Course: - CatsTCMNotescatstcmnotes.com/downloads/Biomedical Treatment of D… · Web...
23
Cours e: Biomedical Diagnostics 2 Date: August 3, 2010 Class #: 3 – Hypertension and Vascular Diseases Hypertension (Cont’d from Class 2) Should do BP check at least 1ce per year. Remember that African Americans are more likely to get HTN. 50million people have this disease, but 30% are unaware of it. Even so, only 50% seek treatment and 25% are actually controlling it. Sheesh. History of high BP should be proven prior to starting on meds, but most docs will start ppl on it quicker than that anyhow due to fear of liability. Stupid law crap. Probably responsible for more death than anything else. Use this chart to determine the magic numbers…135/85 is about as much as you can push the envelope and still have healthy BP. Height, weight, BMI will give you a clue as to whether intervention is Biomedical Treatment of Disease 2 – Class 3 - Summer 2010 www.CatsTCMNotes.com Page 1 of 23 Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Transcript of Course: - CatsTCMNotescatstcmnotes.com/downloads/Biomedical Treatment of D… · Web...

Course: Biomedical Diagnostics 2 Date: August 3, 2010Class #: 3 – Hypertension and Vascular Diseases
Hypertension(Cont’d from Class 2)
Should do BP check at least 1ce per year. Remember that African Americans are more likely to get HTN. 50million people have this disease, but 30% are unaware of it. Even so, only 50% seek treatment and 25% are actually controlling it. Sheesh.
History of high BP should be proven prior to starting on meds, but most docs will start ppl on it quicker than that anyhow due to fear of liability. Stupid law crap. Probably responsible for more death than anything else.
Use this chart to determine the magic numbers…135/85 is
about as much as you can push the envelope and still have healthy BP.
Height, weight, BMI will give you a clue as to whether intervention is needed. Here’s what a physical exam should include when HTN is an issue:
Vital Stat: height, weight, and waist circumference
Funduscopic exam
Retinopathy reflects damage to vessels and indicates blockage and damage in other vessels as well.
Carotid auscultation. Listen for bruits indicating blockage of or aneurysm of vessels.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 1 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

Jugular venous pulsationIndicates the return blood to the heart is blocked and the pressure in the veins is higher than it should be.
Thyroid gland (enlargement) Overactive and underactive thyroid can cause HTN.
Cardiac auscultationFirst heart sound will be loud with hypertension. If heart failure, might hear a 3rd heart sound.
Chest auscultation abdominal exam (bruits, masses, pulsations) Might hear crackling and other sounds in the lungs since this goes along with heart failure. Listen for bruit especially in the major arteries in the trunk.
Exam of lower extremitiesaggressive atherosclerosis…might also find absent or weak pulses due to PAD.
Routine labs include Urinalysis – protein in the urine, presence of sugars, protein casting suggesting leaky
glomerulus. Repeated sore throat might pass to kidneys and attack glom/neph Complete blood count (CBC). Chronic renal failure, could be anemic Electrolytes (potassium, calcium). In cureable BP low K+ could indicate adrenal gland
tumor. Kidney failure will also have high K+. High calcium indicates kidney stones, which damages kidneys and can cause HTN. If there is also a familial connection or history of this is more cause for concern. May just have too much calcium in the diet.
Creatinine. 1.2 – 1.3 max. If over 1.5 suggests 25% loss of kidney fnx. 4.5 = 50% kidney non functioning, 8.5% = need dialysis. When the BP stays high for a long time = kidney damage and this tests shows that.
Glucose Fasting lipids 12-lead electrocardiogram
Normal: recheck in 2 years (see Comments)
1. Prehypertension: SBP 120–139 or DBP 80–89
Prehypertension: recheck in 1 year
2. Stage 1 hypertension: SBP 140–159 or DBP 90–99
Stage 1 hypertension: confirm within 2 months
2 separate office visits)
Stage 2 hypertension: evaluate or refer to source of care within 1 month (evaluate and treat immediately if BP > 180/110)
4. Perform physical exam and routine labs.a
3. Stage 2 hypertension: SBP >160 or DBP>100 (based on average of 2 measurements on different days)
5. Pursue secondary causes of hypertension.6. Treatment goals are for BP < 140/90, unless diabetes or renal disease present (< 130/80).7. Ambulatory BP monitoring is a better (and independent) predictor of cardiovascular outcomes
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 2 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

compared with office visit monitoring; and covered by Medicare when evaluating white-coat hypertension.
Mean arterial pressure should be 90-100.
How do you treat the Prehypertension group? No real treatment. They can modify lifestyle and keep it under the skeery numbers. We really covered this last time, but I guess we’re reviewing. …
Primary HypertensionPrimary Hypertension means there’s no other cause found. Sometimes you’ll see the word “idiopathic” associated with primary htn. Here’s what contributes to it:
Genetic factors Obesity Salt intake – should be no more than about 2g per day (RDA says 2,400mg), but most of us get
around 10g. Sheesh! Sympathetic nervous system hyperactivity
Fight or flight response is way too on-call. Abnormal cardio-vascular system development Low renin-antiotensin levels/activity Alcohol
2 drinks lowers the pressure, but if you consume more the BP increases. Cigarette smoking
Nicotine constricts the blood vessels which increases the arterial pressure Polycythemia
Polycythemia is a condition in which there is an increase in the proportion of blood volume that is occupied by red blood cells, which is measured as hematocrit level.
Secondary Causes of HypertensionIf someone is not responding to drug therapy, you start looking for another cause for their hypertension. Here are some more common causes of secondary htn.
Pheochromocytoma Pheochromocytoma is a vascular tumor of the adrenal gland; hypersecretion of epinephrine results in intermittent or sustained hypertension. Look for labile or paroxysmal hypertension accompanied by sweats, headaches, and palpitations. Some pheochromocytoma patients have café au lait spots. These peeps may be in hypertension crisis.
Renovascular DiseaseRenal Artery stenosis or kinking affects approximately 2% of all hypertension patients. Click here to read an NIH article about it. This condition affects younger hypertension patients less than 20 years old. Conversely, renal patients will have hypertension! If you have a kidney patient, look for hypertension.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 3 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

Renal artery stenosis results from a condition called fibromuscular hyperplasia (most common in females over 50). This is a thickening of the artery by fibrosis and/or muscular hyperplasia. Usually involved the renal arteries which causes stenosis of the artery in several locations which in turn pushes up the arterial pressure and results in hypertension.
Both kinking and stenosis of these lead to excessive renin release. Need a refresher in how renin and angiotensin regulate the blood pressure? I did. Click here.
Look for renal artery stenosis or kinking if you have a hypertension patient who is too young to be a hypertension patient, when hypertension patients are resistant to drugs, when you hear epigastric/renal bruits upon auscultation, if your patients have Peripheral Artery Disease, or when renal function falters after you prescribe ACE inhibitors. How do you test? Radio renography, duplex ultrasound, MRA/CT angio, renal arteriograph.
APKD-autosomal dominant polycystic kidney disease(abdominal or flank masses)
Cushing’s Syndrome Cushing’s syndrome is a hormonal disorder caused by prolonged exposure of the body’s tissues to high levels of the hormone cortisol. Sometimes called hypercortisolism, Cushing’s syndrome is relatively rare and most commonly affects adults aged 20 to 50. People who are obese and have type 2 diabetes, along with poorly controlled blood glucose—also called blood sugar—and high blood pressure, have an increased risk of developing the disorder.
Signs and symptoms of Cushing’s syndrome vary, but most people with the disorder have upper body obesity, a rounded face, increased fat around the neck, and relatively slender arms and legs. Children tend to be obese with slowed growth rates. Other signs appear in the skin, which becomes fragile and thin, bruises easily, and heals poorly. Purple or pink stretch marks may appear on the abdomen, thighs, buttocks, arms, and breasts. The bones are weakened, and routine activities such as bending, lifting, or rising from a chair may lead to backaches and rib or spinal column fractures. Women with Cushing’s syndrome usually have excess hair growth on their face, neck, chest, abdomen, and thighs. Their menstrual periods may become irregular or stop. Men may have decreased fertility with diminished or absent desire for sex and, sometimes, erectile dysfunction. Other common signs and symptoms include severe fatigue, weak muscles, high blood pressure, high blood glucose, increased thirst and urination, irritability, anxiety, or depression, a fatty hump between the shoulders.
Of course, that high blood pressure thing is why we’re talking about this in the first place. 75-85% of Cushing’s Syndrome/Disease patients have hypertension. Why? Because the levels of renin and angiotensin increase!
Guess what else: steroid usage can actually cause Cushing’s because a glucocorticoid excess = Cushing’s. Isn’t that fun news for competitive weight lifters, football players, and A-Rod?
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 4 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Primary hyperaldosteronism High aldosterone levels can cause high blood pressure and low potassium levels; low potassium levels may cause weakness, tingling, muscle spasms, and periods of temporary paralysis. Aldosterone, a hormone produced and secreted by the adrenal glands, signals the kidneys to excrete less sodium and more potassium. Aldosterone production is regulated partly by corticotropin (secreted by the pituitary gland) and partly through the renin-angiotensin-aldosterone system
Hyperparathyroidism (hypercalcemia) A disorder of the parathyroid glands, also called parathyroids. Can be primary or secondary in nature. One or more enlarged, overactive parathyroid glands secretes too much parathyroid hormone (PTH). In secondary hyperparathyroidism, a problem such as kidney failure causes the parathyroids to be overactive. Regardless, the result is a a high level of serum calcium.
Renal parenchymal disease (elevated serum creatinine, abnormal urinalysis),
Poor response to drug therapySystolicBP > 180 or DiastolicBP > 110 mm Hg, or sudden onset of hypertension.
Other causes of secondary hypertension: Estrogen Acromegaly Hyperthyroidism hypothyroidism DRUGS: cyclosporine and NSAIDs
Like 2+ years of constant ibuprofen intake. Shit, man.
Some specific disease categories associated with (but not necessarily causing) hypertension: Sleep apnea
If you snore, you’re likely to get sleep apnea. If you have HTN and apnea, you’re highly likely to stroke out at some point. Nice.
Drugs. Some drugs induce or are related to HTN
Chronic kidney disease Primary aldosteronism Reno-vascular disease Long-term corticosteroid therapy Cushing's syndrome
Which is related to corticosteroid levels also Pheochromocytoma
Pheochromocytoma is a vascular tumor of the adrenal gland; hypersecretion of epinephrine results in intermittent or sustained hypertension
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 5 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Coarctation of the aortaAortic coarctation is a narrowing of part of the aorta (the major artery leading out of the heart). It is a type of birth defect. Coarctation means narrowing. Check out this graphic for a good visual.
Thyroid or parathyroid diseaseHere’s an interesting summary. To flesh out what was touched on above.
Complications of hypertension Excess morbidity and mortality related to hypertension
Risk doubles for each 6 mm Hg increase in diastolic blood
Cardiac Complications – Left Ventricular Hypertrophy congestive heart failure, ventricular arrhythmias (vtac/vfib), myocardial ischemia, myocardial hypertrophy which reduces ability of heart to pump blood (use of steroids will do this too) and sudden death.
Cerebrovascular Disease and Dementia - hemorrhagic and ischemic stroke The longer the bp is high, the higher this risk. The brain gets a lot of silent infarcs or lacunary infarcs. These don’t cause major strokes, but if happen regularly will find that after age 75 you see lots of holes in the brain upon scanning it.
Higher incidence of subsequent dementia of both vascular and Alzheimer types markedly reduced by antihypertensive therapy
Hypertensive Renal Disease – renal insufficiency
i.e., kidney failure. hypertensive nephropathy more common in blacks associated with Diabetes Mellitus Benefits with ACE inhibitor therapy
Aortic dissectionAorta stretches out – blood travels between the layers of the blood vessels. Yow.
Increased atherosclerosisHardened arteries.
Symptoms of Complications of Hypertension Remember this disease is called a silent killer. It’s complications differ depending on what organ/s have suffered as a result. Some things you might see (but not all things you might see) resulting from damage due to hypertension:
HeartAcute failure, MI, left ventricular enlargement/hypertrophy
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 6 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

BrainWake with throbbing headache. Could be tumor or persistent htn. Or perpetual hangover! Usually back of the head headache, will be throbbing. Hypertensive encaphalopathy when diastolic above 120 – dopey, confused, n/v, visual flashes, somnolence
KidneysKidney failure with the associated bad numbers mentioned previously. Pt might wake up at 3am to pass urine. Mandyam says you shouldn’t wake to pee in the night. What? Crazy man. Does indicate more fluid returning to the Kidneys at night. Specific gravity of urine will also vary – may be extra concentrated or extra diluted. Lab work shows elevated numbers. Urine will often have more solid particles.
Eyes and peripheral arteriesVisual disturbances/loss of acuity, etc. TIA in eyes or periphery. Ischemia, leg cramps, temp paralysis. Why do eye doctors look in your eyes at the retinal arteries? They often show the damage first before it affects other body parts. Yet another reason to go to the eye doctor regularly.
Primary Lab work-up (for all patients, but specifically for hypertensive patients) Urinalysis and sediment review
(identifies possible renal disease or end-organ dysfunction)
Basic chemistry including potassium, fasting glucose, blood urea nitrogen, and creatinine (evaluates for renal disease; low or low-normal potassium may be seen in hyperaldosteronism; fasting glucose can assess for diabetes)
Complete blood cell count (evaluates for polycythemia, which can cause secondary hypertension)
Lipid panel(risk stratification for patients with dyslipidemia)
Electrocardiogram (risk stratification in patients with coronary artery disease; evaluate for left ventricular hypertrophy. Look for the funky rhythms in the ECG. Should come with a report keying you in to the disease.
Goal of all this testing: Establish diagnosis Stage that disease based on the classing system to help with mgmt plan Rule out 2ndary htn Identify what has been damaged, what organs to help out. Identify other risk factors that can be modified.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 7 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

Management of Hypertension
Stage 1 hypertension come with debate….do you impose those meds and stuff on them or not? Encourage them to behave and watch their lifestyle…which they probably won’t because we’re Americans and would rather take a damn pill. We’re idiots mostly.
Management of hypertension without drugsOK, so let’s say them comply and don’t want to take the damn pill. They can do the following. These are pretty fundamental changes to make:
DASH diet and weight reduction Reduced alcohol consumption (2 drink max…which also reduces those DUI’s ) Reduced salt intake Gradually increase activity levels
The goals of treatment look like this: Diabetic patients, CKD, should be lower than most because their kidneys and other organs are
already compromised. Pressure should < 130/80 mm Hg Non-diabetics should have a pressure of <140/90 max
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 8 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Management of hypertension with drugsHTN can indeed be controlled with drugs, but bear in mind there are long-term adverse consequences of drug therapy – β blockers and thiazide diuretics, etc. Pulse should be 70-76 and no lower for patients on these meds. Lower and the doc should review what the heck is going on. Thiazides can cause low K+, uric acid numbers. Statins can significantly improve outcomes in DM/Post MI (total and LDL cholesterol levels of < 194 mg/dL and < 116 mg/dL ). 200 – 240 TC numbers can be managed by diet.
DiureticsDiruretics can control about 50% of all hypertension problems. Diuretics include the following:
Hydrochlorothiazides (also abbreviated HCTZ)This is a thiazide class of diuretic. It works by inhibiting the kidneys' ability to retain water. It inhibits the kidney’s ability to sodium reabsorption in the DCT (distal convoluted tube. (They also increase the reabsorption of calcium.) This reduces the volume of the blood, decreasing blood return to the heart and thus cardiac output and, by other mechanisms, is believed to lower peripheral vascular resistance. It’s sometimes used in combination with other anti-hypertensives.
HCTZ’s include Esidrix® and Hydro-Diuril®. They are the cheapest form of control – about .25$ day.
Loop diuretics are diuretics that act on the ascending loop of Henle in the kidney. They are primarily used to treat hypertension and edema often due to congestive heart failure or renal insufficiency. While thiazide diuretics are more effective in patients with normal kidney function, loop diuretics are more effective in patients with impaired kidney function.
Loop diuretics include ethacrynic acid (Edecrin®) Furosemide (Lasix®). You move to these diuretics if the thiazides don’t work. These are potassium losers though, so they require more monitoring. Potassium loss causes cramps in the legs, weakness, etc. Patients might be able to counteract this effect with diet. Docs may switch them to K+ sparing diuretics instead. In addition to loss of K+, these can cause low levels of Mg2+, Ca2+, and Na+. They can also cause high levels of uric acid (and resulting gout) as well as high levels of glucose.
Aldosterone Receptor BlockersThese are used in cases where the aldosterone/renin/angiotensin system is responsible for high blood pressure. These are also called Aldosterone Receptor Antagonists. These drugs are marketed as Amiloride (Midamor®) and Spironolactone (Aldactone®). They are potassium sparing diuretics preventing the absorption of salt in the kidneys. Patients on potassium sparing diuretics should watch potassium consumption in the diet.
Beta (β) blockersUsed in the management of cardiac arrhythmias, cardioprotection after myocardial infarction (heart attack), as well as hypertension control. They diminish the effects of epinephrine and other
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 9 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

stress hormones. That’s the up-side. The downside is that they can cause heart failure, aggravate respiratory problems, produce nightmares, significantly slow heart rate causing bradycardia, exacerbate bronchospasms, cause AV block, produce nasal congestion, result in Raynaud's phenomenon, increase triglyceride levels and decrease HDL (good cholesterol) levels. Drugs in this class include:
Acebutolol(Sectral®) Atenolol(Tenormin®) Metoprolol(Lopressor®) Pindolol (Visken®) Propranolol (Inderal®)
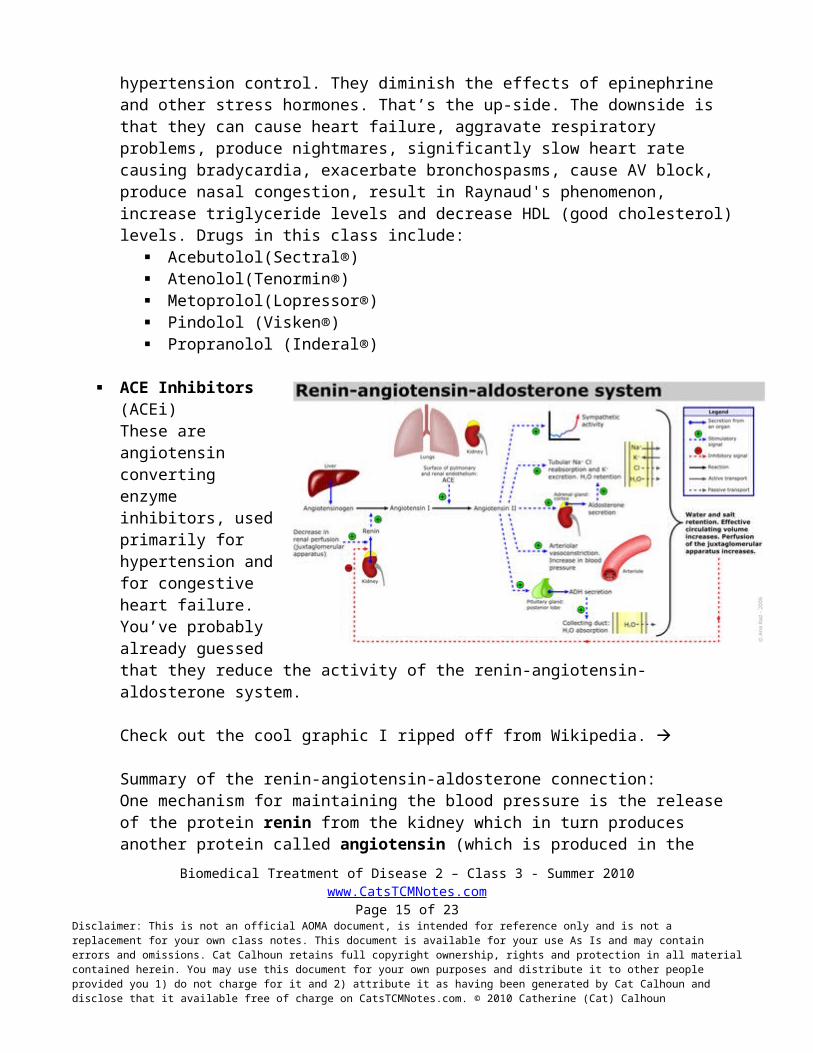
ACE Inhibitors (ACEi)These are angiotensin converting enzyme inhibitors, used primarily for hypertension and for congestive heart failure. You’ve probably already guessed that they reduce the activity of the renin-angiotensin-aldosterone system.
Check out the cool graphic I ripped off from Wikipedia.
Summary of the renin-angiotensin-aldosterone connection: One mechanism for maintaining the blood pressure is the release of the protein renin from the kidney which in turn produces another protein called angiotensin (which is produced in the liver and delivered into the blood supply). Angiotensin’s production then signals the adrenal gland to produce aldosterone. Under normal circumstances, this system is activated in response to a fall in blood pressure as well as markers of problems with the salt-water balance of the body, like decreased sodium concentration in the distal tubule (DCT), decreased blood volume and stimulation of the kidney by the sympathetic nervous system.
In these situations, the kidneys release renin which acts as an enzyme and cuts off all but the first 10 amino-acid residues of the angiotensinogen floating in the blood. These 10 residues are then known as angiotensin I. Angiotensin I is then converted to angiotensin II by angiotensin converting enzyme (ACE) which removes a further 2 residues and is found in the pulmonary circulation as well as in the endothelium of many blood vessels. The system in general aims to increase blood pressure by increasing the amount of salt and water the body retains, although angiotensin is also very good at causing the blood vessels to constrict.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 10 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Where were we? Oh yes.
ACE inhibitors are an initial medication used to control blood pressure. Speaking personally, when I was on BP control meds my doc jumped directly to these and just skipped the diuretics altogether. Why would she do that? Look at the chart in the next section. Hint: I’m white, female and I was under 40 when I was diagnosed with hypertension. (By the way, I’m not on them now and it’s 10 years later. What happened? I lost 20 lbs, started exercising and got a divorce which significantly reduced my stress level. )
ACEi’s block the conversion from Angiotensin I to Angiotensin II and have some fun side effects associated with this activity such as: a persistent dry cough (thought to be linked to bradykinin levels), hypotension, dizziness, renal dysfunction, hyperkalemia, angioedema, taste alteration and rash, acute renal failure. Almost needless to say it, but they are contraindicated in pregnancy. Some ACEi’s available on the market: Candesartan (Atacand®), Eprosartan (Teveten®), Irbesartan (Avapro®), Losartan (Cozaar®).
Deciding What Med What Hypertension Patient Gets (The ABCD Rule)So how do you decide which patient should get which med? Here’s a fun chart to help you out.
A=Ace inhibs or ARB’s B = Beta blockers C = CCB’s D = diuretics
B and D can actually induce more new-onset diabetes. Younger peeps are often prescribed A or B while people over 55 generally get C or D.
Note that African Americans are more likely to have hypertension, are more susceptible to complications, and respond differently to ACEinhib’s and ARB’s than non-African Americans do. It is critical to establish followup habits with regular lipid and ECG testing in addition to getting hypertension patients on meds.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 11 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun

Hypertensive CrisisA hypertensive emergency is severe hypertension (high blood pressure) with acute impairment of an organ system (especially the central nervous system, cardiovascular system and/or the renal system) and the possibility of irreversible organ-damage. In case of a hypertensive emergency, the blood pressure should be lowered aggressively over minutes to hours with an antihypertensive agent.
You might see hypertensive encephalopathy, which presents with headache, irritability, confusion, and altered mental status due to cerebrovascular spasms. You might also see hypertensive nephropathy which presents with hematuria, proteinuria, and progressive renal dysfunction. Hypertensive crisis might also emerge as an intracranial hemorrhage, aortic dissection, preeclampsia-eclampsia, pulmonary edema, unstable angina, or myocardial infarction.
To manage the the crisis reduce the pressure by no more than 25% over a span of 1 or 2 hours. Then move the patient toward a level of 160/100 mm Hg within 2–6 hours. Why so slow? Excessive reductions may precipitate coronary, cerebral, or renal ischemia. One way to do this is with adrenoceptor or α - blockers. These substances relax arterial smooth muscle, reduce BP, and have no adverse effects on the serum lipid levels. They do increase HDL and reduce total cholesterol actually, so yay. These drugs include
Prazosin (Minipress®) Terazosin (Hytrin®) Doxazosin (Cardura®)
A guy with prostate problems can benefit from this too because it dilates the vessels allowing him to void the bladder. He’ll thank you for this ‘cuz nobody likes that feeling. Yay again.
Pulmonary Heart Disease – Cor Pulmonale
Cor Pulmonale is pulmonary heart disease is enlargement of the right ventricle of the heart as a response to increased resistance or high blood pressure in the lungs. Chronic cor pulmonale usually results in right ventricular hypertrophy (RVH), whereas acute cor pulmonale usually results in dilation.Hypertrophy is an adaptive response to a long-term increase in pressure. Individual muscle cells grow larger and change to drive the increased contractile force required to move the blood against greater resistance. Dilation is a stretching of the ventricle in response to acute increased pressure.To be classified as cor pulmonale, the cause must originate in the pulmonary circulation system. Two major causes are vascular changes as a result of tissue damage (e.g. disease, hypoxic injury, chemical agents, etc.), and chronic hypoxic pulmonary vasoconstriction. RVH due to a systemic defect is not classified as cor pulmonale. When untreated, cor pulmonale can lead to right-heart failure and death.
A patient with cor pulmonale will have symptoms and signs of chronic bronchitis and pulmonary emphysema (elevated jugular venous pressure, parasternal lift, edema, hepatomegaly, ascites, RV hypertrophy and eventual failure). They could develop chronic productive cough, wheezing, possible
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 12 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
clubbing of fingers, exertional shortness of breath, easy fatigue/weakness, and low O2 levels (85% or less). They will need oxygen supplementation, salt/fluid restriction, and diuretics. They generally live less than 5 years when reach failure levels.
Vascular disease
Abdominal aortic aneurysm (AAA) is something to be aware of! 10% of people over 65 have it. Palpate all bellies over this age at least 1ce per year. Listen for bruit. May be asymptomatic and only detected during a routine physical examination or a diagnostic study. However, it might also present as severe back or abdominal pain, a pulsatile mass, and hypotension (which can indicate rupture…which is fatal 90% of the time). Most abdominal aneurysms originate below the renal arteries. 5–8% of men over the age of 65 years have it. You can detect it by the prominent aortic pulsation.
Rupture causes hypotension and shock. In shock, which is the body’s response to severe stress, the patient goes into sympathetic overdrive – they might be losing fluids somehow – vomiting, diarrhea, internal bleeding (like aneurysm rupture), etc. Could be heart pumping poorly or heart attack, pneumothorax or pulmonary embolism pushing on the heart or blocking left ventricle, pancreatitis/inflammation releasing cytokines which open up all membranes so that fluids seep from one compartment to another, could be septic shock which stresses body heavily.
Hypotension, Sweating and other signs of sympathetic response. Tachycardia Oliguria Altered mental status Peripheral hypoperfusion and hypoxia Release of and increase in the levels of norepinephrine, renin, ADH, glucagon (because stress
requires energy and glucagon converts stored glycogen back to glucose), cortisol (which could also be due to stress) and growth hormones
Septic shock will present with fever, chills , hypotension , hyperglycemia and altered mental status. Septic shock is due to infection and proliferation of gram-negative bacteremia: (E coli, Klebsiella, Proteus, and Pseudomonas).
HypotensionDefinition: Systolic of 90mmHg or less. Drop of more than 10-20 mm and an increase in pulse of more than 15 when they change positions. Call 911 and give basic life support as needed.
Orthostatic hypotension means the person is blacking out or fainting due to overstimulation of vagal system. Older people are more likely to have this due to lack of elasticity of vessels, so can’t compensate for positional changes. Diabetics have this in profound levels. There is a greater than normal decline in bp when getting up from lying down position.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 13 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Vascular DisordersVascular disorders of lower limbs will first show in toes – looks a lot like toes rotting….cuz they are. How does this start?
Aneurysms of Abdominal Aorta (AAA)Common, but usually asymptomatic (see section above for more detail). Might show as severe back or ab pain, pulsatile mass. Sudden hypotension indicates rupture. AAA is often combined with atherosclerosis in lower extrems in 25% of patients. Therapy consists of beta blockers, surgery and graft. There’s a survival rate of 80% or so after graft. Of course, if it isn’t detected and it ruptures, there is a 90% fatality rate.
Peripheral Artery Aneurysms in the popliteal and/or femoral arteries. Also associated with aortic aneurysms. Can cause gangrene because the circulation is impeded to the lower limb.
Lower Extremity Occlusive DiseaseIndicates arterial disease in general. Patient will get intermittent claudication – cramps then sit down and goes away. Indicates possible concommitant atherosclerosis, diabetes, hypertension, erectile dysfunction. Patient will/may have gangrene/ischemia signs.
The triad of bilateral hip and buttock claudication, erectile dysfunction, and absent femoral pulses is known as Leriche's syndrome.
Tests to diagnose vascular disorders Feel for peripheral pulses.
Absent/ diminshed peripheral pulses. You can also compare the ankle to the brachial pulse. This is called the ABI (ankle-brachial index) - a normal ratio of ankle to brachial systolic blood pressures is 1.0; less than 0.8 is consistent with claudication. Really, pressures should match in upper and lower limbs.
Look for resting pain and nonhealing ulcers Lipid-lowering medications have been shown to produce a 40% risk reduction for new-onset claudication or worsening of claudication. These patients can also take phosphodiesterase inhibitor, cilostazol (100 mg orally twice daily), carnitine and possibly ginkgo biloba.
Acute Limb Ischemia If a limb suddenly goes white, this is a red flag (pardon the color pun) indicating acute ischemia which can be embolic, thrombotic, or traumatic in nature.
Symptoms are the 6 P’s of acute limb ischemia: Pain Pallor Pulselessness Paresthenia
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 14 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun
Poikilothermia (internal temperature matches the external temperature…kind of like a reptile)
Paralysis
90% are embolic, especially cardiac. Give these patients heparin (which immediately starts clearing the clots) and possibly an embolectomy! This is an emergency, dangit! You could only have a 6 hour window to keep ‘em alive!
Thromboangiitis Obliterans (Buerger's Disease) This is a different kind of white limb/ischemia. Again, the limb goes white, but the tissues still feel warm, not cold. The causes of this are unknown. Most are ment over 40, smokers and european or asiatic. They will have claudication and resting pain (often in the arch of the foot or calf), possible necrosis or ulcerations. Their proximal pulses will be present, but not the distal ones.
Some possible disease diagnoses that go along with Buerger’s Disease: SLE, clotting disorders, ingestion of ergot (bread mold), and cannabis arteritis (spasm of vessels due to a big hit of weed, dude). These patients desperately need to stop smoking . . .cigarettes especially (and maybe weed too).
More on vascular disorders in the following class.
Biomedical Treatment of Disease 2 – Class 3 - Summer 2010www.CatsTCMNotes.com
Page 15 of 15Disclaimer: This is not an official AOMA document, is intended for reference only and is not a replacement for your own class notes. This document is available for your use As Is and may contain errors and omissions. Cat Calhoun retains full copyright ownership, rights and protection in all material contained herein. You may use this document for your own purposes and distribute it to other people provided you 1) do not charge for it and 2) attribute it as having been generated by Cat Calhoun and disclose that it available free of charge on CatsTCMNotes.com. © 2010 Catherine (Cat) Calhoun