Cranial Nerve Vii
38
CRANIAL NERVE VII (FACIAL NERVE) Introduction Functional components Deep/nuclear origin Central connections Superficial origin Course Relations Branches of communication Branches of distribution Applied aspects Cranial Nerve VII - Facial Nerve Component overview Branchial motor component Origin and central course Intracranial course Intracranial course, cont'd Extracranial course & final innervation Voluntary control of facial muscles Voluntary control of facial muscles, cont'd Lower motor neuron lesion (LMN) Bell's palsy LMN lesions of the facial nerve LMN lesions, acoustic neuromas Upper motor neuron (UMN) lesions Overview, visceral motor component Origin and central course Intracranial course
-
Upload
asish-geiorge -
Category
Documents
-
view
236 -
download
2
description
g
Transcript of Cranial Nerve Vii

CRANIAL NERVE VII (FACIAL NERVE)
Introduction
Functional components
Deep/nuclear origin
Central connections
Superficial origin
Course
Relations
Branches of communication
Branches of distribution
Applied aspects
Cranial Nerve VII - Facial Nerve
Component overview Branchial motor component Origin and central course Intracranial course Intracranial course, cont'd Extracranial course & final innervation Voluntary control of facial muscles Voluntary control of facial muscles, cont'd Lower motor neuron lesion (LMN) Bell's palsy LMN lesions of the facial nerve LMN lesions, acoustic neuromas Upper motor neuron (UMN) lesions
Overview, visceral motor component Origin and central course Intracranial course Greater petrosal nerve Chorda tympani
Overview, special sensory component

Peripheral course Central course Central course, cont'd
Overview of general sensory component Central course Central course, cont'd Central course, cont'd
Peripheral lesions of the facial nerve Peripheral lesions of the facial nerve, cont'd
Cranial Nerve VII - Facial Nerve Page 1 of 28
Component Overview
The facial nerve has four components with distinct functions:
Branchial motor(special visceral efferent)
Supplies the muscles of facial expression; platysma, posterior belly of digastric muscle; stylohyoid, and stapedius.
Visceral motor(general visceral efferent)
Parasympathetic innervation of the lacrimal, submandibular, and sublingual glands, as well as mucous membranes of nasopharynx, hard and soft palate.
Special sensory(special visceral afferent)
Taste sensation from the anterior 2/3 of tongue; hard and soft palates.
General sensory(general somatic afferent)
General sensation from the skin of the external auditory meatus and from a small area behind the ear.
Branchial motor fibers constitute the largest portion of the facial nerve.
The remaining three components are bound in a distinct fascial sheath from the branchial motor fibers. Collectively these three components are referred to as the nervus intermedius.
Component Overview

Last revised: March 22, 1998
Cranial Nerve VII - Facial Nerve Page 2 of 28
Branchial Motor Component
The largest component of the facial nerve.
Provides voluntary control of the muscles of facial expression (including buccinator, occipitalis and platysma muscles), as well as the posterior belly of the digastric, stylohyoid and stapedius muscles.
Note the branchial motor components of the facial nerve:

Cranial Nerve VII - Facial Nerve Page 3 of 28
Origin and Central Course
The branchial motor component originates from the motor nucleus of CN VII in the caudal pons.
Fibers leaving the motor nucleus of CN VII initially travel medially and dorsally to loop around the ipsilateral abducens nucleus (CN VI) producing a slight bulge in the floor of the fourth ventricle - the facial colliculus.
Fibers then course so as to exit the ventrolateral aspect of the brainstem at the caudal border of the pons in conjunction with the nervus intermedius components of CN VII.

Cranial Nerve VII - Facial Nerve Page 4 of 28
Intracranial course
Upon emerging from the ventrolateral aspect of the caudal border of the pons, all of the components of CN VII enter the internal auditory meatus along with the fibers of CN VIII (vestibulocochlear nerve).
The fibers of CN VII pass through the facial canal in the petrous portion of the temporal bone. The course of the fibers is along the roof of the vestibule of the inner ear, just posterior to the cochlea.

Figure 7-4. Intracranial course- branchial motor components of the facial nerve. Facial nerve origin and inner ear anatomy.
Cranial Nerve VII - Facial Nerve Page 5 of 28
Intracranial Course, cont'd
At the geniculate ganglion the various components of the facial nerve take different pathways.
Fibers of the branchial motor component pass through the geniculate ganglion without synapsing, turn 90 degrees posteriorly and laterally before curving inferiorly just medial to the middle ear to exit the skull through the stylomastoid foramen.
The nerve to the stapedius muscle is given off from the facial nerve in its course through the petrous portion of the temporal bone.

Cranial Nerve VII - Facial Nerve Page 6 of 28
Extracranial Course and Final Innervation
The posterior auricular nerve, nerve to the posterior belly of the digastric and the nerve to the stylohyoid muscle are given off upon the facial nerve's exit from the stylomastoid foramen.
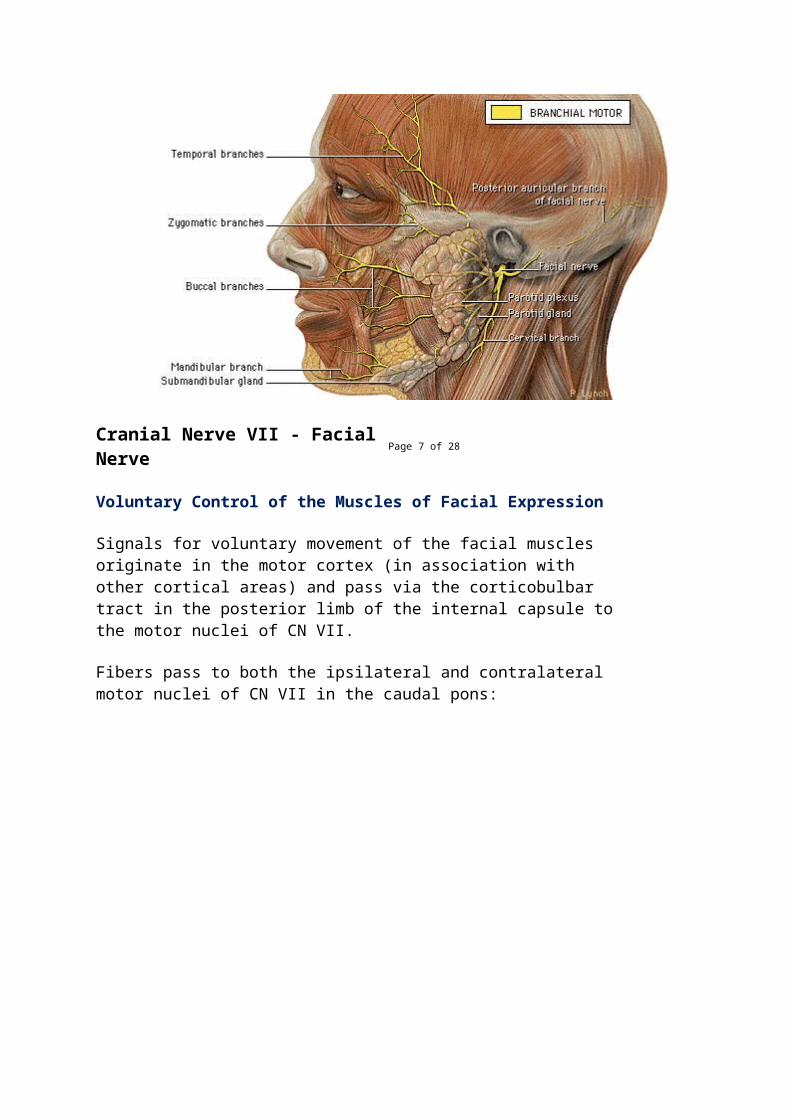
The remaining fibers enter the substance of the parotid gland and divide to form the temporal, zygomatic, buccal, mandibular, and cervical branches to innervate the muscles of facial expression.
Cranial Nerve VII - Facial Nerve Page 7 of 28
Voluntary Control of the Muscles of Facial Expression
Signals for voluntary movement of the facial muscles originate in the motor cortex (in association with other cortical areas) and pass via the corticobulbar tract in the posterior limb of the internal capsule to the motor nuclei of CN VII.
Fibers pass to both the ipsilateral and contralateral motor nuclei of CN VII in the caudal pons:
Cranial Nerve VII - Facial Nerve Page 8 of 28
Voluntary Control of the Muscles of Facial Expression
The portion of the nucleus that innervates the muscles of the forehead receives corticobulbar fibers from both the contralateral and ipsilateral motor cortex.
The portion of the nucleus that innervates the lower muscles of facial expression receives corticobulbar fibers from only the contralateral motor cortex.
This is very important clinically as central (upper motor neuron) and peripheral (lower motor neuron) lesions will present differently.

Cranial Nerve VII - Facial Nerve Page 9 of 28
Lower Motor Neuron (LMN) Lesion
Results from damage to the motor nucleus of CN VII or its axons.
A LMN lesion results in the paralysis of all muscles of facial expression (including those of the forehead) ipsilateral to the lesion.
Cranial Nerve VII - Facial Nerve Page 10 of 28
Clinical Correlation - Bell's Palsy
A LMN lesion of CN VII which occurs at or beyond the stylomastoid foramen is commonly referred to as a Bell's Palsy.
Characteristic indications of a LMN lesion or Bell's Palsy include the following, on the affected side:
Marked facial asymmetry

Atrophy of facial muscles
Eyebrow droop
Smoothing out of forehead and nasolabial folds
Drooping of the mouth corner
Uncontrolled tearing
Loss of efferent limb of conjunctival reflex (cannot close eye)
Lips cannot be held tightly together or pursed
Diificulty keeping food in mouth while chewing on the affected side
Clinical Correlation - LMN Lesions of Facial Nerve (VII)
A LMN lesion of CN VII in conjunction with deficits associated with CN VI (abducens nerve) indicate a lesion in the brainstem which affects both the motor nucleus of CN VII and the abducens nucleus. Clinical Correlation - LMN Lesions of Facial Nerve (VII)
A LMN lesion of CN VII in conjunction with deficits associated with CN VIII (vestibulocochlear nerve) are characteristic of a lesion in the region of the

internal acoustic meatus.
An example of this type of lesion is an acoustic neuroma:
Cranial Nerve VII - Facial Nerve Page 13 of 28
Clinical Correlation - Upper Motor Neuron (UMN) Lesion
Results from damage to neuronal cell bodies in the cortex or their axons that project via the corticobulbar tract through the posterior limb of the internal capsule to the motor nucleus of CN VII.
With an UMN lesion, voluntary control of only the lower muscles of facial expression on the side contralateral to the lesion will be lost.
Voluntary control of muscles of the forehead will be spared due to the bilateral innervation of the portion of the motor nucleus of CN VII that innervates the upper muscles of facial expression.
UMN lesions are usually the result of a stroke.

Cranial Nerve VII - Facial Nerve Page 14 of 28
Overview of Visceral Motor Component
Parasympathetic component of the facial nerve.
Consists of efferent fibers which stimulate secretion from the submandibular, sublingual, and lacrimal glands, as well as the mucous membranes of the nasopharynx and hard and soft palates.
Cranial Nerve VII - Facial Nerve Page 15 of 28
Origin and Central Course
The visceral motor component originates from a diffuse collection of cell bodies in the caudal pons just below the facial nucleus known as the superior salivatory nucleus.
Fibers course so as to exit the ventrolateral aspect of the brainstem at the caudal border of the pons as part of the nervus intermedius portion of CN VII. these fibers donot loop around the abducens nucleus.
The nervus intermedius exits the brainstem just lateral to the branchial motor component.

Intracranial Course
Upon emerging from the ventrolateral aspect of the caudal border of the pons, all of the components of CN VII enter the internal auditory meatus along with the fibers of CN VIII (vestibulocochlear nerve).
Within the facial canal the visceral motor fibers divide into two groups to become the greater petrosal nerve and the chorda tympani:
The greater petrosal nerve supplies the lacrimal, nasal, and palatine glands.
The chorda tympani supplies the submandibular and sublingual glands.

Course of the Greater Petrosal Nerve
At the geniculate ganglion the greater petrosal nerve turns anteriorly and medially exiting the temporal bone via the petrosal foramen and entering the middle cranial fossa.
Figure 7-15a. Course of the greater petrosal nerve through the temporal bone.
The greater petrosal nerve passes deep to the trigeminal ganglion to enter the foramen lacerum. The nerve traverses the foramen and enters a canal at the base of the medial pterygoid plate in conjunction with sympathetic fibers (deep petrosal nerve) branching from the plexus following the internal carotid artery. The parasympathetic and sympathetic fibers together make up the nerve of the pterygoid canal.
Upon exiting the pterygoid canal, pre-ganglionic parasympathetic fibers of CN VII synapse in the pterygopalatine ganglion which is suspended from the fibers of the maxillary division of the trigeminal nerve (V2) in the pterygopalatine fossa.

Post-ganglionic parasympathetic fibers then follow the fibers of V2 to reach the lacrimal gland (via the lacrimal nerve) and the mucous membranes of the nasal and oral pharynx.
Course of the Chorda Tympani
The pre-ganglionic fibers of the chorda tympani branch from the other fibers of CN VII as they pass through the facial canal just posterior to the middle ear.
The fibers pass through the middle ear in close relationship with the tympanic membrane and exit the base of the skull to enter the inferotemporal fossa:
Figure 16a. Course of the chorda tympani, inner ear.
In the inferotemporal fossa the chorda tympani joins the fibers of the lingual branch of the mandibular division of CN V (V3).
CN VII pre-ganglionic fibers synapse in the submandibular ganglion suspended from the lingual nerve (V3). Post-ganglionic fibers then either enter the submandibular gland directly or again follow the lingual nerve before branching to innervate the sublingual gland:

Overview of Special Sensory Component
Consists of afferent fibers which convey taste information from the anterior 2/3 of the tongue and the hard and soft palates.
Peripheral Course
Chemoreceptors of the taste buds located on the anterior 2/3 of the tongue and hard and soft palates initiate receptor (generator) potentials in response to chemical stimuli.
The taste buds synapse with the peripheral processes of special sensory neurons from CN VII. These neurons generate action potentials in response to the taste bud's receptor potentials. The peripheral processes of these neurons follow the lingual nerve and then chorda tympani to the petrous portion of the temporal bone (similar to the path followed by the efferent visceral motor fibers).

Figure 7-18a. Chorda tympani and the lingual nerve.
The cell bodies of these primary afferent neurons reside in the geniculate ganglion:
Figure 7-18b. Geniculate ganglion.Central Course
The central processes of the special sensory neurons pass from the geniculate ganglion through the facial canal and enter the brainstem as part of the nervus intermedius portion of CN VII.
The fibers then join the caudal portion of tractus solitarius and ascend to synapse in the rostral portion of the nucleus solitarius - also referred to as the gustatory nucleus:

Central Course
Ascending secondary neurons originating from nucleus solitarius project both ipsilaterally and contralaterally to the ventral posteromedial (VPM) nucleus of the thalamus.
Tertiary neurons from the thalamus project via the posterior limb of the internal capsule to the area of the cortex responsible for taste.
Cranial Nerve VII - Facial Nerve Page 23 of 28
Overview of General Sensory Component
A minor component of CN VII.
The general sensory component consists of afferent fibers which convey general sensory information from the skin of the concha of the external ear and from a small area of skin behind the ear. It may also supplement the mandibular division of CN V in providing sensation from the wall of the acoustic meatus and the outer surface of the tympanic membrane.

Cranial Nerve VII - Facial Nerve Page 24 of 28
Central Course
The cell bodies of these primary sensory neurons reside in the geniculate ganglion. The peripheral processes of these neurons pass from the skin of the external ear and small region of skin behind the ear through the stylomastoid foramen in conjunction with the fibers of the branchial motor component of CN VII.
They then course through the petrous portion of the temporal bone to the geniculate ganglion.
From the geniculate ganglion, the central processes of these general sensory fibers travel through the facial canal of the petrous portion of the temporal bone and exit the internal acoustic meatus.
Central Course

The central processes of the general sensory neurons enter the brainstem as part of the nervus intermedius portion of CN VII. The fibers then descend in the spinal tract of the trigeminal nerve to synapse in the spinal nucleus CN V.
Central Course
Ascending secondary neurons originating from the spinal nucleus of CN V project to the contralateral ventral posteromedial (VPM) nucleus of the thalamus via the anterolateral system.
Tertiary neurons from the thalamus project via the posterior limb of the internal capsule to the sensory cortex of the post-central gyrus.
Peripheral Lesions
By using your knowledge of the anatomy of the facial nerve, the location of a lesion can be determined by the presence or absence of certain deficits.
A lesion in the facial canal proximal to the branching of the greater petrosal nerve and chorda tympani is characterized by the following:

Paralysis of all the muscles of facial expressionipsilateral to the lesion (LMN lesion of the branchial motor component of CN VII).
Loss of secretion from lacrimal gland and mucous membranes of nasal and oral pharynx ipsilateralto the lesion (lesion of the greater petrosal nerve, visceral motor component of CN VII).
Loss of secretion from submandibular and sublingual glands ipsilateral to the lesion (lesion of the chorda tympani, visceral motor component of CN VII).
Loss of taste from anterior 2/3 of tongueipsilateral to the lesion (lesion of the chorda tympani, special sensory component of CN VII).
Loss of general sensation from concha of external ear and small area of skin behind the ear (general sensory component of CN VII).
Deficits in hearing and/or vestibular functionsipsilateral to the lesion (associated with CN VIII).
Intact general sensation to the tongue (supplied by CN V3).
If the lesion was distal to the greater petrosal nerve but proximal to the chorda tympani the patient would present as above, except that secretory functions of the lacrimal, nasal, and palatine glands would be intact.
Cranial Nerve VII - Facial Nerve Page 28 of 28
Peripheral Lesions
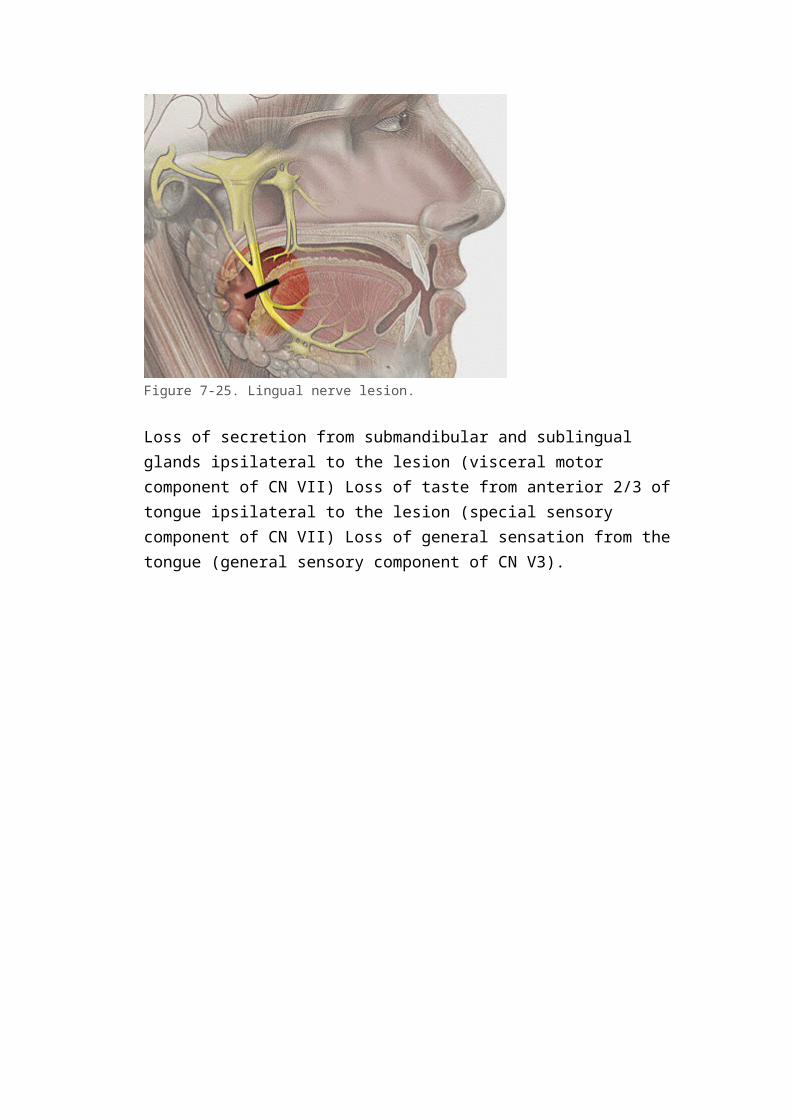
A lesion which affected the lingual nerve just distal to its junction with the chorda tympani would present as follows:

Figure 7-25. Lingual nerve lesion.
Loss of secretion from submandibular and sublingual glands ipsilateral to the lesion (visceral motor component of CN VII) Loss of taste from anterior 2/3 of tongue ipsilateral to the lesion (special sensory component of CN VII) Loss of general sensation from the tongue (general sensory component of CN V3).

Cranial Nerves
website-hit-counters.com
FollowersBlog Archive
▼ 2009 (12)
o ▼ November (12)
Introduction
OLFACTORY NERVE
OPTIC NERVE
OCCULOMOTOR NERVE
TROCHLEAR NERVE & ABDUCENT NERVE
TRIGEMINAL NERVE
FACIAL NERVE:
VESTIBULOCOCHLEAR NERVE
THE GLOSSOPHARYNGEAL NERVE
VAGUS NERVE
ACESSORY NERVE
HYPOGLOSSAL NERVE
About MeA M B E R M U N I R
View my complete profile
FRIDAY, NOVEMBER 6, 2009
FACIAL NERVE:It is the 7th Cranial Nerve.It has a medial motor root and a lateral sensory root, the nervous intermedius.
FUNCTIONAL COMPONENTS
Special Visceral (brachial) Efferent
· Nucleus of the facial nerve lies in the lower part of Pons supplies various muscles innervated by facial nerve. The part of nucleus that supplies muscles of the upper part of the face receives corticonuclear fibers from the motor cortex

of both the right and left sides. In contrast the part of nucleus that supplies muscles of the lower part of the face receive corticonuclear fibers only from the opposite side of cerebral hemisphere.
General Visceral efferent (parasympathetic)
· Superior salivatory nucleus lies in lower part of pons. It sends fibers through the facial nerve and its chorda tympani branch to the Submandibular ganglion for the supply of Submandibular and sublingual salivary glands.· Lacrimatory nucleus lies near the salivatory nuclei gives fibers that pass through facial nerve and its branches relay in the pterygopalatine ganglion and supply the lacrimal gland.
Special Visceral afferent
· Nucleus of tractus solitarius (gustatory) carries taste sensation from anterior 2/3rd of the tongue and from the palate.
General Somatic Afferent fibers
They probably innervate a part of skin over the ear. The nerve does not give any direct branches to the ear but some fibers may reach it through communication with vagus nerve. Proprioceptive impulses from muscles of the face are believed to travel through branches of trigeminal nerve to reach the mesencephalic nucleus of the nerve
MOTOR ROOTSupplies Muscles of face, scalp, auricle, buccinator, platysma, Stapedius, stylohyoid & posterior belly of diagastric
SENSORY ROOTIt carries the taste fibers from anterior two thirds of tongue, floor of mouth and palate.It also conveys parasympathetic secretromotor fibers to Submandibular and sublingual salivary glands, lacrimal gland and glands of nose and palate.
ORIGINThe two roots of facial nerve emerge from the anterior surface of brain between the pons and medulla oblongata. They pass laterally forward in the posterior

cranial fossa with the Vestibulocochlear nerve to the opening of internal acoustic meatus. At the bottom of the meatus the nerve enters the facial canal runs laterally above the vestibule of labyrinth until it reaches the medial wall of tympanic cavity. (Middle ear)Here the nerve expands to form sensory Geniculate ganglion. The nerve then bends sharply backwards above the promontory, on arriving at the posterior wall of the middle ear, it curves downward. On the medial side of the aditus of the mastoid antrum. It descends in the posterior wall of middle ear, behind the pyramid and finally emerges through the stylomastoid foramen.
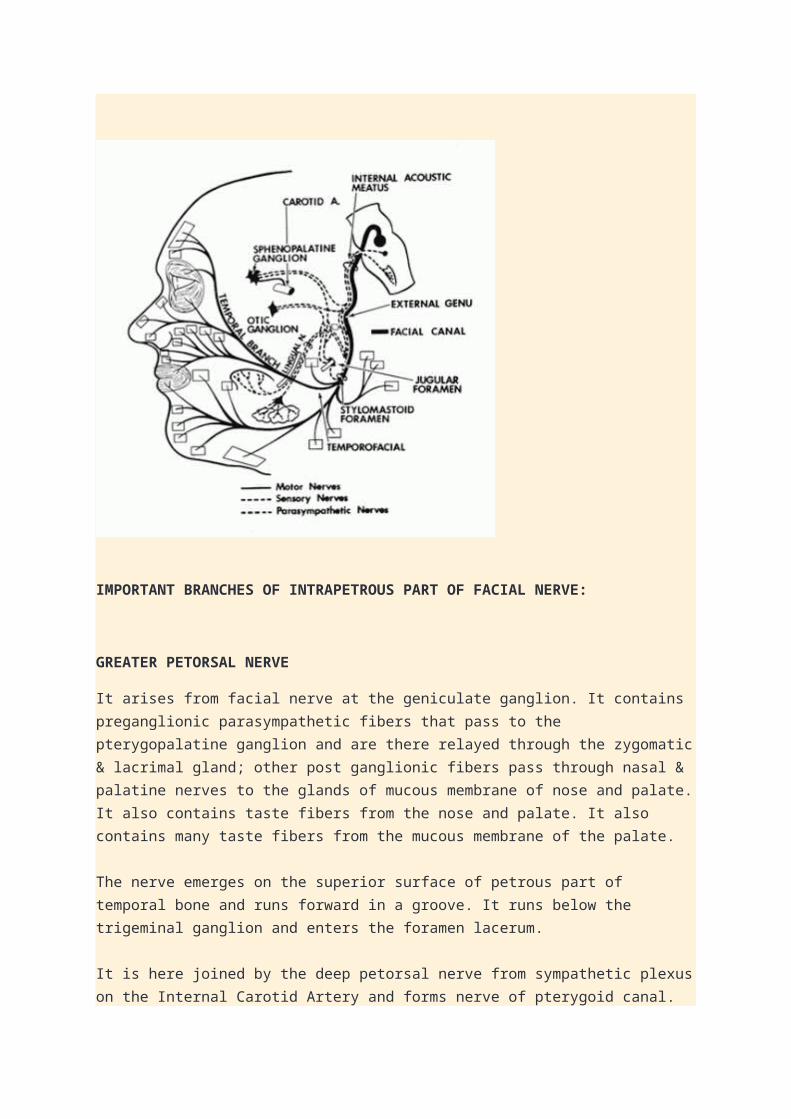
IMPORTANT BRANCHES OF INTRAPETROUS PART OF FACIAL NERVE:
GREATER PETORSAL NERVE
It arises from facial nerve at the geniculate ganglion. It contains preganglionic parasympathetic fibers that pass to the pterygopalatine ganglion and are there relayed through the zygomatic & lacrimal gland; other post ganglionic fibers pass through nasal & palatine nerves to the glands of mucous membrane of nose and palate. It also contains taste fibers from the nose and palate. It also contains many taste fibers from the mucous membrane of the palate.
The nerve emerges on the superior surface of petrous part of temporal bone and runs forward in a groove. It runs below the trigeminal ganglion and enters the foramen lacerum.
It is here joined by the deep petorsal nerve from sympathetic plexus on the Internal Carotid Artery and forms nerve of pterygoid canal. This passes forward and enters the pterygopalatine fossa where it ends in the pterygopalatine ganglion.
THE NERVE TO STAPEDIUSIt arises from the facial nerve as it descends in the facial canal behind the pyramid. It supplies the muscle with in the pyramid.
CHORDA TYMPANIIt arises from the facial nerve above the stylomastoid foramen. It enters the middle ear close to posterior border of tympanic membrane. It then runs forward over the tympanic membrane and crosses the root of the handle of the malleus. It lies in the interval between the mucous membrane and the fibrous layer of tympanic membrane.Taste fibersThe nerve leaves the middle ear through petrotympanic fissure and enters infratemporal fossa where it joins the lingual nerve. Chorda tympani contain many taste fibers from the mucous membrane covering the anterior two thirds of tongue. (not the vallate papillae)Taste fibers are the peripheral processes of the cells in the Geniculate ganglion.Parasympathetic secretomotor fibersThe nerve also contains pre ganglionic parasympathetic secretomotor fibers that reach the Submandibular ganglion and are there relayed to the Submandibular and sublingual salivary gland.As the nerve runs forward in the substance of parotid gland. It divides into 5 terminal branches

BRANCHES AT ITS EXIT FROM THE STYLOMASTOID FORAMEN
THE POSTERIOR AURICULAR NERVE:It arises just below the stylomastoid foramen. It ascends between the mastoid process and the external acoustic meatus and supplies the· Auricularis posterior· The Occipitalis· Intrinsic muscles on the back of the auricle
THE DIAGASTRIC BRANCHIt arises close to the previous nerve. It is short and supplies the posterior belly of diagastric muscle.
THE STYLOHYOID BRANCHIt may arise with the diagastric branch. It is long and supplies the stylohyoid muscle.

TERMINAL BRANCHES WITH IN THE PAROTID GLAND
THE TEMPORAL BRANCHIt emerges from the upper border of the gland and suppliesThe anterior and superior auricular musclesThe frontal belly of occipitofrontalisThe orbicularis occuliThe corrugator supercilli
THE ZYGOMATIC BRANCHIt emerges from the anterior border of the gland and supplies the orbicularis occuli
THE BUCCAL BRANCHIt emerges from the anterior border of gland below the parotid duct and supplies the buccinator muscle and muscles of upper lip and nostril.
THE MANDIBULAR BRANCHIt emerges from the anterior border of the gland and supplies the muscles of lower lip.
THE CERVICAL BRANCHIt emerges from the lower border of the gland and passes forward in the neck below the mandible to supply depressor anguli oris muscle.
The facial nerve is the nerve of second arch and supplies all muscles of facial

expression. It does not supply skin but its branches communicate with branches of trigeminal nerve.
EXAMINATIONRoutinely only the motor function of the 7th nerve is tested.
MOTOR FUNCTION· When 7th nerve is paralyzed, the patient may complain of inability to close the eyelid, collection of food in the mouth and dribbling of saliva on the affected side of the mouth and deviation of the angle of the mouth towards the opposite side.
On inspection, palpebral fissure may be wide and nasolabial fold may be flattened on theparalyzed side.· Ask the patient to frown or wrinkle the forehead.
There would be no wrinkling on the affe cted side.
· Ask the patient to close the eyes; the affected side will remain open and there will be brisk upward rolling of the eye ball (Bell’s phenomenon). To test the power of orbicularis occuli ask the patient to close the eyes as strongly as possible while you try to open the upper eyelids. The affected side will be weak.· Ask the patient to inflate the cheek and tap on both sides with finger. The weak side will be deflated easily.· Ask the patient to show the teeth. The angle of mouth will be deviated
towards the healthy side.· The patient cannot whistle as air escapes from the paralyzed side.· The patient will complain of unusually loud sounds on paralyzed if nerve to Stapedius is involved.
TASTETest taste of the anterior two third of the tongue by following technique.· Get solutions of four common tastes- sweet, salt, sour and bitter.· Instruct the patient to identify the taste, either by writing or raising fingers, e.g. one finger if taste is sweet, two fingers if salty and so on.· Ask the patient to protrude the tongue. Hold it with a gauze, dry it and test each side separately.· Put a drop of each solution one by one and ask for response.· Test bitter at the end.
SECRETOMOTOR FUNCTIONLacrimation and salivation can be tested by various tests but it is not done routinely.
INTERPRETATION
The facial nerve is the most commonly affected cranial nerve by lesion of both upper motor neuron and lower motor neuron.
UPPER MOTOR NEURON LESIONManifestations are on the opposite side. Upper half of the face (wrinkling of the forehead, closure of the eyelid) is less severely affected because the part of the facial nerve nucleus which supplies muscles of the upper half of the face is connected with both cerebral hemispheres; the part of the facial nerve nucleus which supplies muscles of lower half of the face is connected only with the contra lateral cerebral hemispheres. Smiling and other emotional movements are usually preserved in UMN lesion because there is a separate path for these movements.
LOWER MOTOR NEURON LESIONWhole of the ipsilateral half of the face is affected. Bell’s palsy is the most common cause of isolated lower motor neuron facial palsy. Etiology is unknown. The lesion is in the facial canal.
As facial nerve has a long route and gives off branches at various sites, the site of lesion can be localized with considerable precision.
· If the lesion is after the nerve exits from the skull, there is only weakness of the facial muscles.· If the lesion is in the facial canal, between the chorda tympani and branch to Stapedius, in addition to motor weakness, there is loss of taste as well.· If the lesion is between the branch to Stapedius and internal auditory

meatus, there is hyperacusis on the affected side, in addition to motor weakness and loss of taste.· Geniculate ganglion can be affected by herpes zoster(Ramsay Hunt syndrome). In addition to other features of facial palsy, there are vesicles in that part of external auditory meatus which gets sensory supply from the facial nerve.· If the lesion is in the internal auditory meatus, in addition to the features of facial nerve palsy, 8th nerve is also paralyzed.· If the lesion is in the cerebello-pontine angle, there are signs of cerebellar dysfunction and 5th, 6th, 7th, and 8th nerves are also involved.· In pontine lesion, along with the facial nerve, the 6th nerve is also paralyzed and there is upper motor neuron hemiplagia on the opposite side.

Posted by Amber Munir at 12:20 PM
3 comments:
1.
Dr.Shireen October 25, 2011 at 6:16 AM
Very helpful post.Thanks a lot!
Reply
Replies
1.
Amber Munir June 26, 2012 at 8:04 AM ur welcum :)
Reply

2.
Richelle Yeexin December 9, 2013 at 10:49 PM
Thank you this is a good explanation!
Reply
Newer Post Older Post Home
Subscribe to: Post Comments (Atom)


















