Cover Sheet for Example Documentation for PHAB · PDF fileexample of Health Department...
47
Cover Sheet for Example Documentation for PHAB Domain 2 Standard 1 Measure 1 The following documentation has been submitted to ASTHO for the Accreditation Library as a potential example of Health Department documentation that might meet the PHAB Standard and Measure 2.1.1 . This document is not intended to be a template, but is a reference as state health agencies develop and select accreditation documentation specific to the health department's activities. Please note that the inclusion of documentation in this library does not indicate official approval or acceptance by PHAB. Document Title: Completeness Review SOP - General; Salmonella and Pertussis Protocols Revised; Completeness Review - Pertussis Contact Worksheet Document Date: 2014 Version of Standards and Measures Used: 1.0 Related PHAB Standard and Measure Number Domain: 2 Standard: 1 Measure: 1 Required Documentation: RD 1 Short description of how this document meets the Standard and Measure’s requirements: Infectious disease investigations at the Maine CDC are initially assessed by an epidemiologist on-call, and subsequently assigned to appropriate infectious disease epidemiologists. This process is documented in the 2014. Specific procedures, including investigation steps, case definitions, laboratory testing, and reporting requirements are included for two specific diseases. Submitting Agency: Maine Center for Disease Control and Prevention Staff Contact Name: Nancy Birkhimer Staff Contact Position: Accreditation and Performance Improvement Manager Staff Contact Email: [email protected] Staff Contact Phone: 207-287-5716
Transcript of Cover Sheet for Example Documentation for PHAB · PDF fileexample of Health Department...
Cover Sheet for Example Documentation for PHAB Domain 2 Standard 1 Measure 1
The following documentation has been submitted to ASTHO for the Accreditation Library as a potential example of Health Department documentation that might meet the PHAB Standard and Measure 2.1.1 . This document is not intended to be a template, but is a reference as state health agencies develop and select accreditation documentation specific to the health department's activities.
Please note that the inclusion of documentation in this library does not indicate official approval or acceptance by PHAB.
Document Title:
Completeness Review SOP - General; Salmonella and Pertussis Protocols Revised; Completeness Review - Pertussis Contact Worksheet
Document Date:
2014
Version of Standards and Measures Used: 1.0
Related PHAB Standard and Measure Number
Domain: 2 Standard: 1 Measure: 1 Required Documentation:
RD 1
Short description of how this document meets the Standard and Measure’s requirements: Infectious disease investigations at the Maine CDC are initially assessed by an epidemiologist on-call, and subsequently assigned to appropriate infectious disease epidemiologists. This process is documented in the 2014. Specific procedures, including investigation steps, case definitions, laboratory testing, and reporting requirements are included for two specific diseases.
Submitting Agency:
Maine Center for Disease Control and Prevention
Staff Contact Name:
Nancy Birkhimer
Staff Contact Position:
Accreditation and Performance Improvement Manager
Staff Contact Email: [email protected]
Staff Contact Phone:
207-287-5716
ID EPI SOP
Category Number Applicability ID Epi Program Effective Date August 16, 2012
Approved by:
Reviewed on: 03/04/2014 Subject: Epi-on-call duties- General Purpose: To outline the duties of Epi-on-call for the purposes of standardization. Procedures: Table of contents
1. Preparing to go on call …………………………………………………. 1 2. Routine EOC work ……………………………………………………… 2 - 4 3. Closing cases …………………………………………………………… 5 4. Investigating outbreaks ………………………………………………… 5 5. Investigating notifiable conditions in out-of-state residents ……….. 5 6. Administrative help …………………………………………………….. 5 7. Other information ………………………………………………………. 5 8. Additional EOC Duties …………………………………………………. 5 9. References ………………………………………………………………. 6-7
1. Preparing to go on call a. Software access: Before going on call, new Epidemiologists-on-Call (EOC) should gain
access to the following software: i. [email protected] inbox (and access to send emails from it) ii. Consult Database iii. NEDSS (Epidemiologist II permission) iv. STARLIMS v. ImmPact
b. Get key to lock box. c. Training
i. Conduct the following activities up to one month prior to going on call: 1. NEDSS training with Data Manager 2. Practice entry with the NEDSS test environment using previous case review
copies 3. Enter non-investigated lab reports: Giardia, MRSA (invasive), GBS (non-
infant) 4. Practice closing cases (refer to ‘NEDSS case documentation’) 5. Start gathering list of EOC Reference Sheets (see Reference) 6. Shadow epi-on-call
ii. Conduct the following activities during the first week of being on call: 1. Central epis will create a schedule whereby one will sit with you each day,
especially during the morning, and then be available for questions for the rest of the day.
2. Refer to ‘Routine EOC Work’ in this SOP for guidance.
2. Routine EOC work 1
a. Perform the following duties each morning: i. Make sure CFV button is turned off/pressed (light is green when “on”). ii. When admin staff is unavailable, unlock cabinets.
1. Key 29: Surv. Room cabinets, black and white cabinets behind the door (Epi Room)
2. Key 33: D2 Current Epi Data (Hallway) 3. Key 40: Past Year Cases (Hallway) 4. Key 41: Open Cases, stacked cabinets (Epi Room)
iii. Check Epi Staff Calendar for absences (S:\Operations\Calendars\EpiStaffCalendar) iv. Check Med Epi (S:\Operations\Calendars) and SMEOC schedules (Q:\After Hours
On-Call\Schedules\Subject Matter Expert On-Call) v. Take notes at Epi AM call, type up notes (use Epi AM Notes Template), save as
PDF, and send out PDF by noon using Epi AM call distribution list. Be sure to save the notes under the correct month in S:\Operations\Meetings\EpiAMNotes\EpiNotes[YEAR].
vi. Perform StarLims EOC Query and EOC Rabies Query: EOC is responsible for checking the EOC Query and the EOC Rabies Query in StarLims. EOC will identify any submissions of public health importance and can initiate investigation or other follow up activities as needed. This query shall be checked at least twice daily, preferably in the morning and afternoon. From StarLims, go to QBE Reports and under Report Template select EOC Query and EOC Rabies Query, one at a time. Set the date for one day prior through the present date to miss any records that came in since the last check. The query will pull new lab test submissions for selected diseases (see StarLims Reporting Matrix).
b. Perform these activities throughout the day: i. Keep track of cases and consults assigned each day. Get a clean Epi-on-Call Daily
Checklist and on the flip side keep a tally of consults and investigations, making note of which field epidemiologists (FEs) are out. Circle consults and investigations that are sent out-of-area.
ii. Consults: Check the disease.reporting inbox. Forward consults to the appropriate FE by public health district, or by another method if a FE is absent (see Assignment of Disease Reports and Consultations SOP).
1. Epidemiology staff is expected to maintain core service hours, 8:00 am – 5:00 pm. Consults related to existing cases and received during core hours will be assigned to the epi investigating this event. Investigating epidemiologists will attempt to provide immediate assistance/response to urgent consultations and reports during core hours. Non-urgent consultations and reports will be responded to within one business day. In the event an epi is not able to respond in the given time frames, he/she will notify the EOC who will work with the Program Manager or other epis to respond appropriately.
2. If consults come directly to your phone, document on a blue sheet and send out to the appropriate FE.
3. You may need to forward consults to agency partners such as Agriculture or USDA, or ME CDC partners such as the immunization (MIP) or Health Inspections Programs (HIP).
4. See Table 1 for resources available to assist you in assigning non-reportable conditions consults.
Table 1: Management of non-reportable conditions Condition Resource
Consults regarding livestock; State Veterinarian/Interim State Veterinarian
2
EEE in turkeys (EEE results should go to Vector Epi) Dead birds If >=3 dead birds, forward consult to USDA. If <3,
advise caller to safely dispose of birds. Food/Water Borne Complaints Food/Water Borne Complaint SOP HIV/STD/Hep C HIV/STD/Viral Hepatitis Program Manager for
forwarding to the appropriate subject matter expert (SME)
Immunization Maine Immunization Program: [email protected]
Non-Reportables (bed bugs, lice, mold, etc.)
Non-Reportables SOP
TB TB Control Coordinator or designee Other non-infectious conditions Maine CDC Staff Telephone Listing and Maine
CDC Staff Location Listing to determine the best contact. Verify in your email that this is the appropriate person to handle the contact.
If a consult comes in through constituent services:
Forward or respond appropriately, cc’ing the administrator who initially took the call
iii. Disease Reports: Disease reports will come in either by phone (recorded on a blue
sheet by admin staff), fax, or electronically via NEDSS. Check the wire basket periodically for blue sheets and paper lab reports.
1. Epidemiology staff is expected to maintain core service hours, 8:00 am – 5:00 pm. Disease reports related to existing cases and received during core hours will be assigned to the Epidemiologist investigating this event. Investigating epidemiologists will attempt to provide immediate assistance/response to urgent consultations and reports during core hours. Non-urgent consultations and reports will be responded to within one business day. In the event an epidemiologist is not able to respond in the given time frames, they will notify the EOC who will work with the Program manager or other epidemiologists to respond appropriately.
2. Entering Paper Disease Reports in NBS: EOC and Administrative Staff will enter all new disease reports in to NBS. Only reports deemed to be a duplicate report (e.g. report matches exact report already in NBS) will not be entered.
a. Search for the cases in NEDSS by DOB. i. If there are no entries for that DOB, you can search by name to
ensure that this is truly a new case and not an incorrect DOB. 1. If this is a hepatitis B disease report, do not assume this is a
new case until you check the Hepatitis B Registry. The Registry is sorted alphabetically by last name.
a. If the case does not appear in the Registry, enter the report in NEDSS and send out for investigation based on the Hepatitis algorithm. b. If the case is in the Registry, enter the lab in NEDSS inserting a comment that this is known since YEAR, and submit (no investigation); delete record from the Registry and save the changes.
2. If this is a disease report for another disease besides hepatitis B, enter the report and assign the case for investigation based on the EOC Quick Reference.
3. If this is a disease report for an out of state resident, enter the lab in NEDSS and enter into the comment section the
3
date that interstate notification was sent. Fax the Interstate Notification Form and all labs to the appropriate state health department using the State Epi Contact List. File alphabetically in the out-of-state folder in the D2 Current Epi Data cabinet (hallway). Also refer to Out Of State Investigation SOP.
ii. If two cases have the same name and DOB, determine by address if they are the same person. This may require a call to the reporting laboratory. After confirming they are the same person, merge them manually. If there is any uncertainty that this is the same person, do not merge.
2. Managing electronic lab reports: Check NEDSS in the following order. a. Documents Requiring Security Assignment: Add the correct
condition/jurisdiction by clicking ‘transfer ownership’ unless it is a condition that is handled by another program. After you make a change, the entry will leave this queue and go into ‘Documents Requiring Review’
b. Documents Requiring Review: Ignore Lyme and Influenza reports (SMEs are actively reviewing these). Use your EOC Quick Reference to determine which conditions need to be assigned for investigation and which can be marked as reviewed. Never create an investigation directly from an entry in ‘Documents Requiring Review’. Rather, look up the patient by date of birth (DOB) to avoid duplicate entry. Follow b.iii.1.a.
iv. Routinely check NEDSS and disease.reporting inbox throughout the day. v. Routinely check the fax machines and wire basket (in Epi Room) for new disease
reports. vi. Assign cases. Write patient ID/investigation ID on lab report and name of FE. vii. As needed, merge patients in NEDSS and manage associations. Send email to
FE of change if necessary. viii. As time allows, close cases (see ‘Closing Cases’)
c. Perform these activities at the end of the day: i. Make files for non-paperless investigations assigned that day; file paperless
investigations alphabetically. ii. Count the number of consults assigned to the field and those that you handled
yourself. Enter on the Daily Checklist. iii. Email/call AHOC/MEOC to notify of any issues that have come up during the day
that may result in afterhours calls. iv. Check off the tasks completed (should be all) on the Daily Checklist; file this in the
Program Manager’s mailbox. v. When admin staff are unavailable:
i. Lock cabinets. ii. Make sure CFV button is turned on at 5:00pm (green). iii. Make sure the faxes have enough paper at the end of the day, especially at the
end of the week. 3. Closing Cases
a. As completed case report forms come in by fax, find the correct case file in the top of the open cases cabinet, add the completed case report form to the front of that case’s file, and file in the bottom tier of the wire basket in the Epi Room.
b. Close all cases by the end of the day take the closed case files from the bottom of the basket and close in NEDSS (under ‘approval queue for closed cases’). Use the Closing Cases Checklist to verify certain demographics fields are completed, case status is
4
correct, then approve. File closed cases alphabetically in the top of the closed cases wire basket in the top drawer of the Bottom Open Cases Cabinet in the Epi Room.
c. When closing outbreaks, verify that data on case report form match that in the outbreak database, make sure the outbreak is closed, write closed and the date in red on the outbreak report form. Ensure that if line list created is checked that a printed line list came in with the case report form. You may need to print this yourself from the line list option in the left column of the outbreak database screen. Put the closed file on the top of the closed cases wire basket in the top drawer of the Bottom Open Cases Cabinet in the Epi Room.
4. Investigating outbreaks
a. See Outbreak Protocol, S:\DiseaseSurveillance\Outbreaks.
5. Investigating notifiable conditions in out-of-state residents a. See Out-of-State Investigation SOP
6. Administrative help:
a. Administrative assistant can enter lab reports in NEDSS for these conditions: i. MRSA, invasive ii. GBS, invasive iii. Giardia
7. Additional EOC Duties a. At the beginning of a month, move the last month’s ‘not investigated’ folder to the far
right of the drawer, remove the papers from the previous year of the current month and give to Data Manager (Amy) for review; otherwise, shred.
b. Filing: Manage Epi Room Cabinet Folders (from front to back- see table): Table 3: Epi Room Cabinet Folders
File Action CO Poison File lab reports for carbon monoxide and other environmental conditions. STD/HIV/HCV File all HIV, STD, and HCV labs.
If HCV report has Hepatitis A or B positive results, write ‘copy to EOC’ on the top right, make a copy, and file the original in this folder. Keep the other copy and treat as a normal lab report.
5
Lyme labs File all Lyme lab reports HAI program File all HAI lab reports (still send Peg HAI consults) Rabies submission forms
File all negative and unsatisfactory lab reports with most recent date at the front
Rabies PEP forms File all rabies PEP reporting forms from the fax; Admin checks this folder and will enter these into NEDSS and then file elsewhere
Known chronic Hep B File all hep B lab reports after determining that they are known chronic cases. Enter lab report into NEDSS. Write ‘known chronic’ and patient ID on the top right. For more info, see ‘Epi-on-call management of hepatitis B lab reports.’
MRSA non-invasive File all MRSA lab reports with a non-invasive specimen source (i.e., wound)
Validation file When a paper lab report (or blue sheet disease report) comes in from NorDx, initial the report, make a copy, and file copy in this folder. File or act on the originals as appropriate. – NOT CURRENTLY ACTIVE
References:
1. Epi AM Notes Template, Epi Notes.doc, S:\Operations\Meetings\EpiAMNotes 2. Epi AM call distribution list (available electronically) 3. StarLims Reporting Matrix, StarLims Reporting Matrix_10252011.xlsx, S:\Policies,
Procedures & Plans\ID EPI\Epi-On-Call 4. Assignment of Disease Reports and Consultations (S:\Policies, Procedures &
Plans\ID EPI\Working Drafts) 5. Epi-on-Call Daily Checklist, Epi-on-CallChecklist0811.docx, S:\Policies, Procedures &
Plans\ID EPI\Epi-On-Call 6. Non-Reportables SOP, SOP11-OPS-Non-Reportables.doc, S:\Policies, Procedures &
Plans\ID EPI\Operations 7. Food/Water Borne Complaint SOP, SOP11-DIS-Food-Water Borne Complaints (Final)
5-1-11.docx, S:\Policies, Procedures & Plans\ID EPI\Operations 8. Maine CDC Staff Telephone Listing, Location List by Floor.doc, H:\Maine CDC Phone-
Locations Lists 9. Maine CDC Staff Location Listing, MCDC Staff Phone List.doc, H:\Maine CDC Phone-
Locations Lists 10. Hepatitis B Registry, ChronicHepatitisB.xls, S:\Disease Data\Hep B Registry 11. Hepatitis algorithm, hbv_algorithm (3).doc, S:\DiseaseSurveillance\HepB\Investigation 12. EOC Quick Reference, Epi-On-Call Quick-Ref_061412.xls, S:\Policies, Procedures &
Plans\ID EPI\Epi-On-Call 13. Interstate Notification Form, INTERSTATE_NOTIFICATION.doc, S:\Disease
Data\Forms & Templates (Dis Surveill) 14. State Epi Contact List, , State Epi Contacts 2010.pdf,
S:\Reference\PhoneDirectories\NationalHealthDepts 15. Out Of State Investigation SOP, SOP10-OPS-Out Of State Investigation.doc,
S:\Policies, Procedures & Plans\ID EPI\Operations 16. HETL EOC Notification SOP, SOP10-OPS-HETLEOCNotification_92910.doc,
S:\Policies, Procedures & Plans\ID EPI\Operations 17. White Powder SOP, White Powder SOP 3-19-12.doc,
S:\DiseaseSurveillance\RicinPoisoning\Investigation 18. Epi-on-call management of hepatitis B lab reports, Hep B surveillance algorithm.doc,
S:\DiseaseSurveillance\HepB 19. Varicella Investigation NEDSS entry, Varicella investigation NEDSS entry.docx,
S:\DiseaseSurveillance\Varicella\Investigation 20. Closing Cases Checklist 21. Outbreak Database, 2010outbreaks_FrontEnd.mdb,
S:\DiseaseSurveillance\Outbreaks\Database\Outbreak Databases
6
22. County/Town list 23. Zip code directory 24. Hospital quick code 25. Lab quick code 26. Lab entry spreadsheet 27. Epi Assignments (SME list)- needs updating 28. NEDSS case documentation (case closing checklist) 29. Epi-on-call management of hepatitis B lab reports 30. Naming rabies in NEDSS cheat sheet 31. HETL requisition email
Associated SOPs (available at S:\Policies, Procedures & Plans\ID EPI\Operations)
1. Non-Reportables SOP 2. Food/Water Borne Complaint SOP 3. Out-of-State Investigation SOP 4. HETL EOC Notification SOP 5. White Powder SOP 6. Assignment of Disease Reports and Consultations (S:\Policies, Procedures &
Plans\ID EPI\Working Drafts) 7. Work absence communication
Attachments: All references in order listed above
7
Maine Department of Health & Human ServicesMaine Center for Disease Control and Prevention
Salmonellosis Investigation Protocol
______________________________________________ 2/24/2014 2/2017
Stephen Sears, MD, MPH Effective Date Review Date State Epidemiologist
A. Salmonella - NonTyphoid
Reporting RequirementsMandatory report for laboratory confirmed cases. Report within 48 Hours
Case Definition
Clinical DescriptionAn illness of variable severity commonly manifested by diarrhea, abdominal pain, nausea, and sometimes vomiting. Asymptomatic infections may occur, and the organism may cause extraintestinal infections.
Laboratory Criteria for DiagnosisSuspect: Detection of Salmonella from a clinical specimen using a non-culture based method
Confirmed: Isolation of Salmonella from a clinical specimen.
Case ClassificationSuspect: A case that meets the suspect laboratory criteria for diagnosis
Probable: A clinically compatible case that is epidemiologically linked to a confirmed case, i.e., a contact of a confirmed case or member of a risk group as defined by public health authorities during an outbreak.
Confirmed: A case that meets the confirmed laboratory criteria for diagnosis. When available, O and H antigen serotype characterization should be reported.
CommentBoth asymptomatic infections and infections at sites other than the gastrointestinal tract, if laboratory confirmed, are considered confirmed cases that should be reported.
2/24/2014 2/2017Effective Date Review Date
pMaine Center for Disease Control and Prevention
Salmonellosis Investigation Protocol
Case Definition
within 48 HoursReporting RequirementsMandatory report for laboratory confirmed cases. Report
g
A. Salmonella - NonTyphoid
Both asymptomatic infections and infections at sites other than the gastrointestinal tract, if y p glaboratory confirmed, are considered confirmed cases that should be reported.
Salmonellosis – Investigation Protocol
Laboratory Testing Services Available
Most hospital and private laboratories conduct testing for Salmonella. The Maine Health and Environmental Testing Laboratory (HETL) also conducts testing (PCR and culture). All isolates must be sent to HETL for confirmation, serotyping and molecular subtyping using Pulsed Field Gel Electorphoresis (PFGE).
Purpose of Surveillance and ReportingMonitor trends in incidence and risk factors for diseaseAssess the burden of diseaseIdentify and control outbreaks Recommend preventative action as appropriate
Case Investigation
Initiate investigation within 48 hours of receipt of case reportContact health care provider for demographic and clinical informationInterview case or parent of a minoro Confirm demographics, symptom onset and durationo Use 72 hours prior to symptom onset, question case about potential exposureso If you have made at least 3 attempts with messages with no answer, over 48 hours,
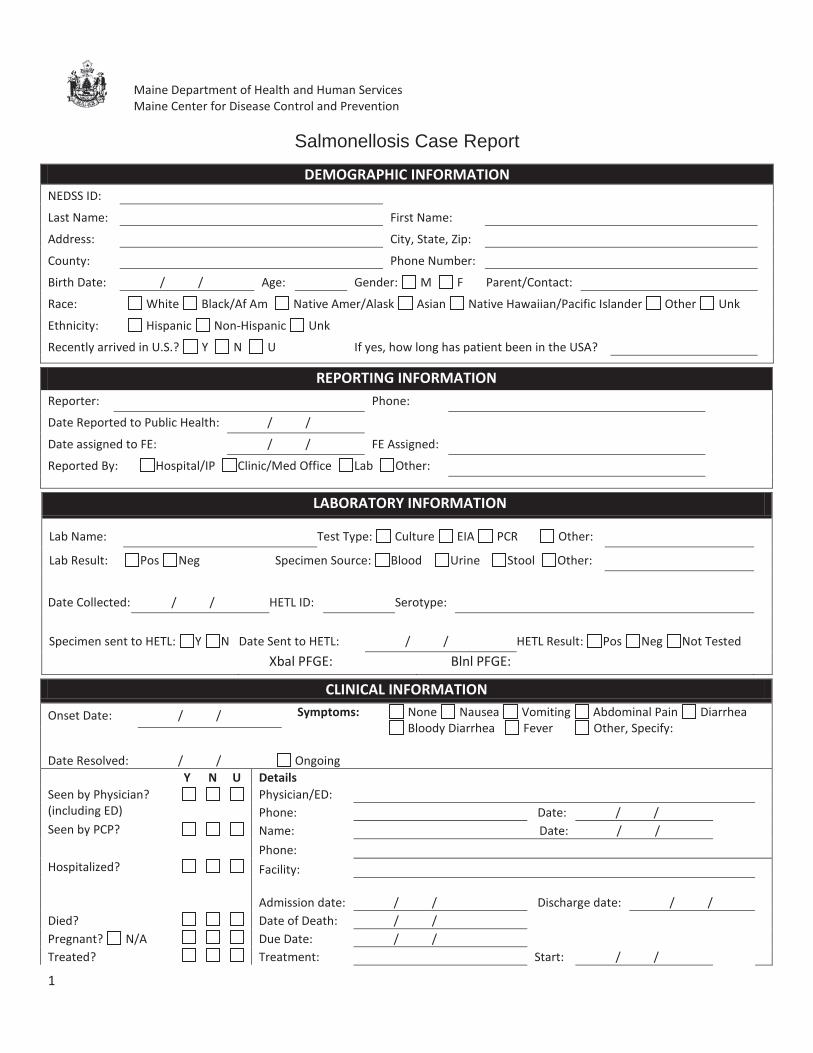
send letter to Case address requesting interview (see lost to follow up SOP).Complete Salmonellosis Case Report Form and enter into NEDSSIf paratyphi A, B or C serotype: Complete Federal CDC Typhoid and Paratyphoid Fever Surveillance Form. Note: questions ask for a different time period for travel history (30 days) and asks additional questions not on our form – an additional interview will be necessaryContact supervisor of case-patient and send exclusion letter if case-patient is in a sensitive occupation (see Managing Special Situations section)Consult with Medical Epidemiologists (ME) as needed
Recommendations for Control of Case and Contacts
Recommendation for CasePrevent ongoing transmission by:
Using proper hand hygieneUsing proper sanitation methods for food processing and preparationRefraining from preparing food for othersDisinfection of diaper changing areas and toilet facilities.
Recommendations for ContactsCulture stools of symptomatic household contacts involved in food handling, direct patient care, or daycare
2
Case Investigation
Initiate investigation within 48 hours of receipt of case reportContact health care provider for demographic and clinical informationInterview case or parent of a minoro
pConfirm demographics, symptom onset and duration
og p y p
Use 72 hours prior to symptom onset, question case about potential exposureso
p y p q p pIf you have made at least 3 attempts with messages with no answer, over 48 hours,y p gsend letter to Case address requesting interview (see lost to follow up SOP).
Complete Salmonellosis Case Report Form and enter into NEDSSIf paratyphi A, B or C serotype: Complete Federal CDC Typhoid and Paratyphoid Fever p yp yp p yp ypSurveillance Form. Note: questions ask for a different time period for travel history (30q p y (days) and asks additional questions not on our form – an additional interview will bey )necessaryContact supervisor of case-patient and send exclusion letter if case-patient is in a p psensitive occupation (see Managing Special Situations section)Consult with Medical Epidemiologists (ME) as needed
Salmonellosis – Investigation Protocol
Exclusions
CaseIndividuals should be excluded from providing direct patient care, providing childcare or food handling until diarrheal symptoms have resolved (CDC-HICPAC, American Academy of Pediatrics, Maine Food Code, Control of Communicable Diseases Manual). Exclusion for asymptomatic infected individuals in high risk settings may be indicated for those with questionable hygiene habits (Control of Communicable Diseases Manual).
Symptomatic Contacts See special situations below
Asymptomatic Contacts No restrictions
Managing Special Situations: Daycares, Schools, Healthcare Settings
Consult with Medical Epidemiologist prior to sending letters.
Recommendations for Daycare Centers
ExclusionExclude children and staff with diarrhea until diarrhea resolves (American Academy of Pediatrics). In cases where proper hygiene is questionable, may recommend exclusion of child and/or staff until receiving 2 negative stool samples separated by 24 hours with the first sample taken at least 48 hours after the completion of antibiotics, if antibiotics were prescribed (Control of Communicable Diseases Manual).
StrategiesIf a confirmed case of salmonellosis occurs in a childcare setting (employee or child):
Daycare directors should be contacted immediately and informed of the case.Confidentiality requirements need to be explained. Information is shared with the director on a need to know basis. Basic (non-identifying) information should be shared with staff and parents.Identify any staff or children with Salmonella like symptoms (diarrhea) and recommend testing and exclusion.Parents and staff must be notified. A letter (templates available on S drive) with the Salmonella fact sheets should be sent to parents/guardians and staff.
Recommendations for Schools
ExclusionExclude children and staff with diarrhea until diarrhea resolves (American Academy of Pediatrics).
3
Salmonellosis – Investigation Protocol
StrategiesIf a case of salmonellosis occurs in a kindergarten or preschool class, or a class where hygiene may not be optimal, more stringent control measures may be needed. See Daycare section above.Notification letters and fact sheets should be distributed to parents and guardians in certain situations - for example, a case handles food for other students.
Recommendations for Healthcare Settings
ExclusionWork with Infection Control and/or Employee Health Office to exclude clients or staff with symptoms.Symptomatic staff should not provide direct care and/or prepare or handle food during infectious period. Infected staff can fulfill other duties that do not involve food handling and/or direct care (CDC-HICPAC).In cases where proper hygiene is questionable, may recommend exclusion of staffmember until he/she obtains 2 negative stool samples separated by 24 hours with the first sample taken at least 48 hours after the completion of antibiotics, if antibiotic was prescribed (Control of Communicable Diseases Manual).
Managing Infected Food Handlers
A food handler is any person directly preparing or handling food. This can include a healthcare or childcare provider.
PreventionEnforce strict hygiene and good hand washing behaviors.Properly clean and cook foods.Maintain a kitchen and establishment in accordance with state regulations.
Control Strict hygiene and hand washing should be practiced.Enhance surveillance for diarrheal illness of staff.
ExclusionExclude food handlers with symptoms of diarrhea until (Maine Food Code):
Employee is asymptomatic for at least 24 hours; ORWritten medical documentation from a health practitioner states the symptom is from a noninfectious condition
In cases where proper hygiene is questionable, may recommend exclusion of staff until he/she obtains 2 negative stool samples separated by 24 hours with the first sample taken at least 48 hours after the completion of antibiotics, if antibiotics were prescribed (Control of Communicable Diseases Manual).
4
Salmonellosis – Investigation Protocol
StrategiesContact the manager/supervisor of the food handler and explain the confirmed case and steps that need to be taken. Confidentiality requirements need to be explained. Information is shared with the manager on a need to know basis.Review a complete food handling history of the case, for the 3 days before symptom onset, in order to determine if the public needs to be notified of possible exposure to Salmonella. Contact the Medical Epidemiologist or the Food-borne Epidemiologist once you complete this section to discuss next steps as needed.Contact the Foodborne Disease Epidemiologist to notify the Division of Environmental Health, Health Inspection Program (HIP) or the Department of Agriculture, Conservation and Forestry (DACF), Quality Assurance and Regulations Division for institution follow-upas needed.Coordinate interviews with other food handlers at the facility about recent illness with HIP or DACF, depending on agency involved in facility inspection.
B. Salmonella Typhi (Typhoid Fever)Clinical DescriptionAn illness caused by Salmonella enterica serotype Typhi that is often characterized by insidious onset of sustained fever, headache, malaise, anorexia, relative bradycardia, constipation or diarrhea, and nonproductive cough. However, many mild and atypical infections occur. Carriage of serotype Typhi may be prolonged.
Laboratory criteria for diagnosisIsolation of serotype Typhi from blood, stool, or clinical specimen
Case ClassificationProbable: a clinically compatible case that is epidemiologically linked to a confirmed case in an outbreak
Confirmed: a clinically compatible case that is laboratory confirmed.
Comment: Isolation of the organism is required for confirmation. Serologic evidence alone is not sufficient for diagnosis. Asymptomatic carriage should not be reported as typhoid fever. Isolates of Salmonella enterica serotype Typhi are reported to the Enteric Diseases Epidemiology Branch, Division of Foodborne, Waterborne, and Enteric Diseases, National Center for for Emerging and Zoonotic Infectious Diseases, CDC, through the Laboratory-Based Enteric Disease Surveillance (LEDS). In addition, a National Typhoid and Paratyphoid Fever Surveillance report form should be submitted for all cases (can be found here: http://www.cdc.gov/nationalsurveillance/typhoid_surveillance.html).
InvestigationConsult with Medical Epidemiology Initiate investigation within 24 hours of receipt of case reportContact health care provider for demographic and clinical informationo After 3 attempts, during regular business hours, use alternative means to obtain
necessary information
5
Investigation
B. Salmonella Typhi (Typhoid Fever)
Consult with Medical Epidemiology Initiate investigation within 24 hours of receipt of case reportgContact health care provider for demographic and clinical informationo
p g pAfter 3 attempts, during regular business hours, use alternative means to obtain pnecessary information
Isolation of the organism is required for confirmation. Serologic evidence alone is not g q gsufficient for diagnosis. Asymptomatic carriage should not be reported as typhoid fever.g y p g p ypIsolates of Salmonella enterica serotype Typhi are reported to the Enteric Diseasesyp yp pEpidemiology Branch, Division of Foodborne, Waterborne, and Enteric Diseases, Nationalp gyCenter for for Emerging and Zoonotic Infectious Diseases, CDC, through the Laboratory-g g gBased Enteric Disease Surveillance (LEDS). In addition, a National Typhoid and ( ) ypParatyphoid Fever Surveillance report form should be submitted for all cases
Clinical Descriptiony
pAn illness caused by Salmonella enterica serotype Typhi that is often characterized by y yp yp yinsidious onset of sustained fever, headache, malaise, anorexia, relative bradycardia, constipation or diarrhea, and nonproductive cough. However, manyy mild and atypical
y
infections occur. Carriage of serotype Typhi may be prolonged.p p g
Salmonellosis – Investigation Protocol
Interview case or parent of a minoro Confirm demographics and symptom onset and durationo Use 14 days prior to symptom onset to question about potential exposures. The
incubation period is 3 to 60 days with the usual range 8-14 days.o Identify if case in a high-risk occupationContact supervisor of case and send exclusion letter if case is in a sensitive occupation (see Managing Special Situations section)Complete the CDC Typhoid Fever Surveillance Report Form and the NEDSS report form for Salmonellosis.Fax completed CDC Typhoid Fever Surveillance Report Form to the central office.In order to determine if the public needs to be notified of possible exposure to Salmonellatyphi, if the case is a food handler, a complete food handling history of the case for the 14 days before symptom onset needs to be reviewed.Illness duration, without treatment may last 3-4 weeks.
ExclusionRelease from supervision of health authorities (for food handlers, health care related care, and children under 5 years of age attending daycare) is based on not fewer than 3 consecutive negative stool cultures at least 24 hours apart and obtained at least 48 hours after any antimicrobials, and not earlier than one month after onset of symptoms. If any of these are positive, obtain cultures at monthly intervals during the 12 months following onset until at least 3 consecutive negative cultures are obtained (American Academy of Pediatrics, Maine Food Code, CDC-HICPAC, Control of Communicable Diseases Manual). Food handlers require written documentation from a health care practitioner that states the employee is free from S. typhi infection AND approval from the health authority (Maine Food Code, 2-201.13(C)).Chronic carriers of Salmonella typhi should be excluded from food handling and from providing medical care. Carrier state may be prolonged, > 1 year. See bullet above for terms to return to food handling or providing medical care (Control of Communicable Diseases Manual)Consideration should be given to obtaining at least 2 negative stool and urine cultures,taken at least 24 hours apart, from household and close contacts before allowing them to be employed in sensitive occupations, such as food handling (Control of Communicable Diseases Manual)
For all household contacts of confirmed case: A household contact who is a food employee must be excluded until one of the following conditions is met (Maine Food Code):
More than 14 calendar days have passed since the last day the employee was potentially exposed; ORMore than 14 calendar days have passed since the employee’s household contact became asymptomatic
6
Interview case or parent of a minoro
pConfirm demographics and symptom onset and duration
og p y p
Use 14 days prior to symptom onset to question about potential exposures. They p y p q pincubation period is 3 to 60 days with the usual range 8-14 days.
op y
Identify if case in a high-risk occupationContact supervisor of case and send exclusion letter if case is in a sensitive occupationp(see Managing Special Situations section)Complete the CDC Typhoid Fever Surveillance Report Form and the NEDSS report formpfor Salmonellosis.Fax completed CDC Typhoid Fever Surveillance Report Form to the central office.yIn order to determine if the public needs to be notified of possible exposure to Salmonellap p ptyphi, if the case is a food handler, a complete food handling history of the case for the 14yp pdays before symptom onset needs to be reviewed.Illness duration, without treatment may last 3-4 weeks.
Salmonellosis – Investigation Protocol
References
See the following references for clinical information including identification, description of infectious agent, occurrence, reservoir, mode of transmission, incubation period, period of communicability, susceptibility, and further clinical information.
American Academy of Pediatrics. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed., Elk Grove Village, IL: American Academy of Pediatrics; 2012: 136-142, 635-640.American Academy of Pediatrics, Managing Infectious Diseases in Child Care and Schools, 2nd Edition p. 37-44, 2009.Centers for Disease Control and Prevention. Case Definitions, http://www.cdc.gov/osels/ph_surveillance/nndss/PHS/infdis2011.htmCenters for Disease Control and Prevention. Salmonella.http://www.cdc.gov/salmonella/Centers for Disease Control and Prevention. Salmonella Infection and Animals.http://www.cdc.gov/healthypets/diseases/salmonellosis.htmCenters for Disease Control and Prevention. Typhoid Fever.http://www.cdc.gov/nczved/divisions/dfbmd/diseases/typhoid_fever/technical.htmlCenters for Disease Control and Prevention. National Typhoid and Paratyphoid Fever Surveillance. http://www.cdc.gov/nationalsurveillance/typhoid_surveillance.htmlHeymann, David L., ed., Control of Communicable Diseases Manual, 19th Edition, p. 534-540, Washington DC, American Public Health Association, 2008. Maine Food Code. Chapter 2. http://www.maine.gov/dhhs/eng/el/rules.htmSiegel JD, Rhinehart E, Jackson M, Chiarello L, and the Healthcare Infection Control Practices Advisory Committee, 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings http://www.cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf. (CDC-HICPAC references in protocol is Appendix A page 93)
Attachments
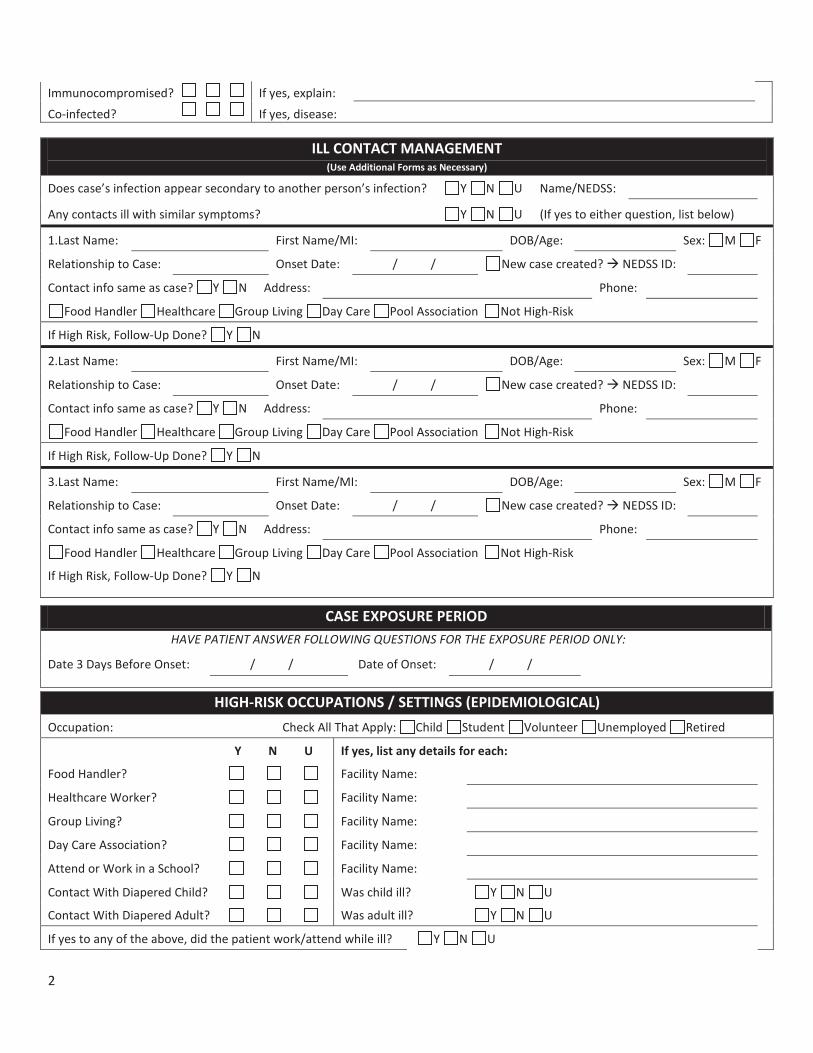
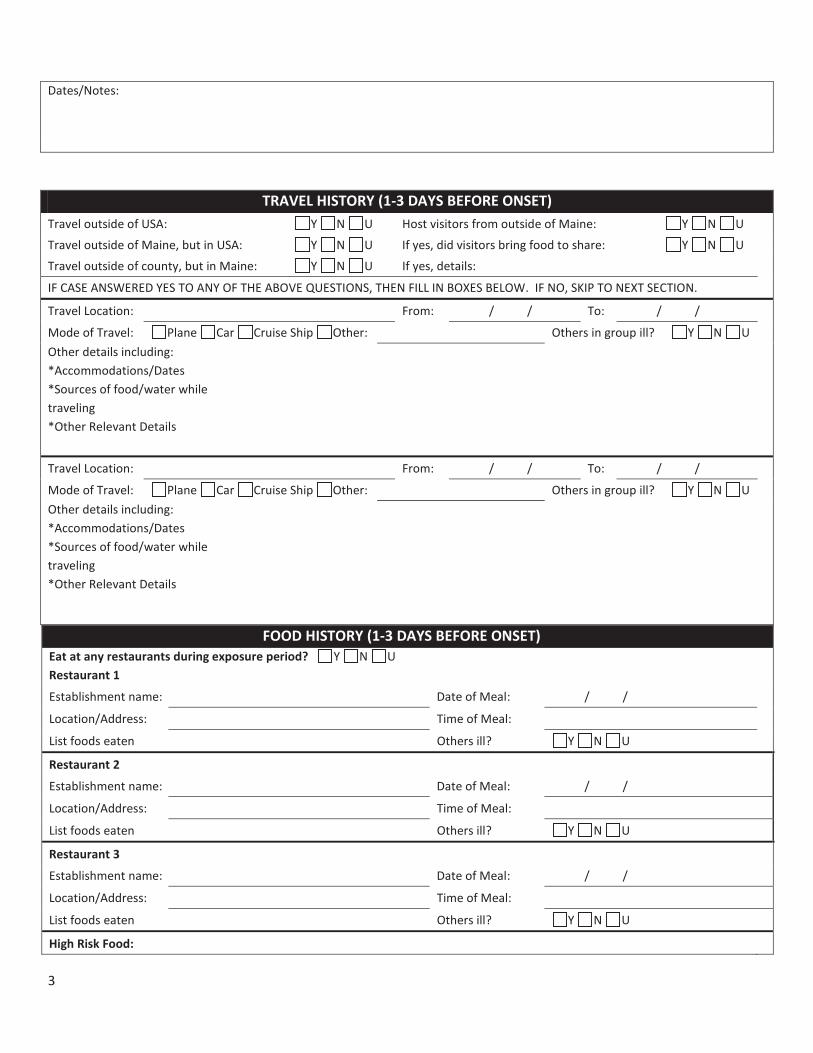
1. Salmonellosis case investigation form2. CDC Typhoid and Paratyphoid Fever Surveillance report form3. Salmonellosis Fact Sheet4. Exclusion letter5. Salmonellosis School Health Manual
7
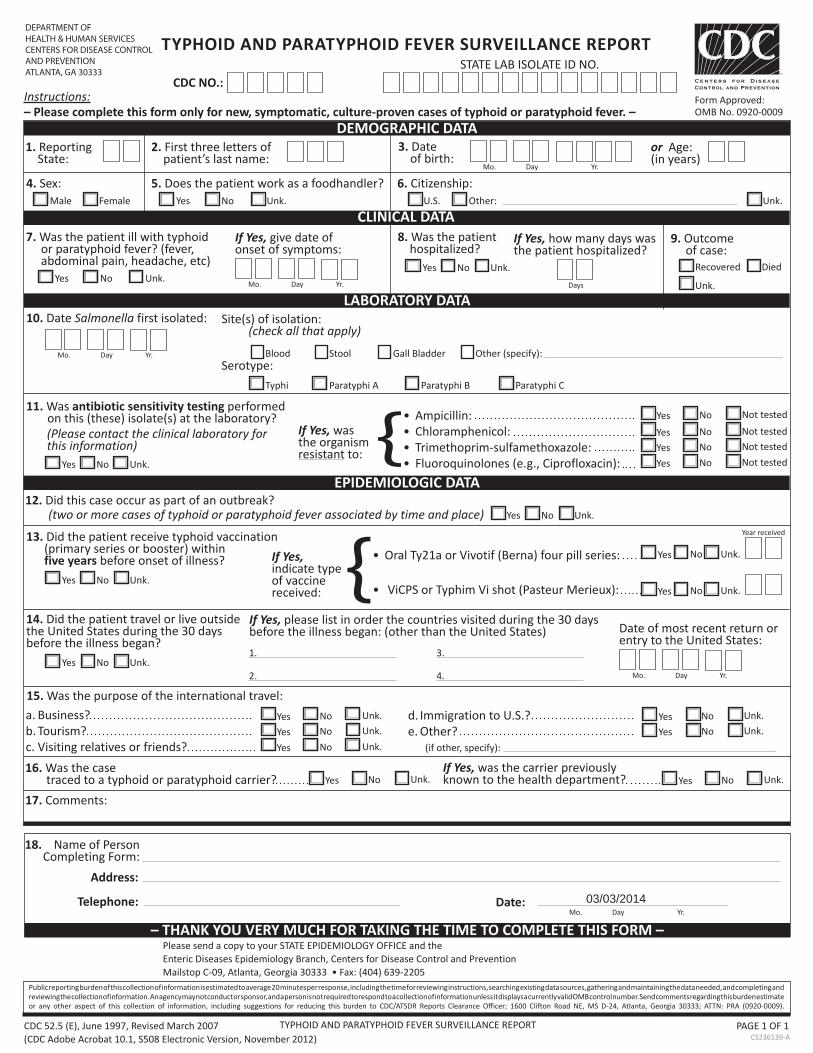
TYPHOID AND PARATYPHOID FEVER SURVEILLANCE REPORT
TYPHOID AND PARATYPHOID FEVER SURVEILLANCE REPORTSTATE LAB ISOLATE ID NO.
Instructions:– Please complete this form only for new, symptomatic, culture-proven cases of typhoid or paratyphoid fever. –
1. Reporting State:
4. Sex: 5. Does the patient work as a foodhandler?
7. Was the patient ill with typhoid If Yes, give date of 8. Was the patient 9. Outcome or paratyphoid fever? (fever, onset of symptoms: hospitalized? of case: abdominal pain, headache, etc)
11. Was antibiotic sensitivity testing performed on this (these) isolate(s) at the laboratory?
12. Did this case occur as part of an outbreak?
13. Did the patient receive typhoid vaccination (primary series or booster) within five years before onset of illness?
14. Did the patient travel or live outside the United States during the 30 days before the illness began?
15. Was the purpose of the international travel:
16. Was the case traced to a typhoid or paratyphoid carrier?17. Comments:
18. Name of Person Completing Form:
Address:
Telephone: Date:
CDC NO.:Form Approved:OMB No. 0920-0009
2. First three letters of 3. Date or Age: patient’s last name: of birth: (in years)
6. Citizenship:
If Yes, how many days was the patient hospitalized?
10. Date Salmonella first isolated: Site(s) of isolation: (check all that apply)
Serotype:
If Yes, wasthe organismresistant to:
If Yes,indicate typeof vaccine received:
If Yes, please list in order the countries visited during the 30 days before the illness began: (other than the United States) Date of most recent return or
entry to the United States:
If Yes, was the carrier previously known to the health department?
DEMOGRAPHIC DATA
CLINICAL DATA
LABORATORY DATA
EPIDEMIOLOGIC DATA
Mo. Day Yr.
Male Female Yes No Unk. U.S. Other: Unk.
Yes No Unk. Recovered DiedYes No Unk.
Mo. Day Yr. Days Unk.
Mo. Day Yr. Blood Stool Gall Bladder Other (specify):
Typhi Paratyphi A Paratyphi B Paratyphi C
Yes No Not tested
Yes No Not testedYes No Not tested
Yes No Unk. Yes No Not tested
Yes No Unk.
Yes No Unk.
Yes No Unk.Yes No Unk.
1. 3.Yes No Unk.
2. 4. Mo. Day Yr.
Yes No Unk. Yes No Unk.Yes No Unk. Yes No Unk.Yes No Unk.
Yes No Unk. Yes No Unk.
Mo. Day Yr.
DEPARTMENT OFHEALTH & HUMAN SERVICESCENTERS FOR DISEASE CONTROL AND PREVENTIONATLANTA, GA 30333
Ampicillin:(Please contact the clinical laboratory for Chlorthis information) { amphenicol:
Trimethoprim-sulfamethoxazole:Fluoroquinolones (e.g., Ciprofloxacin):
(two or more cases of typhoid or paratyphoid fever associat
{ed by time and place)
Oral Ty21a or Vivotif (Berna) four pill series:
ViCPS or Typhim Vi shot (Pasteur Merieux):
a. Business?b. Tourism?c. Visiting relatives or friends?
Year received
d. Immigration to U.S.?e. Other?
(if other, specify):
– THANK YOU VERY MUCH FOR TAKING THE TIME TO COMPLETE THIS FORM –Please send a copy to your STATE EPIDEMIOLOGY OFFICE and theEnteric Diseases Epidemiology Branch, Centers for Disease Control and Prevention
Public reporting burden of this collection of information is estimated to average 20 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing andreviewing the collection of information. An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate
PAGE 1 OF 1
03/03/2014
Maine Department of Health and Human Services Maine Center for Disease Control and Prevention
Salmonellosis Case Report
DEMOGRAPHIC INFORMATION NEDSS ID:
Last Name: First Name:
Address: City, State, Zip:
County: Phone Number:
Birth Date: / / Age: Gender: M F Parent/Contact:
Race: White Black/Af Am Native Amer/Alask Asian Native Hawaiian/Pacific Islander Other Unk
Ethnicity: Hispanic Non-Hispanic Unk
Recently arrived in U.S.? Y N U If yes, how long has patient been in the USA?
REPORTING INFORMATION Reporter: Phone:
Date Reported to Public Health: / /
Date assigned to FE: / / FE Assigned:
Reported By: Hospital/IP Clinic/Med Office Lab Other:
LABORATORY INFORMATION
Lab Name: Test Type: Culture EIA PCR Other:
Lab Result: Pos Neg Specimen Source: Blood Urine Stool Other:
Date Collected: / /
HETL ID: Serotype:
Specimen sent to HETL: Y N Date Sent to HETL: / / HETL Result: Pos Neg Not Tested
Xbal PFGE: Blnl PFGE:
CLINICAL INFORMATION Onset Date: / / Symptoms: None Nausea Vomiting Abdominal Pain Diarrhea
Bloody Diarrhea Fever Other, Specify:
Date Resolved: / / Ongoing Y N U Details Seen by Physician? (including ED)
Physician/ED: Phone: Date: / /
Seen by PCP? Name: Date: / / Phone: Hospitalized? Facility:
Admission date: / / Discharge date: / /
Died? Date of Death: / / Pregnant? N/A Due Date: / / Treated? Treatment: Start: / /
1
Immunocompromised? If yes, explain:
Co-infected? If yes, disease:
ILL CONTACT MANAGEMENT (Use Additional Forms as Necessary)
Does case’s infection appear secondary to another person’s infection? Y N U Name/NEDSS:
Any contacts ill with similar symptoms? Y N U (If yes to either question, list below)
1.Last Name: First Name/MI: DOB/Age: Sex: M F
Relationship to Case: Onset Date: / / New case created? NEDSS ID:
Contact info same as case? Y N Address: Phone:
Food Handler Healthcare Group Living Day Care Pool Association Not High-Risk
If High Risk, Follow-Up Done? Y N
2.Last Name: First Name/MI: DOB/Age: Sex: M F
Relationship to Case: Onset Date: / / New case created? NEDSS ID:
Contact info same as case? Y N Address: Phone:
Food Handler Healthcare Group Living Day Care Pool Association Not High-Risk
If High Risk, Follow-Up Done? Y N
3.Last Name: First Name/MI: DOB/Age: Sex: M F
Relationship to Case: Onset Date: / / New case created? NEDSS ID:
Contact info same as case? Y N Address: Phone:
Food Handler Healthcare Group Living Day Care Pool Association Not High-Risk
If High Risk, Follow-Up Done? Y N
CASE EXPOSURE PERIOD HAVE PATIENT ANSWER FOLLOWING QUESTIONS FOR THE EXPOSURE PERIOD ONLY:
Date 3 Days Before Onset: / / Date of Onset: / /
HIGH-RISK OCCUPATIONS / SETTINGS (EPIDEMIOLOGICAL) Occupation: Check All That Apply: Child Student Volunteer Unemployed Retired
Y N U If yes, list any details for each:
Food Handler? Facility Name:
Healthcare Worker? Facility Name:
Group Living? Facility Name:
Day Care Association? Facility Name:
Attend or Work in a School? Facility Name:
Contact With Diapered Child? Was child ill? Y N U
Contact With Diapered Adult? Was adult ill? Y N U
If yes to any of the above, did the patient work/attend while ill? Y N U
2
Dates/Notes:
TRAVEL HISTORY (1-3 DAYS BEFORE ONSET) Travel outside of USA: Y N U Host visitors from outside of Maine: Y N U
Travel outside of Maine, but in USA: Y N U If yes, did visitors bring food to share: Y N U
Travel outside of county, but in Maine: Y N U If yes, details:
IF CASE ANSWERED YES TO ANY OF THE ABOVE QUESTIONS, THEN FILL IN BOXES BELOW. IF NO, SKIP TO NEXT SECTION.
Travel Location: From: / / To: / /
Mode of Travel: Plane Car Cruise Ship Other: Others in group ill? Y N U Other details including: *Accommodations/Dates *Sources of food/water while traveling *Other Relevant Details
Travel Location: From: / / To: / /
Mode of Travel: Plane Car Cruise Ship Other: Others in group ill? Y N U Other details including: *Accommodations/Dates *Sources of food/water while traveling *Other Relevant Details
FOOD HISTORY (1-3 DAYS BEFORE ONSET) Eat at any restaurants during exposure period? Y N U Restaurant 1
Establishment name: Date of Meal: / /
Location/Address: Time of Meal:
List foods eaten Others ill? Y N U
Restaurant 2
Establishment name: Date of Meal: / /
Location/Address: Time of Meal:
List foods eaten Others ill? Y N U
Restaurant 3
Establishment name: Date of Meal: / /
Location/Address: Time of Meal:
List foods eaten Others ill? Y N U
High Risk Food:
3
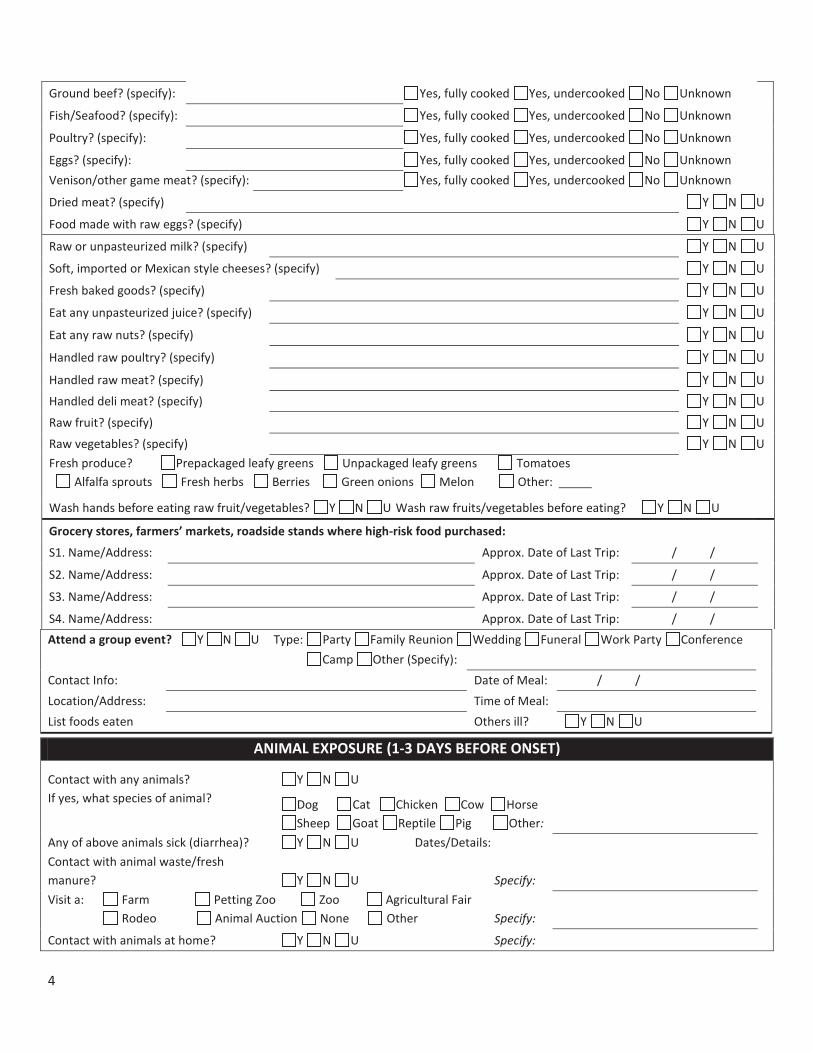
Attend a group event? Y N U Type: Party Family Reunion Wedding Funeral Work Party Conference
Camp Other (Specify): Contact Info: Date of Meal: / / Location/Address: Time of Meal: List foods eaten Others ill? Y N U
ANIMAL EXPOSURE (1-3 DAYS BEFORE ONSET)
Contact with any animals? Y N U
If yes, what species of animal? Dog Cat Chicken Cow Horse Sheep Goat Reptile Pig Other:
Any of above animals sick (diarrhea)? Y N U Dates/Details: Contact with animal waste/fresh manure? Y N U Specify:
Visit a: Farm Petting Zoo Zoo Agricultural Fair Rodeo Animal Auction None Other Specify:
Contact with animals at home? Y N U Specify:
Ground beef? (specify): Yes, fully cooked Yes, undercooked No Unknown
Fish/Seafood? (specify): Yes, fully cooked Yes, undercooked No Unknown
Poultry? (specify): Yes, fully cooked Yes, undercooked No Unknown
Eggs? (specify): Yes, fully cooked Yes, undercooked No Unknown Venison/other game meat? (specify): Yes, fully cooked Yes, undercooked No Unknown
Dried meat? (specify) Y N U
Food made with raw eggs? (specify) Y N U
Raw or unpasteurized milk? (specify) Y N U
Soft, imported or Mexican style cheeses? (specify) Y N U
Fresh baked goods? (specify) Y N U
Eat any unpasteurized juice? (specify) Y N U
Eat any raw nuts? (specify) Y N U
Handled raw poultry? (specify) Y N U
Handled raw meat? (specify) Y N U
Handled deli meat? (specify) Y N U
Raw fruit? (specify) Y N U
Raw vegetables? (specify) Y N U Fresh produce? Prepackaged leafy greens Unpackaged leafy greens Alfalfa sprouts Fresh herbs Berries Green onions Melon
Tomatoes Other:
Wash hands before eating raw fruit/vegetables? Y N U Wash raw fruits/vegetables before eating? Y N U
Grocery stores, farmers’ markets, roadside stands where high-risk food purchased:
S1. Name/Address: Approx. Date of Last Trip: / /
S2. Name/Address: Approx. Date of Last Trip: / /
S3. Name/Address: Approx. Date of Last Trip: / /
S4. Name/Address: Approx. Date of Last Trip: / /
4

Handle pet foods/treats? Y N U Specify:
New pet? Y N U Specify:
If yes, is new pet sick? Y N U
Place of Purchase? Pet Store Shelter Private Other:
Wash hands after contact with animals? Y N U If yes: Always Sometimes
5
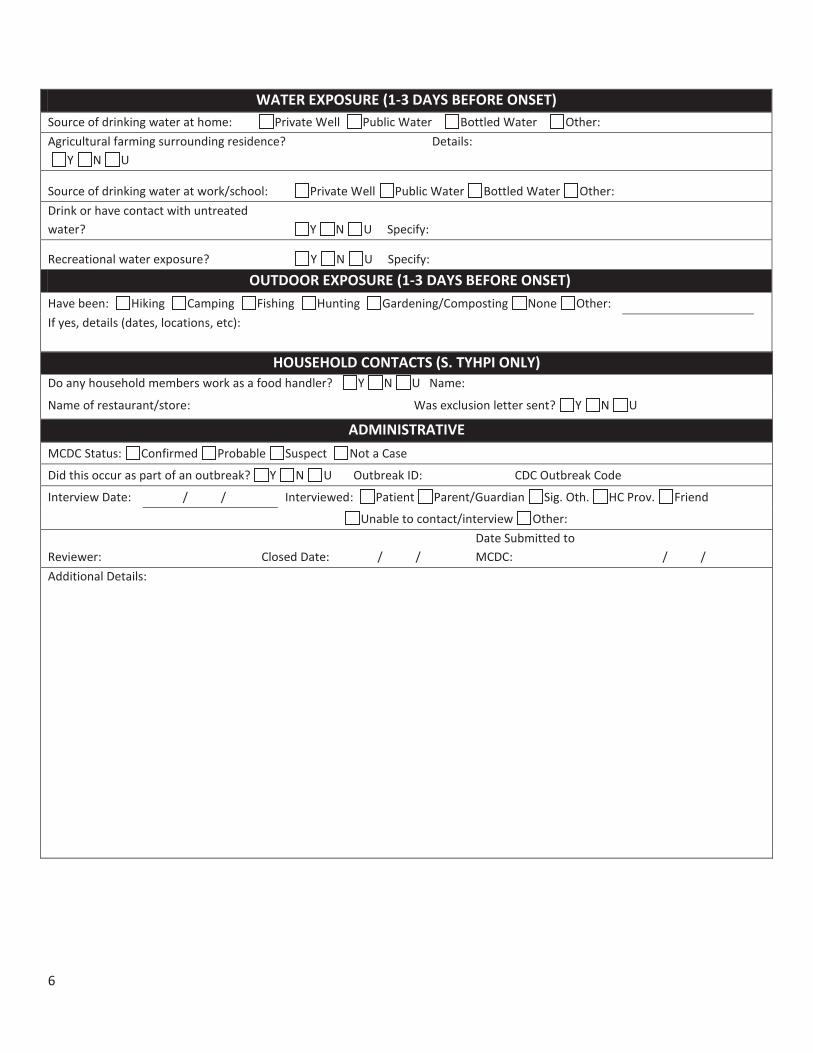
WATER EXPOSURE (1-3 DAYS BEFORE ONSET) Source of drinking water at home: Private Well Public Water Bottled Water Other: Agricultural farming surrounding residence? Y N U
Details:
Source of drinking water at work/school: Private Well Public Water Bottled Water Other:
Drink or have contact with untreated water? Y N U Specify:
Recreational water exposure? Y N U Specify:
OUTDOOR EXPOSURE (1-3 DAYS BEFORE ONSET)
Have been: Hiking Camping Fishing Hunting Gardening/Composting None Other:
If yes, details (dates, locations, etc):
HOUSEHOLD CONTACTS (S. TYHPI ONLY) Do any household members work as a food handler? Y N U Name:
Name of restaurant/store: Was exclusion letter sent? Y N U ADMINISTRATIVE
MCDC Status: Confirmed Probable Suspect Not a Case
Did this occur as part of an outbreak? Y N U Outbreak ID: CDC Outbreak Code
Interview Date: / / Interviewed: Patient Parent/Guardian Sig. Oth. HC Prov. Friend
Unable to contact/interview Other:
Reviewer: Closed Date: / / Date Submitted to MCDC: / /
Additional Details:
6

SalmonellosisFact Sheet
What is Salmonellosis?Salmonellosis is an illness caused by a group of bacteria called Salmonella. There are over 2,000 different types of Salmonella, and the bacteria can cause disease in both humans and animals. Salmonella is a major cause of diarrheal illness in the United States.
What are the signs and symptoms?Symptoms usually appear between 6 and 72hours after swallowing the bacteria. The most common signs of illness are:
DiarrheaStomach cramps Fever Headache Nausea and sometimes vomiting
Illness usually lasts 5 to 7 days, and most peoplerecover without treatment. In some people the bacteria may move from the intestines into the blood or other body sites and cause more severe illness. The elderly, infants, and people with weakened ability to fight off germs are more likely to have severe illness. Some people may not look or feel sick, but may still shed the bacteria in their stools and pass the bacteria to others.
How is it spread?Salmonella bacteria must be swallowed to cause illness. Usually this happens when someone eats food contaminated with the bacteria that has not been properly handled, prepared or cooked.
The illness may spread from person to person ifpeople do not wash their hands well with soap and water after using the toilet, changing diapers, or touching animals or reptiles. People who get the bacteria on their hands can spread it to anyone or anything they touch, especially food, which can then make others sick if the food is not cooked well enough to kill the germs.
Salmonella may be spread from person to person in places where hygiene may be poor.
What types of food are commonly linked with Salmonellosis?Salmonella is commonly found in uncooked food products from farm animals. Examples include eggs, egg products, meat, meat products, poultry, milk, and dairy products. In recent years, contaminated fruits and vegetables have been found to be the source of outbreaks. Salmonellacan be in any type of food if the bacteria get on the food at any time between processing, cooking, and eating. For example, an infected food handler may get the bacteria on the food if his or her hands are not washed well before preparing food. Cooking well done and complete processing will kill the bacteria and make food safe to eat.
What are some non-food sources of Salmonella?Salmonella have been found in the feces of both sick and apparently healthy people and animals. Many pets and farm animals, including dogs and cats, pet turtles, reptiles, chicks, poultry, cattle and swine, can carry the bacteria. Reptiles are very likely to carry Salmonella and people should always wash their hands immediately after contact with them. Animals might not show signs of being infected, but may still pass germs to people.
How is it treated?Most people who are otherwise healthy recover without treatment. In healthy people, treatment with antibiotics may cause them to shed the bacteria in their stools for a longer period of time and increase the risk of passing Salmonella to others.
Antibiotics may be needed if infection spreads from the intestines to other parts of the body. Infants, the elderly and those who may not be able to fight off the infection on their own may also need antibiotics. It is important for all people with diarrhea to drink plenty of fluids to avoid dehydration.
How can you know for sure if you have Salmonellosis?Your healthcare provider may ask you for a sample of your stool so the laboratory can test for Salmonella. It takes the lab several days to do this test.
How can Salmonellosis be prevented?You can prevent salmonellosis and other diseases by following these steps:
Always wash your hands thoroughly with soap and water
o Before eating or preparing food o After using the toileto After changing diaperso After touching pets or other
animals (especially reptiles).
Thoroughly cook all food products from animals, especially poultry and eggs.
Do not eat raw or cracked eggs, raw unpasteurized milk or any other dairy product made with raw unpasteurized milk.
Keep foods that will be eaten raw, such as fruits and vegetables, away from food products from animals. Wash your hands, utensils, and work surfaces that have been in contact with raw poultry before you make a salad.
If you are caring for a person with salmonellosis or diarrhea, wash your hands well after contact with the person’s stool. After changing diapers, be sure to clean changing area well and wash hands carefully.
Avoid letting infants or young children come into contact with reptiles, such as turtles or iguanas. If they do, make sure to wash their hands thoroughly with soap and water. Reptiles (including turtles) are not appropriate pets for small children and should not be in the same house as an infant.
If you have a child in daycare who has salmonellosis or diarrhea, let the daycare provider know so they can take extra steps to prevent spread of illness. Children with diarrhea should stay out of daycare until their diarrhea stops. The daycare provider should contact the Maine Center for Disease Control and Prevention (Maine CDC) for information on how to prevent spread of salmonellosis in the daycare.
Contact your healthcare provider whenever you experience diarrhea for more than a few days.
Are there any restrictions for people with Salmonellosis?Yes. The Maine CDC will determine which restrictions apply in a specific situation. An infected food handler, child care worker or health care worker needs to stay out of work while ill. Contact Maine CDC at 1-800-821-5821 for specific information.
Salmonellosis in MaineThe Maine CDC investigates all reported cases of salmonellosis to identify sources of public health concern and to prevent further spread of the disease.
Where can I get more information?For more information contact your healthcare provider or local health center. You can also contact the Maine Center for Disease Control and Prevention by calling 1-800-821-5821 or visiting the website www.maine.gov/idepi. The federal Centers for Disease Control and Prevention website - http://www.cdc.gov/salmonella – is another excellent source of health information.
Updated 1/21/2014Source of Information: Centers for Disease Control and Prevention http://www.cdc.gov/salmonella/ (accessed 1/21/2014)
To:
From:
Date:
Your employee, insert name of employee, has been reported to the Maine Center for Disease Control and Prevention as having a diarrheal illness. To protect the health of coworkers, customers, and attendees, Maine Center for Disease Control and Prevention policy prohibits individuals with diarrhea from engaging in the following activities: food handling or food serving, attending a childcare center or providing childcare in a center, or direct patient care. The individual named above is prohibited from performing the listed activities until the condition checked below is met. The individual or guardian has been informed of these requirements.
A. ___ The employee may return to work (daycare) on _____________, at which time she/he may resume her/his normal duties (activities).
B. ___ The employee (child) may return to work (daycare) when her/his diarrhea has stopped.Even after the diarrhea has stopped, the employee (child) may continue to carry the agent responsible for her/his symptoms. To prevent transmission, it is imperative that careful handwashing be performed after using the toilet and as otherwise appropriate during the performance of his/her duties (activities).
C. ___ Release from this restriction depends upon the completion of laboratory work* which demonstrates that the employee (child) is no longer able to pass the illness on to others. The employee (child) may return to her/his usual duties (activities) following your receipt of notification from the employee’s (child’s) physician or the Maine Center for Disease Control and Prevention.
D. ____ The employee may return to work when more than 7 calendar days have passed since the employee’s symptoms of vomiting or diarrhea has resolved.
E._____ For asymptomatic employees, the employee may return to work when more than 7 calendar days have passed since the employee’s diagnosis if no symptoms have developed.
If you have any questions please contact the Maine Center for Disease Control and Prevention at 1-800-821-5821.
*Laboratory work is 2 negative stool specimens, separated by at least 24 hours and obtained at least 48 hours after the completion of any prescribed antibiotics.
Salmonellosis
Definition:Salmonellosis is caused by a bacteria called Salmonella.
Signs and symptoms:Symptoms include diarrhea, fever and abdominal cramps. Illness lasts for 4 to 7 days.
Transmission:Salmonellosis is primarily transmitted to a person through swallowing the bacteria from a contaminated item.Illness may result from consumption of contaminated food, unpasteurized (raw) milk, water that has not been disinfected, or contact with cattle, chickens or the feces of infected people or animals.
Diagnosis:Salmonellosis is diagnosed by clinical symptoms and laboratory tests. Laboratory tests include testing of stool, blood, urine or other body fluid for the presence of salmonella bacteria.
Role of the School Nurse:Prevention
Provide education to students and staff regarding good hand washing with soap and waterPromote proper hand washing after handling animals, especially reptiles and baby chicks or ducks or avoid having reptiles and baby chicks or ducks in the classroomAvoid swallowing water when swimming or playing in lakes, ponds, streams, and any swimming pools (including backyard “kiddie” pools)Exclude symptomatic students and staff from school and school trips, especially involving swimmingProvide education on good food safety practicesPromote washing of fruits and vegetablesAvoid unpasteurized dairy and juice products
Treatment RecommendationsIf symptoms are noted, the child should be referred to their primary care provider for treatmentNon-specific supportive therapy, including hydration, is importantAntibiotics should not be used to treat salmonellosis, except for severely ill and hospitalized individuals
ExclusionsStudents should be excluded from school while symptomatic with diarrheaEducational modifications may be warranted in children with a positive diagnosisSee Maine Food Code for exclusions for staff handling food
Reporting RequirementsSalmonellosis is a reportable disease – report to Maine CDC at 1-800-821-5821
Resources:Maine CDC salmonella website (including fact sheet)http://www.maine.gov/dhhs/boh/ddc/epi/disease/salmonellosis.shtml
Maine Food Code: http://www.maine.gov/dhhs/mecdc/environmental-health/el/rules.htmDOE Child Nutrition Services http://www.maine.gov/education/sfs/index.htmlFederal CDC Salmonella website http://www.cdc.gov/salmonellaUSDA food safety website http://www.fsis.usda.gov/food_safety_education/index.aspFDA food safety website http://www.fda.gov/FoodFederal CDC raw milk website http://www.cdc.gov/foodsafety/rawmilk/raw-milk-index.htmlFederal CDC healthy swimming website http://www.cdc.gov/healthywater/swimming/
2Updated 1/21/2014
Pe Maine Department of Health & Human ServicesMaine Center for Disease Control and Prevention
PertussisInvestigation Protocol
_Oct 8, 2013__ __10/2016__Stephen Sears, MD, MPH Effective Date Review DateState Epidemiologist
Reporting Requirements
Reportable immediately by telephone on recognition or strong suspicion of disease.
Case Definition
BackgroundBordetella pertussis is the most poorly controlled bacterial vaccine-preventable disease in the U.S., with peaks in disease occurring every 3-5 years. Although routine childhood vaccination has resulted in substantial reductions in disease, the number of reported pertussis cases has been steadily increasing since the 1980s. Notable peaks in disease occurred in 2004 (25,827 cases, 27 deaths), 2010 (27,550 cases, 27 deaths), and most recently in 2012 when more than 41,000 cases and 18 deaths were reported, the largest number of cases in the U.S. since 1959. Furthermore, the epidemiologic features of pertussis have changed in recent years with an increasing burden of disease among fully-vaccinated children and adolescents.
Clinical Criteria
of the following signs or symptoms: Paroxysms of coughing; ORInspiratory whoop; ORPost-tussive vomiting; ORApnea (with or without cyanosis) (FOR INFANTS AGED <1 YEAR ONLY)
Laboratory Criteria for DiagnosisIsolation of B. pertussis from a clinical specimenPositive PCR for pertussis
Epidemiologic LinkageContact with a laboratory-confirmed case of pertussis*.
Case Classification
pMaine Center for Disease Control and Prevention
PertussisInvestigation Protocol
_Oct 8, 2013 _ _ 10/2016Effective Date _ ___ _
Review Date____ ___
Reporting Requirements
Reportable immediately by telephone on recognition or strong suspicion of disease.
pertussis is the most poorly controlled bacterial vaccine-preventable disease in the p p y pU.S., with peaks in disease occurring every 3-5 years. Although routine childhood vaccination p g y y ghas resulted in substantial reductions in disease, the number of reported pertussis cases has p pbeen steadily increasing since the 1980s. Notable peaks in disease occurred in 2004 (25,827y g p ( ,cases, 27 deaths), 2010 (27,550 cases, 27 deaths), and most recently in 2012 when more ) ( ) ythan 41,000 cases and 18 deaths were reported, the largest number of cases in the U.S.p gsince 1959. Furthermore, the epidemiologic features of pertussis have changed in recentp g p gyears with an increasing burden of disease among fully-vaccinated children and adolescents.
Case Definition
BackgroundBordetella
Clinical Criteria
Pertussis – Investigation Protocol
Probable
at least one of the following symptoms: o Paroxysms of coughing; ORo Inspiratory "whoop"; ORo Post-tussive vomiting; ORo Apnea (with or without cyanosis) (FOR INFANTS AGED <1 YEAR ONLY); AND
Absence of laboratory confirmation; ANDNo epidemiologic linkage to a laboratory-confirmed case of pertussis.
Or, FOR INFANTS AGED <1 YEAR ONLY:Acute cough illness of any duration, with at least one of the following signs or symptoms:
o Paroxysms of coughing; oro Inspiratory “whoop”; oro Post-tussive vomiting; or o Apnea (with or without cyanosis)
ANDPolymerase chain reaction (PCR) positive for pertussis
Or, FOR INFANTS AGED <1 YEAR ONLY:Acute cough illness of any duration, with at least one of the following signs or symptoms:
o Paroxysms of coughing; oro Inspiratory “whoop”; oro Post-tussive vomiting; or o Apnea (with or without cyanosis)
ANDContact with a laboratory-confirmed case of pertussis.
ConfirmedAcute cough illness of any duration, with isolation of B. pertussis from a clinical specimen.
OR
o Paroxysms of coughing; ORo Inspiratory "whoop"; ORo Post-tussive vomiting; ORo Apnea (with or without cyanosis) (FOR INFANTS AGED <1 YEAR ONLY);
ANDPolymerase chain reaction (PCR) positive for pertussis.
OR Cough i
o Paroxysms of coughing; ORo Inspiratory "whoop"; OR
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 2
Pertussis – Investigation Protocol
o Post-tussive vomiting; ORo Apnea (with or without cyanosis) (FOR INFANTS AGED <1 YEAR ONLY)
ANDContact with a laboratory-confirmed case of pertussis*.
Comment(s)*Note: An illness meeting the clinical case definition should be classified as "probable" rather than "confirmed" if it occurs in a patient who has contact with an infant aged <1 year who is
cough duration <14 days (classified as "probable" case).
Laboratory Testing Services Available
There are three types of diagnostic tests for pertussis:Culture: available at Health and Environmental Testing Laboratory (HETL) and some diagnostic laboratoriesPolymerase chain reaction (PCR): available at HETL and some diagnostic laboratoriesSerology: available in some laboratories but is not standardized and should not be relied on as a criterion for laboratory confirmation. This is not available at HETL.
The reliability of each test depends on the stage of the disease during which the specimen is collected. Please refer to the Laboratory Submission Information Sheet on pertussis available on the HETL website (attachment 1).
Purpose of Surveillance and ReportingTo ensure appropriate exclusion and antimicrobial treatment of pertussis cases, To identify close contacts, including high-risk contacts, of pertussis cases who require antimicrobial prophylaxis To identify and control pertussis outbreaks and monitor the use of antimicrobials and/or vaccine as outbreak control measuresTo compare vaccine efficacy and to distinguish vaccine failure from failure to vaccinateTo monitor disease trends and severity
Case Investigation
Initial case investigation should be initiated within one working day of receipt of reportDocument case investigation on the Pertussis Surveillance Worksheet (attachment 2) and in NEDSS.
o Complete vaccine history information for all cases. In situations where the vaccination records cannot be located, records should be cross-checked in IMMPACT 2.
o Interview the case or parent to identify all public places or events attended by the case during the infectious period. This includes, school, daycare and healthcaresettings
o Record any close contact with an enrollee or employee of a high-risk setting (i.e. a hospital, daycare center or long-term care facility) during the infectious period.
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 3
Case Investigation
Initial case investigation should be initiated within one working day of receipt of reportrrg g y p pDocument case investigation on the Pertussis Surveillance Worksheet (attachment 2) and in NEDSS.
o Complete vaccine history information for all cases. In situations where the p yvaccination records cannot be located, records should be cross-checked in IMMPACT 2.
o Interview the case or parent to identify all public places or events attended by the p y p p ycase during the infectious period. This includes, school, daycare and healthcaresettings
og
Record any close contact with an enrollee or employee of a high-risk setting (i.e. a y p y g g (hospital, daycare center or long-term care facility) during the infectious period.
Pertussis – Investigation Protocol
o Identify symptomatic household and other close contacts for whom testing, treatment, and exclusion are recommended. The case or parent should inform close contacts to notify PCP for treatment and if PCP requires testing. If a close contact is symptomatic it is more expedient to start treatment and exclusion rather than test. Testing may be implicated if individual is unsure of symptoms and does not want to be excluded for 5 days. A negative test allows individual to continue medication but resume activities.
o Identify asymptomatic household and other close contacts for whom antimicrobial prophylaxis is recommended (see Recommendations for Contacts section below)Case or parent should inform close contacts to notify PCP for prophylaxis prescription. An office visit and testing is not recommended
o Identify any high-risk cases or contacts, including: infants < 1 yr, pregnant women, healthcare workers, and others who have direct contact with infants
o Investigate < 3 month infants with the infant clinical guidance ( attachment 3)EOC should alert FE that case is infant<3 months. These cases require prompt attention.
o Contacts identified in case and outbreak investigations should be recorded on the Pertussis Contact Worksheet (attachment 4)
o Conduct a final interview for each case. The final interview should be completed no earlier than 14 days after cough onset. Investigations documenting 2-week cough duration can be closed as soon as the investigation is complete.
o Every attempt should be made to promote a single point of contact with the community for both consults and recommendations.
Recommendations for Control of Case and Contacts
Recommendations for CasesIf the case is identified < 21 days after the onset of symptoms, treatment with anappropriate antibiotic (see table below) is recommended. The symptoms of pertussis may be modified if treatment is begun early, during the catarrhal stage. If begun later in the course of illness, treatment will decrease the infectious period but may not decrease the duration of cough or severity of disease.Hospitalized cases should be placed on droplet precautions and in a separate room (if possible) until completion of at least 5 days of treatment. Some treatment regimens may last longer.Treatment and isolation are not recommended if it has been >21 days since symptom onset.
Recommendations for ContactsA case is considered to be infectious for 21 days after symptom onset or until 5 days of antibiotic treatment has been completed. In general, close contacts of sporadic cases are defined as persons who:
Had face-to-face exposure within 3 feet of a confirmed case, in the absence of respiratory protection (this includes all household contacts), orHad direct contact with oral, respiratory or nasal secretions from a confirmed case (via cough, sneeze, sharing food/eating utensils, or through the performance of medical procedures such as mouth/nose/throat exam, mouth-to-mouth resuscitation, broncoscopy or suctioning), in the absence of respiratory protection, or
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 4
Identify symptomatic household and other close contacts for whom testing, y y p gtreatment, and exclusion are recommended. The case or parent should inform pclose contacts to notify PCP for treatment and if PCP requires testing. If a closey q gcontact is symptomatic it is more expedient to start treatment and exclusion rather y p pthan test. Testing may be implicated if individual is unsure of symptoms and does g y p y pnot want to be excluded for 5 days. A negative test allows individual to continue medication but resume activities.
o Identify asymptomatic household and other close contacts for whom antimicrobialy y pprophylaxis is recommended (see Recommendations for Contacts section below)p p y ( )Case or parent should inform close contacts to notify PCP for prophylaxis p yprescription. An office visit and testing is not recommended
op p gIdentify any high-risk cases or contacts, including: infants < 1 yr, pregnant y y g g y , pwomen, healthcare workers, and others who have direct contact with infants
o Investigate < 3 month infants with the infant clinical guidance ( attachment 3)g g ( )EOC should alert FE that case is infant<3 months. These cases require prompt attention.
o Contacts identified in case and outbreak investigations should be recorded on the Pertussis Contact Worksheet (attachment 4)
o( )
Conduct a final interview for each case. The final interview should be completed nopearlier than 14 days after cough onset. Investigations documenting 2-week cough y g gduration can be closed as soon as the investigation is complete.
og p
Every attempt should be made to promote a single point of contact with the y p pcommunity for both consults and recommendations.
Pertussis – Investigation Protocol
Shared the same co
ChemoprophylaxisChemoprophylaxis with an appropriate antibiotic (see table below) is recommended for all asymptomatic close contacts during this period. If the last exposure occurred > 21 days ago, chemoprophylaxis is not recommended. Symptomatic close contacts should be referred to a healthcare provider for medical evaluation, testing and treatment according to recommendations for cases above.
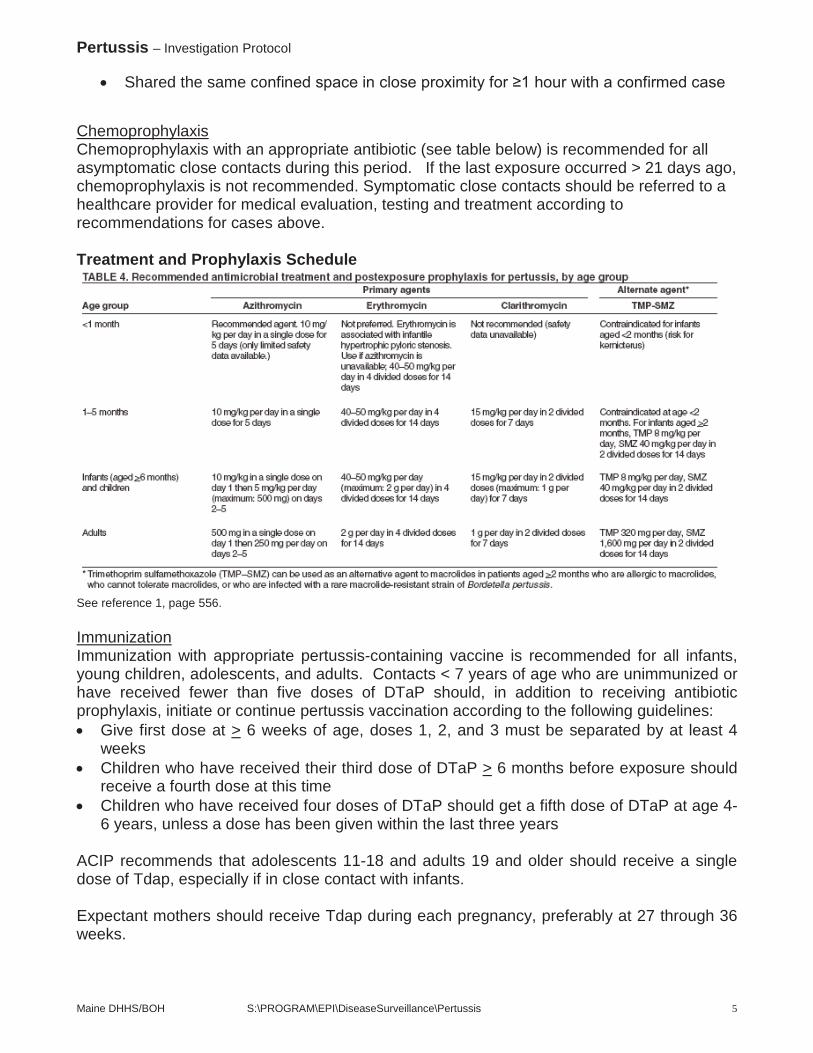
Treatment and Prophylaxis Schedule
See reference 1, page 556.
Immunization Immunization with appropriate pertussis-containing vaccine is recommended for all infants, young children, adolescents, and adults. Contacts < 7 years of age who are unimmunized or have received fewer than five doses of DTaP should, in addition to receiving antibiotic prophylaxis, initiate or continue pertussis vaccination according to the following guidelines:
Give first dose at > 6 weeks of age, doses 1, 2, and 3 must be separated by at least 4 weeksChildren who have received their third dose of DTaP > 6 months before exposure should receive a fourth dose at this timeChildren who have received four doses of DTaP should get a fifth dose of DTaP at age 4-6 years, unless a dose has been given within the last three years
ACIP recommends that adolescents 11-18 and adults 19 and older should receive a single dose of Tdap, especially if in close contact with infants.
Expectant mothers should receive Tdap during each pregnancy, preferably at 27 through 36 weeks.
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 5
Pertussis – Investigation Protocol
For a complete set of immunization recommendations for infants, children, adolescents, and adults, refer to http://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/index.htmland to the Vaccine Information Sheets at: http://www.cdc.gov/vaccines/hcp/vis/index.html
Recommendations for OutbreaksCreate a facility outbreak in NEDSS if the outbreak is located in a county with a rate less than the state pertussis rate. Vaccine Preventable Diseaseepidemiologist will send data updates routinely by county.
Outbreak definitions vary according to the outbreak setting:School and Childcare Settings – Case by Case basis. Discuss with VPD epidemiologist. Hospital, Institutions, and Clinics – One case of healthcare or facility transmission
Mass chemoprophylaxis and vaccination are not generally recommended as outbreak control measures. Please refer to the Guidelines for the Control of Pertussis Outbreaks at http://www.cdc.gov/vaccines/pubs/pertussis-guide/guide.htm and the Managing Special Situations section below for setting-specific outbreak control recommendations.
Exclusions
CasesIf the case is still within the infectious period (<21 days after symptom onset), s/he should be excluded from work, school, daycare and social activity for 5 days after initiation of appropriate antibiotic therapy. If the case is untreated, it is recommended that s/he be excluded from work, school, daycare and social activity for 21 days after the onset of symptoms. If it has been > 21 days since symptom onset, the case is no longer infectious, and no exclusions are recommended.
Symptomatic contactsExclusion recommendations are the same as for cases, regardless of disease history,immunization status, or laboratory test result.
Asymptomatic contactsNo exclusion is generally recommended. If an asymptomatic contact becomes symptomatic s/he should be treated as a case and excluded for the first 5 days of treatment.
Managing Special Situations: Schools, Daycares, Healthcare Settings, Institutions
Schools and DaycaresSymptomatic students and staff should be treated and excluded according to recommendations above.
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 6
Pertussis – Investigation Protocol
Asymptomatic students and staff identified as close contacts should not receive chemoprophylaxis. Daycare staff and students will be evaluated on a case by case basisInvestigator should notify the school nurse and provide a template letter when the first pertussis case is identified in a school.Prophylaxis is not recommended for classroom exposures unless the contact is at high riskProphylaxis in daycare classes will be evaluated on a case by case basisParents and employees should be notified of possible pertussis exposures with a letter. (S:\DiseaseSurveillance\Pertussis\Letters ) which can be modified to the specific situation. If the investigation identifies a large number of symptomatic contacts for whom testing is recommended, consider notifying local area physicians and laboratories and providing them with a copy of the school/daycare letter to prepare them for an increase in parent calls and anticipate the need to order additional pertussis test kits. A copy of the letter should be provided to the Epi-on-call and AHOC.Other control measures, e.g. vaccine clinics, closure, will be determined on a case by case basis
Healthcare Settings and InstitutionsHealthcare professionals should observe standard precautions and wear respiratory protection when examining a patient with a cough illness suspected or confirmed to be pertussisSymptomatic healthcare workers should be treated and excluded according to recommendations for cases. Patient and staff contacts of healthcare workers or patients diagnosed with pertussis should be identified by the facility and receive chemoprophylaxis.Exposed, unprotected healthcare workers should receive chemoprophylaxis promptly Healthcare workers should be up-to-date on Tdap vaccine Active surveillance should be conducted by the healthcare institution for 42 days after the onset of the last known case
References:
See the following references for clinical information including identification, description of infectious agent, occurrence, reservoir, mode of transmission, incubation period, period of communicability, susceptibility and further clinical information.
1. American Academy of Pediatrics, Pertussis. In: Pickering LK, Baker CJ, Kimberlin, DW, Long SS, eds. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, Illinois: American Academy of Pediatrics, 2012
2. American Public Health Association, Pertussis. In: Heymann D, ed., Control of Communicable Diseases Manual, 19th Edition, Washington, DC: American Public Health Association, 2008.
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 7
Pertussis – Investigation Protocol
3. Centers for Disease Control and Prevention, Pertussis. In: Atkinson W, Hamborsky J., McIntyre L and Wolfe C, eds. Epidemiology and Prevention of Vaccine-Preventable Diseases (Pink Book), 12th Edition, Atlanta, Georgia: Centers for Disease Control and Prevention, 2011.
4. Centers for Disease Control and Prevention. Guidelines for the Control of Pertussis Outbreaks, National Immunization Program, 2000. http://www.cdc.gov/pertussis/outbreaks/guide/index.html
5. CDC Pregnancy and whooping cough http://www.cdc.gov/vaccines/adults/rec-vac/pregnant/whooping-cough/get-vaccinated.html
6. CDC Pertussis. www.cdc.gov/pertussis
Attachments
1. Laboratory Submission Information Sheet – Pertussis, http://www.maine.gov/dhhs/etl/micro/submitting_samples.htm
2. Pertussis Surveillance Worksheet, Appendix 11-2; Manual for the Surveillance of Vaccine-Preventable Diseases (5th Edition, 2011), Chapter 10: Pertussis.
3. Instructions for Using the Pertussis Surveillance Worksheet, Appendix 11-1; Manual for the Surveillance of Vaccine-Preventable Diseases (4th Edition, 2008), Chapter 10:Pertussis.
4. Pertussis Contact Worksheet5. Pertussis Fact Sheet6. Pertussis in Infants- Guidance for Clinicians,
http://www.maine.gov/dhhs/mecdc/infectious-disease/epi/vaccine/documents/Pertussis-Infants-Guidance-Clinicians.docx
Maine DHHS/BOH S:\PROGRAM\EPI\DiseaseSurveillance\Pertussis 8
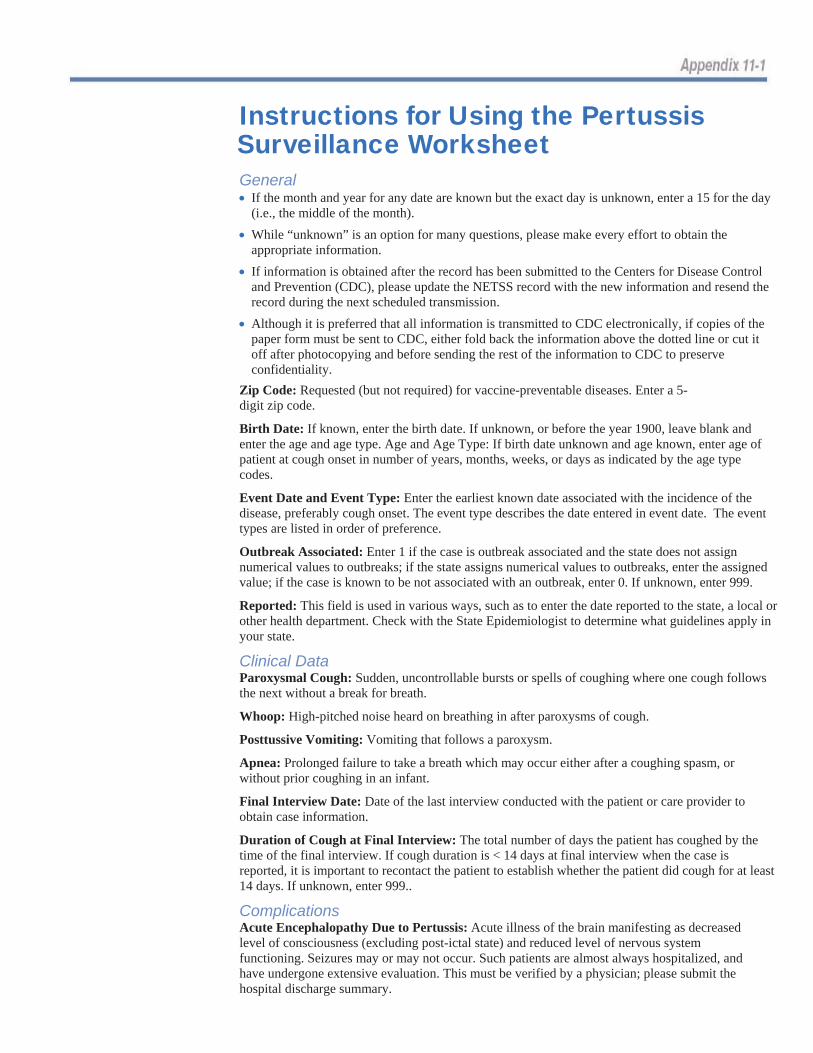
Instructions for Using the Pertussis Surveillance Worksheet General If the month and year for any date are known but the exact day is unknown, enter a 15 for the day (i.e., the middle of the month).
While “unknown” is an option for many questions, please make every effort to obtain the appropriate information. If information is obtained after the record has been submitted to the Centers for Disease Control and Prevention (CDC), please update the NETSS record with the new information and resend the record during the next scheduled transmission. Although it is preferred that all information is transmitted to CDC electronically, if copies of the paper form must be sent to CDC, either fold back the information above the dotted line or cut it off after photocopying and before sending the rest of the information to CDC to preserve confidentiality.
Zip Code: Requested (but not required) for vaccine-preventable diseases. Enter a 5-digit zip code.
Birth Date: If known, enter the birth date. If unknown, or before the year 1900, leave blank and enter the age and age type. Age and Age Type: If birth date unknown and age known, enter age of patient at cough onset in number of years, months, weeks, or days as indicated by the age type codes.
Event Date and Event Type: Enter the earliest known date associated with the incidence of the disease, preferably cough onset. The event type describes the date entered in event date. The event types are listed in order of preference.
Outbreak Associated: Enter 1 if the case is outbreak associated and the state does not assign numerical values to outbreaks; if the state assigns numerical values to outbreaks, enter the assigned value; if the case is known to be not associated with an outbreak, enter 0. If unknown, enter 999.
Reported: This field is used in various ways, such as to enter the date reported to the state, a local or other health department. Check with the State Epidemiologist to determine what guidelines apply in your state.
Clinical Data Paroxysmal Cough: Sudden, uncontrollable bursts or spells of coughing where one cough follows the next without a break for breath.
Whoop: High-pitched noise heard on breathing in after paroxysms of cough.
Posttussive Vomiting: Vomiting that follows a paroxysm.
Apnea: Prolonged failure to take a breath which may occur either after a coughing spasm, or without prior coughing in an infant.
Final Interview Date: Date of the last interview conducted with the patient or care provider to obtain case information.
Duration of Cough at Final Interview: The total number of days the patient has coughed by the time of the final interview. If cough duration is < 14 days at final interview when the case is reported, it is important to recontact the patient to establish whether the patient did cough for at least 14 days. If unknown, enter 999..
Complications Acute Encephalopathy Due to Pertussis: Acute illness of the brain manifesting as decreased level of consciousness (excluding post-ictal state) and reduced level of nervous system functioning. Seizures may or may not occur. Such patients are almost always hospitalized, and have undergone extensive evaluation. This must be verified by a physician; please submit the hospital discharge summary.
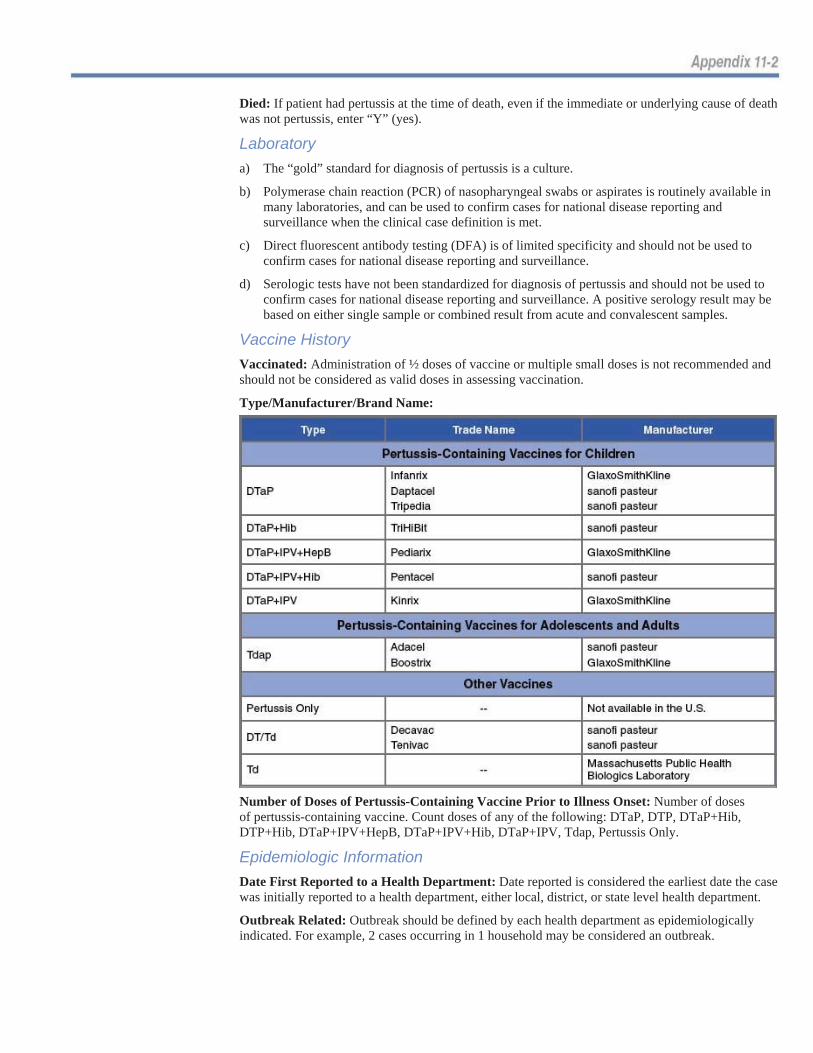
Died: If patient had pertussis at the time of death, even if the immediate or underlying cause of death was not pertussis, enter “Y” (yes).
Laboratorya) The “gold” standard for diagnosis of pertussis is a culture.
b) Polymerase chain reaction (PCR) of nasopharyngeal swabs or aspirates is routinely available in many laboratories, and can be used to confirm cases for national disease reporting and surveillance when the clinical case definition is met.
c) Direct fluorescent antibody testing (DFA) is of limited specificity and should not be used to confirm cases for national disease reporting and surveillance.
d) Serologic tests have not been standardized for diagnosis of pertussis and should not be used to confirm cases for national disease reporting and surveillance. A positive serology result may be based on either single sample or combined result from acute and convalescent samples.
Vaccine History Vaccinated: Administration of ½ doses of vaccine or multiple small doses is not recommended and should not be considered as valid doses in assessing vaccination.
Type/Manufacturer/Brand Name:
Number of Doses of Pertussis-Containing Vaccine Prior to Illness Onset: Number of doses of pertussis-containing vaccine. Count doses of any of the following: DTaP, DTP, DTaP+Hib, DTP+Hib, DTaP+IPV+HepB, DTaP+IPV+Hib, DTaP+IPV, Tdap, Pertussis Only.
Epidemiologic Information Date First Reported to a Health Department: Date reported is considered the earliest date the case was initially reported to a health department, either local, district, or state level health department.
Outbreak Related: Outbreak should be defined by each health department as epidemiologically indicated. For example, 2 cases occurring in 1 household may be considered an outbreak.

Epi-Linked: A patient who has had close contact with a culture-confirmed case, and cough onset in the period from 30 days before to 30 days after cough onset in the culture-confirmed case, where the timing of the contact was compatible with the incubation period of pertussis (6–20 days).
If Patient is <12 Months Old: Provide age of mother at infant’s birth, and weight of infant in pounds and ounces or kilograms and grams.
Setting (Outside Household) of Further Documented Spread from This Case: Indicate setting outside household in which secondary transmission of pertussis from the case occurred.
Number of Contacts in Any Setting Recommended Antibiotics: Enter the number of contacts for whom chemoprophylaxis was recommended.
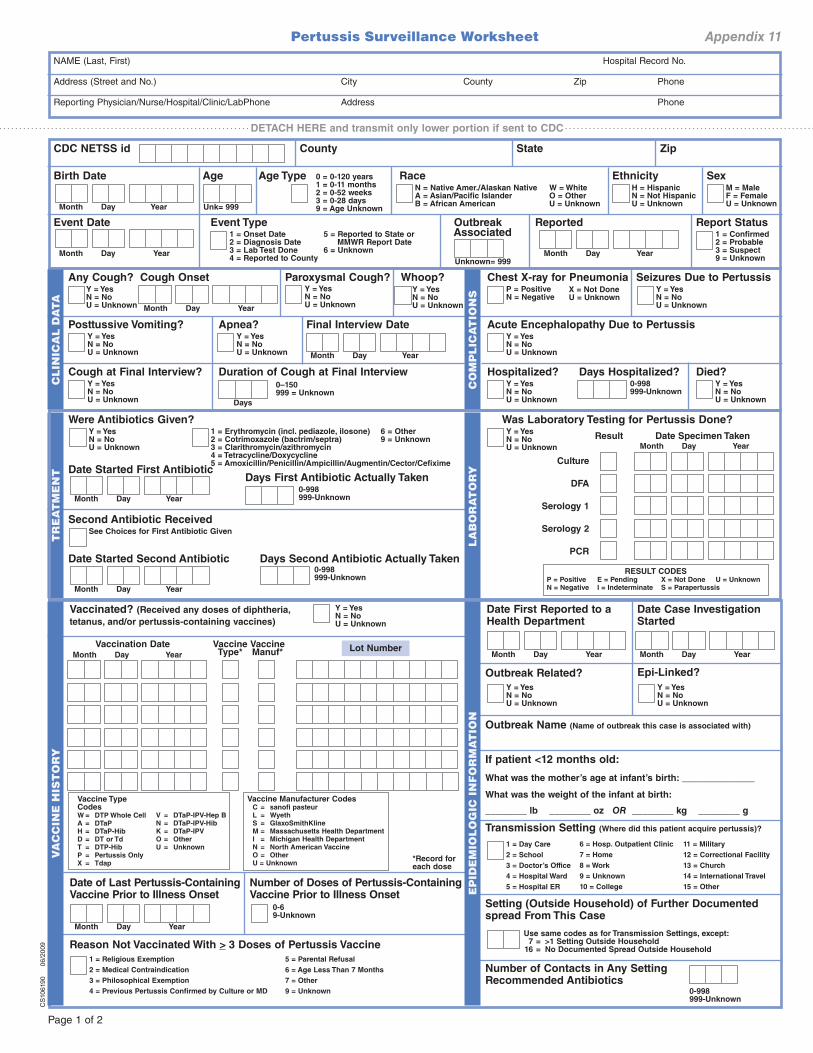
Pertussis Surveillance Worksheet Appendix 11
NAME (Last, First) Hospital Record No.
Address (Street and No.) City County Zip Phone
Reporting Physician/Nurse/Hospital/Clinic/LabPhone Address Phone
DETACH HERE and transmit only lower portion if sent to CDC
CDC NETSS id County State Zip
Birth Date
Month Day Year
Age
Unk= 999
Age Type 0 = 0-120 years1 = 0-11 months2 = 0-52 weeks3 = 0-28 days9 = Age Unknown
Race
N = Native Amer./Alaskan Native A = Asian/Pacific Islander B = African American
W = WhiteO = OtherU = Unknown
Ethnicity H = HispanicN = Not HispanicU = Unknown
SexM = MaleF = FemaleU = Unknown
Event Date
Month Day Year
Event Type1 = Onset Date2 = Diagnosis Date3 = Lab Test Done4 = Reported to County
5 = Reported to State or MMWR Report Date
6 = Unknown
Outbreak Associated
Unknown= 999
Reported
Month Day Year
Report Status1 = Confirmed2 = Probable3 = Suspect9 = Unknown
Y = YesN = NoU = Unknown
V
CS
1061
90
0
6/20
09
Vaccinated? (Received any doses of diphtheria,
tetanus, and/or pertussis-containing vaccines)
______________
________ ________ ________ ________
AC
LIN
ICA
L D
AT
Any Cough?Y = YesN = NoU = Unknown
Cough Onset
Month Day Year
Paroxysmal Cough? Y = YesN = NoU = Unknown
Whoop? Y = YesN = NoU = Unknown
Posttussive Vomiting? Y = YesN = NoU = Unknown
Apnea? Y = YesN = NoU = Unknown
Final Interview Date
Month Day Year
Cough at Final Interview? Y = YesN = NoU = Unknown
Duration of Cough at Final Interview
Days
0–150999 = Unknown
TM
EN
TT
RE
A
Were Antibiotics Given?Y = YesN = NoU = Unknown
1 = Erythromycin (incl. pediazole, ilosone)2 = Cotrimoxazole (bactrim/septra)3 = Clarithromycin/azithromycin4 = Tetracycline/Doxycycline5 = Amoxicillin/Penicillin/Ampicillin/Augmentin/Cector/Cefixime
6 = Other9 = Unknown
Date Started First Antibiotic
Month Day Year
Days First Antibiotic Actually Taken0-998999-Unknown
See Choices for First Antibiotic Given
Second Antibiotic Received
Date Started Second Antibiotic
Month Day Year
Days Second Antibiotic Actually Taken0-998999-Unknown
YV
AC
CIN
E H
IST
OR
Month Day Year
Vaccination Date VaccineType*
Vaccine Type CodesW = DTP Whole Cell
A = DTaP
H = DTaP-Hib
D = DT or Td
T = DTP-Hib
P = Pertussis Only
X = Tdap
V = DTaP-IPV-Hep B
N = DTaP-IPV-Hib
K = DTaP-IPV
O = Other
U = Unknown
accine Manuf*
Vaccine Manufacturer Codes C = sanofi pasteur
L = Wyeth
S = GlaxoSmithKline
M = Massachusetts Health Department
I = Michigan Health Department
N = North American Vaccine
O = Other
U = Unknown
Lot Number
*Record for each dose
Date of Last Pertussis-ContainingVaccine Prior to Illness Onset
Month Day Year
Number of Doses of Pertussis-ContainingVaccine Prior to Illness Onset
0-69-Unknown
5 = Parental Refusal
6 = Age Less Than 7 Months
7 = Other
9 = Unknown
Reason Not Vaccinated With _ > 3 Doses of Pertussis Vaccine
1 = Religious Exemption
2 = Medical Contraindication
3 = Philosophical Exemption
4 = Previous Pertussis Confirmed by Culture or MD
TIO
NS
CO
MP
LIC
A
Chest X-ray for Pneumonia P = PositiveN = Negative
X = Not DoneU = Unknown
Seizures Due to Pertussis Y = YesN = NoU = Unknown
Acute Encephalopathy Due to PertussisY = YesN = NoU = Unknown
Hospitalized? Y = YesN = NoU = Unknown
Days Hospitalized? 0-998999-Unknown
Died? Y = YesN = NoU = Unknown
YT
OR
LA
BO
RA
Was Laboratory Testing for Pertussis Done?Y = YesN = NoU = Unknown
Result
RESULT CODESP = Positive E = Pending X = Not Done U = Unknown
N = Negative I = Indeterminate S = Parapertussis
Month Day Year
Date Specimen Taken
Culture
DFA
Serology 1
Serology 2
PCR
EP
IDE
MIO
LO
GIC
IN
FO
RM
AT
ION
Date First Reported to a Health Department
Month Day Year
Date Case Investigation Started
Month Day Year
Outbreak Related?
Y = YesN = NoU = Unknown
Epi-Linked?
Y = YesN = NoU = Unknown
Outbreak Name (Name of outbreak this case is associated with)
If patient <12 months old:
What was the mother’s age at infant’s birth:
What was the weight of the infant at birth:
lb oz OR kg g
Transmission Setting (Where did this patient acquire pertussis)?
1 = Day Care
2 = School
3 = Doctor’s Office
4 = Hospital Ward
5 = Hospital ER
6 = Hosp. Outpatient Clinic
7 = Home
8 = Work
9 = Unknown
10 = College
11 = Military
12 = Correctional Facility
13 = Church
14 = International Travel
15 = Other
Use same codes as for Transmission Settings, except: 7 = >1 Setting Outside Household 16 = No Documented Spread Outside Household
Setting (Outside Household) of Further Documented spread From This Case
Number of Contacts in Any Setting Recommended Antibiotics
0-998999-Unknown
Page 1 of 2
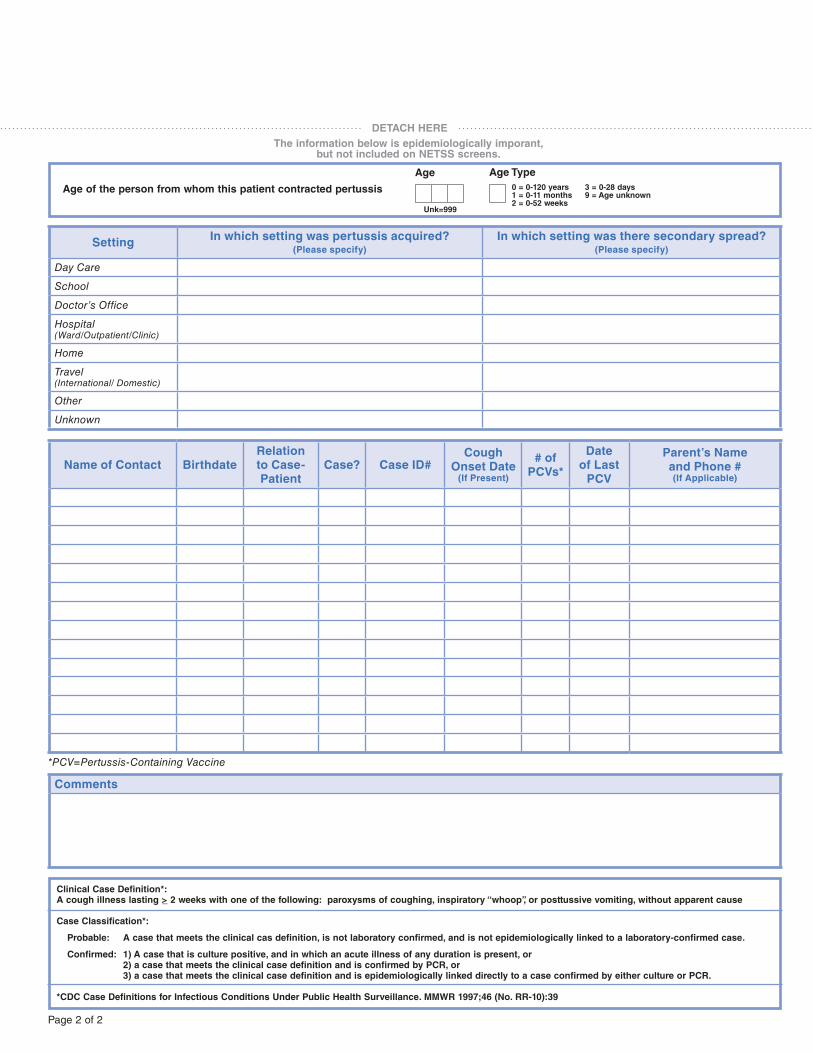
DETACH HERE
The information below is epidemiologically imporant, but not included on NETSS screens.
Age of the person from whom this patient contracted pertussis
Age
Unk=999
Age Type
0 = 0-120 years 1 = 0-11 months 2 = 0-52 weeks
3 = 0-28 days9 = Age unknown
SettingIn which setting was pertussis acquired?
(Please specify)
In which setting was there secondary spread?(Please specify)
Day Care
School
Doctor’s Office
Hospital (Ward/Outpatient/Clinic)
Home
Travel (International/ Domestic)
Other
Unknown
Name of Contact Birthdate
Relation
to Case-
Patient
Case? Case ID#Cough
Onset Date(If Present)
# of
PCVs*
Date
of Last
PCV
Parent’s Name
and Phone #
(If Applicable)
*PCV=Pertussis-Containing Vaccine
Comments
Clinical Case Definition*:
A cough illness lasting >_ 2 weeks with one of the following: paroxysms of coughing, inspiratory “whoop”, or posttussive vomiting, without apparent cause
Case Classification*:
Probable: A case that meets the clinical cas definition, is not laboratory confirmed, and is not epidemiologically linked to a laboratory-confirmed case.
Confirmed: 1) A case that is culture positive, and in which an acute illness of any duration is present, or
2) a case that meets the clinical case definition and is confirmed by PCR, or
3) a case that meets the clinical case definition and is epidemiologically linked directly to a case confirmed by either culture or PCR.
*CDC Case Definitions for Infectious Conditions Under Public Health Surveillance. MMWR 1997;46 (No. RR-10):39
Page 2 of 2
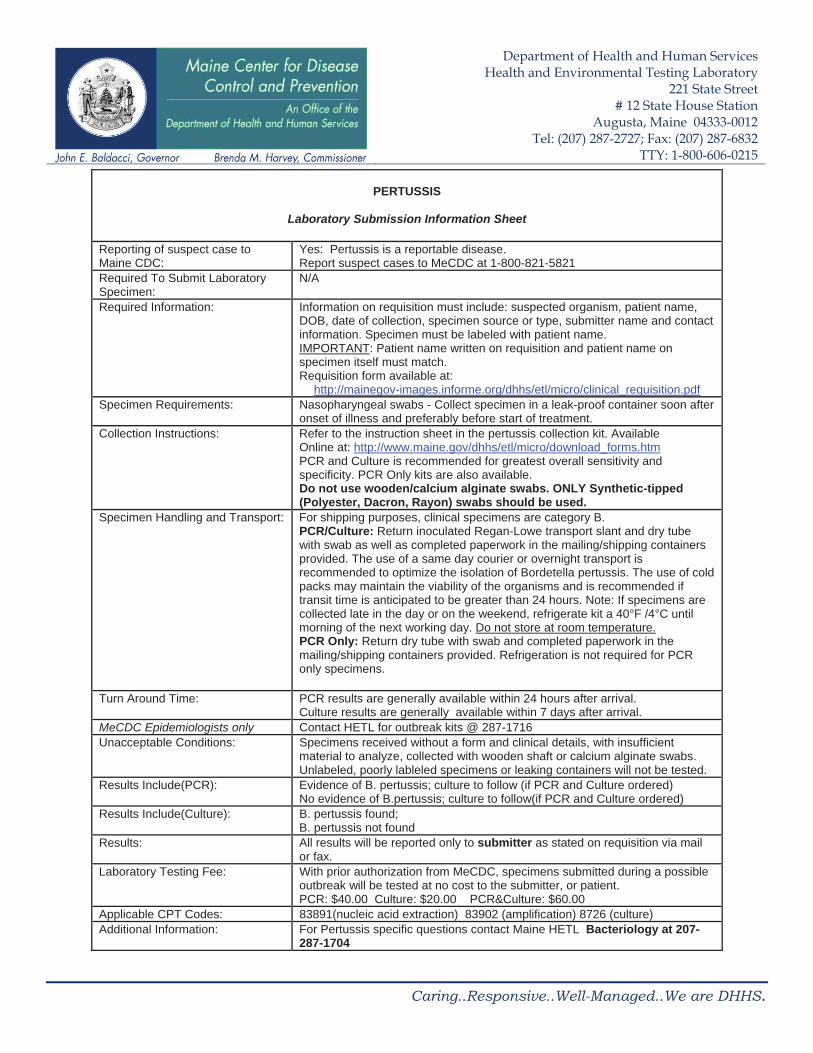
Department of Health and Human Services Health and Environmental Testing Laboratory
221 State Street # 12 State House Station
Augusta, Maine 04333-0012 Tel: (207) 287-2727; Fax: (207) 287-6832
TTY: 1-800-606-0215
PERTUSSIS
Laboratory Submission Information Sheet
Reporting of suspect case to Maine CDC:
Yes: Pertussis is a reportable disease. Report suspect cases to MeCDC at 1-800-821-5821
Required To Submit Laboratory Specimen:
N/A
Required Information: Information on requisition must include: suspected organism, patient name, DOB, date of collection, specimen source or type, submitter name and contact information. Specimen must be labeled with patient name. IMPORTANT: Patient name written on requisition and patient name on specimen itself must match. Requisition form available at:
http://mainegov-images.informe.org/dhhs/etl/micro/clinical_requisition.pdfSpecimen Requirements: Nasopharyngeal swabs - Collect specimen in a leak-proof container soon after
onset of illness and preferably before start of treatment.Collection Instructions: Refer to the instruction sheet in the pertussis collection kit. Available
Online at: http://www.maine.gov/dhhs/etl/micro/download_forms.htmPCR and Culture is recommended for greatest overall sensitivity and specificity. PCR Only kits are also available. Do not use wooden/calcium alginate swabs. ONLY Synthetic-tipped (Polyester, Dacron, Rayon) swabs should be used.
Specimen Handling and Transport: For shipping purposes, clinical specimens are category B. PCR/Culture: Return inoculated Regan-Lowe transport slant and dry tube with swab as well as completed paperwork in the mailing/shipping containers provided. The use of a same day courier or overnight transport is recommended to optimize the isolation of Bordetella pertussis. The use of cold packs may maintain the viability of the organisms and is recommended if transit time is anticipated to be greater than 24 hours. Note: If specimens are collected late in the day or on the weekend, refrigerate kit a 40°F /4°C until morning of the next working day. Do not store at room temperature.PCR Only: Return dry tube with swab and completed paperwork in the mailing/shipping containers provided. Refrigeration is not required for PCR only specimens.
Turn Around Time: PCR results are generally available within 24 hours after arrival. Culture results are generally available within 7 days after arrival.
MeCDC Epidemiologists only Contact HETL for outbreak kits @ 287-1716 Unacceptable Conditions: Specimens received without a form and clinical details, with insufficient
material to analyze, collected with wooden shaft or calcium alginate swabs. Unlabeled, poorly lableled specimens or leaking containers will not be tested.
Results Include(PCR): Evidence of B. pertussis; culture to follow (if PCR and Culture ordered) No evidence of B.pertussis; culture to follow(if PCR and Culture ordered)
Results Include(Culture): B. pertussis found; B. pertussis not found
Results: All results will be reported only to submitter as stated on requisition via mail or fax.
Laboratory Testing Fee: With prior authorization from MeCDC, specimens submitted during a possible outbreak will be tested at no cost to the submitter, or patient. PCR: $40.00 Culture: $20.00 PCR&Culture: $60.00
Applicable CPT Codes: 83891(nucleic acid extraction) 83902 (amplification) 8726 (culture) Additional Information: For Pertussis specific questions contact Maine HETL Bacteriology at 207-
287-1704
Caring..Responsive..Well-Managed..We are DHHS.
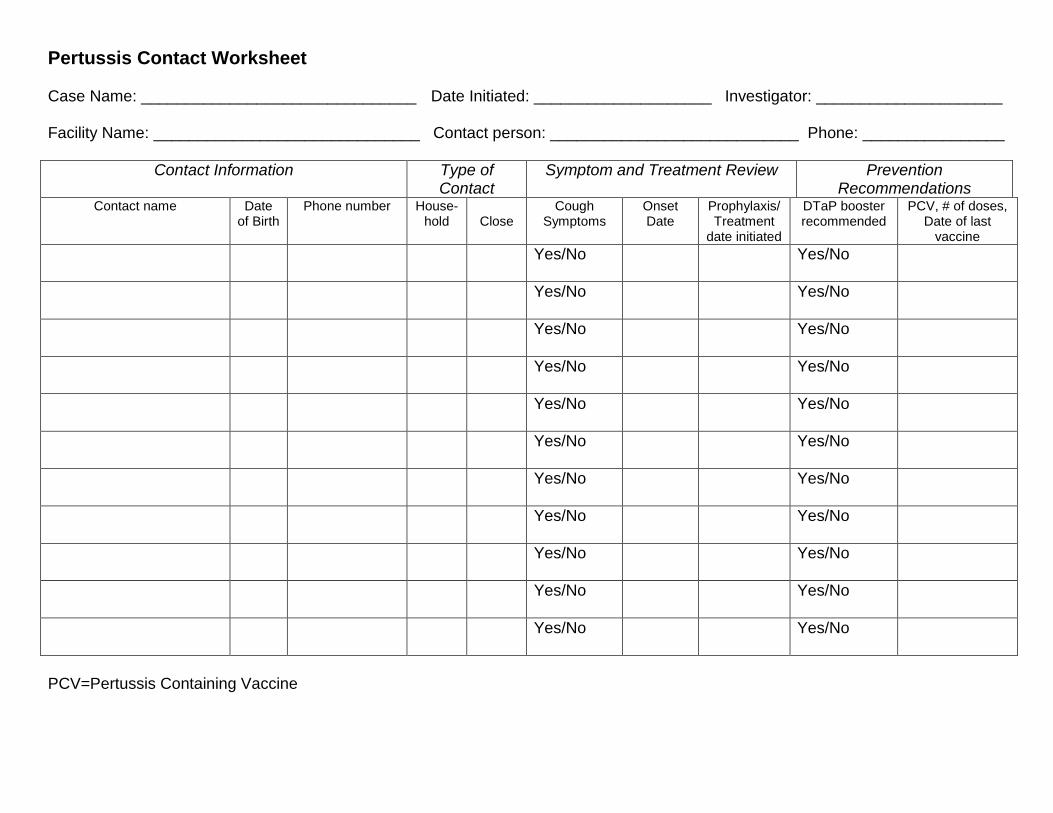
Pertussis Contact Worksheet Case Name: _______________________________ Date Initiated: ____________________ Investigator: _____________________ Facility Name: ______________________________ Contact person: ____________________________ Phone: ________________
Contact Information Type of Contact
Symptom and Treatment Review Prevention Recommendations
Contact name
Date of Birth
Phone number House- hold
Close
Cough Symptoms
Onset Date
Prophylaxis/ Treatment
date initiated
DTaP booster recommended
PCV, # of doses, Date of last
vaccine
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
PCV=Pertussis Containing Vaccine
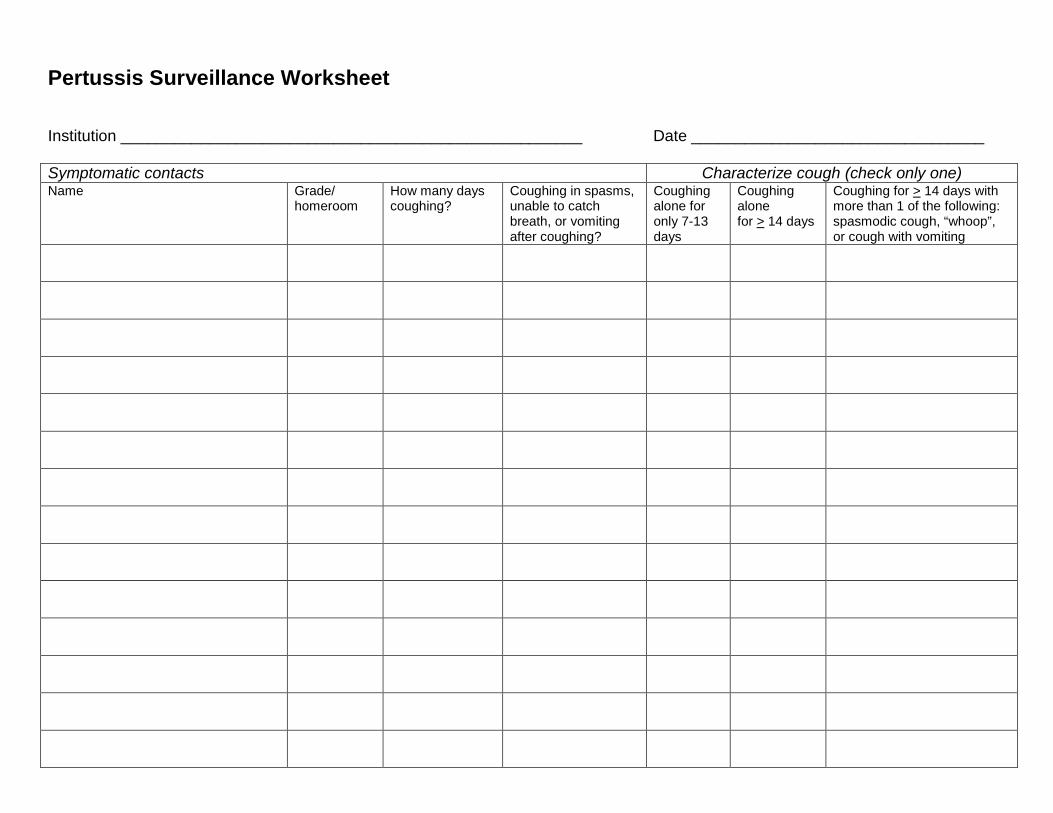
Pertussis Surveillance Worksheet Institution ____________________________________________________ Date _________________________________ Symptomatic contacts Characterize cough (check only one) Name Grade/
homeroom How many days coughing?
Coughing in spasms, unable to catch breath, or vomiting after coughing?
Coughing alone for only 7-13 days
Coughing alone for > 14 days
Coughing for > 14 days with more than 1 of the following: spasmodic cough, “whoop”, or cough with vomiting
PertussisFact Sheet
What is pertussis?Pertussis, or whooping cough, is caused by bacteria called Bordetella pertussis. Pertussis can be very serious, especially in infants. It mainly affects the breathing.
What are the signs of pertussis?The first signs of pertussis are similar to a cold (sneezing, runny nose, low-grade fever, and a cough). These signs start 5 to 21 days after exposure. After one or two weeks of illness, the cough gets worse.
The cough occurs in sudden, uncontrollable bursts where one cough follows the next without a break for breath. Many children will make a high-pitched whooping sound when breathing in after a coughing episode. Whooping is less common in infants and adults.After a coughing spell, the person may throw up.Between coughing spells, the person seems well, but the illness is exhausting over time.Over time, coughing spells become less frequent, but may continue for several weeks or months.
How do you catch pertussis?A person has to breathe in droplets from an infected person to get sick. Pertussis is spread from person to person through the air. For example, a person may catch pertussis by standing close (less than 3 feet away) to an infected person who is coughing or sneezing.
When and for how long can a person spread pertussis? Pertussis is most likely to spread to others early in the illness. Persons with pertussis can no longer spread the disease once they have completed 5days of treatment with antibiotics. However, persons with pertussis who do not take antibiotics can spread the disease during the first 21 days they are sick.
What are the complications?Severe pertussis is more likely in infants than in older children or adults. The most common complication of pertussis is pneumonia. Seizures, swelling of the brain and death are rare but possible.
Who gets pertussis?People of all ages can get pertussis, even people who have been vaccinated or have had pertussis infection in the past. It is most common in school-aged children and teenagers, but cases in adults continue to occur. Older children and adults usually have less severe illness, but they can still spread the disease to infants and young children.
Is there any treatment?Pertussis can be treated with antibiotics.Treatment should be started early to prevent the spread to others and can lessen the symptoms of illness. Cough may continue for many weeks after treatment especially if treatment isn’t started until late in the illness. Pertussis bacteria die off naturally after three weeks of coughing. Antibiotics are not recommended if a person has already been coughing for 21 days or more.
Why did my healthcare provider tell me or my child to stay home for 5 days?You can still spread pertussis to others until you take 5 days of antibiotics. Disease can spread quickly in schools or the workplace.
What will happen if I do not want to take the antibiotics? If you do not take the antibiotics, you will need to stay away from others for 21 days after you start to become sick. This includes staying home from daycare, school, work or events.
Is there a lab test for pertussis? Yes. To test for pertussis, your healthcare provider may insert a swab (like a long q-tip) into your nose. The lab will test the material on the swab to see if they can find the bacteria that causes pertussis.
Is there a vaccine for pertussis? Yes, there are vaccines for infants, children, preteens, teens, and adults. The childhood vaccine is called Dtap, and the Pertussis booster for adolescents and adults is called Tdap.
People who catch pertussis after being vaccinated have milder illness and are much less likely to be hospitalized or die from the disease.
Vaccines prevent 200,000 cases of pertussiseach year in the US. Talk to your healthcare provider about getting vaccinated against pertussis.
How can pertussis be prevented? Vaccinate all children on time. Speak with your provider to see if you should get a booster vaccine. This is the best way to prevent pertussis.
Other ways to prevent pertussis are to:
Avoid close contact with others who are sick or coughing Wash your hands oftenStay at home if you are illCover your cough with a tissue or cough into your sleeveUse routine cleaners and disinfectants toremove these bacteria from surfaces or objects.See your healthcare provider if you have signs of pertussis or have been in close contact with someone who has pertussis.
Where can I get more information?For more information contact your healthcare provider or local health center. Infectious Disease Epidemiology website: http://www.maine.gov/dhhs/mecdc/infectious-disease/epi/index.shtmlThe federal Centers for Disease Control and Prevention website - http://www.cdc.gov – is another excellent source of health information.
Created on 8/10/07. Updated 9/10/2013.Sources of Information: Centers for Disease Control and Prevention (accessed 9/10/2013)
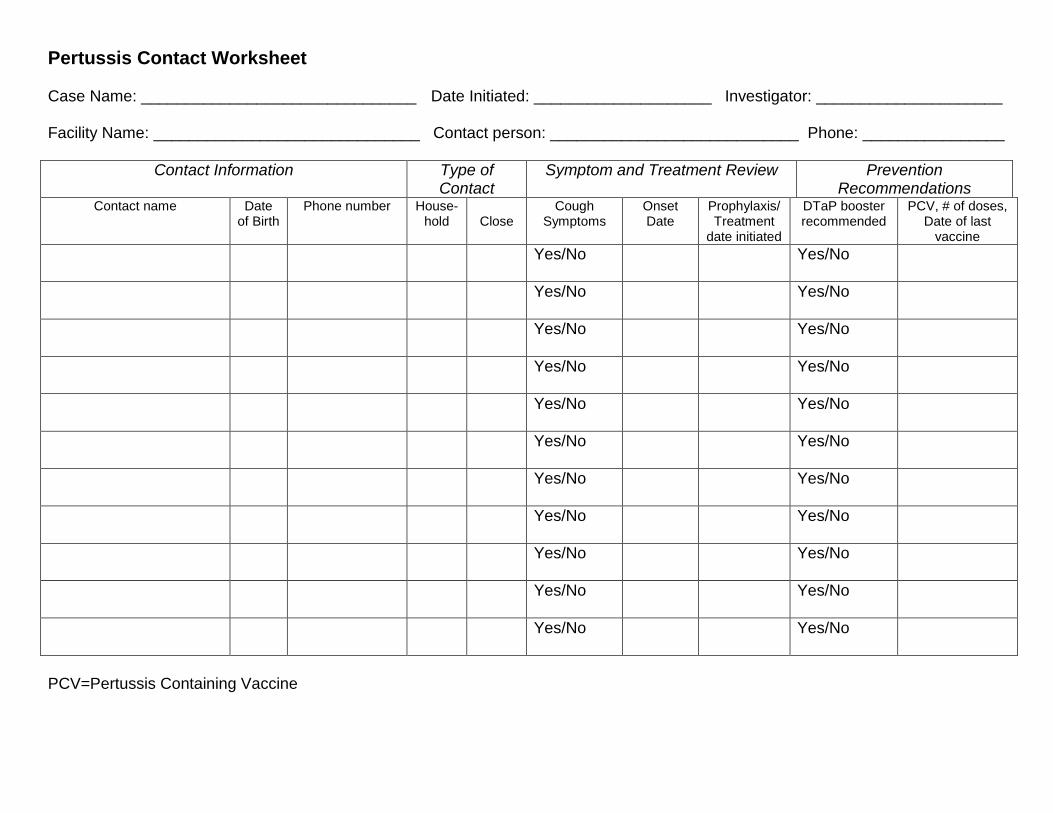
Pertussis Contact Worksheet Case Name: _______________________________ Date Initiated: ____________________ Investigator: _____________________ Facility Name: ______________________________ Contact person: ____________________________ Phone: ________________
Contact Information Type of Contact
Symptom and Treatment Review Prevention Recommendations
Contact name
Date of Birth
Phone number House- hold
Close
Cough Symptoms
Onset Date
Prophylaxis/ Treatment
date initiated
DTaP booster recommended
PCV, # of doses, Date of last
vaccine
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
Yes/No Yes/No
PCV=Pertussis Containing Vaccine
Pertussis Surveillance Worksheet Institution ____________________________________________________ Date _________________________________ Symptomatic contacts Characterize cough (check only one) Name Grade/
homeroom How many days coughing?
Coughing in spasms, unable to catch breath, or vomiting after coughing?
Coughing alone for only 7-13 days
Coughing alone for > 14 days
Coughing for > 14 days with more than 1 of the following: spasmodic cough, “whoop”, or cough with vomiting