
Craig&Young,&MD& - American College of Sports …forms.acsm.org/2014ATPC/PDFs/56 Young.pdf ·...
24
CraigYoung, MD
Transcript of Craig&Young,&MD& - American College of Sports …forms.acsm.org/2014ATPC/PDFs/56 Young.pdf ·...

Craig Young, MD

! 1903 Thomas & Cushing cervical rib syndrome & surgical tx
! Scalenus an=cus syndrome -‐ Adson maneuver ! Costoclavicular syndrome -‐military brace posi=on test
! Subcoracoid-‐pectoralis minor syndrome -‐arm hyperabduc=on
! 1956 Peete groups as “TOS”

! “Thoracic outlet” borders ! 1st rib ! Clavicle ! Subclavius muscle ! Costoclavicular ligament ! Anterior scalene muscle
Wikipedia
! Interscalene triangle – space demarcated by anterior & middle scalenes & 1st rib ! Scalene hiatus -‐ space between anterior & middle scalenes ▪ Brachial plexus & subclavian artery pass through
! Costoclavicular space (between 1st rib & clavicle)
! Subcoracoid space (region beneath pectoralis minor tendon

! By event ! Trauma, repe==ve stress, postural abnormali=es
! By affected structure ! Neurogenic -‐ compression of brachial plexus. ▪ 90% of all TOS cases
! Arterial —compression of the subclavian artery ! Venous —compression of the subclavian vein ! Neurovascular
! By cause of compression ! Scalenus an=cus—muscle growth/inflamma=on ! Cervical rib syndrome
! Non-‐specific -‐ controversial

! 1 per million persons ! Young to middle aged ! Women more common ! Compression of brachial plexus by fibrous band from 1st thoracic rib to bony anomaly @C7 level
! Scalenus Anticus Syndrome

! Lower trunk most involved ! Thenar eminence > ulnar hand intrinsics> medial forearm
! Motor >> sensory ▪ Medial forearm>medial had

! Long h/o aching medial upper extremity ! Patchy sensory loss medial upper extremity ! Motor abnormali=es in C8 & T1 nerve root distribu=on ! T1 median & ulnar nerve–innervated muscles ! C8 median, ulnar & radial innervated muscles

! localized tenderness to palpa=on over the supraclavicular or subcoracoid space
! Posi=onal exacerba=on tests ! Adson maneuver ! Military brace posi=on ! Arm hyperabduc=on tests ! Wright test ! Roos stress test
! Gold standard electrodiagnos=c tes=ng (EDX)

! Non-‐surgical (PT, lifestyle modifica=on, steroid injec=on)
! Surgical resec=on ! Good prognos=c indicators ▪ Scalene block response ▪ Younger pa=ent ▪ Shorter dura=on of symptoms ▪ Non-‐smoker

! Uncommon ! Suspicious findings
! Long h/o aching medial upper extremity ! Patchy sensory loss medial upper extremity ! Motor abnormali=es in C8 & T1 nerve root distribu=on
! Posi=onal exacerba=on tests reproduce S&S ! Electrodiagnos=c tes=ng (+)


! Tested shoulder in slight abduc=on & extension.
! Pa=ent extends neck & turns head toward affected shoulder.
! Pa=ent inhales while examiner palpates ipsilateral radial pulse.
! Posi=ve test = pulse diminishes or paresthesias ! Unless maneuver causes symptoms on asymptoma=c side as well.
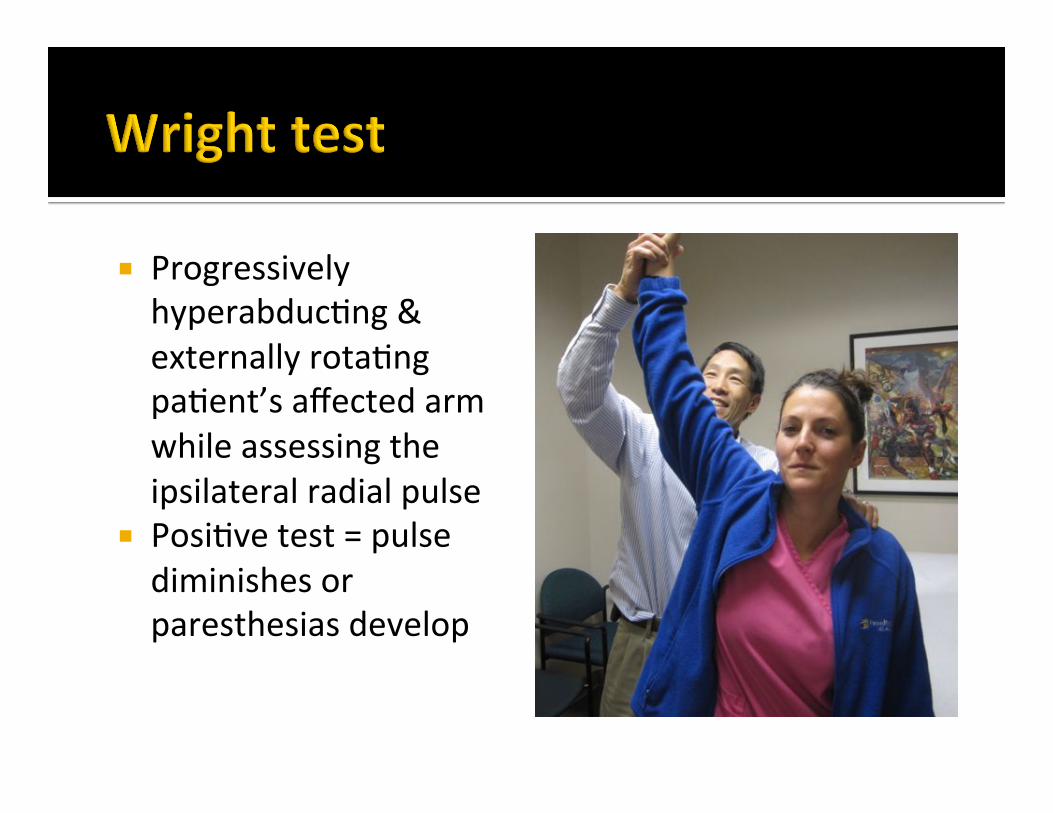
! Progressively hyperabduc=ng & externally rota=ng pa=ent’s affected arm while assessing the ipsilateral radial pulse
! Posi=ve test = pulse diminishes or paresthesias develop

! Elbow flexed to 90° shoulder 90 ° abduc=on & externally rotated 90° (90-‐90-‐90 posi=on)
! Head rotated away from test side
! Posi=ve test = disappearance of pulse

! Pa=ent standing ! Passively extends & abducts arm to 30°
! Pa=ent hyperextends head & neck
! Posi=ve test = diminishing radial pulse

! Posi=on both shoulders in 90°of abduc=on & external rota=on with 90°elbow flexion
! Pa=ent opens & closes hands for several minutes.
! Posi=ve test = reproduc=on of symptoms

! East test ! Similar to Roos but arms just abducted overhead
! Halstead maneuver ! Similar to Adson maneuver except head turned to contralateral side & examiner applies downward trac=on on test arm

! Rare ! Usually unilateral ! Young adults ! Subclavian artery compression between anterior scalene & large bony anomaly ! Fully formed cervical rib (the most common anomaly) ! Protuberant supernumerary bony process ! Deformed first thoracic rib

! Rare ! Usually unilateral ! Adult ! Spontaneous thrombosis of subclavian or axillary vein ! Underlying compressive anomaly that predisposes

! Rare ! Usually unilateral ! More common in adult men ! Post clavicular trauma
! Mid-‐sham fracture

! High “incidence” (up to 8% popula=on according to one proponent)
! Frequent bilateral occurrence; ! Lack of consistent S&S ! No EDX or vascular imaging abnormali=es ! Variable treatment outcomes

! Aralasmak A. Cevikol C. Karaali K. Senol U. Sharifov R. Kilicarslan R. Alkan A. MRI findings in thoracic outlet syndrome. Skeletal Radiol 2012; 41:1365–74
! Ferrante MA. The thoracic outlet syndromes. Muscle Nerve 2012; 45: 780-‐95.
! Rochlin DH. Likes KC. Gilson MM. Christo PJ. Freischlag JA. Management of unresolved, recurrent, and/or contralateral neurogenic symptoms in pa=ents following first rib resec=on and scalenectomy. J Vasc Surg 2012; 56(4):1061-‐8.

! Thompson RW. Challenges in the treatment of thoracic outlet syndrome. Texas Heart Ins=tute J 2012; 39(6):842-‐3
! Tsao BE. Ferrante MA. Wilbourn AJ. Shields RW. Electrodiagnos=c features of true neurogenic thoracic outlet syndrome. Muscle Nerve 2014; 49: 724–7.
! Twaij H, Rolls A, Sinisi M, Weiler R. Thoracic outlet syndromes in sport: a prac=cal review in the face of limited evidence — unusual pain presenta=on in an athlete. Br J Sport Med 2013; 47:1080-‐84


















