
Craniofacial Osseointegration - OSSEO 2019€¦ · Osseointegration Conference Handbook 2013. The...
105
The Sage Gateshead 6 - 8 June 2013 www.osseo2013.com © Richard Bryant The 4 th International Symposium on Bone Conducting Hearing — Craniofacial Osseointegration Conference Handbook 2013
Transcript of Craniofacial Osseointegration - OSSEO 2019€¦ · Osseointegration Conference Handbook 2013. The...

The Sage Gateshead 6 - 8 June 2013 www.osseo2013.com
© R
icha
rd B
ryan
t
The 4th International Symposium on Bone Conducting Hearing — Craniofacial Osseointegration
Conference Handbook 2013

The 4th International Symposium on Bone Conducting Hearing
— Craniofacial Osseointegration
I am pleased to welcome you to the fourth international symposium on bone conduction hearing – craniofacial osseointegration being held this year at the Sage Gateshead in Newcastle-upon-Tyne. Following on from our successful international meetings in Canada, Sweden and the USA we are all looking forward to seeing what the North East has to offer.
Aside from being a great opportunity for you to hear and see the latest developments in our field, our social programme will ensure that you have time to enjoy your surroundings and meet up with colleagues and friends.
With key themes including new solutions, technologies and paediatric solutions alongside a range of international keynote speakers, this year’s symposium is shaping up to be one of the most successful yet.
Make sure you enjoy yourself and are able to get as much as you can from our extensive programme.
Glad you could join us.
Ian Johnson
Conference Chair, International Symposium on Bone Conducting Hearing
Welcome
3 Welcome

6
7
8
11
12
16
18
67
133
161
General Information
Conference Highlights
Conference Programme
Accompanying Persons Programme
Keynote Speakers
Sponsors & Exhibitors
Oral Abstracts - Thursday
Oral Abstracts - Friday
Oral Abstracts - Saturday
Poster Abstracts
Contents
4 Welcome
Thank you for all the hard work of the scientific committee, for their input in the conference programme and in reviewing abstracts .
Many thanks also to Benchmark Communications, our expert conference organisers who have managed and planned this event from start to finish.
Finally, thanks to all sponsors and exhibitors for their efforts in making this symposium a success.
Acknowledgements
5 Welcome

General Information
Registration & Conference Information Desk
The conference desk is situated on the Concourse Level at the West entrance before entering the exhibition area. This will be staffed at all times. The registration desk will be open at the following times
• Thursday 6 June 08:30 - 17:30
• Friday 7 June 08:00 - 17:45
• Saturday 8 June 08:00 13:00
You will be able to pick-up your social event tickets here too.
NGI Help Desk
The Newcastle Gateshead Initiative Tourist Information team will have their own stand right next to the conference registration desk to give advice on what to see and do in the region. They will be available on Thursday and Friday until 13:00.
Security
Please wear your name badge at all times; it is your pass to gain access to the Conference sessions.
Cloakroom Facilities
The Cloakroom facilities are situated opposite the registration desk and are free of charge.
Parking
The Sage Gateshead car park is situated directly behind the building and has lift access to the venue. There is a special delegate rate of £4 Per Day for OSSEO attendees. Please pick up a parking ticket from the registration desk.
Exhibition and Posters
The Exhibition will take place on the Concourse Level with the Poster Exhibition situated on Hall 1 and 2 level 1 foyers.
Conference Sessions
The main conference sessions will be held in Hall 1, Hall 2 and the Barbour Room these are all easily accessible from the main concourse level and will be sign-posted.
Here to Help
We will have staff situated throughout the venue for you to approach if you have any queries.
Lunch and Refreshments
Tea and Coffee will be served during conference breaks within the exhibition area. A buffet lunch will also be served in this area giving you an ideal opportunity to visit our exhibitors.
Taxis
If you require a taxi please ask at the registration desk.
6 General Information
Conference Highlights
Thursday 6 June
Conference Opening Welcome – Hall 1Time: 9.30 – 10.00
Hear from your conference chair and enjoy the sounds of the region as the conference is officially opened with a traditional Northumberland Piper.
Guest Speaker Presentation: Isabelle de Groote – Hall 1Time: 10.00 – 10.30
Isabelle will be giving insights into the palaeoanthropological past with her session entitled ‘Keeping an Ear Out for Our Fossil Ancestors’. With her
work analysing and interpreting the newly discovered excavation notes from Taforalt Cave and her position as a Post Doctoral Researcher in the at The National History Museum, we are honoured to include her in this year’s programme.
Welcome Reception – Concourse LevelTime: 17.30 -19.30
Kick-back and relax after the first day of sessions whilst enjoying views of the River Tyne at the conference welcome reception taking place at the Sage Gateshead.
Friday 7 June
Guest Speaker Presentation: Dr. Bill HoggetsTime: 8.30 – 9.00
Bill is a highly engaging and informative speaker and will be giving the audience a look into a comparison trial of prescription and verification of bone anchored devices. With his current post as Program Director of Bone Conduction Amplification at the Institute for Reconstructive Sciences in Medicine at the University of Alberta, delegates will benefit from his work in this area.
Conference Dinner at the Discovery MuseumTime: 19.15 – 23.30
Marvel at the museum’s wealth of maritime and scientific history as you receive a welcome drink in the impressive main atrium. The focal point and the backdrop for the reception will be the Turbinia ship, a ship that changed the face of maritime history and which was, at one time, the fastest ship in the world.
Guests will then make their way, courtesy of a traditional Northumberland Piper, to the prestigious Great Hall to enjoy a delicious 3- course meal.
Saturday 8 June
Guest Speaker Presentation: Professor Stefan StenfeltTime: 8.30 – 9.00
With his extensive publications in the area of bone conduction, Stefan will be sharing his knowledge on just what is possible in the field in his session titled ‘ Binaural Hearing with Bone Conduction Stimulation – What is Possible’. With its look at what can be achieved this is not a session to be missed.
Excursion to Alnwick CastleTime: 13.00 – 17.30
With an enticing history from the medieval crusades, to the gunpowder plot all the way to Quidditch matches, Alnwick Castle (also known as the ‘Windsor of the North’) is an event not to be missed.
Delegates will take a personal tour of the castle which will culminate in a traditional Afternoon-Tea in the splendour of the Great Hall. A selection of sandwiches, scones and specialist teas will be on offer for you to enjoy.
7 Conference Highlights
‘Don’t forget our round table sessions happening throughout the conference duration; this is your chance to put your questions to the experts.’
Conference Programme
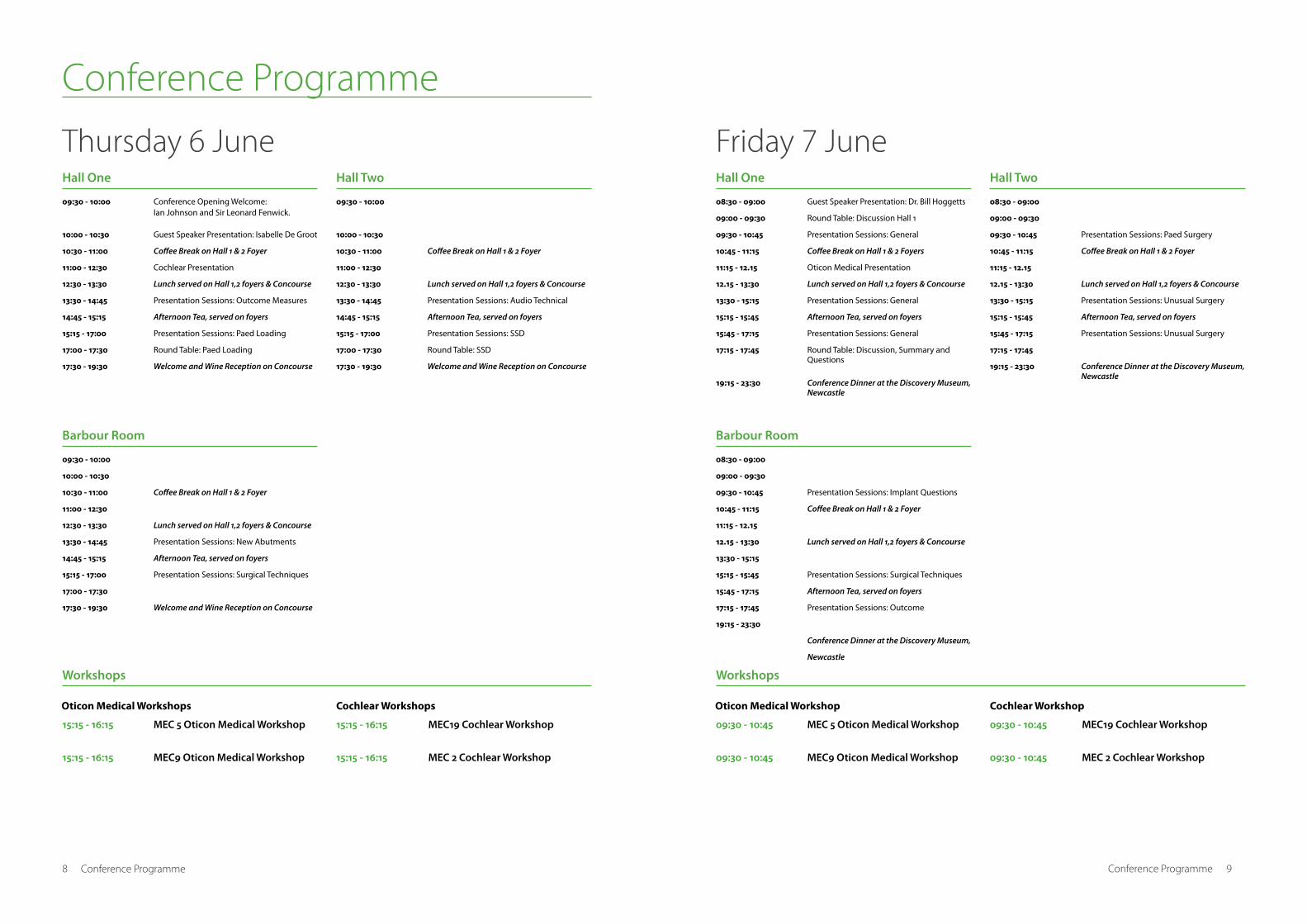
Thursday 6 June
8 Conference Programme
09:30 - 10:00
10:00 - 10:30
10:30 - 11:00
11:00 - 12:30
12:30 - 13:30
13:30 - 14:45
14:45 - 15:15
15:15 - 17:00
17:00 - 17:30
17:30 - 19:30
09:30 - 10:00
10:00 - 10:30
10:30 - 11:00
11:00 - 12:30
12:30 - 13:30
13:30 - 14:45
14:45 - 15:15
15:15 - 17:00
17:00 - 17:30
17:30 - 19:30
15:15 - 16:15
15:15 - 16:15
15:15 - 16:15
15:15 - 16:15
MEC 5 Oticon Medical Workshop
MEC9 Oticon Medical Workshop
MEC19 Cochlear Workshop
MEC 2 Cochlear Workshop
09:30 - 10:00
10:00 - 10:30
10:30 - 11:00
11:00 - 12:30
12:30 - 13:30
13:30 - 14:45
14:45 - 15:15
15:15 - 17:00
17:00 - 17:30
17:30 - 19:30
Conference Opening Welcome: Ian Johnson and Sir Leonard Fenwick.
Guest Speaker Presentation: Isabelle De Groot
Coffee Break on Hall 1 & 2 Foyer
Cochlear Presentation
Lunch served on Hall 1,2 foyers & Concourse
Presentation Sessions: Outcome Measures
Afternoon Tea, served on foyers
Presentation Sessions: Paed Loading
Round Table: Paed Loading
Welcome and Wine Reception on Concourse
Coffee Break on Hall 1 & 2 Foyer
Lunch served on Hall 1,2 foyers & Concourse
Presentation Sessions: New Abutments
Afternoon Tea, served on foyers
Presentation Sessions: Surgical Techniques
Welcome and Wine Reception on Concourse
Coffee Break on Hall 1 & 2 Foyer
Lunch served on Hall 1,2 foyers & Concourse
Presentation Sessions: Audio Technical
Afternoon Tea, served on foyers
Presentation Sessions: SSD
Round Table: SSD
Welcome and Wine Reception on Concourse
Hall One
Barbour Room
Workshops
Hall Two
Oticon Medical Workshops Cochlear Workshops
Friday 7 June
08:30 - 09:00
09:00 - 09:30
09:30 - 10:45
10:45 - 11:15
11:15 - 12.15
12.15 - 13:30
13:30 - 15:15
15:15 - 15:45
15:45 - 17:15
17:15 - 17:45
19:15 - 23:30
08:30 - 09:00
09:00 - 09:30
09:30 - 10:45
10:45 - 11:15
11:15 - 12.15
12.15 - 13:30
13:30 - 15:15
15:15 - 15:45
15:45 - 17:15
17:15 - 17:45
19:15 - 23:30
09:30 - 10:45
09:30 - 10:45
09:30 - 10:45
09:30 - 10:45
MEC 5 Oticon Medical Workshop
MEC9 Oticon Medical Workshop
MEC19 Cochlear Workshop
MEC 2 Cochlear Workshop
08:30 - 09:00
09:00 - 09:30
09:30 - 10:45
10:45 - 11:15
11:15 - 12.15
12.15 - 13:30
13:30 - 15:15
15:15 - 15:45
15:45 - 17:15
17:15 - 17:45
19:15 - 23:30
Guest Speaker Presentation: Dr. Bill Hoggetts
Round Table: Discussion Hall 1
Presentation Sessions: General
Coffee Break on Hall 1 & 2 Foyers
Oticon Medical Presentation
Lunch served on Hall 1,2 foyers & Concourse
Presentation Sessions: General
Afternoon Tea, served on foyers
Presentation Sessions: General
Round Table: Discussion, Summary and Questions
Conference Dinner at the Discovery Museum, Newcastle
Presentation Sessions: Implant Questions
Coffee Break on Hall 1 & 2 Foyer
Lunch served on Hall 1,2 foyers & Concourse
Presentation Sessions: Surgical Techniques
Afternoon Tea, served on foyers
Presentation Sessions: Outcome
Conference Dinner at the Discovery Museum,
Newcastle
Presentation Sessions: Paed Surgery
Coffee Break on Hall 1 & 2 Foyer
Lunch served on Hall 1,2 foyers & Concourse
Presentation Sessions: Unusual Surgery
Afternoon Tea, served on foyers
Presentation Sessions: Unusual Surgery
Conference Dinner at the Discovery Museum, Newcastle
Hall One
Barbour Room
Workshops
Hall Two
Oticon Medical Workshop Cochlear Workshop
9 Conference Programme

Conference Programme
Saturday 8 June
10 Conference Programme
08:30 - 09:00
09:00 - 09:30
09:30 - 10:45
10:45 - 11:15
11:15 - 12:15
12:15 - 12:30
12:30 - 13:00
13:00
15:30
17:30
08:30 - 09:00
09:00 - 09:30
09:30 - 10:45
10:45 - 11:15
11:15 - 12:15
12:15 - 12:30
12:30 - 13:00
13:00
15:30
17:30
Guest Speaker - Prof Stefan Stenfelt
Round Table: Discussion, Setting
Presentation Sessions: Paed Audiology
Coffee Break on Hall 1 & 2 Foyer
Presentation Sessions: Localisation
Close of Conference - Ian Johnson
Speaker from the next Conference - Dr Bill Hoggetts
Excursion to Alnwick Castle departs the Sage
Afternoon Tea served at Alnwick Castle
Excursion arrives back at the Sage
Presentation Sessions: Multicentre Experience
Coffee Break on Hall 1 & 2 Foyer
Presentation Sessions: Sound Systems
Excursion to Alnwick Castle departs the Sage
Afternoon Tea served at Alnwick Castle
Excursion arrives back at the Sage
Hall One Hall Two
Accompanying Persons Programme
11 Conference Programme
The Angel of the North, Durham Cathedral and the Bowes Museum
Date: Thursday 6 JuneTime: 09.00Pick-up/ drop-off point: The Sage GatesheadReturning: 17.30
Visit the iconic Angel of the North, the symbol of the North East as you make your way to the historic city of Durham. This statue, rising 20 metres from the ground, dominates the skyline. Made from 200 tonnes of steel and with a wingspan of 54 metres it is an experience not to be forgotten.
Next stop on the tour is Durham, a picturesque University town, home to the world renowned Durham Cathedral and the World Heritage Site of Durham Castle.
You will be invited to take a guided tour of this Romanesque Cathedral which will include the shrines of St Cuthbert and the Venerable Bede.
A scenic drive through County Durham leads to The Bowes Museum in the market town of Barnard Castle. Housed in a majestic, French-styled building and commissioned by John and Josephine Bowes this museum has been described as the ‘Victoria and Albert Museum of the North’. The impressive collection includes French, Spanish and Italian art, tapestries and porcelain. The prize exhibit is the exquisite mechanical Silver Swan, a work of art much loved and admired by generations of visitors to the museum.
Hadrian’s Wall and Hexham
Date: Friday 7 JuneTime: 09.00Pick-up/ drop-off point: The Sage GatesheadReturning: 17.30
Visit some of the best preserved remains of the Roman occupation of Britain. Built almost 2000 years ago by the Emperor Hadrian, the wall serves as a permanent reminder that this was the North West frontier of a vast and powerful Empire.
Whilst visiting the wall you will also have the opportunity to visit Chesters Roman Fort which is considered to be the best remains of a cavalry fort in Great Britain. A guided tour will be provided.
The tour will culminate in a visit to Hexham where you will be able to spend the day exploring the town and its abbey.
For those of you who are accompanying a delegate to OSSEO 2013, we have arranged an exciting programme of events to keep you busy during conference hours.
We would also like to invite you to the Wine Reception and Conference Banquet, they key social events taking place around the symposium
If your accompanying person does not yet have a ticket for the reception or dinner, these can be purchased at the regisitration desk

Keynote Speakers Keynote Speaker
Biography
Dr. Isabelle De Groote’s research interests include palaeoanthropology, evolutionary anthropology, functional morphology, evolutionary anatomy, human variation, adaptation, primate morphology and biological anthropology. She is currently working with Dr Louise Humphrey (Human Origins Group, Department of Palaeontology), at the Natural History Museum, on a project that has the goal to analyse and interpret the newly discovered excavation notes from Taforalt Cave. This will be combined with the data Isabelle collected on the skeletal collection. The results and publications will provide a background for future grants to expand the work on DNA and stable isotope studies of the Epipalaeolithic in the Maghreb.
Synopsis
In this talk we will explore how humans evolved and what the role of the bones of the ear are in disentangling the story of how we became human.
As palaeoanthropologists, we endeavour to explain how humans evolved and more importantly, what it means to be human. Because of the lack of soft tissue preservation we work only with fossilised bones to help us reconstruct human evolution. It is for this reason that we explore every bone in the body to see what information it holds: not only do the bones of the ear tell us about the evolution of the ability to hear the human voice and to use language but they also give us information on how our brains developed and how we evolved to be balanced when habitually walking on two legs – something only humans do.
Dr. Isabelle De Groote
Keeping an ear out for our fossil ancestors
Post Doctoral Researcher, Palaeontology Department, The Natural History Museum
13 Key Note Speaker

Keynote Speaker
Biography
Dr. Bill Hodgetts is an Associate Professor in the Department of Speech Pathology and Audiology at the University of Alberta. He has a joint appointment with the Institute for Reconstructive Sciences in Medicine (iRSM), as program director of Bone Conduction Amplification. He obtained his B.A. in Psychology and his M.Sc. in Audiology at the University of Western Ontario. He received his Ph.D. in Rehabilitation Sciences at the University of Alberta. His research involves developing and refining the prescription, verification, and validation of bone anchored hearing aids.
Synopsis
The talk will contain a history objective measure of Bone-Anchored Devices. Current methods that we recommend to verify devices. The talk will cover how the technology is used in the Lab and how it can be used clinically by all BAHD audiologists. And why this is important:. We have been working for a few years of developing a generic prescriptive rationale for BAHD that can be used regardless of manufacturer. The study presented will be a comparison of frequency responses within each of the manufacturer’s devices. Cochlear and Oticon both have proprietary prescriptive rationales within their software and we will compare outcomes with those proprietary fittings to the outcomes from a generic fitting rationale. It will be very important for audiologist to learn about the prescription and verification aspects that are now possible with each of the companies devices.
Dr. Bill Hodgetts
Prescription and Verification of Bone Anchored Devices: A Comparison Trial
Program Director, Bone Conduction Amplification, Institute for Reconstructive Sciences in Medicine, University of Alberta/ Covenant Health/ Alberta Health Services and Associate Professor, Department of Speech Pathology and Audiology, Faculty of Rehabilitation Medicine, University of Alberta, Edmonton, Alberta, Canada.
14 Key Note Speaker
Keynote Speaker
Biography
Stefan Stenfelt is currently professor and head of technical audiology at Linköping University in Sweden. He is a trained biomedical engineer (M.Sc. EE) from Chalmers University of technology where he also received a PhD in 1999. After his PhD on bone conduction physiology he spent a couple of years at Stanford University working on sound transmission in the human skull. Stenfelt has published extensively in the area of bone conduction and has 40+ journal articles, several book chapters, and numerous conference contributions in the area. Beside his interest in bone conduction, Stenfelt’s research interests include hearing diagnosis, hearing physiology, hearing aids and cognitive hearing science. Stenfelt shares his time between university and the hearing clinic and is senior researcher at Linnaeus Centre for Hearing and Deafness.
Synopsis
The talk will focus on the ability to use binaural cues for better speech perception when bone conducted sound is applied bilaterally. Data from 30 subjects where we have measured spatial release from masking and masking level difference for speech stimuli for both BC and AC stimulation. Data on precedence effect, inter-aural level difference discrimination and inter-aural time difference discrimination that can give theoretical insight to the difference between binaural hearing with AC and with BC. The talk will focus to a large extend on the benefits for BAHA subjects to use bilateral fittings and also the importance of the position for the BAHA implant in the skull.
Prof. Stefan Stenfelt
Binaural hearing with bone conduction stimulation – what is possible
Professor and Head of Technical Audiology, Linköping University
15 Key Note Speaker

Fringe Event Sponsor
Starkey Laboratories are global leaders in hearing technology and innovation.
Exclusively to the UK market place, Starkey are delighted to offer specialist bone conduction solutions in both a spectacle aid and headband format which offer an alternative option for patients who may require or prefer a non-surgical alternative.
Sponsors
Platinum Sponsor
Cochlear is proud to be a sponsor of OSSEO 2013 and have the opportunity to showcase new possibilities for bone conduction patients. Not only are we celebrating 100,000 Baha® users at the conference, we are also introducing two new bone conduction implant systems. The Baha 4 Connect System, including the truly wireless Baha 4 Sound Processor and recently released Baha DermaLock™ Abutment (BA400), provides patients with wireless freedom and soft tissue preservation. We are also excited to present the Baha 4 Attract System that sets new standard for transcutaneous
hearing performance, wearing comfort and simplicity.
Gold Sponsor
At Oticon Medical we combine more than a century of experience in audiology and sound processing with decades of pioneering experience in hearing implant technology. Our “People First” philosophy is a direct heritage from Oticon. Every product we create – from sound processors and surgical components to fitting, counseling and support tools – is designed with user needs in mind. With a strong focus on creating lifelong patient outcomes, our starting point will always be the patient’s everyday challenges and how to overcome them. We aim to empower all users of hearing implant systems to realize their full potential and live life to the fullest.
16 Sponsors
Exhibitors
Interacoustics - Exhibitor
Interacoustics launches the SKS10 Skull Simulator, the world’s first device to perform technical measurements on bone anchored hearing instruments. Compatible with all Ponto and BAHA devices, SKS10 simulates the mechanical impedance of the head to allow accurate measurement of how the bone anchored device is performing.
Phonak - Exhibitor
Phonak’s goal is to improve the quality of life of people with hearing loss. Phonak is the innovative force in hearing acoustics. With our creative solutions, we strive to overcome technological limitations - so that all people are able to hear, understand and fully enjoy life’s rich landscapes of sound.
Sophono - Exhibitor
Sophono, Inc. is a Colorado, USA-based medical device manufacturer specializing in abutment-free, implantable, bone conduction hearing systems. Sophono leverages an uncomplicated surgical procedure with a third-generation sound processor to offer a technologically and cosmetically superior system. The innovative approach utilizes a removable external sound processor secured by surgically-implanted magnets.
Otometrics – Exhibitor
Otometrics is the world’s leading manufacturer of advanced hearing assessment and verification equipment for audiology. Specialising in integrated solutions for complex patients Otometrics has recently launched several major new innovations to provide clinicians with unprecedented opportunities for the testing and verification of patients with cochlear implants and bone anchored devices.
Ear Shop
EarShop was established in 2013 by a family of Audiologists and is managed by Nina Reade, Audiological Scientist. After much experience in public sector implementing a National programme a gap was noticed for patient care. Implants were provided but not accessories. Patients didn’t know where to obtain them. A full range of services are available from our Clinic at 78 Eccles Street, Dublin we also have an online presence.
Auditdata - Exhibitor
Auditdata develops innovative and user-friendly solutions for audiology. AuditBase System is the preferred patient management system for public audiology clinics in the UK. It includes a cutting-edge OtoSurgery module, where you can collect core data for the patient surgery and research purposes and take advantage of audiometry specialism features
Osstell - Exhibitor
Today more than 10 000 clinicians all over the world use the Osstell ISQ to diagnose their implants. Especially valuable when treating patients at risk and trying to reduce treatment time. Osstell AB is based in Gothenburg Sweden where we develop, manufacture and market our products globally.
The Ear Foundation – Exhibitor
The Ear Foundation brings together experts in the latest hearing technology, and in the development of communication & language.
We provide services throughout the UK, Internationally and online.
Hearing loss has a huge impact and technologies can transform the lives of deaf children, young people & adults but only with support.
Sonitus Medical – Exhibitor
Sonitus Medical Inc. is a privately held medical device company that markets the SoundBite hearing system, the world’s first hearing and communication solution that imperceptibly transmits sound via the teeth. Relying on the principle of bone conduction, this nearly invisible ITM (in-the-mouth) hearing device is simple and non-invasive
ENT & Audiology News – Exhibitor
ENT & audiology news is a unique bi-monthly publication combining first class articles, conference news, book reviews, journal reviews and information on the latest product and company developments from every aspect of ENT and audiology. Our circulation averages 17,100 in over 140 countries, making us a truly world-wide publication.
17 Exhibitors

Oral Abstracts - Outcome MeasuresThursday 6 June
13:30 - 14:45
Hall One
19
Subjective benefit following the addition of a second
BP100 softband TM processor for children with
bilateral conductive hearing loss.
Introduction:
Since the introduction of the Baha softband TM in 2002 the need for early surgical intervention has been eliminated until the child is of sufficient age and size to allow for successful implantation. Traditionally children with a bilateral conductive hearing loss (BCHL) have been fitted with a headband with only one bone conductor, however recent studies on adults have demonstrated that bilateral bone conductors provide the patient with a sense of direction. This study aims to establish whether there is any additional benefit for a child with a BCHL to have the addition of a second sound processor.
Method:
15 children were identified with a BCHL currently using a Baha Softband TM with a unilateral BI300 sound processor on the poorer hearing side for more than 3 months. All carers (and/or children) completed validated questionnaires before the fitting of a bilateral BI300 Baha Softband TM These validated questionnaires were repeated following both a three month and six month period of bilateral Baha Softband TM use. Questionnaires used included: Infant-Toddler Meaningful Auditory Integration Scale (ITMAIS), Glasgow Children’s Benefit Inventory (GCBI) and Children’s Home Inventory for Listening Difficulties (CHILD)
Results:
A significant subjective improvement was identified in all children following three months using a bilateral Baha Softband TM. Further assessment at six months demonstrated a sustained improvement with the addition of the second BP100 processor.
Conclusions:
All children with BCHL should be fitted with a headband with bilateral bone conduction devices. The practice of using a unilateral bone conduction device in these children should be discouraged.
Rupan Banga
Anne Child
Andrew Reid
Ann-Louise McDermott

20
Bone-Anchored Implantation Outcomes
and Complications: The University of Miami
Experience
Introduction:
Bone anchored implantation is an effective treatment for various forms of hearing loss. As experience with this treatment option grows, institutions have seen an evolution in the manufactured devices, surgical techniques, and evaluative measures. This study investigates the combined experience in bone anchored implantation at a tertiary care academic medical center over a ten year period.
Method:
A retrospective review of all patients undergoing bone anchored implantation at the University of Miami Ear Institute from 2003-2012 was conducted including adult and pediatric patients. Demographic information, surgical details, complications, preoperative objective measures and audiologic outcomes were reviewed.
Results:
A total of 144 patients were identified during the study period. The mean age of the population was 53 years, including 12 pediatric patients. The majority of patients were primarily English speakers (84.1%) with 59 (41%) male patients and 85 (59%) female patients. The majority of devices were Cochlear BAHA (76.9%), followed by Oticon Ponto Pro and Sophono. For those patients completing testing, the mean postoperative aided SNR loss was 3.6 dB, median 2.5 dB. The rate of complications for the cohort is reviewed, including extrusions and patient-directed abutment removals.
Conclusion:
Bone anchored implantation can provide useful hearing rehabilitation for patients with a variety of conditions. It remains a safe treatment option with a minimal rate of major complications, and a low but not insignificant incidence of minor side effects.
Daniel Jethanames
Hilary Snapp
Simon Angeli
Fred Telischi
Long-term quality of life assessment in patients
with auricular prostheses
Introduction:
To investigate quality of life of people with an auricular prosthesis.
Method:
A retrospective case series study was conducted. Quality of life was evaluated by an open-ended question form and three questionnaires: the Glasgow Benefit Inventory, the Rosenberg Self-Esteem scale and the standard Medical Outcome Study Short-Form 12. The occurrence of peri-implant skin reactions (defined by Holgers), along with fixture stability and prosthesis data, were evaluated in 29 implants from 10 patients. The follow-up period varied between several months and more than 17 years.
Results:
The three questionnaires showed an improvement in quality of life scores for all patients, and all patients would recommend the prosthesis. Skin reactions that needed treatment (i.e., Holgers grades 2-4) were seen in 6.2% of all observations; 44.8% of the implants demonstrated either no reaction at all or redness only around the implant. A significant correlation was found between the Rosenberg Self-Esteem score and the number of prosthesis replacements.
Conclusion:
In general, patients seemed to be satisfied with the auricular prostheses, which did improve their quality of life. Furthermore, the quality of life was enhanced with higher quality prostheses and with proper hygiene to prevent skin reactions.
21
Myrthe Hol
Hanneke Kievit
Godelieve W.J.A. Verhage-Damen
Koen J. Ingels
Emmanuel A.M. Mylanus

Patient perceptions and experiences of living with a
Bone Anchored Hearing Aid (BAHA).
Introduction:
BAHA has been shown to be an effective audiological intervention however there is very little evidence to show what it is really like to live with a BAHA. The aim of this investigation is to provide a patient voice of what is happening within the BAHA community using a qualitative research methodology to allow for a better understanding of the perspectives and experiences of people living with BAHA.
Method:
6 purposively selected BAHA users are interviewed in their own homes to provide a rich, detailed description of how things are experienced by BAHA users first hand, described in their own words. The focus of the interview is unstructured and open ended, with the patient leading the direction and topics covered during the interview. The interviews are audio recorded and transcribed at a later date to allow data analysis of the results.
Results:
This investigation provides an in depth description of the lived experience of BAHA users and will present clinicians and researchers with a new insight into their individual perspectives, from the patient’s point of view.
Conclusion:
By identifying BAHA user perspectives on help seeking and the clinical encounter we will be able to identify key aspects of our service delivery and consider changes that are deemed necessary. We will also be able to consider the relevance of current outcome measures and thus improve future patient care. Qualitative research has the ability to generate new information that may otherwise be overlooked.
22
Suzanne Marley
Ian J M Johnson
BAHA - experience of World Hearing Center,
Kajetany, Poland
Aim:
The aim of the study was to compare hearing thresholds of classic bone conduction hearing aid, previously used by patients, to BAHA.
Method:
Our method of choice of treatment of hearing loss in patients with different malformations of the ear is implantation of titanium fixture and installation of abutment with subcutaneous tissue reductions (without taking skin-graft). It was done as a one-stage procedure in adults, good bone quality and uneventful surgery or as a two-stage procedure in patients with poor bone quality and small children. After surgery the fixture was allowed to integrate for a period of 3-4 months before the sound processor was fitted (BAHA BP100; BAHA Divino, BAHA Compact or BAHA Classic 300). After one and six months of using the sound processor full audiometric tests were made. Our material contents 115 patients with conductive and mixed hearing losses including 69 children from 3 year of age (with congenital malformations) and 46 adults up to 60 year of age (most of them with acquired defects).
Results:
The acoustic results are good and constant. In our patients opinions there is better sound quality, higher comfort and cosmetic appearance with BAHA comparing it with the previous aid. Level of benefit is based on prepared by our team questionnaire. Results of using BAHA system in patients with this indications shown, that is good, from audiological point of view, and comfortable for patients method of treatment.
23
Piotr H. Skarzynski
Maciej Mrowka
Lukasz Olszewski
Henryk Skarzynski

24
Quality of life outcomes bone-anchored hearing
device (BAHD) surgery in children with single
sided sensorineural deafness
Introduction:
In adults with single sided deafness, studies have shown both objective and subjective improvement in audiologic metrics with a bone-anchored hearing device (BAHD). Compared to the adult population, there is less experience of the outcome of using a BAHD in children with single sided deafness. The aim of this paper is to report our experience in a series of children with single sided sensorineural deafness where a BAHD was used for auditory rehabilitation.
Method:
Retrospective case review of eight children (4 male & 4 female) who had BAHD surgery for single sided sensorineural deafness between 2007-2010 in a tertiary referral centre. Outcome measures used included Glasgow Children’s Benefit Inventory (GCBI), Single sided Deafness (SSD) Questionnaire and change in health benefit scores (visual analogue scale).
Results:
All but one of the children showed a positive GCBI score; the child that reported a negative score was due to low self-confidence and self-esteem issues secondary to bullying at school. The results of the SSD questionnaire were generally positive with a mean satisfaction score of the BAHD as 9/10. All the children had an improvement in heath benefit.
Conclusion:
Our findings add further evidence to support patient perceived benefit of a BAHD in single sided sensorineural deafness in the paediatric population.
Jayesh Doshi
Rupan Banga
Ann Child
Rebecca Lawrence
Andrew Reid
David Proops
Ann-Louise McDermott
25
The Development of a National BAHA Registry
Method:
An invitation to clinics across the UK led to a working group to develop a National Registry of users, collecting anonymous information. The decision was made to keep the data collected limited initially to encourage participation and completeness, and ethical advice was followed. The National Registry is a small, focussed database, collecting information including numbers, ages, hearing loss, aetiologies, indications , timings from surgery to placement and long-term useage rates. It provides group data, accessible to all via the website, and provides clinics with their individual data for their own use.
Results:
To date, information has been collected on over 1,500 patients by 7 large participating centres; data will be presented on age at implantation, level and type of hearing loss, typical times to fitting and useage rates. It will provide evidence on the numbers of those being fitted in the group who have unilateral losses.
Conclusion:
In an era of evidence based health-care services which are increasingly financially challenged the need for the continuing and sustained collection of such data, which is readily understood by patients, families, professionals and non-specialists alike is increasingly vital. The National Registry is the first attempt to address this issue. Registry development supported by The Ear Foundation, Cochlear Europe and Oticon Medical.
Sue Archbold
Huw Cooper
Ann Louise McDermott
Marion Atkins

Oral Abstracts - Audio TechnicalThursday 6 June
13:30 - 14:45
Hall Two
27
Bone Conduction Implant (BCI) Technical design
aspects and verification method on the first
patient
Introduction:
The Bone Conduction Implant (BCI) has been developed and recently implanted for long-term use in the first patient. The BCI leaves the skin intact after healing compared with the percutaneous bone-anchored hearing aid (BAHA).
Method:
The BCI consists of an externally worn sound processor, and an implanted unit called the Bridging Bone Conductor (BBC). The BBC contains a passive implant and uses an inductive link for communication similar to cochlear implants. The BCI sound processor has been implemented in an efficient Application Specific Integrated Circuit (ASIC) design. In addition, a nasal sound pressure (NSP) measurement method was used during surgery to verify that the BBC operates properly before closing the incision.
Results:
It was found that the BCI has similar output to the ear level BAHA devices. The output force of the BCI is robust for skin flap thickness range of 2-10 mm. Moreover, it was shown that the NSP measurement on the first patient was a proper method for verification of the implant functionality during surgery.
Conclusion:
The Bone Conduction Implant has been developed and implanted in the first patient and the performance and verification methods show that the implant performs as expected after surgery. The NSP will be used as the verification method during coming BCI surgeries.
Hamidreza Taghavi
Bo Håkansson
Mans Eeg-Olofsson
Sabine Reinfeldt
Karl-Johan Fredén Jansson

28
Hearing analysis in bone anchored hearing aid
device.
Introduction:
Analyzing different aspects: intelligibility, attenuation offered skin in the testing with simulator and fruquency discrimination in B.A.H.A.
Method:
We testing each patient (n:50), by direct connection to the device and masking the contralateral ear if it is necessary, with speech audiometry using lists of words and pseudo-words, with and without the device, comparing the intelligibility by SRT (Speech reception threshold) and SDS (Speech discrimination score). Also we analyze the intelligibility following the procedure SNR to +10dB, 0dB,-5dB, both with white noise, how daily noise (cafetery). Moreover, we compare the values obtained with the percutaneous stimulation with transcutaneous (simulator) by speech audiometry at same intensity and free field tonal. Finally, to assess the discrimination of frequencies we use pairs of harmonic tones 440-349; 440-369; 440-392; 440-415; 440-440; 440-466; 440-493; 440-523; 440-554, and pairs of pure tones for 500Hz (485-515Hz to intervals of 3Hz), 1000Hz (985-1015Hz to intervals of 3Hz) and 2000Hz (1975-2025 to intervals of 5Hz).
Results:
With the device the SRT: 48.03db (58.18db, pseudowords list); without the devices the URV: 86.25. Silent intelligibility was 57,9 %, 84,7 % and 92,1 % for +30, +40 and +50db. Intelligibility in SNR (white noise), +10db:52,35 %; +0db:16,18 %;-5db:2,65 %. In SNR (daily noise), +10db:46,47 %; +0db:32,1 %;-5db:12,1 %. Comparing simulator with final device, we obtain for the same intensity (average 80dB), an intelligibility of 72,1 % and 92.1 % respectively. Frequency discrimination for harmonic tones is 93 %.
Conclusion:
The B.A.H.A provides optimal hearing performance.
Ignacio Pla-Gil
Jaime Marco Algarra
Paz Martínez Beneyto
Ignacia Pitarch
Antonio Morant Ventura
Do higher Compression ratios improve speech
perception for Baha users?
Introduction:
Today, the effect of the compression ratio (CR) and the maximum power output (MPO) of bone anchored speech processors is not well understood. The aim of this study was to compare speech understanding and subjective preferences with different settings of CR and MPO.
Method:
12 Baha users participated in this study. For four consecutive periods of two weeks each, each participant was fitted with a BP110, programmed with two out of a total of 8 settings. These settings were the combinations of four different CR (1.0, 1.3, 1.6, 2.0) and two different MPO (maximal possible MPO, and MPO minus 5 dB). After each 2-week period, speech understanding in quiet and noise was measured. Patients rated their subjective hearing impressions in a diary and chose the preferred setting in the last session.
Results:
For the 4 subjects (33%) with the poorest speech understanding in noise, higher CR improved speech understanding in noise. Other than that, neither speech understanding in quiet nor in noise was found to be influenced significantly by the CR or by the MPO. Subjectively, 11 of the 12 subjects preferred a moderate CR of either 1.3 or 1.6, only 1 subject preferred a CR of 1.0. 9 subjects preferred maximal MPO, 3 MPO-5dB.
Conclusion:
Within the investigated range of values, compression ratio and MPO seem to have little influence on speech understanding. Subjectively, medium compression ratios (1.3 or 1.6) as opposed to no or higher compression ratios (1.0 or 2.0) and higher MPOs are usually preferred.
29
Anja Kurz
Mark Flynn
Tobias Good
Marco Caversaccio
Martin Kompis

Influence of skin attenuation on fitting and speech
understanding with transcutaneous Baha
Introduction:
Transcutaneous bone conduction hearing aids may have several advantages over percutaneous Bahas. There may be lower infection rates and the cosmetic appearance may be better. However, skin attenuation will require a different fitting of the sound processor and may limit maximal effectively available output power and thus influence speech understanding.
Method:
In this ongoing study with 16 experienced Baha users, a magnetic adapter plate is connected to the existing abutment. A standard Baha sound processor is attached to a second magnetic plate. Between the adapter plate and the second magnetic plate, damping material is placed, mimicking the attenuation of the soft tissue between an implanted magnetic adapter and an external worn sound processor. Speech tests in quiet and in noise in aided and in unaided condition are performed. The sound processor is connected through the standard abutment and through the magnetic transmission including three different magnet strengths. Loudness growth, aided and unaided thresholds are measured in all conditions.
Results:
Results from the first patients will be presented.
30
Anja Kurz
Mark Flynn
Marco Caversaccio
Martin Kompis
31
Benefit of the fixed directional mode of the Baha
BP100 and the Baha BP110
Introduction:
The Baha BP100 and BP110 sound processors feature dual-microphone directional noise reduction systems. In both processors, either adaptive or fixed directional modes can be selected. The objective of both modes is to improve speech-to-noise ratio and thus speech understanding in noisy environments. In 2011, a technical report showed no directional benefit in noise for the BP100 sound processor and challenged the effectiveness of its directional system.
Method:
Four investigations from our department comparing the omnidirectional and the fixed directional mode were analyzed: (1) Speech understanding with a BP100 for speech from the front and noise from the rear (S0N180), (2) speech understanding with a BP110 for speech from the front and noise from the rear, (3) speech understanding with a BP110 for speech from the front and noise from the side of the Baha, and (4) skull simulator measurements of white noise from the front (0°) and from the side (90°) with a BP100 and a BP110.
Results:
In all four investigations, a significant, beneficial effect of the fixed directional mode was observed. In the S0N180 situation, speech understanding in noise was improved, on average, by 2.2 dB for the BP100 and by 1.9 dB for the BP110. For noise from the side, the average improvement was 1.1 dB. Similarly, the skull-simulator measurements clearly show an attenuation for sound from the side.
Conclusion:
So far, all investigations at our department show that the directional multi-microphone noise reduction system of the BP100 and the BP110 are effective.
Anja Kurz
Marco Caversaccio
Martin Kompis

Comparison of multiple-channel nonlinear versus
single-channel linear processing strategies for
osseointegrated bone conduction implants in mixed
hearing loss
Introduction:
Evaluation of directionality of a multiple-channel nonlinear (M-BCI), BAHA BP110, compared to a single-channel linear bone conduction implant sound processor (S-BCI), BAHA Intenso, in patients with mixed hearing loss.
Method:
20 patients with mixed hearing loss were included in the study. For both sound processors aided thresholds and speech perception in noise were measured. Two configurations were used for speech in noise testing: S0N0 and S0N180. The M-BCI was tested in both omnidirectional and directional mode. Patients were fitted with the S-BCI and evaluated 3 weeks later. The M-BCI was fitted and, again 3 weeks later, evaluated. Patients compared both sound processors with the APHAB questionnaire.
Results:
Aided thresholds were poorer for the S-BCI in the high frequency range. In the S0N0 condition, the M-BCI-thresholds were 1.7 dB (SD 2.2dB, p = 0.002) more favorable than with S-BCI. For the S0N180 configuration an improvement of 5.8 dB (SD 2.8dB, p < 0.001) was seen for the directional mode relative to S-BCI. The directional mode of the M-BCI results in an improvement of 1.9 dB (N = 15, SD 1.9dB) relative to the omnidirectional mode (p = 0.003). The APHAB showed statistically significant improvement with the M-BCI on all subscales relative to S-BCI.
Conclusion:
Better speech intelligibility in noise with M-BCI than with S-BCI was attributed to better high-frequency gain provided by the M-BCI. In the S0N180 condition, the directional microphone contributed to better results. Improved signal processing strategies may have contributed to subjective preference for the M-BCI.
32
Jolien Desmet
Arjan Bosman
Ad Snik
Peggy Lambrechts
Myrthe Hol
Emmanuel Mylanus
Marc De Bodt
Paul Van de Heyning
Oral Abstracts - New AbutmentsThursday 6 June
13:30 - 14:45
Barbour Room

Clinical Experience with the New Baha Implant
(BA 400)
Introduction:
Bone achored hearing aid (BAHA) is one of the satisfactory solutions for the hearing improvement of the patients with conductive type hearing loss when conventional middle ear surgeries or hearing aids are out of choice.
Methodology:
The new BAHA abutment (BA 400) offers surgical and audiological advantages. The experience with patients implanted with BA 400 between December 2012 and May 2013 at Hacettepe University Otolaryngology Department is presented. Demographic data, etiology of the conductive type hearing loss, details of the surgical technique and the follow up of the patients are included.
Results:
The outcomes of the operations are discussed in terms of surgical and audiological results.
Conclusions:
The technical improvement of the BAHA implant reveals satisfactory results for the surgeons, audiologists and as well the patients.
34
Gamze Atay
Münir Demir Bajin
Levent Sennaroglu
Mehmet Yarali
Gonca Sennaroglu
Global Experience and Outcomes of the
Cochlear™ Baha ® BA400 Dermalock abutment
using no soft tissue reduction surgical technique.
Introduction:
Recently, pre-clinical studies demonstrated the potential of an hydroxyapatite abutment coating to enable integration between soft tissue and the abutment (a concept called Dermalock). This soft tissue integration enables a significant reduction in peri-abutment pocket formation. Thereby, potentially enabling safe Baha surgery without soft tissue reduction. To further investigate the potential benefits of this technology, the BA400 abutment with an increased concave shape and hydroxyapatite coating was available to a number of facilities for six months.
Method:
In total, data was reported on over 196 abutments from 178 patients (Europe: N=102, Americas: N=76) at >50 centres with reports at surgery, follow-up and then three months post-operative. Data was provided in terms of surgical time, soft tissue depth, surgical technique, abutment size selected, pain and numbness, Holgers grade, and any reported adverse events.
Results:
The results indicated a significant reduction in surgical time combined with no increase in reported Holgers Index or adverse events. The surgical technique was either linear (66.5%) or other technqiues such as to use a punch or C-shaped incision. Importantly, the technique of placing the abutment outside of the incision line provided improved results. The 8mm (45.3%) and 10mm (35.4%) abutments were more common than the 6mm (10.6%) or 12mm (8.7%). All surgeries apart from one were conducted without the need for soft tissue reduction.
Conclusion:
In summary, the data supports the revised approach may result in improved outcomes in terms of surgical time, pain, numbness and cosmetic appeal while not increasing the reported complications.
35
Mark Flynn
Helena Wennaker
Pete Webber

Soft tissue stability around hydroxyapatite-coated
Baha abutments using a simplified surgical
technique
Objectives:
Two animal studies were performed to investigate soft tissue stability around Baha abutments of different designs and materials, placed using a minimally invasive surgical technique without tissue reduction. The first study concluded that hydroxyapatite provides enhanced dermal adherence and significantly reduced pocket depths compared to titanium abutments; the best result was achieved with hydroxyapatite-coated abutments with a pronounced concave shape. The aim of the second animal study, presented in detail below, was to histologically compare soft tissue integration of hydroxyapatite-coated concave abutments and commercially available titanium Baha abutments using a statistically powered sample size.
Method:
Twenty-four hydroxyapatite-coated abutments (test: Similar to CE Marked Cochlear Baha BA400 Abutments) and twenty-four standard titanium Baha abutments (control: Cochlear Baha BA300 Abutments), pre-mounted onto Baha implants (Cochlear Baha BI300), were inserted in the skull of eight adult sheep without performing skin reduction. After a 4-week healing time, implants and abutments with surrounding tissue were retrieved for qualitative and quantitative histology. For statistical comparisons a mixed model analysis was used.
Results:
Qualitative histological assessment showed healthy soft tissues around the abutments with limited or no signs of inflammation. Tight adherence between hydroxyapatite-coated test abutments and surrounding dermis was consistently observed, while less firm adherence was generally noted on control abutments. Morphometric measurements showed significantly smaller pocket depth (p=0.0013) and less epidermal downgrowth (p=0.0003) for test compared to control implants.
Conclusion:
The results confirm that hydroxyapatite-coated concave abutments improves soft tissue adherence and reduces epidermal downgrowth and pocket formation compared to standard titanium Baha abutments. In conjunction with surgery without tissue reduction, soft tissue stability could also be achieved.
36
Mark Flynn
Stina Wigren
Anna Larsson
Marcus Andersson
Ulf Nannmark
New BIA400. Two different surgical techniques
Introduction:
Results of the new implant BA400 comparing 2 different surgical techniques.
Method:
We report 11 cases (8 women and 3 men), of 55 years of average (76-16 years) which etiology in all was chronic otitis media. As audiological data, the average threshold bone conduction is of 41.11dB with average air-bone gap of 34.44Db, they all present a of speech discrimination score > 65 %. Speech reception threshold (SRT): 72.5dB without the device vs 44.67dB with the device. 36 % of the patients had previous hearing aid. We compare two surgical techniques, the first (intra-incision) performed in 6 patients and placing the implant in the same incision. Second technique (extra-incision), performed in 5 patients and it consists of extracting the implant, using a biopsy punch, lateral to the incision that has been sutured before.
Results:
The tissue thickness average was of 6.45mm. The depth of drill was 4mm in all the cases. The average time of both techniques is 25 minutes approximately; none of the patients need subcutaneous tissue reduction. Abutment length was 12mm (4 cases); 10mm (2 cases); 8mm (4 cases) and 6mm (1 case). The number of visits was similar for both techniques, average of 8.09, although the rate of complications and Holgers’s index it was
minor for the extra-incision technique.
Conclusion:
Both technologies offer ideal results comparing with old implant. We prefer the extra-incision technique for fewer complications.
37
Ignacio Pla-Gil
Paz Martínez Beneyto
Ignacia Pitarch
Antonio Morant Ventura
Carmen Bécares
Felip Ferrer Baixauli,

New solutions in BAHA implantology our first
experiences with one-stage FAST surgery of BA400
hydroxyapatite coated implant
Introduction:
The surgical procedure for BAHA implantation has been continuously modified with the aim of improving and shortening it. With the widely used methods, involving soft tissue reduction, as well as in the international practice, so do we have wound healing problems, flap necrosis being the worst case scenario. With these experiences in mind we had been awaited the introduced hydroxyapatite coated BA400 implant, has been designed to allow minimally invasive surgical techniques involving no or minimal soft tissue reduction.
Method:
Being involved in a closed market release we had the opportunity to introduce the new, one-stage, FAST surgical method (placing an implant together with a pre-mounted abutment in one step). On the 12th of October 2012, we have performed 3 implantations on 3 adult patients. Through a retro-supraauricular, approximately 25mm long linear incision, a safe approach could be gained. The under-preparation of only the posterior incision line, provided its sufficient mobilization for a tension-free closure.
Results:
During regular follow ups, according to the Holgers classification, no pathological signs were seen. After 12-16 days the soft tissue was sufficiently healed, so the sound processor fitting could happen. Audiological assessments have been carried out, as well as questionnaires were filled out about the presenting complaints, lacking any significant ones.
Conclusion:
Based on our first experiences the FAST surgery is clearly simpler and easier, involving no or minimal soft tissue reduction. The postoperative healing period is significantly shorter, with less complication rates, however the provided improvement in hearing performance is still great.
38
Laszlo Rovo
Janos Jarabin
Ferenc Toth
Jozsef Geza Kiss
39
Evaluation of the Cochlear BA400 abutment in
reducing the frequency of skin reactions
Introduction:
Soft tissue reaction is the most common complication of the osseointegrated auditory implant. A hydroxyapatite (HA) coated abutment (BA400) was developed by the cochlear corporation in an attempt to reduce the incidence of soft-tissue reactions in percutaneous implants. The purpose of this study is to evaluate the efficacy of hydroxyapatite abutment coating in reducing soft tissue complications.
Method:
A multi-center prospective study of 100 participants that underwent osseointegrated auditory implantation with the BA400 abutment are included. All patients had linear incision with minimal to no subcutaneous tissue dissection. The surgery time, soft tissue thickness, abutment length, and incidence of post-operative soft-tissue reactions are measured using the Holger’s grading scale. Data was collected at surgery and at 1, 3, 6, 12, 24 weeks following implant/abutment placement.
Results:
78 patients (73 adults/5 pediatrics/1 bilateral) have been implanted so far with no loss of implant or revision surgery required. Complete analysis of the results will be presented.
Conclusion:
The preliminary findings reveal that operative time is reduced by 50% when using the hydroxyapatite coated abutment without soft-tissue dissection. The long-term effectiveness of the HA coating in reducing soft tissue complications requires further investigation.
Jack Wazen
George Poulos
Julie Daugherty

Oral Abstracts - Paed LoadingThursday 6 June
15:15 - 17:00
Hall One
41
Evaluation of the stability of bone anchored
hearing implants in children.
Introduction:
Successful implantation requires good implant stability at the time of the initial surgery and this must be maintained over time. Knowledge of osseointegration in children is not well understood and they present a wide variety of different challenges to the clinician.
Aims:
To measure the stability of the BI300 implant in accordance with the current two stage surgical procedure. Implant Stability Quotient (ISQ) values used.To monitor the peri-abutment (BA300) soft tissue status using the Holgers Classification.
Methods:
ISQ measurements were taken at fixtures/sleeper level at the first and second stage of surgery. ISQ measurements from the abutment were recorded at second stage surgery, “loading”™, 2, 3, 6 and 12 months post loading.
Results:
25 children were implanted with the BI300 implant system and BA300 abutment between January 2012 and December 2012 High ISQ values were identified at fixture level at the time of surgery in all children with adequate bone thickness and no significant increase at the second stage. Very thin bone had low ISQ values but a significant increase was recorded at the second stage of surgery. One traumatic fixture failure occurred. Two children had a Grade 3 soft tissue score.
Conclusions:
There was no obvious difference between the ISQ of either of the implant systems used. Following a 12 week period of osseointegration there did not appear to be a significant difference in the ISQ value from the time of initial surgery in children with sufficient bone thickness. Those children with very thin bone thickness had a very stable implant with appropriate ISQ values more than 6 months post loading.
Konstance Tzifa
Andrew Reid
Ann-Louise McDermott

Does the BAHA stability change in different age
groups?
Introduction:
The osseointegration of BAHA(bone anchored hearing aid) can be influenced by a number of factors including the patient’s age as the rate of bone metabolism changes. The purpose of this study was to assess whether there is any change in the stability of BAHA in patients of different age groups in the adult population.
Method:
The Osstell RFA(resonant frequency analysis) recording device measures the resonance in a magnetic field of a 1 cm commercially manufactured attachment(Smartpeg) that is screwed onto the BAHA abutment. RFA measurement was obtained intraoperatively, and converted into implant stability quotient(ISQ). Patients were fitted with CochlearTM BAHA BI300 series using a one stage procedure. Data was collected prospectively over a period of 21 months.
Results:
A total of 215 consecutive cases were included in the study. The age range was from 21 years to 84 years, with the mean and median age of 55 years. The mean ISQ ranged from 64.1 to 66.25 in different age groups. No statistically significant difference was detected between the over 60 years group and the under 60 years group.
Conclusion:
As there is no significant difference in the abutment stability, the same BAHA loading schedule can be used for the adult patients in all age groups.
42
Jayesh Doshi
Rupan Banga
Anne Child
Konstance Tzifa
Andrew Reid
Ann-Louise McDermott
43
The Role of Stability Measurements of the Baha
System in Children
Introduction:
Bone conduction implant (e.g. Baha(R)) stability can objectively be measured over time using radio-frequency analysis (RFA). Adult studies suggest that the Cochlear(TM) Baha(R) BI300 Implant may be loaded as soon as the soft tissue wound is healed. We aimed to assess implant stability in children using RFA measurements.
Method:
Consecutive children having a Cochlea(TM) Baha(R) BI300 Implant had RFAs taken peri-operatively, 1 week post-surgery, within 3 months of surgery and then subsequently at least 3 monthly. RFAs were also measured at loading of the hearing processor and at 1 week post-loading. Our standard practice has been to load the implant at 3-6 months post-operatively.
Results:
9 children had 10 Cochlear(TM) Baha(R) BI300 implants (8 unilateral and 1 bilateral) with a mean age of 9 years 4 months (4 years 9 months to 13 years 5 months). The mean time to loading of the hearing processor was 3.3 months (3 to 5 months, n=9). Mean follow up was 9 months (6 weeks to 23 months). Peri- and post-operative RFA measurements will be discussed with 6 children having RFAs sufficiently high for hearing processor loading much earlier post-implantation. Implant stability was maintained after loading with the hearing processor.
Conclusion:
This study indicates that a larger study is warranted to evaluate both the role of sequential RFA measurements in the timings of Baha(R) hearing processor loading and the possibility of loading at 4-6 weeks in selected children. Subsequently RFA measurements may also be used to decide between single- and two-stage surgery.
Mark Felton
Penny Feltham
Rachel Andrew
Iain Bruce

Early Baha implantation in children: the 16-year
experience of a tertiary care referral center
Introduction:
Baha surgery can be performed in very young children, providing they have sufficient skull thickness. Strategies adopted in order to lower implant age include two-stage surgery and the use of bone augmentation techniques. The present study reports on the experience of Bambino Gesù Children’s Hospital, a large referral center for pediatric disease, on early Baha implantation in children.
Method:
The clinical records of children undergoing Baha surgery in our Institution from 1996 to 2012 were reviewed. Data concerning surgery, fixture stability measured by means of Resonance Frequency Analysis at abutment level, complications and functional outcome were considered.
Results:
52 children were implanted (mean age at implant = 8.3 ±6,8 years, age range = 3-17 years). Surgery was performed with 3-mm fixtures in 45 children. 20 subjects received single-stage (group I) and 32 two-stage Baha surgery (group II). Bone augmentation techniques were used in 6 children in group II. Age at implantation was significantly lower in group II (6.8 ±4 years) than in group I (9.8±3.4 years). The complication rate, stability at 1 year follow-up and functional gain did not differ significantly between the two groups.
Conclusion:
Early Baha implantation can be safely performed in young children, both as a two-stage and as a single-stage procedure. A two-stage surgery and bone augmentation often allow implantation of subjects with thin skulls and under 5 years. However, single-stage surgery with a 3-mm fixture should be chosen whenever possible in order to provide patients with earlier auditory rehabilitation and spare them one surgical operation.
44
Pasquale Marsella
Alessandro Scorpecci
Concettina Pacifico
45
Evidence For Early Loading of Osseointegrated
Implants for Bone Conduction at Four Weeks
Introduction:
The purpose of our study was to directly measure the stability of the Baha abutment using Resonance Frequency Analysis (RFA) and to report on the change in stability over time for implants loaded 4 weeks post-operatively.
Methods:
The principle behind RFA is to obtain a numerical value relating to stability âthe implant stability quotient (ISQ). An Osstell recording device was used to obtain the ISQ measure which is the resonance in a magnetic field of a 1 cm commercially manufactured attachment (Smartpeg) screwed on to the abutment. ISQ measurements were obtained at surgery, 1 week, 4 weeks and 16 weeks post implant surgery.
Results:
Prospectively sixty-eight consecutive patients were recruited with a male to female ratio of 23:45. Nineteen patients had bilateral Baha devices fitted giving a total of 88 implants. The average ISQ change (delta) for the cohort gives a value of 0 at time of surgery. The change in ISQ at 1 week was - 0.10 (95%CI= 0.74), at 4 weeks was 1.21 (95%CI= 0.59), and at 16 weeks was 1.60 (95%CI= 0.77).
Conclusion:
Successful early loading of the baha sound processor has been achieved. RFA provides a reliable means of assessing stability for loading and measuring implant stability in the longer term. This data supports the evidence for early loading at 4 weeks with good clinical safety.
Claire McLarnon
Ian Johnson
Tom Davison
John Hill
Beverly Henderson
Denise Leese
Suzanne Marley

46
Evaluation of Baha implant stability in children.
Introduction:
To measure the stability, as determined by Implant Stability Quotient (ISQ) values, of Baha implants placed according to the protocol for FAST (one-stage) surgery in children. Early sound processor fitting in children based on the skin reactions evaluation and obtained ISQ values at 8 weeks after implantation.
Methods:
In an open, prospective study 10 children with Baha implant were included. Implant stability quotient (ISQ) values were recorded using resonance frequency analysis at the time of implantation and at 10 days, at 8 and 12 weeks, and at 6 months after surgery. Skin reactions were evaluated according to the Holgers classification. Sound processor fitting was performed from 8 weeks after implantation.
Results:
Mean ISQ values, measured in children with Baha BIA300 Implant 4 mm between 0 and 6 months were compared to the published results of obtained ISQ values with the same type of implant in adults. These results combined with the observation of skin reactions according to Holgers classification allowed for early sound processor fitting in children. No reduction in mean ISQ values was observed after implant loading.
Conclusion:
The level of osseointegration reached with the implants in children similar values as in adults at 8-10 weeks after implantation. This was sufficient to support the sound processor.
Jozef Mierzwinski
Maria Drela
Piotr Laz
Maturation of Skull Properties: Implications for Soft
band Bone-Anchored Hearing Systems
Introduction:
The objectives of this study were to investigate: (i) mechanical impedance of the skin-covered skull for infants of different ages and adults, and (ii) transcranial attenuation of bone-conducted (BC) stimuli. It is well established that there are frequency-dependent infant-adult differences in physiological BC thresholds yet little is known about the mechanisms responsible for these differences. Understanding the properties of the infant skull is critical for optimal fitting and verification of soft band bone-anchored hearing systems (BAHS).
Method:
Participants were 0-1, 1-2, 2-4, and 4-7 years of age and adults. Mechanical impedance was measured with BCAL software using a BAHS transducer, B&K 8001 impedance head, and custom-designed holding device for a 100-10,000 Hz frequency sweep. Transcranial BC attenuation was estimated by comparing sound pressure in the ear canal for 500-4000 Hz stimuli presented at a temporal bone (ipsi- and contralateral to test ear) and forehead placement.
Results:
For frequencies below 1000 Hz, significant infant-adult differences in mechanical impedance magnitude were noted for infants 0-4 years of age. No age-related differences were found in impedance above 2000 Hz. Averaged across frequency and position, transcranial attenuation was greater infants 0-2 years of age compared to adults. All children 1-7 years of age showed greater attenuation from the forehead-to-ipsilateral mastoid compared to contralateral-to-ipsilateral mastoid, whereas adults showed no differences in attenuation.
Conclusion:
These findings suggest that infant-adult differences in skull properties contribute to differences in BC sound transmission, factors that should be considered when developing BAHS fitting protocols for infants.
47
Susan Small
Allison Mackey
Bill Hodgetts

Early Loading of Osseo-integrated Implants for
Bone Conduction in a Paediatric Population
Introduction:
The purpose of our study was to directly measure the stability of the implanted abutment using Resonance Frequency Analysis (RFA) in a paediatric population.
Methods:
RFA provides a numerical value relating to stability- the implant stability quotient (ISQ). This is obtained by measuring the resonance of a smartpeg which is screwed on to the implanted abutment in a magnetic field using an Osstell recording device. ISQ values above 55units may be considered stable for loading. All patients were fitted with the new CochlearTM BahaBI300 series implant using a one-stage procedure and loaded between 1 and 16 weeks post-operatively. RFA measurements were obtained at surgery, 4 weeks, and 16 weeks post implant surgery.
Results:
Prospectively 22 consecutive patients were recruited with an age range of 2 to 16 years, a mean age of 9 years. Eight patients had bilateral Bahas fitted giving a total of 30 implants. Average time to loading was 6 weeks. Average ISQ results for the cohort gives a value of 61units (95%CI=2.03) at time of surgery. At 4 weeks =62units (95% CI=2.97), at 16 weeks =63units (95%CI=3.18). There were no surgically failed implants to date.
Conclusion:
The RFA results suggest that there is immediate stability of the BI300 abutment at the time of surgery and the stability is maintained. This is a novel approach to assessing stability of the implant and provides evidence for safety in earlier loading in children.
Claire McLarnon
Ian Johnson
Tom Davison
John Hill
Beverley Henderson
Denise Leese
Suzanne Marley
48 49
Evaluation of the stability of Baha implants in
children
Introduction:
Successful osseointegration after implant treatment relies on the achievement of good implant stability at the time of surgery and maintained stability over time. Resonance frequency analysis (RFA) is a tool for objectively measuring implant stability. Reports of successful use of Baha implants in children are found, but knowledge about osseointegration in children is very limited. Development of protocols for Baha surgery and sound processor fitting in children of different ages is missing.
Method:
Ten children, aged 2-15 years, were implanted according to a 1-stage or 2-stage surgical procedure without skin-thinning and were followed for 1 year. RFA was measured during surgery and at 4 following time points. The time for sound processor fitting was noted as was any skin or implant complication.
Results:
In younger children more complications than in adults were noted during the first year. Implant loss and skin problems were the most frequent noted problems. RFA could give information of when to load the implant. The stability did not follow the ageing of the developing child.
Conclusion:
It is possible to implant young children with a 1- or 2-stage procedure without skin-thinning, but a frequent follow up is needed during the first implant year. RFA measuring can indicate individual loading, but is different between individuals.
Malou Hultcrantz

Oral Abstracts - SSDThursday 6 June
15:15 - 17:00
Hall Two
Baha or middle ear implant (VSB) in congenital
unilateral conductive hearing loss?
Introduction:
To enable stereophonic hearing, patients with congenital unilateral conductive hearing loss (UCHL) have been fitted with bone-conduction implants. First reports suggested limited audiological benefit. It was speculated that the inevitable cross stimulation played a part, when using bone-conduction stimulation. The application of a middle ear implant (VSB) coupled directly to the cochlea, eliminates cross stimulation and, therefore, might be the better option.
Method:
Five patients with congenital UCHL using the VSB device participated; 1 patient from Antwerp, 2 from Lubeck and 2 from Nijmegen. Directional hearing was studied with the magnetic search coil induced technique. Listeners point a head-fixed laser in the perceived direction of different stimuli with roved bandwidth and amplitudes. For comparison, data from the Nijmegen database were used of patients with congenital UCHL, provided with a Baha device.
Result:
All the patients had unaided scores above chance level, despite roving of the amplitude of the broadband stimulus. Localization of low-pass stimuli was less accurate, indicating that subjects were using monaural spectral cues for sound-localization in the unaided condition. All the patients improved their score with the VSB or Baha switched on. Significant differences between the groups were not found. Conclusions: The results suggest that either cross stimulation is not a main issue or that there are other differences between the devices that play an interfering role, like frequency response and sound processing. These factors are discussed.
Martijn Agterberg
Henning Frenzel
Thomas Somers
Cor Cremers
AdSnik
51

52
Unilateral deafness: Is there a treatment of choice?
Introduction:
There are various treatment options in severe to profound unilateral hearing loss (UHL): no treatment, conventional contralateral routing of signal (CROS) hearing aids, bone-anchored hearing implant (BAHI), or cochlear implant (CI).
Method:
101 patients with severe to profound UHL were examined before and after testing CROS aids and BAHI. CI was recommended if the patients met our inclusion criteria for CI: duration of deafness 10 years, intact auditory nerve. Evaluation covered the subjective assess-ment of the devices (SSQ questionnaire), speech understanding in noise, and localization ability.
Results:
About 25% of the patients were satisfied with their unaided condition and did not want to wear external devices. Patients with significantly lower results with CROS aids and BAHI after 3 week test period of each device, prefered CI. After 12 months of BAHI and CROS aid experience, patients showed a slight tendency to better results with BAHI. CI patients showed significantly better localization ability and speech understanding in noise, compared to Baha and CROS patients after 12 months.
Conclusion:
Comprehensive information about all UHL treatment options as well as testing pe-riods are required. CI offer a significantly best speech understanding and localization ability after 12 months than. BAHI are an alternative option if patients do not meet the inclusion criteria for CI, or if they do not want cochlear implantation.
Susan Arndt
Roland Laszig
Frederike Hassepass
Thomas Wesarg
BAHA’s effect in subjects with unilateral
sensorineural hearing loss
Introduction:
It is estimated that about 2 percent of the Danish population only have hearing in one ear. People with monaural hearing often have difficulties in many situations i.e. hearing in background noise and sound localization. The aim of this study was to explore the effect of a bone-anchored hearing aid (BAHA) on speech perception in noise, localization of sound, and on hearing a speaker from the deaf side in subjects with unilateral sensorineural hearing loss (USNHL).
Methodology:
The Danish version of the Speech, Spatial, and Qualities of Hearing Scale (SSQ) questionnaire was filled in by 15 subjects with USNHL and BAHA. A control group of subjects with USNHL not using BAHA was found in a prior study. Inclusion criteria in both groups were hearing thresholds in the better ear at < 20 dB HL at 250, 500 and 1000 Hz, < 30 dB HL at 2000 Hz, < 40 dB HL at 4000 Hz and > 80 dB HL at frequencies 250-4000 Hz in the poorer ear. Results: No significant differences were found between the group with BAHA and the control group in any of the questions in the SSQ questionnaire.
Conclusions:
When using the SSQ questionnaire to compare a group of subjects with USNHL using BAHA to a control group with USNHL not using a BAHA, the BAHA cannot be shown to have any significant effect positive or negative on speech perception, localization of sounds, or on hearing a speaker from the deaf side.
Mette Braendgaard
Steen Østergaard Olsen
Lars Holme Nielsen
53

54
The Effects of Bone-Anchored Hearing Devices on
Tinnitus in Patients with Single-Sided Deafness
Introduction:
Tinnitus is often reported as disturbing sequela in patients with single-sided deafness. While there is considerable evidence that cochlear implants and hearing aids can improve tinnitus disturbance, there are no published reports on the effectiveness of bone-anchored hearing devices on tinnitus control. The present study investigates whether a bone-anchored hearing device alters the characteristics of tinnitus in patients with single-sided deafness.
Method:
Thirty adult patients with single-sided deafness and tinnitus, who meet candidacy and undergo bone-anchored hearing aid implantation are included in the study. Tinnitus was measured prior to and at 1, 3, 6 and 12 months following fitting of the Oticon Medical Ponto sound processor. The Tinnitus Handicap Inventory (THI), Tinnitus Reaction Questionnaire (TRQ), a Visual Analogue Scale (VAS) for subjective loudness of tinnitus and an abbreviated version of the Tinnitus History Questionnaire (THQ) are used. Psychoacoustic measurements including tinnitus pitch matching for frequency and loudness are also recorded.
Results:
Measurements of the THI, TRQ, VAS etc were submitted for statistical analysis using ANOVA. The final analysis will be presented.
Conclusions:
Based on the preliminary results, it appears that the bone-anchored hearing devices may have limited impact on the characteristics of tinnitus in patients with single-sided deafness. Further investigation is needed.
Jack Wazen
George Poulos
Transcranial attenuation as a measure to predict
the outcome of a bone conduction implant trial
in single sided deaf patients
Introduction:
There is no consensus that transcranial attenuation (TA) has a significant influence on the decision of a bone conduction implant (BCI) candidate to opt for BCI surgery. We aim to verify if the measurement of TA can have a clinical implication in the decision of a single sided sensorineural deaf (SSD) patient after a BCI trial.
Method:
Data of 66 SSD BCI candidates who did a BCI trial with a sound processor on a test band were analyzed. Unmasked bone conduction thresholds between 0.25 and 4kHz were measured ipsi- and contralaterally using a type B-71 bone vibrator pre-implantation and direct bone conduction through the sound processor post-implantation. TA was calculated in all patients.
Results:
28 SSD patients decided to get a BCI after the trial period (BCI+) whereas 39 patients declined BCI surgery (BCI-). TA was higher in the BCI- group at 2kHz (7dB vs. 2dB). Extremely high TA values (Mean TA+1SD) were more frequent in the BCI- group at 0.5 (n=7 vs. n=0) and 2kHz (n=11 vs. n=2). Post-implantation (n=19), TA at 2kHz is, unlike at other frequencies, lower than pre-implantation (-5dB).
Conclusion:
At 2kHz TA was lower in the BCI+ group. Higher TA values were more frequent in the BCI- group. Extreme TA values do seem to play a role in the decision of a SSD patient whether or not to undergo BCI surgery and should therefore be measured in all patients prior to
55
Jolien Desmet
Rajae Bouzegta
Anouk Hofkens
Peggy Lambrechts
Kristen Wouters
Marc De Bodt
Paul Van De Heynins

An investigation into the effect of handedness
and side of hearing loss on the benefit of BAHA
use in unilaterally deaf patients
Overview:
The Freeman implant team are seeking to add to evidence in support of the use of bone anchored hearing aids for unilateral hearing loss. Success with this group of patients is not always as good as we would wish and negative outcomes compromise the availability of treatment for many who would benefit. It was decided to survey Newcastle’s 171 unilaterally deaf bone anchored hearing aid users to investigate whether handedness and side of hearing loss had any significant impact on the benefit gained from the use of a bone anchored processor. The part of the brain responsible for language recognition is normally situated in the left hemisphere for right handed people, however for the left handed population, the language centre may be in either hemisphere or may be spread across both. 171 patients were surveyed, 93 replied and of those 73 were able to provide the necessary information. Left handed to right handed ratio was around 1:9, with 32 left sided and 41 right sided hearing losses. Each patient provided their cause and duration of hearing loss as well as handedness. The Abbreviated Profile of Hearing Aid Benefit questionnaire assessed benefit. Initial findings confirm that, on average, all the groups gained significant benefit from processor use and that left handed, left sided deaf users had the greatest benefit scores. Although numbers of left handed patients are necessarily small, there is the potential that as further patients are added to the series, clinicians will be have another indicator to likely success.
56
Denise Leese
S Marley
T Davison,
I Johnson
57
Evaluation of methods for comparing devices for
unilateral hearing loss
Introduction:
Evaluation of bone conduction devices for unilateral hearing loss (UHL) is complicated by device differences. Microphone locations vary from behind the pinna to in the ear canal. Sound delivery to the skull may be by a module positioned in the ear canal, on an osseointegrated post, over an implanted component, or held against the teeth. The purpose of this study was to investigate the efficacy of methods for assessing the benefits of bone-conduction devices that employ either an osseointegrated post (BAHI) or a dental component (SoundBite).
Method:
Nine adult BAHI wearers with UHL wore either a BAHI or a SoundBite exclusively for 30 days. The devices then were swapped and worn exclusively for another 30 days. Sound-field thresholds, sound localization measures, perception of speech in babble and a benefit questionnaire (APHAB) were administered for each trial period.
Result:
Aided thresholds were better for SoundBite than for BAHI. Compared to the unaided condition, both devices provided benefits for sound localization ability and for speech perception in babble but there was no difference between devices. The APHAB scores were better for SoundBite than for BAHI.
Conclusions:
The most useful performance measures were aided sound-field thresholds for low and medium frequencies, speech perception measures where the target speech came from the impaired side or in front and the interfering babble came from the better-hearing side, and the APHAB scores.
Gerald Popelka
Brian Moore

58
Relation between preoperative and
postoperative speech discrimination and
localisation abilities of unilaterally deaf patients
with bone-anchored hearing systems
Introduction:
Acquired unilateral hearing loss reduces the ability to localise sounds and to discriminate speech in background noise. The aim of this study is to compare preoperative and postoperative speech discrimination in noise and localisation abilities of unilaterally deaf patients using a bone-anchored hearing system (BAHS) on the deaf side.
Method:
So far 17 adult patients have been included in the study. Preoperative unaided and via BAHS at test band aided as well as postoperative aided speech discrimination in noise is measured using the Hochmair-Schulz-Moser sentence test for 3 different presentation conditions. Speech and noise levels were both fixed at 65 dB. Localisation was assessed using an array of 7 speakers at head level separated by 30° azimuth in a frontal semicircle. Stimuli consisted of sentences of the Oldenburg sentence test presented at 65 dB. Postoperative tests were performed 12 months after initial device activation.
Results:
In the most difficult condition, when speech is presented on the deaf ear and noise on the normal-hearing ear, postoperative speech discrimination is significantly better than preoperative aided speech discrimination, and both significantly exceed preoperative unaided performance. However, in the opposite condition postoperative speech discrimination is significantly poorer than preoperative aided speech discrimination, but both do not differ from unaided preoperative performance.
Conclusion:
In the most difficult presentation condition, preoperative aided speech discrimination seems to underestimate postoperative speech discrimination and thus the benefit of BAHS for patients with unilateral deafness. However, preoperative aided speech discrimination might overestimate postoperative speech discrimination in the opposite condition.
Thomas Wesarg
Roland Laszig
Antje Aschendorff
Frederike Hassepass
Susan Arndt
59
Quality of life and quality of sound in different
indications for BAHA
Introduction:
The BAHA is used in certain patients with conductive or mixed hearing loss, as well as in patients with single sided deafness (SSD) to avoid the head shadow effect. Besides audiological results, quality of life (QOL) and quality of sound measurement has recently become more important to evaluate the outcome of BAHA users.
Patients and method:
60 BAHA patients were included in group 1 (conductive / mixed hearing loss). To evaluate QOL the Glasgow Benefit Inventory (GBI), the Nijmegen Cochlear Implant Questionnaire (NCIQ) and the Hearing Implant Sound Quality Index (HISQUI) were used. Questions about BAHA use and change in tinnitus were included. 75 patients with SSD (group 2) were encouraged to try the BAHA headband during 2 weeks and to undergo audiological measurements.
Results:
In group 1 the mean GBI score was 36, the general, social, and physical scores being 52, 9, and 1, respectively. The NCIQ showed improvement in the 6 categories. The mean HISQI score was 146, which means a good quality of sound perception. All patients in group 2 showed a significant improvement in free field audiometry with background noise and the Ling test. Only 20% of the patients were implanted. Tinnitus significantly decreased in both groups. Overall, QOL results were better in group 1.
Conclusions:
The use of BAHA increases QOL in patients with conductive or mixed hearing loss. BAHA has a positive effect upon tinnitus. In spite of objective improvement with the headband, indication of BAHA in SSD has to be individualized.
Lekue A
Lassaletta L
Sánchez-Cuadrado I
Pérez Mora RM
Gavilán J

Oral Abstracts - Surgical TechniquesThursday 6 June
15:15 - 17:00
Barbour Room
61
Optimization of Baha care delivery for improved
patient access and fiscal performance
Objective:
To define the Baha value stream in order to optimize patient flow and to remove non-value added steps in order to provide improved patient access and financial viability for our program.
Method:
Using standard methods of value stream mapping, we identified each component of patient care starting with initial patient contact to the center, time to scheduling appointments with the surgeon and audiology team, the authorization process, surgical supplies and procedure, and follow-up programming. The resources required and costs were calculated for each step. Non-value added (in respect to the patient) steps and services were removed. A future state map was generated balanced with skill-task alignment focused on the proper resources being delivered when needed. Our cost per unit service was calculated after reviewing 32 consecutive cases from our 2012 pool of patients modeling costs with the initial value stream compared to the current process.
Results:
The optimized program allows for patients identified in clinic to be evaluated on a just-in-time basis, completing their assessment and submission for payment authorization in one day. This is reduced from an average of 27 days. The overall Baha program is now profitable and has access for evaluation within one week of inquiry. All Baha care is delivered by audiologists who do CI, hearing aids and diagnostic audiology testing. This removes the need for specialized Baha audiologists.
Conclusions:
This study was effective at creating an optimized program for Baha care delivery that ensured patient access and fiscal viability.
Douglas D. Backous
Heather Lambert
Stacey Watson

62
A novel method to identify cover screw in the
second stage of BAHA surgery using portable
ultrasound scanner
Introduction:
It is sometime difficult to identify the coven screw or cover screw space in the second stage BAHA surgery due to soft tissue and bony overgrowth. This dilemma can result in an incision on the thin skin flap in an inappropriate location; more time of operation and increase chance of post-operative infection.
Method:
In this study, a hand held portable ultra sound scanner was used per-operatively adopting an aseptic method to identify the cover screw during second stage of BAHA surgery in consecutive 29 cases. The hand held probe used in sterile sheath was applied in the horizontal and vertical axis and exact location of underlying cover screw was identified and marked by a skin-marking pen before exploration. We have presented our experience during the evaluation of this new method.
Results:
In the first 3 cases the localisation was slightly off the mark due to the learning curve. However in subsequent 27 cases we worked out the skin marking much more accurately and the localisation was excellent. This method not only confers increased confidence about fixture location to the surgeons but also significantly reduces the surgical time and avoids unnecessary skin flap damage.
Conclusions:
Awareness of this method is paramount for Paediatric Otologists to reduce wound size in staged implant surgery.
Debabrata Biswas
Jaydip Ray
Julia Addam-Williams
A comparison of two Bone Anchored Hearing
Aid (BAHA) surgical techniques
Introduction:
Since 1977, BAHA surgical techniques have evolved from the original Tjellström skin graft to the recent Nijmegen simple linear incision. The various techniques aim to achieve optimal osseo-integration and minimise soft tissue reactions or implant loss. Soft tissue reactions, using these techniques and their variations, have been compared in several studies. Generally, full thickness grafts and pedicled flaps have been associated with high rates of soft tissue reaction (typically 50%). We compare two techniques utilised at Frimley Park Hospital. Technique A utilised a pedicled split skin graft while B used a modified partial thickness pedicled graft.
Method:
A retrospective review of the medical records was undertaken of 20 consecutive BAHA patients using the two separate techniques. 10 patients underwent technique A and 10 technique B. Comparison of soft tissue reaction rates (Holgers classification) and required outpatient follow-up appointments was made between the two. The results were analysed using Fishers Exact test.
Conclusion:
Technique B provided a method yielding relatively rapid healing and less associated adverse soft tissue outcomes. As a result, the number of follow ups required prior to fitting the BAHA is reduced. This has financial implications as less clinic time is required for each patient undergoing the procedure.
63
Sam Cartwright
Da Johnathan
Je Mitchel

Bone conduction improvement after middle ear
ossicular chain reconstruction
Introduction:
middle ear diseases are the most prevalent causes of surgically correctable hearing loss, among them the ossicular chain dysfunctions have most extensive effects on patients hearing. Successful reconstruction of this chain certainly improves the air conduction thresholds and seals the air-bone gap on audiogram. But the effect of this reconstruction on bone conduction, though physiologically expectable has not been yet clarified and only few standard clinical trials, mostly retrospective, have been reported. The goal of this study was to determine the efficacy of ossicular chain reconstruction on bone conduction.
Methods:
In a case control prospective clinical trial study the bone conduction thresholds of speech frequencies were studied in 68 patients before and after middle ear surgery. In order to determine the rate of effectiveness of ossicular chain reconstruction on bone conduction, the patients were categorized in 2 groups. In the first group the middle ear surgery and ossicular chain reconstruction were carried out in the same session and in the second group the reconstruction was postponed to another stage. By using paired-samples t-text the changes of the mean bone conduction thresholds was evaluated for each frequency before and after surgery in each group.
Result:
there was a significant improvement in bone conduction in 1 and 2 kHz frequencies in reconstruction group with a maximum of 9.7 dB in 2 kHz. In non-reconstruction group no singnificant changes was noted in any frequency. Conclusion: improvement of bone conduction after ossicular chain reconstruction is an indicator of its role in this type of sound conduction. Our findings showed changes of bone conduction as a mechanical phenomenon affected by activity of ossicular chain. In other words, BC threshold is not solely influenced by cochlear function.
Farbood Kalantari
Saleh Mohebi
64
Newcastle Bone Anchored Hearing Aid (BAHA)
Surgical Technique
Introduction:
There are several different surgical techniques are available for BAHA surgery. We will describe Newcastle’s way of BAHA together with the advantages of this technique. This method is used for both adult and pediatric patients. Unilateral or bilateral. A general anesthetic is always used. Patients are admitted one hour per operatively and discharged approximately two or three hours after the procedure. The operative site is shaved, and prepped using an iodine solution A template of the abutment is used as a guide for the incision and drilling. Local anaesthetic is administered, this also raises the skin prior to the inverted incision. An inverted incision is the choice of incision for Newcastle. This gives excellent access particularly for revision surgery of post neurological patients. A 4mm drill countersink is used A widening drill is used The abutment is then inserted. A biopsy punch is used in order to create an opening for the abutment. An absorbent suture is used for skin closure. Atticoat and Allevelyn dressings are applied together with a healing cap. stability of the implant is tested. Patients are discharged the same day and are followed up in a dedicated nurse led clinic after a week. This method is quick and reliable which including the operative technique gives the patient a 4-5 hour hospital experience This reliable method of surgical access is used for both primary and revision surgery. The reported complication rates and infection rates are low. This technique is applicable to both adult and pediatric cases.
Megan Brette
65

Punch procedure for BAHA implantation: clinical
outcome compared to the Nijmegen linear
surgical technique
Introduction:
Surgical technique for BAHA implantation has been simplified over the years. The Nijmegen technique, commonly used, is achieved through a small linear incision and has proven its efficacy. A dermatologic biopsy punch has been proposed more recently. We compared the Nijmegen technique to a punch procedure.
Method:
a sample of 17 consecutive patients implanted with a BI300 (Cochlear), were sorted out through the surgical technique used (Nijmegen technique vs punch procedure). In contrast to the Nijmegen technique, the punch procedure did not require a 3-cm skin incision but only a 4-5 mm punch hole, that could be associated with a 2 mm-incision up and down in some cases. No subcutis resection was performed provided that the abutment emerged more than 2 mm from the skin. In other cases, a 1-cm subcutis reduction was done. Nine patients underwent the punch procedure with a 9-mm BI300 abutment. The 8 remaining patients had a 6-mm abutment. All patients had single-staged procedures.
Results:
17 adults (10 women, 53+/-9 yo) were implanted. Mean follow-up was 12 months (ext 1-14). Nine underwent a punch procedure. No removal or change of the abutment was required with the punch procedure vs. 2 for the Nijmegen procedure, but this was not statistically significant (Chi-square=2.55; DOF=1). Some patients needed local care for skin irritation with no significant difference between groups (7 for the punch vs. 4; Chi-square=1.43; DOF=1).
Conclusions:
The punch procedure appears to be both easy and fast with the same results than the Nijmegen procedure.
66
Thierry Mom
Nicolas Saroul
Laurent Gilain
Oral Abstracts - General Friday 7 June
09:30 - 10:45
Hall One

68
Sound localization abilities of unilateral hearing
impaired children and adults fitted with
a bone-conduction device
Introduction:
Sound localization in the horizontal plane requires neural processing of binaural difference cues in timing (ITD) and sound level (ILD). Spectral pinna cues are used for localization in the vertical plane. The binaural cues are absent or weakened in patients with respectively single sided deafness (SSD) or unilateral conductive hearing loss (UCHL). Our data confirm and further extend results of recent studies on the use of sound localization cues in unilateral hearing impaired children and adults.
Method:
Sound localization abilities are investigated with the magnetic search coil induced technique (Bremen et al., 2010). Horizontal and vertical head-movements are recorded. Stimuli consist of broadband (0.5-20 kHz), high-pass (3-20 kHz) and low-pass (0.5-1.5 kHz) noise roved over a large range (45-65 dB SPL).
Results:
In our setup it is possible to demonstrate that for listeners who lack binaural cues, sound level is not an adequate cue. Other listeners (mainly listeners with single sided deafness) are able to use spectral cues for the localization of sounds in azimuth. Listeners with acquired unilateral conductive hearing loss who were fitted with a bone-anchored hearing implant were able to localize sounds on the basis of restored use of ILDs and ITDs.
Conclusions:
We suggest that bone-conduction devices provide successful use of ITDs and ILDs for listeners with UCHL and that relatively good monaural localization abilities of SSD patients are not deteriorated by a bone-conduction device.
Martijn Agterberg
Myrthe Hol
Marc Van Wanrooij
Emmanuel Mylanus
JohnVan Opstal
Ad Snik
69
On the evaluation of a new digital bone-
anchored hearing device
Introduction:
Bone-anchored hearing devices have developed rapidly during the past few years. Digital devices featuring directional microphones, feedback cancellation, and wind noise reduction have shown to be a major improvement over their analogue counterparts. However, users of bone-anchored hearing devices still encounter problems when communicating in everyday situations, in challenging listening conditions, and when communicating with line phones and cell phones. There is room for improvement with respect to reducing feedback and artefacts arising from dynamic feedback cancellation systems, and to reducing sound distortions at medium and high sound levels. Therefore, in this study the performance of a newly developed bone-anchored hearing device will be evaluated relative to that of current digital devices.
Method:
Twenty users with a bilateral conductive or mixed hearing loss will evaluate the efficacy of a newly developed bone-anchored hearing device with respect to speech communication, feedback (suppression), and wireless connectivity. All users have ample experience with a digital bone-anchored hearing device. The evaluation will involve speech perception in noise (SPIN) measures, APHAB and SSQ questionnaires and a proprietary questionnaire for rating speech intelligibility, sound quality, listening effort, and communication abilities.
Results:
The experiments will be carried out during the spring of 2013. Data are not yet available.
Conclusions:
The experiments will finish in May 2013. Conclusions will be presented at the conference.
Arjan Bosman
Ad Snik
Emmanuel Mylanus
Myrthe Hol

It sounds ok until I leave the clinic! The benefits
of introducing the virtual environment into
clinical practice.
Introduction:
Assessing the benefit of a BAHA pre implantation is a challenge for any clinician. Whilst one is able to undertake a battery of tests in the clinical environment and a patient is able to report the degree of subjective benefit of the device in sound treated conditions this rarely reflects the auditory experience on leaving the clinic. Many centres now offer patients a home trial with the BAHA, allowing them to make a personal assessment of the benefit of the device in a situation they are familiar with and currently find challenging. The benefit of this trial is however subjective to each individual and the conditions under which they either choose or gain the opportunity to trial the device. The introduction of virtual test environment (VTE) surround sound systems into Audiology practise now provides the opportunity to assess a patients ability to hear in common environments such as the busy city centre, restaurants, the workplace etc.. by replicating the situation in the clinic room.
Method:
This study reviews the outcomes of 10 patients assessed in clinic using a GN Otometrics surround sound VTE to replicate the auditory and visual conditions usually experienced by a patient undertaking a home BAHA trial. Clinical assessment data and COSI outcomes from 3 patient identified situations are evaluated and compared pre and post home trial demonstrating the benefits of using the VTE in clinic and as a predictor of long term benefit.
Results:
The study demonstrates the the benefits of introducing the VTE into the BAHA clinic as a tool for optimising BAHA set up and predicting outcomes in the real world environments, thus alleviating the need for time consuming and unsupervised home trials. It raises ethical questions about the methods used to assess suitability for BAHA and the questions how robust the home trial is as an accurate means of assessment.
William Brassington
Nicholas Ward
70 71
First clinical outcomes of the Cochlear Baha(R)
Attract System
Introduction:
This paper presents the first clinical outcomes and hearing performance of the Cochlear Baha Attract System from a multi-centre prospective clinical investigation. The Baha Attract system is a passive transcutaneous system where sound is transmitted as vibrations from an externally worn sound processor through the skin to an internal magnet attached to the Cochlear Baha BI300 screw fixture.
Method:
Hearing and surgical outcomes from the first ten (N=10) adult patients who received this new system will be presented. All had either single-sided sensorineural deafness (SSD), or bilateral conductive or mixed hearing loss and were candidates for the percutaneous BAHA system. Data was collected comparing pre- and post-surgical outcomes from measures of aided hearing performance, speech recognition in quiet, and speech recognition in noise. Additionally, data was collected in terms of surgical approach, post-operative healing and subjective reports of benefit.
Results:
Surgical outcomes and hearing performance data will be presented. We will discuss indications for use, sound processor selection and suitability of this new intervention in comparison with percutaneous options.
Conclusion:
The Baha Attract system provides an alternative hearing option for adults with single-sided sensorineural deafness, conductive or mixed hearing loss.
Henrik Smeds
Mark Flynn

72
Audiological results and patient satisfaction with
Baha BP 110 and Ponto Pro Power: Results of a
prospective clinical study
Purpose:
The purpose of this study was to investigate the audiological outcomes and patient satisfaction for two new power bone-anchored devices: The Ponto Pro Power (Oticon Medical) and the BP110 (Cochlear).
Methods:
Patients (N = 10) experienced with bone-anchored devices and with a bone conduction PTA (0.5 - 4.0 kHz) threshold equal or better than 55 dB HL on the implanted side were included in the study. Patients tested the devices in a balanced cross-over design. Audiological outcome was determined by aided threshold, intelligibility of monosyllables (Freiburger) and speech reception thresholds in noise (OLSA, S0N90 or S0N270) for the respective devices and settings (omni- and full-directional mode). The subjective benefits were evaluated by the APHAB, SSQ-C questionnaire and a handling questionnaire which addresses operating the device, occurrence of feedback and annoyance to wind noise. Patients received a fitting of each device according to the manufacture’s guidelines followed by a 3-week period of everyday usage of the device. Audiological and subjective evaluations of the devices were done at the end of each test period.
Results:
Preliminary results indicate similar performance for the two devices in terms of speech intelligibility, but the subjective ratings differ. The study is ongoing, and will be completed in the spring of 2013. The potential discrepancy between objective and subjective data will be discussed.
Conclusion:
Conclusions will be presented at the conference.
Susan Busch
Thomas Giere
Hannes Maier
73
Efficacy in Chinese patients with bilateral aural
atresia using bone-anchored hearing aids
Objective:
To evaluate the efficacy and satisfaction of bone-anchored hearing aids in patients with bilateral aural atresia.
Method:
16 patients with bilateral aural atresia were fitted with soft-band Baha for over 3 months, and then received unilateral Baha implantation using modified surgery technique, when reconstructing the auricle. Mean pure-tone threshold and speech audiometry test results were compared among patients without hearing aid, with soft-band Baha, and with implanted Baha. Scores from the Baha user questionnaire and Glasgow children’s benefit inventory (GCBI) were used to measure patient satisfaction and subjective health benefit.
Results: The mean pure-tone thresholds of the patients were (64.8±5.9) dBHL without hearing aid, (30.2±3.7)dBHL with soft-band Baha, and (20.3±3.9) dBHL with implanted Baha. The differences of the paired comparison were significant (p<0.05). The average decline in pure-tone threshold was (36.2±8.0) dB HL with soft-band Baha, and an additional decline of (12.2±3.4)dBHL was achieved with implanted Baha. The average gain in speech discrimination scores (SDS) were (3.00±1.07)% without hearing aids and(89.39±5.83)% with implanted Baha in sound field of 45dBHL. SDS were (57.55±10.30)% without hearing aids and (91.19±4.16)% with implanted Baha in sound field of 65dBHL. The average gains in SDS were statistically significant tested with 45dB HL and 65dB HL respectively (p<0.05). Sound reception threshold (SRT) without hearing aids were (63.1±5.9<dB HL and (24.7±3.5<dB HL with implanted Baha. The average difference in SRT was obvious (p< 0.05). The Baha application questionnaire demonstrated excellent patient satisfaction. The general benefit score was 35.59±14.35.
Conclusion: Baha remains one of the most reliable methods of auditory rehabilitation and improves quality of life for patients with Artesia.
Xiaowei Chen

Oral Abstracts - Paed SurgeryFriday 7 June
09:30 - 10:45
Hall Two
Peri-operative considerations for children
undergoing bone anchored hearing device
surgery
Introduction:
To identify important factors in the peri-operative management of children undergoing BAHD surgery in a paediatric tertiary centre, placing particular emphasis on co-morbidity and the implications of airway management and anaesthetic technique.
Methods:
Retrospective case note review of all Children undergoing BAHD surgery between January 2008 and January 2011.
Results:
194 children were identified and 134 case notes were available for analysis. 353 anaesthetics were identified. 45.5% of the children had a recognised syndrome or dysmorphism and 17% had a congenital cardiac anomaly. 16% of the children were classed as a grade 3 or 4 laryngoscopy but 83.3% were managed with a laryngeal mask. 11.9% of the children had an intraoperative complication and 4.8% a postoperative complication. 88.4% of children were managed as day cases.
Conclusions:
Children suitable for Bone Anchored Hearing Device (BAHD) surgery are a heterogeneous group, ranging from those with isolated pinna malformations to those children with complex head and neck or cardiac syndromes. They often require multiple operations. As BAHD surgery has become more common and as its indications have expanded, the perioperative management has evolved. The proportion of children with congenital heart disease has remained constant, but there has been a marked reduction in the number of children with syndromes involving the head and neck. We have found that even in complex craniofacial cases, the laryngeal mask is increasingly being used with good results. However, advanced paediatric airway experience was still required in a small number of cases, heightening the awareness that specialised paediatric support services are necessary for a comprehensive BAHD programme
75
Rupan Banga
Andrew Reid
David Proops
Ann-Louise McDermott
Monica Stokes

Age-related Variability in Pediatric Scalp Thickness:
Implications for Soft Tissue Reduction in
Percutaneous and Transcutaneous Bone Conduction
Auditory Prostheses
Introduction:
Soft tissue complications remain the largest disadvantage of Bone Anchored Hearing Aids (BAHA). A move towards minimal soft tissue reduction has been reported due to availability of longer and coated abutments. In addition, new transcutaneous bone conduction options are available where the fidelity of sound transmission will depend on the thickness of intervening soft tissue. Our objective is to examine whether age-related differences in scalp thickness exist and determine whether an age-adjusted approach to soft tissue reduction is warranted.
Method:
Children undergoing BAHA or cochlear implantation underwent 2 scalp thickness measurements, first at the conventional BAHA site (upper) and second, 1.5cm below (lower). Correlation between age and scalp thickness was assessed using the Pearson Correlation Coefficient.
Results:
Measurements from 45 children (age 9 months-17 years (mean 6 years)) demonstrated scalp thicknesses ranging from 2-7mm (lower) (mean= 4.1mm) and from 3-7mm (upper) (mean=4.3mm). A strong correlation was seen between age and both upper (r=0.67; p<0.01) and lower (p=0.84;p<0.01) measurements. A natural division in the dataset occurred at 9 years with children < 9 displaying little variability in scalp thickness and no correlation between age and scalp thickness (r=0.16,p=0.3).
Conclusion:
As a group, scalp thickness varies significantly with age. However children < 9 consistently have scalp thicknesses of 3-4mm. Only after 9 years did scalp thickness begin and continue to increase significantly with age. The lack of variability in scalp thickness in children <9 years does not support the use of an age-adjusted approach to soft tissue reduction in this group.
76
Sharon Cushing
Edward Park
Karen Gordon
Blake Papsin
77
Conventional Bone Conduction Hearing Aids -
Useful as a paediatric clinical tool or not?
Introduction:
At Birmingham Childrens Hospital approximately 35% (n=60) of all children fitted each year with hearing aids are fitted with a conventional bone conduction hearing aid (CBHA). We are using the term CBHA to describe an analogue or digital post aural hearing aid which has been adapted for bone conduction use, whereby the hearing aid is cited contralaterally to the transducer, on either a hard or soft headband. In 2010 a retrospective audit was done to investigate the reasons for CBHS’s being fitted between 1/9/09 – 31/8/2010, as opposed to air conduction hearing aids which are the cheaper option. In 2012, the same patients that were involved in the original audit were re-examined to investigate how many of these patients were still using the CBHA. Of those that were, their subjective evaluation of the hearing aid was obtained via a questionnaire and, of those that weren’t, the reasons for discontinued use were obtained from examination of their audiology records. The results of both audits will be presented in this clinically based presentation, demonstrating that conventional bone conduction hearing aids can be beneficial as an option for children with a conductive hearing loss which is believed to be transient or where BAHA surgery is not imminent.
Sheena Hartland
Konstance Tzifa
Rebecca Lawrence
Theofano Tikka

Bone-anchored hearing aid insertion and
reduction of hearing disability in adults and
children with congenital ear malformations
Introduction:
The bone-anchored hearing aid (BAHA) is increasingly used to take advantage of satisfactory cochlear function in patients with congenital abnormalities of the external and middle ear. This study explores the effects of BAHA insertion on the quality of life in patients with congenital ear malformations.
Method:
Twenty adults and four children with congenital ear malformations were recruited from a tertiary referral centre in the North of England. Participating adults completed a Glasgow Benefit Inventory (GBI), while the parents of recruited children completed the Children’s Glasgow Benefit Inventory (CGBI) following BAHA insertion. Patient demographics, associated diagnoses, post-insertion complications and additional comments were documented.
Results:
GBI scores demonstrated a significant improvement in quality of life with mean scores of +41 and +50 in total and general categories. All patients expressed satisfaction with their BAHAs and parental satisfaction was also noted in the CGBI. There was no excess of complications, particularly with regard to placement and maintenance of abutments, in both adults and children. Three patients reported infections, which were managed simply.
Conclusion:
The BAHA is an important tool in reducing hearing disability in adults and children with congenital ear malformations. All patients in the study described an improved quality of life and a significantly increased level of general wellbeing. This study demonstrates the high level of satisfaction of patients with congenital ear anomalies following BAHA placement.
78
Emma McNeill
Ian Johnson
Tom Davison
Denise Leese
Suzanne Marley
79
Cochlear Implanted Recipient Observational Study
(IROS) of the adolescent patients implanted with the
Baha system in the Children’s Hospital in Bydgoszcz,
Poland.
Introduction:
An assessment of trends in current clinical practices reveal that there is a published evidence of clinically observed benefits from the use of implanted devices providing various types of stimulation in hearing impaired subjects. However the reported data shows wide disparity in clinical experience, clinical practices and the subsequent outcomes. Evident is a distinct lack of patient-related data gathered for prospectively implanted patients including true baseline interval data and subsequent longitudinal follow-up at consistently timed evaluation intervals. Thereofre, an international, multicentre initiative was undertaken with the aim to prospectively, longitudinally compare repeated measures of benefits for implanted hearing-impaired subjects, acting as their own intra-subject control, using the subjective evaluation tools provided via an electronic platform for data entry within a secured environment.
Method:
Evaluations at baseline and annual follow-up for up to 3 years post implant. Evaluation tools include subjective self-assessment scales (SSQ and HUI Mk III), patient profile forms, as well as the hearing threshold measures. Patients were included in the study after the surgery, but prior to the first switch on session.
Results:
This is to present the single centre results inclusive preliminary demographic, epidemiological and the self-assessment data from the baseline evaluation of the adolescent patients with Baha ® system prospectively included in the study since August 2012.
Conclusion:
Data is consistently gathered as a part of the multicentre international initiative in order to provide statistically valid data to support patient management decisions at the clinical, administrative, reimbursement and regulatory levels locally, nationally and internationally.
Jozef Mierzwinski
Maria Drela
Piotr Laz

Surgical and audiological retrospective analysis
of outcomes in paediatric Baha users.
Introduction:
Application of Baha system in patients with conductive, mixed hearing loss or with SSD is widely known and well supported by the literature procedure in adults, as well as in children. Simultaneously, the knowledge about the osseointegration process in children is limited. Especially, the data of implant stability in children is missing. There is also a limited access to data on the audiological results in children. Children with Baha constitue a heterogenous and demanding group of patients in terms of diagnostics. Benefit from the Baha system treatment is conditioned by the osseointegration proces shown by the implant stability results gathered during the surgery and recorded over time.
Method:
The demographic and epidemiological data were recorded. The ISQ data were gathered, as well as audiological results based on the comparison of outcomes with and without the sound procesor. Additionally, the soft tissue and the area around implant were observed according to the Holgers’ scale.
Results:
25 patients implanted under 18 years of age since November 2011 in the Children’s Hospital in Bydgoszcz, Poland were included in the study. Majority of patients (52%) received Baha system as a treatment of SSD. 24% of patients had bilateral conductive or mixed HL and 4 patients suffered from unilateral HL. ISQ values were scored only for those patients with BIA300 (n=7) and on average the result was 69. Audiological benefit from Baha was calculated.
Conclusion:
Most significant audiological benefit from Baha procedure was observed in patients with mixed hearing loss.
Jozef Mierzwinski
Maria Drela
Piotr Laz
80
Oral Abstracts - Implant QuestionsFriday 7 June
09:30 - 10:45
Baubour Room

82
Technical and Research investigations in the
development of the Cochlear Baha(R) Attract
System
Introduction:
In the development of a new transcutaneous Baha system, a number of key technical questions were addressed through feasibility research. These involve (a) efficient transcutaneous sound transmission, (b) determining the optimum retention force, and (c) estimating performance expectations between transcutaneous and percutaneous systems.
Method:
Laser Doppler Vibrometry (LDV) was used to estimate sound transmission to the promontory in a series of cadaver studies. Estimation of the optimum force and pressure for the retention/transmission of the system was determined through a series of experiments. To estimate the hearing performance, a unique test setup attaching a soft tissue model to the abutment of existing percutaneous patients enabled comparison of unaided, percutaneous and transcutaneous transmission.
Results:
The results of the LDV investigation confirmed the transmission advantages of using the BI300 implant as a more effective method of transmission compared to systems that used multiple non osseointegrated screws. The softband measures highlighted the important relationship between force and pressure to ensure good sound transmission, secure retention and to avoid soft tissue complications. The comparison of the system with existing Baha patients determined that it is possible to develop a transcutaneous system with minimal performance loss compared to percutaneous systems.
Conclusion:
The development of the Baha Attract system required a number of fundamental technological innovations and scientific investigations. The result is a system that overcomes many of the limitations of previous systems and provides an alternative to the percutaneous Baha system.
Mark Flynn
Johan Land
Annelen Hedin
Jenny Andersson
Dan Nystrom
Erik Holgersson
Ponto wide implant: A 12-month prospective study
of stability, skin reaction and implant loss.
Introduction:
The new Ponto wide implant is designed with a wider diameter and maximized bone-to-implant contact area. The objective is to investigate the Ponto wide implant considering initial stability, stability over time, implant loss and skin reaction.
Method:
A prospective single-centre study of patients demographic and implant data. The patients were operated with linear incision technique with subcutaneous skin-reduction and followed for one year. At surgery and at all follow-up visits (10 days, 6 weeks, 6 months and 12 month after surgery) implant stability was measured using ISQ. At all follow-up visits a clinical evaluation was made were skin status is assessed and classified according to Holgers.
Results:
Twenty-four adults (25 -71 years) underwent operation and follow up. Fourteen patients have so far been observed for 12 months. The Ponto wide implant showed a good initial stability and a stable ISQ development over time. No adverse skin reactions were observed, and there were neither implant extrusion nor need for skin revision surgery.
Conclusion:
The results revealed a highly stable implant with few skin reactions.
83
Søren Foghsgaard

84
MRI induced torque and demagnetization in
retention magnets for Bone Conduction Implants
Introduction:
Performing Magnetic Resonance Imaging (MRI) examinations of patients using implantable medical devices involves safety risks both for the patient and the implant. Hearing implants often use two permanent magnets, one implanted and one external, for the retention of the external transmitter coil over the implanted receiver coil to achieve an optimal signal transmission. The implanted magnet is subjected to a magnetic torque induced by the MRI scanner. In this paper, the degree of demagnetization and a comparison between measured and simulated induced torque is studied for the retention magnet used in the Bone Conduction Implant.
Method:
The torque has been measured and simulated in a homogeneous static magnetic field of 1.5 Tesla. For the experiment, twelve same size permanent magnets with two different coercive fields were used. The magnetic field was generated by a dipole electromagnet. Demagnetization was measured at 1.5 Tesla by the loss in retention force. For the simulations the software COMSOL Multiphysics was used.
Results:
The maximum measured torque was in average 0.206 Nm for the magnets with highest coercive field. Almost all retention force was lost due to demagnetization (71.4%) for the magnets with the lowest coercive field and only 7.7 % for the magnets with the highest coercive field.
Conclusion:
It was found that MRI induced torque of retention magnets can be investigated by a simulation model, but a minor correction might be needed at higher fields. The demagnetization results suggest that a magnet with highest possible coercive field should be used.
Karl-Johan Freden Jansson
Måns Eeg-Olofsson
Bo Håkansson
Sabine Reinfeldt
HamidrezaTaghavi
Bone anchored hearing aid surgery without tissue
reduction - the Lady Edith Wolfson Medical Center
experience.
Introduction:
Tissue preservation in bone anchored hearing aid surgery is becoming increasingly important. Since July 2012, we have been peforming bone anchored hearing aid surgery without tissue reduction. We present our results and technique.
Method:
Restrospective case review.
Results:
Thus far, 10 patients have been implanted either with a Ponto implant by Oticon Medical, or BIA300 and BIA400 by Cochlear. One patient presented with a local skin reaction Holgers grade I which responded to local antimicrobial cream alone. One patient had skin overgrowth which completely resolved when replacing the abutment with a longer one. All other cases had an unremarkable recovery and followup.
Conclusion:
Performing no skin reduction appears to be feasable and as safe as surgery with tissue reduction and in our opinion superior due to reduced impact on cosmesis and recovery time. We strongly recommend adopting this as the standard of care.
85
Avi Goldfarb

A prospective comparison between the
new wide and conventional Ponto implants:
6-months data in first 20 patients
Introduction:
This report provides a comparison between the new Ponto 4.5-mm wide implant in comparison to the 3.75-mm conventional Ponto implant.
Method:
In this randomized, prospective clinical trial, the first cluster of 20 adult patients was randomly assigned to the wide (test) implant and conventional (control) implant in a 2:1 (test:control) ratio. ISQ-values were measured at implant surgery as a baseline, and at 1, 2, 3, 4, 6, and 12 weeks, and 6 months post surgery. Skin reactions according to Holgers’ grading scale were monitored during follow-up. All implants were loaded at 3 weeks after implant surgery. Subjective benefit was measured using the APHAB, GHSI, and GBI questionnaires.
Results:
No implants were lost during the 6-months follow-up time. One patient (control implant) required soft tissue revision surgery. Mean absolute ISQ values for the test implant were higher than for the control implant. Both implants showed a safe ISQ tendency over time. Skin reactions were comparably low, with only 1 adverse skin reaction (Holgers grade 2, test implant). Both test and control implants provided subjective benefit for the patients.
Conclusion:
The current short-term data suggest that both test and control implant are a secure treatment option for patients requiring BAHI.
Rik Nelissen
Emmanuel A.M. Mylanus
Myrthe K.S. Hol
86
Comparison of ultrasound vs. transcutaneous
needle assessment of skin flap thicknes and required
abutment in surgery without tissue reduction.
Introduction:
When performing tissue preservation, an accurate assessment of skin flap thickness is essential in selecting the correct length of abutment for the patient. The recommended technique involves puncturing the skin with a needle and measuring its thickness. We compare this method with ultrasonographic measurement of of the skin.
Methods:
In all patients undergoing bone anchored hearing implantation surgery without tissue reduction we measured the thickness of the skin with a portable ultrasound and then compared the measured thickness with that received with a needle. Actual thickness was physically measured after the incision was made.
Results:
Introduction of the needle caused skin dimpling which resulted in a measured thickness approximately 2 mm less than that measured with the ultrasound. The actual skin thickness during surgery was the same as measured with the ultrasound.
Conclusion:
Ultrasonography is a more accurate method of assessing the skin thickness and thus the length of the abutment. The advantage of this method is the fact it is non-invasive and can be performed in the office prior to the operation. In non skin-reduction surgery it is also possible to assess whether this is feasible or that some tissue reduction is warranted. In places where not all abutment sizes are kept in stock, it is possible to pre-plan and order an appropriate length abutment prior to surgery.
87
Avi Goldfarb

Oral Abstracts - GeneralFriday 7 June
13:30 - 15:15
Hall One
89
Speech comprehension in background noise
in SSD patients using Baha after a Vestibular
Schwannoma surgery
Introduction:
Since September 2010, 13 patients after a retrosigmoid approach to the vestibular schwannoma (VS) with a consequent single-sided deafness (SSD) have been implanted with the Baha (bone anchored hearing aid).
Method:
Patients underwent testing of speech coprehension without Baha, 6 weeks and one year after the Baha setting. Score of understanding of sentences in the noise backgroud was calculated in three different situations: 1) SnhNssd signal from the normal hearing side, noise from the deaf side, 2) S0N0 signal and noise from the front, 3) SssdNnh signal from the deaf side, noise from the normal hearing side. Tests were conducted in a sound-treated room with 3 loudspeakers situated in the angle + 45o, 0o and - 45o in the 0.75m distance from the subject´s head.
Results:
We have found no differences in S0N0 situations in 65dB:65dB test configuration. For the S0N0 65dB:70dB configuration there is an improvement with Baha after 6 weeks and 1 year, but the difference is not statistically significant. The oposite situation is in SssdNnh condition where patients reached statistically significant improvement for both 65dB:65dB and 65dB:70sB configurations, after 6 weeks and also after 1 year (p=0.037; resp. 0.0014).
Conclusion:
We consider the Baha implant should be an integral part of the care for patients with SSD after vestibular schwannoma surgery. Our data proved statistically significant improvement of a speech comprehension in a background noise.
Acknowledgments:
The research was supported by IGA MZ CR (grant No. NT/11543-6).
Jan Boucek
Libor Cerny
Jan Vokral
Jiri Skrivan

Comparison of Hearing in Noise Performance
between Cochlear Baha and Wireless CROS
Hearing aid Technology in SSD Patients
Introduction:
In this pilot study, ten experienced Baha recipients with single sided unilateral deafness were evaluated by a signal to noise hearing test, the BKB SIN , with their existing Baha device in the implanted state and then with a fitting with the Phonak Wireless CROS (Phonak Audeo S SMART III + CROS wireless microphone using Hi-Bann wireless linking) In earlier studies, CROS devices were compared to Baha where data was favorable for the Baha treatment with respect to hearing in noise performance. During this period CROS technology was not as developed as it is today with respect to cosmetics and performance claims. The purpose of this presentation is to provide the audience with details of speech in noise performance scores during this comparison activity. Discussion of the testing condition and set up as well as the benefits and limitations of this test protocol will be discussed.
George Cire
90
Improving stereo separation of bilateral bone-
anchored hearing aids using cross-talk cancellation.
Introduction:
The benefit of bilateral bone-anchored hearing aids (BAHAs) is limited by interaural cross-talk. In principle, cross-talk could be eliminated using cross-talk cancellation (CTC); inverted signals could be added to each BAHA that cancel out the cross-talk from the contralateral BAHA at the ipsilateral cochlea. In order to implement CTC, the attenuation and phase shift of the cross-talk signal must be known.
Method:
The phase and level of the crosstalk signal was measured psychoacoustically in normally hearing listeners wearing each BAHA attached with a softband. Level was measured by matching the level of a headphone-presented probe tone using a beat-detection technique. Phase was measured using binaural unmasking of a headphone presented tone against BAHA-presented noise. From this information, CTC was implemented using two BAHAs. The resulting stereo separation was measured using a similar beat-detection technique.
Results:
Interaural phase, measured up to 1 kHz, was found to be 150-180 in all listeners. Interaural attenuation varied across frequency and across listeners. CTC improved stereo separation at low frequencies by 10-15 dB.
Conclusion:
Interaural phase and attenuation generated by BAHAs can be measured in normally hearing listeners and used to produce substantial improvements in stereo separation. Although these results demonstrate proof of concept, there are substantial challenges in determining interaural attenuation in the clinic, because the mixed presentation modes used here will not be possible with BAHA users.
91
John Culling
Robin Hunt
Yaser Najaf
Steven Backhouse

Stability, survival, and tolerability of the Baha
BI300 implant: 3-year data from a prospective
multicenter clinical investigation
Introduction:
This study reports on the 3-year stability, survival, and tolerability data of a novel bone anchored hearing implant (BAHI) in comparison to the previous generation implant (Branemark).
Method:
In this open, randomized, prospective, controlled, multicenter clinical trial, 77 adult patients were included. The test implant (Cochlear Baha BI300) and the control implant were randomly assigned in a 2:1 ratio. Implant stability quotient (ISQ) values were determined at implantation as a baseline. ISQ values were recorded during follow-up, together with skin reactions according to Holgers’grading system, at 10 days, 4, 6, 8, and 12 weeks, 6 months, and 1, 2, and 3 years after implant surgery. Implants were loaded with the sound processor from 6 weeks after implantation.
Results:
Mean absolute ISQ values were higher for the test implants than for control implants. The same tendency in mean ISQ values over time was seen in both implants. Skin reaction rates were comparable initially, but diverged from 6 months post implantation. One test implant was lost and 1 implant was electively removed.
Conclusion:
Both test and control implants show an ISQ tendency suggesting stabile implants, with higher absolute values for the test implants. The current 3-year data indicate the test implant to be a secure successor to the well-known control implant
92
Maarten De Wolf
Rik C. Nelissen
Joacim Stalfors
Mons Eeg-Olofsson
Kevin Green
Mark C. Flynn
Mike Rothera
Emmanuel A.M. Mylanus
Myrthe K.S. Hol
The 15 year experience of being the MDT
counsellor/coordinator of the Tullamore BAHA
programme.
Introduction:
The Midland Regional Hospital Tullamore (MRHT) has conducted principal MDT BAHA programme in Ireland for the last 15 years. This ran concurrently with the development of the first ENT CNS role within the state . The nurse’s role within this programme became one of a counsellor and coordinator. This presentation discusses the key aspects of the role development.
Method:
A phenomenological approach is utilised to identify themes and key aspects to the nurses’ role as a counsellor / coordinator.
Conclusion:
In this role the CNS uses both knowledge and experience of ENT nursing practice to help clarify the patients expectations of both the surgical and rehabilitative aspects of their care. The counselling aspect of the role involves informing patients about the process and supporting patients in their decision making to either proceed or withdraw from the programme. Post operative wound management, ear care and hearing rehabilitation and hollistic after care complete the role.
93
Howard Savage Jones
Theresa Frawley

Challenges in the design of a Bone Conduction
Implant
Introduction:
Treatment with conventional bone conduction devices was considerably improved by the introduction of percutaneous bone anchored hearing aids (BAHA) in the 1980ies. Although the BAHA is a well-functioning system there are some complications related to the permanent skin penetration. In the late 1990s we started to look at some alternatives that did not need the permanent penetration of the soft tissues. The main challenges to develop a Bone Conduction Implant allowing intact skin will be discussed in this presentation.
Method:
Main challenges were: Where to place and how to attach the transducer? What type of transducer should be used and how to seal the whole implant? How to transmit and receive the sound through soft tissues of variable thickness? How to measure/verify implant performance in vivo?
Results:
A new transducer element was developed with sufficient small size and power capability called Balanced Electromagnetic Separation Transducer. It was found that the mastoid portion of the temporal bone was most sensitive to induced vibrations and also offered the required space for the implant. Attachment was made in the bottom of a drilled recess with flat contact between the transducer casing and the skull bone. It was also found that a passive amplitude modulated radio frequency transmitter driving an induction link offered sufficient vibration output at an acceptable current drain from battery.
Conclusion:
The BCI is developed and will be tested on a first patient as an alternative to the BAHA treatment.
94
Bo Håkansson
Mans Eeg-Olofsson
Sabine Reinfeldt
Hamidreza Taghavi
Karl-Johan Fredén Jansson
Carina B Johansson
Joacim Stalfors
95
A Visible Ear Simulator Case Study : Bone
Anchored Hearing System placement.
Introduction:
The Visible Ear Simulator (VES) is a freeware simulator for ear surgery available at: http://ves.cg.alexandra.dk/ The VES project is an ongoing research cooperation between surgeons from the Danish National Hospital, and software developers from the Alexandra Institute supported by the Oticon Foundation. At this time, the VES can simulate and teach rigid bone drilling procedures such as a mastoidectomy and posterior tympanotomy for chronic otitis media and CI. The simulator is widely used around the world. It has been translated into Chinese and additional versions in German, Spanish, Portuguese, French and Russian are in preparation.
Currently our research focus is on the development of a robust physical simulation system that can handle soft tissue deformation as well. Given such a physics system, the future development of the simulator will focus on two major areas: First, we will develop methods that allows the user to construct custom temporal bones and scenarios by using imported clinical CT and MRI data to mold the shape of the original temporal bone and still retains the high fidelity graphics of the histological specimen. Secondly, we will develop an enhanced simulation environment, in which soft tissues such as the skin, drum, vessels and nerves are made available for surgery as interactive, deformable components. This may involve the simulation of skin incisions and allow for the simulation of cholesteatoma removal, CI electrode insertion and bone anchored hearing system placement.
The presentation will discuss the possibilities, benefits and limitations encountered when attempting to simulate a bone anchored hearing system placement procedure using our system.
Peter Trier
Karsten Noe
Mads Sølvsten Sørensen

Oral Abstracts - Unusual SurgeryFriday 7 June
13:30 - 15:15
Hall Two
Unusual approaches for Round Window Vibroplasty
(RWV) with Vibrant Sound Bridge ®. (VSB)
Introduction:
RWV with VSB is done for restoring hearing in patients with severe conductive or mixed hearing loss who are not suitable candidates for ossicular chain reconstruction. Congenital malformation of the middle ear/inner ear and postmastoidectomy cavity pose surgical challenges when doing RWV.
Method:
Two unusual approaches for the RWV in relation to the facial nerve were performed in our institution. In the first patient with congenital abnormality of the middle ear/inner ear, vibroplasty was done through a retro facial approach. In the other patient who had canal wall down mastoidectomy surgery for cholesteatoma, a tunnel was made in the high facial ridge lateral to the facial nerve. Selected video representations of the surgeries will be shown.
Results:
Both patients had significant benefit in hearing and speech perception. Consonant-vowel Nucleus-Consonant (CNC) testing at 70dBSPL improved from 44% unaided to 96% in the aided condition in the first patient and 48% to 100% in the other patient. In the Hearing in Noise Test (HINT) done in quiet, the hearing improved from 74.12 to 40.94 dBSPL in the first and 67.29 to 49 dBSPL in the second patient. HINT testing done in noise revealed Signal to Noise ratio (SNR) improvement from 12 dB unaided to 2.82 dB with VSB in the first and 9.29 to 0 dB in the second patient. There were no surgical complications or instances of device extrusion.
Conclusion:
Alteration of the surgical approaches may need to be considered when performing round window vibroplasty in patients with abnormal anatomy and unusual post mastoidectomy cavity.
97
Venkatakarthikeyan Chokkalingam
Daniel Jethanamest
Hillary Snapp, Simon Angeli
Fred Telischi

98
First Bone Conduction Implant surgery-surgical
and audiological aspects.
Introduction:
The Bone Conduction Implant (BCI) is a transcutaneous direct bone conduction hearing system where the implanted Bridging Bone Conductor (BBC) is covered by intact skin. The external sound processor is attached to the skin with magnetic force and signals are transmitted via an inductive link to the transducer. The BCI has been developed to avoid skin complications and osseointegration failures occurring with the percutaneous BAHA solution. The first patient implanted with the BCI had a unilateral mixed hearing loss and intact mastoid bone.
Method:
The transducer part of the BBC was positioned at 5-6 mm depth and in direct contact with the bony structure of the mastoid bone, with its center point 20 mm behind and slightly above the bony ear canal opening. Preoperative Cone Beam Computed Tomography (CBCT) was used to optimize the position of the BBC and the securing bar for the transducer. The audiological assessment will compare results from sound field tone thresholds, speech reception threshold in quiet and signal to noise thresholds at speech levels with a transcutaneous Baha device versus the BCI.
Results:
The surgery was uneventful and was performed according to plan. A postoperative CBCT confirmed that the BCI was positioned according to the preoperative planning. The audiological assessment is still to be performed and will be presented.
Conclusion:
BCI surgery is safe. Utilizing CBCT in preoperative planning can facilitate the placement of the BCI in an optimal position in the skull bone.
Mans Eeg-Olofsson
Sabine Reinfeldt
Hamidreza Taghavi
Joacim Stalfors
Karl-Johan Fredén Jansson
Bo Håkansson
Comparison between a new implantable
transcutaneous bone conductor and
percutaneous bone-conduction hearing implant
Introduction:
Despite good results on osseointegration and limited skin reactions with percutaneous bone conductors, there remains room for improvement. Especially in children, adverse events with percutaneous bone conductors might occur more frequently. Transcutaneous bone conductors, if powerful enough, can provide a solution that minimizes adverse events and implant loss. This study compares a new transcutaneous bone conduction hearing aid, the Sophono Alpha 1 (Sophono), with the percutaneous Baha system (Baha).
Method:
In our tertiary referral centre, twelve patients (age 5-12 years) with congenital unilateral conductive hearing loss were enrolled in the study as follows: 6 patients with the Sophono and 6 with the Baha. Both clinical results and audiological data were gathered. For an objective audiological comparison between both systems, we used a skull simulator.
Result:
The skin reactions were comparable between both groups, in the Baha group 1 implant was lost 1 month after second phase surgery. The users received audiological benefits from both systems. The Baha-based outcome was slightly better compared with Sophono-based results in sound field thresholds, speech recognition threshold, and speech comprehension at 65 dB. The skull simulator demonstrated that the Baha device has an output that is 10-15 dB higher compared with the Sophono device.
Conclusion:
The Sophono offers appealing clinical benefits of transcutaneous bone conduction hearing, however, the audiological challenges of transcutaneous application remain, as the Sophono does not exceed percutaneous application regarding audiological output.
99
Myrthe Hol
Rik C. Nelissen
Martijn J.H. Agterberg
Cor W.R.J. Cremers
Ad F.M. Snik

Sophono™ implant for patients with bilateral ear
malformation: preliminary data from a tertiary care
referral center
Introduction:
Since 2011, a transcutaneous bone-anchored auditory implant (Sophono ™ has been available for patients affected by bilateral, conductive hearing loss which cannot be corrected by surgery. Aim of this study is to report on a pediatric tertiary care referral center’s experience with the device.
Method:
The clinical records of subjects receiving a Sophono ™ implant in Bambino Gesù Pediatric Hospital, Rome, in 2012 were reviewed. Data concerning surgery, complications and functional outcome were considered.
Results:
In 2012, 5 patients received a Sophono device in our Institution (mean age = 15±6 years, age range = 8-20 years). All of them had bilateral, syndromic otodysplasia. No major intraoperative complications occurred. Post-operative complications included 1 patient developing a skin ulceration below the external magnet and 1 patient reporting pain from using the device for more than 4 hours consecutively. Mean free-field PTA (0.5-3 kHz) with the device was 32 dB HL, and mean functional gain as compared to the unaided condition was 41 dB HL .
Conclusion:
Sophono ™ implants can be a valuable alternative to conventional, percutaneous bone-conduction hearing aids (Baha) in patients affected by bilateral ear malformation. Anyway, to ensure the success of the treatment, several cautions have to be taken, such as careful pre-operative assessment of skull bone thickness and close post-operative follow-up of the skin under the external processor. Moreover, patients should be encouraged to use the least powerful magnet so as to avoid major skin reactions.
100
Alessandro Scorpecci
Concettina Pacifico
101
The Skin Punch Technique for Bone Anchored
Hearing System Placement
Objectives:
To demonstrate a new technique for the placement of an osseointegrated bone conduction hearing aid fixture and abutment.
Method:
instead of creating a thin skin flap or using an incision with undermining, 4 millimeter or 6 mm skin punches were used to remove a core of soft tissue to bone or periosteum. Drilling and insertion otherwise proceeded in a standard fashion.
Results:
48 procedures were performed on 45 adult and pediatric patients with 6-42 months follow-up. Four patients sustained spontaneous extrusions of the fixture. Three underwent successful replacement with no further problems for over more than 9 months. Otherwise there were no complications, and peri-pedestal skin irritation has been substantially reduced compared to standard techniques.
Conclusions:
with sufficient irrigation and longer pedestals, successful placement of an osseointegrated bone conduction fixture is possible using an easier, faster technique with fewer post-operative skin complications. The technique is advantageous when using the new hydroxyapatite coated abutments where better soft tissue approximation is desired. The higher rate of extrusions compared to flap techniques will be discussed.
Michael Novak
Ryan Porter

Novelty in bone conduction implants surgery.
Introduction:
The latest developments in BAHA abutment design ensured the reduction of the surgery time, and due to quality of the osseointegration processes, shortening of first sound processor switch-on time.
Method:
We implanted 9 BA 400 abutments in 8 patients (6 with bilateral microtia, bilateral atresia of the external auditory canal, 1 with bilateral atresia of the external auditory canal only, 1 - after surgical treatment of the chronic otitis media). The age of patients varied from 8 to 31 years. The soft tissue reduction was not required in all patients. The abutment height in 5 patients was 8 mm, in 3 cases - 6 mm, in 1 patient - 10 mm (plus 2 mm to the soft tissue thickness).
Results:
The surgery time was reduced up to 23 minutes. The mean ISQ testing values increased postoperatively in 7 of 9 patients on 7th day and in 6 patients on 14th day. Soft tissue complications were recorded on 7th day in 3 patients, two of them had abutments covered by skin (2nd grade by Holger’s classification). On the 14th day no inflammation was obtained in all operated patients. The sound processor was switched-on one month after surgery in all operated patients.
Conclusion:
It was shown that the use of the BA 400 abutment reduces the surgery time by 2.5 times, the time of the osseointegration and the sound processor switch-on by 2.5-3.0. It is concluded that to reduce the soft tissue early postoperative complications further investigations are required.
102
Sergey Osipenkov
Neyla Mileshina
Vigen Bakhshinyan
Georgy Tavartkiladze
103
Initial Experience of the CochlearTM BAHA®
BIA400 in a Tertiary Referral Centre
Introduction
Newcastle upon Tyne BAHA Programme is a tertiary referral centre and was involved in the initial controlled market release of the BA400 abutment. The new system has three advantages – less soft tissue reduction, variable length of abutment and a coating of hydroxyapatite to promote skin adhesion and reduce infection. The initial results will be presented.
Methods
All patients underwent a one stage, no tissue reduction technique surgery. Standard allevyn dressing was applied. Abutment stability (assessed using the (RFA) Ostell Resonant Frequency Analysis), skin reactions (classified using the Holger score) and operative time, were assessed on patients implanted with the BIA400.
Results
Data was collected in 55 consecutive BIA400 implants . Age range was 6 – 81 years with a mean of 53 years. The mean intraoperative RFA was 57.4, and the post-operative mean RFA at one week was 60.3. At one week the Holger inflammation score was 0 in all but 3 cases, demonstrating no significant inflammation. No other complications were noted. The surgical time required to insert the BIA400 was significantly reduced owing to the fact that wide subcutaneous tissue reduction is no longer required. This in turn delivered a more cosmetically acceptable post-operative appearance.
Conclusion
Our initial impression of BIA400 is that it is as safe and as effective as previous models. The refinement of the surgical technique has led to shorter surgical times, with no obvious detrimental consequences in this study.
Vik Veer
Ian Johnson

Two Segments Osseointegration for Prosthetic
Rehabilation of Microtia
Objective:
Simplifing the configuration of craniofacial osseointegration, and improving the strength for a two part implant system.
Method:
First the anchor point orientation on the temporal bone was determined by CT, followed by the embedding operation. Three months later the titanium cylinder which replaces the traditional abutment is fitted. Finally, the titanium bar for mounting the prosthesis was connected to the cylinder by TIG or laser welding.
Result :
No adverse reaction occured after the osseointegration. The bar structure resulted in a weight reduction of more than 40%, and the strength was increased 2-3 times with positive patient feedback.
Conclusion:
The two-segment implant system could meet the need for microtia osseointegration in advanced meterials. The weight reduction reduces discomfort, and the simplified structure enhances the patients rehabilitation process. However, the TIG welding was more difficult than the traditional assembly stage.
Wang Kai,
Tian-yu Zhang
105
Oral Abstracts - Surgical TechniquesFriday 7 June
13:30 - 15:15
Barbour Room
107
Prevalence and management of trauma related
injury to percutaneous implants in the pediatric
population.
Introduction:
While common complications of Bone Anchored Hearing Aids (BAHA) relate to the surrounding soft tissues, percutaneous implants are also susceptible to trauma. Our objective was to examine the prevalence and management of one implant complication resulting from head trauma in children.
Method:
All cases of BAHA performed at our pediatric institution between 1996 and 2012 were reviewed for a history of trauma. The demographics, clinical characteristics, management and outcome of identified cases were further reviewed.
Results:
Five cases of trauma occurred in 202 cases over a 16 year period. In all cases, BAHA was initially performed as a two-stage procedure (stage I - 18 months or older; stage II - 6 months later). In 3 cases the implant was retained with the skull fracturing around it. Management included abutment removal and wound irrigation in the operating room. In these cases it was not possible to remove the implant given the strength of osseointegration. In the remaining 2 cases the implant extruded at impact and these were managed with local wound care and systemic antibiotics. All 5 children ultimately underwent revision 2nd stage utilizing their “sleeper”™ implant, most commonly 6 weeks post injury, with one child undergoing 2nd stage at the time of abutment removal.
Conclusion:
Head trauma is frequent in the pediatric population and in children with percutaneous implants this can uncommonly lead to implant intrusion or extrusion. Revision surgery is typically required, however early, uncomplicated return to device use can occur particularly when a “sleeper”™ implant is present.
Sharon Cushing
Vicky Papaioannou
Blake Papsin
Soft Tissue Reactions and Treatment in Bone-
Anchored Hearing Aid Implantation: A Twenty
Year Experience
Aim:
One of the major challenges in successful long-term use of bone-anchored hearing aids is maintaining healthy, reaction-free soft tissues around the implant. Complications from tissue responses can range from simple visible redness to necrosis resulting in implant loss. We report our extensive long-term experience with soft tissue reactions in patients implanted and followed over twenty years, subsequent treatments, and compare our data to the literature.
Method:
Retrospective review of data compiled on 442 patients implanted and followed regularly between 1991 and 2011. At each patient encounter following implantation, reactions of surrounding soft tissues were recorded, along with status and stability of implants. Resulting interventions were documented.
Results:
We will report soft tissue reactions based on physical appearance according to the Holger classification, as well as measured height of excessive tissues surrounding the implant. Implant stability is measured by palpable mobility and periotest data. Treatments used for soft tissue problems will be presented. Rates of complications are compared to those previously documented in the literature.
Conclusion:
Soft tissue reactions resulting from bone-anchored hearing implants can occur even years after initial surgery. Regular maintenance and frequent observation are recommended to prevent complications and maximize hearing aid benefit.
106
Bill Hodgetts
Richard Liu
Amberley Ostevik

Oral Abstracts - GeneralFriday 7 June
15:45 - 17:15
Hall One
108
Soft tissue reactions in patients with BAHA
Introduction:
In the study we wanted to establish the correlation between the degree of soft tissue reactions and body mass index (BMI), age and gender.
Methods:
All patients that have been operated at our department were followed-up in the period between 9 to 1 years. The soft tissue reactions were classified according to the Holgers classification on regular patient visits. BMI was calculated in every patient. The changes were followed at least once a year.
Results:
47 patients were evaluated. 58 % were operated because of the chronic otits with mixed or conductive hearing loss, 20 % had unilateral or bilateral atresia and 16% had SSD, other indications were otoscleosis and syndromic patients. Grade of Holgers classification significantly correlated at 0.01 level with BMI (Spearmans rho 0.452). Holgers grade also significantly differed between sexes in females the skin reactions were less frequent. ANOVA test did not show a statistical difference between patients with diifferent indications.
Conclusion:
If performed carefully, the surgery for the BAHA has a favorable outcome, regardless the technique used. Holgers classification may change during the years. Skin reactions can be treated with local therapy or systemic therapy if the skin irritation appears and may turn to a normal grade. Adipose patients should be treated with special care because they are more prone to soft tissue reactions.
Janez Rebol

Bone Anchored Hearing Aid Case Series - a Twenty-
Four Year Experience
Introduction:
The bone anchored hearing aid (BAHA) programme at the Queen Elizabeth Hospital in Birmingham has been successfully running since our first BAHA insertion in 1988. To date, there have been over 1600 individual BAHAs have been implanted at the centre and this case series reports the demographic, audiological, operative and follow up outcome data.
Method:
1405 patients have undergone BAHA insertion, a significant proportion of which have bilateral aids. Each individual implanted aid has been thoroughly investigated to give an extensive database of pre, peri and post-operative information. Using the current patient database for demographics, the clinical noting system for clinic letters and operative notes, the audiological database for hearing thresholds and local specialist databases from the audiologists and clinical nurse specialists for post operative outcomes, we have constructed an all-encompassing source of data.
Results and Conclusion:
We will present the results of our twenty-four year experience of BAHA insertion and will evaluate important aspects of the pre, peri and post-operative period in order to draw conclusions on our current work to ultimately influence future practice.
111
Elizabeth Ross
Chris Coulson
James Rainsbury

The Benefit of Geriatric Bone Anchored Hearing Aids
Introduction:
Bone anchored hearing systems have proven to be an effective amplification solution for conductive, mixed, and profound unilateral sensorineural hearing losses, though the benefits relative to the risks in older patients are uncertain.
Method:
Single center retrospective case series study performed by an experienced surgeon in patients over the age of 50. Data regarding age, gender, indication, diabetes, hypertension, thyroid disease, smoking, body mass index, surgical technique, implant and abutment length, and revisions were collected. A telephone survey using the Glasgow Benefit Inventory was completed.
Results:
A total of 26 patients from 2003-2012 were identified, with a mean age of 65 years (53-77 years), 42% male and 58% female. The indications were equally divided between conductive/mixed hearing loss (C/MHL) and single sided deafness (SSD). Linear incision technique was used in 31%, dermatone in 69%. ), the most common comorbid disorder was hypertension 61.5 % and thyroid disease (38.55). There were two implant losses, and soft tissue revision and abutment replacement occurred in 15% and 23% respectively. Glasgow Benefit Inventory quality of life surveys were collected on 9 patients, and indicated patient benefit (Total normalized score +37.33). General Benefit and Social Benefit were strong (+50.0 and +28.4 respectively), though there was a negative trend in physical benefit (-3.7) possibly reflecting advancing age and associated increasing medical problems.
Conclusions:
The bone-anchored hearing system performs well in the older patients and provides benefit to its recipients , though the need for revision surgery was significant.
113
Alan Webster
Brian McKinnon
Jamie Segel
112
Protocol to study whether Baha treatment in
patients with conductive or mixed hearing loss is
evidence based
Introduction:
According to the Oxford classification, the highest level of evidence (level 1) can only be reached by performing randomized clinical trials. Randomization excludes selection bias. When comparing Baha to conventional hearing devices, randomization might lead to ethical issues (as Baha requires surgery). Then, a pre-post intervention evaluation is the next option (level 4) or an individual cohort study (level 2b). As an example of the latter option, comparative effectiveness research project (CER) can be carried out, comparing different health service interventions, like Baha versus reconstructive surgery in atretic ears, Baha versus acoustic device in running ears, etc. First step to study acoustic and bone conduction devices like Baha is to obtain objective data using well-defined simulators. Usually, small scale clinical trials can validate such an objective evaluation. Then the next step is a cost-effectiveness evaluation and calculation of qaly’s (quality-of-life (QoL) adjusted life years). Cost not only comprises direct and indirect cost of the intervention and aftercare but also, in case of a successful treatment, cost savings owing to better participation in our society. Furthermore, to determine qaly’s, expected life years is an important parameter, which has to be replaced by the (unknown) years of effective device use. Considering these factors, a protocol will be presented that enables CER studies, and a model to assess qaly’s.
Ad Snik

Bone anchored hearing aids versus middle ear
implants in mixed and sensorineural hearing
loss. Patients self-assessment.
Aim of the study:
To compare the satisfaction of the patients using bone anchored hearing aids (BAHA) and middle ear implants (MEI) in mixed and sensorineural hearing loss (SNHL).
Method:
Evaluation of the subjective satisfaction of the patients using BAHA and MEI, with a simple quick questionnaire, repeated prospectively at each consultation.
Results:
The duration of use per day, the global improvement of hearing, the improvement of speech recognition in noise, the comfort of use, the aesthetic-visibility, the skin tolerance, the sound localization and the global satisfaction where evaluated by self assessment, in 134 patients using BAHA in mixed HL, 66 patients using BAHA in single sided deafness (SSD), 28 patients using MEI in mixed HL, 119 patients using MEI in SNHL.
Conclusion:
BAHA and VSB in mixed HL are used full time or near by more than 80% of patients, less for the MEI in SNHL. For hearing, the MEI in mixed HL have the best scores, but MEI are not superior to BAHA for hearing in noise, and MEI in SNHL have the lower scores. The comfort and aesthetic scores are better with MEI than BAHA. With BAHA, subjective skin tolerance is worst than objective examination. 97% of patients find they localize sounds with BAHA in SSD. The satisfaction rate is superior to 90% with BAHA, to 80% with MEI in mixed HL, 70% with MEI in SNHL.
115
Thibaud Dumon
Non-invasive Assessment of Bone-Anchored
Hearing Aid Implant Stability Independent of
Structural Components
Introduction:
The ability to evaluate the stability of implants during the healing phase and throughout their life is extremely useful in practice; however, it can be problematic if the abutments must be removed to perform the assessment. An impact procedure has been developed which provides an assessment of the stability (stiffness) of the bone/implant interface without removal of the abutment that is independent of the components between the interface and the impacting location. The stability of the interface can then be determined regardless of the fixture and abutment being employed. In this study the developed technique was evaluated by determining the stiffness of the implant/material interface with a variety of bone-anchored hearing aid abutments.
Method:
The assessment procedure recorded and interpreted the accelerometer signal measured during an impact of the fixture/abutment system. To evaluate the interface stability without the influence of the intervening components, a numerical procedure and mathematical model of the system was incorporated into the interpretation. Using a specific measurement protocol, the recorded signal is matched to the numerical model allowing the stiffness of the interface to be determined. Testing of various components with the same interface was carried out to evaluate the effectiveness of the model in eliminating the effects of the intervening structure on the calculation of the stiffness.
Conclusion:
Within experimental error, the differences in mechanical properties of the individual components could be accounted for within the model. It was found that the stiffness measured at the interface is independent of the specific components used.
114
Lindsey Westover
Don Raboud
Gary Faulkner
Bill Hodgetts

Oral Abstracts - Unusual SurgeryFriday 7 June
15:45 - 17:15
Hall Two
116
The BAHA in borderline severe mixed hearing
loss
Introduction:
Bone anchored hearing implants give excellent auditory rehabilitation in pure conductive hearing loss However in mixed hearing loss, the higher the bone conduction threshold the less predictable will be the benefit for the patient from the results of pure tone audiogramm testing alone. Speech audiograms in best aided condition are paramount to judge on the presumed patient’s benefit with direct bone conduction with power devices. In borderline severe mixed hearing loss, this is crucial for differential indication with respect to cochlear implantation.
Methods:
This study is a retrospective review of the cases treated at the University Hospital Homburg 1989-2004 and University Hospital Heidelberg, Germany 2004-2012. Out of a total of 415 patients treated with titanium implants, 188 patients received bone anchored hearing implants.
Results:
Bilateral BAHA power devices gave the best amplification. Bilateral BAHA Cordelle II was the treatment for 3 patients. However, the current version of the head level worn power device as the BP 110 seem to provide better sound quality in addition to the advantage of receiving sound closer to the natural position. However, one patient with osteopetrosis did not reach sufficient amplification despite positive subjective testing.
Conclusions:
Bilateral BAHA power devices are valuable hearing solution for patients with borderline severe mixed hearing loss when preoperative testing in terms of both objective as well as subjective scores indicate sufficient amplification and speech intelligibility. Of course, in progressive hearing loss, this might be only temporary before cochlear implantation is warranted.
Philippe Federspil

119
Surgical Experience with retrosigmoid
implantation of the Bonebridge of MedEI
Introduction:
The Bonebridge has initiated a new era in the treatment of patients with bone-anchored hearing aids. We report our surgical experience with the Bonebridge in retrosigmoid implantation.
Method:
10 patients were operated under general anaesthesia. There were made preoperative CT scans for planning the right implantation side. Patients were covered with antibiotics for five days. On the first postoperative day the patients were discharged. The patients were followed two weeks post-surgery together with the first fitting.
Results:
All patients were successfully retrosigmoid implanted with the Bonebridge. The dura was exposed in all patients. The sinus was exposed in 2 patients. There were no injuries of dura or sinus. One post-operative inflammation occurred after 10 days. This patient was treated conservatively with pressure dressing and antibiotics. There were no major complications.
Conclusion:
The Bonebridge can be successfully implanted in the retrosigmoid position. An accurate preoperative planning with CT scans is very important. The surgeon must have experience in the exposure of the dura and the sinus.
Rolf Benedikt Salcher
Hannes Maier
Burkard Schwab
Thomas Lenarz
118
Bone Conduction Hearing Sensitivity in Normal
Hearing Subjects Transcutaneous stimulation at
BAHA vs BCI position
Introduction:
The Bone Conduction Implant (BCI) position is closer to the cochlea than the standard BAHA position. Studies on bone conducted sound transmission in cadaver skulls using laser Doppler vibrometry (LDV), have shown increased acceleration of the cochlea for smaller distance between the stimulation position and the cochlea. The aims of this study are to investigate if stimulation closer to the cochlea implies improved hearing sensitivity in live humans, and to compare the results with ear-canal sound pressure (ECSP) measurements and previous LDV measurements.
Method:
The difference in hearing thresholds from transcutaneous stimulation at the BAHA and BCI positions in the frequency range of 125 Hz to 8 kHz was determined. The ECSP was measured by a small probe tube inserted close to the tympanic membrane in the frequency range of 100 Hz to 10 kHz. All measurements were done at 20 normal hearing subjects both ipsi- and contralaterally.
Results:
Ipsilaterally, the BCI position gave 3-14 dB higher hearing sensitivity compared to the BAHA position for all frequencies. There were non-significant differences between hearing threshold shifts and ECSP differences for most frequencies up to 4 kHz, where ECSP was above noise floor. Hearing threshold results were similar to previous LDV measurements except at low frequencies where the BC sensitivity improved and the acceleration remained unchanged. The transcranial attenuation was 3-8 dB higher for stimulation at the BCI position.
Conclusion:
Present results confirm previous LDV measurements except at low frequencies. Subjective threshold shift can be replaced by objective ECSP difference.
Sabine Reinfeldt
Bo Håkansson
Hamidreza Taghavi
Mans Eeg-Olofsson

121
Bonebridge - the first surgical experience and 6
months results
Introduction:
Bonebridge was introduced by Medel in June 2012. We implanted several patients by the end of 2012. Patients were meticulously assessed before surgery from audiological and radiological point of view. Surgical procedure was typical as for bonebridge and there was no complication during surgery. During presentation will be shown audiological results and patients satisfaction from used device . Presentation of 15 cases were analysed. In conclusion we can say that for patients with appropriate anatomical conditions is good soultion and it is not very invasive procedure
Piotr H. Skarzynski
Marek Porowski
Maciej Mrowka
Lukasz Olszewski
Henryk Skarzynski
120
A new semi-implantable transcutaneous Bone
Conduction Hearing Device. Clinical, surgical
and audiological outcomes in patients with
congenital ear canal atresia
Introduction:
We have developed a new partially implantable BCHD without a percutaneous abutment and have been using it clinically for seven years now. The principle of this BCHD is a magnetic coupling and acoustic transmission between implanted and external magnets. The goal of this study was to evaluate its clinical and audiological results in patients with unilateral or bilateral congenital aural atresia.
Methods:
Magnets are implanted into shallow bone beds in a one step procedure. The skin above the magnets is slightly thinned. The external device is fixed with counter magnets in a base-plate. Patients: 20 patients who have been implanted due to congenital atresia showed up for this follow up study. The follow up period was 19.3 ± 12.2 months with a range from 0.2 - 46,6 months. The average age of the patients at the time of implantation was 12.4 years.
Results:
The average hearing gain was 28.6 dB ± 8.8 dB HL and the suprathreshold word-recognition tests increased by 61.6% ± 25.3 %. Strength of the magnetic force that the patients had chosen themselves measured 0.9 ± 0.4 N with a range from 0.3 - 1.8 N. Skin thickness over the implants measured sonographically was 3.9 ± 0.8 mm.
Discussion:
This new bone conducting hearing device only needs one operation, has a very low risk for complication and a hearing gain similar to other bone conducting hearing aids. We have found high comfort and safety of this system and conclude that it is a valuable alternative to other BCHD.
Ralf Siegert

New developments in bone anchored hearing
aids enabling new surgical approaches offering
possibilities for improvements in clinical
outcome and patient satisfaction.
Introduction:
By the introduction of longer abutments with suitable designs and rounded and smoother shapes as well as the introduction of wider implants, significant improvements regarding clinical outcome, patient satisfaction and surgical procedure has been made possible. Design concepts for suitable tissue interaction in various patient groups were studied with the aim of combining the needs for a safe and simplified surgical technique offering the patients minimal soft tissue trauma with reduced numbness and scar tissue formation as well as quicker healing and improved cosmetic results.
Objective
The objective was to conclude the benefits and possible drawbacks of the most recent developments, and to demonstrate possible new surgical approaches and how proper implant components can be chosen in these situations. Specific biomechanical considerations for different patient groups will be discussed and guidelines will be presented. A number of key implant design parameters were investigated in technical and biomechanical terms and the results will be presented.
Conclusion
A conclusion is that implant and abutment design and selection is of great importance when applying these new developments in clinical practice, however it also opens up for significant benefits for the patients.
123
Patrik Westerkull
122
Virtual planning and visualisation of the first
Bone Conduction Implant surgery
Introduction:
The Bone Conduction Implant (BCI) was recently approved by the Medical Products Agency in Sweden for long-term implantation in patients within a clinical study. The first surgery was performed in December 2012. This study describes the preoperative virtual planning before the surgery, surgical highlights and visualisation of the post-surgical result.
Method:
A preoperative cone beam computed tomography (CBCT) of the planned surgical area was performed utilizing high-resolution unit, 3D Accuitomo 170 (J. Morita Mfg Corp, Kyoto, Japan) and virtually remodelled in the software SurgiCase from Materialise, Belgium. In the 3D virtual model, the surgery was planned considering individual anatomical details and the measurements for the BCI including the securing plate with four screws. For real-life visualisation a stereolithographic model was constructed. After surgery the position of the BCI was confirmed with CBCT and 3D-modelling.
Results:
The position for the BCI and the direction of the securing bar was planned and optimized according to the patient’s bone structure and air-cells in the temporal bone posterior of the ear canal. The BCI (dimensions 14x10x6mm) was planned to be installed in level with the cortical surface. The virtual plan corresponded well with the preoperative surgical experience. Postoperative CBCT 3D-remodelling showed the implant in the planned position with optimal bone contact for both BCI and the securing plate.
Conclusions:
The pre-operative virtual planning using CBCT can be used to optimize the position for the BCI and contribute to safe surgery.
Joacim Stalfors
Henrik Lund
Bo Håkansson
Hamidreza Taghavi
Sabine Reinfeldt
Karl-Johan Fredén Jansson
Carina Johansson
Mans Eeg-Olofsson

Oral Abstracts - OutcomeFriday 7 June
15:45 - 17:15
Barbour Room
124
Comparison Study of Bone-Anchored Hearing
Aid Complications Using the 9mm Abutment
versus 6mm Abutment at Initial Implantation
Introduction:
The purpose of this study was to assess differences in the incidence and type of complications encountered with implantation of the bone-anchored hearing aid (BAHA) when using the 9mm abutment versus 6mm abutment at initial implantation.
Method:
One hundred thirty consecutive patients underwent single-stage BAHA implantation using either the 9mm or 6mm abutment at initial surgery. Clinical outcomes assessed for the two groups included the incidence, type and management of postoperative complications. Abutment size, age, gender, indication for surgery, BAHA type, duration of follow-up and patient co-morbidities to include body mass index were evaluated as potential factors affecting outcomes.
Results:
Average duration of follow-up was 16 months. Postoperative complications occurred in 38 (29.2%) patients. Twenty-four (18.4%) patients experienced minor complications requiring simple, local care; eight (6.1%) patients required in-office procedural intervention; and six (4.6%) patients required revision surgery in the operating room. Implant extrusion occurred in 3 (2.3%) patients. Patients receiving the 6mm abutment at initial surgery were significantly more likely to encounter a complication requiring in-office procedural intervention or revision surgery (p=0.001).
Conclusion:
Minor complications following bone-anchored hearing aid implantation are common. The vast majority of these complications are due to localized skin reactions, most of which are readily addressed through local care. Patients receiving the 9mm abutment during initial implantation are significantly less likely to require in-office procedural intervention or revision surgery postoperatively as compared to those receiving the shorter, 6mm implant at initial surgery.
Sean Wise
Jacqueline LaRouere
Dennis Bojrab
Michael LaRouere

BAHA Surgery without Soft Tissue Reduction
The Torbay Experience
Introduction:
We at Torbay, have be trialling, Baha surgery, without soft tissue reduction ( WOSR ), following its suggestion at ‘09 Osseo Congress. This idea appealed to us, as we had already noticed that, patients with chronic soft tissue inflammation and thickening around the abutment, responded well, when changed to a longer abutment. Certain medical comorbidities, can increase operating time, delay wound healing and increase postoperative morbidity.
Method:
Initially we offered this technique ( WOSR ), to patients with medical comorbidities that could interfere with surgery and wound healing. The results being encouraging, we now offer this to all our Baha patients. The technique involves using a 6mm skin punch with a vertical incision running through, for access. No soft tissue reduction is done. Bone work proceeds as usual ( single stage, using the 8.5, 9 or 12mm abutment ). Patients are seen a week after surgery for suture removal, by which time, the wound has healed. Loading is done at two months. Results: We have performed twenty five Baha operations, without soft tissue reduction, over the last three years. Of these, twenty four patients, use their Baha regularly. Two patients went on to need soft tissue reduction, due to persistent inflammation. The remaining patients are doing well.
Conclusion:
Results so far, have been very promising, with consistently good outcomes (decreased operating time, decreased postoperative morbidity). This technique could certainly be considered in patients with relevant comorbidities.
Shyam Singam
F.P Houlihan
127 126
A clinical view of the aetiology of skin reactions
in BAHA patients:
Introduction:
Fixture site skin reactions are an ever present potential complication of per cutaneous OII’s. Aetiology is multifactorial and though mechanisms are still subject to debate.
Method:
We reviewed 100 cases retrospectively, selecting Holger’s II/III reactions for further analysis. This was supplemented by prospective histological sampling of tissue derived from the OII fixture site: Split skin samples from dermatome raised pedicled flaps in the traditional one stage soft tissue reduction techniques. Full thickness skin samples from linear scalp sparing procedure. Circumferential resection of Holger’s III granulation reaction
Results:
The presence of superficial skin debris is associated with fixture site skin reactions. Cases developing repetitive H III reactions tended to have a history of keloid, dermatitis or syndrome associated skin changes. Clinically pronounced scar proliferation with a delayed timeline in maturation and a prolonged period of soft tissue shearing at the skin/fixture interface.
Conclusion:
The role of keratin debris retention is contributory to the development of fixture site skin reactions; a knowledge of the dermatological history may influence both surgical technique to be adopted and choice of abutment.
Howard Savage Jones
Theresa Frawley

129
Baha200 and Minimally Invasive Surgical Results
Objective:
• Toreportontheresultsandcomplicationsarisingfromusingaminimaltissue removal procedure for the placement of an osseointegrated hearing implant (Baha200).
• Tocommentontheadvantagesanddisadvantagesforthistechniquecompared to the more standard techniques.
Study Design:
Retrospective study in tertiary academic center of the all patients undergoing minimally invasive single-stage osseointegrated implant surgery (Baha) from 2008-2010. Technique: A small incision (1.5cm) with little to no soft tissue (fat only) removal with good skin to periosteum fixation after placement of a 4mm screw and 8.5mm abutment.
Results:
Thirty-four adults were assessed (18-45 month follow-up). No patients experienced hair loss, significant numbness, cosmetic defects, intraoperative or audiologic complications. Seven patients required some combination of bactroban, steroid ointment and/or oral antibiotic for mild erythema around the abutment in the first 2 months post-op. Two patients required conservative management for delayed skin reactions (3.5 mo & 2.5 years). Five of these nine patients had one more episode requiring topical treatment. All reactions resolved in about 2 weeks. One patient (thick scalp and >1.5cm soft tissue removal) was not treated with topical therapy and just had minor debridement in the office.
Conclusions:
We have demonstrated comparable outcomes to other surgical techniques with less cosmetic and other associated complaints. This study indicates that a less invasive approach for the surgical implantation of the osseointegrated auditory implant (Baha) may have merit in patients.
Pete Weber
A novel approach to attaching auricular
prostheses to osseointegrated implants
Introduction:
The use of titanium retained prostheses has revolutionized the field of craniofacial prosthetic reconstructions. The change to clips or magnets from glue offered significant advantages which will be discussed. The purpose of this paper is to introduce a novel concept of using the BI300 abutment customarily used for BAHA to retain the prosthesis ,with the BAHA attachment clip secured to its undersurface .
Method:
Five patients requiring auricular prostheses are presented, with details on the case presentation, technique of implantation, and preparation of the prostheses.
Results:
All 5 patients are satisfied with their prostheses, and their retention mechanisms. The prostheses are firmly attached with minimal to no soft tissue reactions.
Conclusion:
This new approach to attaching an auricular prosthesis to the titanium implant offers the stability and security of the bar clips without the bar, and better attachment than the magnets. It allows for easier soft tissue care without sacrificing prosthesis stability.
128
Jack Wazen
David Trainer

Soft Tissue Reactions as a Function of Abutment and
Incision Type in Osseointegrated Implant Surgery
Introduction:
The purpose of this study is to determine whether the frequency and grade of soft tissue reactions after percutaneous osseointegrated titanium implant placement are independent of abutment or incision type.
Method:
A retrospective case review of adult patients with bone-anchored hearing implant placement between January 2010 and December 2012 were included in the study. The modified Holger’s scale scores were recorded and analyzed to compare rate of soft tissue reactions between the original Cochlear abutment (n = 20), the BI300 abutment (n = 38), and the Oticon Ponto system (n = 30). The frequency and grade of soft tissue reactions utilizing a linear incision were compared to the dermatome flap.
Results:
A total of 88 patients averaged 6 follow-up visits with an average length of follow-up of 349 days. 92% of patients (81/88) had a grade 0 or 1 at all visits. The distribution of grade 2 or higher reactions (8%) among the three different implant systems and incision types is presented.
Conclusions:
The combination of the newer abutments and the linear incision appears to have reduced the frequency of soft tissue reactions. The incidence of grade 2 to 4 soft tissue reactions was too small to achieve statistical significance when comparing the different types of implants.
131
Jack Wazen
George Poulos
Julie Daugherty
Pre-surgical evaluation of retroauricular
subcutaneous tissue thickness in Baha surgery
Introduction:
An important step in the Baha surgery is subcutaneous tissue managing. The proper preparation of the implant s ite depends on relevant tissue removal, which is combined with preliminary retroauricular tissue thickness or the selection of the abutment height for the surgery without soft tissue removal.Authors attempt to measure the retroauricular subcutaneous tissue thickness and try to trace the correlation with objective parameters such as sex, height, weight, and age.
Method:
Standard ultrasound with liner transducer probe was applied to measure the tissue thickness. Group of hundred randomly selected patients were enrolled in the study. Sex, weight, height, and age were correlated with retroauricular tissue thickness; results also were calculated for body mass index.
Results:
The retroauricular subcutaneous tissue thickness ranged between 2.0 and 11.0 mm with the mean value of 5.25 mm. Statistical validation revealed strong correlation with weight and body mass index. Statistical difference was found between retroauricular subcutaneous tissue thickness and sex, confirming women to have thinner subcutaneous tissue than men. The age of the patient also was predictive but without the linear correlation. Conducted measurements revealed no association between retroauricular subcutaneous tissue thickness and height of the patients enrolled in the study.
Conclusion:
Our results provide a predictive value during preoperative counseling of patients and planning the surgery. Basic information obtained during the examination can help choose the optimal implantation technique. The ultrasound examination applied in the study turned to be an easy and reliable method to assess the retroauricular tissue thickness before the surgery.
130
Maciej Wrobel
Mariola Popko
Witold Szyfter

Bone anchored hearing devices in children with
unilateral conductive hearing loss: A patient/
carer perspective
Introduction:
To determine the outcome of a bone anchored hearing device in children with a unilateral conductive hearing loss.
Method:
A retrospective case note analysis was undertaken in a tertiary referral paediatric hospital. All children/carers had completed a Glasgow Children’s Benefit Questionnaire following a period of at least six months from implantation as part of their Bone Anchored Hearing Device (BAHD) program.
Results:
A total of 17 children with a unilateral conductive hearing loss were implanted with a BAHD between 2005 and 2010. The age of the children at implantation was 6 years, 3 months to 16 years. The average age was10 years and 6 months. All children had educational difficulties for considerable time before a bone anchored hearing device had been considered. Qualitative subjective outcome measures demonstrated a significant benefit. The vast majority of patients reported improved social and physical functioning as well as improved quality of life. All 17 patients were using their bone anchored hearing device on a daily basis at when seen12 months following implantation.
Conclusions:
These children typically present late to the BAHD program. There is a significant improvement in quality of life for children with unilateral hearing loss implanted when fitted with a BAHD. There is a high patient satisfaction and improvement in health status reported by the children/carers. BAHDs have an important role in the management of children with symptomatic unilateral hearing loss and an earlier trial should be considered.
133
Rupan Banga
Jayesh Doshi
Anne Child
Andrew Reid
Ann-Louise McDermott
Oral Abstracts - Paed AudiologySaturday 8 June
09:30 - 10:45
Hall One

135
Paediatric Multidisciplinary Microtia & Atresia
Clinics
Introduction:
A number of children referred for surgical intervention for their hearing loss also have outer ear malformations that will also need to be managed surgically. Planning the clinical management and surgery for these patients is complex and complicated by the number of professionals involved. Parents typically attend multiple appointments and can find it difficult to amalgamate the information they receive from different services. The Multidisciplinary Microtia and Atresia clinics provide a ‘one stop shop’ to improve the management for these complex patients.
Method:
Multidisciplinary clinics were established in 2008 for children with hearing loss and outer ear malformation. The Auditory Implant team coordinate and host four clinics each year. The clinics involve ENT, Plastic Surgery, and Maxillo-Facial consultants, a Prosthetist, an Audiologist and Speech and Language Therapist from the Auditory Implant team and a Speech and Language Therapist from the Cleft Palate Team. Babies and children of all ages are seen. A range of literature have been developed to support these clinics and streamline the information received by families.
Results:
The clinics allow joint planning and decision making with parents around the best order for surgical procedures, correct positioning of hearing implants in relation to surgically reconstructed or prosthetic ears, and the best surgical approaches for maximising of later surgeries. The clinics have also resulted in more collaborative working practises with plastics and ENT consultants operating together for very complex cases, and all professionals sharing new clinical and technology developments within their fields.
Conclusion:
The multidisciplinary clinics allow more effective and efficient management of this complex population. Parents report greater satisfaction with the multidisciplinary clinic compared to attending all separate medical appointments.
Emma Stark
Mr D. Jiang
Mr A. Fitzgerald-O’Connor
134
Families’ views and experiences of Bone
Anchored Hearing Aid Use with their Children: a
Study by Interviews
Introduction:
This study qualitatively explores the views and experiences of families on obtaining and using a BAHA device.
Method:
Data were collected via semi-structured interviews from 10 families from different geographical regions of the UK. All the interviews were audio recorded and transcribed verbatim. Thematic content analysis was then used to interrogate the data
Results:
Four main themes and 16 sub themes were identified in the participants’ accounts which describe their BAHA journey. The four main themes were: The impact of deafness, Experiences of the care pathway, Making an informed choice and Getting and using a BAHA.
Conclusion:
Findings indicate how the use of BAHA was valued by families. Although participants identified that BAHA devices improve both the clarity and directionality of sound, the most consistently reported benefits related to social, psychological and educational functioning. BAHA devices were perceived to give children the opportunity to interact with others reducing isolation and improving self esteem and self identity. However, the findings also demonstrate that BAHA devices are not without challenges. Responses identified how professionals need to provide accurate information to families to aid them with the complicated decision making process they are working through in deciding whether to have a BAHA or not. The availability of appropriate advice, information and support (including peer support) is an important part of this process. Families were clear that there were system errors in relation to their care package and these experiences can have a negative impact on their experiences of the device itself.
Imran Mulla
Nicola Wright
Sue Archbold

137
Triage towards CROS hearing aid or Bone Conduction
Device of patients with single sided deafness
Introduction:
It is our purpose to optimize counseling of patients with single sided deafness (SSD) towards a wireless CROS hearing aid or a selection for Bone Conductive Devices (BAHA). Studies performed in the first years of this century do show a patient-preference for a Bone Conduction Device (BCD) above a classic wired CROS-device with traditional earmould. Nowadays we have the availability of modern BCDs and modern CROS devices with wireless FM transmission and open fittings with thin tubes.
Method:
Since 2006 we do offer our SSD patients counseling and trials with a CROS hearing aid and a BCD. Questionnaires (APHAB) are used to compare unaided versus aided situations.
Results:
Results of the APHAB questionnaires will be discussed. Contrary to older studies performed in our center we do find comparable benefit between CROS hearing aids and BCDs and a growing interest of our patients for a CROS hearing aid (43% BCD, 57% CROS).
Conclusions:
Patient selection for efficient and successful BCD implantation in patients with SSD remains challenging. Based on our group results, triage should include a test with a wireless CROS Hearing Aid and evaluation based on questionnaires.
Wim Soede
Johan Frijns
136
Categorization of amplification options for
mixed hearing loss
Introduction:
To compare amplification options for mixed hearing loss, we studied the maximum output of these options, or, in other words, the loudest sounds that could be produced without distortion. Devices were set in linear amplification mode and unlimited. If possible, objective measurements were used. Maximum output was expressed in dB HL.
Method:
Baha was studied on the skull simulator. For the middle ear implants, we had to study the maximum output in patients. They used either the VSB (with actuator coupled directly to the cochlea; n=6) or the Codacs device (n=5). Saturation of these devices was measured with a microphone in the ear canal, measuring the actuator’s radiated sound level, as a function of input level. (Measured) gain was added to obtain output levels. Results. Averaged at 0.5, 1, 2 kHz, the maximum output was 67 dB HL for the Baha Divino, 80 dB HL for the Baha Cordelle, 85 dB HL for the VSB and above uncomfortable loudness for Codacs.
Conclusion:
This audiological evaluation showed that the Baha Divino can be used up to a 35 dB HL sensorineural component, the Cordelle up to 50, the VSB up to 55 and the Codacs to values exceeding a sensorineural component of 70 dB HL. The maximum output of the VSB varied considerably, probably depending on the effectivity of the coupling of the actuator to the cochlea.
Ad Snik
Joost Zwartenkot
Jef Mulder
Emmanuel Mylanus

Oral Abstracts - Multicentre ExperienceSaturday 8 June
09:30 - 10:45
Hall Two
138
A vibration investigation of a flat surface contact
to skull bone for direct bone conduction
transmission in sheep skulls - in vivo
Introduction:
Despite that percutaneous bone-anchored hearing aids (BAHA) are successful in treating patients with conductive hearing loss, there are some drawbacks related to the need of a permanent skin penetration. The Bone Conduction Implant (BCI) system is designed as an alternative to the BAHA since it leaves the skin intact. Hypothesis: The BCI attached with a flat surface contact will offer efficient and linear vibration transmission over time.
Method:
BCI dummy implants were installed in three sheep skulls in vivo to study the vibration transmission characteristics over time. Mechanical point impedances and vibration transfer response functions of the BCI implants were measured at the time of surgery and after a healing period of eight months.
Results:
In one sheep both implants healed without complications. In the other two sheep the implants were either partially loose or lost to follow up. In the sheep with stable implants it was found by the resonance frequency shift of the mechanical point impedance that a more stable integration between the implant and bone tissue as seen in osseointegrated surfaces developed over time. It was also shown that the transcranial vibration transmission remains stable and linear. Providing bone chips in the contact between the implant and the bone did not enhance vibration transmission.
Conclusion:
The mechanical point impedances and vibration transfer response functions indicate that the BCI implants integrate over time and that transmission conditions remain stable over time.
Hamidreza Taghavi
Bo Håkansson
Mans Eeg-Olofsson
Carina B. Johansson
Anders Tjellstrom
Sabine Reinfeldt
Tomas Bergqvist
Joakim Olsson

141
Bone-anchored hearing implant (Baha BI300)
loading at 3 weeks: stability and tolerability after
2 years
Introduction:
Earlier loading of bone-anchored hearing implants (BAHI) with the sound processor than the previously recommended 12 weeks after surgery provides a shorter waiting period for patients to benefit from their device. However, sufficient stability and tolerability of the implant before loading is essential for implant survival. Short-term results indicated 3-week loading to be safe, however, long-term effects are not yet known.
Method:
In this randomized, prospective clinical trial, 30 consecutive adult patients received the Cochlear Baha BI300. Implant stability quotient (ISQ) values were determined at implantation as a baseline. ISQ values were recorded during follow-up, together with skin reactions according to Holgers’ grading system, at 10 days, 3, 6, and 12 weeks, 6 months, and 1 and 2 years after implant surgery. Implants were loaded with the sound processor 3 weeks after implantation. Subjective benefit was gathered by means of the Glasgow Benefit Inventory (GBI) questionnaire.
Results:
One implant was lost before loading. ISQ values showed a dip 10 days post implantation followed by an increase to values higher than the baseline. Loading the implant showed no negative influence on ISQ values, which also remained stabile above baseline until 2-year post implantation. Skin reactions were observed incidentally over all visits (11.1%) and were generally mild (Holgers 1 in 10.1% and Holgers 2 in 1.0%). The GBI demonstrated subjective benefit.
Conclusion:
These 2-year data suggest that early loading of this BAHI 3 weeks post implantation in patients with good bone quality can be regarded as safe.
Myrthe Hol
Rik C. Nelissen
Hubert T. Faber
Catharina A.J. Dun
Cor W.R.J. Cremers
Emmanuel A.M. Mylanus
140
The burden of care of percutaneous BAHA:
Health economics analysis based on our 20 year
journey.
Introduction:
The literature on the cost-effectiveness of BAHA is scarce. There are no large studies addressing the health economics of the burden of postoperative care. Our skin response results focus on the long term burden of care for implant sites, with an emphasis on the health economics of maintenance and follow-up from both societal healthcare and patient perspectives.
Method:
We carried out a retrospective study of 430 patients from our skin response database over 20 years. Our outcome measures include cost of routine maintenance and the projected costs over the lifetime of the patient from both healthcare and patient perspectives. Considerations in the model include age, distance traveled, cost of travel, cost of visits when no issues present and cost of visits when unexpected events occur.
Results:
75% of patients had at least one unexpected events assessment(UEA). Of these events, 2/3rds were due to poor skin response with Holger’s grade 3 or higher. 20% were due to the processor. 3% were due to the implant. The cost of 4294 maintenance visits was C$944,680 and C$1,116,880 (with intervention from professionals). The cost to the patient was C$2,544.
Conclusion:
This observational study of the long term burden of care of BAHA patients has funding implications when setting up a proper maintenance program. We explore the implications for fully implantable or transcutaneous devices. We discuss future apps that might reduce the cost of maintenance.
Bill Hodgetts
Allan Ho
Amberley Ostevik

143
Audiological and quality of life evaluation of
Baha ® treatment - results of the multicenter
study
Full list of co-authors: W. Szyfter, L. Borucki, P. Dobosz, W. Domka, M. Drela, W. Gawecki, R.
Gibasiewicz, G. Grajewski, G. Horbacz-Jary, W.M. Iciek, A. Jankowski, D. Jurkiewicz, B. Kibilda, M.
Kida, D. Komar, J. Kusmierczyk, K. Maron, T. Matuszczyk, T. Mierzwa, J. Mierzwinski, E. Olszewska, K.
Przytula-Kandzia, M. Pyd, C. Stankiewicz, M. Stieler, A. Slaska-Kaspera, M.Wróbel, M. Zadrozniak
Introduction:
The aim of the study was to collect and evaluate the audiological and QoL results in patients implanted with Baha ® system in Poland.
Method:
17 ENT Departments in Poland performing Baha ® implantation participated in the study. 286 patients were registered in the database, out of which 155 underwent the audiological examination. Speech audiometry in noise (S:65dB, N: 10SNR) was performed preoperatively, at the day of loading the implant, 1 and 2 months after the first sound processor fitting. The Glasgow Benefit Inventory was completed for each patient 3 months after.
Results:
Patients were divided into groups according to the hearing loss: bilateral, unilateral mixed or conductive and single sided deafness (SSD). Preoperatively, the poorest speech in noise results were observed in the group with bilateral hearing loss on average, the speech in noise understanding was 34% (n=52), and the best were recorded in the group with SSD: 82% average speech in noise understanding (n=6). In the group with unilateral hearing loss (n=23) the speech recognition in noise on average was 59%. The Baha ® system improved audiological outcomes of all patients. The most significant benefit was scored in the group with bilateral conductive hearing loss an average benefit was 116% at the point of 2M after the first fitting. The best speech in noise outcomes were observed in a group with SSD: benefit of 35%. GBI questionnaires were sent to 101 patients and the response rate was 52%. The most significant change in health status was indicated by the patients with bilateral hearing loss (38 scores in total GBI scale; n=38).
Maciej Wrobel
A Long Term Multi-Site Study of the Safety and
Benefit Study of the SoundBite Hearing System
Introduction:
A new bone conduction device with a removable dental component (SoundBite) is functionally similar to surgically implanted bone anchored devices but eliminates the need for surgery. The purpose of this study was to determine the safety and benefit of this device over a 12 month period.
Method:
From 13 independent sites across the USA, 70 adults who were diagnosed with single sided deafness (SSD) and who elected to use the SoundBite device were enrolled under an Institutional Review Board protocol. At 6 months (N=63) and 12 months (N=24), each completed the Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire and a second questionnaire centered on SSD issues.
Results:
There were no serious adverse events. There were five minor issues ranging from a common superficial mouth sore to loss of a very old dental crown deemed unrelated to wearing the device and all were resolved after appropriate intervention. Mean APHAB scores improved significantly for ease of communication (p <0.001), background noise (p <0.001), reverberation (p <0.001) and global benefit (p <0.001). A high percentage of subjects reported communication improvement and overall satisfaction with the device.
Conclusion:
The SoundBite device is safe with regular use with no serious adverse events and only a small number of minor issues that were resolved. The SoundBite device also provides significant benefit at six and twelve months of regular use. Patient satisfaction with the device is high.
142
Gerald Popelka
Richard Gurgel
Clough Shelton

Magnetic Resonance Imaging and Temporal Bone
Implants: Paediatric considerations
Introduction:
Percutaneous Bone Anchored Hearing Implants (BAHI) are a widely accepted form of hearing rehabilitation but recent technological advances have led to greater choice of implant system. These include transcutaneous devices with magnetic components [Alpha 1 (Sophono, Bonebridge, (Medel)-paediatric license awaited] and Middle Ear Implants [Vibrant Soundbridge (Medel)].
Aim:
To identify the number of children with a percutaneous BAHI on a paediatric BAHI programme who would not have been eligible for a transcutaneous implant due to their need for Magnetic Resonance Imaging (MRI).
Method:
Retrospective case review of all children with a BAHI at the Birmingham Children’s Hospital (Jan 2009-Oct 2012). Review of all radiological procedures performed for each child before and after implantation.
Results:
206 children were identified with a BAHI. 49% had significant medical co-morbidities, predominantly neurosurgical, cardiac and syndromic abnormalities. 28% of this cohort had required one or more MRI scans. Other imaging modalities were not an appropriate alternative.
Conclusion:
A significant proportion of our tertiary paediatric center cohort would not have been eligible for these newer devices because of their need for MRI scans. The Alpha 1 device and MEI vibrant soundbridge are contraindicated for MRI scanning. The Bonebridge is MRI conditional up to a 1.5 Tesla MRI scan, however many centers use 3 and 7 Tesla MRI scanners. Since an MRI scan is the modality of choice in children, clinicians should be very mindful of the consequences of choosing these transcutaneous implants in the paediatric population particularly when other forms of hearing rehabilitation are available.
145
Sara Schneiders
Jayesh Doshi
Katherine Foster
Andrew Reid
Ann-Louise McDermott
144
MRI Scanning And Bone Anchored Hearing Aid
Insertion
Introduction:
With the introduction of abutment free bone anchored hearing aids (BAHA), the affect of implantation and subsequent contraindication to magnetic resonance imaging (MRI) must be considered. Magnetically coupled internal and external devices prevent future MRI scanning and therefore must be carefully considered during the patient selection process.
Method:
Looking at the entire cohort of patients who underwent a traditional BAHA fixture insertion with an abutment over 24 years at a tertiary ear nose and throat department in the West Midlands, we quantified the number of patients who had undergone an MRI scan both pre and post insertion. We not only searched for MRI scans at the tertiary centre, but also at two further local hospitals to improve the accuracy of our results.
Results: Of the 1405 patients, we have shown that a significant number of patients who underwent BAHA insertion with an abutment have subsequently had an MRI scan.
Conclusion:
We will highlight the main considerations when selecting patients for abutment free, magnetically coupled BAHAs, drawn from our research and results from the three local hospitals interrogated.
Elizabeth Ross
Chris Coulson
James Rainsbury
Observations on RFA results - to see more
Introduction:
Standard resonance frequency analysis is performed in two perpendicular planes to the implant, which register two ISQ values—maximal and minimal—which can occasionally be equal to each other. Higher ISQ value indicate a more stable system. However, different ISQ values in measured planes indicate that stability is not uniform, i.e. not symmetric in measured planes.
Method:
We analyzed the results of repeated RFA measurements over time from a series of 45 patients implanted with the Baha BI300 at the Department of Otolaryngology, Poznan University of Medical Sciences. Attention was focused on the differences between marginal (minimal and maximal) recorded values of ISQ in a single patient, defined as the average-ISQ value [(maximal ISQ value + minimal ISQ value)/2] and delta-ISQ (maximal ISQ value - minimal ISQ value)
Results:
The average-ISQ value increased from 58.43 at the time of implant placement to 61.89 at the end of the observation period, with a minimum recorded value of 56 and a maximum of 64.5. Delta-ISQ showed a maximal drop from 3.86 at the time of surgery to 1.93 after one month. Significant differences were observed between surgery and a month later, but also between one week and one month after surgery.
Conclusions:
Our data demonstrate that differences between recorded stabilities of the implant in different planes based on ISQ values tend to decrease over time, indicating that the implant acquires symmetrical stability, which may reflect the good quality of the bone-implant interface.
147
Maciej Wrobel
Wojcich Gawecki
Witold Szyfter
Oral Abstracts - LocalisationSaturday 8 June
11:15 - 12:15
Hall One

149
Baha-mediated rehabilitation of patients with
unilateral deafness: selection criteria
Introduction:
Patients with a single sided-deafness (SSD) can be rehabilitated by means of a BAHA device. However some patients are disappointed by this auditory implant or by preoperative tests if any. This study aimed at clarifying the reasons of BAHA refusal by some SSD patients.
Method:
All patients with a SSD eligible for a BAHA rehabilitation underwent preoperative specific auditory tests in stereo-auditorium (SAT). They were tested in noise with a simplified HINT test, the noise being in front at 60 dB, and Fournier-dissyllabic-word list addressed on the deaf side, with and without the BAHA device worn on a head band. The Glasgow Health Status Inventory (GHSI) questionnaire was administered. Patients refusing the implantation were given a specific questionnaire to explain the reasons of their refusal.
Results:
102 patients underwent the SAT over a 5-year period. The implantation rate was 29%. The improvement in understanding of speech-in-noise was 22% +/- 11% for patients agreeing to the implantation versus 13% +/- 11% for the others. Age, aetiology of deafness and duration of auditory deprivation had no influence on the implantation decision. The four principal reasons were: absence of perceived benefit during stereo-audiometric testing, requirement for surgery, cost of the solution, and aesthetics.
Conclusion:
Only the preoperative improvement in understanding of speech-in-noise from BAHA worn on a headband was predictive of the patient’s acceptance of surgical BAHA implantation.
Thierry Mom
Nicolas Saroul
Yoann Pavier
Mohamed Akkari
Laurent Gilain
148
Localization and speech performance in
SoundBite recipients
Introduction:
Utilizing the teeth versus an osseointegrated implant to transmit sound to the functioning cochlea, the SoundBite system is a non-surgical approach to overcome irresolvable conductive or profound unilateral hearing loss. Unique to this system is the microphone placement in the ear canal, potentially allowing for improved spatial hearing over traditional bone anchored implant (BAI) recipients.
Method:
Localization ability was prospectively studied in 3 SoundBite and 10 bone anchored implant recipients with single-sided deafness (SSD). A control group of 10 normal hearing subjects were included for comparison. Localization was assessed with and without device using an array of 24 speakers emitting narrow and broad band signals. The speakers span 360 degrees and are arranged in the horizontal plane with 19 front speakers separated by 10 degrees and 5 rear speakers separated by 30 degrees. Speech in noise performance was evaluated using the QuickSIN test materials.
Results:
A comparison of localization performance between the SoundBite and BAI system will be presented. Preliminary results indicate that the SoundBite system provides similar performance as compared to the BAI system for both localization and speech in noise performance.
Conclusion:
Patients with SSD receive significant improvement in speech in noise for both systems, but no improvement in localization. Microphone placement does not appear to impact localization ability in the SSD population.
Hillary Snapp
Fred Holt
Fred Telischi
Suhrud Rajguru

Localization outcomes of BAI recipients with
residual hearing in the profound ear
Introduction:
We previously reported on outcomes with bone anchored implants (BAI) in individuals with residual hearing and found that these patients may benefit under the single-sided deafness (SSD) indication. However, objective improvement was found to be independent of the amount of residual hearing and pre-operative word recognition scores. The purpose of this study was to investigate whether residual hearing contributes to improved localization performance in this population.
Method:
Localization ability was prospectively studied with and without device using an array of 24 speakers emitting narrow and broad band signals, spatially separated by 10 degrees in the front and 30 degrees in the rear. A comparison group of 10 SSD BAI users without residual hearing, and a control group of 10 normal hearing subjects were included for comparison. Subjective outcomes were reported using the Speech, Spatial, Qualities Scale.
Results:
A comparison of localization performance between the outcomes in patients undergoing BAI for SSD with residual hearing (< 90dB PTA) and BAI users without residual hearing (> 90dB PTA) will be presented. Preliminary data indicates that the residual hearing group reports improved localization and spatial hearing over the SSD BAI users. This is expected to be correlated to degree of residual hearing and will be assessed objectively.
Conclusion:
Individuals treated by BAI for SSD with residual hearing in the implanted ear report improved subjective spatial hearing. Objective localization ability may demonstrate improved performance by degree of residual hearing.
151
Hillary Snapp
Fred Holt
Daniel Zeitler
Fred Telischi
Suhrud Rajguru
BAHA cannot be expected to alleviate hearing
problems in subjects with USNHL
Introduction:
Individuals with unilateral sensorineural hearing loss (USNHL) have difficulties understanding speech from the affected side, perceiving speech in noisy environments and localizing sounds. BAHA are used by subjects with USNHL, but there is little evidence to show the efficacy of BAHA in the treatment. The aim of this study was to explore disabilities among adults with USNHL compared to subjects with good hearing, and to clarify whether there is theoretical base for the assumption, that BAHA would alleviate hearing challenges connected with USNHL.
Methodology:
The Danish version of the Speech, Spatial and Qualities of Hearing Scale (SSQ) questionnaire was filled in by 98 subjects with USNHL and 89 normal-hearing subjects. Results: The SSQ-ratings by subjects in the reference group were generally higher than in the USNHL group. Speech recognition in difficult situations, localization, and the estimation of distance from sound sources were rated significantly worse by the USNHL than by the normal subjects. Subjects from the USNHL group rated speech understanding in easy environments and sound quality no differently from those in the normal hearing reference group.
Conclusions:
Speech recognition in difficult situations, localization and distance estimation are partly or in full dependant on human functions that require inputs from two ears, and can therefore not be expected to be improved by the use of BAHA. Since subjects with USNHL already rate speech understanding in easy environments and sound quality equally high as normally hearing subjects do, these aspects cannot be expected to improve with the use of BAHA.
Steen Østergaard Olsen
Lotte Hagen Hernvig
Lars Holme Nielsen
150

Oral Abstracts - Sound SystemsSaturday 8 June
11:15 - 12:15
Hall Two
Sound Quality Differences Between Advanced Bone
Anchored Hearing Devices
Introduction:
Current BAHD users can choose between two similar devices. Patients perceive sound quality as an important factor in deciding between technologies, but little is currently known about sound quality in BAHDs. To date, no direct systematic measures of sound quality differences have compared these new devices, and a lack of blinded studies in previous work demonstrates the need for further study.
Method:
This study included subjects of three types: normal hearing listeners, non-power users, and power users (25 to date, 40 expected). Each subject was fitted with both Oticon and Cochlear BAHD´s according to manufacturer-recommended prescriptions for their individual loss. Normal hearing listeners were fitted with a flat conductive loss. Each programmed device was then used with a skull simulator to take three recordings (music, male & female speech), each at two stimulation levels (60 dB and 75 dB SPL). Recordings were normalized and post-processed to remove unwanted effects of the recording mechanism. Subjects were then presented with the randomized recordings via two custom-encased transducers (one from each manufacturer) and rated sound quality comparatively using a computer with sliders from 1 to 10 for each recording.
Results:
While this study is currently ongoing, results to date have demonstrated a small but significant difference between devices in both power and normal-hearing listener groups. No significant trends have emerged among the non-power users.
Conclusion:
These preliminary group results demonstrate a need for further study with an increased sample size to determine if these early differences are real or if they are an artifact of insufficient power.
152
Herman Lundgren
Bill Hodgetts
Tyler Wetter
Herman Lundgren
Amberley Ostevik

155
Understanding the feedback pathway in bone
anchored hearing solutions
Introduction:
In the last three to four years we have witnessed the introduction of newer Baha sound processors with advanced features and programming capabilities. Combined with this we have also seen the negative effects of mechanical and acoustical feedback also increase. This investigation documents the feedback in the Baha system and provides solutions on how it can be mitigated through measurements of individual feedback margin and adjustments in programming.
Method:
This investigation will use the measurement of open loop gain to determine the feedback margin of the Baha sound processor in a number of different situations. We will measure the effects of (a) type of feedback (acoustics, mechanical or skull radiation), (b) sound processor location (e.g. abutment, softband or non skin penetrating solution) and (c) signal processing configuration (e.g. microphone setting, or compression setting).
Results:
It is clear from the data collected that each situation affects the feedback margin differently. The two most important aspects of the individual’s feedback margin are the radiation of sound back from the skull and the method of attachment.
Conclusion:
The effect of feedback is more troublesome in a bone anchored solution than conventional hearing aids due to the nature of bone conduction, the location of the sound processor close to the skull and the variety of methods of attachment. To mitigate these aspects the introduction of individualised feedback measurements is an important clinical tool which should improve the experience for the patient.
Mark Flynn
154
A Clinical Study of Early Loading of the Oticon
Medical Ponto 4.5mm Wide Implant
Introduction:
The primary aim of this study is to assess implant stability, implant loss, adverse skin reactions and quality of life benefit following surgical implantation of the Oticon Ponto 4.5 mm osseointegrated auditory implant. The secondary aim is to determine the feasibility of early processor loading three weeks after surgical implantation and to investigate if there is a relationship between the type of post-operative skin reactions, demographic data of subjects (medication use/medical co-morbidities) and the surgical technique used for implantation.
Method:
This prospective, multicenter design study, will evaluate eighty adult participants 18 years or older who meet audiological and medical candidacy for a bone-anchored hearing system. They will undergo implantation of the Oticon 4.5 mm wide implant and a second 3.75 mm implant (sleeper implant). If not contraindicated, sound processor loading will occur three weeks later. Implant stability will be measured using Radio Frequency Analysis (RFA) at surgery, 1, 3, 6, 12, 26 and 52 weeks and Quality of life benefit will be assessed by the Glasgow Benefit Inventory at 3 and 12 months following surgery.
Results:
26 participants have been implanted thus far. Preliminary findings reveal comparable implant stability to previously published studies. There have been no implant losses and skin reactions are limited to grade 0 and 1 of the modified Holger’s grading scale.
Conclusion:
The preliminary findings appear to confirm the safety of early loading of the Oticon 4.5mm wide implant. Participants showed satisfaction with the earlier use of their processor with no added complications.
Jack Wazen
Seilesh Babu
Wayne Shaia
Julie Daugherty
George Poulos

Implant losses are more frequent in some
patients
Introduction:
The knowledge about implant losses in extracranial applications is still limited. This study examined the long-term survival, reason for implant loss and need for implant replacement in a large cohort with long follow-up.
Method:
Retrospective study on patients who had bone-anchored hearing aid (Baha) surgery between January 1977 and December 2011 were identified from operating lists. Data regarding all implant surgery were retrieved from patient records.
Results:
During the study period 571 patients underwent Baha surgery. Follow up time were up to 33 years, median follow up 6,6 years. We excluded 7 patients that had no notes. A total of 763 implants were inserted. Of these, 141 (18 %) implants were lost, 109 (14%) due to lost osseointegration, 21 (3 %) due to trauma and 11 were removed. 27 patients had one implant re-installation, while 5 patients had re-installation two times , 9 patients were re-installed three times and 5 patients were re-installed four to six times. Of 141 lost implants, 78 (55 %) were lost in patients having two or more implant losses and this group included 19 patients.
Conclusions/implications:
Within the study 14 % of the implants failed due to lost osseointegration. There is a small group of patients experiencing implant loss more frequently
157
Anna Larsson
Anders Tjellstrom
Joacim Stalfors
Improving speech in noise hearing performance of
users of the Baha(R) sound processor with wireless
accessories.
Introduction:
The key need of hearing impaired individuals is improved speech understanding in challenging listening situations. While, directional microphones provide an improvement, a new potential solution is wireless transmission technology to transmit the talker’s signal directly to the Baha sound processor. A new generation of DSP technology available in the Baha 4 sound processor incorporate the 2.4GHz ISM transmission technology to transmit the signal from remote microphone.
Method:
Patients (N=20) with a Baha system participated in this investigation. Each patient wore a Baha 4 sound processor paired to a 2.4GHz wireless microphone “mini-mic” worn by the talker. Testing took place in a isolated sound booth with two loudspeakers. The Swedish version of the HINT test was used to determine the 50% level of speech recognition in noise. Speech was presented from the front loudspeaker (0) with noise from the rear loudspeaker (180). Three test situations were conducted: (1) omni-directional microphone, (2) automatic directional microphone, and (3) a wireless microphone was placed 15cm in front of the front loudspeaker.
Results:
The wireless configuration demonstrated the largest benefit in hearing performance in noise. Additionally, subjective reports using a visual analogue scale (VAS) indicated that the participants found it easier to listen to the test material using the wireless accessory than with the conventional sound processor level microphone in this test situation.
Conclusion:
Results of the study conclude that sound processor incorporating wireless technology improve speech recognition in noise compared with conventional bone conduction sound processor. The clinical situations and implications of this new technology will be discussed.
156
Mark Flynn
Jenny Andersson
159
Integration of a skull simulator into a bone
anchored hearing aid clinical service
Introduction:
Globally, adult and paediatric programmes that provide bone anchored hearing aid services have been disadvantaged as there has been an absence of technical equipment to measure the force output produced by the range of bone anchored hearing aid devices that are available. Specifically, during the pre-operative phase, clinicians need to ensure that devices provided for trial periods are working according to technical specifications so that the patient experience is appropriate. The ability to provide quality assurance of sound processors when they are received from manufacturer is required to provide the clinician with assurance that they are working as intended and that it is not a potentially faulty processor. Further, the investigation of patient reported device faults is limited as no technical measurements can be made. This paper aims to introduce the first clinically accessible system which will provide a platform for clinicians to quality assure and validate device function thereby removing the inherent subjectivity which is currently employed by most services. This paper will report on how a skull simulator can be integrated in a clinical service with reference to the potential benefits and limitations.
Gary Norman
Stella Appleton
Nasir Rashid
158
The Mechanical Point Impedance of the Skin-
Penetrated Human Skull: A Comparative Study
Introduction:
Mechanical point impedance (MPI) of the skin penetrated human skull, due to its effect on Bone Anchored Hearing Devices (BAHD) behavior, is an important property to consider within design and prescription of BAHD´s. Previous work in this field includes relatively low sample size; Therefore, to increase our understanding of MPI, a comparative study was completed involving many subjects with differing etiologies.
Method:
Forty Five BAHD users with varying etiologies were coupled to a Bruel and Kjaer Type 8001 Impedance Head via Cochlear’s traditional snap coupling (12 subjects were also tested with Oticon’s coupler). A swept sine was presented to subjects through a BEST transducer at 401 logarithmically spaced pure tone frequencies (100 - 10k Hz). MPI was recorded via custom software and a National Instruments DAQ. Mass compensation was carried out using MATLAB.
Results:
The results obtained through this study agree with those demonstrated within the literature. Inter-subject variability was relatively low, with 95% confidence intervals around mean MPI of less than +/- 3dB over the tested frequency range. When various patient characteristics were considered (age, gender, etiology) slight differences in MPI were noted.
Conclusion:
The low variability found across subjects suggests that a mean MPI can be used as a reasonable estimate of individual MPI. The small differences found between inter-subject demographics demonstrate MPI as being a biomechanical property relatively robust to patient variability. Further study should include investigation into infant/child MPI, as developmental stages may play an important role in skull mechanics.
Herman Lundgren
Fausto Woelflin
Bo Hånsson
Bill Hodgetts
Dylan Scott

Poster Abstracts1 Case Study: A new application for Telemedicine -
the Bone Anchored Hearing Aid (BAHA)
2 Analogue and digital sound processing in boneconduction
devices
3 Surgical and audiological effectiveness of the
Baha system as a treatment for hearing loss
4 Audiological outcomes of the bone conduction system Bonebridge (Med-El) in single-sided-deafness cases
5 The impact of a reduced bone mineral density in the course of postoperative pituitary failure on an osseointegration process of a Baha system - case analysis
6 The Ponto implant: short-term retrospective data
on implant survival and subjective benefit
7 Patient Requested Explantations in Bone-
Anchored Hearing Devices
8 Clinical evaluation of a new concept of the
percutaneus bone conduction system with respect
to surgical technique and design of the abutment.
9 Baha System in C hildren with CHARGE-Syndrome
10 Three case reports of a redesigned Baha abutment
and simplified surgical technique
11 Bone-anchored hearing aids significantly reduce outpatient visits
12 Auditory rehabilitation by bone anchored implants in Charge syndrome: A case report
13 New, simplified implantation technique for the Sophono device
14 Outcome of Baha in patients with middle ear and outer ear pathologies
15 Objective quantification of bone conduction thresholds in Newborns using otoacoustic emissions
16 Bone anchored systems on softband for children with temporary conductive hearing problems and special needs.
17 Bone Anchored Hearing Aid, binaural equipment: Profit in percentage of discrimination in noise.
18 Wound healing & maturation: aetiological factors in BAHA fixture site skin reaction
19 TuLiD - Tullamore Life Style Descriptor: A dual centre evaluation.
20 Linear scalp sparing (LSS) approach: Early evidence of benefits
21 Effects on resonance frequency: human head compared to skull-simulator
22 A Non-ossicular Piezoelectric Middle Ear Implant: Feasibility Study
23 Single-Stage BAHA and Mastoid Obliteration
24 BAHA in the elderly -the closing gap towards cochlear implant
25 Decreased rate of complications with the use of the lateral linear incision
26 The Use of BAHA System in Infants with Bilateral Conductive Hearing Loss due to Ear Malformations.
27 Surgical and audiological evaluation of a new connective interface for Cochlear Baha
28 Patient Outcomes for a ‘Small but Perfectly Formed’ BAHA Service
29 Binaural hearing with bone conduction stimulation in normal hearing subjects
30 Hearing performance with two high-power Baha sound processors
31 BAHA® in children with bilateral aural dysgenesis. Our experience with 23 operated cases.
32 Evaluation of the surgery time, skin reactions, aesthetic outcomes and implant stability of two Baha® system models
33 The use of bilateral Baha® with soft band in a case of deletion 18q23
34 The Paediatric BAHA programme at Royal Manchester Children’s Hospital: An audiological overview of our experiences
35 Titanium fixtures for bone-conduction devices and the influence of type 2diabetes mellitus
36 Multiple Auditory Steady State Response Air-Bone Gaps in children with hearing loss.
37 Clinical assessment of Baha implants stability in children with craniofacial malformations
38 Upgrading BAHA patients - Clinical Experiences and Outcomes
39 Measurement of resonance frequencies of BAHA patients comparing different osteosysthesis systems
40 Amplification and speech and language development in children with atresia
41 The use of a daily alternating method in comparing two osseointegrated bone conduction implant sound processors in patients with single sided deafness.
42 World’s first DermaLock implantation in Goldenhar syndrome
43 Possible approaches of programming the BP100 sound processor in a group of patients with unilateral mixed hearing loss – partial results.
Nasal sound pressure measurements for
transcutaneous bone conduction stimulation
on normal hearing subjects
Introduction:
To objectively verify the functionality of a new Bone Conduction Implant (BCI) system in a patient during surgery before the wound is closed is of utmost importance. Previously it has been discovered that ear-canal sound pressure (ECSP) could be measured to verify the function of the BCI. However, the ear-canal is close to the surgical area and hard to reach, and some patients do not have ear-canals. An alternative measure is the nasal sound pressure (NSP). The aim of this study is to investigate NSP from bone conduction (BC) stimulation at two positions of the skull, and to compare it to ECSP.
Method:
Transcutaneous BC stimulation on both sides of the skull in 20 normal hearing subjects was used. The BC transducer was placed at the BCI position, as close to the ear canal as possible, and at the Bone Anchored Hearing Aid (BAHA) position. The NSP was measured with a probe tube microphone in a foam-plug inserted 8 mm both ipsi- and contralaterally. The ECSP was also measured close to the tympanic membrane for all stimulations, both ipsi- and contralaterally.
Results:
The NSP was higher ipsilaterally than contralaterally and higher for stimulation at the BCI position compared to the BAHA position. Furthermore, the NSP was generally higher than the ECSP.
Conclusion:
NSP is suitable as a verification test during BCI surgery. This has also been confirmed in surgery of the first BCI patient. The completely non-invasive NSP will also be used to follow-up the BCI implant over time.
160
Sabine Reinfeldt
Bo Håkansson
Hamidreza Taghavi
Mohammad Ghoncheh
MaryamShirinkar
Karl-Johan Fredén Jansson
Mans Eeg-Olofsson

Analogue and digital sound processing in bone-
conduction devices
Introduction:
In the last decennium sound processing in bone-conduction devices (BCD) has become digital instead of analogue. Other technical developments like directional microphones have further improve the BCD. However for directional hearing these modifications might have undesirable consequences. In this study we investigate the effects of digital sound processing and directional microphones on sound localization abilities.
Method:
Patients who are still using an analogue BCD (Baha compact or classic) are invited. After fitting of a digital BCD (Baha divino, bp100 or Ponto Pro) sound localization abilities of stimuli with different bandwidths (broadband 0.5-20 kHz, high-pass 3-20 kHz and low-pass, 0.5-1.5 kHz) is investigated. Stimuli are roved over a large range (45-65 dB SPL). Sound localization abilities are investigated in the unaided and aided condition and with different settings (omnidirectional, and directional). Subjects are also asked to adjust the sound level of their BCD. Our main interest is the time delay of about 3 to 4 ms in the digital devices.
Results:
Surprisingly, variations in device settings and alternations between the analogue and digital device only slightly affected sound localization abilities.
Conclusions:
We suggest that patients can adapt rapidly to these changes and that studying the underlying neural correlates is crucial to guide further modifications of BCDs.
Martijn Agterberg
Marc Van Wanrooij
Myrthe Hol
John Van Opstal
AdSnik
163
Case Study: A new application for Telemedicine -
the Bone Anchored Hearing Aid (BAHA)
Case Study:
A new application for Telemedicine - the Bone Anchored Hearing Aid (BAHA)
Introduction:
Telemedicine is defined by the World Health Organisation (WHO) as the practice of health care using interactive audio, visual and /or data communication i.e. internet. This includes healthcare delivery, diagnosis, consultation and treatment. The application of telemedicine appears to be gradually expanding. We present the first known documented case report detailing the role telemedicine, as electronic correspondence, assisting in the patient pathway for Bone Anchored Hearing Aid (BAHA) fitment and aftercare.
Method:
Patient was a 42 year old gentleman, treated at the Freeman Hospital (Newcastle Upon Tyne, UK). He suffered unilateral hearing loss post treatment for a posterior fossa ependymoma. Electronic consultation, at times including digital photographs, were used at each step of the BAHA patient journey due to the patient living over 350 miles away.
Results:
This case highlights the multiple potential benefits gained from appropriate integration of telemedicine in the BAHA journey. The benefits include; triage capability of potential BAHA candidates, reduction in number of appointments and e-correspondence acting as an information source for the patient.
Conclusion: Through appropriate integration of this method of communication benefits could be gained for both patient and NHS.
Cheryl Coulter
Ian Johnson
162

Audiological outcomes of the bone conduction
system Bonebridge (Med-El) in
single-sided-deafness cases
Introduction:
In single-sided deafness cases (SSD), the alternative to cochlea implantation is the treatment with CROS (Contra-lateral Routing of Signals) systems. The routing to the contra-lateral side can be done either with conventional hearing aids or with bone conduction hearing systems. Usually the later devices require a percutaneous fixation screw to feed the sound from the deaf side to the bone. The Bonebridge (Med-El), a new system with transcutaneous RF transmission, avoiding a percutaneous screw is CE marked and available on the market since 2012. In this study we investigated audiological outcomes in SSD patients with the Bonebridge.
Methods:
5 patients with SSD (SNHL 20 dB HL on the contra-lateral side), from the ENT Dept. at the Medical University Hannover, implanted with a Bonebridge were analysed retrospectively. All patients had tried out a bone-anchored hearing system before surgery. Tests included unaided and aided AC thresholds and Freiburg monosyllables recognition scores at 65 and 80 dB SPL in sound field with the contra-lateral ear blocked. Speech intelligibility in noise was tested using the Oldenburg speech-in-noise-test and subjective benefit was assessed with the APHAB.
Results:
Mean aided thresholds in sound field audiograms with the Bonebridge were 24 dB HL (PTA, 0.5 - 4 kHz). Monosyllable scores at 65 dB SPL were improved by 71% compared to unaided. Our results demonstrate that the Bonebridge is a realistic alternative to percutaneous bone conduction instruments in the treatment of SSD.
Thomas Giere
Burkard Schwab
Rolf Benedikt Salcher
Hannes Maier
ThomasLenarz
165
Surgical and audiological effectiveness of the
Baha system as a treatment for hearing loss
Introduction:
To evaluate the surgical and audiological effectiveness of the Baha system in patients with conductive as well as mixed hearing loss and sudden sensorineural deafness (SSD).
Methods:
Thirty two patients with different types of hearing loss (conductive n=1, mixed n=31 and SSD n=2) were included in this study. PTA and speech recognition were measured. The average age of patients was 55 years (range: 23-80 years). The implantation was performed in general (n=15) and local anaesthesia (n=19) using dermatome technique (n=25) as well as the linear incision (n=9). There were two patients implanted bilaterally. Two patients were implanted using implants with hydroxyapatite. Patients were fitted 2 weeks to 3 months after Baha surgery.
Results:
The wounds in most patients healed without any complication. The only issues observed in the postoperative care concerned overgrowth of the subcutaneous tissue (n=1), a staphylococcal infection in a patient with diabetes (n=1), a numbness and hypoesthesia of the skin around the implant (n=3) and temporary headaches around the site of implantation (n=1). An improvement in speech discrimination in 80% of patients was observed. The patients subjectively evaluated an improvement of hearing after Baha surgery they assessed it on average as 7,56 in a ten-point scale. Twenty one patients reported an improvement in quality of life associated with hearing.
Conclusion:
Patients implanted with Baha system experienced a benefit in quality of live as well as the improvement in speech recognition. No difference has been observed in the length and healing process between incision techniques.
Ewa Olszewska
Justyna Rutkowska
Marek Rogowski
164

167
The Ponto implant: short-term retrospective data
on implant survival and subjective benefit
Introduction:
This report provides short-term follow-up data on the Ponto bone-anchored hearing implant (BAHI) from our tertiary referral center.
Method:
Thirty-one consecutive patients with a mean age of 51 years who received the 3.75-mm implant between October 2010 and December 2011 were included retrospectively in this study. Implant loss, skin reactions around the implant (according to Holgers’ grading system), revision surgery, and abutment replacements were retrospectively gathered from the patients’ files as objective outcome measures. To obtain information on subjective patient satisfaction, the Glasgow Benefit Inventory (GBI) was used.
Results:
The mean follow-up period was 16.9 months (range, 12.1-25.2 months). One implant was lost. Over a total of 94 follow-up visits, 21 skin reactions were observed in 16 patients; Holgers grade 1 (slight redness, no need for treatment) in 18.1% of the visits, and grade 2 (redness and moist, needing conservative treatment) in 4.3% of the visits. Four 6-mm abutments (12.9%) were replaced for a 9-mm abutment during the follow-up period, of which 1 (3.2%) in combination with revision surgery. In 1 patient keloid formation around the implant was observed. The GBI revealed a moderate subjective benefit.
Conclusion:
The short-term results with these percutaneous implants demonstrate a clinically stable implant with a low percentage of skin reactions that require treatment. Long-term, prospective follow up data are needed to draw more firm conclusions.
Rik Nelissen
Emmanuel A.M. Mylanus
Henricus P.M. Kunst
Ronald J.E. Pennings
Ad F.M. Snik
Myrthe K.S. Hol
The impact of a reduced bone mineral density in
the course of postoperative pituitary failure on
an osseointegration process of a Baha system -
case analysis
Aim:
The evaluation of the impact of reduced bone mineral density in the course of postoperative pituitary failure on an osseointegration process of Baha.
Method:
It is a clinical case study of one patient (woman, 63 years old) with sensory-neural hearing loss implanted with the Baha implant. The patient with a history of pituiarity gland tumor, after pituitary surgery followed by pituitary insufficiency (diabetes insipidus, hypothyroidism). Afterwards, the treatment of supplementing the glucocorticoids, thyroid hormones and vasopressin analogues was performed. The patient is not subjected to hormone replacement therapy due to the menopause. Osteopenia is also verified in bone density examination. The first fitting session was planned 2 weeks after the Baha surgery. The implant stability was measured intraoperatively, 2 weeks after surgery and 2 and 4 months after the surgery. Results: The surgery was performed using a dermatome technique. The implant was placed in the third hole due to the bleeding from the two preceding ones. The implant stability quotient measured intraoperatively was on average 52. At the time of planned implant loading, 2 weeks after the surgery ISQ was 40, therefore athe sound processor loading was delayed. The next ISQ measurement (2 months after surgery) allowed to conduct the first fitting session.
Conclusion:
In spite of some problems with implant stability at the beginning of treatment, an increase of ISQ values in time was observed. A reduced bone mineral density in the course of postoperative pituitary failure has an impact on the implant loading time.
Grzegorz Jamro
Malgorzata Szymanska
Krzysztof Maron
166

Clinical evaluation of a new concept of the
percutaneus bone conduction system with respect
to surgical technique and design of the abutment.
Methods:
Twenty patients divided into two groups were included in the study. Ten patients of Group I received Cochlear BI300 implants and the other ten subjects of Group II were implanted with Cochlear BIA400 (with Hydroxyapatite coated abutment). The implantations in both groups were performed using linear incision techniques. The surgery techniques in Group I included soft tissues reduction, and in the Group II was performer without the this stage. The surgery time for both groups was recorded. Implant stability quotient (ISQ) using resonance frequency analysis was scored in both groups at the time of the surgery, sound processor loading, 1 and 3 months post-surgery. The assessment of the soft tissue reactions was performed using Holgers scale and the aesthetic outcomes were evaluated by surgeons according to the POSAS scale. The pain and discomfort around the implant was observed with the Visual Analogue Scale. Sound processor loading was performed at 4 weeks in the Group I, and 2 weeks post-surgery in Group II.
Results:
There was a significant difference observed in the surgery time between two groups. According to the POSAS scale, the aesthetic outcomes were significantly better for the patients in Group II. Additionally, the data gathered in Visual Analogue Scale indicate less pain and discomfort in Group II.
169
Maciej Wrobel
Wojciech Gawecki
Lukasz Borucki
Tomasz Pastusiak
Witold Szyfter
Patient Requested Explantations in Bone-
Anchored Hearing Devices
Introduction:
Between 2006 and 2012, we have implanted 261 bone-anchored hearing devices. Although our success rate and high patient satisfaction outweigh the complications we have experienced, some patients have requested explantation as they no longer desired to use their bone-anchored system. The purpose of this study is to analyze the underlying reasons for patient dissatisfaction that prompted their request for abutment removal (explantation).
Method:
Retrospective chart review revealed five of the 261 patients (2%) requested abutment removal. The abutment was removed in the office and the implant was left in place to be slowly covered by the surrounding skin. Clinical and audiological data on this group of patients were collected. A summary of the reasons patients provided for their decision to terminate use the bone-anchored system was developed.
Results:
Four of the patients requested explantation due to lack of audiological benefit and one patient suffered chronic local skin reaction and desired removal. Brief case histories will be presented.
Conclusion:
The information gained from this study can be utilized by the surgical team to help improve patient selection and patient education of bone-anchored hearing recipients. It will also provide valuable feedback to the manufacturers of osseointegrated auditory implants for product enhancement.
168
Jack Wazen
Julie Daugherty

Three case reports of a redesigned Baha abutment
and simplified surgical technique
Introduction:
Recently, Cochlear Bone Anchored Solutions AB introduced a Baha hydroxyapatite-coated abutment (BA400) accompanied by a surgical technique without skin thinning. This combination aims to enhance biocompatibility and to reduce complications such as skin inflammation whilst improving the cosmetic result and saving surgical time. Here we present our first experiences with this surgical procedure and follow up of three patients. Moreover we introduce a tool to study the abutments bacterial flora.
Method:
Surgical time, complications, and photographs for the assessment of the cosmetic result were collected in a prospective manner. IS-pro, a novel PCR-based rDNA-interspace region molecular fingerprinting tool will be applied to profile the complete microbiota surrounding the abutment. Not limited by conventional diagnostics in microbiology, it is now possible to determine the species and quantities of the bacteria which colonize the abutment.
Results:
Research shows that hydroxyapatite-coatings may result in an increased skin-implant integration. Recently, Larsson et al. have shown that hydroxyapatite-coated abutments might reduce epidermal downgrowth and pocket formation, which in turn could inhibit the resulting bacterial accumulation, biofilm formation and inflammation. Here we present the bacterial profile of this process around the patients’ abutments which enables an in depth analysis. Additionally, in our experience, the modified surgical technique described by Hultcrantz on average takes 16 minutes (20,13,14) with good cosmetic results.
Conclusion:
Although it is too early to draw conclusions about the improved biocompatibility and complication rates, the surgical results and the use of IS-pro seem promising.
171
Marc Van Hoof
Joost van Tongeren
Janny Hof
Robert J Stokroos
Baha System in Children with CHARGE-Syndrome
Introduction:
Children with CHARGE syndrome (CS) present with a cluster of features including coloboma, heart defects, choanal atresia, retardation of growth or development, genital hypoplasia and ear anomalies (external, middle and inner ear). Hearing-loss in patients with CS can be conductive, mixed or sensorineural.
Method:
Six children with CS referred to our tertiary service for management of hearing-loss were identified for further analysis. Subsequently four of these children were fitted with a bone conduction implant (Baha(R) system) and two underwent cochlear implantation. For the four Baha(R) system children free-field speech audiometry was used to monitor hearing post-operatively. For three of the children Baha(R) system stability was measured with resonance frequency analysis at surgery and sequentially at follow up visits.
Results:
Four cases of Baha(R) system implantation in children with CS are discussed including pre-operative assessment/selection criteria, scans and surgical planning; operative challenges; implant stability post-operatively and hearing benefit. The mean age at surgery was 9 years 11 months (4 years 9 months to 14 years 10 months) and mean follow up was 18 months (6 months to 25 months).
Conclusions:
Children with CS and mixed hearing-loss are challenging when considering how best to maximise hearing potential. Some children with CS will also have external ear abnormalities potentially limiting the use of conventional BTE HAs. Bone conduction implants are an effective hearing solution for selected children with CS and the introduction of no soft tissue reduction’ bone conduction implant techniques has important implications in these children with existing craniofacial dysmorphism.
170
Mark Felton
Penny Feltham
Rachel Andew
Michael Rothera
Iain Bruce

173
Auditory rehabilitation by bone anchored
implants in Charge syndrome: A case report
Introduction:
Charge syndrome (CS) often results in multiple physical, sensory, and behavioral deficits ranging widely in degree of severity. As such, prognosis for development is often tentative in early years making intervention planning difficult. Presented is a case of bilateral hearing loss (HL) in CS demonstrating significant expressive and receptive language improvement with bone anchored implantation (BAI). The challenges of diagnosing and rehabilitating HL will be discussed.
Method:
Single case study retrospective chart review of a 5 y/o female with CS initially presenting with unintelligible speech and minimal receptive language. Audiometrics resulted in right conductive HL and left profound sensorineural HL, however, patient failed to respond to hearing aids. Trial with softband was well tolerated by the patient and speech and language was observed to improve. Surgical and audiometric outcomes are reported and video representations will be provided.
Results:
Six months post BAI activation patient is communicating in both English and Spanish. PBK testing at 60dBSPL resulted in 100% WRS in quiet and 72% with +10dB signal to noise ratio (SNR). BKB SIN testing done in noise revealed SNR loss improvement from unaided (13.5dB) to aided (3.5 dB). There were no surgical complications or failure of osseointegration.
Conclusion:
Patient is thriving academically and socially and Auditory Verbal Therapy reports significant improvements in expressive and receptive language. In pediatric cases where contributing deficits may complicate diagnosis and rehabilitation, BAI may assist in differential diagnosis and improve rehabilitation outcomes.
Hillary Snapp
Alina Lopez
Karalee Needleman
Fred Telischi
Bone-anchored hearing aids significantly reduce
outpatient visits
Introduction:
Bone-anchored hearing aids (BAHAs) are used for a number of indications. These include congenital ear canal atresia or acquired stenosis, recurrent ear infections, hearing aid induced otorrhoea and otosclerosis. We carried out a retrospective case series to evaluate the number of post-BAHA clinic encounters for otorrhoea compared to the pre-operative period.
Method:
We reviewed all patients given BAHAs at our tertiary referral centre from 1994-2011. Patients were identified from our BAHA multidisciplinary team (MDT) database. Notes were retrieved from medical records. All clinic encounters for otorrhoea for a one-year period prior to BAHA surgery were recorded. This was repeated for 18 months following surgery, the first 6 months were excluded to account for post-operative confounding variables.
Results:
A total of 124 patients had received a BAHA. Approximately 40% of these patients were excluded (reasons included lack of paper notes or BAHA indication other than otorrhoea). The average age of those included was 56 years (range 21-76 years). 55% of patients were female. The mean number of clinic visits, per patient in the year prior to BAHA was 2.70 (95% CI 2.10- 3.29). Following BAHA switch-on, the mean was 1.47 (95% CI 0 .85-2.10). The difference was statistically significant (p=0.005). Following the introduction of a BAHA MDT meeting in 2005 the significance increased (p=0.002).
Conclusions:
The fitting of a BAHA in patients with chronic or recurrent otorrhoea results in a statistically significant reduction in clinic visits. This results in improved clinic efficiency and decreased costs while notably decreasing patient morbidity.
172
Shaun Davey
Sachin Patil
Junaid Hanif

175
Outcome of Baha in patients with middle ear
and outer ear pathologies
Objective:
The objective of this study was to evaluate the functional results of the Baha bone anchored hearing system in patients with outer and middle ear pathologies.
Method:
A retrospective review of patients who received the Baha bone anchored hearing device at Çukurova University between 2006 and 2012. Pure-tone audiometry and speech audiometry test results were recorded and are compared to patients who did not receive the Baha device.
Results:
Twenty two patients aged between 6-56 years – 16 females and 6 males – were included in this retrospective study. All patients had middle ear or outer ear pathologies. Three millimetre implants were used in 11 of the patients and four millimetre implants were used in the other 11 patients. Mean pure-tone audiometric thresholds and speech audiometry tests results are presented. A significant improvement in hearing level performance was noted for those recipients who received the Baha device, when compared to those patients who did not. No difference was noted in level of performance based on the implant size.
Conclusion:
The Baha bone anchored system is a reliable method of auditory rehabilitation and significantly improves hearing performance for patients with middle ear and outer ear pathologies.
Ozgurr Surmeli
Ülkü Tuncer
Özgür Tarkan
Süleyman Özdemir
Fikret Cetik
Mete Kiroglu
Funda Akar Atik
Nilay Tezer
New, simplified implantation technique for the
Sophono device
Introduction:
We have developed a new partially implantable BCHD without a percutaneous abutment and have been using it clinically for seven years now. The principle of this BCHD is a magnetic coupling and acoustic transmission between implanted and external magnets. Now we have developed a new, simplified implantation technique, which can be followed by an early fitting of the external device.
Method:
The surgical procedure can be performed under local anesthesia. Two curved incised all the way down to the bone, 5 cm apart from each other, are performed in the temporal region next to the planned position of the implant. Then subperiosteal elevation between the incisions is done with a rasp. The implantable double-magnets are placed up-side-down onto the bone, fixed with 4 micro-screws and the incisions are closed with a running fast absorbable suture. An external base-plate of the device is used as a slight pressure bandage. The primary fitting of the hearing device can be done on the day of surgery.
Discussion:
After having performed more than 150 implantations with the oldtechnique we have now been using a new, very simple technique for the implantation. It can be performed under local anesthesia, it takes only about 15 min and the primary fitting of the hearing device can even be done on the day of surgery. To the best of our knowledge it is the fastest and easiest implantation technique ever being described for any type of implantable hearing device.
174
Ralf Siegert

Bone anchored systems on softband for
children with temporary conductive hearing
problems and special needs.
Introduction:
Some children with cleft palate, Trisomy 21 and other syndrome cannot undergo surgery for tubes for different reasons, such as recurrent infections, ear canal too small, and contra-indication for anaesthesia. In the past, we have prescribed conventional hearing aids but have encountered different problems, such as delays in getting the aids and adjustments needed due to hearing loss fluctuations. Our goal is to give those children access to auditory stimulation using a bone anchored system on softband.
Method:
When a significant conductive hearing problem is identified and the child is not eligible for PE tubes insertion within 3 months, the family is offered to use a bone anchored system on softband while awaiting medical intervention. Regular audiological follow-up is provided. Questionnaires are used to measure the benefits of this program.
Results:
So far, 19 children have benefit from this program. Most parents report regular use of the device and observe significant change in their child’s reaction to sound.
Conclusion:
Using a bone anchored system on softband has proven to be a solution for children with temporary but persistent conductive hearing problems. Compare to conventional aids no adjustment is required with hearing loss fluctuations and manipulation is easier for parents. Risk of over-amplification is also avoided.
177
Anne Marie Foget
Suze Julien
176
Objective quantification of bone conduction
thresholds in newborns using otoacoustic
emissions
Introduction:
Background Measuring hearing thresholds in newborns requires objective methods that base on thresholds of adults. However, there is evidence that bone conduction thresholds in newborns differ from thresholds of adults. This might result in inadequate interpretation of these measurement and of possible hearing loss.
Method:
Distortion product otoacousitc emissions (DPOAE) were elicited in newborns with combined air (f1) and bone conduction (f2) stimulation (ratio f1:f2 = 1:1.22) for the frequencies 850, 1000, 2000 and 4000 Hz. Sound pressure for f1 was kept constant at 60 dB HL, while f2 was increased from 40 dB HL to 70 dB HL. These results are compared the combined DPOAE of normal hearing adults.
Results:
Depending on frequency, bone conduction hearing of newborns differs from bone conduction hearing of adults.
Conclusions:
The differences in skull shape and the open fontanella could be responsible for these differences. Care must be takten in interpretation of bone conduction thresholds in newborns.
Christof Roosli
Bjoern Christian Fausch
Jae Hoon Sim
Rudolf Probst

179
Wound healing & maturation: aetiological factors
in BAHA fixture site skin reaction
Introduction:
Fixture site skin reactions are the commonest factors complicating per cutaneous BAHA management. We review the factors generally considered to be contributing to fixture site skin instability and analyse a patient cohort to assess the model.
Method:
A review of 100 OII procedures was performed to determine The incidence of Holger’s II/III reactions within our cohort, and Individual case analyses evaluated in terms of dermatological history, an arbitrary wound maturation timeline of 6 months and clinical fixture site assessment.
Results:
Holger’s II/III occurred in X%. The case analyses yielded profiles which indicated one or more events occurring principally within the interval of 6 months following surgery. In most there were associated historical dermatological factors including keloid, dermatitis or syndromal (Down’s). These cases demonstrated common features of delayed maturation of scar tissue with protracted erythema, hypertrophy and capacity for shearing.
Conclusion:
The potential for advanced skin reactions may be predictable on the basis of dermatological history. Features of delayed scar maturation, including a hypertrophic gel matrix with capacity for horizontal shearing prior to condensation of the tissue, results in an unstable skin/fixture interface.
Howard Savage Jones
Theresa Frawley
Bone Anchored Hearing Aid, binaural
equipment: Profit in percentage of
discrimination in noise.
Introduction and Objectives:
Ensure that patients with binaural equipment achieve greater benefit with BAHA devices and quantify the percentage gain on discrimination in noisy enviroments.
Design:
Retrospective descriptive cross-sectional case Venue: Instituto superior of Otolaryngology, Centro Medico Belgrano. Federal Capital. Argentina Materials and Methods: Six patients implanted with the BAHA system between May 2010 and December 2012. The hearing tests used to measure were conventional audiometry and speech audiometry. We evaluated the directional hearing, speech reception in quiet and in noise with diferents masking hearing levels in free field tested uni and bilaterally. All patients were also tested with life quality questionnaries.
Results:
The percentage results in the binaural hearing mode were positive and higher in noisy environments into three categories: directional hearing, binaural hearing and environment soft sound detection. The quality of life tests revealed that 100 percent of the patients reported an improvement and recommend its use. Were found remarkable benefits in the use of bilateral devices.
Conclusions:
Our results show that using the BAHA binaural equipment increases performance and hearing abilities in noise and it is associated with a marked improvement in the patients life quality. This improvement is both caused by bilateral stimulation and by the implied benefit provided by the hearing stereoacsia summation effect.
178
Fernando Javier Diamante
Gisela Fernanda Eldahuk
Julia Saslavsky

181
Linear scalp sparing (LSS) approach: Early
evidence of benefits
Introduction:
A desire to avoid the cosmetic and sensory changes associated with soft tissue reduction (STR) techniques has prompted a change to a scalp sparing approach to OII surgery. We review our early experiences.
Method:
We have conducted a prospective study of patients having an LSS approach and compared initial results with a retrospective review of a cohort who underwent STR techniques.
Results:
Immediate: Reduced surgical time c15minutes under LA Reduced analgesia requirements <24hours post op Prompt wound healing with minimal reaction Delayed: Scalp sensation conserved Cosmetic defect absent Alopecia absent
Conclusion:
The benefits of immediate and delayed effects of surgery are self evident. There is potential for reduction in incidence of Holger’s II/III tissue reactions due to reduction in tissue trauma/loss and consequent diminution in scar tissue production. In the rare event of the patient requiring indefinite abutment removal, a minimum of cosmetic consequence will be evident.
Howard Savage Jones
Theresa Frawley
TuLiD - Tullamore Life Style Descriptor: A dual
centre evaluation.
Introduction:
The TuLiD is a BAHA specific quality of life assessment tool developed for qualitative evaluation of derived benefits. A previous pilot study has been reported and now the results of a dual centre review are presented.
Method:
100 patients, randomly derived from two centres were sampled and reviewed using TuLiD pre and post operatively. 50% had single sided deafness. Results: 95% of patients reported a positive subjective benefit at 6 months post op.
Conclusion:
The tool provides reproducible evidence for the benefits of BAHA. It also helps identify patients with SSD who may require enhanced rehabilitative support to optimised their use of BAHA.
180
Howard Savage Jones
Shyam Singam

183
A Non-ossicular Piezoelectric Middle Ear Implant:
Feasibility Study
Introduction:
Conductive and/or sensorineural hearing loss patients with absent ossicles and a severely damaged middle ear and/or recurrent middle ear infections have limited treatment options. To address this need we have developed a non-ossicular piezoelectric middle ear implant and tested its feasibility in human temporal bones. The implant consists of a 3x5x1mm piezoelectric cantilever that is bonded to the cochlear promontory where it acts to compress the otic capsule. The intended mechanism of sound perception is displacement of the inner ear fluids due to cochlear compression.
Method:
In our experiment, the device was bonded to the cochlear promontory with glass ionomer cement following a wide posterior tympanotomy. The performance of the implant (with disarticulated incudo-stapedial joint) was compared with that of the healthy middle ear presented with 80 dB sound stimulation at frequencies in the range of 250 Hz - 8 kHz.
Outcome measures:
The round window (RW) center velocity, RW volumetric velocity and the RW vibration pattern in response to device actuation and sound stimulation were measured using a 1D scanning laser Doppler vibrometer. Average RW velocity and volumetric velocity in response to the implant was 8 dB lower than for sound stimulation up
to 1 kHz but exceeded motion for sound stimulation at higher frequencies. Comparison of round window vibration pattern showed qualitative similarity between the device and acoustic stimulation. The initial results demonstrate the feasibility of the implant and warrant further assessments of basilar membrane motion, improvement of the device design and development of better surgical implantation procedures.
Akhilesh Kotiya
Manohar Bance
Rob Adamson
Effects on resonance frequency: human head
compared to skull-simulator
Introduction:
Measuring bone anchored hearing systems (BAHS) on a skull-simulator reveals a transfer function quite different from what is known in air-conduction hearing aids. BAHS transducers show a distinct resonance peak in the mid-frequency range. To ensure good sound quality in BAHS it is necessary to optimally suppress this resonance. A challenge in developing BAHS is the design of filters compensating this resonance when the BAHS is placed on the human head. For investigating how BAHS’s behave on human heads compared to a skull simulator, series of measurements have been conducted on a skull simulator and on test patients with specially designed measurement probes. For the probes, accelerometers are mounted to vibrators counter weights. Knowing the mass of the counter weight and applying Newton’s laws of motion, the force input to the vibratory system can be measured. It will be shown how the resonance frequency of individual vibratory systems differ depending on vibrator type and attached mass. Measurements on human heads reveal a lower resonance frequency compared to skull simulator measurements. The average shift in resonance is dependent on the vibrator type. For each vibrator type a large variance can be observed depending on the load. Results show that a shift in resonance frequency and amplitude occurs when placing a BAHS on the skull simulator compared to a human head. This shift is highly dependent on the utilised vibrator type and on the individual’s head.
182
Patrick Maas
Jens Christian Sahl
Bengt Bern

185
BAHA in the elderly - the closing gap towards
cochlear implant
Aim:
Hearing impairment will increase dramatically in the elderly over the next years due to increased life expectancy. Changes are taking place not only in the periphery but also in central auditory pathways and in the brain. Reaching profound hearing loss cochlear implantation is considered. However this procedure could not be recommended in all old patients, esp. these with severe cardio-vascular risk factors and signs of central degeneration. A group of patients undergoing BAHA-implantation instead of CI will be demonstrated with promising results.
Method:
Five patients 75y and older with severe hearing loss and poor speech perception were evaluated. All had previous middle ear surgery and a bone-air gap. They also had a history of cardiac problems or stroke with high risk for longer surgery. All were implanted uni- or bilateral and recovered soon.
Results:
After a period of five weeks the processor was activated and speech perception tests performed. All patients reported easy handling with the processor and sufficient speech recognition.
Discussion:
Older patients not only suffer from hearing loss but also from impaired intellectual performance and learning capacity. If they also are high risk patients for extended surgery BAHA instead of CI should be considered. The promising outcome demonstrates that BAHA might close the gap between conventional hearing aids and CI.
Bertrand Gloddek
Single-Stage BAHA and Mastoid Obliteration
Introduction:
A single-stage fitting of a bone-anchored hearing aid (BAHA) implant and abutment with mastoid obliteration both obviates the need for two separate procedures and utilises the BAHA soft tissue reduction in the mastoid obliteration. Such a procedure has good outcomes in terms of osseointegration and achieving a dry ear.
Method:
We present a 6-patient case series report highlighting the technique of combined BAHA insertion and mastoid obliteration in six patients. All patients underwent the combined procedure described above and were followed up every 3 months for one year. Their hearing thresholds and reports of ear discharge were noted upon follow up.
Results:
All patients at twelve-month follow-up have a good degree of sound localisation and hearing thresholds with their BAHA and are free from the social stigma associated with a foul smelling discharging ear.
Conclusion:
The combined procedure of mastoid obliteration and BAHA abutment insertion is a successful procedure giving an excellent outcome of both improved hearing and a dry ear.
184
Elizabeth Ross
Ajith George
Chris Coulson
Ranit De

The Use of BAHA System in Infants with Bilateral
Conductive Hearing Loss due to Ear Malformations.
Aim:
Our aim is to describe the results of the Audiologic National Programme in Argentina for early detection of hearing loss in a Terciary Pediatric Public Hospital.
Method:
A total of 740 newborns were evaluated to detect hearing loss from March 2011 to November 2012. Average age: 15 days (range 5-60 days). Bilateral aural dysgenesis was diagnosed in 14/740 ( 2 % ) infants. All of them were evaluated with: Audiological BERA (Brainsten Evoked Response Audiometry), Audiometry free field tests and Ling detection test.
Results:
Sensorineural hearing loss was diagnosed in 36/740 cases (5%). Bilateral moderate conductive hearing loss was confirmed in all patients with dysgenesis bilateral. So far, all of them have been using BAHA devices with softband. Average age at fitting the infants was 7.9 months (range 2-25 months).Minimum period of using the softband was 3 months.
Conclusion:
All infants being early treated with BAHA show an improvement of the hearing threshold in the audiometry free field, and in the detection of the 100% of the Ling test. Early fitting of the soft band show a natural adaptation in infants, none of them having rejected it so far.
187
Maria Angela Silva
Patricia Sommerfleck
Maria Eugenia Prieto
Silvia Noemi Breuning
Guillermo Morales
Laura Graciela Quantin
Ruben Santiago Draghi
Patricia Cristina Bernaldez
Decreased rate of complications with the use of
the lateral linear incision
Introduction and Objectives:
Since in 1977 introduced the use of osseointegrated hearing implants, surgical techniques have gradually modified and simplified. The objective of this work is to verify that the choice of the linear incision eccentric decreases the complication rate.
Design:
Cross-sectional retrospective Location: Higher Institute of Otolaryngology. Federal Capital. Argentina.
Method:
80 patients were evaluated over a period of six years which included adults and children. It took into account the use of different techniques used, such as using dematomos, Omega incision and currently used linear abutment eccentric with a 1cm cut. Intraoperative complications were evaluated as flap injuries, blood loss and difficulties of different techniques. Postoperative complications were evaluated, thickening of the skin, infection of the abutment, cranial paresis, persistent pain and failure of osseointegration. The postoperative skin complications are classified according to scale Holgers.
Results:
Comparing surgical techniques, the linear incision is the one with a lower complication rate, while the Linear Eccentric, presents even lower than the linear medial complications.
Conclusions:
The use of eccentric linear incision decreases the complication rate significantly reducing times mainly surgical and post-surgical scarring in the flap. Key words: linear incision BAHA-eccentric
186
Fernando Javier Diamante
Fernanda Gisela Eldahuk

Patient Outcomes for a ‘Small but Perfectly Formed’
BAHA Service
Introduction:
Bone Anchored Hearing Aids (BAHA) have been fitted at Wrexham since 1998. The Service provides BAHAs to ten new patients each year. The service uses a multidisciplinary team approach, has a peer support user group and offers annual review to BAHA users. Recent discussions within BAHA professional circles has raised the issue of the appropriateness of relatively small centres (<15 cases/year) providing BAHA services. Methodology: Outcomes for BAHA users are measured and collected at regular intervals. IOI-BAHA, an adapted version of the IOI-HA questionnaire, is used along side site Reaction and Thickness Scores.
Results:
• 85%ofBAHAusersreportusingtheirBAHAformorethan8hoursaday
• 90%reporttheBAHAhelpedthemeitherquitealotorverymuch
• 75%reporttheyareleftwithonlyslightornodifficulty
• 95%reporttheBAHAisverymuchworththetrouble
• 86%reportthat,withtheBAHA,theirresidualhearingdifficultieshaveonly slightly affected or not affected at all the things they can do
• Lessthan3%reporttheirresidualhearingdifficultiesmorethanmoderately bothered others
• Morethan90%reportaverymuchbetterQualityofLife
• Over70%reporttheBAHAhasmadetheamountofdischargefromtheirears“ much better”
• 88%reportthatusershavemuchlessdiscomfortwiththeirBAHAthanwiththeir previous hearing aids
Conclusion:
Good patient outcomes are not dependent upon high numbers of cases per year.
189
Jane Wild
Anna Home
David Snow
Objective:
Despite extensive soft tissue reduction, the most common complications associated with BAHA implants are related to adverse skin reactions around the abutment. The required soft tissue reduction also adds complexity to the surgical procedure. In this study we aimed to evaluate the surgical and audiological outcomes of a new connective interface of the Cochlear Baha device that is implanted with FAST surgery.
Study design:
A multi-center, retrospective study consisting of three tertiary care institutions for data collection.
Results:
In total 16 patients who underwent BAHA surgery over 5 months were analysed for hearing results, implant stability and surgical complications.
Conclusion:
This study indicates that the new BAHA device with hydroxyapatite coating can be implanted percutaneously without soft tissue reduction. Furthermore the device implanted using the this technique had fewer complications and fewer negative effects than the conventional device/procedure during the 3-6 month follow-up period.
188
Surgical and audiological evaluation of a new
connective interface for Cochlear Baha
Ahmet Kara
Murat Huseyin Yariktas
Serkan Orhan
Ahmet Kara
Merve Durgut
Gurkan Keskin
Yahya Guldiken
Kemal Deger

191
Hearing performance with two high-power Baha
sound processors
Introduction:
With the Baha Intenso and the more recent Baha BP110 Power, two different head-level high-power Baha sound processors are available. The aim of this study was to compare speech understanding with the two processors in quiet and in noise.
Method:
Twenty experienced Baha users with conductive or mixed hearing loss participated in three sessions. In the first session, half of the participants were fitted with a Baha Intenso, the other half with a Baha BP110. After one month of use, aided speech understanding in quiet and in noise was measured and the other test processor was fitted. Another month later, speech understanding with the second sound processor was assessed. For both sound processors, speech understanding was measured in quiet and in noise, with noise arriving either from the front or from the rear.
Results:
Significant improvements were found for both devices for speech understanding in quiet at 50 to 80 dB (+9.6 to +34.8 percent points; p=0.02 to 0.001) and in noise (+6.2 to +13.8 dB, p<0.001). No significant differences were found between the two devices for speech in quiet. For noise from the rear, subjects were able to understand speech at signal-to-noise ratios which were lower (less favorable) by -5.1 dB (p<0.001) when compared to the Baha Intenso.
Conclusions:
Speech understanding is substantially improved by both processors, with no significant differences between the devices in quiet. In noise, speech understanding is significantly better with the Baha BP110 when compared to the Baha Intenso.
Anja Kurz
Marco Caversaccio
Martin Kompis
190
Binaural hearing with bone conduction
stimulation in normal hearing subjects
Introduction:
Previous studies on binaural hearing with bone conduction (BC) stimulation have presented conflicting results. These discrepancies are partly due to usage of stimuli not suitable for BC and heterogeneity of hearing impaired patients using bilateral bone conduction hearing aids (BCHAs). The binaural hearing process relies on interaural time and intensity differences of a sound. Since BC sound is transmitted to both cochleae from one position on the skull, the cross stimulation impedes the interaural separation and introduces an uncertainty towards the ability to utilize binaural hearing functions. In an aim to investigate binaural hearing ability when stimulation is by BC, spatial release of masking test was conducted on normal hearing subjects.
Method:
Binaural hearing with BC stimulation was explored in normal hearing subjects through spatial release of masking test using speech stimuli. The stimulation was bilaterally provided by 1) normal air conduction (AC) with headphones 2) BC transducers at the mastoid position, and 3) BC transducers at the BCHA position. The speech in noise test was conducted for two conditions: 1) co-located and 2) spatially separated.
Results:
Results of the speech in noise test with both AC and BC stimulation illustrate a benefit when speech and noise are spatially separated. The results for the two BC positions were close where BC stimulation at the mastoid showed slightly better results than BC stimulation at the BCHA position. The masking release benefit was approximately half for BC in comparison to results obtained through AC.
Conclusion:
Results of the speech in noise test indicated binaural hearing ability in normal hearing subjects when the stimulation was by BC. However, the binaural benefit was less through BC than AC but the difference between the two BC stimulation positions was small
Mehrnaz Zeitooni
Stefan Stenfelt
Elina Mäki-Torkko

Evaluation of the surgery time, skin reactions,
aesthetic outcomes and implant stability of two
Baha system models
Introduction:
The aim of the study is to investigate the implant stability, the soft tissue reaction and the aesthetic outcomes for two different Baha systems: BIA300 and BIA400.
Methods:
Sixteen patients divided into two groups are included in this study. Seven patients of Group I were implanted with BIA300 system and the other 9 of Group II are implanted with BIA400 (with Hydroxyapatite coated abutment). The implantations were performed using two surgery techniques: a dermatome (Group I) and a linear incision (Group II). The surgery time was recorded. Implant stability quotient (ISQ) using resonance frequency analysis was scored for both groups. The assessment of the soft tissue reactions was performed using Holgers scale and the aesthetic outcomes were evaluated by surgeons according to the Visual Analogue Scale (VAS). The assessment was performed at the day of removing the stitches and at the day of loading the implant. Sound processor loading was performed at 2 weeks post-surgery in both groups.
Results:
ISQ values recorded in both groups were similar. There was a significant difference observed in the surgery time between two groups. Moreover, according to the Visual Analogue Scale, the aesthetic outcomes were significantly better for the patient in the Group II. Conclusion: New BIA400 Baha system allows for faster surgery and improves aesthetic outcomes in patients. Further observations are needed in bigger groups of patients and for long-term results.
193
Tomasz Pychynski
Karolina Goinska-Bednarek
192
Baha in children with bilateral aural dysgenesis.
Our experience with 23 operated cases.
Purpose:
To evaluate outcome and results of Baha surgery in children with bilateral aural dysgenesis in a tertiary pediatric hospital.
Method:
Retrospective case analysis of 23 consecutive children who were implanted from march 2008 to may 2012 with a BAHA device.
Results:
During the study period, 23 children with congenital bilateral aural and ear abnormalities and bilateral moderate conductive hearing loss underwent surgery. Median age at surgery: 8.9 years (range 5-16 years). More than 50% of patients have genetic or chromosomal underlying diagnosis (4/23 Goldenhar syndrome, 5/23 Treacher Collins syndrome, 1/23 Nager syndrome, 1/23 Malpuech facial clefting syndrome and 1/23 Branchio-oculo-facial syndrome). One stage surgery was done in ten cases, all children aged over nine years old. The first ten surgeries were performed with the dermatome created flap technique. Postoperative soft tissues complications were present in 9/23 (39.1%) cases, none in 13 patients with single linear incision. Skin reactions were mild and settled with local treatment. Four required change of abutment and skin reductions. Implant loss occurred in only one child, with underlying Malpuech facial clefting syndrome, 16 months after the date of first step surgery.
Conclusion:
Osseointegrated implants in children have a high success rate for restoring hearing and are specially indicated in bilateral aural and ear abnormalities with moderate conductive hearing loss. Morbidity in these patients can be reduced with a minimal single linear incision and the use of an 8.5 mm initial abutment in children over 8 years of age.
Patricia Cristina Bernaldez
Guillermo Morale
Laura Graciela Quantin
Ruben Santiago Draghi
María Emilia Gonzalez Macchi
Patricia Alejandra Sommerfleck
Silvia Noemi Breuning
María Eugenia Prieto

The Paediatric BAHA programme at Royal
Manchester Children’s Hospital: An audiological
overview of our experiences
Introduction:
The Royal Manchester Children’s Hospital opened in 2009 and has become a specialist tertiary referral centre for children the North West of England. In this time, over 50 children have been assessed for a BAHA. The majority of children referred do not benefit or cannot wear conventional hearing aids. There is also a smaller group of existing paediatric BAHA users, or children with BAHAs who have moved into the area, which is either implanted or issued on a soft- or hard- band.
Method:
This poster will present the results from a retrospective audit of the patients in our paediatric BAHA service (mean age 10 years, SD; 5 years). This includes children with a diverse aetiologies (for example, CHARGE syndrome) as well as typically developing children who have a conductive hearing loss, and/or a profound unilateral hearing loss.
Results:
This poster will discuss our experiences of BAHAs in children including: BAHA candidature, the audiological BAHA assessment process, working with children with complex needs and the challenges of working over a large geographical area.
Conclusion:
Assessing and managing children with BAHAs requires good collaborative working with ENT, as well as flexibility in the audiological approach to best meet the needs of a very diverse group of patients. BAHAs provide effective amplification to children of all ages.
195
Penny Feltham
194
The use of bilateral Baha ® with soft band in a case
of deletion 18q23
Introduction:
The deletion of the long arm of chromosome 18 is one of the commonest deletion syndromes, occurring in 1/40,000 live births. It can be associated with a highly variable phenotype. The most common clinical features include: decreased growth (short stature), facial abnormalities, hypotonia, developmental delay, intellectual disability, congenital aural atresia (CAA) with hearing impairment, limb anomalies and genitourinary malformations. The CAA or narrow auditive canal, is assigned to a 2.3 Mb region on 18q22.3-23 containing a candidate gen possibly involved in transcriptional regulation (zinc finger protein ZNF407) [Veltman et al., 2003].
Method:
We present a one year old girl, whose deletion was detected by a conventional chromosome analysis. She was born at 37 weeks of gestation by cesarean. She presents decreased growth, hypotonia, developmental and language delay (she was evaluated with Vineland adaptative behavior scale) and conductive hearing loss by the obliteration of the inner part of the auditive canal and lack of development of bone component.
Results:
We decided giver her Bahaï System on both sides. In this way, she could get hearing thresholds within normal parameters.
Conclusion:
The use of bilateral Baha with soft band in a case of deletion 18q23, is a good alternative to provide another pathway to perceive environmental and speech sounds since an early age, stimulating naturally the cochlea through bone conduction. The auditory system develops in the early years of life, so, the input of sound through both ears may be of importance for normal development.
Verónica Del Vecchio
Paula Ontivero

Multiple Auditory Steady State Response Air-Bone
Gaps in children with hearing loss.
Introduction:
Auditory Steady State Response (ASSR) it is a useful technique to estimated the behavioral audiogram thresholds in children. The values of BC ASSR are very important to distinguish between different types of hearing loss. There are a few data of the Air-Bone Gap estimation using this technique in patients with actual hearing loss.
Methodology:
The M-ASSR to both air- (AC) and bone- conducted (BC) stimuli were recorded in four groups of children (9-14 years old). Four carrier tones (0.5-4 kHz) modulated in amplitude (77-115 Hz) were mixed together and simultaneously presented at variable intensities (AC 100-10 dB HL; BC 70-10 dB HL). For this investigation we evaluated 11 children with normal hearing (G1=15 ears), 14 patients with conductive hearing loss (G2=15 ears), 14 patients with mixed hearing loss (G3=15 ears) and 10 patients with sensorineural hearing loss (G4=15 ears).
Results:
In all children tested the M-ASSR ABGs estimates shows similar different with the behavioral measures (G1: 2-3 dB; G2 0-4 dB; G3 1-3 dB; G4 0-2 dB) with correlation between physiological ABGs and behavioral estimates for all conditions combined of r =0.96. The results of discriminated analysis including the M-ASSR ABGs and BC thresholds were 100% of G1, 86% in G2, el 51% in G3 and 73 % in G4.
Conclusions:
The M-ASSR it is a useful technique to classify a type of hearing loss in children, differentiating between normal hearing and conductive, mixed or sensorineural hearing loss.
197
Maria Del Carmen Hernndez
Sandra Bermejo
Alexander García
196
Titanium fixtures for bone-conduction devices and
the influence of type 2 diabetes mellitus
Introduction:
The aim of this study is to evaluate whether diabetes mellitus (DM) is a risk factor for titanium fixture loss in bone-conduction devices (BCDs) due to osseointegration failure.
Method:
All patients who received a BCD in a tertiary referral centre at Nijmegen between January 1, 1988 and December 31, 2007 were analyzed in a retrospective case study. The analyses were performed on 833 patients (993 implants), and a subpopulation of patients aged 40 years consisting of 641 patients (739 implants). Patients received a questionnaire asking about the presence of DM at the time of implantation. Data concerning implant loss were retrieved from medical records and the Nijmegen BCD database.
Results:
The total survival rate of the BCD-implant in this population was 90.6%. The prevalence of DM was 9.3%. In the subpopulation of patients aged 40 years or older, the non-DM group lost 5.1% of their implants versus 14% of type 2 DM patients, a statistically significantly difference (p=0.003). Spontaneous loss, loss due to a grade 4 Holgers skin reaction and trauma accounted for 2.2% versus 4.7% (p=0.13), 0.5% versus 2.3% (p=0.1) and 0.6% versus 4.7% (p=0.007), respectively, of implant losses in non-DM versus type 2 DM patients.
Conclusions:
The prevalence of DM amongst the Nijmegen BCD population is higher than the general Dutch prevalence. A statistically significantly higher implant loss was observed during the study period for type 2 DM patients than non-DM BCD wearers.
Hubert Faber
Laura Horstink
Maarten de Wolf
Catharina Dun
Cor Cremers
Myrthe Hol

Upgrading BAHA patients - Clinical Experiences and
Outcomes
Introduction:
The aim of this study was to carry out a retrospective study on the BAHA population at The Emmeline Centre to investigate the outcomes of upgrading existing BAHA users from analogue to digital BAHA processors.
Method:
25 adult patients were randomly selected from the population of BAHA users at the Emmeline Centre for this study. Sound field aided thresholds (SFAT) at 500, 1000, 2000 and 4000 Hz using the previously worn analogue processor were compared with the same measures using the upgraded digital processor.
In addition a telephone survey using the Client Oriented Scale of Improvement (COSI) was carried out as a subjective measure of the BAHA upgrades process.
Results:
Significant reduction in thresholds for the 500 and 1000 Hz frequencies were found with the digital BAHA processors compared to the analogue devices (p<0.001 and p=0.017 respectively). No statistically significant differences were found in the SFAT obtained at 2000 and 4000 Hz (p=0.608 and p=0). The results from the COSI revealed that whilst 51% of responses showed an improvement in difficult listening situations with their digital device, 28% of responses indicated the digital processor was worse and in 21% there was no difference.
Conclusion:
In summary, better SFAT were obtained at 500 and 1000 Hz which may be related to the digital technology within the BAHA. From the COSI the results indicate that the digital processing does not always improve patients hearing in difficult situations.
Thus, whilst advances in technology may lead to benefits and improvements in hearing even in difficult listening situations the degree of benefit is limited and in a small but significant proportion of patients can lead to dissatisfaction or indifference.
199
Joanne Muff
198
Clinical assessment of Baha implants stability in
children with craniofacial malformations
Introduction:
The goals were to evaluate the stability of the abutment, depending on bone thickness, period time from surgery and kind of craniofacial malformation.
Methodology:
Ten children (11 implants, 4 mm long) underwent the 1-stage procedure following the linear incision as well as by using dermatome technique. Clinically it was: Treacher-Collins- 4 ears, bilateral aural malformation, unilateral -3 ears. ISQ values were recorded at the time of implantation and 1, 4 weeks and 3, 6 and 12 months after surgery. In Treacher-Collins group, we notice bone thickness 3mm (two children) and 4 mm one. The average ISQ value was 55 at time surgery, after one week - 54, four week - 56, three months 55, six 60 and one year 66. In-group with bilateral aural malformation the bone thickness was 3 mm and the average ISQ value at time surgery were 58, after one week 56, four week 60, three months 65, 6 months 62 and one year after implantation 66. In-group with unilateral malformation bone thickness was on average 3 mm and implant stability value as following 61, 57, 63, 62, 65, and 64.
Results:
The test implant showed higher mean ISQ values at the time of placement and over time. The level of osseointegration reached with the implants in children with craniofacial malformation 4 weeks after implantation was sufficient to support the sound processor. The test implant system is expected to provide additional benefits related to the improvement of the degree of osseointegration, especially for children with thin or compromised bone
Wieslaw Konopka
Malgorzata Struzycka
Malgorzata Smiechura

Amplification and speech and language
development in children with atresia
Introduction:
In this study, we wanted to begin to address issues surrounding amplification of children with atresia. Specifically, what intervention provides the best outcome and how does the type of intervention, time of first intervention, and compliance correlate with speech and language development?
Design:
Male and female subjects were included in this study if they were between 3 and 6 years of age and had unilateral or bilateral atresia. Subjects were all fit with a bone conduction device on a softband. Subjects completed audiology testing, hearing aid evaluation, speech and language evaluation and a parent or legal guardian completed the Children’s Outcomes Worksheet.
Results:
Subjects ranged in age from 3.5 to 6 years of age with a mean of 4.5 years. The average time between birth and the first amplification device was 2 years with a range from 6 months to 6 years. Daily use of amplification device as measured by parent report and data logging correlates with speech and language abilities. Males exhibited greater delays than females. Males also were fit with their first amplification device on average one year later than females.
Conclusions:
Findings from this study highlight a relationship between time of first amplification, compliance, and speech and language abilities in young children. A larger study needs to be done to more clearly define the relationships between amplification and speech and language delays so recommendations regarding intervention and rehabilitation for this population can be made.
Judy Attaway
Emily Rosario
Christopher Stone
Cindy Sendor
201 200
Measurement of resonance frequencies of BAHA
patients comparing different osteosysthesis
systems
Introduction:
Two different osteosysthesis systems were used to connect a Bone anchored hearing aid (BAHA, Cochlear) the patients’ skull. One subset of patients was provided with the Ti-Epiplating osteosysthesis system (MEDICON eG, Tuttlingen, Germany) while another subset was provided with the BAHA implant (Cochlear Ltd., Australia), a single screw which allows a connection to a bone by osseointegration. The MEDICON implant is shaped as a star and connected with up to five screws which are concentrically located. Thus, the implant stability might differ and result in a different frequency transmission. Resonance frequency analysis stability measurements essentially apply a bending load, which mimics the clinical load and direction and provides information about the stiffness of the implant bone junction.
Method:
Two groups of patients (totally 18) using a BAHA were investigated with the Osstell ISQ implant stability meter (Osstell AB, Gothenburg, Sweden) recording the resonance frequency for two perpendicular vibration modes. Therefore, an Osstell SmartPeg is mounted onto the BAHA abutment and a magnetic field with a broad-band spectrum is applied to it.
Results:
The mean ISQ value reveals increased implant stability for the Cochlear devices as compared to the MEDICON implant. This is also found by comparing subsequently implanted devices in one temporal bone of a human cadaver. Despite no osseointegration could have been occurred, the implant stability was better for the BAHA device. Conclusion The original BAHA device should be used for connecting BAHA sound processors to the skull.
Torsten Rahne

203
World’s first DermaLock implantation in
Goldenhar syndrome
Introduction:
We aimed to discuss the benefits of the new DermaLock Bone anchored hearing aid (BAHA) system and benefits in craniofacial abnormalities through a case study. Goldenhar, is a rare, congenital craniofacial abnormality, first described by Maurice Goldenhar in 1952. Presentation is varied, commonly unilateral underdevelopment of the face, cheeks, mandible and abnormal ear development leading to hearing impairment.
Case Study:
A 35 year old man with Goldenhar syndrome, presented with hearing impairment, microtia, atresia, right facial hypoplasia and an existing right BAHA site. Audiometric Testing showed bilateral conductive hearing impairment , with lack of air conduction on the right.
The patient underwent implantation of a DermaLock BAHA abutment on the left. DermaLock’s unique hydroxyapatite surface layer provides efficient osseointegration, thus quicker outcomes post-operatively with variable abutment length for increased stability. Values of abutment stability (RFA) and tissue around the abutment sites (Holgers’ scale) were measured. At both one week and three month they were satisfactory. After processor fitting at 1 week, GBI patient satisfaction survey, measured at 3 month, demonstrated increased Quality of Life after the BAHA.
Conclusion:
It is clear more implantations DermaLock BAHA need to be undertaken on patients with craniofacial abnormalities. This case showed the first, safe, and successful DermaLock implantation with positive post-operative outcomes both for the surgeon and patient.
Gemma Ridley
Ian Johnson
202
The use of a daily alternating method in
comparing two osseointegrated bone
conduction implant sound processors in patients
with single sided deafness.
Introduction:
Tyler et al. proposed a daily alternating method to compare different strategies in cochlear implants and hearing aids. We aim to verify if daily alternating devices is a useful method to compare two bone conduction implant (BCI) sound processors (SP).
Method:
10 experienced 10 newly fitted SSD patients changed to the Baha BP100 for one week, followed by a period of daily changing sound processors. Speech in noise testing (SPIN) was performed. Patients rated overall satisfaction, clearness of sound and effort of listening in background noise in a diary. The SHQ and the APHAB were also completed.
Results:
No problems with completing the diary have been reported. SPIN showed a head shadow benefit in both aided conditions (Divino: 2,67dB, p= 0.003, BP100: 2,50dB, p = 0.004). No significant difference between both SPs was found. The APHAB showed better results with BP100 concerning ease of communication (18 vs. 24, p = 0.035), background noise (34 vs. 49, p = 0.005) and reverberant conditions (26 vs. 39, p = 0.008). The SHQ showed an improvement in the aided condition and between both SPs (p < 0.05). The diary resulted in a significant difference between both SPs on all subscales (p < 0.005).
Conclusion:
A daily alternating method can be a fast method for a patient to compare two BCI SPs. Both SPs reduce the handicap experienced by SSD patients. Although objective measurements did not show significant differences, a difference in quality has been found between both SPs using the alternating method.
Jolien Desmet
Rajae Bouzegta
Anouk Hofkens
Peggy Lambrechts
MarcDe Bodt
Paul Van de Heyning

Resonance Frequency Analysis as a technique to measure implant stability and osseointegration is fast becoming a global diagnostic standard in the dental industry. With more than 500 articles published in scientific journals it is a proven scientific method as a guide to pre-dictable surgical and restorative protocols. Publications are now also appearing in the BAHA area*.
Manage implants at risk - You’ll find Osstell ISQ especially valuable for achieving more predictable outcomes when treating higher risk pa-tients and implants at risk for failure due to poor integration. Osstell gives you an early warning, as a decreased ISQ value, if osseointegra-tion isn’t progressing as expected. It can help you avoid costs of an implant failure due to premature loading. Osstell can also assist you in being more confident about treating patients with risk factors, more predictably.
Reduce treatment time - If the initial mechanical stability is high enough a one-stage approach is often used together with immediate- or early loading. By measuring again before loading, and compar-ing that value to the baseline value taken at placement, the decision whether to proceed or not is made quick and easy.
www.osstell.com
Your guide to Predictable surgical and restorative protocols
Osstell ISQ
*The New Baha Implant: A Prospective Osseointegration Study.D’Eredità R, Caroncini M, Saetti R.Journal: Otolaryngol Head Neck Surg, 2012
Stability, survival, and tolerability of a novel baha implant system: six-month data from a multicenter clinical investigation.Dun CA, de Wolf MJ, Hol MK, Wigren S, Eeg-Olofsson M, Green K, Karlsmo A, Flynn MC, Stalfors J, Rothera M, Mylanus EA, Cremers CW.Journal: Otol Neurotol, 2011
An experimental evaluation of a new craniofacial implant using the rabbit tibia model: Part II. Biomechanical findings.Sennerby L, Gottlow J, Rosengren A, Flynn M.Journal: Otol Neurotol, 2010
Sleeping Implant in the Temporal Bone: Report of a Case with 20-Year Follow-Up.Granström G, Gröndahl HG, Tjellström A.Journal: Clin Implant Dent Relat Res, 2009
204
Possible approaches of programming the BP100 sound
processor in a group of patients with unilateral mixed
hearing loss – partial results.
Propose:
The little or absent transcranial attenuation of the sound creates some challenges to fit bone conduction devices. When programming the BP100 sound processor for a patient with a unilateral mixed hearing loss, we would like to know if there are more than 1 possibility and which program can provide better hearing perception: (1) a program based on the ear with the bone conduction hearing loss which may deliver actual binaural hearing, or (2) to consider the ear with normal bone conduction thresholds obtained by in situ measure in order to avoid the masking effect or a louder perception in the normal ear? Furthermore, is it worthwhile to use the low frequency adjustment setting to improve the speech discrimination in noise? Our proposal is to describe the partial results of this study.
Methods:
Two patients, adults, with acquired severe mixed hearing loss in one ear and normal hearing in the other were assessed. The bone conduction threshold average was 40dB and 30dB, and in the normal ear 5 and 15dB, respectively for patient 1 and 2. The transcranial attenuation average was 5dB to both patients. The hearing performance was evaluated by the sentence in noise test (SNR +5) with (1) the noise presented at the front and the speak at the front and (2) the noise presented on the deaf side and the speak at the front; (3) monosyllabic recognition test with the normal ear occluded. Speech was presented fixed in 60dBNA. They used the 3 different programs after 3 months of activation, each program for one week. They were evaluated in the conditions: Unaided (U); Program 1 (P1) - program considering the bone conduction thresholds in the deaf ear; program 2 (P2) – linear program considering the thresholds by in-situ measurement program 3 (P3) – the same as P2 with low frequency adjusted setting,
Results:
Patient 1 could not use the P1, referring that all sounds were too loud; the program just became comfortable after reducing 20dB. The patient 2 used the three programs. The patient 1 test in noise score, situation (1) ranged from 88%(U) to 96%; (P3); situation (2) score ranged from 80% (P2) to 90% (P3) ; monosyllabic words from 60%(U) to 92%(P2) .The patient 2 test in noise score in situation (1) ranged from 88%(U) to 96%;(P3); the situation (2) the score ranged from 80% (P2) to 90% (P3); monosyllabic words from 60%(U) to 92%(P2). In their daily routine, both reported preferring program 3.
Conclusion:
There more than one way to program bone conduction devices for patients with unilateral mixed hearing loss. These partial results show that both patients analyzed preferred the linear program based on the normal ear in-situ bone conduction thresholds
Raquel Franco Stuchi-SiaghIulo Sérgio Barauna Filho
Aldo Stamm

Invisible link to better hearing
More possibilities for a lifetime of better hearing
Introducing the Cochlear™ Baha® 4 Systems
Proven hearing performance with soft tissue preservation
Cochlear™ Wireless Phone Clip Cochlear™ Baha® Remote Control Cochlear™ Wireless TV Streamer
Smarter hearing – wireless freedom
Baha 4 Attract System: Baha 4 Connect System:
Baha 4 Sound Processor:
Cochlear is the only company to offer two bone conduction systems, both based on the same strong implant foundation.
100,000 Baha ® users
More than 35 years of Baha® practice
100,000Baha® users
Cochlear™ Wireless Mini Microphone
The Baha 4 Attract System is pending CE approvalThe Baha 4 Sound Processor is not CE approved and not available for sale

ConferencesEventsMedia designConsultancy
benchcom.co.uk
c o m m u n i c a t i o n s
Londont 020 714 [email protected]
Newcastlet 0191 241 [email protected]
Cool, calm and confident. Have loved working with you throughout.
— Chris Bray, Event Director, MS Society
Proud Conference Organisers of OSSEO2013
Auditdata Ltd.Staines-upon-Thames, UKPhone +44 (0) 1784 410 [email protected] • www.auditdata.com
Auditdata - Your Partner in Audiology Solutions
Expert Implant and OtoSurgery modules
Plan and visualise the patient’s pathway
Fast access to both new and completed actions
Designed with expert users
Handle all the communication, financial and clinical aspects of the patient’s pathway
Record key data for research purposes
Contact us for more information!
oming soon . . . coming soon . . . coming soon . . . coming soo
Pinpoint Scotland Ltd’s latest publication – PMFA News – is a bi-monthly review of plastic, maxillofacial, aesthetic surgery andmedicine. PMFA News will include first class articles, conferencereports, book reviews, journal reviews and information on the latestproducts and company developments. Our aim is to offer a platformfor communication, information and education to all specialist areaswithin plastic, reconstructive, aesthetic surgery and medicine. To beginwith the magazine will have a print run of 10,000 and will be mailed torelevant professionals throughout Europe.
Industry leader announced as EditorWe are delighted to announce Professor AndrewBurd as Editor of the magazine. Prof Burd isProfessor and Chief of Plastic, Reconstructive, andAesthetic Surgery at the Chinese University of HongKong and a renowned academic and commentator.
Sign up at www.pmfanews.comto keep informed of our launch date
pmfa news
Pinpoint Scotland Ltd
Magazine Launch
The bi-monthly review of plastic, maxillofacial, aesthetic surgery and medicine
meet the team
Nova McMillanE: [email protected]
Rosaleen ShineE: [email protected]
Heather McLaughlinE: [email protected]
Jennifer FallonE: [email protected]
Diana SpencerE: [email protected]
Joanna ParkE: [email protected]
sales
editorial
admin, diary &courses
features
newsround
audiology matters
regulars
diary
courses & conferences
ReviewsHow I do itTrainee matters
Special focus articles
www.entandaudiologynews.com
Your copy will be a recent issue and is limited to one copy per address. The information you provide will be heldunder the data Protection Act 1998 and your data may be passed on and may be used in further promotions. Ifyou do not want this, please write to Pinpoint Scotland Ltd, ENT & Audiology News, 9 Gayfield Square, Edinburgh, EH1 3NT, UK.
pinpointscotland ltd
Email your details
Name
Job Title/Position
Mailing Address
FREEsample
quote OSSEO13
copy
essential reading for the professionwww.entandaudiologynews.com
ENT&audiology
news
OSSEO conference ad_Layout 1 22/05/2013 08:47 Page 1


















