
CT GE Healthcare
76
clarity CT GE Healthcare imagination at work Delivering Quality Care with the New Optima CT660: From Vision to Reality Page 12 THE MAGAZINE OF CT • NOVEMBER 2011 Veo: Understanding the Impact of Iterative Reconstruction Page 54 Pediatric Hospitals Bring Low-dose CT to the Middle East Page 39 Apple
Transcript of CT GE Healthcare

clarityC T
GE Healthcare
imagination at work
Delivering Quality Care with the New Optima CT660: From Vision to RealityPage 12
T H E m a G a z i N E O F C T • N O V E m B E R 2 0 1 1
Veo: Understanding the impact of iterative ReconstructionPage 54
Pediatric Hospitals Bring Low-dose CT to the middle EastPage 39
apple

2 A GE Healthcare CT publication • www.ctclarity.com
T A b l E o f C o n T E n T s
Publications Team
Kelley Knutson & Jodi YoungCT Clarity EditorsCT Education Managers
Jennifer MaGlobal Marketing Communications LeaderCT and Advantage Workstation
Mary Beth MassatWriter / Editorial Consultant
Nilesh ShahChief Marketing Officer, CT
IntegréDesign/Production
GE Contributors
Andrew AckermanCT Marketing Manager, Performance Segment, Americas
Olivier AddaCT Super Premium Strategic Product Manager, Europe, Middle East & Africa
Dr. Karthik AnantharamanCT Marketing Manager, South Asia
Christophe ArgaudModality Manager, CT, France
Paul Ayestaran Advanced Applications Specialist, Europe, Middle East & Africa
Chelsea BeelerCommunications Manager
Khodor BerroCT Modality Sales Specialist, Kingdom of Saudi Arabia
Nitin BhardwajClinical Applications Specialist, CT, India
Chuck BisordiCT Product Development Specialist
Valerie BrissartCT Marketing Director, Europe, Middle East & Africa
Eugene CharlestonAW Server Product Leader
Kenneth Denison, PhDCT Dose Leader
Melissa DesnoyersClinical Project Manager, CT
Paul EdwardsAW Product Manager
Jennifer EspositoDirector, Dose Services, Americas
Amanda FoxCT Product Developent Specialist
Benjamin FoxGlobal Public Relations Manager
Enrique Garcia-MuñizCT Marketing Manager, Latin America
Laurent GuiralCT & AW Cardiac Clinical Leader, Europe, Middle East & Africa
DeAnn HaasCT Marketing Manager, Leadership Segment, Americas
John JaeckleRegulatory Affairs Manager, MI & CT
Melissa Megumi Shiraishi KurikiCT Advanced Applications Specialist, Latin America
Elena LimCT Product Marketing Leader, Value Segment
Clinical Value: High-Definition CT Improves Triage and Door-to-treatment Times in Emergency Radiology page 34
Customer Spotlight: Seeing Beyond the Naked Eye page 16
GE Healthcare News
Welcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
CT Clarity, the Magazine of CT, Goes Digital . . . . . . . . . . . . . . . . .5
GE Launches New CT Low-dose Webinar Series . . . . . . . . . . . . .5
MD Connect: Connecting Your Oncology Team With Applications… Anywhere . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Low-dose CT Coming to Brazil . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Dose Check Aids Hospitals in Regulating Patient Dose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
General Electric to Expand in Russia With New Joint Ventures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Optima CT660: Taking Performance to a Whole New Level . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Customer Spotlight
A CT Designed for Broader Access . . . . . . . . . . . . . . . . . . . . . . . . .9
Delivering Quality Care: From Vision to Reality . . . . . . . . . . . 12
Seeing Beyond the Naked Eye . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Clinical Value
Meeting the Clinical Need for Low-dose Cardiac Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Implementing Ultra-low Dose CT with Veo at University Hospital, Brussels . . . . . . . . . . . . . . . . . . . . . . . . . . 21
BrightSpeed Elite with IQ Enhance Delivers Speed and Clarity in the Carolinas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
GE Healthcare News: Optima CT660: Taking Performance to a Whole New Level page 8

3www.gehealthcare.com/ct • November 2011
t a b l e o f c o N t e N t s
Emerging Applications in Musculoskeletal CT Imaging . . . . 27
4D CT With Respiratory Gating Helps Locate and Track Lesions to Reduce Target Volumes . . . . . . . . . . . . . 32
High-Definition CT Improves Triage and Door-to-treatment Times in Emergency Radiology . . . . . . . . 34
Pediatric Hospitals Bring Low-dose CT to the Middle East . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Case Study
Low-dose CTA With ASiR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Confirming a Diagnosis of Double Aortic Arch in a Newborn . . . . . . . . . . . . . . . . . . . . . . . . 46
Critical Low-dose Neuro Imaging with ASiR . . . . . . . . . . . . . . 48
Multi-modality Oncology Workflow for Comprehensive Follow-up and Treatment . . . . . . . . . . . . 50
Technical Innovation
Understanding the Impact of Iterative Reconstruction . . . 54
Integration and Information the Cornerstone of Radiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Photon Counting: A New CT Technology Just Over the Horizon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Beyond the Scan
Comprehensive Dose Management Services and Solutions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
Does my Patient Need a CT Scan? . . . . . . . . . . . . . . . . . . . . . . 70
Worldwide Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
© 2011 General Electric Company, doing business as GE Healthcare . All rights reserved . The copyright, trademarks, trade names and other intellectual property rights subsisting in or used in connection with and related to this publication are the property of GE Healthcare unless otherwise specified . Reproduction in any form is forbidden without prior written permission from GE Healthcare .
LIMITATION OF LIABILITY: The information in this magazine is intended as a general presentation of the content included herein . While every effort is made by the publishers and editorial board to see that no inaccurate or misleading data, opinion or statements occur, GE cannot accept responsibility for the completeness, currency or accuracy of the information supplied or for any opinion expressed . Nothing in this magazine should be used to diagnose or treat any disease or condition . Readers are advised to consult a healthcare professional with any questions . Products mentioned in the magazine may be subject to government regulation and may not be available in all locations . Nothing in this magazine constitutes an offer to sell any product or service .
Colleen LockwoodCT Global Marketing Manager
Dusty Majumdar, PhDCT Marketing Manager, Premium Segment, Americas
Holly McDanielCT Product Development Specialist
Andrew MendenRegulatory Affairs Leader
Phil MohCT Masters Series Coordinator
Daniel Morris CT Global Marketing Manager
Vincent NorlockCT Global Marketing Manager
Alyssa NowakCT Product Development Specialist
Christoph ObermeierCT Clinical Education Manager, Europe, Middle East & Africa
Gobinda PalProduct Specialist, CT, India
Karen ProcknowCT Product Development Specialist
Linda PucekCT Segment Marketing Manager, Oncology, Americas
Rick RabySales Specialist, CT
Muhammad Sadiqur RahmanProduct Specialist, CT, Bangladesh
Sundar RKCT Clinical Applications Manager, India
Dario SalvadoriCT Performance & Value Strategic Product Manager, Europe, Middle East & Africa
Mark SemischLead Counsel, GE Healthcare Systems
Stephen SlavensRegulatory Affairs Director, AW
J. Eric StahreGeneral Manager, Global Premium CT
Laurent StefaniGlobal AW Marketing Manager
Andras SzentmiklossyGlobal Product Manager, Oncology
Cristian Toader, PhDCT Premium Strategic Product Manager, Europe, Middle East & Africa
Melhem YounanCT Clinical Leader, EAGM
Pengcheng ZhangMarketing Manager, Oncology
Patricia ZoltowskiCT Education Leader
*Trademark of General Electric Company .
iPad and iPhone are registered trademarks of Apple, Inc .
Android is a trademark of Google, Inc .
Beyond the Scan: Comprehensive Dose Management Services and Solutions page 68
Case Study: Confirming a Diagnosis of Double Aortic Arch in a Newborn page 46
Technical Innovation: Photon Counting: A New CT Technology Just Over the Horizon page 64

4 A GE Healthcare CT publication • www.ctclarity.com
G E H E A lT H C A r E n E w s w E l C o m E
In this issue of CT Clarity, we share our customers’ stories on
how these commitments improve their day-to-day clinical
practice and research: How they are achieving high-quality
diagnostic exams with lower dose thanks to ASiR* and Veo*;
what the impact of high-definition imaging means for their
patients’ diagnoses and treatments; how implementing tools
can enhance workflow and raise clinical productivity to new
levels while expanding clinical collaboration; and, why it is
important to embrace the next era of CT innovation with
spectral dual energy and low-dose imaging.
We have only just begun.
Across the industry—from manufacturer to provider—we are all
more cognizant of the importance of ensuring that CT imaging
produces substantial benefits. In fact, the ability to reduce dose
without affecting image quality is the first thing our customers
say they need. Together, with our clinical partners, we are
exploring the future of low-dose imaging. In one of the first
global, multi-site, clinical trials of its kind, Dr. Rendon Nelson and
Dr. Ehsan Samei are leading the effort to determine, by body part
and anatomy, the dose reduction potential of Veo. Their initial
impression of Veo—it’s a positive game changer.
Professor Johan de Mey also shares his experience with Veo. It
is interesting to note that two stories—from opposite ends of
the world—convey a similar message: the value of Veo extends
beyond its low-dose capabilities. While the images Veo produces
are clearly different from filtered back projection (FBP), these
clinicians report seeing more information in the Veo images
than in FBP. Couple that with the potential to conduct CT scans
at previously unattainable low-dose levels, and the future of
CT looks promising indeed.
Our low-dose initiative involves more than just Veo and ASiR,
however. We’re introducing DoseWatch in conjunction with
comprehensive dose management services and solutions. At GE,
our low-dose CT approach is multi-faceted, including technology,
education, training, and implementation. We’re excited to provide
you with an array of tools that will help you conduct high-quality
CT studies at ultra-low doses.
The near future is even brighter. We continue to build upon
the foundation of Gemstone* Spectral Imaging (GSI) and high
definition (HD) to address current challenges in CT cardiac
imaging. Additionally, this year at RSNA we will display the
Discovery* CT750 HD FREEdom Edition (commercially available
only outside of the US), which is being designed to provide a new
standard in cardiac imaging.
As excited as we are for tomorrow’s advancements, we understand
that there are clinical demands and questions that our customers
need addressed today. Our customers have told us they need
better CT imaging workflows that enhance productivity and
clinical collaboration. Last issue, we introduced you to the
Dexus* workflow. In this edition, Dr. William Shuman shares his
experience with Dexus and why it is important not just for radiology
productivity, but for enhancing access to clinical information
and applications in any location, at any time. You can also read
Dr. Valerie Laurent’s case study on how OncoQuant*, part of
the Dexus family, has made a difference in oncology follow-up
and treatment.
GE’s investment in CT spans the world. We can be a better leader
by listening to our customers from every corner of the globe,
sharing the challenges they face each day, and addressing them
through innovation, research, and development. For many clinicians
throughout the world, offering access to CT imaging is the challenge.
The Brivo* CT315§ and CT325§ are helping to bridge this gap with
high-quality, cost-efficient CT systems. Our customers in India and
China share their initial experiences with the Brivo CT325 and the
impact on patient care.
And, you’ll read how hospitals are able to take their performance to
a whole new level with our exciting new Optima* CT660. Customers
in India, South America, France, and the US are using the
healthymagination and ecomagination validated Optima CT660
to improve their workflow, increase patient and referring physician
demand, enhance patient care, and optimize dose with ASiR.
Together with you, great care by design is attainable for all
countries, cultures, and people. And, if you can’t join us at RSNA
2011, I hope you’ll join us virtually at www.gehealthcare.com to
learn more about how we can all make an impact on the future
of healthcare through CT imaging.
Read on, enjoy, and thanks for your continued support. And,
don’t forget to check out the new digital edition of CT Clarity. n
Leadership, Excellence in Patient Care, ProductivityThree commitments that guide both GE Healthcare CT and our clinical partners
*Trademark of General Electric Company.§Brivo CT315 and CT325 are not for sale in the United States.
Not cleared by the US FDA.
Steve Gray, Vice President and General Manager,
Computed Tomography, GE Healthcare

5www.gehealthcare.com/ct • November 2011
a N N o u N c e m e N t s g e h e a lt h c a r e N e w s
GE Launches New CT Low-dose Webinar Series
Get the latest CT clinical, technical, and operational news
digitally—on the Web, iPad, iPhone, or Android tablet and phone.
CT Clarity is now available online at www.ctclarity.com.
Download the tablet and smartphone applications free of
charge at the Apple Store (www.apple.com) or Android Market
Apps (www.market.android.com). Or, simply scan the QR codes
with your smartphone!
Don’t miss exclusive content that can’t be found anywhere else—
videos, interviews, and expanded clinical images and cases. Easily
search for keywords and hot topics to locate the content that
interests you the most. Share links to articles via email or quick
links to social networks. You can still download the magazine as
a PDF for offline reading. Watch for updates to your app with the
latest news from GE CT. n
For over three decades, GE has been empowering clinicians
and technologists with radiation dose-reducing techniques. This
commitment included innovative education offerings that enable
our customers to maximize their use of these technologies to
image at doses consistent with the ALARA principle. GE will
continue to offer dose education through accredited webinars
that feature a variety of experts who share their experience on
reducing radiation dose. This content is now available to our
customers via the new CT Low-dose Webinar series.
GE offers six modules approved by the ASRT for Category
A CE credits (4.5 total credits):
• Radiation Dose—Current Issues and New Techniques;
• Reducing Radiation Risk in CT Scans for Children;
Download your CT Clarity magazine today at www.ctclarity.com or get your free CT Clarity app at www.apple.com and www.market.android.com. »
• Fundamentals of CT and Radiation Dose;
• Dose Reduction Techniques for Cardiac CT;
• Neuroimaging Considerations; and
• Techniques for Reducing CT Radiation Dose. n
CT Clarity, the Magazine of CT, Goes Digital
More information on the Low-dose Webinar Series can be found at www.gehealthcare.com/ctedu/dosewebinar. »
ctclarity.com Android Apple

6 A GE Healthcare CT publication • www.ctclarity.com
G E H E A lT H C A r E n E w s A n n o u n C E m E n T s
MD Connect: Connecting Your Oncology Team With Applications… Anywhere
Recent innovations in oncology imaging and treatment have
made it possible to treat cancer more effectively. Specifically, more
precise and targeted treatment, coupled with earlier detection,
has led to a remarkable improvement in five-year, disease-free
survival rates for cancer patients. Yet, these new technologies
generate more sophisticated and detailed information that is used
throughout the care cycle, requiring clinicians to utilize different
workstations and applications. For caregivers/clinicians, this
translates to a more complex workflow for processing, connecting,
and collaborating across the continuum of oncology care.
MD Connect is a new, innovative, thin client solution designed
for oncology that addresses the need for a seamless workflow
from scan to plan and monitors treatment effectiveness to
help improve productivity across the cancer care continuum.
Powered by the GE AW Server, it enables plug-and-play access
via virtually any networked computer to the complete suite of
oncology applications from any location or department. As
part of the Dexus workflow environment, MD Connect provides
fast access to a complete portfolio of oncology and radiology
applications—all on one platform. These applications include:
sophisticated tools for virtual simulation; 3D image fusion;
4D motion management; tools to diagnose, stage, and monitor
treatment effectiveness; and more. The tools are designed
to transform the complex into routine and the routine into
more efficient.
MD Connect integrates with the Eclipse™ treatment planning
platform from Varian Medical Systems on one desktop and with
other DICOM-based treatment planning platforms. Compliant
with the IHE-RO standard, MD Connect interoperates across a
multitude of different oncology systems and manufacturers. nEclipse is a trademark of Varian Medical Systems, Inc.
ASiR technology is another CT
advancement that may offer dose
reductions for cardiac and whole-body exams.”**
Dr. Kuroki believes their new, low-dose CT systems will contribute
to the company’s broader vision of modernizing technology,
standardizing operations, and offering responsible, high-quality
imaging. “We looked for a company that shared our philosophy
and long-term vision, demonstrating commitment to the
sustainability and growth of the project,” says Dr. Kuroki. “In
GE, we found a partner that fulfilled all of our expectations and
offered a great cost/benefit ratio for the size of our project with
the Optima and BrightSpeed CT systems.” n
In a move that will broaden the availability and accessibility
of low-dose CT imaging across Brazil, DASA (Diagnosticos
da America SA) has ordered 21 low-dose CT scanners from
GE Healthcare. The sale includes BrightSpeed and Optima
systems featuring ASiR* and will be installed during the
4th quarter of 2011 and 1st quarter of 2012.
The São Paulo-based company is the largest medical diagnostics
provider in Latin America, operating 496 centers in Brazil, with
12,000 employees in 12 of Brazil’s 26 states.
According to Iugiro Roberto Kuroki, MD, Director, Medical Diagnostic
Imaging and Radiology at DASA, “The purchasing of low-dose CT
equipment is in synergy with the company’s philosophy of being
a pioneer in quality and medical responsibility and ensuring
patient access to state-of-the-art diagnostic testing. DASA be-
lieves that CT plays a key role in medicine today, and the
Low-dose CT Coming to Brazil
**In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.

7www.gehealthcare.com/ct • November 2011
a N N o u N c e m e N t s g e h e a lt h c a r e N e w s
The US Food and Drug Administration
has asked all CT manufacturers to pre-populate the CTDIvol Alert
Value at 1,000 mGy. GE’s Dose Check also provides an option to
set a second Alert Value that is applied for exams on patients
under an age threshold determined by each imaging facility.
GE Healthcare representatives will be contacting facilities to
schedule the installation of this FMI (Field Modification Instruction)
on select scanners and deliver an informational packet and
training materials that include:
• Multi-language, updated operator’s manual;
• Computer-based training materials: Dose Check Training
Tutorial & Video CDs; and
• Dose Check Quick Guide for console-side reference. n
As a leader in providing low-dose CT applications, GE Healthcare
invests in initiatives designed to help radiologists and medical
imaging professionals tailor exams to patients of all ages and
conditions. Our commitment to patient safety continues with the
implementation of Dose Check at no cost on most GE CT scanners.
Dose Check is part of the Medical Imaging & Technology Alliance’s
(MITA) Radiation Dose Reduction Plan and CT Dose Check global
initiative. It provides alerts and notifications to scanner operators
when pre-defined radiation dose levels—as determined and set
by the facility—will be exceeded. There are two levels of thresholds:
Notification Values and Alert Values. Notification Values apply
to a single image series (e.g. a single helical series) while Alert
Values apply to a complete exam. Both CTDIvol and/or DLP (Dose
Length Product) values can be set.
Dose Check Aids Hospitals in Regulating Patient Dose
For additional information on Dose Check and a list of scanners scheduled to receive it, please visit www.gehealthcare.com/LowerDoseByDesign. »
approach to growth. It draws on leading-edge R&D, engineering,
and manufacturing expertise from GE centers throughout the
world even as it meets the needs and creates value in our
customers’ home markets.”
The healthcare joint venture between GE and RUSSIAN
TECHNOLOGIES will start with the production of CT scanners and
then expand to other diagnostic medical equipment. The joint
venture may use the recently established joint GE Healthcare—
Medical Technologies Ltd. CT scanner assembly facility in Moscow.
In May 2010, GE Healthcare installed the first Russian-assembled
16-slice CT scanner in one of Moscow’s hospitals. The company
expects to supply over 60 more CTs to hospitals throughout
Russia by year-end 2011.
The Russian government plans to spend more than $30 billion
from 2011 to 2014 on healthcare. GE estimates current Russian
demand for CT scanners alone stands at 3,000 units. n
GE expanded its position in one of the world’s fastest growing
markets by finalizing agreements to set up two new joint
ventures—an Energy JV and Healthcare JV—in Russia. Russian
Prime Minister Vladimir Putin attended the signing ceremony
during the 10th International Investment Forum that took place
Sept. 16, 2011 in Sochi, Russia.
The Healthcare JV agreement was signed by RUSSIAN
TECHNOLOGIES Deputy General Director Dmitry Shugayev and
GE Chairman and CEO Jeffrey Immelt. This JV will manufacture,
assemble, sell, and service a wide range of high-tech medical
diagnostic equipment.
“The establishment of these joint ventures is a positive development
for both GE and Russia,” Immelt said. “We are very excited about
this long-term opportunity that firmly establishes GE’s business
in Russia and reaffirms our global leadership in the energy and
healthcare sectors. Our expansion in Russia reflects GE’s global
General Electric to Expand in Russia With New Joint Ventures

8 A GE Healthcare CT publication • www.ctclarity.com
G E H E A lT H C A r E n E w s A n n o u n C E m E n T s
Hospitals today are faced with having to do more with less. In
the US, a global recession, healthcare reform, changes in the
delivery of patient care including the emergence of Accountability
Care Organizations, the need for low-dose initiatives, and lower
reimbursement have led hospitals to reevaluate purchasing
patterns and priorities.
As a result, hospital administrators are seeking
greater value in their capital equipment
purchases. They want to maximize return-
on-investment, achieve a lower total cost of
ownership, and create an avenue for growth
by developing additional service lines that help
attract new patient groups. Growth is an important
consideration in selecting a CT system that
provides high-quality images and superior
workflow across a plethora of studies—cardiac,
neuro, routine, and trauma/emergency—while opening
up new avenues for profitable growth. Hospital administrators
often seek a system that can help differentiate their services
from the competition.
The recently US FDA-cleared Optima CT660—a 64-channel detector
that is scalable from 32 to 128 slices and GE healthymagination
and ecomagination validated—fulfills these needs. It addresses
the key requirements that many C-suite hospital administrators
seek from new equipment acquisitions: patient care, financial
performance, operational excellence, and market growth.
The Optima CT660 consumes up to 60% less energy than previous
GE CT systems and boasts a 15% lower siting requirement
compared to other 64-channel detector scanners. Lower operational
costs translate to savings of potentially tens of thousands of
dollars over the life of the product. Plus, implementing a scanner
that emits up to 60% less carbon emission on the US grid is one
step toward becoming a “green” hospital.
Financial performance continues with service. GE’s service,
ranked No. 1 in service performance for CT systems by IMV Limited
in 2011,1 provides the highest number of CT field engineers of
any OEM. OnWatch Remote Services can often resolve 45% of
a CT scanner’s service issue(s) remotely.
Operational excellence is the key to market growth.
The Optima CT660 provides a comprehensive
suite of clinical capabilities—starting with the
GE-exclusive ASiR for low-dose imaging across
all anatomies. ASiR has been evaluated for its
lower-dose capabilities in over 75 published
studies. Ten million patients in more than
500 facilities worldwide have been scanned
using ASiR.**
Key applications on the Optima CT660 include: low-
dose cardiovascular imaging with SnapShot* Pulse and
consistent 0.625 mm data acquisition in CT Angiography;
VolumeShuttle* perfusion; Volume Helical Shuttle (VHS) for
perfusion studies up to 12 cm; Lung VCAR* and CTC Pro3D EC
applications for lesion detection, analysis, and follow-up; auto-
segmentation tools matching datasets to MR and PET/CT; and,
fast, efficient, one-touch workflow for emergency departments.
The 12-inch Xtream display on the gantry shows patient information,
protocol settings, and the ability to play relaxing videos. Automatic
patient positioning and a synchronized starting of the exam and
injection further streamline the study so facilities can maximize
patient throughput. The Optima CT660 also delivers a comfortable
patient experience.
The Optima CT660 brings together workflow efficiency, diagnostic
power, and lower equipment and operational costs to address a
new era of exceptional patient care, financial performance, and
operational excellence. n
Optima CT660: Taking Performance to a Whole New Level
References:
1. IMV ServiceTrak* Imaging CT Systems 2011 Report. IMV Medical Information Division, Des Plaines, IL.
**In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.
To view a video about the Optima CT660, please visit www.ctclarity.com/ctclarity/201111#pg8. »

9www.gehealthcare.com/ct • November 2011
c u s t o m e r s p o t l i g h tb r i v o c t 3 2 5 i N i N d i a
Access to healthcare throughout India is improving as a result of Public-Private
Partnerships (PPP). An initiative by the Department of Health & Family Welfare of the
Government of West Bengal (WB) aims to make healthcare facilities available in the
district with the continued development of PPPs through the procurement cell West
Bengal Medical Services Corporation Ltd. (WBMSC). The Brivo§ CT325, a GE Healthcare
healthymagination-validated CT scanner, is a key contributor for increasing access
to advanced CT imaging in the state of West Bengal, India.
Brivo CT325 streamlines patient positioning, which often cuts in half the time it takes us to position the patient in the gantry.
Pranabananda Goswami, DMRD, MD
Mr. Govind Prasad Agarwal, Founder, Midnapore Diagnostics Pvt. Ltd.
A CT Designed for Broader AccessBy Pranabananda Goswami, DMRD, MD,
Jayati Bardhan, MD, Consulting Radiologists, and Mr. Govind Agarwal, Midnapore Diagnostics Pvt. Ltd.
§Brivo CT325 is not for sale in the United States. Not cleared by the US FDA.
C U S T O M E R S P O T L I G H T

10 A GE Healthcare CT publication • www.ctclarity.com
C u s T o m E r s p o T l i G H T b r i v o C T 3 2 5 i n i n d i A
C u s T o m E r s p o T l i G H T
India’s first Brivo CT325 was installed at our facility, Midnapore
Diagnostics Pvt. Ltd. (MDPL), within the premises of R G Kar
Medical College & Hospital (Kolkata). Situated in the heart of
Kolkata, the hospital is a PPP venture between the Government
of West Bengal State and MDPL. Mr. Govind Prasad Agarwal
founded MDPL in 2002 with the objective of providing access to
radiology diagnostic facilities (CT & MRI) for the common people.
In February 2011, the new Brivo CT325 replaced a single-slice
CT. On average, we are performing 45 CT cases each day, which
exceeds 1,200 cases each month. In July 2011, we scanned
1,500 patients on the Brivo CT325, a record for monthly CT
scans at our facility. We are now very comfortable doing more
than 60 cases a day (including 25 to 30 body imaging cases),
which has substantially improved patient care. This was previously
not possible with our single-slice CT scanner. We anticipate that
we will be able to sustain similar capacities in subsequent
months, particularly due to the fact we’ve encountered no
unplanned downtime since the installation.
Midnapore Diagnostics Pvt. Ltd. within the premises of R G Kar Medical College & Hospital.
Volume-rendered 3D image is from digital tilt raw data.
A unique sub-mm high resolution CT image of the inner ear.
CT angiography of the Circle of Willis with faster coverage and high spatial resolution.
Volume-rendered 3D image illustrates a bone tumor in the pelvis.

11www.gehealthcare.com/ct • November 2011
c u s t o m e r s p o t l i g h tb r i v o c t 3 2 5 i N i N d i a
One of our requirements for a new CT scanner was faster
scanning time so that our radiology team could handle higher
patient volumes. Brivo CT325 streamlines patient positioning,
which often cuts in half the time it takes us to position the
patient in the gantry. Our technologists are also impressed with
the compact operating console and additional filming formats.
After six months of use, we are very satisfied with the speed
of the system and the quality of its images. Additionally, we
find the new unique Digital Tilt scan technique helps generate
excellent MPRs (Multi Planar Reformats) and display as routine
tilted images. We do not have to conduct another scan just
to obtain different reconstructions. And, the new innovative
table helps us complete the cases quickly and efficiently.
Perhaps most important to the sustainability of our PPP, the
volume-rendered 3D and HRCT (asymmetric scan) images
are catching the attention of many referring physicians.
In conclusion, we feel that the Brivo CT325 imaging capabilities
fulfill the various clinical needs of healthcare facilities like ours.
Its high image quality and dose-conscious design—combined
with a wide variety of proven, advanced applications—help
us make efficient and confident diagnoses across anatomies—
from the head down to the toes. This helps us provide better
support to other departments in the hospital and to our referral
doctors. Brivo CT325 thus lives up to its claim of extending
quality care to more people at an affordable cost. n
Its high image quality and dose-conscious design—combined with a wide variety of proven, advanced applications—help us make efficient and confident diagnoses across anatomies—from the head down to the toes.
Pranabananda Goswami, MD, DMRD, is a Consultant Radiologist at Midnapore Diagnostics Pvt. Ltd. (Kolkata, India). He also serves as Chief Radiologist and Radiology Director at VIP Apex Medical Center (Kolkata) and Chief Radiologist at ESI Hospital (Kolkata). Dr. Goswami received his medical degree and DMRD from the University College of Medicine (Kolkata) and his MBBS from R G Kar Medical College. He has also served as Assistant Professor of Radiology at R G Kar Medical College.
Portography study demonstrates excellent low contrast detectability.
Volume-rendered 3D image of the kidneys shows good spatial resolution.
MPR depicts the hip and head of femur.

C U S T O M E R S P O T L I G H T
12 A GE Healthcare CT publication • www.ctclarity.com
C u s T o m E r s p o T l i G H T o p T i m A C T 6 6 0 i n i n d i A
In early April 2011, Meenakhi Mission Hospital and Research Centre (MMHRC) acquired
the first Optima CT660 in South India. Our radiology department is recognized as one of
the best in the region, providing various sub-specialties such as interventional radiology
in conjunction with a fully equipped and advanced diagnostic imaging department. The
acquisition of this new CT system will help us manage increasing patient volumes and
provide efficient diagnostic support to other specialties.
The key benefit for our patients is the system’s exceptional performance at low dose levels.
T. Mukuntharajan, MD, MBBS, DMRD
Delivering Quality Care: From Vision to Reality
By T. Mukuntharajan, MD, MBBS, DMRD, Head of the Department of Interventional Radiology & Radiodiagnosis; N. Karunakaran, MD, Consultant Radiologist; and R. Ganesh, MD, Consultant Radiologist, Meenakshi Mission Hospital and Research Centre
13www.gehealthcare.com/ct • November 2011
c u s t o m e r s p o t l i g h to p t i m a c t 6 6 0 i N i N d i a
The Optima CT660 system is the latest generation of multi-
detector CT from GE Healthcare. This new CT system provides
a streamlined workflow that assists our radiologists and
technologists in efficiently managing the heavy patient
workflow. Plus, the Optima CT660 is a GE ecomagination and
healthymagination validated product. The environment-friendly
power-save mode makes the system more energy efficient with
an average electric consumption of up to 60% less compared
to previous GE CT systems.
A key benefit for our patients is the exceptional performance of
the Optima CT660 at optimized radiation dose levels, including
generating high-quality diagnostic images with sub-millimeter
resolution and enabling high performance with innovations such
as backlit diode and high-density interconnects. Specialized
dose reduction techniques, such as Adaptive Statistical Iterative
Reconstruction (ASiR) and SnapShot Pulse (adaptive prospective
cardiac gating), may reduce patient dose for scans including
cardiac studies.**
In the first 72 hours after installation and calibration of the
system at our hospital, we conducted more than 100 patient
exams. This included a myriad of routine and advanced patient
studies including: coronary angiograms; CABG evaluations;
aorotograms; renal angiograms; multiphasic; and perfusion
studies. This system scans at a high pitch with a table speed
of 110 mm/s in the 0.625 mm detector configuration.
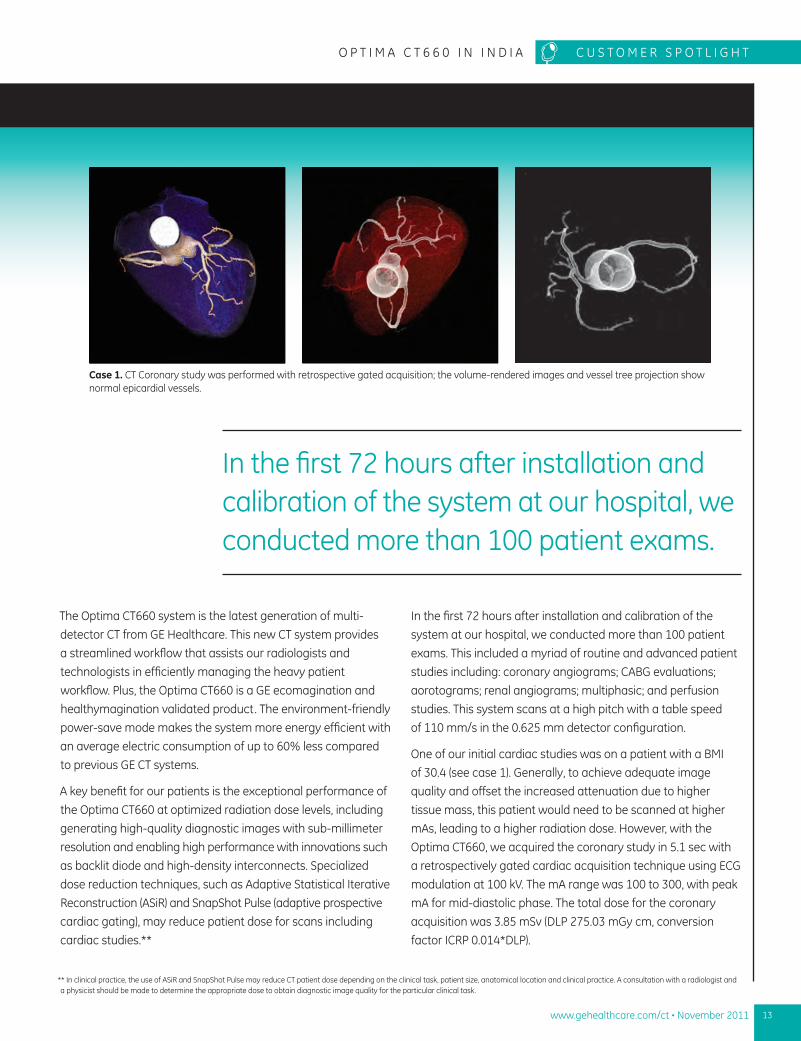
One of our initial cardiac studies was on a patient with a BMI
of 30.4 (see case 1). Generally, to achieve adequate image
quality and offset the increased attenuation due to higher
tissue mass, this patient would need to be scanned at higher
mAs, leading to a higher radiation dose. However, with the
Optima CT660, we acquired the coronary study in 5.1 sec with
a retrospectively gated cardiac acquisition technique using ECG
modulation at 100 kV. The mA range was 100 to 300, with peak
mA for mid-diastolic phase. The total dose for the coronary
acquisition was 3.85 mSv (DLP 275.03 mGy cm, conversion
factor ICRP 0.014*DLP).
** In clinical practice, the use of ASiR and SnapShot Pulse may reduce CT patient dose depending on the clinical task, patient size, anatomical location and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.
Case 1. CT Coronary study was performed with retrospective gated acquisition; the volume-rendered images and vessel tree projection show normal epicardial vessels.
In the first 72 hours after installation and calibration of the system at our hospital, we conducted more than 100 patient exams.

14 A GE Healthcare CT publication • www.ctclarity.com
C u s T o m E r s p o T l i G H T o p T i m A C T 6 6 0 i n i n d i A
C u s T o m E r s p o T l i G H T
Another interesting case is an abdominal angiography for a
patient who presented with suspected SMA ischemia (see case
2). This study was also performed at very low mAs—with a
maximum of 58.8 mA. (The scan technique helical mode was
at 120 kV, 98 mA, 0.6 sec, pitch factor 1.375:1). Angiographic
and routine images from the same data demonstrate excellent
image quality even at a low mA. The total dose for the study
was 2.8 mSv, which is 70% less than the ICRP stated “nominal”
dose of 10 to 20 mSv (ICRP Publication 87, Managing Patient
Dose in Computed Tomography 30[4] Annals of ICRP 2002
[Obtained by EUR-16262 EN Abdomen and Pelvis factor of
0.017 x DLP.]).
The Volara XT* DAS system, a component of the Optima CT660,
provides a very high signal output at low photon levels. The
heavy attenuation produced by the metal hardware in the
patient does not result in severe photon starvation effect
and artifact from dense hardware (see case 3). (Total dose
of 6.3 mSv. DLP 422.96 mGy.cm. Obtained by EUR-16262 EN
Abdomen and Pelvis factor of 0.017 x DLP.)
The Optima CT660 also plays a very important role in our ability
to offer low-dose scanning, which is particularly important for
pediatric imaging. It includes GE’s pediatric color-coded protocols,
the use of 80 and 100 kV settings, and most importantly, the
effective utilization of high-yield performance of the detector
at low mA levels. Together, these features make this system
an appropriate CT imaging solution for pediatric studies.
Case 2. Abdominal angiography with suspected SMA ischemia. 3D volume-rendered image (far right) after one click Autobone Xpress* for removing bones. The VR IVUS ‘like’ view shows atheromatous mixed plaques along the lower aorta–iliac vessels.
Case 3. Axial images from a patient scan post laminectomy status with metal screws in situ—the adjacent bones close to the screws are well visualized without any beam hardening artifact or blooming.

15www.gehealthcare.com/ct • November 2011
c u s t o m e r s p o t l i g h to p t i m a c t 6 6 0 i N i N d i a
T. Mukuntharajan, MBBS, DMRD, is Head of the Department of Interventional Radiology & Radiodiagnosis, Meenakshi Mission Hospital and Research Center (Maduria, Tamilnadu, India). He received his MBBS and DMRD from Madurai Medical College. He specializes in vascular and interventional CT imaging, endoscopic ultrasound, echocardiography, and vascular and non-vascular interventional radiology procedures.
With over 700 beds, Meenakshi Mission Hospital & Research Centre (S.R. Trust ) has grown to be a multi-specialty hospital, touching lives in and around Madurai. The hospital extends the traditional Indian hospitality to international patients, combining it with cutting edge technology, clinical excellence, and compassion to deliver quality healthcare to all patients. S.R. Trust is a non-profit organization registered under the Indian Trust Act (May 9, 1985).
One pediatric case involved an eight-day-old baby who
suffered a head trauma (see case 4). The patient was not
opening their left eye after the trauma and a CT of the head
was ordered for a detailed evaluation. The exam included a
whole brain scan from the floor of orbits with a low-dose
technique and total reported dose of 0.83 mSv (DLP 75.83, ICRP
conversion factor of 0.011 *DLP for ‘zero’ age group), 80 kV, 120
mA, 1 sec axial mode, and detector configuration 0.625 X 32.
The study revealed no traumatic injury or bleed in the brain.
To summarize, after our initial experience scanning 100 patients
in three days, we found the Optima CT660 exhibited tremendous
capabilities in routine and complex studies and provided
exceptional image quality at optimized doses. We think the
Optima CT660 is an ideal CT scanner for virtually any radiology
department seeking eco-friendly, low power consumption,
patient comfort, fast workflow, and low-dose scanning capability
while delivering quality diagnostic images. n
Case 4. Axial images for brain with excellent grey white differentiation. 3D VR and Curved MPR for optic nerves are obtained from the same low dose scans.

C U S T O M E R S P O T L I G H T
16 A GE Healthcare CT publication • www.ctclarity.com
C u s T o m E r s p o T l i G H T B r i v o C T 3 2 5 i n C H i n A
Yichun Yuanzhou Red Cross Hospital is a 318-bed, private, Tier-2 hospital—a medium-
sized hospital often referred to as a district, or township hospital. With more than 250
medical staff in the hospital and varied specialties in the facility, Yichun Yuanzhou Red
Cross Hospital is considered one of the larger and more advanced medical facilities in
Yichun Prefecture-level city.‡ In April 2011, Yichun Yuanzhou Red Cross Hospital installed
its very first CT system—the Brivo§ CT325.
Clinically, we are impressed that the system is easy to use yet doesn’t compromise image quality.
Dr. Yang Shenghong
Seeing Beyond the Naked EyeBy Dr. Yang Shenghong, Director of Radiology, Yichun Yuanzhou Red Cross Hospital
‡ A prefecture-level city is an administrative unit that typically comprises a main central urban area (often with the same name as the prefectural level city) and its much larger surrounding rural area containing many smaller cities, towns, and villages. The larger prefectural level cities can be over 100 km across in size. Prefectural level cities nearly always contain multiple counties, county level cities, and other such sub-divisions. (Source: Wikipedia)
§ Brivo CT325 is not for sale in the United States. Not cleared by the US FDA.

17www.gehealthcare.com/ct • November 2011
c u s t o m e r s p o t l i g h tB r i v o c t 3 2 5 i N c h i N a
When we began our search for a CT scanner, GE was a natural
choice for our hospital and five radiologists. We already
have GE X-ray, fluoroscopy, and ultrasound systems, and
our experience with these other systems has been very good.
So when we selected the Brivo CT325, we knew without
question that it would be a fine, quality system.
After seven months of using the new CT system, we have
realized many benefits for our patients and clinicians.
Clinically, we are impressed that the system is easy to use
yet doesn’t compromise image quality. We have found the
Brivo CT325 has excellent image quality in terms of low contrast
resolution and detectability, especially when compared to CT
systems in this segment that we’ve used at other hospitals. The
digital tilt feature can produce reconstructed images through
helical scanning, reduce scan time, and optimize CT study
workflow. Digital Tilt (DT) is an image reconstruction method on
CT systems that do not have gantry tilt capability. Reformatting
to obtain 2D/3D images with a helical scan is also possible for
certain anatomy such as the sinus or nasal bone.
Yichun Yuanzhou Red Cross Hospital
Ankle reconstruction
Lumbar reconstruction

18 A GE Healthcare CT publication • www.ctclarity.com
C u s T o m E r s p o T l i G H T B r i v o C T 3 2 5 i n C H i n A
C U S T O M E R S P O T L I G H T
For radiologists, design and ergonomics complement the system’s
imaging capabilities. Thanks to a more efficient workflow,
lumbar spine scanning is more streamlined compared to other
CT systems we’ve used. With thin-slice imaging, we can better
visualize anatomy, especially the sinus. This was not attainable
with other CT scanners in this segment that we’ve encountered.
Currently, we conduct approximately 15 CT studies each day.
These CT scanning procedures have been well-received by
residents of the city, who have reported having positive CT
scan experiences. This is good news, given that we expect
patient volume to double within the next 12 months. While
today there are seven Brivo CT325 systems in the Jiangxi
Province, we are proud to be one of the first installed sites. n
Head reconstruction Chest reconstruction
Thanks to a more efficient workflow, lumbar spine scanning is more streamlined compared to other CT systems we’ve used.
Dr. Yang Shenghong is Head of the Department of Radiology and has more than 15 years of experience in his field.
Yichun Yuanzhou Red Cross Hospital in Yi Chun city, Yuanzhou district is located in the northwest of Jiangxi Province. In ancient times, Yuanzhou was known for its education, made famous by Han Yu, a renowned poet in the Tang Dynasty. Yuanzhou lies in Yichun Prefecture-level city and Yichun literally means “Pleasant Spring.”

19www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u ec a r d i a c i m a g i N g
In December 2010, Clinic “La Reine
Blanche” Orléans-France installed an
Optima CT660 with ASiR. In explaining
the reason to select the Optima CT660,
Olivier Genée, MD, cardiologist, says, “The
Optima CT660 fulfilled our requirement
for a 40 mm wide detector.” Another very
important consideration for the facility
is the issue of patient radiation dose,
he adds. With ASiR, the clinicians may
prescribe low-dose CCTA exams.
Predicting CCTA volume is a difficult
task, yet the clinic believed that a
scanner with advanced CTA imaging
capabilities and low dose would increase
patient and referring physician demand.
Therefore, the total cost of ownership—
including a smaller footprint that can
reduce siting costs and lower energy
consumption—was also an important
factor in the facility’s final decision. After
a thorough review of available solutions
and weighing the site’s requirements, Dr.
Genée and his team found the Optima
CT660 best met their needs for an
advanced imaging system with low dose
capabilities—and lower operating costs.
Installation of the Optima CT660 has
modified the diagnostic path in the clinic.
For example, the clinic often requires a
CCTA after an inconclusive scintigraph
scan from a gamma camera before
the patient undergoes a therapeutic
angiography in the cath lab. Interestingly,
as the volume of cath lab procedures
increased, so too did the CCTA exams.
Meeting the Clinical Need for Low-dose Cardiac Studies
Figure 1. Myxome of the left atrium as seen in a retrospectively gated acquisition.
A
C
B
D
Figure 2. The vessel lumen is clearly seen as the calcium blooming is significantly reduced.
A
B
20 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E C A r d i A C i m A G i n G
Dr. Genée says that the CCTA rules out false positives that often
appear during stress tests and supports treatment decisions
regarding coronary conditions. When the CCTA test indicates
a low probability of CAD, the patient can avoid a diagnostic
cath lab procedure. According to the clinic’s practice, patient
selection is determined with the help of a medical prescriber.
If the patient’s heart rate is over 65 bpm, the clinic uses beta-
blockers prior to the CCTA.
Dr. Genée finds that performing CCTA in an emergency setting
may be difficult due to patient arrhythmia or even fibrillation.
The team finds the post processing is very flexible and powerful.
Additionally, the Optima CT660 has allowed Clinic “La Reine
Blanche” Orléans-France to perform new types of cardiac CT
studies, further broadening its clinical expertise. The
clinic conducts examinations of myocardium function in
patients with certain non-echogenic tumors or inaccessible
trans-esophageal ultrasound. Vascular CT exams allow
for accurate diagnosis in cases of aorta dissection when
trans-esophageal ultrasound is not sufficient. Finally, after
the Optima CT660 installation, patients with an indication of
pulmonary embolism can now be examined on site without
transferring them to another hospital.
Asked what he would say to a colleague considering implementing
an Optima CT660, Dr. Genée says, “We are very satisfied
with the Optima CT660 with ASiR. It meets our expectations
and offers an excellent quality-to-investment ratio.” n
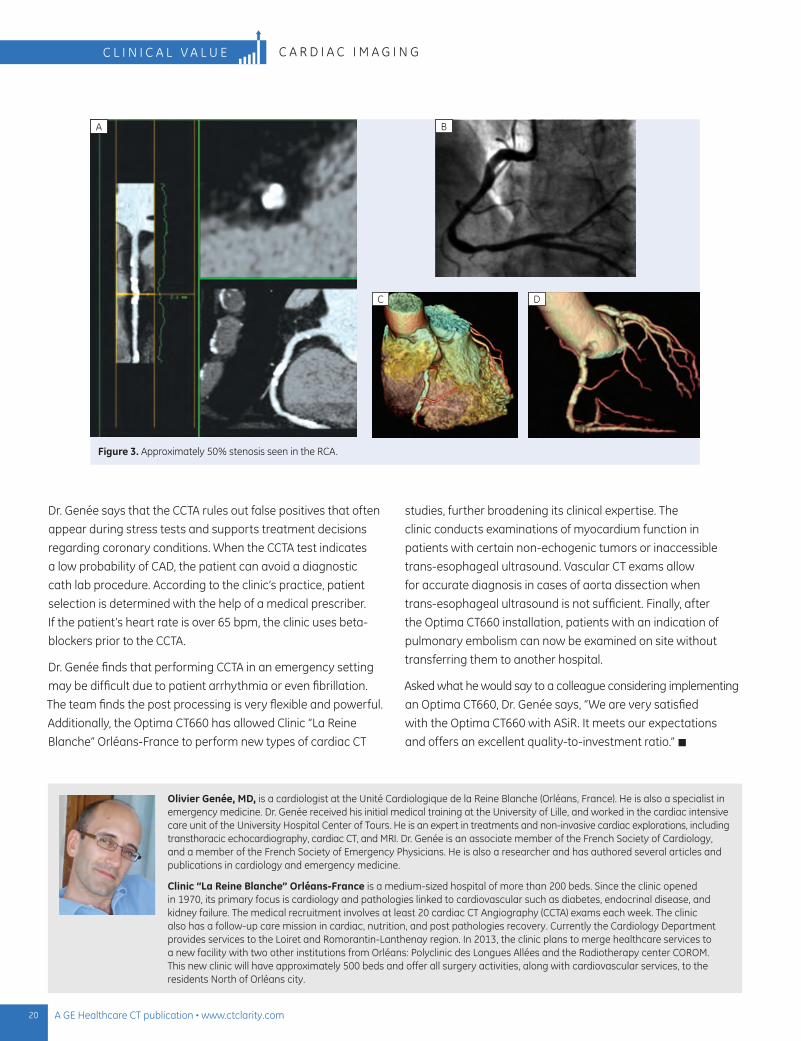
Figure 3. Approximately 50% stenosis seen in the RCA.
B
DC
A
Olivier Genée, MD, is a cardiologist at the Unité Cardiologique de la Reine Blanche (Orléans, France). He is also a specialist in emergency medicine. Dr. Genée received his initial medical training at the University of Lille, and worked in the cardiac intensive care unit of the University Hospital Center of Tours. He is an expert in treatments and non-invasive cardiac explorations, including transthoracic echocardiography, cardiac CT, and MRI. Dr. Genée is an associate member of the French Society of Cardiology, and a member of the French Society of Emergency Physicians. He is also a researcher and has authored several articles and publications in cardiology and emergency medicine.
Clinic “La Reine Blanche” Orléans-France is a medium-sized hospital of more than 200 beds. Since the clinic opened in 1970, its primary focus is cardiology and pathologies linked to cardiovascular such as diabetes, endocrinal disease, and kidney failure. The medical recruitment involves at least 20 cardiac CT Angiography (CCTA) exams each week. The clinic also has a follow-up care mission in cardiac, nutrition, and post pathologies recovery. Currently the Cardiology Department provides services to the Loiret and Romorantin-Lanthenay region. In 2013, the clinic plans to merge healthcare services to a new facility with two other institutions from Orléans: Polyclinic des Longues Allées and the Radiotherapy center COROM. This new clinic will have approximately 500 beds and offer all surgery activities, along with cardiovascular services, to the residents North of Orléans city.

21www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u ev e O : u lT R a - l O W D O S e
University Hospital, Brussels has been using Veo since March 2011.
In addition to ultra-low dose CT imaging—in some instances as
low as plain film radiography—Veo provides new possibilities for
the radiologist to tailor the scan parameters to the patient. For
example, radiologists for years have known that when looking
for a pulmonary embolism, the exam is tailored to the indication
by administering a faster rate of contrast and scanning the bolus
earlier. If the clinician is investigating the possibility of interstitial
disease in the lungs, then the radiologist would perform the CT
scan at a higher resolution and thinner slices.
These examples, while part of the typical radiology practice,
demonstrate the versatility of CT imaging that we have fine-tuned
over the course of 20 years. With Veo in our facility, we have
further expanded CT imaging into clinical possibilities. We have
achieved reduced mA and kV in the acquisition of diagnostic
images and thereby been able to reduce dose to previously
unthinkable levels.**
Enabled with Veo, these new possibilities can be further tailored
to the patient by adjusting CT parameters radiologists have used
for decades. In fact, Veo has opened up new possibilities for
challenging cases and sensitive patients. For example, while Veo
may allow scans at an ultra-low dose, we can still scan at typical
dose levels and obtain images with higher spatial resolution and
better delineation of structures.
The key to the successful implementation of these new scanning
possibilities is determining the appropriate patient group that
will benefit most from the Veo technology and understanding
how it can be used without impacting radiology workflow.
Workflow
Veo is a processing technique that generally requires more time
(estimated from 20 to 80 minutes) to generate a high-quality
image from an ultra-low dose acquisition. In our facility, this has
not presented any issues to our radiology workflow. As in most
Implementing Ultra-low Dose CT with Veo at University Hospital, BrusselsConsiderations for workflow and patient selection By Professor Johan de Mey, MD, PhD, Chair of Radiology, University Hospital, Brussels
** In clinical practice, the use of Veo may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.

22 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E v E O : u lT R A - l O W D O S E
public hospitals across Europe and the US, radiologists perform
their interpretations and reporting in a reading room or back
office, well after the exam has been completed, and not in the
CT room or while the patient is in the scanner.
In our facility, the need for an immediate diagnosis occurs in
approximately 5% of our patients—i.e., emergency cases—and,
therefore, we use ASiR for low-dose CT studies in these instances.
However, even in emergency cases the physician must often
wait 30 minutes for laboratory results, so we believe the
additional time to utilize Veo is not an issue considering other
test results will require time for analysis.
For the technologist, workflow efficiency is also not compromised.
Even with an ultra-low dose scan, the CT scanner immediately
provides images so the technologists can evaluate that the proper
patient positioning was attained for displaying the anatomy or
pathology in question. Our technologist can determine from the
initial images that the exam acquired the desired anatomy.
Patient selection
A critical component to maintaining an efficient workflow using
Veo is identifying patients who would benefit most from an
ultra-low dose exam. Because we only have one Veo (box) at our
facility, we cannot utilize it on each patient receiving a CT scan.
As mentioned above, emergency cases should be evaluated
based on other dose lowering techniques available (e.g., ASiR).
Radiotherapy patients are also often excluded as the amount
of radiation dose from CT is small compared to the treatment
they received.
Although we continue to adapt the patient criteria for Veo
reconstructions, our facility has identified the following patient
groups, who may benefit most from a Veo scan: pediatric patients,
particularly those who require regular scanning and follow-up
due to a disease or affliction, young adults, adults with a disease
requiring regular X-ray or CT imaging follow-up, and adults with
kidney disease.
Veo provides new possibilities for the radiologist to tailor the scan parameters to the patient.
Professor Johan de Mey
A B C
Figure 1. A two-year-old patient with empyema. Exam conducted at DLP 27 mGy.cm with an effective dose of 0.9 mSv (Obtained by EUR-16262 EN, using a pediatric chest factor of 0.031*DLP). Acquisition parameters are 80 kV and 15 mAs.

23www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u ev e O : u lT R a - l O W D O S e
Historically in our facility, pediatric patients with cystic fibrosis
and no health complaints received a lung X-ray every two years.
This was the first pediatric group for which we utilized the Veo
reconstruction. In most cases, the patients are stable, and some
have previously identified lung lesions. We initiated a double-
blind study, substituting the X-ray with low-dose CT performed
at the same dose level as the X-ray. We noticed we could see
more anatomy with the volume CT than the prior X-ray. There were
cases where the CT demonstrated an evolution in pathology
that was previously deemed stable based on the X-ray data. CT
provided the ability to detect lesions more clearly, which in many
instances will impact patient treatment. We ultimately moved
all cystic fibrosis pediatric patients to Veo low-dose CT follow-up.
Young adults are another category where the benefit from ultra-low
dose CT is great. As with pediatrics, the patient’s history and
indications are reviewed to determine the best imaging option
and appropriate low-dose reduction.
Another group of patients who receive low-dose Veo CT scans
at University Hospital are those suffering from Crohn’s Disease.
These patients often have complaints related to this bowel
disease and receive CT exams.
Lastly, for patients with kidney disease we have adjusted our
protocols to lower kVs to help us address iodine use in patients
who may be sensitive to it.
Based on our experience, developing the proper Veo protocols—
both in patient selection and implementing low-dose imaging—is
important for successful implementation. As one of the first sites
to clinically use Veo, we continue to examine Veo’s potential and
implementation on specific patient groups.
One thing we learned is that we cannot uniformly lower dose for
every indication when changing the protocols. For each patient
group, we are still building our experience and determining the
appropriate dose levels. Additional scientific studies, including
the global multi-site clinical study that GE is sponsoring, will
provide additional information to help optimize dose level
protocols for each patient group. n
Johan de Mey, MD, PhD, is Chair of the Radiology Department at University Hospital, Brussels, and a Professor at Brussels University where he is also the coordinator for radiology resident training. Prof. de Mey earned both doctorate degrees at the Vrije Universiteit Brussels; his PhD thesis was CT fluoroscopy in interventional radiology. As Professor, he lectures on radiology anatomy, normal and pathologic radiology and emergency radiology.
Located in the heart of Europe, the University Hospital Brussels is one of Belgium’s premier centers of excellence in healthcare, biomedical research and medical education. One of seven University Hospitals in Belgium, it is closely associated with the Brussels University. University Hospital Brussels has gained recognition at both a national and an international level. With its 700 beds and staff of 3,000, close to 30,000 inpatients and 500,000 outpatients are treated every year.
www.gehealthcare.com/LowerDoseByDesign »
Figure 2. Maxillofacial CT of a nine-year-old patient with a fracture of the inferior orbita. Exam conducted at DLP 38.97 mGy.cm with an effective dose of 0.31 mSv (Obtained by EUR-16262 EN, using a pediatric head factor of 0.008*DLP). Acquisition parameters are 100 kV and 14 mAs.
A B C
Editor’s note: For more information on the global multi-site clinical study, please see article on page 54.

24 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E B r i G H T S p E E d E l i T E w i T H i Q E n H A n C E
Carolinas Imaging Service (CIS) is a joint venture between
Charlotte Radiology and Carolinas HealthCare System located
in metropolitan Charlotte, NC. The group provides patients with
a freestanding, outpatient option across a multitude of imaging
systems and exam types.
In November, 2010, CIS decided to outfit its outpatient imaging
clinic in South Park with a BrightSpeed Elite CT. One clinical area
where the new system has made an impressive impact is in
musculoskeletal (MSK) imaging. Currently, between 15 to 20 MSK
CT studies are performed each day at CIS.
When it comes to MSK, James Coumas, MD, knows bones. He
graduated with a fellowship in musculoskeletal radiology from
Massachusetts General Hospital and reads MSK images full time.
“With 85 radiologists in our group, we have the ability to specialize
into specific regions of the body that interest us. For me, that is
the musculoskeletal system.”
Dr. Coumas is passionate about the work he does in MSK.
“Musculoskeletal radiology spans a spectrum of disease processes
as well as congenital and acquired abnormalities,” he says. “Whether
it’s a congenital anomaly, a response to a debilitating disease
process, an acute sports injury, or aged encumbered degenerative
arthritis, the musculoskeletal system is usually involved.”
The one thing Dr. Coumas loves about CT in general is the speed.
“A patient comes in with pain that is non-specific and CT is used
as a rule-out mechanism for the pain,” he explains. “The advantage
of CT is it takes two minutes; MR is 30 to 45 minutes. When you
are in pain, this is a long time to be on a table for a scan.”
Dr. Coumas is particularly excited about the BrightSpeed Elite
and the IQ Enhance (IQE) feature. IQE allows the group to use
their 16-slice scanner with faster pitch helical scanning at a
similar artifact index level compared to slower helical scanning
without IQE. This coverage speed is equivalent to that of wider
detectors (50 slice equivalent) at the same table speed. This
decreases the length of time per study without a corresponding
loss in image quality, he explains. In fact, Dr. Coumas prefers
using the IQE feature on all MSK cases.
He also does a great deal of referral work with orthopedic surgeons
who have had issues with certain implant recalls. “Artifact
reduction in prosthetic imaging is a large part of our business with
patients 40 to 60 years of age. It is important to have a scan that
you are able to see 360° around the prosthesis to determine if
there is anything loose, fractured, or dislocated (Figure 1).”
Dr. Coumas is enthusiastic about using the BrightSpeed Elite for
his patient cases. “We have 15 scanners in our group and for MSK
workups we currently send all our patients to the BrightSpeed.”
BrightSpeed Elite with IQ Enhance Delivers Speed and Clarity in the Carolinas
“ A patient comes in with pain that is non-specific and CT is used as a rule-out mechanism for the pain. The advantage of CT is it takes two minutes; MR is 30 to 45 minutes. When you are in pain, this is a long time to be on a table for a scan.”
Dr. James Coumas

25www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u eB r i g h t S p e e d e l i t e w i t h i Q e N h a N c e
Patient case with and without IQE
A 68-year-old male patient presented at CIS with a history
of mild chronic obstructive pulmonary disease (COPD). A
chest CT exam with contrast revealed a new right apical cavity
nodule. The comparison images (Figure 2) demonstrate how
the BrightSpeed Elite with IQE can help to reduce the amount
of streaking and windmill artifact in the coronal dataset.
Overall, the BrightSpeed Elite has been a positive decision for CIS.
It’s intelligent, versatile, and user-friendly. Dr. Coumas sums it up
best, “For routine body work, the Brightspeed Elite is all I need.” n
Figure 2. (A) With IQE and (B) without IQE.
A B
Acquisition Protocols:
kV: 120 mAs: 276-436 Slice thickness: 0.625 Coverage: 336 cm Pitch: 1.75
James M. Coumas, MD, specializes in musculoskeletal radiology at Carolinas Imaging Services. He earned his medical degree and completed his residency at the University of Massachusetts Medical School (Worchester) and a fellowship in musculoskeletal radiology at Massachusetts General Hospital.
Charlotte Radiology (CR) is one of the largest and most progressive radiology groups in the nation, serving Mecklenburg and surrounding counties since 1967. With 80+ radiologists with diverse and specialty training—including Mammography, Musculoskeletal, Pediatrics, and Interventional Radiology—CR provides 24/7 coverage for more than 11 hospitals and four outpatient imaging centers (including CIS). In addition to CIS, the group owns and operates 12 breast centers, two vascular and interventional clinics, and an MRI center.
Figure 1. (A) Volume-rendered image; (B) sagittal view image
A B
Acquisition Protocols:
kV: 120 mAs: 191-310 Pitch: 1.375:1 Coverage: 116 mm Scan time: 6.69 sec

26 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E B r i G H T S p E E d E l i T E w i T H i Q E n H A n C E
Helical windmill artifact is caused by the aliasing of the signal.
Aliasing occurs when a signal is sampled too slowly or at a
frequency comparable to or smaller than the signal being
measured and, as a result, obtains an incorrect frequency
and/or amplitude.
The IQE algorithm dynamically detects the presence
of aliasing and automatically corrects for such artifact.
The following case is a great example of how the windmill
helical artifact surrounding bone can be minimized to enhance
the final outcome by scanning with IQE at a pitch of 1.75. This
scan, done in 5.4 seconds, demonstrates the excellent spatial
resolution as well as speed using BrightSpeed Elite with IQE.
Helical Artifact Index is defined as: ((SD value at ROI1)2-(SD
value at ROI2)2)1/2. Two helical data sets were acquired
to compute a Helical Artifact Index. n
Figure 3. (A) With IQE and (B) without IQE
A
Acquisition Protocol:
Scan type: Helical (IQE) kV: 120 mAs: 90-210 Pitch: 1.75 Coverage: 70 mm/s Scan time: 5.4 sec Gantry rotation: 0.8 sec Slice thickness: 1.25 mm SFOV: large DFOV: 32 cm Start/End: S200-I370 Reconstruction: 512 matrix
One data set was acquired at 1.75:1 pitch with table speed of 37.5 mm per rotation with IQE ON at 260 am and other using 0.562:1 pitch with table speed of 11.25 mm per rotation with IQE OFF at 160 mA.
IQE helps to minimize aliasing of the signal
B

27www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u em u s c u l o s k e l e t a l i m a g i N g
With the recent advances in technology and software development,
the utilization of CT in musculoskeletal (MSK) clinical imaging
has undergone tremendous improvements. The most observable
changes are the availability of High Definition (HD) CT data
acquisition and reconstruction, Gemstone Spectral Imaging (GSI)
with monochromatic data, effective metal artifact suppression,
and dynamic 4D evaluation of joints and tendons using volume
helical shuttle.
In this article, we share some of our early experiences with the
new Discovery CT750 HD installed at our hospital.
Emerging Applications in Musculoskeletal CT Imaging By K Murali MD(RD), PDCC, Director of Interventional Radiology, G. Francis DMRD, DNB (RD), Consultant Radiologist, and R. Madan, MBBS, MD, Consultant Radiologist, MIOT Hospital; Sundar RK, Clinical Applications Manager, CT, GE Healthcare
HD Imaging
The HD scanner can acquire 2.5 times more views per rotation
than a typical (non-HD) CT scanner. This results in improved
spatial resolution. The images below are acquired with a high
definition protocol where both HD standard and HD bone
images are reconstructed for analysis for soft tissue as well
as for pathologies involving bone and joints (Figure 1).
Comparative images of normal routine bone reconstruction
and HD scan and reconstruction (Figure 2) show improved spatial
resolution with higher bone details in the HD bone images.
Figure 1. (A) HD standard; (B) HD bone
A B

28 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E m u s C u l o s k E l E T A l i m A G i n G
Figure 2. (A) Routine bone; (B) HD bone
A B
Figure 3. (A) HD standard; (B) HD bone
A B
The HD images clearly demonstrate the comminuted fracture of
calcaneus involving the posterior sub-talar joint. The visualization
of cortical margins and trabecular pattern is clearly seen in the
HD bone image. The spatial resolution of HD images can be up
to 230 microns (calculated using 0% MTF).
Using HD imaging in a knee study, we were able to appreciate
subtle findings such as a hair-line fracture of the patella in the
HD bone image and other soft tissue details in the HD standard
images (Figure 3).

29www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u em u s c u l o s k e l e t a l i m a g i N g
Gemstone Spectral Imaging in implant studies
We use dual energy acquisition with fast kV switching enabled
by the Gemstone Detector in many of our studies on patients
with orthopedic implants. The results were unparalleled and
promising. With the GSI technique, we created monochromatic
images specific for bone and implants. The projection data
based reconstruction technique with metal artifact reduction
software (MARs) helps significantly in the reduction of artifacts
from high density metal implants and allows the accurate
visualization of the underlying bone and adjacent soft tissue.
The 100 keV monochromatic image with MARs was able to show
the implosion of implant into the joint space and producing
pressure erosion of the articular surface of femoral condyle.
The GSI monochromatic technique with MARs is highly useful in
external fixators. Unlike internal fixators, imaging with external
fixators involves more challenging issues due to an increase in
beam-hardening artifacts that are primarily due to the air gap that
exists between the body and the external fixator. We were able
to use GSI with MARs to resolve this complex situation (Figure 6).
Figure 5. (A) 140 kV; (B) 100 keV with MARs
A B
Figure 4. (A) A routine reconstruction at 140 kV from a GSI scan data shows significant beam hardening artifact from the implant hardware. (B) Monochromatic image generated from the same GSI acquisition at 100 keV demonstrates the subtle reduction of metal beam hardening artifact without significant difference. (C) The same image reconstructed with MARs in which artifacts were completely removed and we were able to assess the implant integrity and adjacent tissue as well.
A B C

30 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E m u s C u l o s k E l E T A l i m A G i n G
Figure 6. (A) 140 kV; (B) 70 keV with MARs
A B
Figure 7. (A) Upper limb angiogram for vascular assessment post external fixation of humerus fracture. Note the extensive beam-hardening artifacts from the metal implants obscuring the visualization of the brachial artery. (B) and (C) illustrate 70 keV monochromatic 3D MIP and 3D VR transparency images depicting the normal patent vessel.
A B C
CT is often used to rule out vascular injuries in pre-surgical
and post-surgical orthopedic patients. GSI with MARs helps
us diagnose the presence of vascular injury in these complex
cases with a high degree of confidence.
Figure 7 demonstrates the efficacy of MARs in studies involving
external fixators by removing beam-hardening effects from the
hardware. The 70 keV MARs images show the tibia and the tibial
condyles. The margins and cortex of tibial condyle is well
visualized compared to the 140 kV standard.
Figure 8. These images show dynamic sequences of the ankle joint from flexion phase to extension phase. This demonstrates movement of the non-united fracture fragment and focal reduction in posterior sub-talar joint space with apposition of the talus and calcaneus.

31www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u em u s c u l o s k e l e t a l i m a g i N g
Figure 9. The coronal phased images reveal the movement of large fracture fragment in to the joint space.
Figure 10. The axial KCT images from flexion phase to the extension phase show the subluxation of patella.
Kinematic studies in musculoskeletal imaging
Kinematic evaluation of the joints involves the use of the Volume
Helical Shuttle (VHS) mode of image acquisition. A special
reconstruction algorithm—dynamic pitch reconstruction—is
used to help prevent artifacts due to movement. In our facility,
we have performed kinematic evaluation of studies for joints
including the elbow, wrist, knee, and ankle. Kinematic CT (KCT)
is highly useful in evaluating movement of loose bodies into the
joint space for assessing instability and predicting development
of arthritis.
With the advent of technological developments in CT such as
GSI, MARs, and HD, we are able to overcome previous limitations
in MSK CT imaging. The use of VHS in orthopedic studies has
resulted in the dynamic evaluation of joints. We have used
these new techniques very effectively in the evaluation of
MSK pathologies with a high degree of diagnostic confidence
and accuracy. n
G. Francis, MD, is a senior consultant radiologist at MIOT Hospitals Chennai specializing in MSK and vascular CT. He received his M.B.B.S. from Christian Medical College (Vellore), his D.M.R.D. from Stanley Medical College (Chennai), and his D.N.B. (radio diagnosis) BIR from Madras Medical College (Chennai).
K. Murali, MD, is the Director of Interventional Radiology at MIOT Hospitals Chennai practicing diagnostic and interventional radiology. He received his M.B.B.S. Coimbatore Medical College (City), medical degree from Gujarat University (City), and post-doctoral certificate in neuro and vascular. Dr. Murali has published twelve scientific articles, a text book chapter, and presented numerous scientific papers in national and international conferences.
R. Madan, MBBS, MD, is a Consultant Radiologist at MIOT Hospitals. Dr. Madan received his medical degree from the Government Medical College, Madurai, and his MBBS from Stanley Medical College. He spent three years as a senior resident at Sanjay Gandhi Post Graduate Institute of Medical Sciences. Dr. Madan’s areas of interest are musculoskeletal radiology and image-guided biopsy.
MIOT Hospitals Chennai is a 500-bed, multi-specialty hospital in India founded by a physician. The hospital is recognized as a leading center known for orthopedics and orthopedic research, including joint replacement surgery with 35,000 successful hip and knee replacement and revision surgeries. It is also the first hospital in the Asia-Pacific region and second hospital in the world to have a computer-integrated navigation system for joint replacement surgery. MIOT also has specialized centers for: nephrology, including the largest and most modern nephrology department in the country—performing five renal transplants each month and, in collaboration with Japan, kidney transplants across blood-type groups—and a state-of-the-art dialysis unit; thoracic and cardiovascular care offering endovascular grafting for aortic aneurysm by keyhole surgery procedures and beating heart surgery; neurology and neurosurgery; and pediatric cardiac surgery for treating congenital heart disorders.

32 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E 4 D o n C o l o G y
In order to improve accuracy in radiation therapy for chest and
abdomen cancers, it is necessary to visualize, control, and track
patient specific respiratory motion. Tumors near or around the
diaphragm will likely move with respiration.
Without the means to limit respiration-induced target or organ
motion, large treatment fields have to be used, potentially
resulting in more irradiation of surrounding normal tissues. As
a result, the risk of complications may increase. Conversely, if
smaller treatment fields are used, the target may move out of
the treatment field resulting in an under dose to the target.
Some techniques such as breath-holding, forced shallow
breathing, and respiratory-gated treatment techniques have
been implemented to account for respiratory motion.
Therefore, precise targeting of the tumor and tracking
of respiratory motion are important to patient outcomes.
Since October 2009, we have used Varian’s Real-time Position
Management™ (RPM) System, which uses an infrared tracking
camera and reflective marker to measure the patient’s
4D CT With Respiratory Gating Helps Locate and Track Lesions to Reduce Target VolumesBy Xiaodong He, MD, Radiotherapy and Thermotherapy Center, Shanghai Pulmonary Hospital
Figure 1. (A) Illustrates lesion location in inspiration; (B) shows lesion location in expiration, demonstrating the movement of the lesion during the respiratory cycle.
A B
Real-time Position Management (RPM) System is a trademark of Varian Medical Systems, Inc.

33www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u e4 D o N c o l o g y
We are able to deliver effective patient treatment with customized treatment plans based on each patient’s respiratory cycle.
Dr. Xiaodong He
www.gehealthcare.com/aw/applications/ advantage-4d/ »
respiratory pattern and extent of motion. Advantage 4D*, a
respiratory motion management application on the Advantage
Workstation, helps providers analyze respiration-induced motion
of anatomy based on data acquired using the Varian RPM in
conjunction with the GE RT CT system.
Prior to treatment planning, patient CT images are acquired
and processed in 4D. The patient is scanned using a Cine CT
respiratory protocol and the respiratory waveform file is
simultaneously recorded with an external respiratory gating
system, e.g., RPM. The Advantage 4D software then sorts
and saves the Cine CT image data into phases and intensity
projections (MIP, Average, Min-IP).
With GE’s Cine acquisition, the CT images of the MIP dataset
are utilized in the treatment planning system. We then select
the 4D CT phases corresponding to the 30%~70% breathing
phases of the patient.
In our facility, we are using the 4D data and RPM on approximately
10% of patients—those who have stable and reproducible breathing.
We have found that 4D CT data aids in assessing the tumor
location. Using the GE Advantage 4D with the Varian RPM system
has helped us reduce the inner target volumes. The impact on
patient treatment since the implementation is impressive. We
are able to deliver effective patient treatment with customized
treatment plans based on each patient’s respiratory pattern. We
are experiencing a decline in acute radiation-induced pneumonia
rates, which further increases our confidence in 4D treatment
planning and ability to effectively irradiate the lesion and spare
more surrounding healthy tissue. n
Professor He Xiaodong, MD, is the Chief Physicist and Vice Director of the Radiation Oncology Department at Shanghai Pulmonary Hospital. His research of radiophysics, radiobiology, and thermotherapy includes dosage study on EPID; X-ray beam dose distribution reconstruction; electron beam dose calculating model; enlargement of volume effect in LQ model; bioequivalent DVH (BDVH) calculation; RF thermodosage theorem; and portal image processing technique. He is also well known in China for his expertise on moving target radiation therapy.
Shanghai Pulmonary Hospital is affiliated to Shanghai Tongji University (also known as Shanghai Occupational Disease Hospital). The hospital opened in 1933 and the radiation oncology department—dedicated for lung and esophagus cancers and mediastinal and metastatic tumors—was built in 1989. Oncology equipment includes two Linear Accelerators (one with RPM), a set of large aperture 4D CT simulators, one X-ray simulator, and several treatment planning systems.

34 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E E M E R G E n C Y R A D i O l O G Y
CT has become an important diagnostic tool for the Emergency
Department (ED) physician. A recent study in the Annals of
Emergency Medicine found that in the US, approximately one in
seven ED patients received a CT scan as part of their evaluation.1,2
The top indications for CT use in the ED are abdominal pain, flank
pain, chest pain, shortness of breath, and trauma.
The study examined data from the National Hospital Ambulatory
Medical Care Survey on nearly 100 million patients receiving a CT
scan in the ED between 1996 and 2007. Between 1996 and 2007,
CT use during ED visits increased 330%, with the largest increase
in patients older than 79 (9.1% in 1996 to 29.1% in 2007).
However, the study found a correlation between CT use and
a drop in hospital admissions. According to one of the authors,
Keith Kocher, MD, University of Michigan, the likelihood of
hospitalization or transfer after a CT declined throughout the
study period, from 26% in 1996 to 12.1% in 2007. The rate
leveled off after 2003 despite a continued increase in the
adjusted, overall rate.
In addition to CT possibly correlating to a reduction in the rate
of hospitalization or transfers, the study also found it may impact
decisions about where hospitalizations occur, with a shift away
from expensive ICU admissions.
The following are profiles of two facilities utilizing CT in the ED to
positively impact patient outcomes and help clinicians make the
most appropriate care decisions.
1. Kocker KE, Meurer WJ, Fazel R, et al. National Trends in Use of Computed Tomography in the Emergency Department. Annals of Emergency Medicine 12 Aug 2011; published online
2. Barnes E. Rise in CT use linked to drop in hospital admissions. AuntMinnie.com. Available at http://www.auntminnie.com/index.aspx?sec=sup&sub=imc&pag=dis&ItemID=96135
St. Vincent Hospital
At St. Vincent Hospital (Indianapolis, IN), a Discovery CT750 HD
is an integral part of the hospital’s ED, Level II Trauma Center,
and Stroke Center of Excellence. Since opening the trauma
center, ED volumes have increased, says Nikki Duckworth, RT,
MBA, Manager of Medical Imaging Services. Today, the 39-bed
ED handles an average of 149 patients each day.
High-Definition CT Improves Triage and Door-to-treatment Times in Emergency Radiology
Figure 1. The Discovery CT750 HD scanner installed at St. Vincent Hospital.
Imag
es c
ourt
esy
of S
t. Vi
ncen
t Hos
pita
l.

35www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u ee M e R G e N c Y R a D i O l O G Y
“For routine cases, the nurse manager alerts us when the patient
is ready for CT,” Duckworth explains. “In trauma cases, a mass
page goes out with an estimated time of arrival, so the patient
goes straight to the CT when stabilized.”
For the most severe trauma patients, the CT protocol includes
the head, cervical spine, chest, abdomen, and pelvis, says
Michael Skulski, MD, Chair of Medical Imaging at St. Vincent.
“We want to assess the patient as quickly as possible, and this
system is very good from that perspective.” In fact, Corey Graff,
RT(CT), CT technologist at St. Vincent, is impressed by the exam
split capability on the Discovery CT750 HD. “If I have a trauma
patient and don’t have a patient ID, I can scan all the exams
in our protocol, one after another, and at the end send all the
exams wherever they need to go. I don’t have to re-landmark
and that helps with the patient flow.”
Dr. Skulski adds, “The speed of this system has addressed
the issue of patient motion and with ASiR we’ve decreased
radiation dose by 30% to 40%.** Reformats are virtually
instantaneous, and the trauma surgeons are very impressed
with the quality of the images.”
Selecting the Discovery CT750 HD was a carefully considered
choice. Says Duckworth, “We needed a CT that was fast, could
potentially help us lower radiation dose, and handle a variety
of exams.” This system provides all of the above and more
for St. Vincent.
Dr. Skulski is also impressed with the potential he sees with
Gemstone Spectral Imaging (GSI)—another key factor in selecting
the system. In fact, a physician from another state sought out
St. Vincent because of the GSI technology and referred a hip
replacement patient to the hospital for evaluation. “We could
identify a non-union, incomplete fracture proximally to the hip
replacement, and I’m not certain we would have identified that
without GSI.”
While it is too early for Dr. Skulski to make any definitive clinical
statements on the value of GSI, he’s excited at the potential
benefits. “We are still learning the capabilities of GSI and
haven’t yet scraped the surface of its impact.”
“As a Stroke Center of Excellence, the VolumeShuttle technology has
helped simplify the protocol and added noticeable improvement
to the study by enabling an increase in the area of interest,”
explains Dr. Skulski. Plus, based on outcome data and the
desire to reduce door–to-treatment time, the institution has
changed its initial neuro/stroke protocol from three studies to
one. Stroke patients first receive a non-contrast CT head. After
TPA administration and evaluation, if another CT study is ordered
the patient then receives a non-contrast CT of the head, a CTA
of the head and neck, and CT perfusion—these three studies
comprised the original neuro/stroke protocol. “Our goal is to
improve door-to-treatment time for these patients so they can
begin their anti-coagulation therapy sooner,” explains Dr. Skulski.
With the revised CT protocol using the high definition capabilities
of the scanner, the CT study has dropped from approximately
15 minutes down to three.
Looking back at their system choice, the team at St. Vincent
is confident the Discovery CT750 HD will meet their present
and future needs. Adds Dr. Skulski, “I’m confident with this
scanner we are only at the beginning of exploring new
innovations from GE.”
** In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.
“ As a Stroke Center of Excellence, the VolumeShuttle technology has helped simplify the protocol and added noticeable improvement to the study by enabling an increase in the area of interest.”
Dr. Michael Skulski

36 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E E M E R G E n C Y R A D i O l O G Y
Ludwig-Maximilians University Hospital
In the heart of Munich is one of Europe’s leading medical
research universities and public health centers. The nearly
1,000-bed University Hospital of the Ludwig-Maximilians
University (LMU) is home to one of the largest radiology
departments in Europe and chaired by Professor Maximilian
Reiser, FACR, FRCR, a world-renowned radiologist.
Nearly two years ago, the University Hospital at LMU installed
a Discovery CT750 HD in the ED. According to Professor Ulrich
Linsenmaier, Vice Chair for Clinical Operations in the Department
of Clinical Radiology, it is the most reliable scanner the hospital
has ever had in the ED with nearly no unplanned downtime.
“We’ve seen an increase in patient volume and our ability
to handle a series of emergency patients is important, as
in mass casualties,” Prof. Linsenmaier says. “Now, with the
Figure 2. Low-dose MDCT of the cervical spine; images were obtained on 64-row MDCT standard scanner using FBP (left, DLP of 265.05 mGy-cm) and on the new Discovery CT750 HD scanner using ASiR (right; DLP of 107.36 mGy-cm).
A B
“ By introducing volume image reading in the ED, the workup for a mass casualty patient has decreased from an average of 15 minutes to 8 minutes.”
Professor Ulrich Linsenmaier
Imag
es c
ourt
esy
of L
udw
ig-M
axim
ilian
s U
nive
rsity
Hos
pita
l.

37www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u ee M e R G e N c Y R a D i O l O G Y
Figure 3. Whole-body MDCT in different patients after major trauma (polytrauma) obtained on a Discovery CT750 HD scanner using ASiR; images allow for a quick and comprehensive diagnosis of multiple injuries and fractures of the skull, spine, and even complex peripheral injuries involving bony and vascular structures at the same time.
D E
A B C
F
Discovery CT750 HD in our ED, we have a faster workflow
and prompt access to the imaging data, especially by volume
image reading.
“By introducing volume image reading in the ED, the workup
for a mass casualty patient has decreased from an average of
15 minutes to 8 minutes,” he says. Moreover, the axial, multiplanar,
and volume rendered images are readily available, an important
factor in ED imaging.
“The HD scan mode provides excellent spatial resolution and
scanning of large body volumes,” Prof. Linsenmaier explains.
“The protocols for major trauma patients include long scan fields,
and the X-ray tube performs remarkably well with virtually no
cooling problems,” he adds.
Reducing patient radiation dose with ASiR is an impressive
feature as well. In major trauma cases undergoing whole-body
CT, the ED department has decreased dose by nearly 30%,
Imag
es c
ourt
esy
of L
udw
ig-M
axim
ilian
s U
nive
rsity
Hos
pita
l.

38 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E E M E R G E n C Y R A D i O l O G Y
Michael S. Skulski, MD, is the Department Chair of Radiology at St. Vincent Hospital & Health Services at the 86th Street campus. He graduated from University of Cincinnati College of Medicine and completed a residency in Diagnostic Radiology at Mayo Clinic in Rochester, Minnesota, where he was Chief Resident. In addition, he completed a fellowship in cross-sectional imaging at the Mayo Clinic. Dr. Skulski’s special interests include body imaging, body intervention and non-invasive vascular imaging. He is also a member of the musculoskeletal team with a special interest in foot and ankle imaging.
Nikki D. Duckworth, MBA, RT, is the Manager of Medical Imaging Services at St. Vincent Hospital (Indianapolis) at the 86th Street campus. She graduated from: American Intercontinental University with an MBA in Operations Management; Indiana Wesleyan University with a BS in Business Management; and Indiana University with an AS in Radiologic Science. She is currently studying to become a Fellow of the ACHE (American College of Healthcare Executives). Before working in management, Nikki worked as a MRI, CT, X-ray, and Nuclear Medicine Technologist.
Corey W. Graff, RT(R)(CT), is a CT technologist at St. Vincent Hospital & Health Service (Indianapolis) at the 86th Street campus. He graduated from radiology school at Hancock Memorial Hospital (Greenfield, IN).
As a member of Ascension Health, St. Vincent Health is a part of the largest Catholic, mission-driven, not-for-profit health care system in the United States. St. Vincent Indianapolis Hospital recently earned the Distinguished Hospital for Clinical Excellence™ recognition by HealthGrades, the leading independent healthcare ratings organization.
Corey Graff
Nicole Duckworth
Professor Ulrich Linsenmaier, MD, PhD, is Associate Chair, Associate Professor of Radiology, and Managing Attending Radiologist in the Department of Clinical Radiology at Ludwig-Maximilians-University (Munich). He is the 2011-2013 President of the European Society of Emergency Radiology (ESER). Areas of professional interest include: emergency radiology; interventional radiology (IR); body imaging (MSCT, MRI); and neuroradiology (NR). Professor Linsenmaier has presented more than 200 scientific talks, received three scientific awards, and authored more than 70 original articles and five books. He is a reviewer for The Lancet, European Radiology, Investigative Radiology, European Journal of Radiology, RöFo, Der Radiologe, Der Unfallchirurg.
Munich University Hospital is comprised of two facilities: the nearly 973-bed University Hospital of the Ludwig-Maximilians University (LMU) and 1,349-bed Grosshadern campus. Approximately 500,000 patients receive medical care from the 45 departments and institutes at both campuses. Recognized as one of the major university hospitals in Europe, Munich University Hospital conducts 50,000 surgical interventions each year and is known for its pioneering work in cardiosurgery and outstanding transplantation expertise.
Hospital for Clinical Excellence is a trademark of HealthGrades.
Prof. Linsenmaier says. Significant dose reduction capabilities will
further impact the department’s choice of imaging device, as a
CT image can provide more information than digital radiography.
Currently, the University Hospital performs clinical low-dose CTs
of the C-spine between 0.7 and 1.1 mSv.
In addition to lowering dose, the Discovery CT750 HD is further
impacting the quality of patient care through new capabilities.
Specifically, larger perfusion volumes along with CT angiography
and temporal subtraction imaging (TSI) are used for diagnosing
stroke and pulmonary embolisms (PE).
With these imaging tools, the University Hospital now uses CT
in place of MRI diffusion imaging. “Our protocol combines native
CCT and CTA of the supra aortic vessels with a perfusion scan
of the cerebrum,” explains Prof. Linsenmaier. An additional
advantage of using CT for these patients is the availability
of the scanner 24/7 with direct access in the ED.
“Monitoring the patient is easier and we don’t have to transfer
them out of the ED,” he adds. “We can work up the patient in one
robust exam—this is an entirely new way for us to handle stroke
and PE patients.”
While the potential for reducing dose in complex cases most
impresses Prof. Linsenmaier, he also recommends that other
hospitals seeking to add CT in their ED evaluate system reliability.
“For us, the most important factor is reliability with little unplanned
downtime followed by a strong industrial partner that can
provide excellent technical and applications support.”
He notes that using CT in the ED has increased exponentially
in large institutions over the last decades, and new capabilities
such as Iterative Reconstruction techniques will become even
more important to future CT purchasing plans. “Even with the
increase in scan volumes and use of CT in the ED, we can offer
patients low dose with the Discovery CT750 HD.” And that, he
says, is most impressive.
At both St. Vincent Hospital and the University Hospital of LMU,
CT is a crucial diagnostic tool for trauma and stroke patients.
Speed, image quality, and applications such as GSI, perfusion,
and volume rendering are impacting patient care. n

39www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u el o w - d o s e p e d i a t r i c i m a g i N g
Pediatric Hospitals Bring Low-dose CT to the Middle EastFor years, radiologists have been cognizant of the importance
of limiting pediatric patients’ exposure to radiation dose. Building
on the ALARA principle, the Image Gently Campaign specifically
targets awareness of radiation dose levels to children and
young adults.
However, reducing radiation dose based on a reduction in kV
sometimes results in noisy images that can negatively impact
the radiologist’s diagnostic capabilities. For acutely sick children,
such as those afflicted with heart ailments (anomalies) or
pediatric cancers, treatment planning often requires high-quality
CT images. Yet, radiologists may, in some instances, be hesitant
to order additional CT exams out of concern that the pediatric
patient is being repeatedly exposed to medical imaging radiation.
This is the case in the Kingdom of Saudi Arabia. There, two
leading hospitals are using ASiR to enable a reduction in the
radiation dose delivered to pediatric patients while maintaining
image clarity to provide effective patient treatment.**
The beat goes on
At King Abdulaziz Cardiac Centre, Dr. Fahad Al-Habshan, a
consultant in pediatric cardiology and cardiac imaging, uses
CT to image children prior to open heart surgery.
“We tried to use a lower radiation dose in our CT imaging, but the
images were noisy and hazy,” Dr. Al-Habshan says. “It is always a
balance between the radiation dose and the clarity of the image,
particularly when it comes to small children where we are
* *In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.
“ With ASiR, we obtain the same quality images at a much lower dose—it reduces the noise and produces crisp images.”
Dr. Fahad Al-Habshan

40 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E l o w - d o s E p E d i A T r i C i m A G i n G
looking at small vessels and structures. We need to be very
accurate and precise in our diagnosis of pediatric cardiac
patients, and that has complicated our efforts to reduce dose.”
Specifically, the pediatric cardiology surgeons require high
quality images for surgical planning. “Everything in the operating
room is carefully planned; surprises add precious time that can
increase the complications for very young patients,” he adds.
Good images help the surgeon conduct the procedure in the
shortest time possible to minimize risk to the patient’s safety.
“Children are more sensitive to radiation,” says Dr. Al-Habshan.
However, when the hospital’s LightSpeed* VCT received an ASiR
upgrade in September 2009, low-dose CT imaging became a
reality. “With ASiR, we obtain the same quality images at a much
lower dose—it reduces the noise and produces crisp images,”
explains Dr. Al-Habshan. The difference is significant. “Today
with ASiR, almost all our children are imaged with less than
1 mSv radiation dose,” he adds.
“GE is focused on developing hardware and software that
enhance image quality and lower radiation dose,” says
Dr. Al-Habshan, “and I think that offers more benefit to
the patient than the number of detectors.”
Figure 1. Detecting aortic arch obstruction and coronary compression in a 13-month-old girl using gated CT angiography with ASiR (0.8mSv). (A) Sagittal view reveals the aortic arch and an area of coarctation. (B) 3D reconstructions of the heart demonstrating the aortic anastomosis and the Right Ventricle—Pulmonary Artery conduit. Calculated radiation dose: 20.57 X 2.16 X 0.018 = 0.8 mSv (obtained by 2007 ICRP recommendations using chest factor of 0.018 *DLP for children one to five years).
BA
Figure 2. Confirming a vascular ring with mirror-image branching using CT Angiography with ASiR (0.66 mSv). 3D reconstruction of the heart shows the complete vascular ring, formed by the right aortic arch and the left-sided ductus arteriosus, around the trachea and esophagus. Also seen are the airway and the nasogastric tube in the esophagus. Notice the mirror image branching of the aortic arch, which is very unusual with this type of vascular ring. Calculated radiation dose: 11.77 X 2.16 X 0.026 = 0.66 mSv (obtained by 2007 ICRP recommendations using chest factor of 0.026 * DLP for children under one year).

41www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u el o w - d o s e p e d i a t r i c i m a g i N g
A ray of hope
As the first children’s cancer center in the Middle East, King
Fahad National Centre for Children’s Cancer and Research
is widely recognized as a leading institution that provides
comprehensive oncology care for pediatric cancer patients
throughout the region. The hospital aims to provide the best
level of care in medical imaging through the acquisition of
state-of-the-art equipment and techniques.
“We are very concerned about the possibility of our patients
being over-exposed to radiation dose in CT scanning,” says
Lefian Al Otaibi, MD, Acting Chairman of Radiology and Head
Section, Pediatric Radiology. The center treats patients ranging
in age from three months to 14 years.
Dr. Otaibi’s concern regarding dose began to diminish when
he learned more about ASiR during the installation of the
BrightSpeed Elite CT scanner. “We implemented it immediately
to see the difference in image quality and dose using ASiR, and
it was clearly noticed.”
Figure 3. Chest abdomen pelvis exam of 13-month-old pediatric patient; (A) volume rendered (VR) bone, liver, and kidney; (B) portal vein VR on coronal view; (C) VR with portal. Total acquisition time of 5 sec for 300 mm coverage using ASiR 50% for a DLP=59.04 mGy.cm (Equivalent dose = 0.8 mSv). DLP was 59.04 mGy.cm for an effective dose of 0.8 mSv (obtained by EUR-16262 EN, using a Chest pediatric factor of 0.013*DLP and an Abdomen Pelvis pediatric factor of 0.015*DLP).
BA
C

42 A GE Healthcare CT publication • www.ctclarity.com
C l i n i C A l v A l u E l o w - d o s E p E d i A T r i C i m A G i n G
In fact, the reaction from radiologists was so positive that the
facility launched a new initiative to reduce unnecessary dose
to patients. The initiative includes two principles of radiation
protection: appropriate justification for ordering the procedure
and careful optimization of the radiation dosage used during
the procedure according to age and weight.
“ASiR has allowed us to lower the radiation dose delivered to
our patients compared to our previous scanner,” adds Dr. Otaibi.
“This is a department goal for all routine studies and with
all radiologists.”
The value of ASiR is most important in follow-up, or repeat
exams, particularly for oncology patients who must often
receive annual or bi-annual exams to detect any relapse.
According to Dr. Otaibi, ASiR offers the radiologists the ability
to conduct needed follow-up exams with decreased concerns
of additional radiation dose. “Without ASiR, there are some
follow-up exams we probably would not do,” he says.
In addition to potentially minimizing dose with ASiR, the facility
also utilizes the high pitch on the BrightSpeed Elite to decrease
scan time, says Abdulaziz Bawazeer, Radiology Supervisor.
Figure 4. Chest abdomen pelvis exam of 13-month-old pediatric patient; (A) Aorta plus Aorta VR; (B) MIP Liver and CAP Vessels; (C) Minip Lungs & Bronchus; Total acquisition time of 5 sec for 300 mm coverage using ASiR 50% for a DLP=59.04 mGy.cm (Equivalent dose = 0.8 mSv). DLP was 59.04 mGy.cm for an effective dose of 0.8 mSv (obtained by EUR-16262 EN, using a Chest pediatric factor of 0.013*DLP and an Abdomen Pelvis pediatric factor of 0.015*DLP).
BA
C

43www.gehealthcare.com/ct • November 2011
c l i N i c a l v a l u el o w - d o s e p e d i a t r i c i m a g i N g
www.gehealthcare.com/LowerDoseByDesign »
Fahad Al-Habshan, MD, is a consultant in pediatric cardiology and cardiac imaging at King Abdulaziz Cardiac Centre, National Guards Health Affairs.
King Abdulaziz Cardiac Centre is a tertiary care cardiac center in Riyadh, Saudi Arabia, that conducts approximately 400 open heart procedures on children every year. It is affiliated with one of the largest medical institutions in Riyadh, and provides both adult and pediatric care. The center receives pediatric referrals from all over the country.
Lefian Al Otaibi, MD, is a Consultant Radiologist at King Fahad National Centre for Children’s Cancer and Research and King Faisal Specialist Hospital and Research Center.
Abdulaziz Bawazeer is the Radiology Supervisor at King Fahad National Centre for Children’s Cancer and Research.
The King Fahad National Centre for Children’s Cancer and Research opened in 1997. Located north of Riyadh on a two-acre site, it is an integral part of the King Faisal Specialist Hospital and Research Centre and provides both inpatient and outpatient services to Pediatric Hematology/Oncology patients. Seventy to 80 pediatric stem cell transplants are performed per year. The hospital is locally known as the Children’s Cancer Centre or CCC.
The King Faisal Specialist Hospital and Research Center (KFSH&RC) is a modern state-of-the-art hospital with 894 beds. Located in Riyadh, KFSH&RC is the national referral center for oncology, organ transplantation, cardiovascular diseases, neurosciences and genetic diseases. A full range of primary, secondary, and tertiary health care services is provided.
“When scanning children, we want them to spend less time
within the gantry,” he explains. “That will further help lower
radiation dose and reduce motion, which helps with image
quality. We also provide artwork on the walls of the room and
television screens to help keep the children more comfortable
and relaxed.”
With most patient cases being CAP or HN, both Dr. Otaibi
and Mr. Bawazeer believe it is imperative to reduce dose in all
procedures. Their results with ASiR are impressive; the studies
maintain image quality and provide good visualization of
contrast enhancement at lower dose and noise levels.
“We are confident our patients are receiving optimized dose
without affecting the diagnostic quality of the exam,” notes
Mr. Bawazeer. “And that provides the potential for outstanding
clinical outcomes.”
At King Abdulaziz Cardiac Centre and King Fahad National
Centre for Children’s Cancer and Research, ASiR enables
clinicians to provide the highest level of diagnostic care
at the lowest possible dose. n
“ ASiR has allowed us to lower the radiation dose delivered to our patients compared to our previous scanner. This is a department goal for all routine studies and with all radiologists.”
Dr. Lefian Al Otaibi
Abdulaziz Bawazeer

44 A GE Healthcare CT publication • www.ctclarity.com
C A s E s T u d y L o w - d o s E C A r d i A C i m A G i n G
Contrast ProtocolBrand/type of contrast: Ioversol
Contrast injection rate: 5 cc/sec
Total contrast amount: 80 cc
Saline injection rate: 5 cc/sec
Total saline amount: 40 cc
Acquisition Protocol
Scanner: Optima CT660 with ASiR
Scan type/slice thickness:
Snapshot Pulse / 0.625 mm
Coverage: 40 mm
Rotation time: 0.35 sec
Total elapsed time: 5.1 sec
Total x-ray exposure time: 1.76 sec
mAs: 106.75
kV: 120
Recon kernel: Detail
SFOV: Cardiac large
DFOV: 25 cm
Heart rate: 47 BPM
BMI: 30
ASiR: 40%
Low-dose CTA With ASiRBy Roberto Cury, MD, cardiologist, IDS (Instituro de Diagnóstico de Sorocaba) and Melissa Megumi S. Kuriki, Advanced Application Specialist, GE Healthcare Latin America
When performing stent evaluation by CT, it is preferred to implement low radiation dose
particularly due to the patient’s previous exposure to radiation during the stent placement
procedure in the cath lab. The Optima CT660 may achieve low dose coronary CTA with
ASiR and provide high-quality images for visualizing the lumen and calcified plaque.**
Figure 1. 3D images of the heart showing stents in DCA, Mg, and RCA.
A B
Figure 2. Transparent 3D images showing calcification plaque inside of the stents.
A B
**In clinical practice, the use of Veo may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.

45www.gehealthcare.com/ct • November 2011
c a s e s t u d yL o w - d o s e c a r d i a c i m a g i N g
Patient history
The patient is a 51-year-old male with a BMI
of 30 and family history of coronary disease.
Patient had atypical chest pain at the time
and was indicated for CT to evaluate three
stents, LDA, OM, and RCA, implanted eight
months earlier to rule out in-stent restenosis.
Patient findings
Patient showed no sign of in-stent restenosis;
there was presence of discrete luminal
narrowing in the distal left main of the
coronary artery and the right coronary artery.
Discussion
The Optima CT660 with ASiR provides an
opportunity to conduct a low-dose CT study.
Using ASiR, patient dose was reduced with
high image clarity in the cardiac study. In
our region, the Optima CT660 is the first CT
scanner with low-dose technology, and it
helps demonstrate to patients our concern
regarding patient dose and the environment.
In particular with the cardiac exam, we have
better visualization of the coronary artery,
stents, and calcified plaque. We believe
this system is making a difference in our
clinical diagnosis. n
Figure 3. Oblique images of coronary artery showing stents and calcified plaque with high image quality without beam hardening.
A B
C D
Figure 4. CT coronary study with 2.57 mSv acquired in 5.1 sec with prospective gated acquisition. (DLP 183.77 mGy cm with a conversion factor of ICRP 0.014*DLP)
Roberto Cury, MD, PhD, FSCCT, is the Chief Executive Officer of Virtual Heart, the first cardiac imaging teleradiology group in Brazil. He is also a cardiologist and Director of Cardiac CT and MRI at Samaritano Hospital (Sao Paulo, Brazil). Dr. Cury received his doctorate degree from Santa Casa School of Medical Sciences in Brazil and finished his clinical fellowship in Cardiac CT and MRI at InCor, Heart Institute of Sao Paulo. Dr. Cury was a pioneer in Brazil in the field of Stress Myocardial Perfusion Cardiac CT and concluded his PhD at InCor, Heart Institute of Sao Paulo. He has contributed to the field of cardiovascular imaging with published papers, book chapters, case reports, and invited presentations. Dr. Cury is currently the Director of the SCCT Brazilian International Regional Committee.
Instituto de Diagnósticos Sorocaba (IDS) was founded in 1996 by radiologists who embraced a mission to provide differential and compassionate medical service. Today, IDS provides high-quality diagnostic care to approximately 500 patients each day, offering complete diagnostic services for various laboratory testing and diagnostic imaging, the latter including the latest advanced equipment such as the Optima CT660.
The organization’s management team guides and monitors all activities to ensure fulfillment of the company mission and philosophy and, as a result, IDS has won the confidence and loyalty of physicians and the local population.

46 A GE Healthcare CT publication • www.ctclarity.com
C A s E s T u d y l o w - d o s E p E d i A T r i C C T A
Acquisition ProtocolScanner: LightSpeed VCT
Scan type/slice thickness:
Non-gated/ 0.625 mm
Scan range: 95 mm, aortic arch to diaphragm
mAs: 120 mA
kV: 80 kV
Gantry rotation: 0.4 sec
Radiation time: 0.9 sec
Reconstruction: ASiR at 30%
DLP: 9.36
Calculated radiation dose:
9.36 X 2.16 X 0.026 = 0.5 mSv (using ICRP 2007 conversion factor of 2.16)
Confirming a Diagnosis of Double Aortic Arch in a NewbornBy Fahad Al Habshan, MD, Consultant, Pediatric Cardiology and Cardiac Imaging and Program Director, Pediatric Cardiology Fellowship, King Abdulaziz Cardiac Center, National Guards Health Affairs
Managing children with congenital heart disease (CHD) requires accurate diagnosis prior
to intervention—a task most often accomplished with echocardiography as the primary
diagnostic tool. However, it is not always successful, given the ultrasound’s inherent
limitations in the presence of air, bone, scar, or obesity. In addition, this modality does
not always demonstrate in sufficient detail the complex extra-cardiac vascular
structures, and airway and lung pathologies associated with CHD.
When echocardiography is unable to render a definitive diagnosis, alternative tools
must be applied—tools such as CT angiography (CTA). It has been proven an excellent
alternative, generating detailed images of structures throughout the thorax. However,
the trade off is radiation exposure, which is of special importance for small children
and infants. With GE Healthcare’s Adaptive Statistical Iterative Reconstruction (ASiR), it
is now possible to capture high-quality CTA studies of small children and infants at very
low radiation dose levels.**
Patient history
A newborn was diagnosed antenatally with a double aortic arch. A non-gated, low-dose
CTA exam was ordered to help confirm the diagnosis and assess the airway.
Figure 1. (A) Axial MIP reconstruction at the level of the two aortic arches. RAA: right aortic arch, LAA: left aortic arch. (B) Dose report showing the very low dose with DLP of 9.36.
**In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.
A B

47www.gehealthcare.com/ct • November 2011
c a s e s t u d yl o w - d o s e p e d i a t r i c c t a
Results and findings
A double aortic arch with a complete vascular ring around the trachea
and esophagus is clearly visible in an axial view (Figure 1A). The radiation
dose report (Figure 1B) highlights the low dose used in this study. The 3D
reconstructions include a posterior view (Figure 2A), demonstrating the
double aortic arch with a complete vascular ring around the trachea and
esophagus. Another view (Figure 2B) shows the airway and nasogastric
tube in the esophagus.
The infant underwent surgery to divide the smaller left aortic arch and the
ligamentum arteriosum that is located on the left side. The CTA images
served as the surgeon’s primary roadmap for planning this repair; they
gave him a very clear image in his mind and on the operating-room
screen, improving the quality of care delivered to this patient.
Discussion
Recent advances in CTA have made it an even more useful diagnostic tool.
For example, state-of-the-art multi-detector CT scanners have reduced
scan times to just a few seconds. In children in particular, multi-detector
CTA’s speed may allow the physician to minimize or eliminate the need for
general anesthesia or deep sedation, which is a tremendous advantage
in this population. Furthermore, its spatial resolution promotes accurate
diagnosis of anomalies involving the systemic and pulmonary veins and
arteries, as well as the coronary vessels.
Fortunately, the issue of radiation exposure is now being addressed with
today’s most advanced CT scanners, thanks to new scanning protocols and
software. ASiR has demonstrated its ability to produce images of exceptional
clarity and signal-to-noise at lower radiation doses. The result is we can
scan many of our young patients, including infants and small children,
at doses of less than 1 mSv with consistently excellent image clarity. n
Figure 2. (A) 3D reconstruction with a posterior view showing both aortic arches. RAA: right aortic arch, LAA: left aortic arch. (B) 3D reconstruction with a posterior view showing both aortic arches, the airway (blue), and a nasogastric tube in the esophagus (green). RAA: right aortic arch; LAA: left aortic arch
A
B
Fahad Al Habshan, MD, is Program Director, Pediatric Cardiology Fellowship, at King Abdulaziz Cardiac Center, National Guard Health Affairs (Riyadh, Saudi Arabia). Dr. Habshan is also Assistant Professor, Cardiac Sciences at King Saud Bin Abdulaziz University for Health Sciences (Riyadh). He specializes in pediatric cardiology and cardiac imaging.
As the largest and most advanced medical complex in the Kingdom of Saudi Arabia, National Guard Health Affairs (NGHA) includes medical “cities”strategically located across the land. Perhaps the most impressive of them all is King Abdulaziz Medical City in the capital of Riyadh. This state-of-the-art center is equipped with nearly 1000 beds for conventional, surgical and emergency admissions, and offers nearly all medical specialities—from Pediatric Cardiology and Emergency care that are second to none, to the full range of leading-edge Ambulatory, Primary, Preventive, Surgical and Critical Care services. It boasts the lowest mortality and morbidity rates in the nation. Educating the healthcare providers of tomorrow is also high on the list of the NGHA’s objectives—an objective that is being addressed via the pioneering King Saud Bin Abdulaziz University for Health Sciences, where our author serves as an assistant professor of Cardiac Sciences.

48 A GE Healthcare CT publication • www.ctclarity.com
C A s E s T u d y L O W - d O s E N E u R O W I T H A s I R
Contrast ProtocolBrand/type of contrast:
Iopamidol
Contrast injection rate:
4 ml/sec
Total contrast amount:
60 ml
Saline injection rate:
2 ml/sec
Total saline amount:
30 ml
Acquisition ProtocolScanner: Lightspeed VCT
with ASiR
Scan type/slice thickness:
Volume Helical Shuttle/5 mm
Coverage: 160 mm
Rotation time: 0.4 sec
Total elapsed time:
31.16 sec
Total x-ray exposure time:
17.16 sec
mAs: 150 mA
kV: 100
Need parameter
10 passes
Recon kernel: Soft
SFOV: 32.0 cm
DFOV: 22.1 cm
Effective dose (1207.30 [Total DLP] x 0.0023 [Tissue Factor] for head with phantom 16 cm = 2.77 mSv.
(As per ICRP-60 tissue weighting factor.)
Critical Low-dose Neuro Imaging with ASiRDetection of cerebral Arterio-Venous Malformation (AVM) using VHS on Lightspeed VCT
By Zakir Hussain, MBBS, MD, PhD, Fellow-AIE-Japan, Consultant Radiologist, Square Hospitals Ltd, Dhaka, Bangladesh; and Karthik Anantharaman, MD, Marketing Manager–CT (South Asia), Muhammad Sadiqur Rahman, Product Specialist–CT (Bangladesh), and Nitin Bhardwaj, Clinical Application Specialist–CT (East Zone–India) from GE Healthcare
Beginning with the first CT scanner, CT radiation dose has been a concern in
medical imaging. Even before the advent of multi-detector CT (MDCT), there have
been innovations aimed at developing different techniques to reduce radiation dose
and improve image quality. Dose reduction techniques such as Automated Exposure
Control and BMI-based protocols for cardiac scanning and application of different
image space filters have been successful in helping us limit radiation exposure to
patients undergoing CT scans.
All of these techniques provide the desired level of optimized dose management.
Filtered Back Projection (FBP), the conventional technique in use for almost three
decades to reconstruct the images from raw data, still falls short of expectations
when it comes to obtaining the full potential of reducing radiation dose.
A recent alternative technique is the use of Iterative Reconstruction (IR) to
overcome the limitations of FBP. Adaptive Statistical Iterative Reconstruction (ASiR)
is an IR technology that may help clinicians achieve a confident diagnosis with lower
dose.** ASiR may also enable improvement in low contrast detectability. In routine
imaging at Square Hospitals Ltd, Dhaka, we normally use 40% to 50% ASiR
consistently for all studies.
The following is a case that demonstrates the benefit of ASiR for us in low-dose,
critical, neuro-imaging applications.
Patient history
A 45-year-old male with known right fronto-parietal AVM presented to the radiology
department. Previous history revealed that a CT-guided stereotactic radiosurgery
was performed in November, 2000.
The Volume Helical Shuttle (VHS) scan technique was used to achieve the low-dose,
multi-phasic imaging of the brain vasculature.
**In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.

49www.gehealthcare.com/ct • November 2011
c a s e s t u d yL O W - d O s e N e u R O W I t H a s I R
Results
Right-side frontal and parietal AVM was noted with right middle
cerebral artery (MCA) and right anterior cerebral artery (ACA)
as feeder vessels and superior sagittal sinus and branch of right
transverse sinus being the draining veins. Volume Helical Shuttle
(VHS) was a very useful technique to help us detect feeder and
draining vessels of an AVM.
Discussion
At Square Hospitals Dhaka, we recently upgraded our
LightSpeed VCT system to include ASiR. Until the upgrade,
physicians referring their patients for CT scans to our department
were concerned with the additional radiation exposure in follow-up
scans. This fear has now been addressed with the introduction
of ASiR on the upgraded LightSpeed VCT system. We can now
demonstrate to our referring physicians the capability to deliver
lower radiation dose with ASiR on our CT scanner and, hence, build
confidence among them to refer patients for follow-up studies.
In our experience, ASiR is a significant advancement in CT dose
optimization technology that balances image quality, noise, and
dose. ASiR has made low-dose imaging across body regions a
reality in our facility. In addition, VHS aids our clinical diagnosis
significantly through extended coverage with multi-phasic
information. It also helps achieve different phases of contrast
for the desired anatomy with a fixed amount of contrast. n
Mohammad Zakir Hussain, MBBS, MD, PhD, is a Consultant Radiologist and Head of the Department of Radiology and Imaging at Square Hospitals Ltd. (West Panthapath, Dhaka, Bangladesh). Dr. Hussain received his Doctor of Philosophy in Medical Science (Clinical Subject: Radiology) from the Yamanashi Medical University and his Bachelor of Medicine & Surgery (MBBS) Examination from the institute of Post Graduate Medicine & Research (IPGMR) under the University of Dhaka, Bangladesh. He also completed a post-doctoral fellowship at Yamanashi Medic al University (Japan). Dr. Hussain’s clinical interests are in MRI, CT, and MRS, with special emphasis on coronary CT angiogram and other CT and MR angiogram studies. He helped establish the Interventional Radiological Center of Square Hospital Ltd.
Square Hospitals Limited is a 320-bed, tertiary care hospital. The hospital is an affiliate partner of Methodist Healthcare (Memphis, TN USA), SingHealth (Singapore), Bangkok Hospital Medical Centre, (Thailand), and Christian Medical College (Vellore, India). Square Hospital is located in the heart of Dhaka and aims to serve a greater portion of the capital city. At present it is comprised of: The main hospital building is 18 stories and approximately 450,000 sq. ft.; the second building (ASTRAS) is located across the street and is 16 stories with 136,000 sq. ft.
Figure 1. VHS Study demonstrating AVM in the right frontal and parietal lobes where the feeder vessel is coming from the right MCA and the right ACA.
A
D
B
E
C
F

50 A GE Healthcare CT publication • www.ctclarity.com
C A s E s T u d y O N C O L O G y W O R K F L O W
Acquisition ProtocolScanner: LightSpeed VCT
Scan type/slice
thickness:
Helical 1.25 mm
Pitch: 1.375
Rotation time: 0.6
mAs: 338
kV: 120
By Valerie Laurent, MD, PhD, radiologist, Central University Hospital, Nancy
Abstract
OncoQuant has proved to be an invaluable tool for tracking of oncology studies in
our facility. We can compare a seemingly limitless number of CT, MR, and PET exams.
Moreover, OncoQuant provides a structured workflow for using base lining and NADIR
to determine patient response to treatment according to RECIST guidelines.
Patient history
The patient is a 47-year-old male with liver metastases of an endocrine tumor
in the pancreas. Palliative treatment: first line chemotherapy in December, 2006.
Software
• Dexus workflow software(s) used: OncoQuant
• Length of time used at site: 1 year, used routinely (daily)
• Platform used (Wkst/Server): AW workstation
Patient findings
The patient returned for evaluation in December, 2010. There was a partial response
to treatment followed by progression, and the NADIR was set to the date with the best
response to treatment as per RECIST guidelines.
The summary table was used to assess the percentage of disease progression from
NADIR (Figure 1).
If the calculation is made from the original baseline, the tumor growth since December,
2006 is 11% (Figure 2). But it is important to consider that the gold standard is NADIR
according to RECIST guidelines. Using the RECIST methodology, the October, 2009
review becomes the new reference (NADIR) from which the progression of the disease
should be evaluated. Using the summary table in Figure 1, we can clearly see that there
is an evolution of 73% of the lesions based upon the RECIST 1.1 criteria (total of Dmax of
the initially identified target lesions). This indicates there is a progression of the tumor,
and, therefore, a need to change patient treatment.
Multi-modality Oncology Workflow for Comprehensive Follow-up and Treatment

51www.gehealthcare.com/ct • November 2011
c a s e s t u d yO N c O L O G y W O R K F L O W
Figure 1. Summary Table
Discussion
There are relative inconsistencies with the planning of treatment
and follow-up of oncology cases between different sites and
even between oncologists at the same hospital. Although the
results are directionally correct, repeatability and reproducibility
are often challenges when it comes to comparative results.
With OncoQuant, we were able to establish a consistent,
repeatable, and rapid diagnostic workflow across different cases
and physicians, even utilizing exams from several years prior as
a baseline. We came to find that through this workflow, we were
able to achieve:
• Quick comparison of follow-up exams from the baseline exam;
• Comparison of several exams without virtually any apparent limit;
• Cross registration of chosen target lesions from lesions in the
initial exam;
• Comparison of measurements obtained with an automatic
registration between the initial exam and follow-up exam; Figure 2. Reference of current to the baseline.

52 A GE Healthcare CT publication • www.ctclarity.com
C A s E s T u d y O N C O L O G y W O R K F L O W
Valérie Laurent, MD, PhD, is a radiologist at the Central University Hospital, Nancy (Nancy-Brabois, France). Dr. Laurent has spent over 12 years focusing on abdominal imaging in oncology and during that time has used MRI and CT extensively. She recently received her doctorate degree in 2010.
The Central University Hospital of Nancy comprises a hospital network of over 1,600 beds serving over 600,000 patients with 30,000 emergency entries a year. There are two main locations: one in the center of Nancy and the other in the suburbs of Brabois.
Inaugurated in 1973, the Hospital Brabois for Adult Studies is the cornerstone of the Brabois hospital network serving first as a university hospital within close proximity to the Faculty of Medicine and secondly as the premier regional center for combating cancer with over 945 beds.
Figure 3. Tracking one of the targets on the three first exams.
A B
C
• Consistent results that are table and operator independent;
• Clinical answers that are less tedious to perform and more
objective and independent of the modality, acquisition
technique, and clinician;
• Automatic registration of either two or three different modalities;
• Comparison of parametric data, diffusion, perfusion curves,
and SUV integration of different morphological criteria: RECIST
1.1 (standard), RECIST 1.0, WHO, and any other configured/
user defined criteria; and
• Monitoring of volume evolution even if not stated in the
RECIST guidelines.
Overall, OncoQuant provides a structured and repeatable
workflow that improves the speed and efficiency of follow-up
reviews and creates a method to initiate a standardized
dialogue between several physicians in our network. n

© 2011 General Electric CompanyDOC 1041480
GE Healthcare
Patient Care
Lower Dose
Image Quality
The rules of CT imaging have changed.Introducing Veo,™ the world’s newest low dose technology from GE Healthcare. See the Veo Case Study highlighting 0.07 mSvChest CT exam with Discovery CT750 HDwith amazing image clarity. Innovation is our passion, that’s great care by design.
Available on Discovery CT750 HD
SEE MORE... Visit us!gehealthcare.com/LowerDoseByDesign& at RSNA: South Building, Booth #3335

54 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n v E o
Understanding the Impact of Iterative ReconstructionA new paradigm in the assessment of radiation dose and image clarity
GE Healthcare CT is undergoing a multi-year commitment
to investigate a multi-center study to further demonstrate
the clinical translation of Veo, which is a full model-based
iterative reconstruction (MBIR) capability. The technical
innovation and design of this technique demonstrate the
potential for radiation dose reduction and improvements in
image clarity. CT Clarity recently spoke with two experts leading
the efforts to quantify the impact on diagnostic value: Ehsan
Samei, PhD, Professor of Radiology and Medical Physicist at
Duke University, and Rendon Nelson, MD, Reed and Martha
Rice Professor of Radiology at Duke University. Dr Samei and
Dr. Nelson share, in their words, what they have learned
from the phantom and clinical work to date.
Q: Why, in your opinion, are these studies important to undertake?
Dr. Samei: I believe that radiology is a science. As scientists
we make predictions, have expectations, and conduct studies.
Yet, ultimately, whatever we predict and expect to see must
be confirmed. We often find, from a theoretical or scientific
standpoint, that one solution could have certain advantages,
but when we conduct the clinical trial we realize that certain
nuances in that prediction may have been overlooked. Based
on this belief, while there is strong scientific evidence that the
new iterative reconstructions (IR) are advantageous, we want
to further investigate the potential of MBIR through a clinical trial.
In the spirit of scientific work, we need continued information
for ourselves and for our community—that what we predict
and claim is more broadly proven out.
Dr. Nelson: I agree with Ehsan that it’s important to validate the
results from the phantom trial that we conducted. In actuality,
what we originally projected to achieve in dose reductions (in the
patient trial) is likely more aggressive than what we found was
possible based upon the phantom data. Certain numbers, such
as contrast-to-noise-ratios (CNR), don’t tell the whole story.
There are other parameters indicating that while CNR is higher,
the noise is above and beyond a certain threshold where we are
comfortable diagnosing from those images. So now, we also
have to investigate if our predicted level of dose reduction is
adequate from a diagnostic standpoint.
More importantly, from my standpoint, this is an opportunity to
do something truly unique. The CT manufacturers are all talking
about dramatic dose reductions using IR, but the only way that
we can comprehensively demonstrate what a particular
technique can do in the varied and changing clinical setting is
through a comprehensive clinical trial that extends globally
across different practice settings.
Ehsan Samei, PhD

55www.gehealthcare.com/ct • November 2011
v e o t e c h N i c a l i N N o v a t i o N
Q: What interested you most in agreeing to participate in this clinical research?
Dr. Nelson: I’ve been reading CT scans for 25 years. We were
very excited when the first multi-slice scanners were introduced.
We had the opportunity to do fast imaging, thin slices, and
multi-planar reconstructions (MPRs) routinely. But then we
realized higher radiation doses were in some cases the price we
paid for these additional capabilities. Higher radiation dose has
become a public issue and I’m very interested in the impact of
it. It seems that while some headway has been made by the
manufacturers, the burden to reduce radiation dose remains
squarely on the shoulders of the radiologists. While we, as
radiologists, are getting better at interpreting higher noise
and lower quality datasets for diagnostic purposes, at times
we find ourselves on the edge of image quality. This study
represents an opportunity to address this challenge in a way
that doesn’t firmly rest on the radiologists’ ability to read
images with high noise.
Dr. Samei: What excites me about IR is that it highlights the
need for a better appreciation and quantification of image
quality in CT imaging. We have been very concerned about
radiation dose and there is a great deal of responsibility to
reduce radiation dose. But, while trying to reduce patient dose,
we need to realize that patients do not come to a medical center
to get dosed; rather they come to get imaged. So therefore, it is
Rendon Nelson, MD
extremely important that we do not compromise diagnostic
image quality in the process of acquiring patient images. IR, and
MBIR in particular, may help achieve a confident diagnosis with
lower dose.** That is the most exciting part here—finding a
better balance between image quality and radiation dose.
Q: Considering the various clinical tasks of high and low contrast and resolution, what has surprised you the most in your findings with MBIR?
Dr. Samei: CNR has been the basis of image quality quantification
for decades, starting with a 1948 landmark publication. An
underlying assumption is that the resolution of an imaging
system does not change as a function of dose or contrast. The
noise changes with lower radiation dose—the image becomes
grainier—but the resolution, or the sharpness of the features,
does not change.
What surprised me the most looking at MBIR is that resolution
does change as a function of contrast and dose. So, with MBIR it
was not what a CT medical physicist would naturally expect. As
a result, resolution can be potentially higher but on the flip side,
the methodology that we have relied upon these last 50 years
goes out the window. If the goal of optimizing imaging is to come
up with a balance between image quality and radiation dose,
then we don’t have an ideal metric to measure image quality
and achieve that balance. We cannot optimize something that
we cannot ideally measure. This “discovery” has initiated a new
line of research in imaging physics, namely to develop better
metrics of measuring image quality that can replace CNR.
Dr. Nelson: As Ehsan has alluded, the phantom study uncovered
higher CNR with the MBIR technique using up to 90% less dose.
Yet, when we looked comprehensively at the images, the noise
level at 90% less dose was not well received by the radiologists
who qualitatively examine the images. So, CNR is not the
whole picture.
Based on the phantom data, which we know does not always
directly translate to clinical acceptance, we can predict to
achieve a 70% dose reduction—and that is not from FBP but
rather from the ASiR technique. At our institution, ASiR protocols
reflect dose that is approximately 40% to 50%** of our current
standard of care FBP protocols, and MBIR will be investigated
at 70% lower than that. This is a very aggressive approach,
considering that in the abdomen and pelvis our ASiR dose is
typically 3 to 7 mSv. This very low dose provides interesting
ramifications from a clinical standpoint.
**In clinical practice, the use of MBIR and ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location, and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.

56 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n v E o
I would also add that clinically these images look different,
although they have very good spatial resolution and low contrast
detectability even at low doses. Different doesn’t mean bad; it
just means different and is something that imagers would have
to get used to, particularly those that have been doing
interpretations from FBP for many years.
Q: What have you found to be the most important lessons in assessing image quality and clinical value in the transition from FBP to MBIR?
Dr. Nelson: Through a consortium, whereby we selected a
small number of opinion leaders, initially there was a lot of
concern about the difference in image appearance. Not so
much the difference in noise but the different look and feel that
I alluded to earlier. But a very interesting thing happened. We
realized, as imagers, that even though the MBIR images looked
different, we weren’t missing anything and in some cases, we
saw more information. In our experience, a method for helping
radiologists get used to the different appearance of these
images is to start out by doing a side-by-side comparison of
standard-of-care dose FBP and MBIR datasets followed by a
gradual diminution in dose. Using this format, we have noted
a shift in the radiologist focus from concern over the different
‘look and feel’ to a discussion of ‘how low can I go’.
Dr. Samei: One of the amazing skills that a radiologist has
when interpreting an image is that he/she is able to distinguish
between artifacts and true anatomy. They know that noise is
a characteristic of acquiring images with a limited amount of
dose. Provided they know that the images are noisy, they can
feel confident reading through that noise.
With IR, we have changed the nature of noise. Essentially, our
task is to identify what is real and what is artifact, in the broad
sense of the word—something that is not reflective of patient
anatomy or function. With IR, there is still noise in the images;
even though the magnitude is lower, the texture of it is different.
As long as the radiologist knows that texture and understands
how it manifests itself, he/she will still be able to do a great job
reading through the image. So there are two elements: there is a
training element of understanding the noise texture, and another
element is quantifying the actual limitation that the noise texture
would put on the maximum amount of information that
radiologists can extract from the image.
Q: What can your peers expect to learn from both the phantom and the clinical study?
Dr. Samei: The phantom study provides us with new tools
and methods to characterize image quality for MBIR, taking
into account some of the resolution and noise features of the
reconstruction that I mentioned. It also provides us with a
scientific basis to determine what level of dose reduction is
possible with MBIR without compromising diagnostic quality.
The clinical study will help to substantiate the predictions of
the phantom study clinically, while at the same time providing
a wealth of information to refine the image quality
metrology further.
Dr. Nelson: The phantom study results were used to build the
multi-center trial, but from those results I hope that: a) they will
first be confident that the technique settings we’ve chosen are
adequate and that they can assimilate them into their own

57www.gehealthcare.com/ct • November 2011
v e o t e c h N i c a l i N N o v a t i o N
The Pilot Study of Model-based Iterative Reconstruction using 64-Slice Multidetector-Row CT Datasets Obtained from the
Central Nervous System, Thorax, and Abdomen is designed to provide further evidence of the diagnostic clinical value of Veo
image reconstruction. Prior phantom studies have demonstrated a significant dose reduction potential while maintaining
or improving quantitative image quality metrics as matched to observer results. This study translates those details into the
clinical population via acquisition of data at two different dose levels on the same study subject, then each are reconstructed
utilizing three techniques, FBP, ASiR, and Veo.
Image volumes from subjects scanned for pathology in the posterior fossa, lung cancer staging, focal liver lesions, or
kidney stones will be reviewed by two independent readers blinded to subject, radiation dose level, and image reconstruction
type. Readers rate the ability to detect and characterize pathology of interest as well as provide an overall indication of
diagnostic value including artifact level and impact to recommended treatment path. Incorporation of results from these
four anatomical regions at both radiation dose levels will enable evidence of clinical behavior in tissues presenting both
high and low contrast and resolution challenges for broad assessment of diagnostic image clarity.
Three leading academic institutions in the US are enrolling 120 subjects for this pilot study, which is underway.
Pilot results will be used to fine tune future studies across the globe.
practice; and b) that the image quality is such that they are
confident they can make diagnostic reads from images at this
low dose of radiation. Ultimately, our culture tends to get fired up
on something based on an issue and that’s true with radiation
dose. And that burden is upon us (and includes publishing the
results from this multi-center clinical trial) to prove to the public
that the doses used in CT imaging do not pose a medical
concern to them.
Q: Considering model-based iterative reconstruction, what do you see as the implications for CT imaging in clinical practice?
Dr. Samei: There are two things. We have talked a great deal
about reducing radiation dose, and that is a huge implication
of IR clinically. But what excites me even more is that we have
the opportunity to be on the cutting edge of doing more with
medical imaging—extracting more meaningful information
about the patient. It is possible that we might not reduce dose
as dramatically, or even at all for certain applications, in order
to take advantage of the additional information we get from
IR. There are new applications that we may be able to explore.
So we could now have a new tool in our arsenal to obtain
better information from the patient that would be more
clinically meaningful.
Dr. Nelson: There are two challenges. First, we need to figure
out what radiation dose levels and reductions are appropriate
and reasonable using this technique, particularly in comparison
to the competitive IR techniques on the market right now.
Second, we have to become comfortable with the new look
and feel of these images. But remember like PACS, in a short
period of time, we will have a new group of radiologists coming
through the training programs who may never see an image
from FBP. Just like with all our 48 residents, they have never read
plain film, they are all trained using PACS. So it’s just a matter
of time to make that cultural change, but it will be a new
experience at the onset for those who have been reading images
from FBP for many years.
In terms of implications for CT imaging, I think MBIR will have
a higher impact on CT imaging of the chest, abdomen, and
pelvis. And, these anatomic regions are where we give the
highest dose levels since we often do multiple passes following
the administration of contrast material. We have no problem
doing that in MR but in CT the doses accumulate. So I think
we’ll see a big impact in CT body imaging.

58 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n v E o
Q: Any additional thoughts?
Dr. Samei: One of the beautiful things about CT imaging is
that the field was somewhat homogeneous before IR. Moving
forward, we’ll have a whole lot more heterogeneity in the CT
operation clinically—not in terms of one manufacturer but across
manufacturers. There is a new challenge for imagers—a call to
action—for standardization. In order to confirm the claims by
manufacturers, we need comparable images (from different
manufacturers), so I think we need to be mindful of that as IR
is rolled out.
I do, however, believe this clinical trial is a great step in that
direction, though limited to a single vendor trial. We should be
seeking to create a framework that different sites can implement,
so that we can all achieve a certain level of consistency in image
quality evaluation, in how we discuss image quality improvement,
and in dose reduction.
Dr. Nelson: We are embarking on a comprehensive
evaluation of a new technique and I’m hopeful that this will
set the precedence for future clinical trials that aim to provide
more comprehensive investigations of new techniques.
What I like about this MBIR trial is the technology is relatively
new and we’ll get the results in a relatively short period of time.
We’ll publish the results, hopefully in the next year, and the
impact should be much higher. So it will be interesting to see
what happens—it is a big commitment both financially and in
terms of allocating resources. It was a significant scientific
investment. We also encourage the radiology community
to continue evidence-based studies across the specialty. n
Ehsan Samei, PhD, DABR, FAAPM, FSPIE is a Professor of Radiology, the Director of Carl E. Ravin Advanced Imaging Laboratories, and the Founding Director of the Clinical Imaging Physics Group at Duke University. His research interests include advanced X-ray imaging techniques, translational medical imaging, and image quality and dose metrology aimed towards optimized interpretive, quantitative, and molecular performance. He has been the recipient of 20 extramural grants and has over 500 publications, including 130 referred papers.
Rendon C. Nelson, MD, FACR, FSCBT-MR, is the Reed and Martha Rice Professor of Radiology at Duke University. He is also a Fellow in the American College of Radiology and both a Fellow and Past President of the Society of Computed Body Tomography and Magnetic Resonance. He is a member of the Division of Abdominal Imaging at Duke with clinical interests in hepatobiliary and pancreatic imaging, virtual imaging, percutaneous image-guided intervention, and percutaneous thermal tumor ablation. His research interests include: (1) optimization of diagnostic imaging of the liver, specifically the detection and characterization of focal and diffuse processes by US, CT, and MRI; (2) optimization of radiation dose and image quality in multidetector CT of the body; and (3) percutaneous image-guided thermal ablation of hepatic and renal tumors.
As a leading academic medical center, Duke University is uniquely positioned to transform medicine and health locally and globally through innovative scientific research, rapid translation of breakthrough discoveries and educating future clinical and scientific leaders. Duke is a strong advocate of practicing evidence-based medicine and is a leader in efforts to eliminate health inequalities.
Each year, the 15,000 professionals of Duke University Health System serve patients through more than 60,000 hospital admissions and 1.8 million outpatient visits. For 21 consecutive years, Duke University Hospital has been named among the top 10 in the nation by U.S. News & World Report.
www.ctclarity.com/ctclarity/veosupplement2011#pg1 to read the full interview. »

GE Healthcare
imagination at work
Greater Clarity. At digital speed.
Online. And on tap.
Now you can have complete issues of GE Healthcare’s CT Clarity, the Magazine of CT, right at your fingertips when you’re on the go. The CT Clarity App links you to a vital source for the latest news about GE Healthcare CT on your iPad, iPhone, or Android tablet or phone. Download the free tablet and smartphone applications at the Apple Store (www.apple.com) or Android Market Apps (www.market.android.com). Or, simply scan the QR code below with your smartphone.
Follow us on Twitter: @GEHealthcare
ctclarity.com Android Apple
© 2011 GE Healthcare, a division of General Electric Company.
iPhone and iPad are registered trademarks of Apple, Inc.
Android is a trademark of Google, Inc.

60 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n d E x u s
Radiology embraced the digital revolution more than 20 years
ago. In most hospitals today, radiologists perform their diagnoses
in virtually an all-digital environment. Alternate care sites—
clinics and physician offices—are quickly following in the same
direction, if they are not already there. However, as imaging and
information technology advanced at varying levels over the past
two decades, radiology departments have become a multi-
system environment. As a result, radiologists utilize an array
of systems—many from different manufacturers—to read and
report the patient diagnosis. These systems include, but are not
limited to, PACS, RIS, HIS, Speech Recognition, and advanced
image processing.
As technology changes, so too does our expectation of the
technology. We expect it to positively impact patient care by
enabling us to see the body more clearly with advanced imaging
or post-processing techniques, and enhance our workflow
for physician accuracy and efficiency (particularly important
in emergency cases).
Yet, this multi-system electronic environment may present
a barrier to workflow and efficiency. Advanced processing
workstations were historically separate workstations. Native to
these systems are 3D and other advanced image post-processing
software. Radiologists had to pause in their analysis, physically
move to the image processing workstation, perform the image
analysis, and then push the data back to the PACS. In this
scenario, efficiency and seamless connectivity of patient
information was lost.
Recent integration of advanced processing capabilities
to the PACS diminished the need to utilize a stand-alone
workstation. This was often accomplished by providing
Integration and Information the Cornerstone of RadiologyBy William P. Shuman, MD, FACR, Director of Radiology, University of Washington Medical Center

61www.gehealthcare.com/ct • November 2011
d e x u s t e c h N i c a l i N N o v a t i o N
access to an advanced application server via the desktop.
While this configuration worked, it still presented significant
workflow challenges.
With multiple systems already open on the workstation—HIS,
RIS, PACS—the radiologist was required to navigate and locate/
manage the desktop mindshare. Perhaps more important is
speed and functionality. At the University of Washington, we
use most of our advanced processing capabilities (as do other
sites) with CT colonography, cardiac, spectral dual energy, and
vascular imaging. Having a dedicated advanced image processing
workstation (i.e., AW Workstation) just 20 feet away from the PACS
workstation made it tempting to go over and work on it. However,
this defeated the purpose of a single desktop. As radiologists are
well aware, interruptions to the diagnostic process, including
moving to a dedicated processing workstation, diminish
efficiency and productivity.
While increases in network and processing speed helped
address these issues, a fully integrated program that allowed
us to seamlessly access PACS, RIS, advanced image processing,
and other applications at the same time, on the same workstation,
was highly desired. At our facility, we recently implemented
a new solution that integrates GE’s new AW Server to our
RIS-driven workflow with impressive workflow efficiency results.
Dexus workflow
An integral part of Dexus is the AW Server integration to PACS
and RIS for a single imaging workflow. It also leverages a central
PACS database to enable access to a broad array of advanced
3D visualization and processing tools typically found on the AW.
This environment provides a substantial improvement in the
speed of image post-processing on the PACS. System usability
is also enhanced due to transparent image sharing between
AW and PACS.
By using a thin-client architecture, AW Server enhances the
value of remote access to patient information. This is especially
important for our multi-site healthcare system, where we now
have the ability to scan a patient at any location and provide
the same level of interpretation and analysis regardless of
where the radiologists are situated.

62 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n d E x u s
William P. Shuman, MD, is Director of Radiology at UWMC and Vice Chairman and Professor for the Department of Radiology. Dr. Shuman received his medical degree from State University of New York Syracuse and completed a residency in radiology at the University of Vermont. Dr. Shuman is one of the leaders in creating cardiac CT at UW. Outside of UW, Dr. Shuman has served as Associate Editor for two leading academic peer reviewed journals in radiology, is currently on the Appropriateness Committee of the American College of Radiology, and is the President of the Society of Body CT/MR.
UW Medicine owns or operates Harborview Medical Center, University of Washington Medical Center, Valley Medical Center, Northwest Hospital & Medical Center, a network of seven UW Medicine Neighborhood Clinics that provide primary care, the UW School of Medicine, the physician practice UW Physicians, and Airlift Northwest. In addition, UW Medicine shares in the ownership and governance of Children’s University Medical Group and Seattle Cancer Care Alliance, a partnership among UW Medicine, Fred Hutchinson Cancer Research Center, and Seattle Children’s. The core hospitals, Harborview, UW Medical Center, and Northwest Hospital & Medical Center, together have about 69,000 admissions and about 1.4 million outpatient and emergency room visits to the hospitals and clinics each year. UW Medicine faculty includes four Nobel Prize winners, 33 Institute of Medicine members, 32 National Academy of Sciences members, and 16 Howard Hughes Medical Institute investigators. (Photo courtesy of UW Medicine.)
Speed has historically been an issue with advanced post-
processing in the PACS. It is important that speed be independent
of location—it is the same whether the images are being sent
from a facility in another city or state, or three doors down the
hall. By addressing the speed issue, we anticipate the AW Server
will further impact our ability to perform more advanced analysis
from virtually any location, including at-home night reads when
on-call. As radiology subspecialties continue to grow in demand,
speed will become even more important in the near future.
Clinical collaboration among and between specialties will also
be further enhanced. Utilization of advanced applications in
our diagnostic workflow will increase in our daily routine and
in training residents and fellows. When access was cumbersome
and required an interruption in workflow, there was a natural
reluctance on the part of the radiologist to use 3D image
analysis. Frankly, their productivity would decrease as they
fell further behind on their workload. Now with Dexus, we can
perform 3D analysis directly on the PACS on more patient cases
due to the increase in speed of access and performance, which
impacts the quality of patient care. In our facility, we estimate
that in approximately 10% to 15% of high-tech imaging, 3D
analysis will improve or change the diagnosis.
Finally, training is a critical component and should not be
overlooked. In my opinion, the best scenario is an intuitive
system and software that doesn’t require significant training.
The test of any training program is the extent to which staff
can fully utilize the software while maintaining efficiency—
two weeks after the training session is complete.
Our radiologists expect the new environment will offer the
referring physician, patient, and hospital (our employer) a better
balance between accuracy, quality, and productivity. The way
information from different systems and software is integrated
does matter. We’ve learned that one software environment
with a single database is critical for access to advanced
imaging functionality and the entire diagnostic and image
evaluation process.
Remember, as radiologists, we are integrators of information,
and the more our tools complete these tasks for us, the more
efficient we can be in our diagnoses and consultations. n
“ Remember, as radiologists, we are integrators of information, and the more our tools complete these tasks for us, the more efficient we can be in our diagnoses and consultations. ”
Dr. William P. Shuman
www.gehealthcare.com/aw »

GE HealthcareComputed Tomography
© 2011 General Electric Company *Trademark of General Electric Company.
No company has done more to bring low dose to patients than GE Healthcare. That’s no coincidence — in fact, it speaks to the single purpose that guides our business: helping you deliver high-performance care.
Our approach is built upon a foundation of low-dose technology. But it also encompasses the best practices and industry exposure we’ve amassed for decades. The result is a true end-to-end partnership designed to help you provide lower dose patient care, more efficiently, and more effectively.
You’re here to deliver high-performance care. We’re here to help you do it.
www.gehealthcare.com/LowDoseCT
GreaT Care by DesiGn.
PartnershipDecades of CT experience have made us a strong, dedicated partner who understands healthcare’s complexities
asir*
Lower image noise while improving low contrast
detectability and image quality.
Gemstone* spectral imagingExpand information for clinical
diagnosis and workflow.

64 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n P H o T o n C o u n T i n G
Photon Counting: A New CT Technology Just Over the Horizon
By Tibor Duliskovich, MD, Medical Director CT, GE Healthcare
“CT is mature technology” is frequently heard, implying that
CT has reached its full potential—that nothing revolutionary
is coming down the road. This is simply not true.
In a previous edition of CT Clarity magazine you may remember
reading an article on dual energy CT and its clinical value
and indications. Dual energy imaging, or in GE terminology
“Gemstone Spectral Imaging” (GSI), uses two X-ray energies to
allow improved differentiation of tissues and materials. It also
enables virtual mono-energetic imaging. This post-imaging,
processing technique mimics the use of a very narrow energy
spectrum absorption and enhances material decomposition,
making identifying and removing specific materials from image
data possible. The GSI technique can also generate virtual
un-enhanced images from a single contrast data acquisition.
Clinical applications for GSI are still evolving and there is no
doubt that radiologists will find new ways of utilizing the
additional information that it provides.
X-rays (and all frequencies of light) may be thought of as waves
and particles. In fact, Albert Einstein won his Nobel Prize in
physics for the work he contributed to understanding this wave/
particle duality, and not for his more famous work on the theory
of relativity. Photon counting,** as the name implies, counts
individual X-ray photons (the particles that make up the X-ray
frequency light) hitting the surface of a single photosite of the
detector—essentially, detecting individual events on a nano-
second scale! Unlike all existing technologies that digitize an
integrated signal of an analog response of the detector to
hundreds of events, photon counting counts discrete events
(absorption of a single photon) and as such is “digital in nature”
at the detection phase. Therefore, the electronic noise present
in the detector is not sampled as it remains well below the signal
level created by the thousands of electron-hole pairs generated
by the impact of a single X-ray photon (Figure 1). This gives
very clear input to the reconstruction algorithms. In fact, the
detector resolution can be increased dramatically without a
corresponding increase in statistical noise to achieve higher
spatial and contrast resolution.
But that is not all. The flexibility of photon counting allows other
benefits as well, specifically leveraging the fact that the energy
of the photons may be recorded in as many discrete ranges
(bins) as necessary. Consider that in existing integrated detector
technologies we have two energy spectra along with significant
energy overlap between the two spectral bins (Figure 2).
**Technology in development that represents ongoing research and development efforts. These technologies are not products and may never become products. Not for sale. Not cleared or approved by FDA for commercial availability.

65www.gehealthcare.com/ct • November 2011
P h o t o N C o u N t i N g t e C h N i C a l i N N o v a t i o N
Figure 2. Different approaches to dual-energy acquisition: sequential acquisition and dual-tube detector techniques are prone to temporal mismatch. GSI effectively deals with temporal mismatch. Photon counting makes registration of all energy levels simultaneous and further improves energy separation.
Figure 1. Experimental validation of photon counting vs. conventional CT acquisition. The impact of “zero electronic noise” is apparent in ultra-low dose CT acquisitions. At high doses the “pile-up” effect makes counting individual photons difficult and lowers efficiency of photon counting detector. Technique: 80 kV, 5 mAs, 32*0.625 mm, 0.5 sec axial, 10 mA, window width-1600 HU, window level-160 HU.
The maximum energy for these is determined on the tube side
by switching the kV. However, in photon counting the energy is
discriminated on the detector side, so a single energy tube can
do the job. By separating photons into a larger number of narrower
energy bins, we can improve the mathematical reconstructions
to approach better estimates of true mono-energetic images
and not just simulate that effect mathematically as in the case
of dual energies. The increase in the number of energy bins
along with less energy contamination between the bins may
improve the precision of material decomposition (Figure 3). This
translates into higher-quality, virtual, un-enhanced images and
the ability to remove materials selectively without “bleeding” into

66 A GE Healthcare CT publication • www.ctclarity.com
T E C H n i C A l i n n o v A T i o n P H O T O N C O U N T I N G
neighboring pixels or “contaminating” the data in the beam’s
path. With this technique, voxels containing iodine (contrast agent)
should be easily distinguished from non-contrast containing
voxels, so true vessel lumen may possibly be identified and
reconstructed in 2D and 3D with “suppressed” surrounding tissue.
This data may possibly also be used for high-energy virtual
reconstructions to calibrate PET standard uptake values more
precisely in hybrid PET/CT scanners and to tailor therapeutic
radiation treatment with the goal of better target delineation,
hence sparing healthy tissue.
Another potential benefit of detector-based photon counting
comes from the fact that X-ray tubes continue to operate in
standard conventional single-energy modes. All advanced X-ray
tube technologies including mA modulation, kVp modulation, and
focal spot modulation are planned to be used in photon counting
scanners. Therefore, the tube voltage could be continuously
modulated the same way we currently modulate the tube current
to account for differences in absorption of the body from different
angles. This may allow us to spare superficial tissues such as the
breasts by turning down the mAs while simultaneously increasing
the voltage. Based on the scout image data, it may also allow
a dynamic optimization of imaging protocols and avoidance of
so-called “photon starvation” in order to reduce overall dose
while maintaining diagnostic image quality. Furthermore,
a low kVp beam may be utilized on slim patients.
The beauty of this technology is that the detector always operates
in photon counting mode and the radiologist can decide after
the fact whether to reconstruct a standard CT image or a photon
counting image out of the raw dataset without a need to rescan.
So, for straightforward cases the exam could be fast and generate
fewer images for speed and throughput, yet for difficult cases
the radiologist would have a full arsenal of options to aid in
determining the diagnosis.
When not generating the photon-counting spectral images, the
specifics of absorption of different energy photons at different
depths enable precise weighting of each discrete energy level so
that their contribution to a standard CT image can be fine tuned.
As a result, we expect there will be better quality, standard CT
images with less noise.
The more energy bins we use in photon counting the closer we
can get to true K-edge imaging of multiple elements simultaneously.
Based on a specific “fingerprint” of a K-edge, i.e. the unique shape
of its mass attenuation coefficient, the element can be identified
with certainty (Figure 4). Tagging tumor cells with gold, tantalum,
or other materials and subsequently utilizing photon counting
technology holds hope for allowing reliable detection of very
small, distant metastasis rivaling the sensitivity of PET with the
spatial resolution of the most advanced CT scanners we
have today.
The counting of events happens on a nano-second scale,
enabling extreme precision in recording the energy and time of
the photon-material interaction. This information may be utilized
to eliminate artifacts caused by the non-simultaneous acquisition
of dual energy data, further improving image quality.
Figure 3. Photon Counting Prototype Clinical Study: Full FOV abdominal imaging. Improvements in material decomposition allow for Z-map images that are color coded according to tissue atomic number. Efficient energy separation allows for true mono-energetic images.

67www.gehealthcare.com/ct • November 2011
t e c h N i c a l i N N o v a t i o NP H O T O N C O U N T I N G
All indications of GSI imaging are expected to be applicable to
photon counting technology, as well. Additionally, scientists will
likely develop numerous new applications, expanding the clinical
utility of CT scanning and potentially allowing physicians to detect
disease earlier and with more confidence. The ultimate goal is to
improve patient outcomes.
This article provides only a glimpse of things that may be coming
in the not so distant future, possibly a few generations down the
road. There are even more CT innovations and discoveries yet to
come. Much hard work is needed to mature these new technologies
and generate clinical evidence to support them, otherwise
reimbursement and adoption will be a challenging hurdle.
CT has amazing potential above and beyond the benefits
it already provides! n
Figure 4. The identification of certain materials based on the unique shapes of their Mass Attenuation Coefficients (MAC). The sudden increase in X-ray attenuation at an energy level corresponding to the binding energy of K-shell electrons allows for 100% specific identification.
References
1. J. Eric Tkaczyk, Rogerio Rodrigues, Jeffery Shaw, Jonathan Short, Yanfeng Du, Xiaoye Wu, Deborah Walter, William Leue, Daniel Harrison and Peter Edic, “Atomic number resolution for three spectral CT imaging systems”, Proc. SPIE 6510, 651009 (2007);
2. J. Eric Tkaczyk, David Langan, Xiaoye Wu, Daniel Xu, Thomas Benson, Jed D. Pack, Andrea Schmitz, Amy Hara, William Palicek, Paul Licato and Jaynne Leverentz, “Quantization of liver tissue in dual kVp computed tomography using linear discriminant analysis”, Proc. SPIE 7258, 72580G (2009);
3. J. Eric Tkaczyk, Kristian Andreini, Tan Zhang, Kevin G. Harding, Gil Abramovich, Yana Williams, Christopher A. Nafis and Wenwu Zhang, “CZT smart dicing strategy for cost reduction using defect imaging and random-access machining”, Proc. SPIE 7806, 78060L (2010);
4. J. Eric Tkaczyk, Vladimir Lobastov, Daniel D. Harrison and Adam S. Wang, “Contrast-to-noise of a non-ideal multi-bin photon counting x-ray detector”, Proc. SPIE 7961, 79613O (2011);
5. Adam S. Wang, Daniel Harrison, Vladimir Lobastov, and J. Eric Tkaczyk, “Pulse pileup statistics for energy discriminating photon counting x-ray detectors”, Med. Phys. 38, 4265 (2011);
6. Adam S. Wang, Norbert J. Pelc, “Synthetic CT: Simulating low dose single and dual energy protocols from a dual energy scan”, Med. Phys. 38, 5551 (2011);
7. Wang, A.S.; Pelc, N.J.; “Sufficient Statistics as a Generalization of Binning in Spectral X-ray Imaging“, Medical Imaging, IEEE Transactions on, 30 Issue:1, (2011)
8. Ehsan Samei, Norbert J. Pelc, “Impact of photon counting detector spectral response on dual energy techniques”, Proc. SPIE 7622, 76223L (2010);
9. Taguchi K, Zhang M, Frey EC, Wang X, Iwanczyk JS, Nygard E, Hartsough NE, Tsui BM, Barber WC.’ “Modeling the performance of a photon counting x-ray detector for CT: energy response and pulse
pileup effects”, Med Phys. 38(2):1089-102, (2011)
10. Srivastava, S.; Taguchi, K.; “Improved contrast-to-noise ratio of photon counting clinical x-ray CT images using a model-selection based approach”, Nuclear Science Symposium Conference Record (NSS/MIC), 2010 IEEE
11. X. Wang, K. Taguchi, E. C. Frey, D. Meier, D. J. Wagenaar and B. E. Patt, “Material separation in x-ray CT with energy resolved photon-counting detectors”, Proc. SPIE 7961, 79611V (2011);
Tibor Duliskovich, MD is Medical Director, Computed Tomography, at GE Healthcare. Dr. Duliskovich earned his medical degree from Semmelweis Medical University (Budapest) and was a staff radiologist at Haynal Imre Medical University (Budapest). He led Organizational and Methodological Department at the National Institute of Radiology and Radiation Physics in Hungary, where his department oversaw the design, manufacturing, installation and servicing of medical imaging devices to ensure safety and effectiveness. Prior to assuming his current position at GE, he has held various management positions at medical device and healthcare informatics companies, including DigiX, Inc., Wuestec, Inc., StorCOMM, Inc. Aspyra, Inc.; and Philips Healthcare. Dr. Duliskovich joined GE in January 2011, and in his medical affairs role supports regulatory submissions, marketing, scientific publications, patient safety, and the medical risk assessment process across the CT products; and helps align clinical research activities with business needs from a medical perspective.

68 A GE Healthcare CT publication • www.ctclarity.com
b E y o n d T H E s C A n d o s E M A n A G E M E n T
Comprehensive Dose Management Services and Solutions
GE Healthcare has long recognized the benefits and risks of
radiation in diagnostic imaging and continually strives to develop
technologies and solutions to assist medical imaging providers in
managing these risks. Earlier this year, the US Joint Commission
issued a sentinel event alert on the radiation risks of diagnostic
imaging,1 signaling that accrediting agencies (such as Joint
Commission) may begin inspecting dose management, tracking,
and reporting.
Although dose management is an industry-wide patient care
concern that requires a collaborative effort between physicians,
facilities, and manufacturers, GE Healthcare offers several
programs to help medical imaging providers improve patient
care by better managing, tracking, and reporting dose. GE’s
dose services and solutions assist a medical imaging provider to
monitor and report dose, provide additional or refresher training
for the facility’s staff, optimize protocols to enable low-dose
studies, and perform quality control and quality assurance
testing for regulatory and accreditation organizations.

69www.gehealthcare.com/ct • November 2011
b e y o N d t h e s c a Nd o s e M a N a G e M e N t
Dose services and solutions
For many healthcare facilities, particularly small- to medium-sized
sites, capturing, reporting, and monitoring dose is a challenging
task. Optimizing protocols to further lower dose may fall outside
the realm of expertise for the facility’s staff.
GE Healthcare offers a three-tiered approach to address clinical
informatics, education and optimization, and medical physics.
1. Clinical informatics includes: DoseWatch, an information
technology application that facilitates the tracking, reporting,
and monitoring of dose from multiple manufacturers and
multiple types of imaging devices; Innova Dose Reports for
interventional fluoroscopy provides detailed analytics and
alerts for the end user; and, integration with RIS and PACS to
enhance patient care and facilitate the clinicians’ access to a
patient’s dose exposure history by anatomy and utilize statistical
data/benchmarking to identify opportunities for improvement.
2. Education and optimization services encompass training and
protocol optimization support.
3. Medical physics solutions provide contract services for
accreditation and periodic acceptance and local regulatory
testing, technical support, and consulting.
DoseWatch
GE Healthcare now offers a comprehensive dose tracking and
management system with DoseWatch. Through a facility’s
existing network and IT infrastructure, DoseWatch captures
dose information from imaging devices and organizes the data
by modality and type of imaging protocol. The DoseWatch
database stores all data, records dose by patient, and retains
key acquisition parameters.
In fact, after one year of using DoseWatch, CHU Strasbourg
(France) reports a facility dose reduction due in part to using
Dose Watch in their QA program. “We are all very pleased with
the progress we have made using DoseWatch,” says Professor
C. Roy, MD, Director of Radiology. “We conduct close to 100 CT
exams each day, and thanks to DoseWatch we can get the dose
information we need in a very useable format to help us better
manage our imaging program.”
With the dose monitoring solution, Professor Roy can evaluate
dose management and optimization over a six-month period.
She notes that DoseWatch interfaces directly to the CT system
so it is transparent to the radiology workflow and does not slow
down the examination time.
Professor Roy is also impressed with the ability to access the
patient’s dose history in a few mouse clicks. This is an important
feature as many hospitals are concerned about the dose exposure
for acute-care patients—many who require follow-up CT exams—
and young adult or pediatric patients.
Using DoseWatch, clinicians at CHU Strasbourg can help determine
the appropriate dose level per procedure that can be shared
throughout the imaging and interventional community. That’s
because DoseWatch captures dose information during the
procedure, and that data can then be used to help define dose
targets by type of exam—such as neuro, abdomen, and thorax.
As a result, the number of procedures that may have exceeded a
predetermined dose level in the past have now been reduced at
CHU Strasbourg. The bottom line, it is the patient who wins in terms
of obtaining their diagnostic procedure at a dose that is ALARA.
Adds Professor Roy, “Thanks to this software, we are now
clearly below the target limits set out in the rules while
maintaining the diagnostic quality exams we need. I believe
that with DoseWatch, we have indisputably raised the overall
quality of our medical imaging.” n
For more information on Dose Watch, visit www.gehealthcare.com/ResponsibleImaging. »
Joint Commission Sentinel Event Alert
On August 24, 2011, the Joint Commission issued a Sentinel
Event Alert on the dangers of medical radiation. The
announcement also states that the Centers for Medicare &
Medicaid Services (CMS) will require accreditation of facilities
providing CT, MR, PET, and nuclear medicine in non-hospital
sites beginning January 1, 2012. Additional accredited
requirements may exist on a state-by-state basis.
To view the alert, which contains suggestions by
the Joint Commission for accredited facilities, visit
http://www.jointcommission.org/assets/1/18/SEA_471.PDF
Reference:
1. Available at: http://www.jointcommission.org/assets/1/18/SEA_471.PDF

70 A GE Healthcare CT publication • www.ctclarity.com
b E y o n d T H E s C A n C T A n d r A d i A T i o n d o s E
Today’s diagnostic imaging portfolio offers the clinician
many options: ultrasound, MR, X-ray, SPECT, PET, fluoroscopy,
and CT. In fact, each imaging modality visualizes different
properties of human anatomy or function, and that is
why these technologies are generally not completely
interchangeable.
Does my Patient Need a CT Scan? By Tibor Duliskovich, MD, Medical Director CT, GE Healthcare

71www.gehealthcare.com/ct • November 2011
b e y o N d t h e s c a Nc t a N d r a d i a t i o N d o s e
During my radiology residency, I had a patient with metastatic
liver disease that I diagnosed using ultrasound. The patient
was taken to CT for a pre-operative scan and, given the
technology available at the time, the lesions were not visible
on the non-contrast or contrast CT. My supervisor suspected
I may have made a mistake until she repeated the ultrasound
herself and verified my initial finding.
Examples like this demonstrate what experienced clinicians
already know—that each imaging modality has its strengths
and weaknesses. This is why all the modalities have a
complementary place in the differential diagnostic workup
of a patient. Some may perform better than others in
a particular case—it depends upon the patient’s needs
and the clinical situation at hand. While the above example
highlights a case where CT at that level of development was
not the optimal diagnostic tool for a specific patient, rest
reassured that CT is a vital clinical tool and is here to stay.
In light of recent publicity over radiation from medical
imaging, the public may have forgotten the reason we built
the CT machines in the first place: to help clinicians accurately
diagnose a multitude of life-threatening conditions promptly
with virtually no contraindications. CT is used to determine
emergency treatment pathways, diagnose pathology, monitor
disease treatment, plan radiation therapy, calibrate nuclear
medicine images, and much more. CT scanners help physicians
make informed treatment decisions and save lives every day!
Despite the clear benefits of CT, it is not the answer to all
situations. Once a clinical decision is made to utilize medical
imaging, physicians have an array of diagnostic procedures
at their disposal. Because of this, many institutions follow
evidence-based protocols, called appropriateness criteria,
which take into account the advantages and disadvantages
of each modality for a given clinical imaging task for that
patient. By adhering to these guidelines, providers enhance
the quality of care and contribute to the most efficacious use
of different medical imaging modalities. These professional
guidelines, such as those developed by the American College
of Radiology,1 assist referring physicians and other providers
in making the most appropriate imaging or treatment decision
for a specific clinical condition.
Ultimately, the healthcare professional has the responsibility
to make the best decision for each individual patient and
to select the proper diagnostic algorithm. A healthcare
professional bases his/her decisions on the patient symptoms,
the clinical question being assessed, the patient’s medical
history, the presence of any contraindications to certain
procedures or tests, and many other factors. If CT is deemed
the best choice to achieve the optimal clinical outcome for
the patient, the treating physician will prescribe a specific
type of CT exam. The imaging department will carry out the
prescription consistent with their best practices, available
technology, and in accordance with the current state of
medical practice. The single most important driving force
behind prescribing a CT scan is that the benefit to the patient
outweighs the risks, including the small risk of ionizing radiation,
and no more appropriate alternative procedure is available to
achieve the optimal clinical result.
X-rays are ionizing radiation used in many imaging modalities
to produce images. The image is formed by the portion of X-ray
photons that are not absorbed in the patient’s body, but instead
pass through it to the detector. This should make it clear why,
without radiation, there is no CT image! If there is not enough
radiation the result will be a “noisy” image, which may not be
suitable for diagnosis.

72 A GE Healthcare CT publication • www.ctclarity.com
b E y o n d T H E s C A n C T A n d r A d i A T i o n d o s E
This could lead to a repeat exam, a false positive finding requiring
additional tests and a delay in diagnosis, or, even worse, a false
negative finding. Repeating a CT exam would subject a patient to
additional radiation and, in some instances, intravenous contrast.
For these reasons, radiologists and technologists are trained
to select the proper imaging protocols to answer the clinical
question while keeping the patient’s radiation exposure under
tight control. This is known as the ALARA (As Low As Reasonably
Achievable) principle and it is fundamental to the appropriate use
of CT and other imaging techniques that involve ionizing radiation.
ALARA is based on the assumption that the amount of radiation
utilized should always be the minimal amount required to achieve
the desired result—a clinically useful image.
Although there is no definitive evidence of harm caused by
small amounts of radiation, such as the radiation levels received
annually from so-called “background” sources (e.g., radon),
minimizing radiation exposure is prudent. Therefore, the medical
profession has adopted the no-threshold linear model of
response to radiation, which assumes that the risk of exposure
to ionizing radiation is cumulative over a lifetime and there is no
threshold below which there are no potential effects. On the other
hand, others have adopted a “heuristic” view of ionizing radiation,
with some of the scientific literature supporting the notion that
small amounts of radiation may be beneficial. Regardless of one’s
view, the medical profession agrees that imaging should be
justified, optimized, and in accordance with ALARA to minimize
radiation exposure for patients.
From my perspective as a radiologist, in order to best serve
patients it is preferable to make a confident diagnosis rather
than save a millisievert or two, as the correct diagnosis is
a proven way to save lives. Patients typically feel the same
way and readily support a recommendation for imaging after
consultation with their physician about the risks and benefits
of the exam.
All CT manufacturers are investing in dose reduction
technologies. GE Healthcare is leading the way with the design
of X-ray tubes, collimation, dual energy, automatic beam
modulation, detector technologies, and noise and artifact
reduction algorithms. For more information on GE’s low-dose CT
technology, see www.gehealthcare.com/LowerDoseByDesign.
In addition, GE is incorporating the new MITA dose check feature
on our CT scanners. It provides alerts and notifications to scanner
operators when pre-defined radiation dose levels—as determined
and set by the facility—will be exceeded. There are two levels
of thresholds: Notification Values and Alert Values. Notification
Values apply to a single image series (e.g. a single helical series)
while Alert Values apply to a complete exam. CTDIvol and/or
DLP (Dose Length Product) values can be set. This feature also
is designed to check changes to protocols and keep a record if
levels are exceeded. Furthermore, GE makes available personnel
training and awareness of the relevance of dose reduction, and
this is conveyed to customers during each interaction.
Taking our commitment even further, GE is supporting a dozen
or so clinical studies across the globe focused on specific clinical
applications that are investigating pushing the dose limits even
lower. These studies will provide us with clinical evidence to
make crucial decisions on potentially reducing dose levels
further while providing adequate clinical imaging. There are
also new technologies on our horizon (see photon counting
article on page 64) that may provide additional radiation
dose reduction for our patients.
In addition to technical innovation, GE actively participates
in industry and professional groups working on national dose
registries and other policy initiatives to support and expand
the science behind CT for the benefit of our customers and
their patients. n
For a full list of references,
visit www.ctclarity.com/ctclarity/201111#pg72.
Tibor Duliskovich, MD, is Medical Director, Computed Tomography, at GE Healthcare. Dr. Duliskovich earned his medical degree from Semmelweis Medical University (Budapest) and was a staff radiologist at Haynal Imre Medical University (Budapest). He led the Organizational and Methodological Department at the National Institute of Radiology and Radiation Physics in Hungary, where his department oversaw the design, manufacturing, installation and servicing of medical imaging devices to ensure safety and effectiveness. Prior to assuming his current position at GE, he has held various management positions at medical device and healthcare informatics companies, including DigiX, Inc.; Wuestec, Inc.; StorCOMM, Inc.; Aspyra, Inc.; and Philips Healthcare. Dr. Duliskovich joined GE in January 2011, and in his medical affairs role supports regulatory submissions, marketing, scientific publications, patient safety, and medical risk assessment process across the CT products; and helps align clinical research activities with business needs from medical perspective.
References
1. Available at http://www.acr.org/SecondaryMainMenuCategories/quality_safety/app_criteria.aspx

73www.gehealthcare.com/ct • November 2011
b e y o N d t h e s c a Nw o r l d w i d e e d u c a t i o N
A clinical education specialist by your side whenever you need it
AppsLinq* is a new remote training service for troubleshooting
and training that will help your CT department solve application-
related problems, improve efficiency, and develop important
new skills.
Enabled through broadband connectivity, a clinical education
specialist can follow the CT console or AW workstation in real
time through a secure Broadband connection. This allows CT
application training to take place as if the clinical education
specialist is in the imaging department by your side.
Redefining applications training
AppsLinq revisits traditional online training and places emphasis
on practicality. It combines the hands-on benefits of on-site
training with the convenience and fast response time of distance
learning. Also, it allows training to be conducted in available time
slots within the hectic schedule of an imaging department.
Once the intial training on-site has been delivered, AppsLinq
provides an ideal solution to complete your ongoing training
in combination with technology and clinical classrooms. n
For the latest information on training for Europe, Middle East,
and Africa, visit www.gehealthcare.com/clinicaleducation. »“I forgot how to…”
“Help me with an advanced application...”
Refresh training on CT or workstation applications
Quick support to avoid patient flow disruptions
Application support to prepare challenging exams
Customized training sessions to best fit the day’s busy schedule
Europe, Middle East, and Africa Clinical Education

74 A GE Healthcare CT publication • www.ctclarity.com
b E y o n d T H E s C A n w o r l d w i d E E d u C A T i o n
CT Masters Series
The CT Masters Series are advanced training courses designed
for radiologists, cardiologists, and radiologic technologists.
The courses provide a unique opportunity for participants to
learn from experts and receive individual attention in order
to maximize their learning experience and ensure that they
acquire the skills and confidence necessary for success.
Training is offered in cardiac CT angiography, peripheral
CT angiography, Gemstone Spectral Imaging, virtual
colonoscopy, and CT dose reduction. The CT Masters Series
curricula are designed with industry requirements in mind. The
cardiovascular-focused courses are endorsed by the Society
of Cardiovascular Computed Tomography (SCCT). n
United States Clinical Education
CTA of the Coronaries: From Novice to Expert
Tracy Q. Callister, MD, FSCAI
Hyatt Place
Hendersonville, TN
Cardiac CTA: Beyond the Coronaries Tracy Q. Callister, MD, FSCAI
Hyatt Place
Hendersonville, TN
Cardiac CTA: Advanced Course
Matthew Budoff, MD
Harbor UCLA
Los Angeles, CA
Peripheral CTA: Advanced Course
Matthew Budoff, MD
Harbor UCLA
Los Angeles, CA
Cardiovascular

75www.gehealthcare.com/ct • November 2011
b e y o N d t h e s c a Nw o r l d w i d e e d u c a t i o N
For dates, CME information, and training opportunities,
visit: www.gehealthcare.com/gectmasters
or call 262-312-7148.
India Clinical EducationHealthcare in India, like many emerging economies, is challenged by the small population of trained radiologists and radiology
technicians across the region’s vast geography. This lack of coverage is the main barrier to increasing access to healthcare
in the region. To address this challenge, GE Healthcare’s South Asia CT Team is initiating a training program for radiology
technicians in association with the Society of Indian Radiographers (SIR), the largest radiographer society in the region. The first
residential training program is expected in the fourth quarter of 2011 with plans to initiate training programs at a later date for
radiology consultants in advanced CT Technologies, such as low-dose CT imaging and Gemstone Spectral Imaging.
For more information on CT Educational programs in South Asia, please email [email protected] n
Cardiovascular CTA for Technologists
Joey Glass, RT(R)(CT)
Cardiology Associates
Mobile, AL
Cardiovascular CTA for CT Technologists
Rob Jennings, RT(R)(CT)
Judy Lane, RT(R)(CT)
Fairfax Radiological Consultants, P.C.
Fairfax, VA
Cardiac Imaging with CT: Advanced Certification
Ronald P. Karlsberg, MD
Cardiovascular Medical Group
of Southern California
Beverly Hills, CA
Cardiovascular
Gemstone Spectral Imaging Workshop
James P. Earls, MD
GE Healthcare Institute,
Waukesha, WI
Gemstone Spectral Imaging
Virtual Colonoscopy for Radiologists
Abraham H. Dachman, MD, FACR
GE Healthcare Institute,
Waukesha, WI
Virtual Colonsocopy
CT Dose Reduction and Scanning Techniques
Mannudeep K. Kalra, MD
GE Healthcare Institute,
Waukesha, WI
Low Dose Imaging

More Clarity. Now on tap.
GE Healthcare
Now you can have complete issues of GE Healthcare’s CT Clarity, the Magazine of CT, right at your fingertips when you’re on the go. The CT Clarity App links you to a vital source for the latest news about GE Healthcare CT on your iPad, iPhone, or Android tablet or phone. Download the free tablet and smartphone applications at the Apple Store (www.apple.com) or Android Market Apps (www.market.android.com). Or, simply scan the QR code below with your iPhone.
Apple
Follow us on Twitter: @GEHealthcare
© 2011 GE Healthcare, a division of General Electric Company.
iPhone and iPad are registered trademarks of Apple, Inc.
Android is a trademark of Google, Inc.
CT-0494-11.11-EN-US


















