
CS 2015 Mechanical Properties of Lung and Chest Wall Christian Stricker Associate Professor for...
30
CS 2015 Mechanical Properties of Lung and Chest Wall Christian Stricker Associate Professor for Systems Physiology ANUMS/JCSMR - ANU [email protected] http:/ /stricker.jcsmr.anu.edu.au/ Mechanics. pptx THE AUSTRALIAN NATIONAL UNIVERSITY
-
Upload
melinda-parsons -
Category
Documents
-
view
228 -
download
10
Transcript of CS 2015 Mechanical Properties of Lung and Chest Wall Christian Stricker Associate Professor for...

CS 2015
Mechanical Properties of Lung and Chest Wall
Christian StrickerAssociate Professor for Systems Physiology
ANUMS/JCSMR - ANU
[email protected]://stricker.jcsmr.anu.edu.au/Mechanics.pptx
THE AUSTRALIAN NATIONAL UNIVERSITY

CS 2015

CS 2015
Aims
At the end of this lecture students should be able to
• explain different types of air flow conditions;
• identify determinants of airway resistance (RAW);
• illustrate the concepts of static and dynamic
compliance and how these are measured;
• demonstrate why a small lung volume is harder to
inflate than a larger; and
• point out how surfactants increase compliance.

CS 2015
Contents
• Airway resistance– Air flow conditions
– Locations and determinants of RAW
– Transmural pressure
• System compliance and its elements– Static & dynamic compliances
– Alveolar surface tension
– Laplace’ law and alveolar pressure
– Surfactants and compliance

CS 2015
Determinants of RAW
• Air flow conditions
• Locations and determinants of RAW
• Transmural pressure
• Modulation of RAW
CS 2015
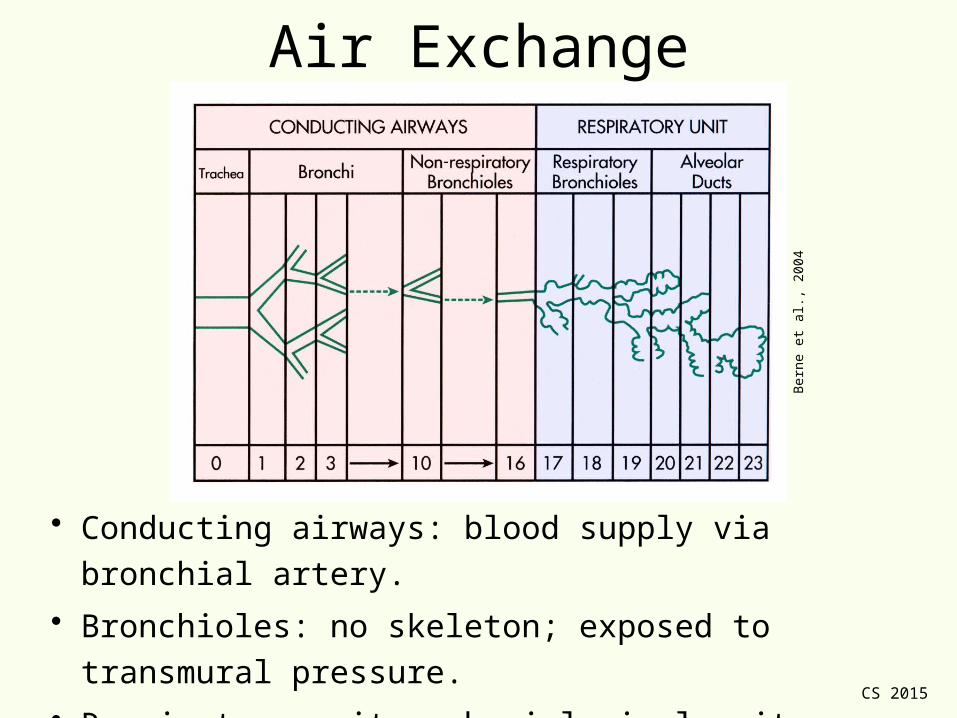
Air Exchange
• Conducting airways: blood supply via bronchial artery.
• Bronchioles: no skeleton; exposed to transmural pressure.
• Respiratory unit = physiological unit, where O2 and CO2
are exchanged; blood supply via pulmonary artery.
Ber
ne e
t al.,
200
4

CS 2015
Consequences for Air Flow
• Flow over vocal cords is biggest and decays later to small
values in alveolar airways.
• Functional consequence: ~ turbulent flow over vocal cords;
but ~ laminar flow in alveolar airways.
Bor
om &
Bou
lpae
p, 2
003

CS 2015
Flow Conditions in Airways• Since airways are bifurcated, turbulence arises at
bifurcation points.
• Flow in airways is transitional (in between laminar
and turbulent).
• Ohm’s law is used to determine RAW (airway and
tissue deformation):
• Contribution to RAW:
Boron & Boulpaep, 2003

CS 2015
Determinants of RAW
• Under laminar flow conditions,
with η viscosity, l length and r radius.
• Normally, viscosity is constant (air); altered
with pressure (altitude, diving) & gas mixtures.
• Elements of RAW (around TV)
– Rvisc ~ 40% (dynamic parameter; flow dependent).
• Laminar and turbulent conditions (80%)
• Tissue resistance (“friction” between elastic fibres; 20%)
• Inertia (very little)
– Relast ~ 60% (static parameter; volume dependent).

CS 2015
RAW and Lung Volume
• Lung volume affects airway diameter, particularly airways
without skeleton: during E, tension release (alveolar size ↓)
and positive pressure on bronchioli → r ↓; during I, vice
versa.
• It is easier to breath in than out (air trapping…).
• COPD: r↓ → RAW↑. To maintain ventilation, flow↑.
Mod
ified
from
Bor
on &
Bou
lpae
p, 2
003

CS 2015
Transmural Pressures
• Affects bronchioles
• During forced I, positive
transmural pressure keeps
small airways open.
• During forced E, when Ppl >
0, transmural pressure can
become ≤ 0; i.e. airways
collapse.
• Can be seen in flow-volume
loop: airway closure.
Modified from Hlastala & Berger 2001

CS 2015
Modulation of RAW
• Smooth muscle tone– Parasympathetic: bronchial constriction and mucus production ↑.
– Sympathetic: β2-action (smooth muscle relaxation, secretion ↓).
• With ↑ → local airway dilation; ↓→ local airway constriction.
Ber
ne e
t al.,
200
4

CS 2015
Compliance of Breathing System
• Static & dynamic compliances
• Alveolar surface tension- Laplace’ law and alveolar pressure
- Surfactants and compliance

CS 2015
Compliance of Breathing System
Static compliance: no flow, volume fixed
Dynamic compliance: both flow, volume change
CT = total compliance (breathing system)
CL = lung compliance
CCW = thorax (chest wall) compliance

CS 2015
How to Measure Compliances• Shown with body
plethysmograph.– Required for Cdyn.
– Not necessary for Cstatic (no
flow…).
• Cstatic with valve and
spirometer only.– Measured during expiration
(see later).
– PA and ΔVL measured
simultaneously after halting
flow (= Poral): at each
volume, PA measured.
Modified from Boron & Boulpaep, 2003

CS 2015
Static Lung Compliance (No Flow)
• Total system compliance (CT) can be
measured after breathing out (“relaxation
curve”); linear within range of TV.
• Both lung (CL; fibrosis – too small;
emphysema – too large) and chest-wall
compliance (CCW; skoliosis) are needed
clinically.
• CT is related to CCW and CL via
• Requires that Ppl be measured with each
volume change.
• Within TV, CL ~ CCW ~ 2 CT, ~ 0.1 L/cm
H2O.Modified from Hlastala & Berger 2001

CS 2015
Static CL and Pathology
• Static CL important in
pathophysiology.
• Emphysema (“overblown”
lung) has large
compliance at FRC: loss
of recoil (elastance; 1/CL).
• Conversely, fibrosis
reduces CL and FRC: too
much recoil …Modified from Boron & Boulpaep, 2003

CS 2015
Dynamic Compliance• Example for TV
• Hysteresis (CCW move)
• Cdyn at end of E > than at
beginning of I.– For both I and E, smaller at
beginning than at end.
– Elastic recoil > at end of I
which helps at start of E
• Cstat ≈ average Cdyn (which
is typically a bit smaller).
• Effort sets width of
hysteresis.Modified from Despopoulos & Silbernagl 2003

CS 2015
Compliances in Disease• Emphysema with a high static
compliance and a wide
dynamic hysteresis (work! -
recoil lost).
• Asthma increases
compliance; TV at FRC↑;
large expiratory work
(increased RAW).
• RDS has low static and
dynamic compliance and TV
at high pressures.Modified from Koller, 1979

CS 2015
Alveolar Surface Tension
Laplace’ law
Surfactants
CS 2015
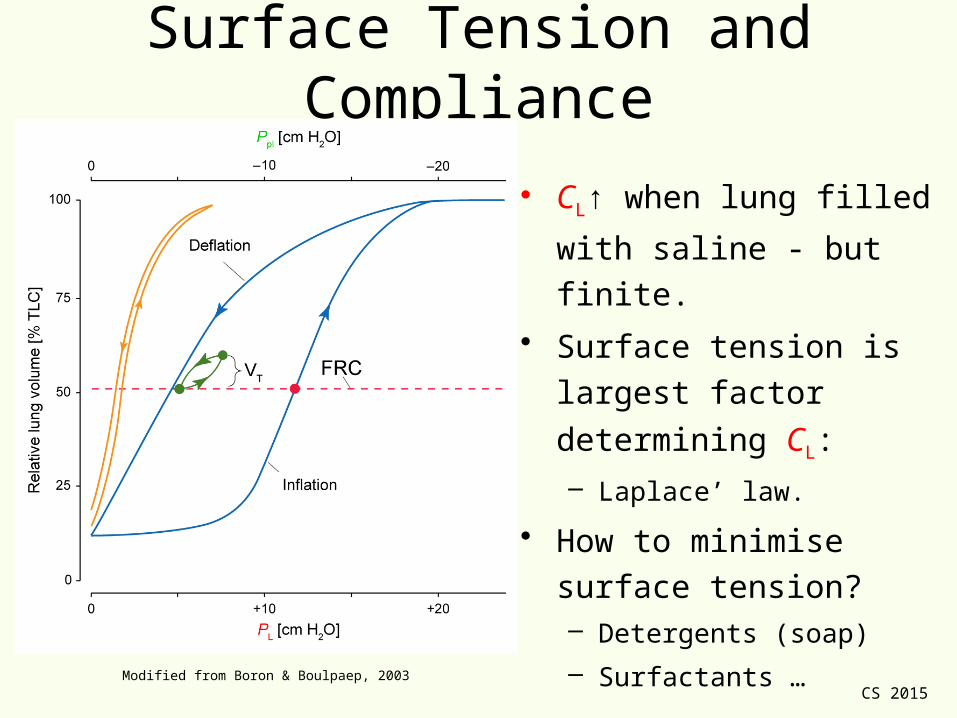
Surface Tension and Compliance
• CL↑ when lung filled with
saline - but finite.
• Surface tension is largest
factor determining CL:
– Laplace’ law.
• How to minimise surface
tension?– Detergents (soap)
– Surfactants …
Modified from Boron & Boulpaep, 2003

CS 2015
What Every Child Knows…
• What is the hardest part to
blowing up a balloon?– Initial volume change…
– Becomes easier as you inflate…
– Ultimately so easy, it can be
blown apart…

CS 2015
Laplace’ Law
•
• Precoil in B is 2 x that in A.
• If A and B are coupled in series,
what happens?– B blows A up.
• To counter this, alveoli are– interdependent: physically
interconnected with each other; and
– lined with surfactant.
Mod
ified
from
Bor
on &
Bou
lpae
p, 2
003

CS 2015
Surfactants and Surface Tension• Surfactant (surface-active agent)
• Reduces surface H2O and hence
surface tension: it is an attractive force
of surface molecules that tends to
minimise surface area.
• Combination of dipalmitoylphosphatidyl-
choline and apoproteins (SP-A/B/C/D).
• Secreted by alveolar type II cells
• Can easily be destroyed with O2.
• Produced shortly before birth; problem
in premature babies (respiratory
distress syndrome).– Steroid priming for 2-3 d can initiate
surfactant expression.
Modified from Boron & Boulpaep, 2003

CS 2015
Surface Expression• Surfactants form micelles.
• Dynamic system:– During I, as alveolar surface
increases and [surfactant]
decreases, surfactant from
micelles is recruited to surface.
– During E, alveolar surface de-
creases, [surfactant] is higher
and micelles re-form.
• Role:– Reduction in surface tension:
keeps alveoli “open”.
– Keeping alveoli dry.Modified from Hlastala & Berger 2001

CS 2015
Ventilation and Surfactants
• Rapidly expanding alv. →
[surfactant]↓ → CA↓ →
ventilation↓.
• Slowly expanding alv. →
[surfactant]↑ → CA↑ →
ventilation↑.
• Homeostatic principle to
open alveoli to ~ similar volume.
Modified from Boron & Boulpaep, 2003

CS 2015
Take-Home Messages• Flow in bronchi is transitional, in alveoli
laminar.
• RAW is volume dependent; is neurally
modulated.
• CL is ~2 x CT; is linear in range of TV.
• A small alveolus requires a larger pressure to increase its volume than a large one;
• Hysteresis in V-P loop is result of surface tension and Laplace’ law; and
• Surfactants reduce surface tension and ease alveolar ventilation.
CS 2015
MCQAnna May, a 43 year-old female, has an extensive lung
function analysis. As she exhales under static conditions from
FRC + 1 L to FRC, her oesophageal pressure changes from -
10 to -5 cm H2O and the alveolar pressure from 5 to 0 cm
H2O. What is the best estimate of her static lung compliance?
A. 0.5 L / cm H2O
B. 5.0 cm H2O / L
C. 0.1 L / cm H2O
D. 2.0 cm H2O / L
E. 0.2 L / cm H2O

CS 2015
That’s it folks…

CS 2015
MCQAnna May, a 43 year-old female, has an extensive lung
function analysis. As she exhales under static conditions from
FRC + 1 L to FRC, her oesophageal pressure changes from -
10 to -5 cm H2O and the alveolar pressure from 5 to 0 cm
H2O. What is the best estimate of her static lung compliance?
A. 0.5 L / cm H2O
B. 5.0 cm H2O / L
C. 0.1 L / cm H2O
D. 2.0 cm H2O / L
E. 0.2 L / cm H2O


















