CRICOS No. 00213J Mary Sheehan TRB Human Factors Workshop Marriott Wardman Hotel, Washington, DC,...
27
CRICOS No. 00213J Mary Sheehan TRB Human Factors Workshop Marriott Wardman Hotel, Washington, DC, USA 12 January 2014 Criteria & challenges for a model of best practice for rehabilitation & treatment associated with an ignition interlock program
-
Upload
omar-revel -
Category
Documents
-
view
218 -
download
2
Transcript of CRICOS No. 00213J Mary Sheehan TRB Human Factors Workshop Marriott Wardman Hotel, Washington, DC,...

CRICOS No. 00213J
Mary Sheehan
TRB Human Factors Workshop
Marriott Wardman Hotel, Washington, DC, USA
12 January 2014
Criteria & challenges for a model of best practice for rehabilitation & treatment associated
with an ignition interlock program

Current project Austroads tender SS1755
• Should an alcohol treatment component be included with interlocks for drink driving offences?
• Specific focus on alcohol treatment appropriate for use in road safety domain

The Problem
What, if any, type of rehabilitation program should be used with an interlock intervention to reduce long term drink driving re-offending?

Effective management
• Established international evidence indicates that interlocks are the most effective management of recidivism while they are installed.
• Recidivism rates return to control (no interlock) levels when they are removed.

1. Alcohol problem/dependency treatments
Long term rehabilitation treatment for alcoholism through special purpose clinics and may or may not consider drink driving.

2. Drink driving alcohol treatment
A combination of education and treatment for alcohol misuse with specific outcome focus on separating drinking and driving.
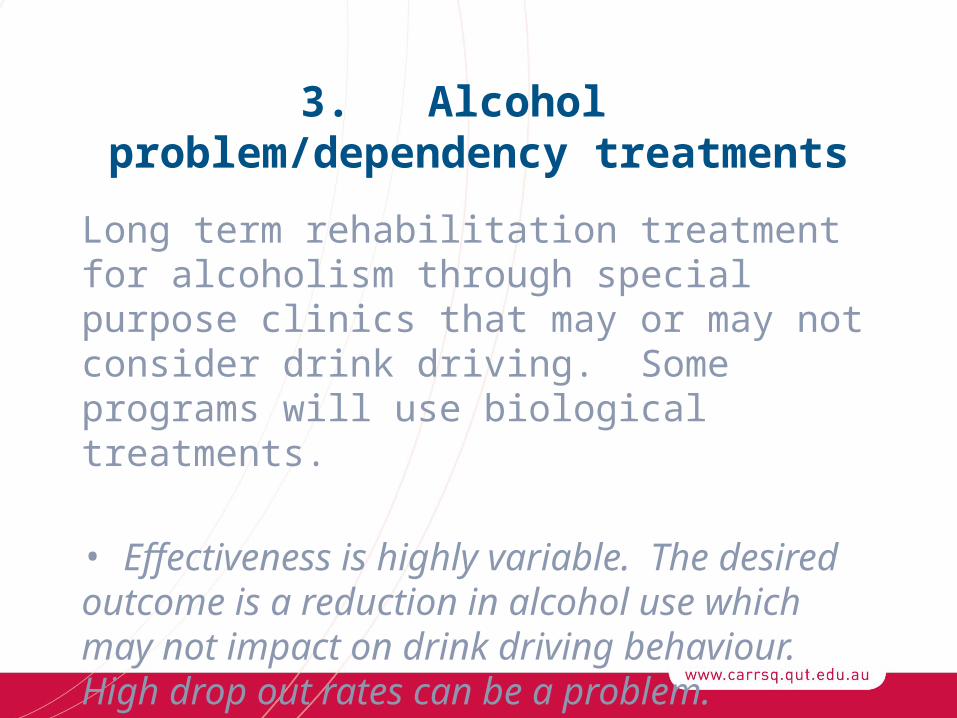
3. Alcohol problem/dependency treatments
Long term rehabilitation treatment for alcoholism through special purpose clinics that may or may not consider drink driving. Some programs will use biological treatments.
• Effectiveness is highly variable. The desired outcome is a reduction in alcohol use which may not impact on drink driving behaviour. High drop out rates can be a problem.
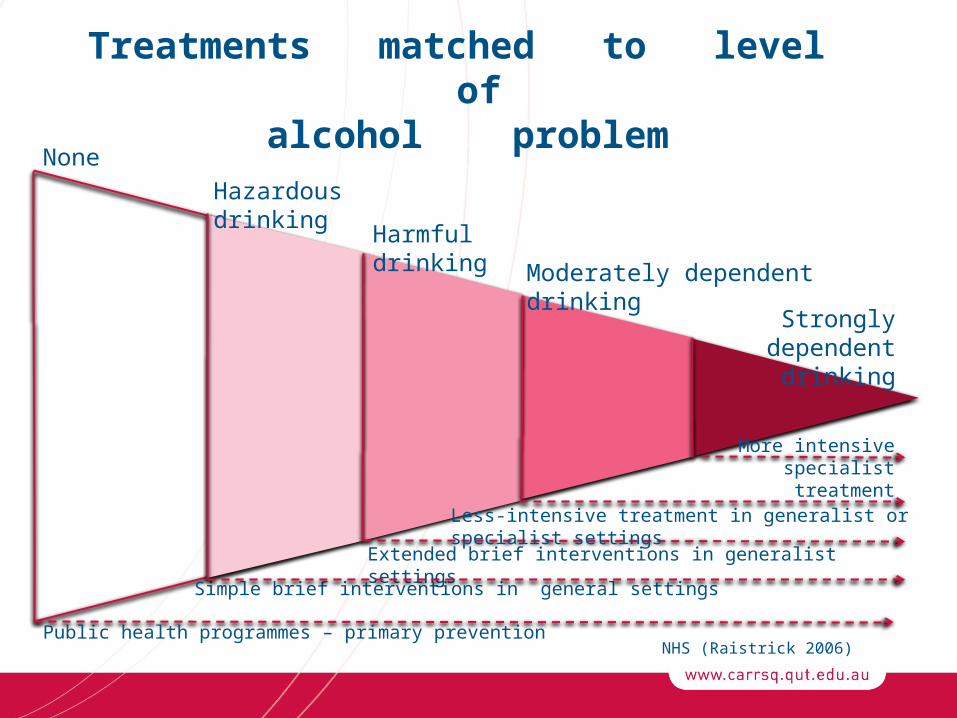
Treatments matched to level ofalcohol problem
NHS (Raistrick 2006)
None
Public health programmes – primary prevention
Simple brief interventions in general settings
Extended brief interventions in generalist settings
Hazardous drinking
Harmful drinking
Moderately dependent drinking
Strongly dependent drinking
More intensive specialist treatment
Less-intensive treatment in generalist or specialist settings

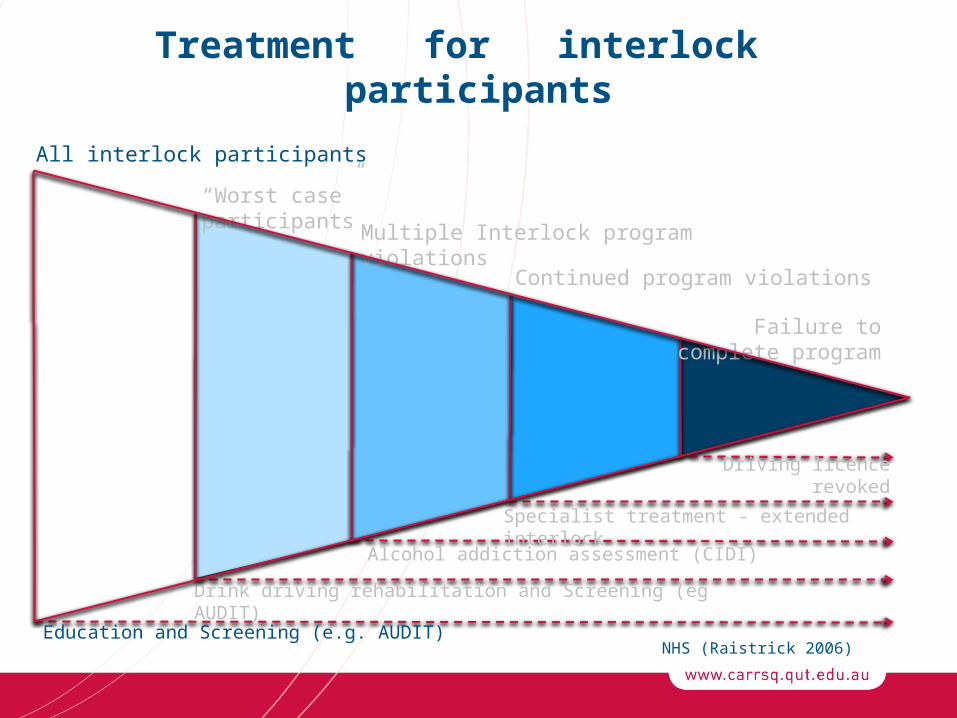
Treatment for interlock participants
NHS (Raistrick 2006)
All interlock participants
“Worst case” participants
Multiple Interlock program violations
Continued program violations
Failure to complete program
Education and Screening (e.g. AUDIT)
Drink driving rehabilitation and Screening (eg AUDIT)
Alcohol addiction assessment (CIDI)
Specialist treatment - extended interlock
Driving licence revoked
Treatment for interlock participants
NHS (Raistrick 2006)
All interlock participants
“Worst case” participants
Multiple Interlock program violations
Continued program violations
Failure to complete program
Education and Screening (e.g. AUDIT)
Drink driving rehabilitation and Screening (eg AUDIT)
Alcohol addiction assessment (CIDI)
Specialist treatment - extended interlock
Driving licence revoked

Treatment for interlock participants
NHS (Raistrick 2006)
All interlock participants
“Worst case” participants
Multiple Interlock program violations
Continued program violations
Failure to complete program
Education and Screening (e.g. AUDIT)
Drink driving rehabilitation and Screening (eg AUDIT)
Alcohol addiction assessment (CIDI)
Specialist treatment - extended interlock
Driving licence revoked

Treatment for interlock participants
NHS (Raistrick 2006)
All interlock participants
“Worst case” participants
Multiple Interlock program violations
Continued program violations
Failure to complete program
Education and Screening (e.g. AUDIT)
Drink driving rehabilitation and Screening (eg AUDIT)
Alcohol addiction assessment (CIDI)
Specialist treatment - extended interlock
Driving licence revoked

Treatment for interlock participants
NHS (Raistrick 2006)
All interlock participants
“Worst case” participants
Multiple Interlock program violations
Continued program violations
Failure to complete program
Education and Screening (e.g. AUDIT)
Drink driving rehabilitation and Screening (eg AUDIT)
Alcohol addiction assessment (CIDI)
Specialist treatment - extended interlock
Driving licence revoked

Treatment for interlock participants
NHS (Raistrick 2006)
All interlock participants
“Worst case” participants
Multiple Interlock program violations
Continued program violations
Failure to complete program
Education and Screening (e.g. AUDIT)
Drink driving rehabilitation and Screening (eg AUDIT)
Alcohol addiction assessment (CIDI)
Specialist treatment - extended interlock
Driving licence revoked

What are the outcomes for treatment for recidivists?
• Full rehabilitation from alcohol dependency?
• Separation of drinking from driving?
OR
• No driving without an interlock?
Exiting the interlock programme(1)
When should participants exit the programme?– ‘Exit period’ e.g. 3 months with no lockouts?– Ceased alcohol consumption?– No tampering?

Exiting the interlock programme(2)
• Should those who fail the interlock programme have their licence revoked permanently without an interlock?
• Should failed participant be mandated to an extended interlock programme?

Goals of interlock programme
Reduced road crashes and associated injuries and fatalities
BY
Reducing recidivism.

What should be the optimal outcome for drink drivers in
interlock programmes?
Full rehabilitation from alcohol dependency?
OR
Separation of drinking from driving?
OR
No licence without an interlock?

Alcohol addiction assessment for multiple interlock violations
• After how many violations?
• Is this early enough for assessment or should all participants attend substance abuse assessment at the start of the interlock program?

Priorities in Interlock Rehabilitation
• High level BAC fails/lockouts that occur after the original learning period should be used as additional screening information and alert for probable addiction (and therefore treatment).
• There should be introductory education that includes explaining the interlock and how it will work when they are driving.

Priorities in Interlock Rehabilitation (cont’d)
• Records of interlock failures and non-failures should be used as part of the assessment process at the completion of the sentencing period.
• Circumvention, driving after a failed test, and driving another vehicle are all serious violations.
Priorities in Interlock Rehabilitation (cont’d)
• Interlock data should be combined with a therapist assessment to determine interlock program exit.
• At the end of sentencing, people who have a history of interlock fails should be required to attend treatment before re-licensing.

Priorities in Interlock Rehabilitation (cont’d)
• Records of interlock failures and non-failures during the interlock sentence period should be linked to motivation to change strategies including the possibility of reduced fees for failure-free records.
• Interlock should be fitted as early as possible during licence suspension.

Priorities in Interlock Rehabilitation (cont’d)
• Alcohol addiction severity assessment/
screening should be used with all interlock participants.
• There should be education that is personalised and takes participants’ drinking patterns into account.

Priorities in Interlock Rehabilitation (cont’d)
• Education, including counselling, should be part of the interlock participation.
• BAC fails in the initial period should not be considered a serious violation.
• Treatment should be required (mandatory) for persons violating the program.

Questions?
CRICOS No. 00213J
Acknowledgements:AustroadsJurisdiction representatives