans see a chiropractor annuallychiropractor annually
• Minority populations are not Minority populations are not benefiting from chiropractic carebenefiting from chiropractic care
• Chiropractic is not helping eliminate Chiropractic is not helping eliminate health disparitieshealth disparities
• Bottom line: Bottom line: it’s the right thing to it’s the right thing to do!do!

Different cultures have Different cultures have different health behavior and different health behavior and
health riskshealth risks

Examples of US Health Behavior Examples of US Health Behavior Differences: Differences: Reduced Physical Reduced Physical
ActivityActivity
• WomenWomen• Lower income/educationLower income/education• African-Americans and HispanicsAfrican-Americans and Hispanics• Older adultsOlder adults
by age 75, 33% men, 50% women by age 75, 33% men, 50% women have no physical activity at allhave no physical activity at all
Source: Healthy People 2010

Examples of US Health Examples of US Health Behavior Differences: Behavior Differences: overweight/obesity*overweight/obesity*
• ALL: 50%!!ALL: 50%!!• Lower income women and Lower income women and
adolescentsadolescents• African American/Mexican African American/Mexican
American womenAmerican women
*overweight: BMI 25; 25; obese: BMI obese: BMI 3030

Examples of US Health Examples of US Health Behavior Differences: Behavior Differences:
smokingsmoking• Among adolescents:Among adolescents:
39% white39% white 33% Hispanic33% Hispanic 20% African American20% African American
• Among adults:Among adults: Highest in Am. Ind., blue collar and Highest in Am. Ind., blue collar and
militarymilitary HS dropouts 3x rate of college gradsHS dropouts 3x rate of college grads

Examples of US Health Risk Examples of US Health Risk Differences: Differences: Chronic LB Chronic LB
DisabilityDisability
• Activity limitation, rate per 1000 Activity limitation, rate per 1000 adults:adults: AsianAsian 1515 HispanicHispanic 2828 WhiteWhite 3232 African AmericanAfrican American 3636 American IndianAmerican Indian 6868
by raceby race

Examples of US Health Risk Examples of US Health Risk Differences: Differences: Chronic LB Chronic LB
DisabilityDisabilityby income and by income and
educationeducation
poorpoor mid/mid/highhigh
2828
hs hs dropdrop
hs hs gradgrad
somsome e
collcollActivity limitation, rate per 1000 adultsActivity limitation, rate per 1000 adults
7777
2424
54543535

Examples of US Health Risk Examples of US Health Risk Differences: Differences: DiabetesDiabetes
0
5
10
15
20
25
WhiteWhite
8%8%
1414%%
1616%%
1818%%
Afr-AmAfr-Am Mex-Mex-AmAm
Am. Am. Ind.Ind.
a g e s 5 0 - a g e s 5 0 - 5 95 9

Examples of US Health Risk Examples of US Health Risk Differences: Differences: Unintentional Unintentional
InjuryInjury
• leading COD ages 1-44leading COD ages 1-44• ages 65+ higher rate for fireages 65+ higher rate for fire• all non-whites higher rate for fireall non-whites higher rate for fire• Males 2x-4x rate for drowning Males 2x-4x rate for drowning • American Indians 3x higher rate overallAmerican Indians 3x higher rate overall

Examples of US Health Risk Examples of US Health Risk Differences: Differences: Intentional Intentional
InjuryInjury
• Homicide 3rd COD ages 5-14Homicide 3rd COD ages 5-14• Homicide 2nd COD ages 15-24Homicide 2nd COD ages 15-24• Homicide rate for Afr. Am. aged 15-Homicide rate for Afr. Am. aged 15-
24 2x rate for Hispanics and 14x 24 2x rate for Hispanics and 14x rate for whitesrate for whites
• Suicide 3rd COD ages 15-24; whites Suicide 3rd COD ages 15-24; whites higher although Af. Am. rate risinghigher although Af. Am. rate rising
Doctor-patient communication Doctor-patient communication and rapport are affected by and rapport are affected by
cultural differencescultural differences

Cross-Cultural Communication BarriersCross-Cultural Communication Barrierson BOTH sides: doctor and patienton BOTH sides: doctor and patient
• Stereotypes affecting perceptionsStereotypes affecting perceptions• RolesRoles
authority figuresauthority figures gendergender familyfamily
• Personal vs. impersonal stylePersonal vs. impersonal style• Non-verbal cuesNon-verbal cues• LanguageLanguage• Respect (it’s a two-way street!)Respect (it’s a two-way street!)

Communication issuesCommunication issues
• Language (spoken and written)Language (spoken and written) Non-English speakersNon-English speakers Educational levelEducational level Acceptable topicsAcceptable topics
• VoiceVoice Loudness/pitchLoudness/pitch SilenceSilence
• Body languageBody language personal spacepersonal space touchtouch gestures/facial expressionsgestures/facial expressions eye contacteye contact










![A Consumer’s Guide to Chiropractic Care · California Board of ChiropraCtiC ExaminErs [ 3 ] What is a Chiropractic Adjustment and Chiropractic Care? A chiropractic adjustment is](https://static.fdocuments.net/doc/165x107/5afc83ce7f8b9a68498b9600/a-consumers-guide-to-chiropractic-board-of-chiropractic-examiners-3-what.jpg)