CRITICAL CARE M&M Adam Noyes PGY-3 Justin Goralnik PGY-2.
21
CRITICAL CARE M&M Adam Noyes PGY-3 Justin Goralnik PGY-2
-
Upload
rodney-oliver -
Category
Documents
-
view
231 -
download
7
Transcript of CRITICAL CARE M&M Adam Noyes PGY-3 Justin Goralnik PGY-2.

CRITICAL CARE M&M
Adam Noyes PGY-3Justin Goralnik PGY-2

Cause of Death
Hydrochloric Acid Ingestion pH 1 It is a highly corrosive, strong mineral acid
with many industrial uses (household cleaning).
Hydrochloric acid is found naturally in gastric acid.

Caustic Ingestions
The clinical features of caustic ingestions vary widely. Early signs and symptoms may not correlate with the severity
and extent of tissue injury. Patients may complain of oropharyngeal, retrosternal or
epigastric pain, dysphagia/odynophagia, or hypersalivation. Persistent severe retrosternal or back pain may indicate
esophageal perforation with mediastinitis. Other findings include vomiting, hematemesis, and persistent,
localized abd tenderness, rebound, and rigidity that may indicate esophageal or gastric perforation with peritonitis.
Caustic injury to the oropharynx causes pain and inability to clear pharyngeal secretions with persistent drooling.
Hoarseness, stridor, aphonia and respiratory difficulties are less common and result from caustic burns of the epiglottis and larynx.
Fever, tachycardia, and shock generally imply the presence of more severe and extensive injury.

Caustic Ingestions
Alkali ingestions damage the esophagus more than the stomach or duodenum.
Either acid or alkali can also induce both laryngeal and tracheobronchial injury.
Acids cause more severe gastric injury.
In contrast to the more viscous alkaline solutions, acid preparations tend to pass quickly into the stomach, causing less esophageal damage.

Caustic Ingestion
Acid ingestion produces a superficial coagulation necrosis that thromboses the underlying mucosal blood vessels and consolidates the connective tissue forming an eschar.
Because acid solutions cause pain upon
contact with the oropharynx, the amount of acid ingested tends to be limited.

HCl Necrosis

Acids and Bases
A study comparing outcomes of acid or alkali ingestion found that outcomes were overall worse for those who ingested acid.
Such patients had significantly more severe mucosal injury, were more likely to be hospitalized in the ICU, have systemic complications or perforation, and had higher mortality.
Poley JW, Gastrointest Endosc. 2004;60(3):372.

Pathologic Severity of Injury
Caustic injuries to the gastrointestinal tract are classified pathologically, similar to burns of the skin: First-degree injury results from superficial
mucosal damage and is characterized by focal or diffuse erythema, edema, and hemorrhage. No scar formation.
Second-degree injury shows mucosal and sub-mucosal damage, ulcerations, exudates, and vesicle formation. Granulation tissue and then a fibroblastic reaction, produces a scar and possible stricture.
Third-degree injury is transmural and is characterized by deep ulcers and black discoloration and perforation of the wall.

Diagnosis and Staging
Oropharynx may reveal edema, erosions, or deep necrosis with grayish pseudomembranes.
Absence of oropharyngeal burns does not preclude the presence of esophageal or gastric injury. Thus, upper endoscopy should be performed during the first 24 hours after ingestion to evaluate esophageal and gastric damage, establish prognosis, and guide therapy.
Endoscopy is contraindicated in patients who are hemodynamically unstable, have evidence of perforation, or exhibit severe oropharyngeal or glottic edema and necrosis.

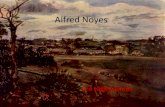
Endoscopy
Endoscopy demonstrated complete necrosis from the hypopharynx to the pylorus. a Hypopharynx (upper part: tracheal tube). b Esophagus. c Gastric corpus. d Gastric antrum.

Diagnosis and Staging
A grading system for esophageal injury to predict clinical outcome with corrosive ingestions. Grade 0 – Normal Grade 1 – Mucosal edema and hyperemia Grade 2A – Superficial ulcers, bleeding,
exudates Grade 2B – Deep focal or circumferential
ulcers Grade 3A – Focal necrosis Grade 3B – Extensive necrosis

Staging and Prognosis
The following correlations between endoscopic grading and prognosis have been observed: Patients with grades 1 and 2A have an excellent
prognosis without significant acute morbidity or subsequent stricture formation.
Patients with grades 2B and 3A develop strictures in 70-100 % of cases.
Grade 3B carries a 65 % early mortality and the need for esophageal resection in most cases.

Staging and Prognosis
Mucosal injury grade 3 is associated with a high rate of systemic complications including bleeding and perforation.
In a large retrospective study, patients with grade 3B mucosal injuries were at greater risk of prolonged hospital stay (OR 2.4), ICU admission (OR 10.8), and gastrointestinal and systemic complications (OR 4.2 and 4.1, respectively).
Mortality of patients with one or more systemic
complications was considerably high (45%). Dalus et al. reported a 100% mortality in patients with perforation or orotracheal fistula.
Cheng HT, BMC Gastroenterol. 2008;8:31.

Management
Patients suspected of having significant ingestions (based on history, symptoms, or endoscopic findings of grade 2B or greater injury) should generally be treated in a surgical or medical intensive care unit in order to manage the acute, life-threatening complications of injury (mediastinitis, peritonitis, respiratory distress, shock) and to decrease the risk of developing late esophageal strictures.
Endoscopy should be performed as soon as possible, ideally within 24 hours, in order to assess the magnitude and extent of injury.

Management
If the epiglottis or the larynx is edematous, endotracheal intubation is contraindicated and a tracheostomy should be performed for airway control.

Management
Grade 2b–3b injuries have a high risk to develop post-acute strictures and should be treated by early endoscopic dilatation.
Robustelli et al. suggested to perform CT scan in every patient with endoscopic grade 3 burn to detect early signs of perforation.
Prophylactic antibiotic therapy is generally recommended.

Management
Esophagectomy may be required for patients with severe strictures.
The need to perform surgery for caustic injuries has a persistent long-term negative impact on survival and functional outcome.
In addition, clinical signs of perforation, mediastinitis, or peritonitis are indications for emergency surgery.

Management
It is also important to recognize that certain agents and procedures are contraindicated in the presence of caustic ingestions: Use of emetics is contraindicated because vomiting
re-exposes the esophagus and the oropharynx to the caustic agent, further aggravating injury.
Neutralizing agents (weakly acidic or basic substances) should not be administered because damage is generally instantaneous. Furthermore, neutralization releases heat that adds thermal injury to the ongoing chemical destruction of tissue.
Nasogastric intubation to remove any remaining caustic material is contraindicated because it may induce retching and vomiting which can compound injury and possibly lead to perforation of the weakened esophagus or stomach.

Late Sequelae
After resolution of the initial injury patients are at risk for developing esophageal strictures and esophageal squamous cell carcinomas.
Up to one-third of patients who suffer caustic esophageal injury develop esophageal strictures, primarily in those with grade 2B or 3 injuries.
The peak incidence of dysphagia due to esophageal stricture formation after corrosive esophageal injury is two months, although it can occur as early as two weeks or as late as years after ingestion.

Late Sequelae
The risk for development of esophageal squamous cell carcinoma is 1000-fold higher in victims of alkali ingestion compared to the general population (annual risk of 2.6 per 100,000).
In one study of 63 patients, the mean latency period for development of esophageal cancer was 41 years.
Nearly all reported patients with corrosion carcinoma had consumed an alkali, although two of three patients in one study had consumed acid.
The risk of gastric cancer does not appear to be increased.
Appelqvist P. Cancer. 1980;45(10):2655

THANK YOU!