
Course: Nuchal Cystic Lesions - SonoWorld 2014/Nuchal... · Course: Nuchal Cystic Lesions Faculty:...
41
Course: Nuchal Cystic Lesions Faculty: Tu T.T. Le, MD, Philippe Jeanty, MD, PhD
Transcript of Course: Nuchal Cystic Lesions - SonoWorld 2014/Nuchal... · Course: Nuchal Cystic Lesions Faculty:...

Course: Nuchal Cystic Lesions
Faculty: Tu T.T. Le, MD, Philippe Jeanty, MD, PhD
Course objectives: After completing this course, the participant should be able:
•••• to recognize the abnormal cysts of neck and face
•••• to discuss differential diagnoses of these conditions
•••• to discuss with the parents the prognosis of these conditions
Target audience: Physicians, sonographers and others who perform and/or interpret OB ultrasound.
Instructions: This Internet-based tutorial requires that you read through the text and related images in their entirety. You may read it from your browser or from hard copy after printing it out. In addition, it is suggested that you refer to references in the bibliography to reinforce the information presented by the author. Following completion of the tutorial, click on "Take the Quiz". After scoring a passing score of 70% or higher you will be taken to a secure payment page where you will have the opportunity to pay the CME fee and receive your certificate.
System requirements: In order to complete this program you must have a computer with a recent version of Chrome or Internet Explorer, and a printer, which is configured to print from the browser.
Volume Pricing: This course is $25.00 for 1 credit. You will receive your CME credits and certificate for this course. Four credit hours for $60.00. ($15.00 per credit). You will receive your credits and certificate for this course plus 2 vouchers which you can use immediately or at a future date. Eight credit hours are $80.00. ($10.00 per credit). You will receive your credit and certificate for this course plus 6 vouchers which you can use immediately or at a future date.
Customer Assistance: For any questions or problems concerning this program, or for problems related to the printing of the certificate, please contact IAME at 802-824-4433 or [email protected]
Estimated time for completion of tutorial: approximately 120 minutes
Date of review and release: March, 2012
Expiration Date: March, 2015
Disclosure: In compliance with the Essentials and Standards of the ACCME, the author of this CME tutorial is required to disclose any significant financial or other relationships they may have with the manufacturer(s) of any commercial product(s) or provider(s) of any commercial service(s) discussed in this program.
Drs. Le and Jeanty have indicated that they have no such relationships to disclose.
Nuchal cystic lesions: Although slightly arbitrary, it is convenient to divide the cystic lesions of the neck in 3 categories:
1.Mostly cystic masses: •••• Lymphangioma
•••• Cystic hygroma
•••• Meningocele
•••• Epidermal scalp cyst
2.Mixed cystic and solid: •••• Hemangiolymphangioma
3.Mostly solid lesions with included cystic components: •••• Hemangioma
•••• Teratoma
•••• Neuroblastoma
1. Mostly cystic cyst:
1.1. Lymphangioma: Adapted and updated from Adrian Clavelli,MD.
1.1.1. Definition: Lymphangiomas are a group of various abnormalities whose etiology is developmental defects of the lymphatic vessels.
Lymphangiomas are made up of lymphatic vessels and are, fundamentally, endothelial cells limiting spaces and supporting connective tissue. There are three groups:
• simple lymphangioma, formed by lymphatic capillaries;
• cavernous lymphangioma, formed by bigger lymphatic vessels with a fibrous adventitia;
• cystic lymphangioma, commonly called cystic hygroma
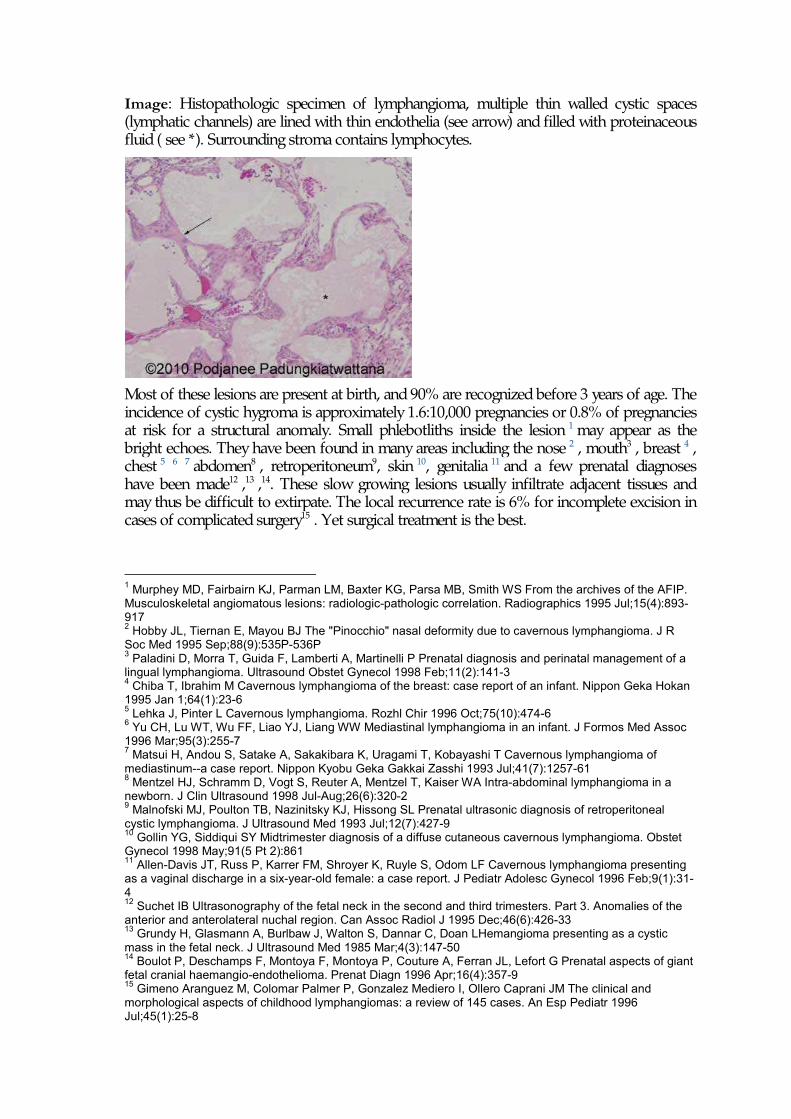
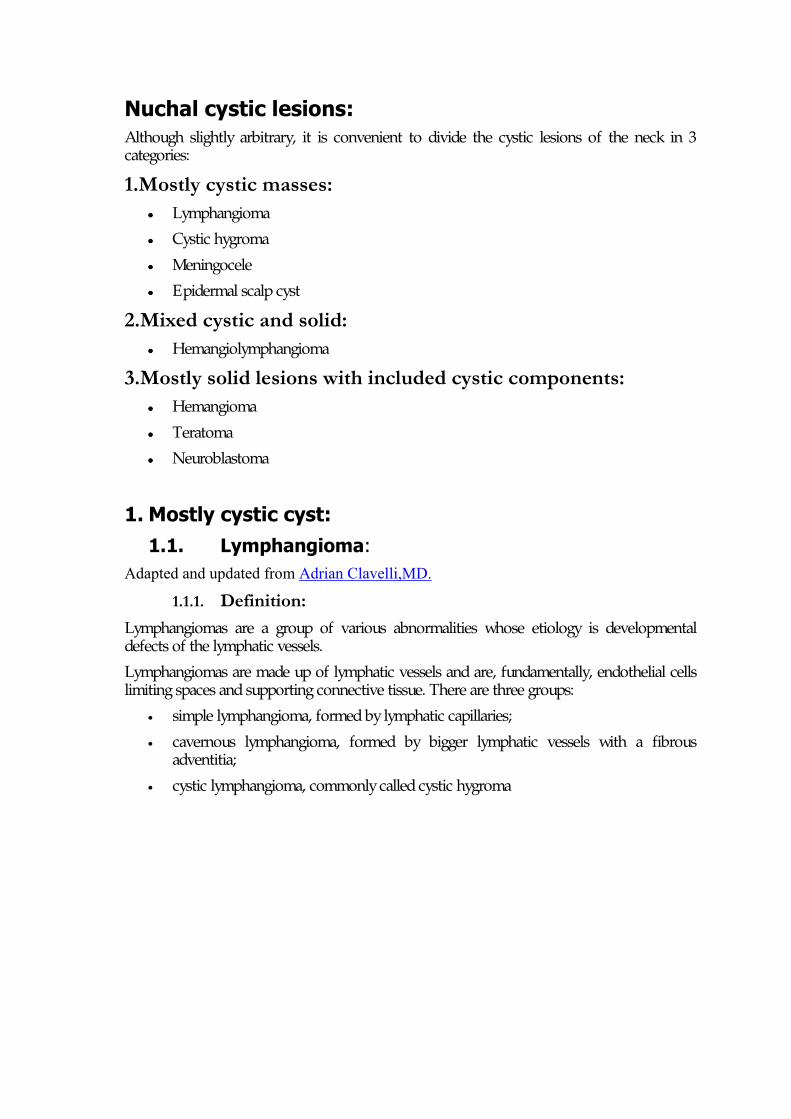
Image: Histopathologic specimen of lymphangioma, multiple thin walled cystic spaces (lymphatic channels) are lined with thin endothelia (see arrow) and filled with proteinaceous fluid ( see *). Surrounding stroma contains lymphocytes.
Most of these lesions are present at birth, and 90% are recognized before 3 years of age. The incidence of cystic hygroma is approximately 1.6:10,000 pregnancies or 0.8% of pregnancies at risk for a structural anomaly. Small phlebotliths inside the lesion 1 may appear as the bright echoes. They have been found in many areas including the nose 2 , mouth3 , breast 4 , chest 5 6 7 abdomen8 , retroperitoneum9, skin 10, genitalia 11 and a few prenatal diagnoses have been made12 ,13 ,14. These slow growing lesions usually infiltrate adjacent tissues and may thus be difficult to extirpate. The local recurrence rate is 6% for incomplete excision in cases of complicated surgery15 . Yet surgical treatment is the best.
1 Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, Smith WS From the archives of the AFIP. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics 1995 Jul;15(4):893-917 2 Hobby JL, Tiernan E, Mayou BJ The "Pinocchio" nasal deformity due to cavernous lymphangioma. J R Soc Med 1995 Sep;88(9):535P-536P 3 Paladini D, Morra T, Guida F, Lamberti A, Martinelli P Prenatal diagnosis and perinatal management of a lingual lymphangioma. Ultrasound Obstet Gynecol 1998 Feb;11(2):141-3 4 Chiba T, Ibrahim M Cavernous lymphangioma of the breast: case report of an infant. Nippon Geka Hokan 1995 Jan 1;64(1):23-6 5 Lehka J, Pinter L Cavernous lymphangioma. Rozhl Chir 1996 Oct;75(10):474-6 6 Yu CH, Lu WT, Wu FF, Liao YJ, Liang WW Mediastinal lymphangioma in an infant. J Formos Med Assoc 1996 Mar;95(3):255-7 7 Matsui H, Andou S, Satake A, Sakakibara K, Uragami T, Kobayashi T Cavernous lymphangioma of mediastinum--a case report. Nippon Kyobu Geka Gakkai Zasshi 1993 Jul;41(7):1257-61 8 Mentzel HJ, Schramm D, Vogt S, Reuter A, Mentzel T, Kaiser WA Intra-abdominal lymphangioma in a newborn. J Clin Ultrasound 1998 Jul-Aug;26(6):320-2 9 Malnofski MJ, Poulton TB, Nazinitsky KJ, Hissong SL Prenatal ultrasonic diagnosis of retroperitoneal cystic lymphangioma. J Ultrasound Med 1993 Jul;12(7):427-9 10 Gollin YG, Siddiqui SY Midtrimester diagnosis of a diffuse cutaneous cavernous lymphangioma. Obstet Gynecol 1998 May;91(5 Pt 2):861 11 Allen-Davis JT, Russ P, Karrer FM, Shroyer K, Ruyle S, Odom LF Cavernous lymphangioma presenting as a vaginal discharge in a six-year-old female: a case report. J Pediatr Adolesc Gynecol 1996 Feb;9(1):31-4 12 Suchet IB Ultrasonography of the fetal neck in the second and third trimesters. Part 3. Anomalies of the anterior and anterolateral nuchal region. Can Assoc Radiol J 1995 Dec;46(6):426-33 13 Grundy H, Glasmann A, Burlbaw J, Walton S, Dannar C, Doan LHemangioma presenting as a cystic mass in the fetal neck. J Ultrasound Med 1985 Mar;4(3):147-50 14 Boulot P, Deschamps F, Montoya F, Montoya P, Couture A, Ferran JL, Lefort G Prenatal aspects of giant fetal cranial haemangio-endothelioma. Prenat Diagn 1996 Apr;16(4):357-9 15 Gimeno Aranguez M, Colomar Palmer P, Gonzalez Mediero I, Ollero Caprani JM The clinical and morphological aspects of childhood lymphangiomas: a review of 145 cases. An Esp Pediatr 1996 Jul;45(1):25-8
1.1.2. Ultrasound findings The ultrasound appearance is that of an irregular mass varying from hypo- to hyperechoic. They can have thin- or thick-walled septa, be unicameral, or multilocular and cystic. They can also contain scattered low-level echoes, a solid component, or fluid/fluid levels. The borders of lymphangiomas are indistinct. Some may have intrathoracic extension.
On color Doppler, there is little or no flow detected within the mass.
Any large neck masses may compress the esophagus (causing polyhydramnios prenatally) and the airways (causing respiratory distress at birth). Lymphangiomas can also be part of Klippel-Trenaunay syndrome.
1.1.3. Prognosis: When the whole lesion can be extracted, the prognosis is good. Complete resection is, however, not always possible, as the masses tend to be infiltrative. The lesion does not need to be totally removed if dissection is impossible, since it is not malignant. Large cysts can be sclerosed.
Of course, if the chromosomes are abnormal, the prognosis is poor.
1.1.4. Case report: This is a case of cervical lymphangioma diagnosed at 25 weeks. The lymphangioma grew progressively during the gestation. The patient opted to continue the pregnancy. The baby was delivered at 38 weeks (cesarean section). The baby was hospitalized immediately in neonatology unit and intubated. He died after few hours from respiratory insufficiency.
1.1.4.1. Case 1:
Cervical view at 33 weeks showing cystic lymphangioma
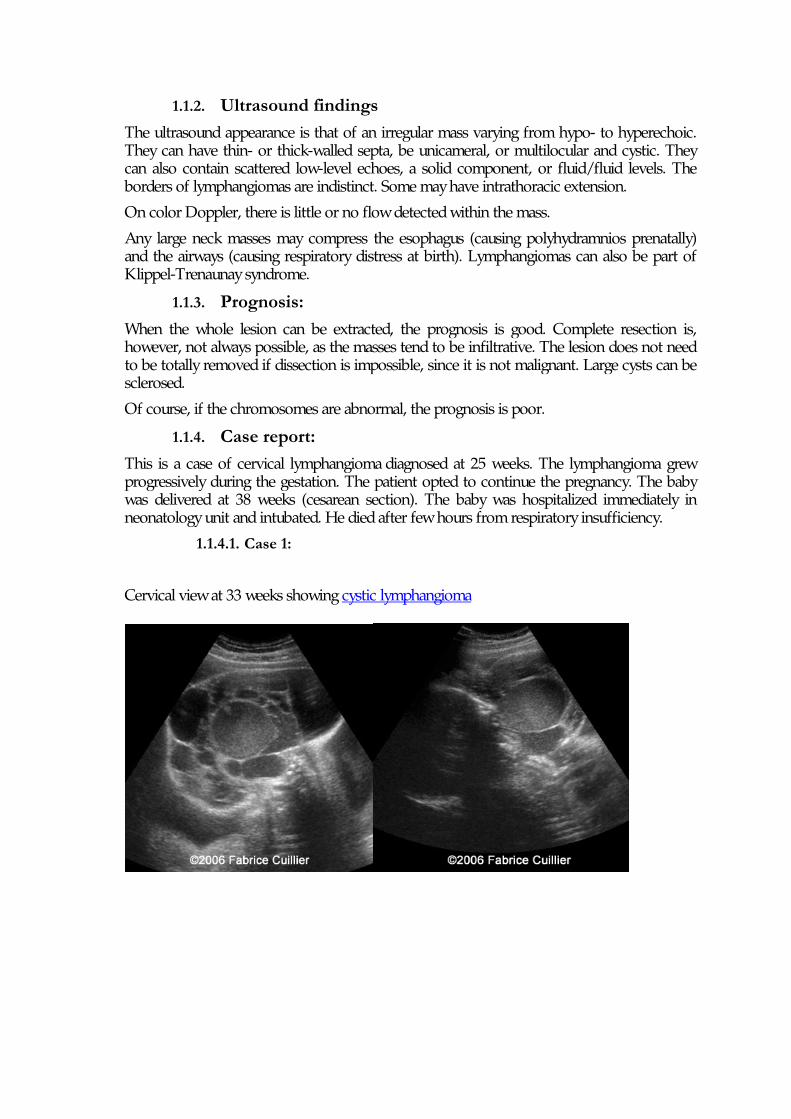
3D view at 33 week
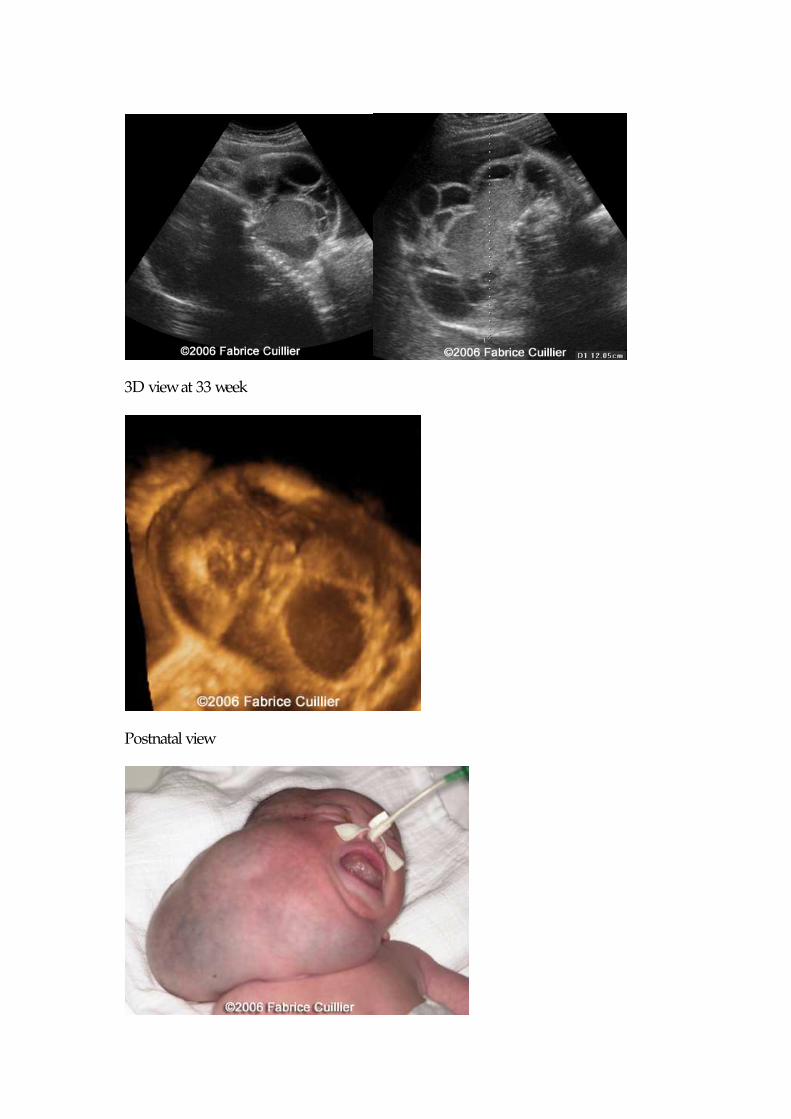
Postnatal view
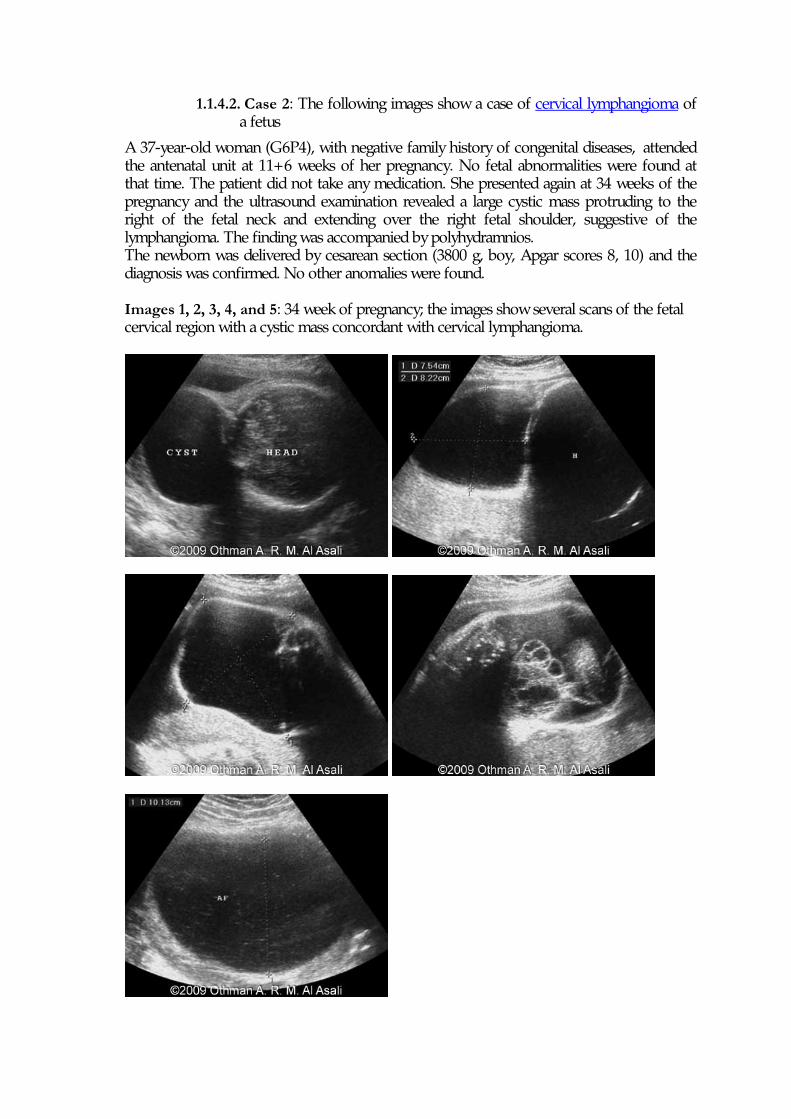
1.1.4.2. Case 2: The following images show a case of cervical lymphangioma of a fetus
A 37-year-old woman (G6P4), with negative family history of congenital diseases, attended the antenatal unit at 11+6 weeks of her pregnancy. No fetal abnormalities were found at that time. The patient did not take any medication. She presented again at 34 weeks of the pregnancy and the ultrasound examination revealed a large cystic mass protruding to the right of the fetal neck and extending over the right fetal shoulder, suggestive of the lymphangioma. The finding was accompanied by polyhydramnios. The newborn was delivered by cesarean section (3800 g, boy, Apgar scores 8, 10) and the diagnosis was confirmed. No other anomalies were found. Images 1, 2, 3, 4, and 5: 34 week of pregnancy; the images show several scans of the fetal cervical region with a cystic mass concordant with cervical lymphangioma.
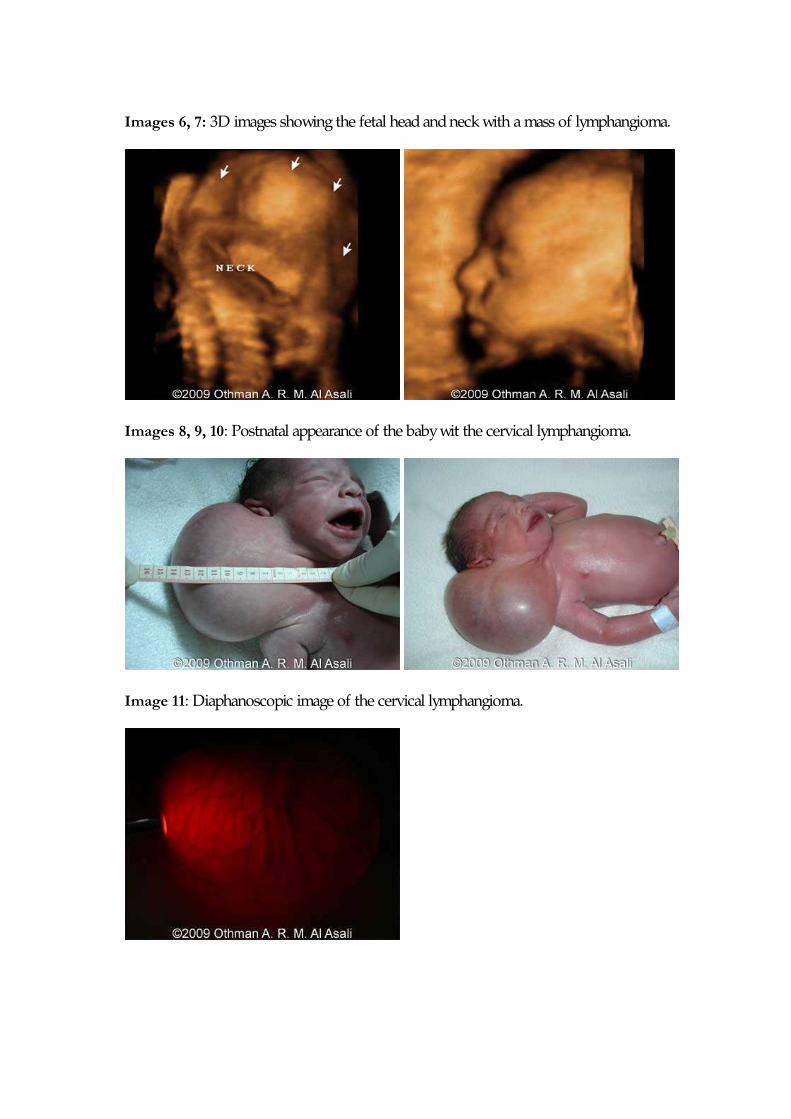
Images 6, 7: 3D images showing the fetal head and neck with a mass of lymphangioma.
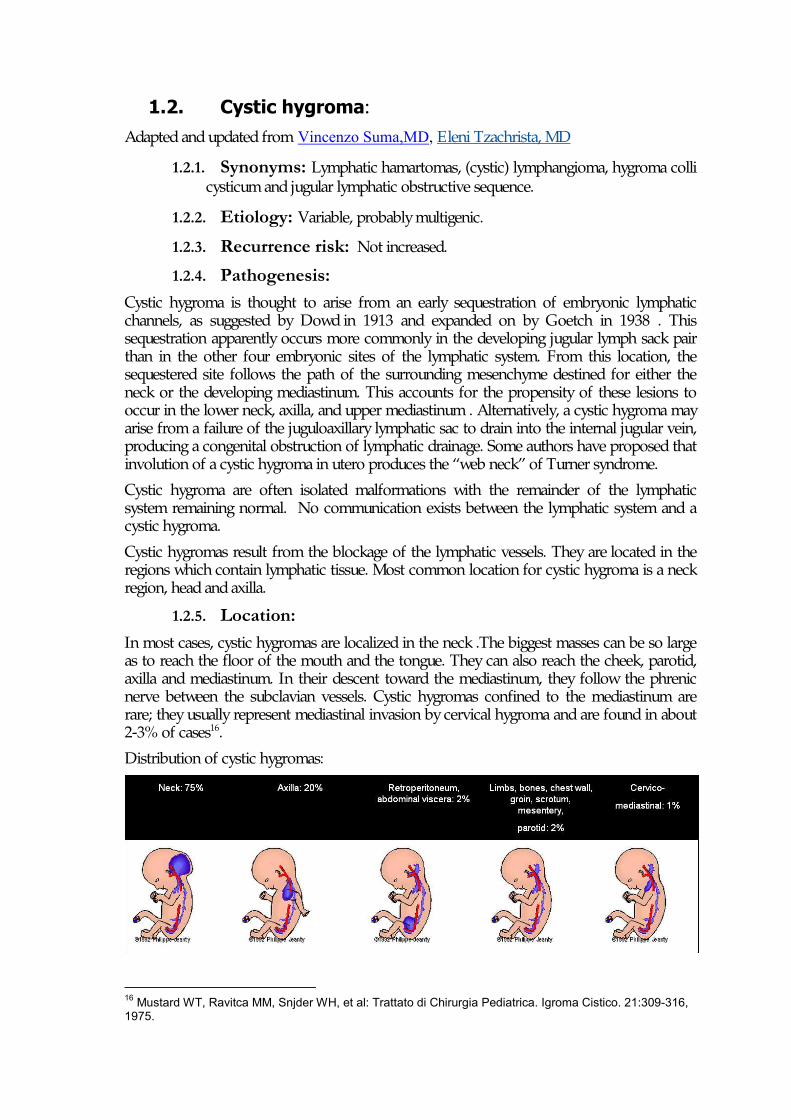
Images 8, 9, 10: Postnatal appearance of the baby wit the cervical lymphangioma.
Image 11: Diaphanoscopic image of the cervical lymphangioma.
1.2. Cystic hygroma: Adapted and updated from Vincenzo Suma,MD, Eleni Tzachrista, MD
1.2.1. Synonyms: Lymphatic hamartomas, (cystic) lymphangioma, hygroma colli cysticum and jugular lymphatic obstructive sequence.
1.2.2. Etiology: Variable, probably multigenic. 1.2.3. Recurrence risk: Not increased.
1.2.4. Pathogenesis: Cystic hygroma is thought to arise from an early sequestration of embryonic lymphatic channels, as suggested by Dowd in 1913 and expanded on by Goetch in 1938 . This sequestration apparently occurs more commonly in the developing jugular lymph sack pair than in the other four embryonic sites of the lymphatic system. From this location, the sequestered site follows the path of the surrounding mesenchyme destined for either the neck or the developing mediastinum. This accounts for the propensity of these lesions to occur in the lower neck, axilla, and upper mediastinum . Alternatively, a cystic hygroma may arise from a failure of the juguloaxillary lymphatic sac to drain into the internal jugular vein, producing a congenital obstruction of lymphatic drainage. Some authors have proposed that involution of a cystic hygroma in utero produces the “web neck” of Turner syndrome.
Cystic hygroma are often isolated malformations with the remainder of the lymphatic system remaining normal. No communication exists between the lymphatic system and a cystic hygroma.
Cystic hygromas result from the blockage of the lymphatic vessels. They are located in the regions which contain lymphatic tissue. Most common location for cystic hygroma is a neck region, head and axilla.
1.2.5. Location: In most cases, cystic hygromas are localized in the neck .The biggest masses can be so large as to reach the floor of the mouth and the tongue. They can also reach the cheek, parotid, axilla and mediastinum. In their descent toward the mediastinum, they follow the phrenic nerve between the subclavian vessels. Cystic hygromas confined to the mediastinum are rare; they usually represent mediastinal invasion by cervical hygroma and are found in about 2-3% of cases16.
Distribution of cystic hygromas:
16 Mustard WT, Ravitca MM, Snjder WH, et al: Trattato di Chirurgia Pediatrica. Igroma Cistico. 21:309-316, 1975.
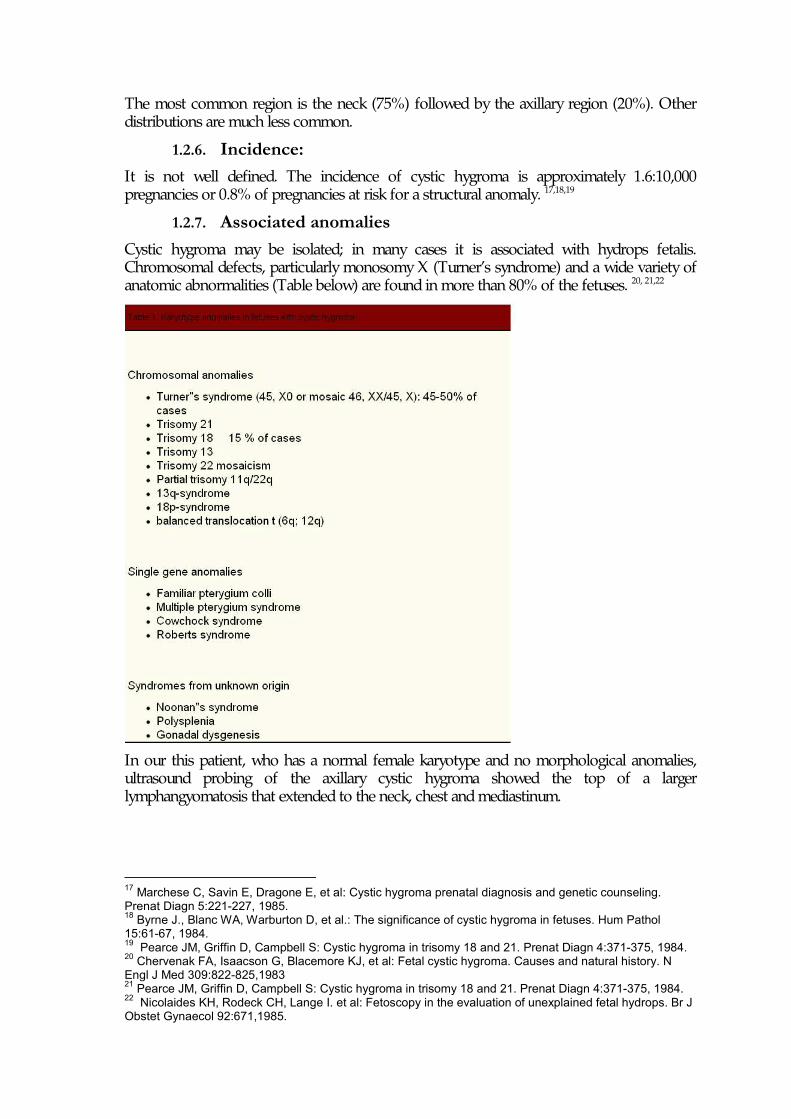
The most common region is the neck (75%) followed by the axillary region (20%). Other distributions are much less common.
1.2.6. Incidence: It is not well defined. The incidence of cystic hygroma is approximately 1.6:10,000 pregnancies or 0.8% of pregnancies at risk for a structural anomaly. 17,18,19
1.2.7. Associated anomalies Cystic hygroma may be isolated; in many cases it is associated with hydrops fetalis. Chromosomal defects, particularly monosomy X (Turner’s syndrome) and a wide variety of anatomic abnormalities (Table below) are found in more than 80% of the fetuses. 20, 21,22
In our this patient, who has a normal female karyotype and no morphological anomalies, ultrasound probing of the axillary cystic hygroma showed the top of a larger lymphangyomatosis that extended to the neck, chest and mediastinum.
17 Marchese C, Savin E, Dragone E, et al: Cystic hygroma prenatal diagnosis and genetic counseling. Prenat Diagn 5:221-227, 1985. 18 Byrne J., Blanc WA, Warburton D, et al.: The significance of cystic hygroma in fetuses. Hum Pathol 15:61-67, 1984. 19 Pearce JM, Griffin D, Campbell S: Cystic hygroma in trisomy 18 and 21. Prenat Diagn 4:371-375, 1984. 20 Chervenak FA, Isaacson G, Blacemore KJ, et al: Fetal cystic hygroma. Causes and natural history. N Engl J Med 309:822-825,1983 21 Pearce JM, Griffin D, Campbell S: Cystic hygroma in trisomy 18 and 21. Prenat Diagn 4:371-375, 1984. 22 Nicolaides KH, Rodeck CH, Lange I. et al: Fetoscopy in the evaluation of unexplained fetal hydrops. Br J Obstet Gynaecol 92:671,1985.
1.2.8. Ultrasound findings Cystic hygroma formed by multiple cysts ranging from a few millimeters to several centimeters in size. These cysts are filled with a lymph-like clear or sometimes echogenic fluid. The diagnostic clues of cystic hygroma include: asymmetric, thin-walled multiseptate, cystic masses of the posterolateral aspects of the neck with absence of meningocele, cephalocele, and calvarial defects.
1.2.9. Differential diagnosis Thyroglossal duct cyst, branchial cleft cyst, (dermoid and epidermoid cyst), bronchogenic (visceral) cyst, hamartoma of the mandible and cervical thymic cyst are all differential diagnoses for cystic hygroma of the anterior neck. Encephalocele and meningocele should be added for lesions of the posterior neck.
1.2.10. Prognosis The prognosis depends on the presence or absence of associated hydrops, chromosomal aberrations and anatomic defects.
Spontaneous resolution of a cystic hygroma of the neck in a fetus affected by Turner’s syndrome 23 and a fetus with normal karyotype have been described24.
The presence of hydrops fetalis or lymphangiectasia indicates a poor prognosis, with a mortality rate of 100 percent within a few weeks from diagnosis25.
Two reports 26,27 suggest that isolated cystic hygroma in a typical location in the neck or axilla may have a better prognosis.
In the literature, 32 cases of cystic hygroma in children are reported. In 12 cases the hygroma was localized in the neck, while in the remaining cases it was in rare sites28. Of these, six had hygromas in the axilla and chest wall, five in the mesentery and nine had lymphangiomas localized in various uncommon sites such as cervico-mediastinum, retroperitoneum, scrotum and multiple sites.
The complete excision of the cystic mass was possible in 23 cases 28. In another seven cases, only partial removal was possible because of the size of the cystic mass. Two of the twenty-three patients who underwent complete excision died during the postoperative period. It appears that the prognosis for these babies depends largely on the anatomical location and size of the tumors and on the ability of the pediatric surgeon to remove the masses.
1.2.11. Management: Standard obstetrical care.
23 Chodirker NB, Harman CR, Greenberg LR: Spontaneous resolution of a cystic hygroma in a fetus with Turner Syndrome. Prenat Diagn 8:201-206, 1988. 24 Baccichetti C, Lenzini E, Suma V, et al: Spontaneous resolution of cystic hygroma in a 46,XX normal female. Prenat Diagn 6:399-404, 1990 25 Frigoletto FD, Birnholz JC, Driscoll SG, et al: Ultrasound diagnosis of cystic hygroma. Am J Obstet Gynaecol. 136:962-964 26 Hoffman-Tretin J, Koenigsberg M, et al: Antenatal demonstration of axillary cystic hygroma. J Ultrasound Med 7:233-235, 1988. 27 Benacerraf BR, Frigoletto FD: Prenatal sonographic diagnosis of isolated congenital cystic hygroma unassociated with lymphedema or other morphologic abnormalities. J Ultrasound Med 6:63-66, 1987. 28 Singh S, Baboo ML, Pathak LC: Cystic lymphangioma in children: report of 32 cases including lesions at rare sites. Surgery 69:947-951,1987.
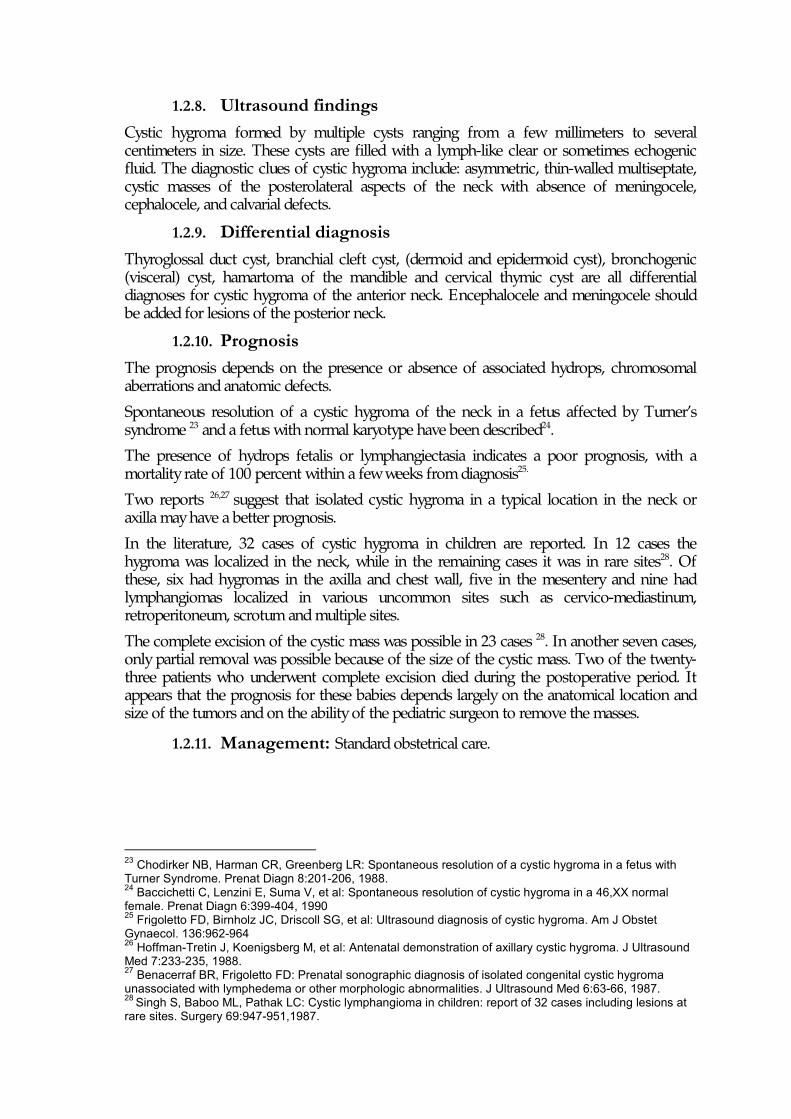
1.2.12. Case report: 1.2.12.1. Case 1:
Images at 13 weeks and 2 days: The sonographic findings were:septated cystic hygroma
• pleural effusion • hydrothorax • suspicion of a cardiac defect • ascites • edema
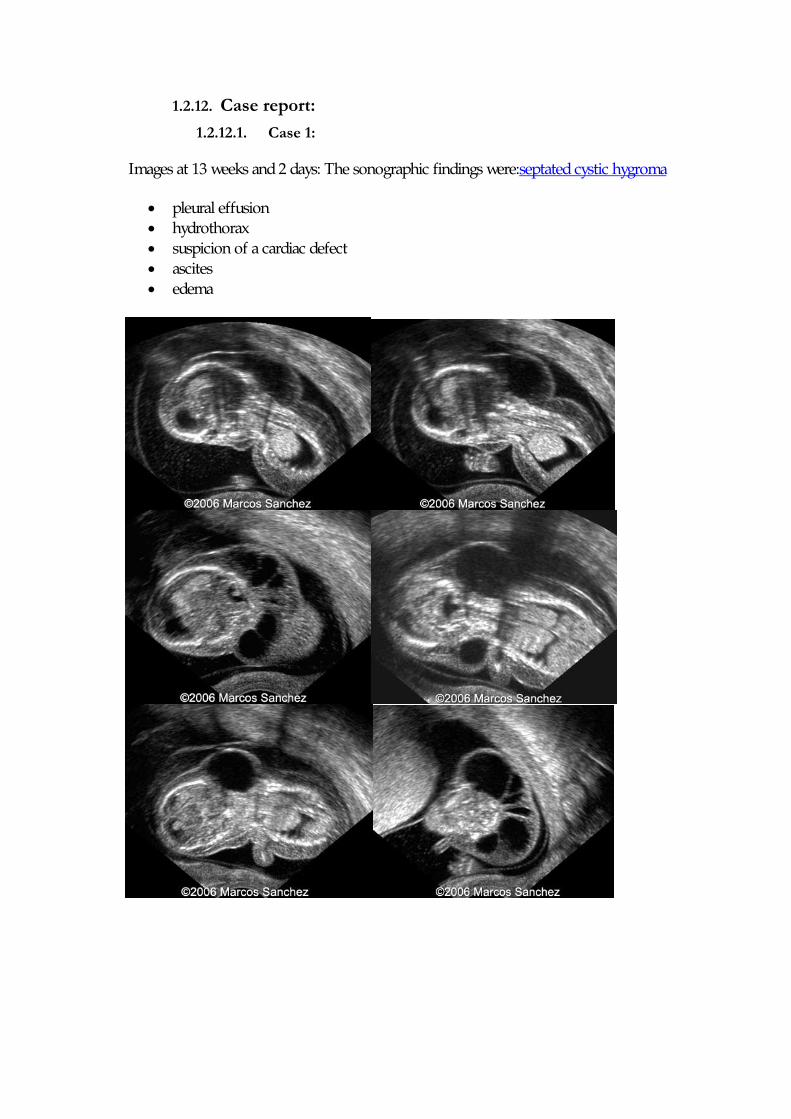
1.2.12.2. Case 2:
This second trimester fetus demonstrates a very thick nuchal edema with cystic hygroma:
The cystic hygroma extends down the back of the fetus and pleural effusions are visible:
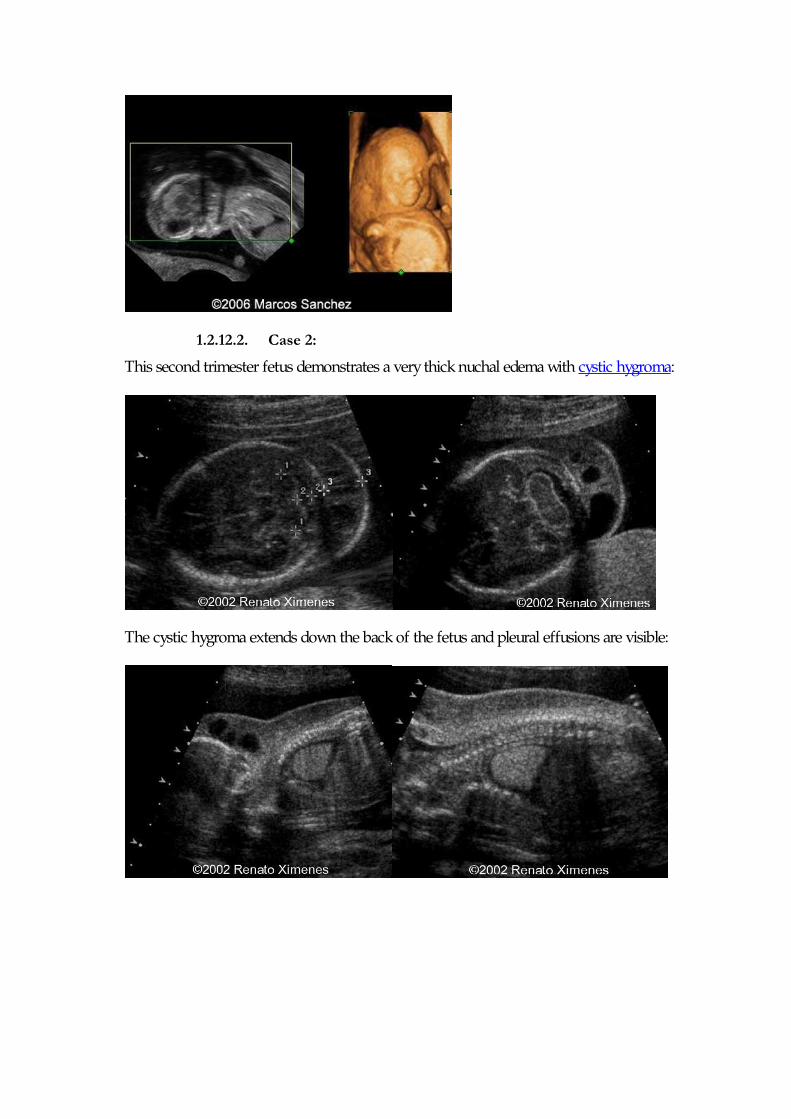
Postnatal Images:
This baby had several other associated anomalies , and diagnosis was Muliple Pterygium syndrome.
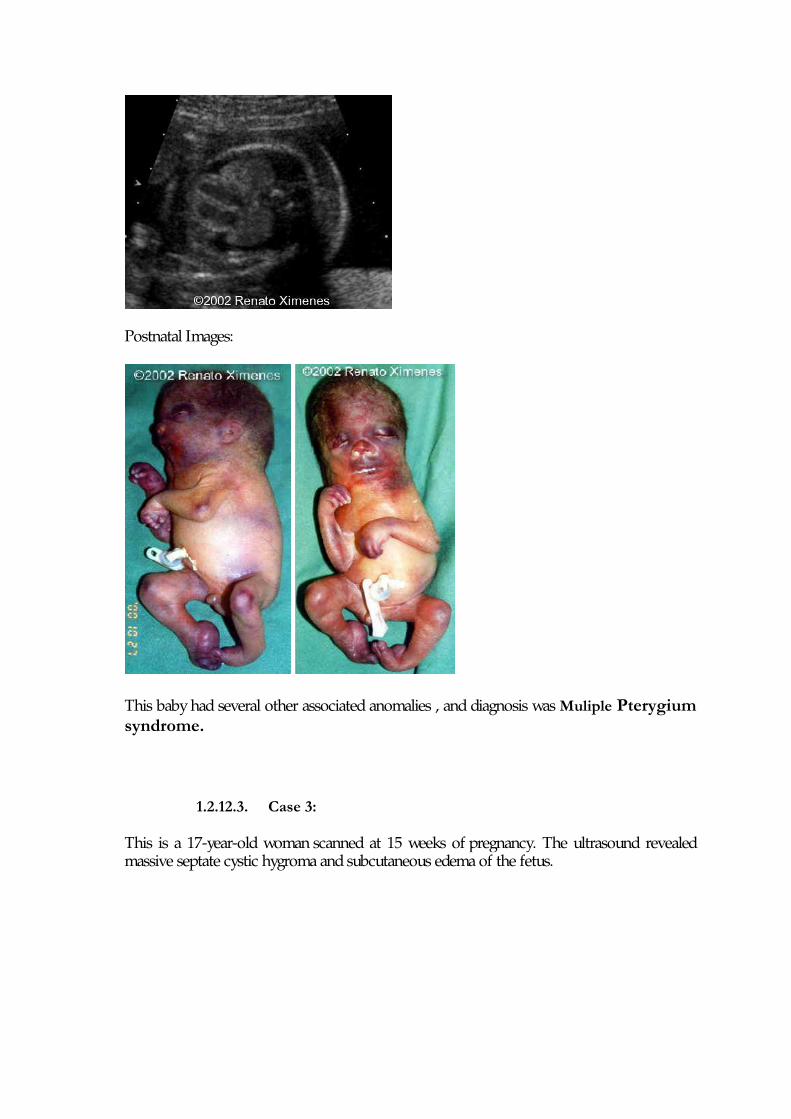
1.2.12.3. Case 3:
This is a 17-year-old woman scanned at 15 weeks of pregnancy. The ultrasound revealed massive septate cystic hygroma and subcutaneous edema of the fetus.
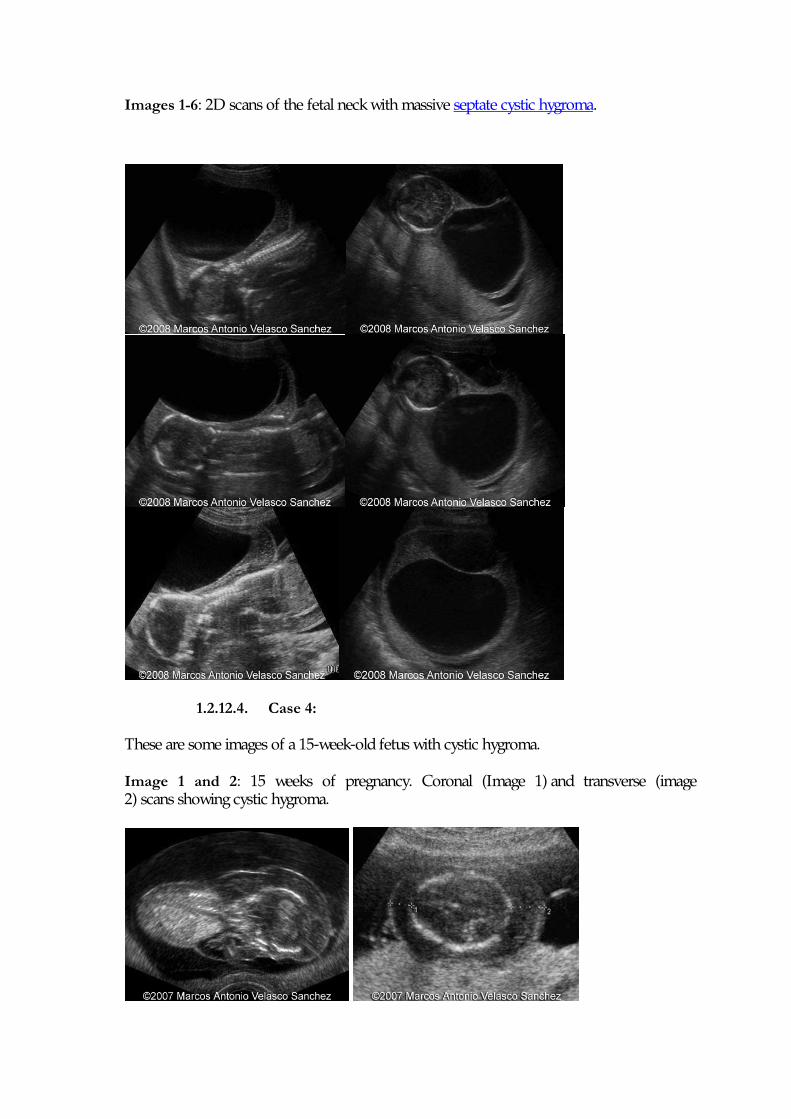
Images 1-6: 2D scans of the fetal neck with massive septate cystic hygroma.
1.2.12.4. Case 4:
These are some images of a 15-week-old fetus with cystic hygroma.
Image 1 and 2: 15 weeks of pregnancy. Coronal (Image 1) and transverse (image 2) scans showing cystic hygroma.
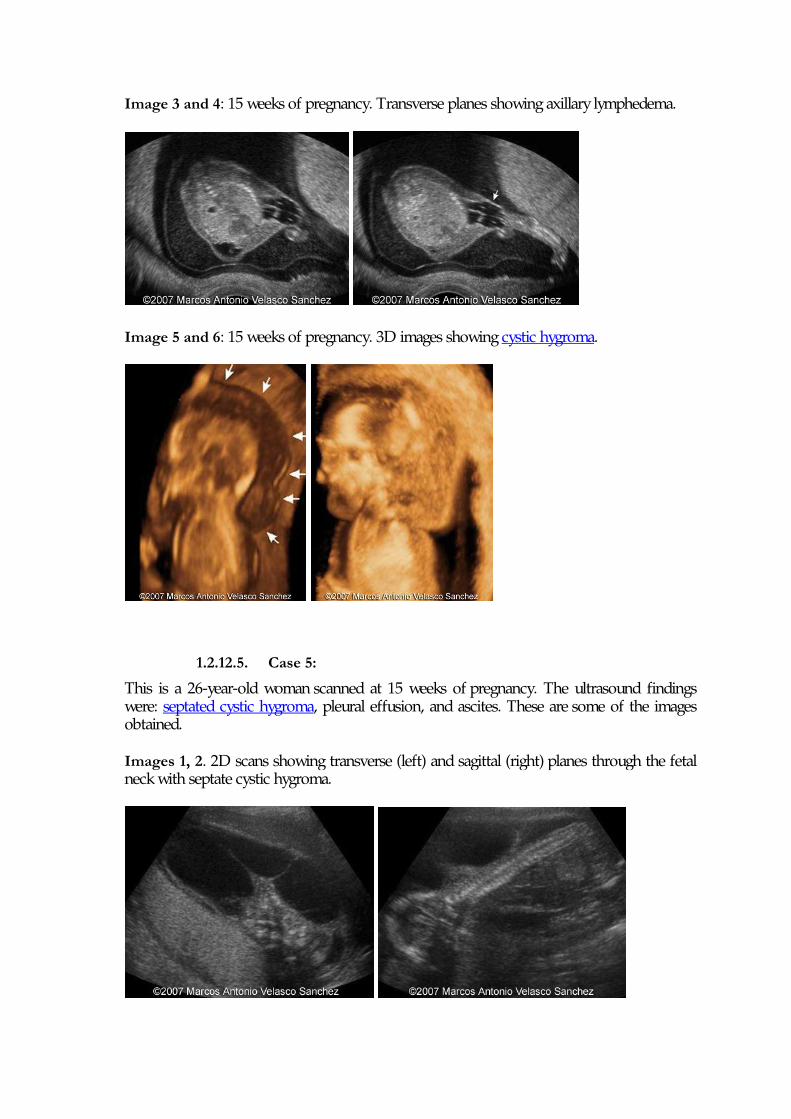
Image 3 and 4: 15 weeks of pregnancy. Transverse planes showing axillary lymphedema.
Image 5 and 6: 15 weeks of pregnancy. 3D images showing cystic hygroma.
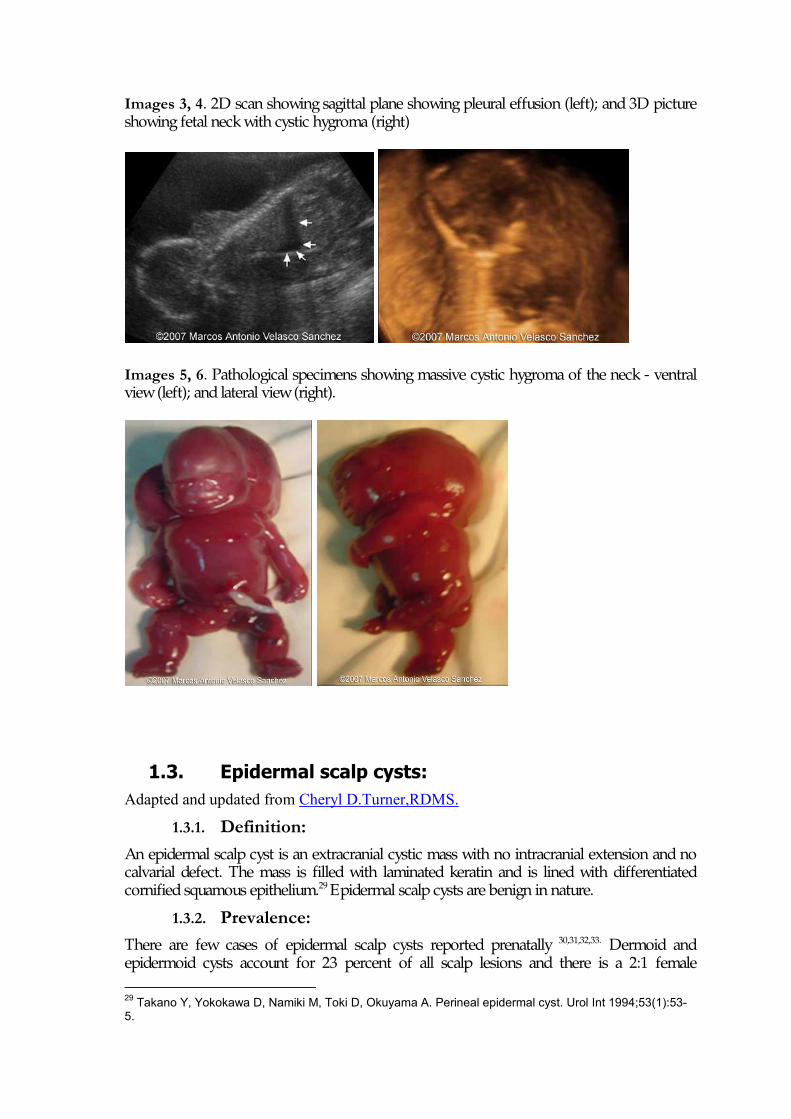
1.2.12.5. Case 5:
This is a 26-year-old woman scanned at 15 weeks of pregnancy. The ultrasound findings were: septated cystic hygroma, pleural effusion, and ascites. These are some of the images obtained.
Images 1, 2. 2D scans showing transverse (left) and sagittal (right) planes through the fetal neck with septate cystic hygroma.
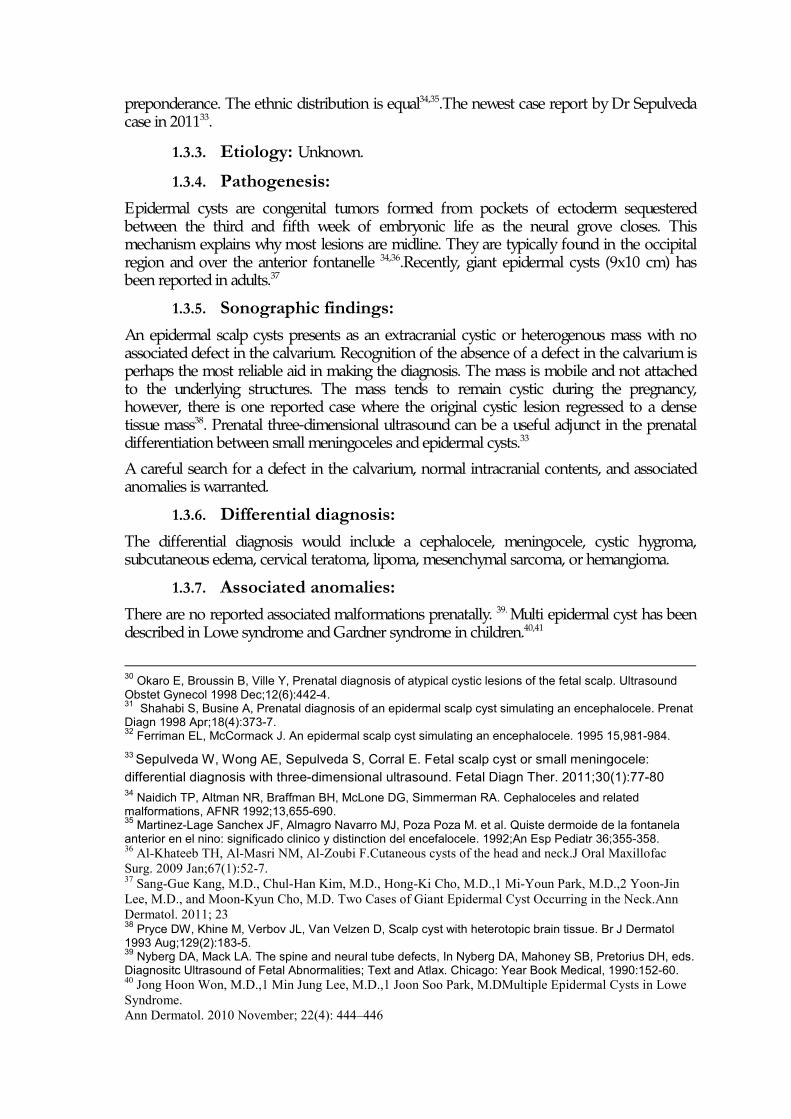
Images 3, 4. 2D scan showing sagittal plane showing pleural effusion (left); and 3D picture showing fetal neck with cystic hygroma (right)
Images 5, 6. Pathological specimens showing massive cystic hygroma of the neck - ventral view (left); and lateral view (right).
1.3. Epidermal scalp cysts: Adapted and updated from Cheryl D.Turner,RDMS.
1.3.1. Definition: An epidermal scalp cyst is an extracranial cystic mass with no intracranial extension and no calvarial defect. The mass is filled with laminated keratin and is lined with differentiated cornified squamous epithelium.29 Epidermal scalp cysts are benign in nature.
1.3.2. Prevalence: There are few cases of epidermal scalp cysts reported prenatally 30,31,32,33. Dermoid and epidermoid cysts account for 23 percent of all scalp lesions and there is a 2:1 female 29 Takano Y, Yokokawa D, Namiki M, Toki D, Okuyama A. Perineal epidermal cyst. Urol Int 1994;53(1):53-5.
preponderance. The ethnic distribution is equal34,35.The newest case report by Dr Sepulveda case in 201133.
1.3.3. Etiology: Unknown. 1.3.4. Pathogenesis:
Epidermal cysts are congenital tumors formed from pockets of ectoderm sequestered between the third and fifth week of embryonic life as the neural grove closes. This mechanism explains why most lesions are midline. They are typically found in the occipital region and over the anterior fontanelle 34,36.Recently, giant epidermal cysts (9x10 cm) has been reported in adults.37
1.3.5. Sonographic findings: An epidermal scalp cysts presents as an extracranial cystic or heterogenous mass with no associated defect in the calvarium. Recognition of the absence of a defect in the calvarium is perhaps the most reliable aid in making the diagnosis. The mass is mobile and not attached to the underlying structures. The mass tends to remain cystic during the pregnancy, however, there is one reported case where the original cystic lesion regressed to a dense tissue mass38. Prenatal three-dimensional ultrasound can be a useful adjunct in the prenatal differentiation between small meningoceles and epidermal cysts.33
A careful search for a defect in the calvarium, normal intracranial contents, and associated anomalies is warranted.
1.3.6. Differential diagnosis: The differential diagnosis would include a cephalocele, meningocele, cystic hygroma, subcutaneous edema, cervical teratoma, lipoma, mesenchymal sarcoma, or hemangioma.
1.3.7. Associated anomalies: There are no reported associated malformations prenatally. 39. Multi epidermal cyst has been described in Lowe syndrome and Gardner syndrome in children.40,41
30 Okaro E, Broussin B, Ville Y, Prenatal diagnosis of atypical cystic lesions of the fetal scalp. Ultrasound Obstet Gynecol 1998 Dec;12(6):442-4. 31 Shahabi S, Busine A, Prenatal diagnosis of an epidermal scalp cyst simulating an encephalocele. Prenat Diagn 1998 Apr;18(4):373-7. 32 Ferriman EL, McCormack J. An epidermal scalp cyst simulating an encephalocele. 1995 15,981-984. 33 Sepulveda W, Wong AE, Sepulveda S, Corral E. Fetal scalp cyst or small meningocele: differential diagnosis with three-dimensional ultrasound. Fetal Diagn Ther. 2011;30(1):77-80 34 Naidich TP, Altman NR, Braffman BH, McLone DG, Simmerman RA. Cephaloceles and related malformations, AFNR 1992;13,655-690. 35 Martinez-Lage Sanchex JF, Almagro Navarro MJ, Poza Poza M. et al. Quiste dermoide de la fontanela anterior en el nino: significado clinico y distinction del encefalocele. 1992;An Esp Pediatr 36;355-358. 36 Al-Khateeb TH, Al-Masri NM, Al-Zoubi F.Cutaneous cysts of the head and neck.J Oral Maxillofac Surg. 2009 Jan;67(1):52-7. 37 Sang-Gue Kang, M.D., Chul-Han Kim, M.D., Hong-Ki Cho, M.D.,1 Mi-Youn Park, M.D.,2 Yoon-Jin Lee, M.D., and Moon-Kyun Cho, M.D. Two Cases of Giant Epidermal Cyst Occurring in the Neck.Ann Dermatol. 2011; 23 38 Pryce DW, Khine M, Verbov JL, Van Velzen D, Scalp cyst with heterotopic brain tissue. Br J Dermatol 1993 Aug;129(2):183-5. 39 Nyberg DA, Mack LA. The spine and neural tube defects, In Nyberg DA, Mahoney SB, Pretorius DH, eds. Diagnositc Ultrasound of Fetal Abnormalities; Text and Atlax. Chicago: Year Book Medical, 1990:152-60. 40 Jong Hoon Won, M.D.,1 Min Jung Lee, M.D.,1 Joon Soo Park, M.DMultiple Epidermal Cysts in Lowe Syndrome. Ann Dermatol. 2010 November; 22(4): 444–446
1.3.8. Prognosis: There are four cases of epidermal scalp cyst reported 30,31. In two of the three cases, the cyst remained a small anechoic mass throughout the gestation as it did in our experience. One case reports the original cystic lesion had regressed to a dense tissue mass by 26 weeks gestation 30. In all cases, no reported associated anomalies were identified. The prognosis is excellent. No intervention is required.
1.3.9. Recurrence risk: All cases are sporadic; therefore the recurrence risk is low.
1.3.10. Management: Recognition of extracranial masses is important because of their benign nature. It is crucial to identify if a defect is present in the calvarium. When the bony defect is small the diagnosis is very difficult. A transvaginal scan with a high-frequency transducer or MRI may further delineate the mass and confirm that there is no intracranial extension. There have been at least two reported cases where the pregnancy was terminated for benign lesions. One was an occipital hemangioma and the other was an epidermal scalp cyst 32,42 The presence of an extracranial mass must lead to a careful consideration of the differential diagnosis. When prenatal diagnosis of an epidermal scan cyst is made with confidence, no further intervention is warranted.
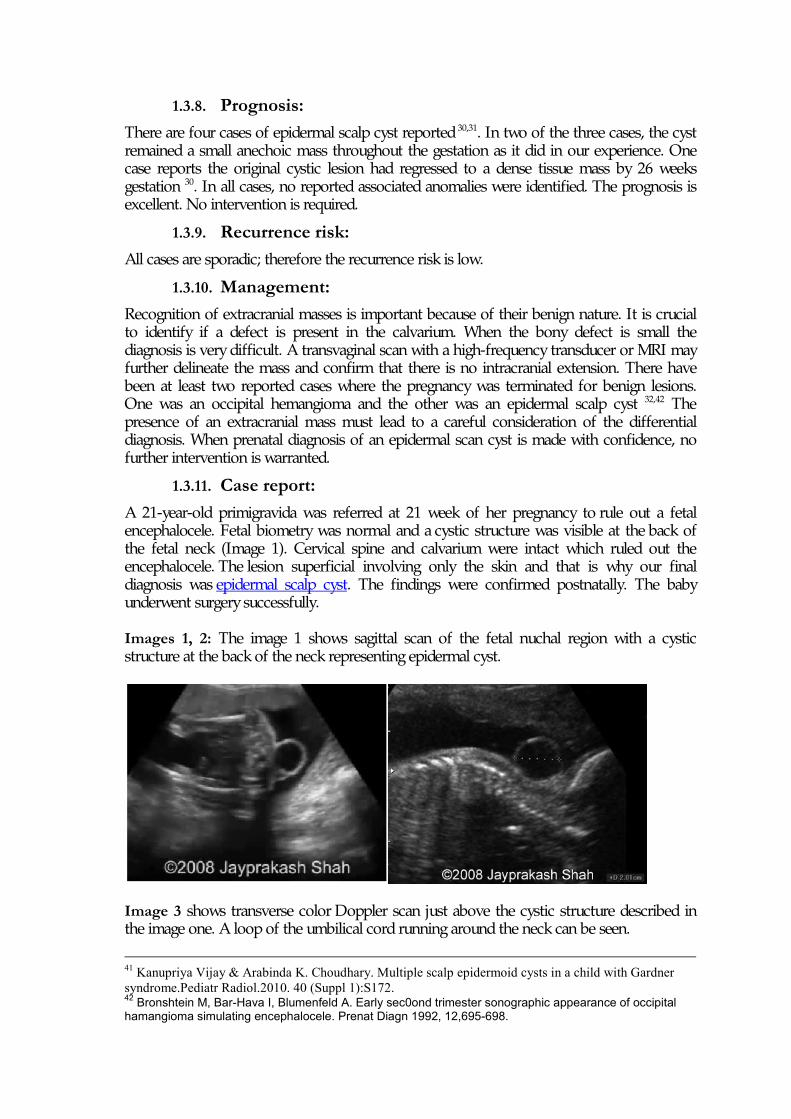
1.3.11. Case report: A 21-year-old primigravida was referred at 21 week of her pregnancy to rule out a fetal encephalocele. Fetal biometry was normal and a cystic structure was visible at the back of the fetal neck (Image 1). Cervical spine and calvarium were intact which ruled out the encephalocele. The lesion superficial involving only the skin and that is why our final diagnosis was epidermal scalp cyst. The findings were confirmed postnatally. The baby underwent surgery successfully. Images 1, 2: The image 1 shows sagittal scan of the fetal nuchal region with a cystic structure at the back of the neck representing epidermal cyst.
Image 3 shows transverse color Doppler scan just above the cystic structure described in the image one. A loop of the umbilical cord running around the neck can be seen.
41 Kanupriya Vijay & Arabinda K. Choudhary. Multiple scalp epidermoid cysts in a child with Gardner syndrome.Pediatr Radiol.2010. 40 (Suppl 1):S172. 42 Bronshtein M, Bar-Hava I, Blumenfeld A. Early sec0ond trimester sonographic appearance of occipital hamangioma simulating encephalocele. Prenat Diagn 1992, 12,695-698.
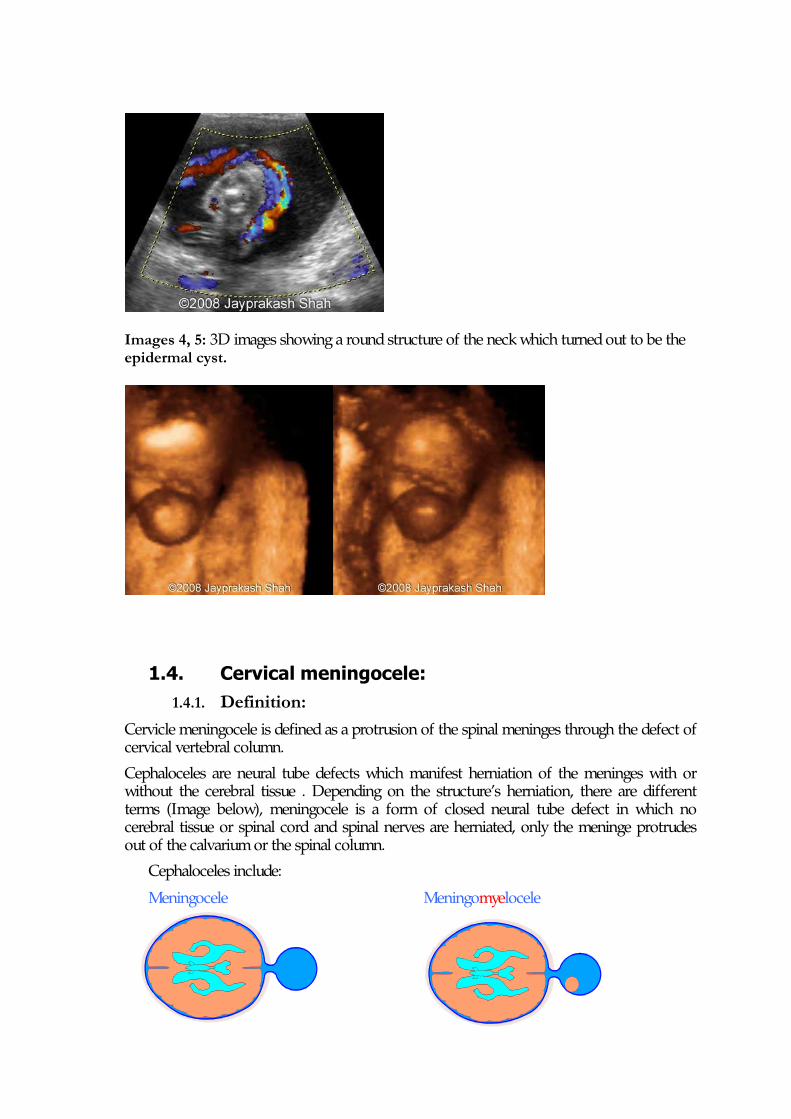
Images 4, 5: 3D images showing a round structure of the neck which turned out to be the epidermal cyst.
1.4. Cervical meningocele:
1.4.1. Definition: Cervicle meningocele is defined as a protrusion of the spinal meninges through the defect of cervical vertebral column.
Cephaloceles are neural tube defects which manifest herniation of the meninges with or without the cerebral tissue . Depending on the structure’s herniation, there are different terms (Image below), meningocele is a form of closed neural tube defect in which no cerebral tissue or spinal cord and spinal nerves are herniated, only the meninge protrudes out of the calvarium or the spinal column.
Cephaloceles include:
Meningocele Meningomyelocele

Encephalocele Encephalocystocele
1.4.2. Incidence: According to CDC, it is estimated that 4,000 pregnancies in the United States each year are affected by neural tube defects. Of that number, approximately 2,500 infants are born.
The meningocele can be revealed on skull and spine defect as well. The spinal meningocele is mostly located posterior to the spinal cord (80% of spinal meningocele case)50, including thoracic spine (70%), thoracolumbar junction(12%), lumbosacral (13%) and cervical (3%) spine. Men is equally affected to women is.43,44
Rarely, they could be seen as anterior and lateral meningocele. 1.4.3. Pathology: The cervical meningocele is a malformation that occurs during the neural tube’s development. There are 3 stages of the spinal cord development: gastrulation (week 2-3), primary neurulation ( week 3-4) and seconday neurulation ( week 5-6). At week 3-4, nine out of tenth of the spinal cord is formed. The final stage is the time for conus medullaris and filum terminal formation45,43. Some rare cases of anterior sacral meningoceles have been reported in which the failure of fusion of the sacrum results in the sacrum meninge herniation46, into the sacral hollow. Because of their occult location, they typically present later on in life with protean neurologic, urological or gastrointestinal complaints.47,48,49
1.4.4. Associated findings: 43 Lee HJ, Cho DY. Symptomatic spinal intradural arachnoid cysts in the pediatric age group: description of three new cases and review of the literature. Pediatr Neurosurg 35:181-187, 2001 44 Fobe JL, Nishikuni K, Gianni MA. Evolving magnetic resonance spinal cord trauma in child: from hemorrhage to intradural arachnoid cyst. Spinal Cord 36:864-866, 1998 45 Feltes CH, Fountas KN, Dimopoulos VG, et al. Cervical meningocele in association with spinal abnormalities. Childs Nerv Syst 20:357-361, 2004 46 Kontopoulos EV, Oyelese Y, Nath C, et al. Maternal anterior sacral meningocele in pregnancy. J Matern Fetal Neonatal Med 17:423-425, 2005. 47 Kubota Y, Kojima Y, Kohri K. . Maternal anterior sacral meningocele presenting as acute urinary retention in pregnancy. Int J Urol. 2012 Mar;19(3):279-80. 48 Lefere M, Verleyen N, Feys H, Somers JF. Anterior sacral meningocoele presenting as acute urinary retention. A case report. Acta Orthop Belg. 2009 Dec;75(6):855-7. 49 Anup Mohta, Swarup Das, and Rishi Jindal, Anterior sacral meningocele presenting as constipation. J Pediatr Neurosci. 2011 Jan-Jun; 6(1): 40–43.
90% of patients have associated occult spinal lesions such as tight filum terminale, split cord malformation, and epidermoids.50 1.4.5. Sonographic findings: A fluid-filled sac protrudes from the occipital region or posterior neck, no solid mass in side.
1.4.6. Pronosis: fairly good if there is no associated anomalies, and if the skin covers fully the herniation sac, if not, there would be a leakage of cerebrospinal fluid.
1.4.7. Management: Surgery needs to be performed shortly after birth prevent infection and restructure the exposed area of the herniation.
1.4.8. Differential diagnosis: Cervical meningocele can be differentiated from:
• Epidermal scalp cyst.33
• Cystic hygroma.51,52
1.4.9. Case report: 1.4.9.1. Case 1:
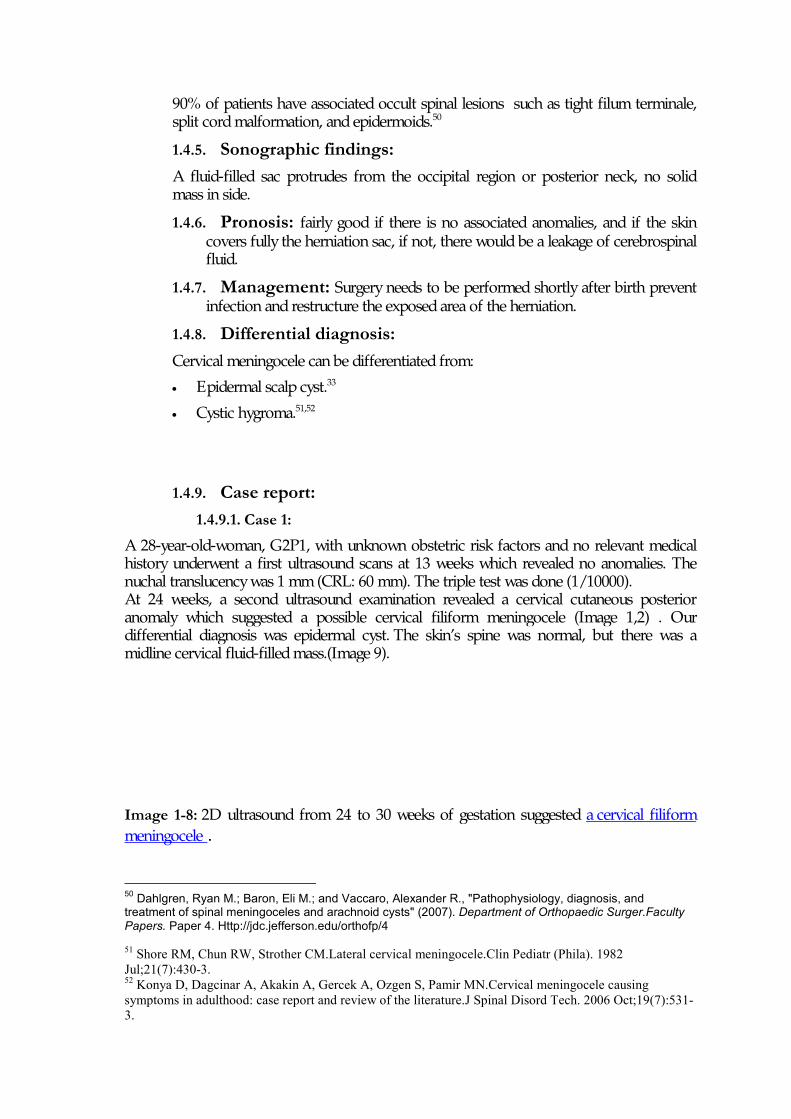
A 28-year-old-woman, G2P1, with unknown obstetric risk factors and no relevant medical history underwent a first ultrasound scans at 13 weeks which revealed no anomalies. The nuchal translucency was 1 mm (CRL: 60 mm). The triple test was done (1/10000). At 24 weeks, a second ultrasound examination revealed a cervical cutaneous posterior anomaly which suggested a possible cervical filiform meningocele (Image 1,2) . Our differential diagnosis was epidermal cyst. The skin’s spine was normal, but there was a midline cervical fluid-filled mass.(Image 9). Image 1-8: 2D ultrasound from 24 to 30 weeks of gestation suggested a cervical filiform meningocele .
50 Dahlgren, Ryan M.; Baron, Eli M.; and Vaccaro, Alexander R., "Pathophysiology, diagnosis, and treatment of spinal meningoceles and arachnoid cysts" (2007). Department of Orthopaedic Surger.Faculty Papers. Paper 4. Http://jdc.jefferson.edu/orthofp/4 51 Shore RM, Chun RW, Strother CM.Lateral cervical meningocele.Clin Pediatr (Phila). 1982 Jul;21(7):430-3. 52 Konya D, Dagcinar A, Akakin A, Gercek A, Ozgen S, Pamir MN.Cervical meningocele causing symptoms in adulthood: case report and review of the literature.J Spinal Disord Tech. 2006 Oct;19(7):531-3.
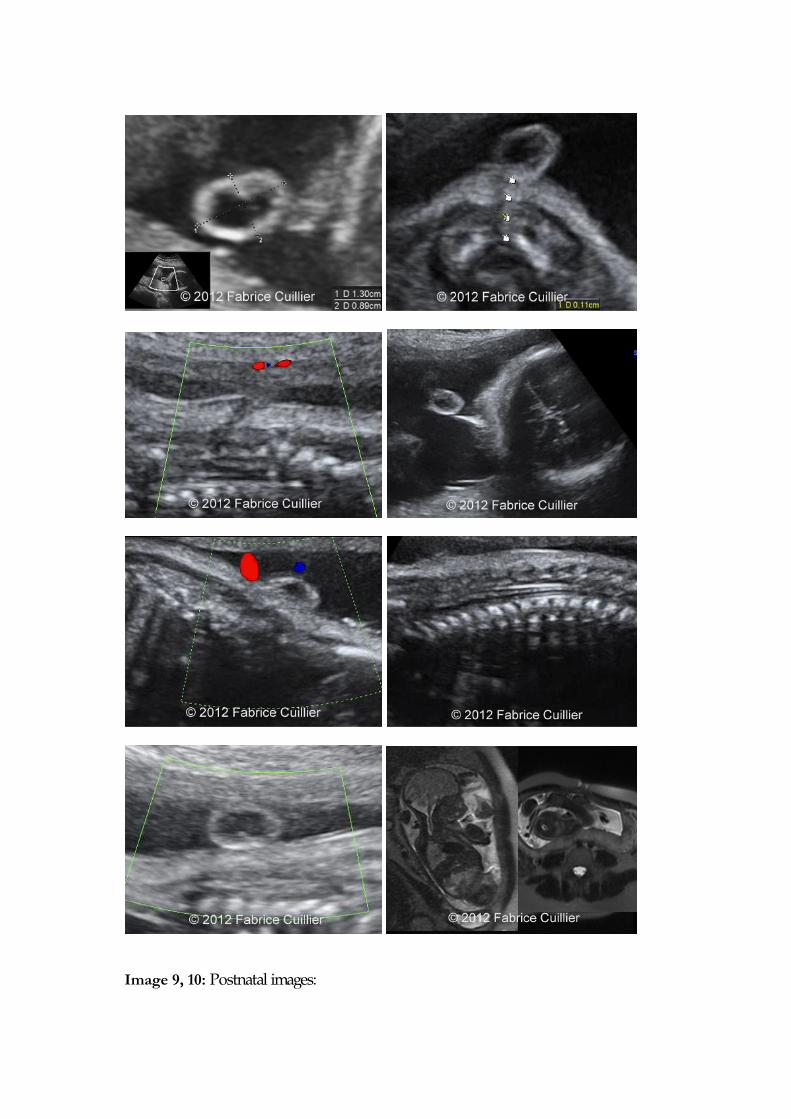
Image 9, 10: Postnatal images:
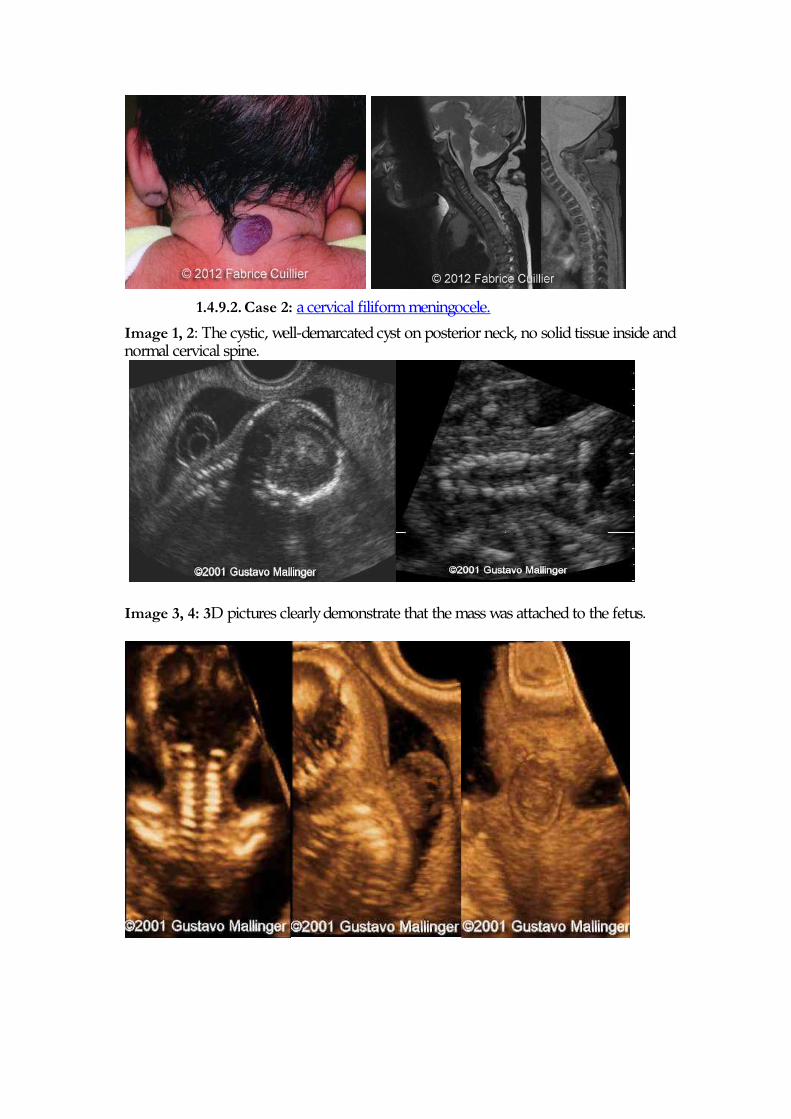
1.4.9.2. Case 2: a cervical filiform meningocele.
Image 1, 2: The cystic, well-demarcated cyst on posterior neck, no solid tissue inside and normal cervical spine.
Image 3, 4: 3D pictures clearly demonstrate that the mass was attached to the fetus.
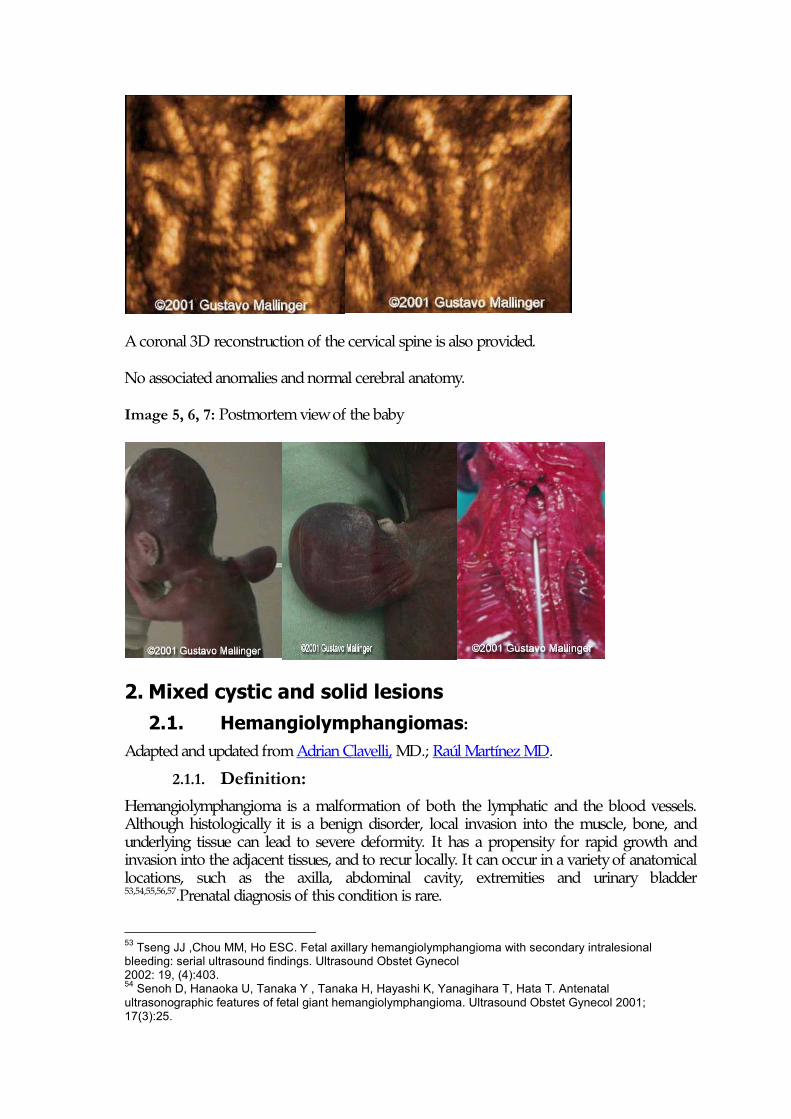
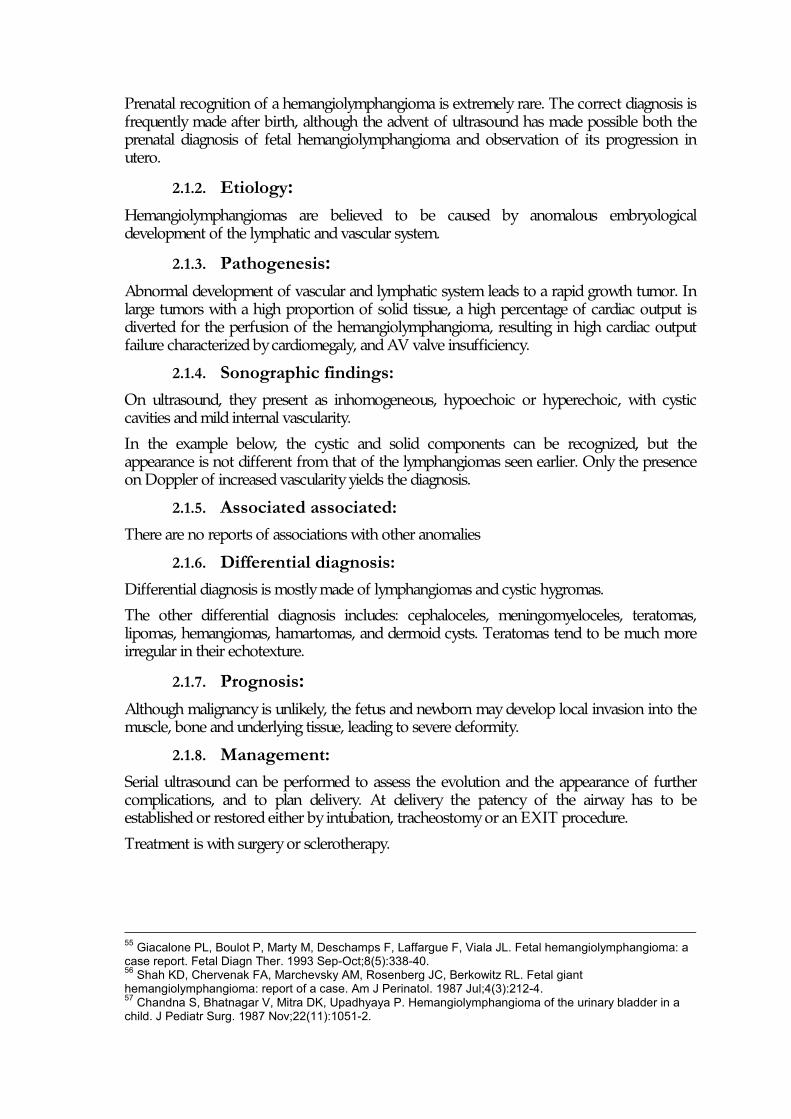
A coronal 3D reconstruction of the cervical spine is also provided.
No associated anomalies and normal cerebral anatomy.
Image 5, 6, 7: Postmortem view of the baby
2. Mixed cystic and solid lesions
2.1. Hemangiolymphangiomas: Adapted and updated from Adrian Clavelli, MD.; Raúl Martínez MD.
2.1.1. Definition: Hemangiolymphangioma is a malformation of both the lymphatic and the blood vessels. Although histologically it is a benign disorder, local invasion into the muscle, bone, and underlying tissue can lead to severe deformity. It has a propensity for rapid growth and invasion into the adjacent tissues, and to recur locally. It can occur in a variety of anatomical locations, such as the axilla, abdominal cavity, extremities and urinary bladder 53,54,55,56,57.Prenatal diagnosis of this condition is rare.
53 Tseng JJ ,Chou MM, Ho ESC. Fetal axillary hemangiolymphangioma with secondary intralesional bleeding: serial ultrasound findings. Ultrasound Obstet Gynecol 2002: 19, (4):403. 54 Senoh D, Hanaoka U, Tanaka Y , Tanaka H, Hayashi K, Yanagihara T, Hata T. Antenatal ultrasonographic features of fetal giant hemangiolymphangioma. Ultrasound Obstet Gynecol 2001; 17(3):25.
Prenatal recognition of a hemangiolymphangioma is extremely rare. The correct diagnosis is frequently made after birth, although the advent of ultrasound has made possible both the prenatal diagnosis of fetal hemangiolymphangioma and observation of its progression in utero.
2.1.2. Etiology: Hemangiolymphangiomas are believed to be caused by anomalous embryological development of the lymphatic and vascular system.
2.1.3. Pathogenesis: Abnormal development of vascular and lymphatic system leads to a rapid growth tumor. In large tumors with a high proportion of solid tissue, a high percentage of cardiac output is diverted for the perfusion of the hemangiolymphangioma, resulting in high cardiac output failure characterized by cardiomegaly, and AV valve insufficiency.
2.1.4. Sonographic findings: On ultrasound, they present as inhomogeneous, hypoechoic or hyperechoic, with cystic cavities and mild internal vascularity.
In the example below, the cystic and solid components can be recognized, but the appearance is not different from that of the lymphangiomas seen earlier. Only the presence on Doppler of increased vascularity yields the diagnosis.
2.1.5. Associated associated: There are no reports of associations with other anomalies
2.1.6. Differential diagnosis: Differential diagnosis is mostly made of lymphangiomas and cystic hygromas.
The other differential diagnosis includes: cephaloceles, meningomyeloceles, teratomas, lipomas, hemangiomas, hamartomas, and dermoid cysts. Teratomas tend to be much more irregular in their echotexture.
2.1.7. Prognosis: Although malignancy is unlikely, the fetus and newborn may develop local invasion into the muscle, bone and underlying tissue, leading to severe deformity.
2.1.8. Management: Serial ultrasound can be performed to assess the evolution and the appearance of further complications, and to plan delivery. At delivery the patency of the airway has to be established or restored either by intubation, tracheostomy or an EXIT procedure.
Treatment is with surgery or sclerotherapy.
55 Giacalone PL, Boulot P, Marty M, Deschamps F, Laffargue F, Viala JL. Fetal hemangiolymphangioma: a case report. Fetal Diagn Ther. 1993 Sep-Oct;8(5):338-40. 56 Shah KD, Chervenak FA, Marchevsky AM, Rosenberg JC, Berkowitz RL. Fetal giant hemangiolymphangioma: report of a case. Am J Perinatol. 1987 Jul;4(3):212-4. 57 Chandna S, Bhatnagar V, Mitra DK, Upadhyaya P. Hemangiolymphangioma of the urinary bladder in a child. J Pediatr Surg. 1987 Nov;22(11):1051-2.
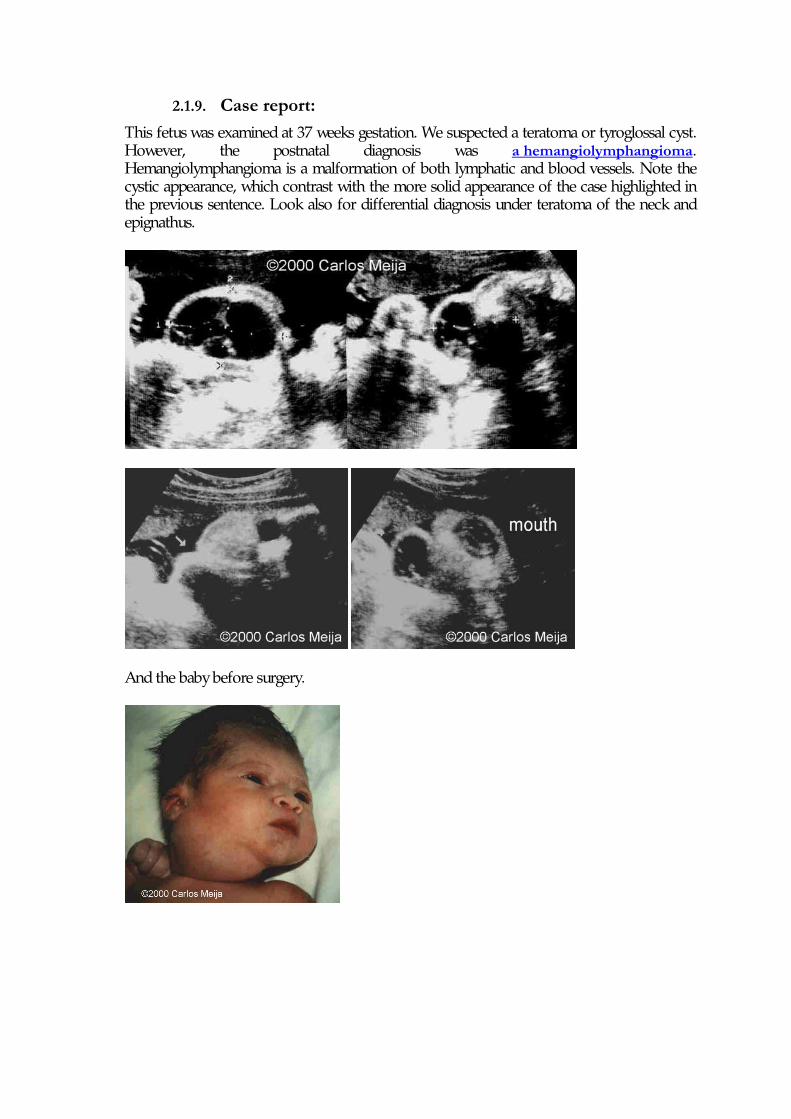
2.1.9. Case report: This fetus was examined at 37 weeks gestation. We suspected a teratoma or tyroglossal cyst. However, the postnatal diagnosis was a hemangiolymphangioma. Hemangiolymphangioma is a malformation of both lymphatic and blood vessels. Note the cystic appearance, which contrast with the more solid appearance of the case highlighted in the previous sentence. Look also for differential diagnosis under teratoma of the neck and epignathus.
And the baby before surgery.
3. Mostly solid lesions with included cystic components:
3.1. Hemangioma: Adapted and updated from Adrian Clavelli,MD ; Frantisek Grochal, MD.
3.1.1. Definition: Hemangiomas are benign tumors made up of blood vessels. They are classified as:
•••• Cavernous
•••• Capillary (strawberry)
•••• Mixed
Strawberry hemangiomas are red protuberant masses that may occur on any area of the body but in particular on the face, scalp, back, and anterior chest. 1-3% of infants have some and girls are 3 times more likely then boys to have some. They may be solitary or multiple. Spontaneous regression is common (60% of these lesions involute with the first 5 year, and most of the rest by 10 years). It has been reported that those diagnosed prenatally migh actually involute faster than those diagnosed postnatally 58 MRI has occasionally been performed 59 to differentiate from a cephalocele60, but the ultrasound appearance is usually characteristic 61,62,63,64,65. These are commonly found in the head66, heart67,68 , limbs 69,70 and liver 71, 72, 73, abdomen 74 , skin 75 and cord76 . A rare complication is a thrombocytopenic coagulopathy: the Kasabach-Merritt syndrome.
58 Boon LM, Enjolras O, Mulliken JB Congenital hemangioma: evidence of accelerated involution. J Pediatr 1996 Mar;128(3):329-35 59 Kramer LA, Crino JP, Slopis J, Hankins L, Yeakley J Capillary hemangioma of the neck: prenatal MR findings. AJNR Am J Neuroradiol 1997 Sep;18(8):1432-4
60 Sherer DM, Perillo AM, Abramowicz JS Fetal hemangioma overlying the temporal occipital suture, initially diagnosed by ultrasonography as an encephalocele. J Ultrasound Med 1993 Nov;12(11):691-3
61 Suchet IB Ultrasonography of the fetal neck in the second and third trimesters. Part 3. Anomalies of the anterior and anterolateral nuchal region. Can Assoc Radiol J 1995 Dec;46(6):426-33 62 Shipp TD, Bromley B, Benacerraf B The ultrasonographic appearance and outcome for fetuses with masses distorting the fetal face. J Ultrasound Med 1995 Sep;14(9):673-8 63 Lasser D, Preis O, Dor N, Tancer ML Antenatal diagnosis of giant cystic cavernous hemangioma by Doppler velocimetry. Obstet Gynecol 1988 Sep;72(3 Pt 2):476-7 64 McGahan JP, Schneider JM Fetal neck hemangioendothelioma with secondary hydrops fetalis: sonographic diagnosis. J Clin Ultrasound 1986 Jun;14(5):384-8 65 Grundy H, Glasmann A, Burlbaw J, Walton S, Dannar C, Doan LHemangioma presenting as a cystic mass in the fetal neck. J Ultrasound Med 1985 Mar;4(3):147-50 66 Boulot P, Deschamps F, Montoya F, Montoya P, Couture A, Ferran JL, Lefort G Prenatal aspects of giant fetal cranial haemangio-endothelioma. Prenat Diagn 1996 Apr;16(4):357-9
67 Eckstein FS, Heinemann MK, Mielke GJ, Greschniok A, Bader P, Ziemer G Resection of a large right atrial hemangioma in a neonate after prenatal diagnosis. Ann Thorac Surg 1999 Sep;68(3):1074-5
68 Tseng JJ, Chou MM, Lee YH, Ho ES In utero diagnosis of cardiac hemangioma. Ultrasound Obstet Gynecol 1999 May;13(5):363-5 69 Raman S, Ramanujam T, Lim CT Prenatal diagnosis of an extensive haemangioma of the fetal leg: a case report. J Obstet Gynaecol Res 1996 Aug;22(4):375-8 70 Goncalves LF, Pereira ET, Parente LM, Vitorello DA, Barbosa UC, Saab Neto JA Cutaneous hemangioma of the thigh: prenatal diagnosis. Ultrasound Obstet Gynecol 1997 Feb;9(2):128-30.
71 Morris J, Abbott J, Burrows P, Levine D Antenatal diagnosis of fetal hepatic hemangioma treated with maternal corticosteroids.Obstet Gynecol 1999 Nov;94(5 Pt 2):813-5
Cavernous hemangiomas are masses of dilated vessels deep in the skin. They appear as pale, skin-colored, red, or blue masses that are not as sharply defined as the strawberry hemangiomas. They also may undergo spontaneous resolution. Prenatally they may be responsible for hydrops77. Some rare cases of carvenous hemangioma was also found in the nasal cavity and the maxillary sinus.78,79,80,81
3.1.2. Incidence: Hemangiomas are the most common tumors of infancy. Infantile hemangiomas occur in 4% to 10% of white infants, and they are 3 to 5 times more commonly seen in female infants, most frequently in whites and less commonly in those of African or Asian descent 82. Congenital hemangiomas are much more rare.
3.1.3. Recurrence risk: Most hemangiomas occur sporadically, but some families with autosomal dominant inheritance have been reported 83.
3.1.4. Pathogenesis: Pathogenesis of congenital hemangiomas is not very well understood. Some authors believe that they could originate from either invading angioblasts that differentiate toward a placental phenotype or form embolized placental cells. Erythrocyte type glucose transporter
72 Chuileannain FN, Rowlands S, Sampson A Ultrasonographic appearances of fetal hepatic hemangioma. J Ultrasound Med 1999 May;18(5):379-81 73 Dreyfus M, Baldauf JJ, Dadoun K, Becmeur F, Berrut F, Ritter J Prenatal diagnosis of hepatic hemangioma. Fetal Diagn Ther 1996 Jan-Feb;11(1):57-60
74 Maynor CH, Hertzberg BS, Kliewer MA, Heyneman LE, Carroll BA Antenatal ultrasonographic diagnosis of abdominal wall hemangioma: potential to simulate ventral abdominal wall defects. J Ultrasound Med 1995 Apr;14(4):317-9
75 Treadwell MC, Sepulveda W, LeBlanc LL, Romero R Prenatal diagnosis of fetal cutaneous hemangioma: case report and review of the literature. J Ultrasound Med 1993 Nov;12(11):683-7
76 Miller KA, Gauderer MW Hemangioma of the umbilical cord mimicking an omphalocele. J Pediatr Surg 1997 Jun;32(6):810-2
77 Sharara FI, Khoury AN Prenatal diagnosis of a giant cavernous hemangioma in association with nonimmunehydrops. A case report. J Reprod Med 1994 Jul;39(7):547-9
78 Starska K, Lukomski M, Danilewicz M. Hemangioma cavernous of the nasal cavity and the maxillary sinus--case report and review of the literature. Otolaryngol Pol. 2006;60(6):955-7. 79 Jammal H, Barakat F, Hadi U.Maxillary sinus cavernous hemangioma: a rare entity. Acta Otolaryngol. 2004 Apr;124(3):331-3. 80 Engels T, Schörner W, Felix R, Witt H, Jahnke V. Cavernous hemangioma of the maxillary sinus. HNO. 1990 Sep;38(9):342-4. 81 Lahoz Zamarro MT, Galvé Royo A, Royo J, Valero J, Cámara F. Cavernous hemangioma of the maxillary sinus. Acta Otorrinolaringol Esp. 1990 May-Jun;41(3):197-9. 82 Krol A, MacArthur CJ. Congenital hemangiomas: Rapidly Involuting and Noninvoluting Congenital Hemangiomas. Arch Facial Plast Surg, Sep 2005; 7: 307 - 311. 83 Walter JW, North PE, Waner M, Mizeracki A, Blei F, Walker JW, Reinisch JF, Marchuk DA. Somatic mutation of vascular endothelial growth factor receptors in juvenile hemangioma. Genes Chromosomes Cancer. 2002 Mar;33(3):295-303.
isoform 1 (GLUT1), a glucose transporter enzyme, is uniquely expressed on endothelial cells of hemangiomas but not in surrounding normal vascular endothelium84. Lymphatic endothelial hyaluronan receptor-1 (LYVE-1), a specific marker for normal and tumor-associated lymphatic vessels, was strongly expressed in tumor cells of infantile hemangiomas but was absent during involution. That is why some authors believe that endothelial cells in proliferating infantile hemangioma are arrested in an early developmental stage of vascular differentiation.85 Some overlapping clinical and pathologic features can be found among rapid involuting congenital hemangiomas, non-involuting congenital hemangiomas and infantile hemangiomas. These observations support the hypothesis that these vascular tumors may be variations of a single entity “ab initio”, but it is unknown whether the progenitor cell for these uncommon congenital vascular tumors is the same as for common infantile hemangioma 86.
3.1.5. Diagnosis: The diagnosis clues of probably suggested are: of huge vascular beds, and color Doppler flow imaging could depict marked blood flow in the solid part of the mass.
3.1.6. Sonographic findings: Usually hypoechoic lesions mostly confined to the subcutaneous fat with diffuse vasculature. Some of the vessels show a venous flow signal, while others demonstrated low resistant arterial flow87. Large and irregular feeding arteries are in disorganized patterns, arterial aneurysms, direct arteriovenous shunts, and intravascular thrombi are present 88. Sonographically detectable hemangiomas are usually of the cavernous type, which involve not only cutaneous vessels but also larger venous sinusoids in the deep dermis and subcutaneous tissues. The most common appearance is that of a solid mass with an echotexture similar to placenta, but cystic hemangiomas have also been reported89. Hemangiomas do not change bony anatomy in the region.
3.1.7. Differential diagnosis: •••• Lymphangioma ( include cystic hygroma)
•••• Hemangiolymphangiomas
•••• Nuchal teratoma
•••• Neuroblastoma
84 North PE, Waner M, Mizeracki A, Mihm MC Jr. GLUT1: A newly discovered immunohistochemical marker for juvenile hemangiomas. Hum Pathol, 2000; 31(1):11-22. 85 Dadras SS, North PE, Bertoncini J, Mihm MC, Detmar M. Infantile hemangiomas are arrested in an early developmental vascular differentiation state. Mod Pathol. 2004; 17:1068-1079. 86 Berengauer B, Mulliken JB, Enjolras O, Boon LM, Wassef M, Josset P, Burrows PE, Perez-Atayde AR, Kozakewich HP. Rapidly involutiing congenital hemangioma: clinical and histopathologic features. Pediatr Dev Pathol., 2003 Nov-Dec; 6(6): 495 – 510. 87 Rogers M, Lam A, Fischer G. Sonographic findings in a series of rapidly involuting congenital hemangiomas (RICH). Pediatr Dermatol. 2002 Jan-Feb;19(1):5-11. 88 Grisey A, Roth P, Martin A, Czorny A, Riehl-Duvinage C, Maillet R, Schaal JP. Prenatal diagnosis and management of a case of rapidly involuting congenital hemangioma. Review of literature. J Gynecol Obstet Biol Reprod (Paris), 2006 Jun; 35(4): 405-10. 89 Callen PW. Masses of the face and anterior neck. In: Ultrasonography in obstetrics and gynecology. 2000. W.B. Saunders Company. Page 316.
3.1.8. Prognosis: Good, rare complication. Rapidly involuting congenital hemangioma promptly resolve postnatally over the early months of life, with complete resolution, sometimes with residual atrophy, occurring at less than 1 year of age in most of the patients87.
3.1.9. Management: Management is different to each location of hemangiomas, the size of the mass and the vascularization. Embolization and complete removal the mass could be necessary. Hemangiomas typically recur following incomplete surgical excision.
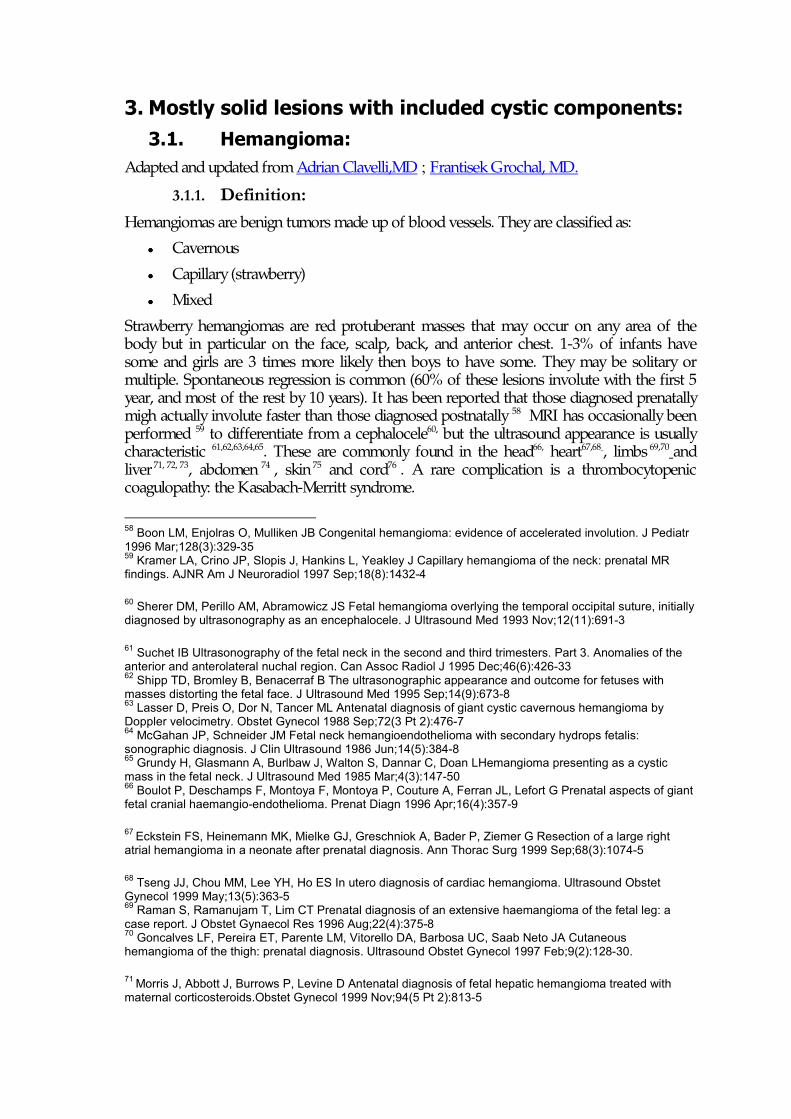
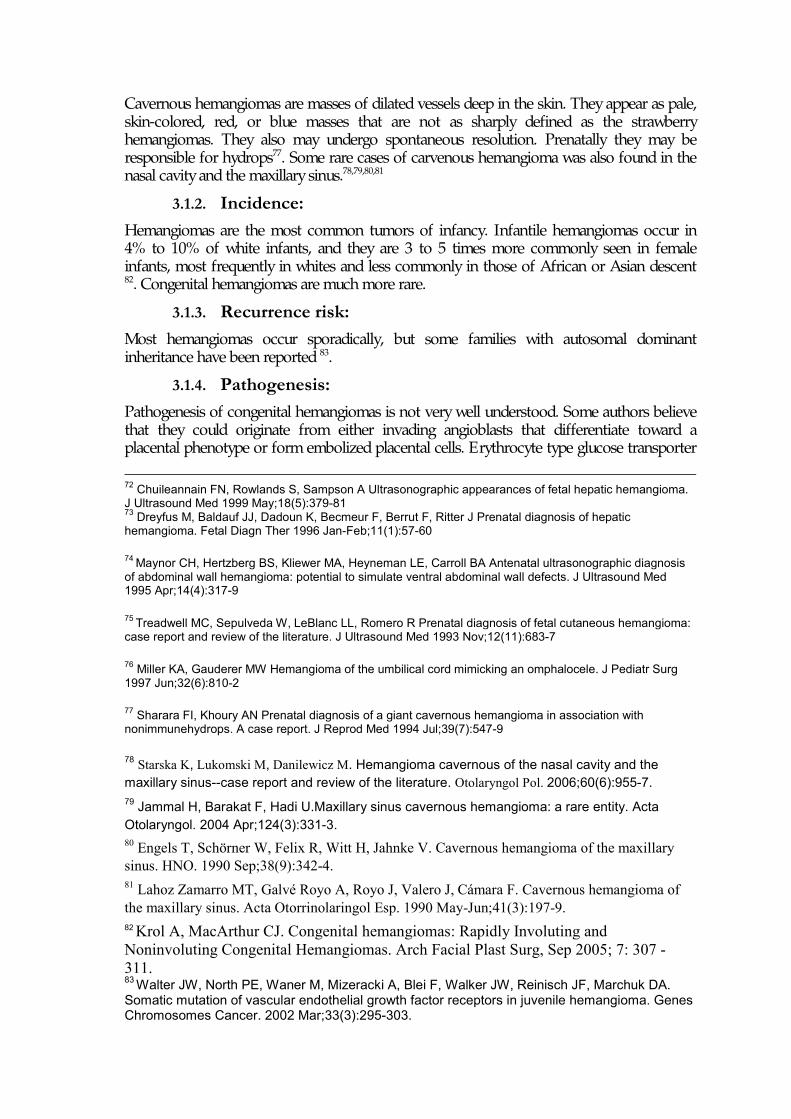
3.1.10. Case report: Images 1, 2. Transverse sections through the skull showing tumor (hemangioma) in nuchal region with rich vascularization.
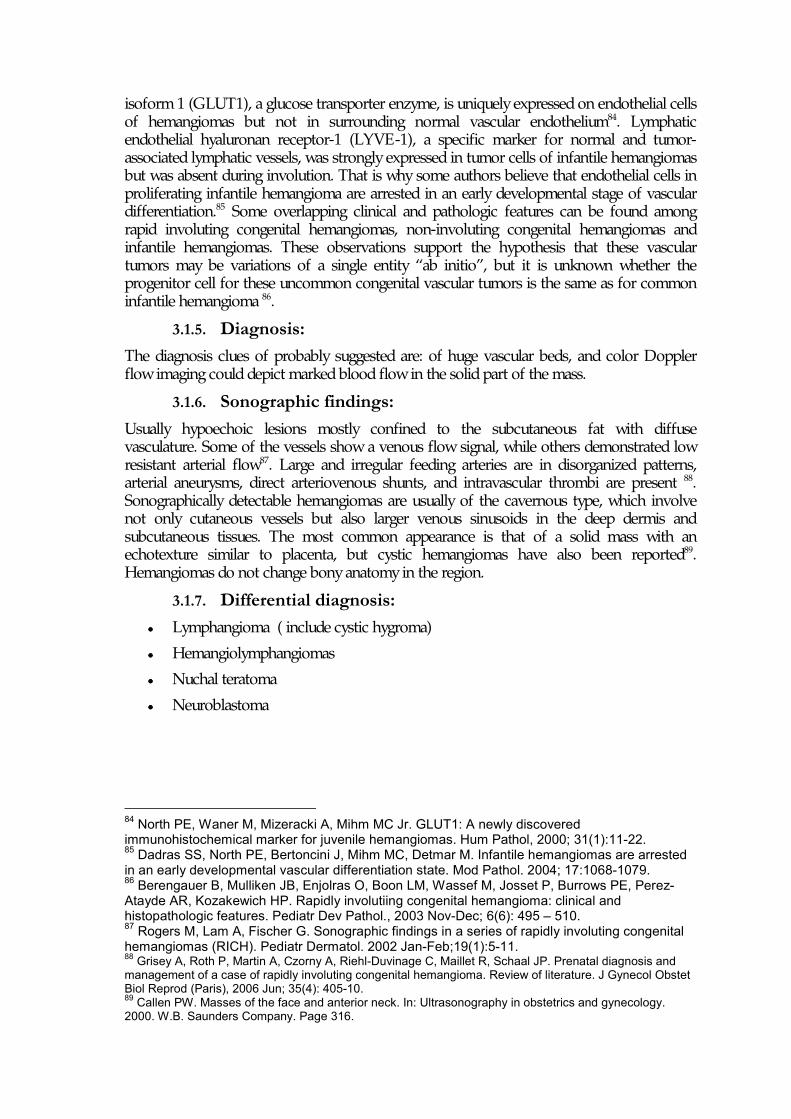
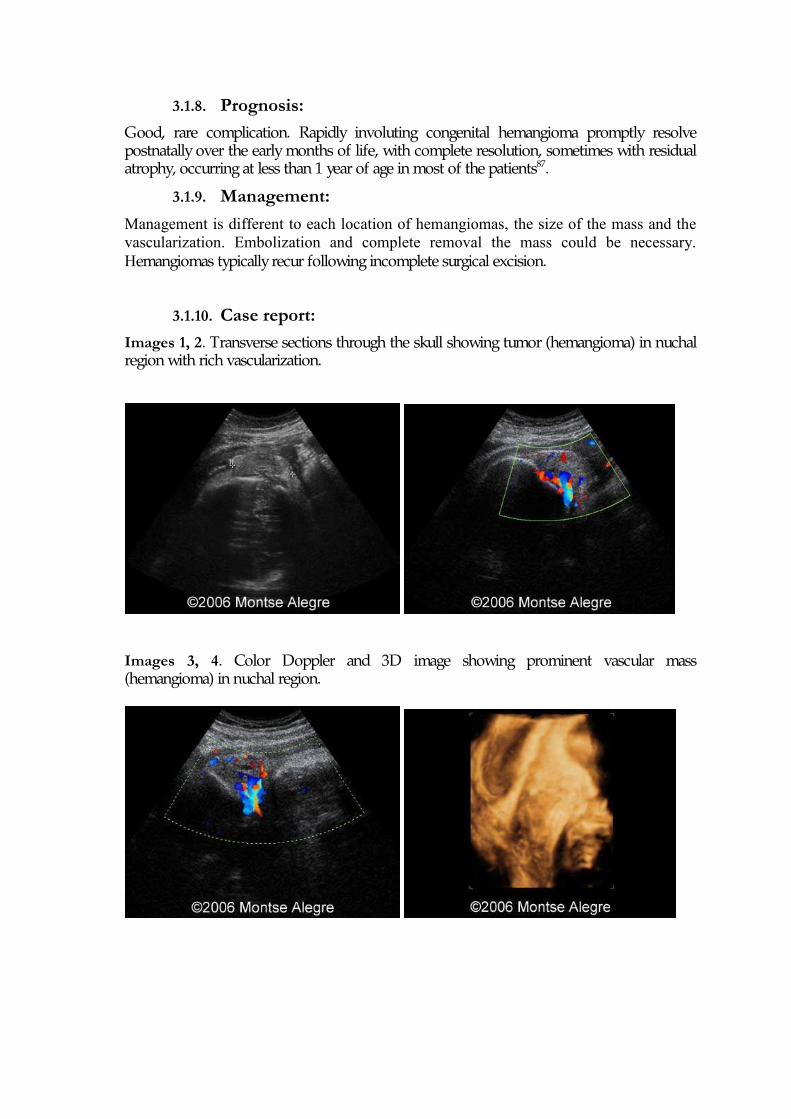
Images 3, 4. Color Doppler and 3D image showing prominent vascular mass (hemangioma) in nuchal region.
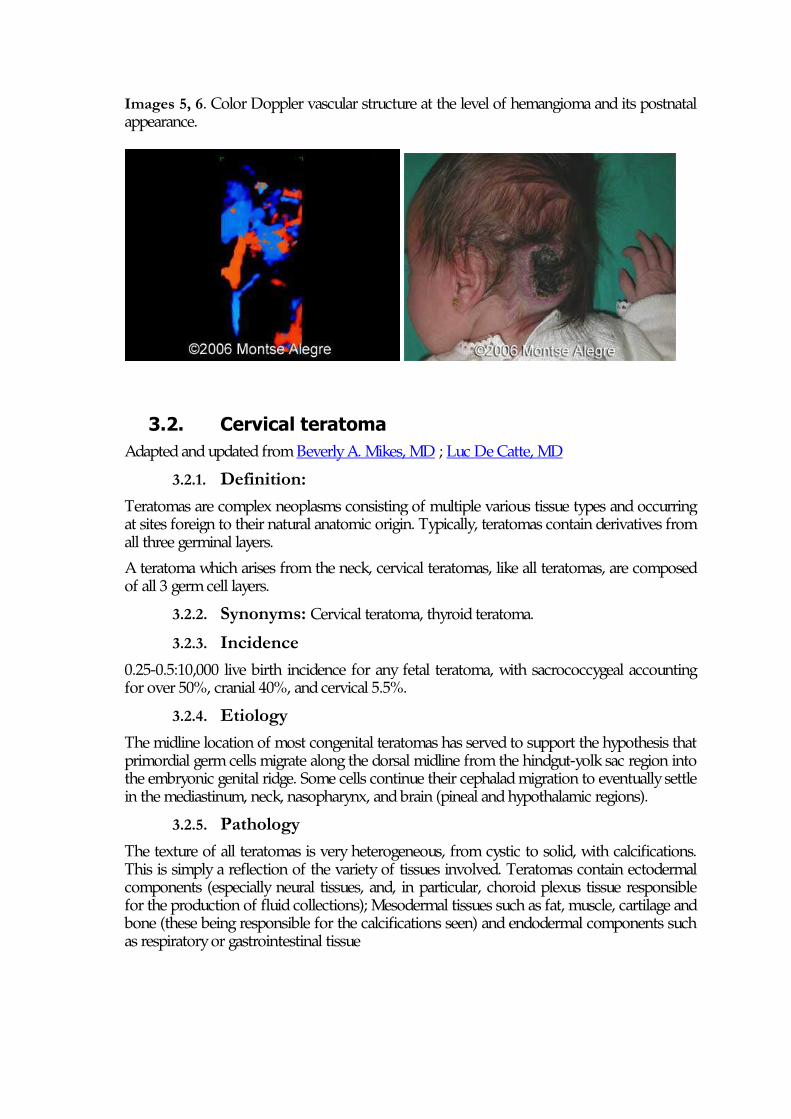
Images 5, 6. Color Doppler vascular structure at the level of hemangioma and its postnatal appearance.
3.2. Cervical teratoma Adapted and updated from Beverly A. Mikes, MD ; Luc De Catte, MD
3.2.1. Definition: Teratomas are complex neoplasms consisting of multiple various tissue types and occurring at sites foreign to their natural anatomic origin. Typically, teratomas contain derivatives from all three germinal layers. A teratoma which arises from the neck, cervical teratomas, like all teratomas, are composed of all 3 germ cell layers.
3.2.2. Synonyms: Cervical teratoma, thyroid teratoma.
3.2.3. Incidence 0.25-0.5:10,000 live birth incidence for any fetal teratoma, with sacrococcygeal accounting for over 50%, cranial 40%, and cervical 5.5%.
3.2.4. Etiology The midline location of most congenital teratomas has served to support the hypothesis that primordial germ cells migrate along the dorsal midline from the hindgut-yolk sac region into the embryonic genital ridge. Some cells continue their cephalad migration to eventually settle in the mediastinum, neck, nasopharynx, and brain (pineal and hypothalamic regions).
3.2.5. Pathology The texture of all teratomas is very heterogeneous, from cystic to solid, with calcifications. This is simply a reflection of the variety of tissues involved. Teratomas contain ectodermal components (especially neural tissues, and, in particular, choroid plexus tissue responsible for the production of fluid collections); Mesodermal tissues such as fat, muscle, cartilage and bone (these being responsible for the calcifications seen) and endodermal components such as respiratory or gastrointestinal tissue
3.2.6. Associated anomalies Associated anomalies are rare; the following have been reported once each: imperforate anus, chondrodystrophia fetalis, hypoplastic left ventricle with pulmonary hypoplasia, cystic fibrosis, metastasis.
3.2.7. Complications: Polyhydramnios, trachea, mandible, cervical vessels and hypoglossal nerve compression.
3.2.8. Sonographic findings: Heteroechogenic mass, from cystic to solid with calcifications. Furthermore, they appear pedunculated as they bulge out of the neck; they are symmetric, unilateral and well delineated. Many will be associated with polyhydramnios resulting from esophageal obstruction.
3.2.9. Prognosis: Depends on the size of the tumor and the tracheal compression.
Malignant degeneration and recurrence are exceptional. Affected fetuses may have growth restriction. Hyperextension of the neck and dystocia are seen at delivery due to malpresentation.
After birth, the immediate danger is respiratory compromise from airway obstruction, but the neck musculature also is abnormally developed and newborns have poor tone. Furthermore. they may have severe reflux and feeding difficulties.
These tumors tend to be large, requiring extensive neck dissection. Even in infants treated surgically, the mortality rate ranges from 9%-17%. Although teratomas are usually nonmalignant, they result in a high mortality of 80%-100%, with 15% of fetuses stillborn.
3.2.10. Differential diagnosis includes: •••• Hamartomas
•••• Hemangioma: homogeneously echogenic or mixed cystic and solid appearence +color flow and pulsed Doppler flow
•••• Cystic hygromas : asymmetric, thin walled, multiseptated cystic masses of the posterolateral aspect of the neck, sporadically echogenic solid components, midline septation, sometimes associated with hydrops.
•••• Goiter: bilobed anterior neck mass adjacent to the midline, solid-mixed-cystic-like appearence, fetal tachycardia, polyhydramnion.
•••• Teratoid cysts
•••• Epignathus
•••• Cervical neural tube defects
•••• Branchial cleft cysts.
3.2.11. Management:
Adequate ventilatory support and surgical excission as soon as possible.
3.2.12. Case report: 3.2.12.1. Case 1:
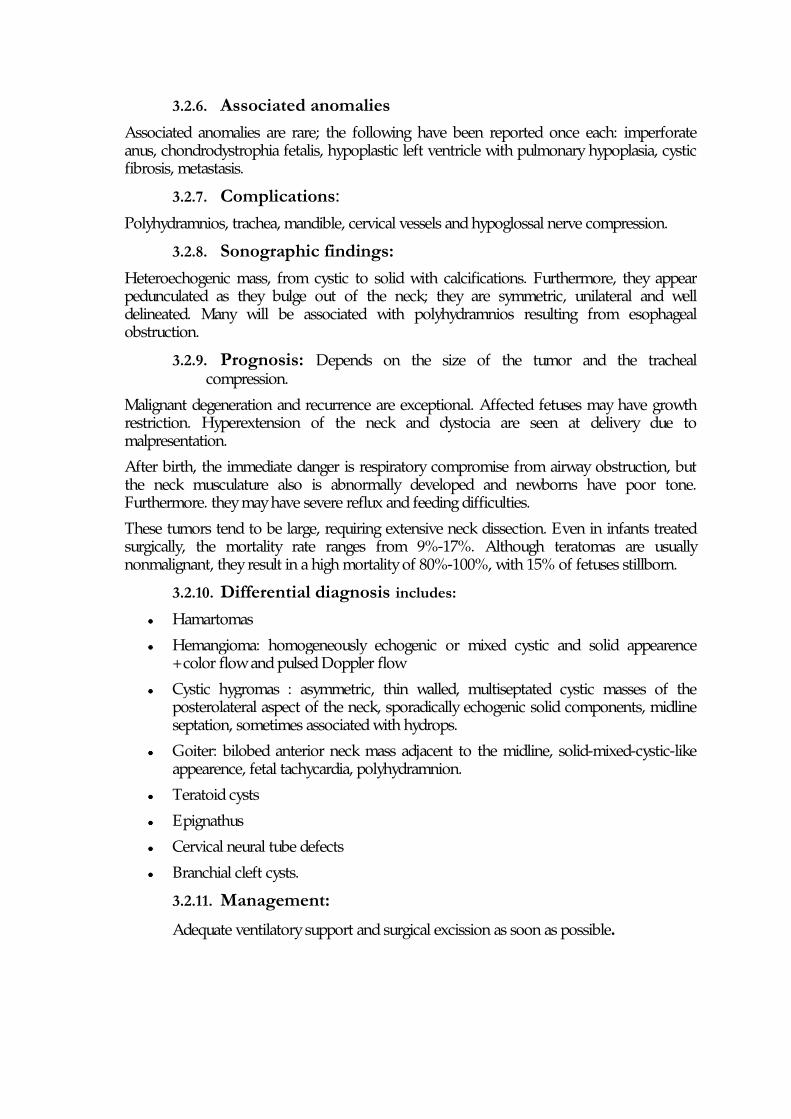
Ultrasound evaluation demonstrated a right sided solid cervical mass emanating from just below the fetal ear and continuing down the side of the fetal neck measuring 2.5 cm. Color flow Doppler demonstrated blood supply from the mass orientating directly off the right carotid. There were no other structural anomalies and no evidence of fetal hydrops. The tumor grew rapidly, about a centimeter a week initially, and evolved over the course of her pregnancy from a solid mass to a large, semi-cystic structure with vascularity only around the periphery.
A diagnosis of immature teratoma Grade III, with no elements of yolk sac present was determined on pathological examination. The infant did exceptionally well post-operatively, and was discharged home on postoperative day fifteen. Images 1-4: 23 weeks, solid, encapsulated cervical mass (3-4 cm in diameter), with upper margin just below the ear and located along the side of the neck.
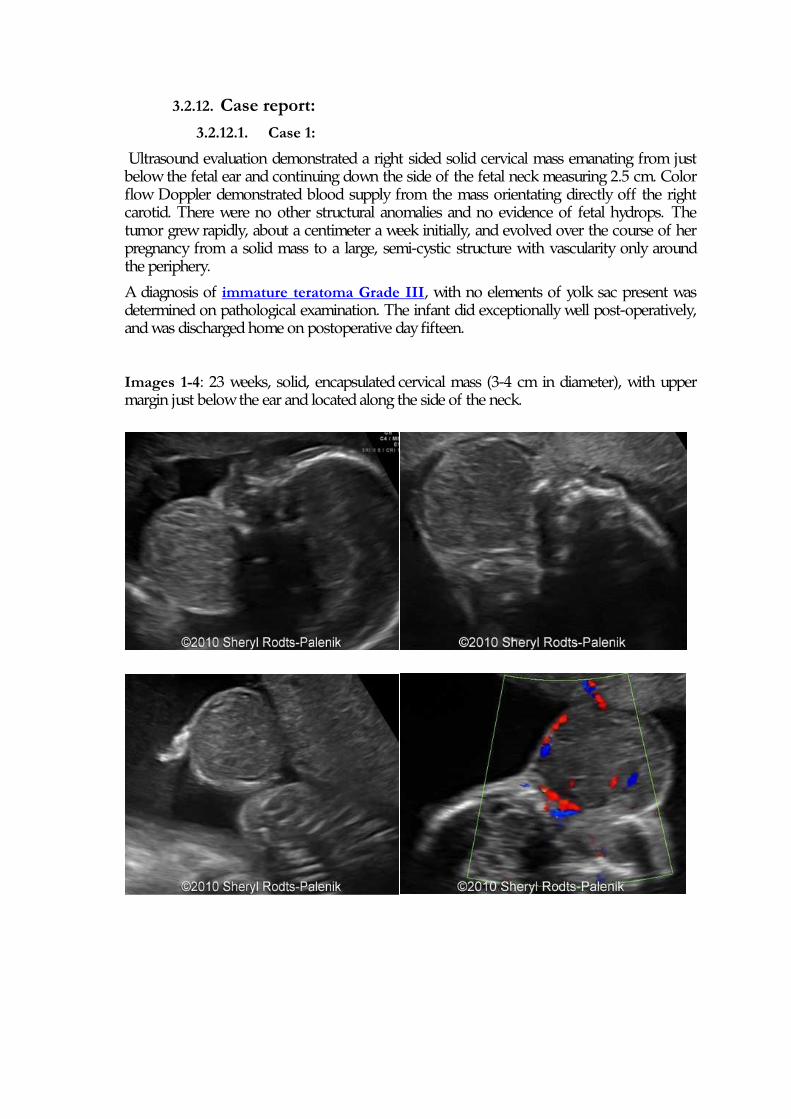
Images 5-6: 25 weeks, Doppler imaging of the tumor mass showing blood supply straight from the carotid artery.
Images 7,8: 34 weeks, note the size of the tumor and semi-cystic structure.
Images 9,10: 37 weeks, delivery via cesarean section, note the large mass on the right side of the fetal neck.
3.2.12.2. Case 2:
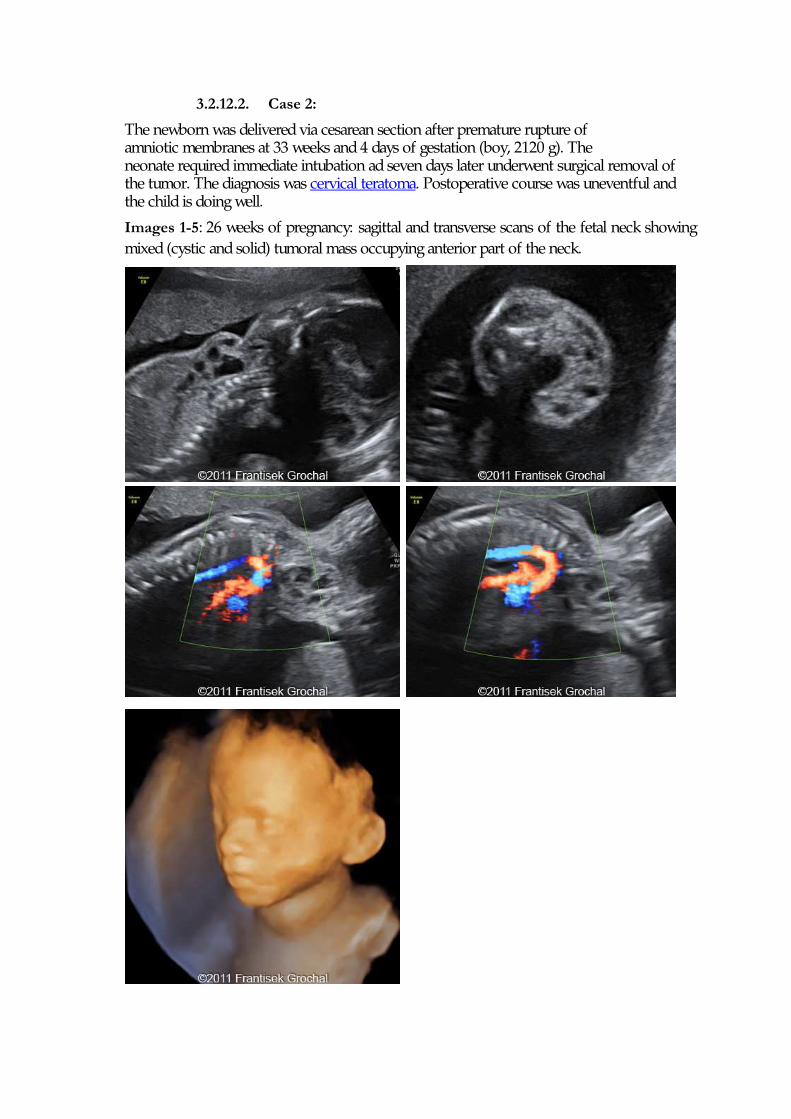
The newborn was delivered via cesarean section after premature rupture of amniotic membranes at 33 weeks and 4 days of gestation (boy, 2120 g). The neonate required immediate intubation ad seven days later underwent surgical removal of the tumor. The diagnosis was cervical teratoma. Postoperative course was uneventful and the child is doing well.
Images 1-5: 26 weeks of pregnancy: sagittal and transverse scans of the fetal neck showing mixed (cystic and solid) tumoral mass occupying anterior part of the neck.
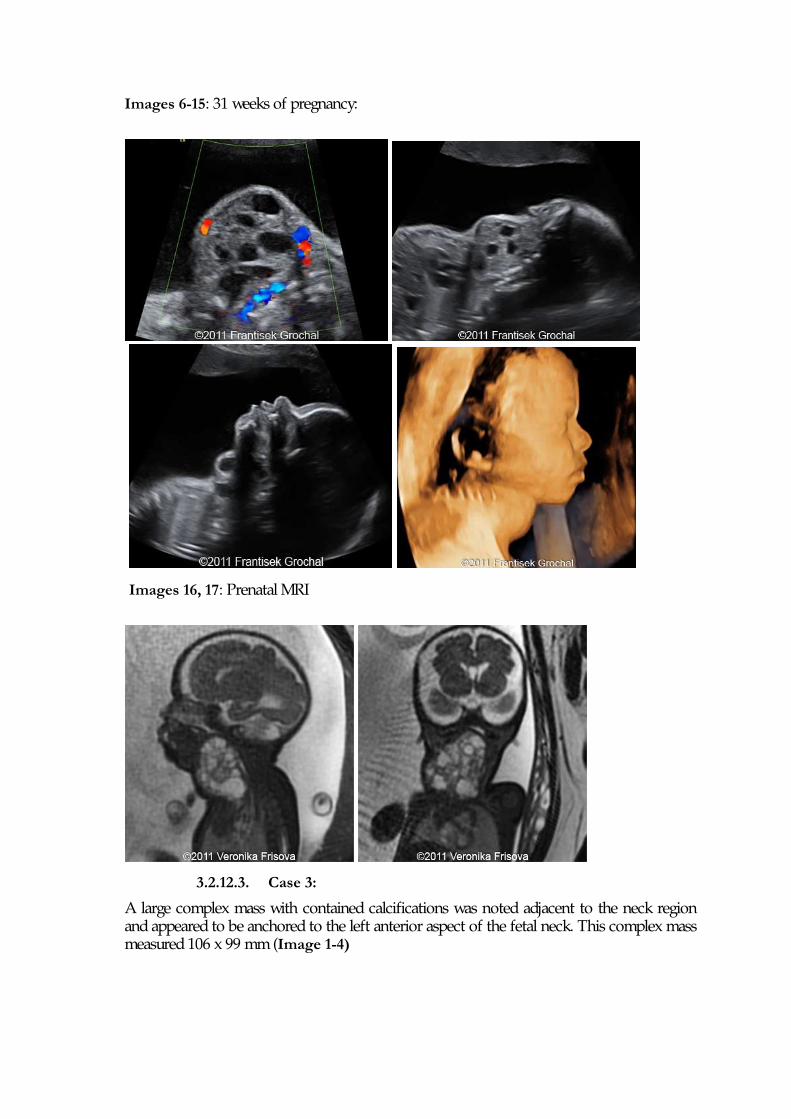
Images 6-15: 31 weeks of pregnancy:
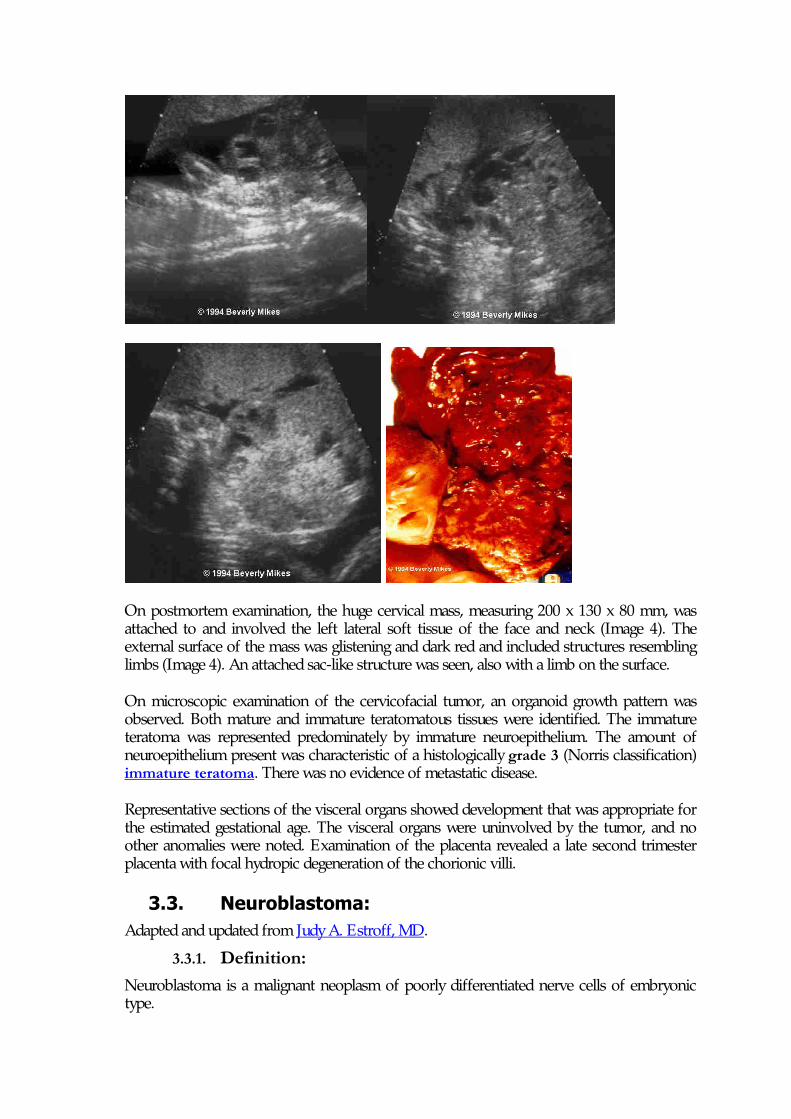
Images 16, 17: Prenatal MRI
3.2.12.3. Case 3:
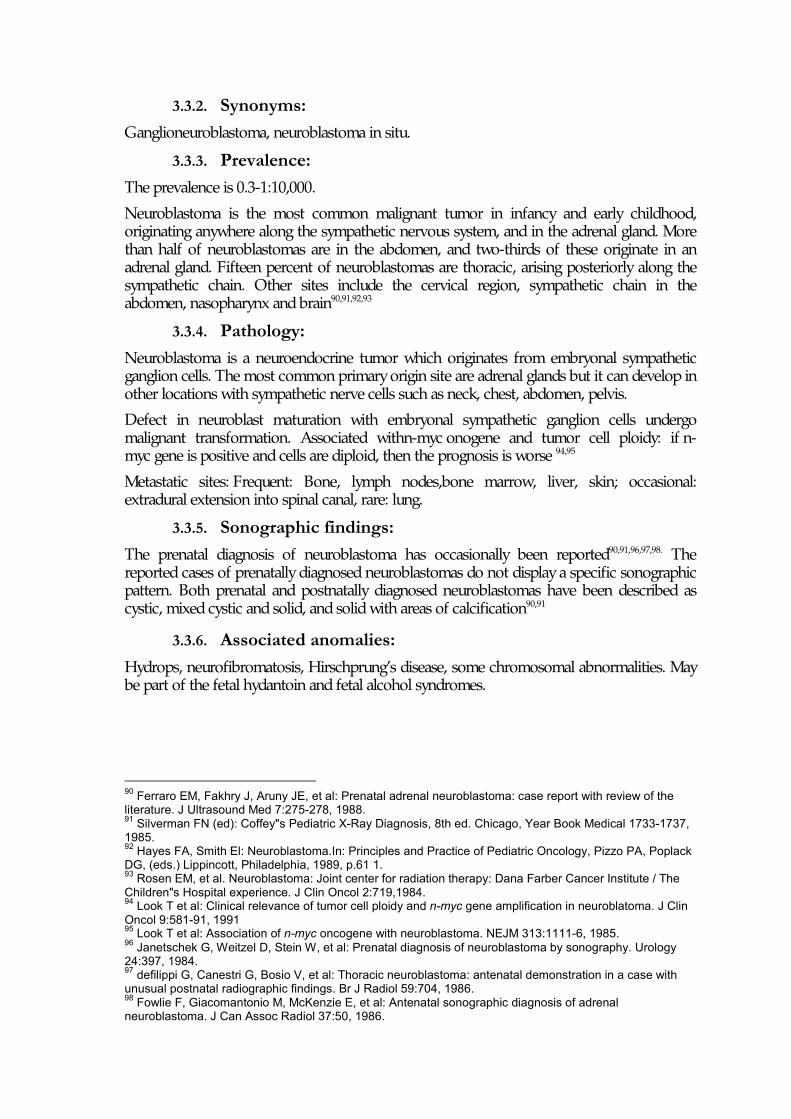
A large complex mass with contained calcifications was noted adjacent to the neck region and appeared to be anchored to the left anterior aspect of the fetal neck. This complex mass measured 106 x 99 mm (Image 1-4)
On postmortem examination, the huge cervical mass, measuring 200 x 130 x 80 mm, was attached to and involved the left lateral soft tissue of the face and neck (Image 4). The external surface of the mass was glistening and dark red and included structures resembling limbs (Image 4). An attached sac-like structure was seen, also with a limb on the surface.
On microscopic examination of the cervicofacial tumor, an organoid growth pattern was observed. Both mature and immature teratomatous tissues were identified. The immature teratoma was represented predominately by immature neuroepithelium. The amount of neuroepithelium present was characteristic of a histologically grade 3 (Norris classification) immature teratoma. There was no evidence of metastatic disease.
Representative sections of the visceral organs showed development that was appropriate for the estimated gestational age. The visceral organs were uninvolved by the tumor, and no other anomalies were noted. Examination of the placenta revealed a late second trimester placenta with focal hydropic degeneration of the chorionic villi.
3.3. Neuroblastoma: Adapted and updated from Judy A. Estroff, MD.
3.3.1. Definition: Neuroblastoma is a malignant neoplasm of poorly differentiated nerve cells of embryonic type.
3.3.2. Synonyms: Ganglioneuroblastoma, neuroblastoma in situ.
3.3.3. Prevalence: The prevalence is 0.3-1:10,000.
Neuroblastoma is the most common malignant tumor in infancy and early childhood, originating anywhere along the sympathetic nervous system, and in the adrenal gland. More than half of neuroblastomas are in the abdomen, and two-thirds of these originate in an adrenal gland. Fifteen percent of neuroblastomas are thoracic, arising posteriorly along the sympathetic chain. Other sites include the cervical region, sympathetic chain in the abdomen, nasopharynx and brain90,91,92,93
3.3.4. Pathology: Neuroblastoma is a neuroendocrine tumor which originates from embryonal sympathetic ganglion cells. The most common primary origin site are adrenal glands but it can develop in other locations with sympathetic nerve cells such as neck, chest, abdomen, pelvis.
Defect in neuroblast maturation with embryonal sympathetic ganglion cells undergo malignant transformation. Associated withn-myc onogene and tumor cell ploidy: if n-myc gene is positive and cells are diploid, then the prognosis is worse 94,95
Metastatic sites: Frequent: Bone, lymph nodes,bone marrow, liver, skin; occasional: extradural extension into spinal canal, rare: lung.
3.3.5. Sonographic findings: The prenatal diagnosis of neuroblastoma has occasionally been reported90,91,96,97,98. The reported cases of prenatally diagnosed neuroblastomas do not display a specific sonographic pattern. Both prenatal and postnatally diagnosed neuroblastomas have been described as cystic, mixed cystic and solid, and solid with areas of calcification90,91
3.3.6. Associated anomalies: Hydrops, neurofibromatosis, Hirschprung’s disease, some chromosomal abnormalities. May be part of the fetal hydantoin and fetal alcohol syndromes.
90 Ferraro EM, Fakhry J, Aruny JE, et al: Prenatal adrenal neuroblastoma: case report with review of the literature. J Ultrasound Med 7:275-278, 1988. 91 Silverman FN (ed): Coffey"s Pediatric X-Ray Diagnosis, 8th ed. Chicago, Year Book Medical 1733-1737, 1985. 92 Hayes FA, Smith El: Neuroblastoma.In: Principles and Practice of Pediatric Oncology, Pizzo PA, Poplack DG, (eds.) Lippincott, Philadelphia, 1989, p.61 1. 93 Rosen EM, et al. Neuroblastoma: Joint center for radiation therapy: Dana Farber Cancer Institute / The Children"s Hospital experience. J Clin Oncol 2:719,1984. 94 Look T et al: Clinical relevance of tumor cell ploidy and n-myc gene amplification in neuroblatoma. J Clin Oncol 9:581-91, 1991 95 Look T et al: Association of n-myc oncogene with neuroblastoma. NEJM 313:1111-6, 1985. 96 Janetschek G, Weitzel D, Stein W, et al: Prenatal diagnosis of neuroblastoma by sonography. Urology 24:397, 1984. 97 defilippi G, Canestri G, Bosio V, et al: Thoracic neuroblastoma: antenatal demonstration in a case with unusual postnatal radiographic findings. Br J Radiol 59:704, 1986. 98 Fowlie F, Giacomantonio M, McKenzie E, et al: Antenatal sonographic diagnosis of adrenal neuroblastoma. J Can Assoc Radiol 37:50, 1986.
3.3.7. Differential diagnosis: Adrenal site: renal duplex anomaly or tumor, adrenal cyst or hemorrhage are less likely. Extra-adrenal site: solid mass of lung, pelvis, head or neck.
3.3.8. Prognosis: Better with younger age and lower stage at diagnosis. Better with primary thoracic site of tumor. Some may mature into ganglioneuroma.
More than half of patients are less than two years of age at diagnosis. Seventy-five percent of tumors are discovered prior to four years of age. The prognosis ranges from over 90% survival if discovered in patients under one year of age, to less than 10% survival when discovered in older children90-93 . Accurate early diagnosis is crucial, as the best prognosis is in the youngest patients.
3.3.9. Recurrence risk: unknown.
3.3.10. Management: Evans staging system: Stage I: Tumor confined to the organ or structure of origin. Stage II: Tumor extending in continuity beyond the organ or structure of origin but not crossing the midline. Regional lymph nodes on homolateral side may be involved. Stage III: Tumor extending in continuity beyond the midline with or without positive regional nodes. Stage IV: Distant metastases. Stage lV-S: Stage I-II primaries with metastases to liver, skin and/or bone marrow (not bone). Almost all stage IV-S are infants. Stage I: Surgical resection; no other treatment. Stage II: Surgical resection in infants. Older children: chemotherapy with or without added radiation. Stage III & IV. Surgical debulking, then chemotherapy and radiation. Bone marrow transplant in high risk patients (older patients and those with n-myc amplification).
3.3.11. Case report:
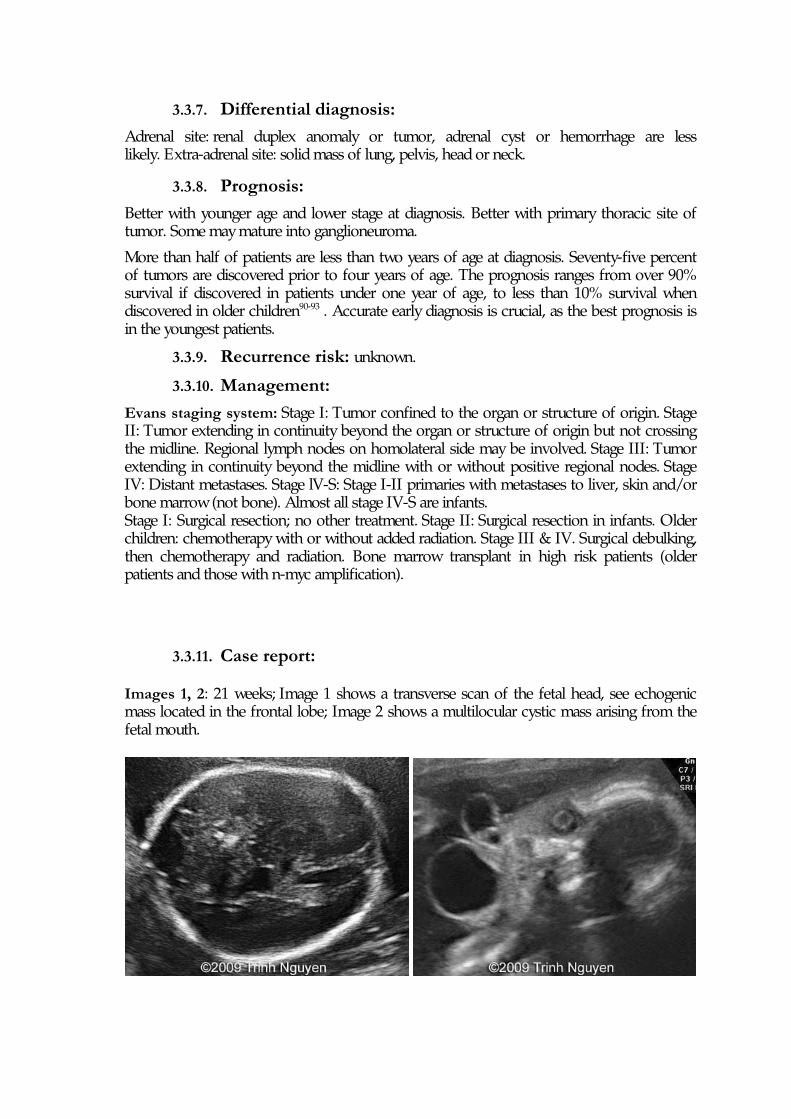
Images 1, 2: 21 weeks; Image 1 shows a transverse scan of the fetal head, see echogenic mass located in the frontal lobe; Image 2 shows a multilocular cystic mass arising from the fetal mouth.
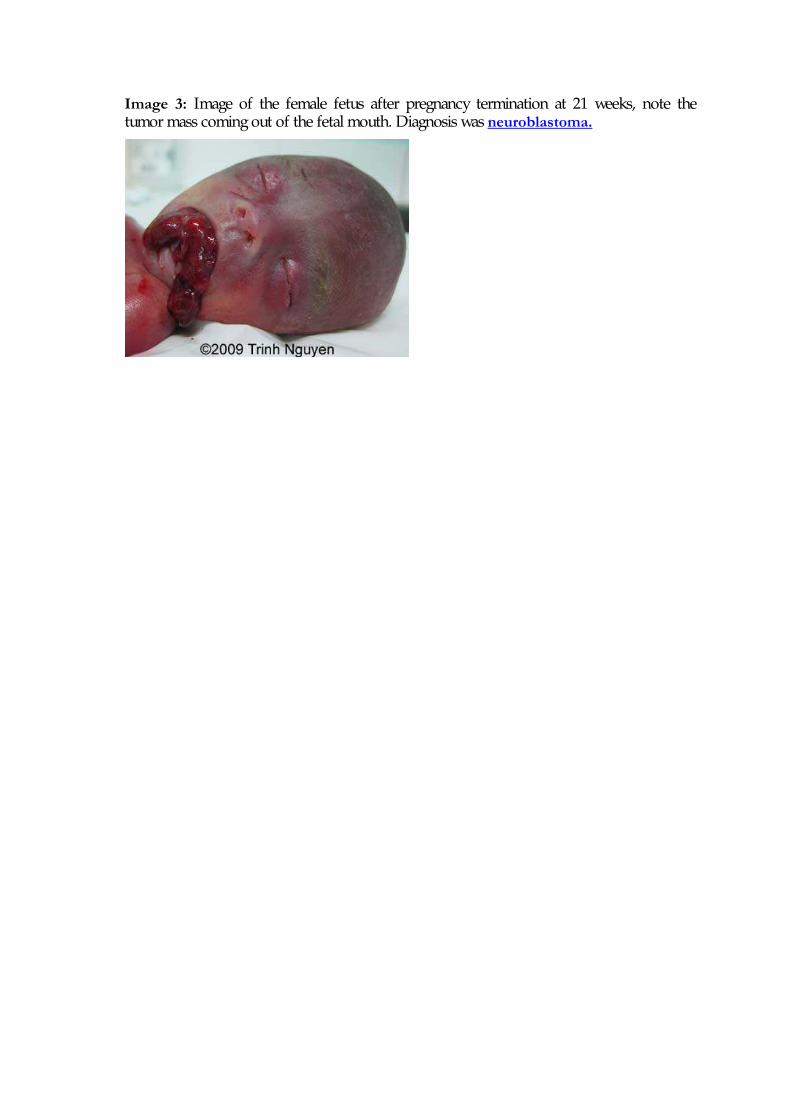
Image 3: Image of the female fetus after pregnancy termination at 21 weeks, note the tumor mass coming out of the fetal mouth. Diagnosis was neuroblastoma.
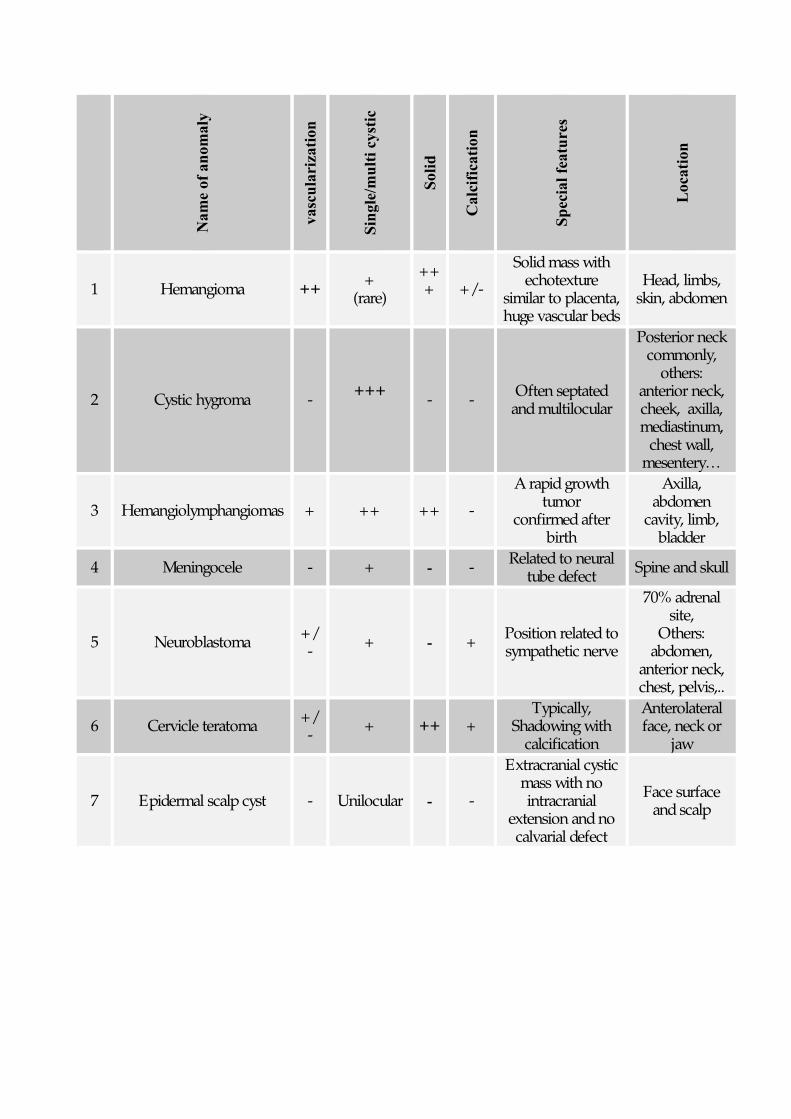
Name of anomaly
vascularization
Single/multi cystic
Solid
Calcification
Special features
Location
1 Hemangioma ++ + (rare)
+++
+/-
Solid mass with echotexture
similar to placenta, huge vascular beds
Head, limbs, skin, abdomen
2 Cystic hygroma - +++ - - Often septated
and multilocular
Posterior neck commonly,
others: anterior neck, cheek, axilla, mediastinum,
chest wall, mesentery…
3 Hemangiolymphangiomas + ++ ++ -
A rapid growth tumor
confirmed after birth
Axilla, abdomen
cavity, limb, bladder
4 Meningocele - + - - Related to neural tube defect Spine and skull
5 Neuroblastoma +/- + - + Position related to
sympathetic nerve
70% adrenal site,
Others: abdomen,
anterior neck, chest, pelvis,..
6 Cervicle teratoma +/- + ++ +
Typically, Shadowing with
calcification
Anterolateral face, neck or
jaw
7 Epidermal scalp cyst - Unilocular - -
Extracranial cystic mass with no intracranial
extension and no calvarial defect
Face surface and scalp



![Evaluation of hepatic cystic lesions...treatment[5,6]. Currently, clinicians must also be aware of changes in the epidemiology of certain hepatic cystic lesions. Echinococcosis has](https://static.fdocuments.net/doc/165x107/5f0882797e708231d4225d6c/evaluation-of-hepatic-cystic-lesions-treatment56-currently-clinicians-must.jpg)

![Pancreatic Cytopathology Cystic Lesions Cytol… · Cystic Lesions Cystic Lesions Of The Pancreas [Practical Issues] ... 1-2% of all pancreatic tumors LMP epithelial tumor of uncertain](https://static.fdocuments.net/doc/165x107/5f6d9c61a7374f61f46d815c/pancreatic-cytopathology-cystic-lesions-cytol-cystic-lesions-cystic-lesions-of.jpg)












