Course 2 Unit 1 Part A B C D 1 Teacher Mariska Ronteltap [email protected] Treatment...
46
Course 2 Unit 1 Part A B C D 1 Teacher Mariska Ronteltap [email protected] Treatment aspects for urine, faeces and greywater
-
Upload
tariq-mock -
Category
Documents
-
view
221 -
download
1
Transcript of Course 2 Unit 1 Part A B C D 1 Teacher Mariska Ronteltap [email protected] Treatment...

Course 2 Unit 1Part A B C D
1
Teacher
Mariska [email protected]
Treatment aspects for urine, faeces and greywater

Content:Part A – Basics and overviewPart B – General treatment aspects for urinePart C – General treatment aspects for faeces
Part D – General treatment aspects for greywater (in separate file)
Course 2 Unit 1

Course 2 Unit 1
Part A: Basics and overview
Course 2 Unit 1

Where does Course 2 fit in the overall sanitation system scheme?
EE
Course 2, Units 1-7

Where does C2 Unit 1 fit in the overall sanitation system scheme?
EE

Another way of looking at it: Course 2 in the scheme of nutrient recycling
Sanitised urine and faeces (“ecosan products”)
Human excreta
Crop & Harvest
Consumption followed by urination / defecation
Focus of Course 2
Sanitisation steps
Apply as fertiliser and soil conditioner

Aims of treatment of urine, faeces and greywater
The main aims of treatment are:
1. Sanitisation (= pathogen kill) protect public health
2. Groundwater protection indirectly, this also protects public health (see Course 1 Unit 3 Part A)
3. For ecosan: enable safe reuse
There can also be secondary aims, which may vary, but
they need to get lower priority (see later in this presentation).

Pathogen = disease-causing micro-organism (a biological agent that causes disease or illness to its host)
Enteric or enteral = pertaining to the intestine– Intestine = the portion of the alimentary canal extending from the stomach to the anus
Source: www.wikipedia.org
What is a pathogen and what is enteric? Course 2 Unit 1

Definition of terms: disinfection, sanitisation, sterilisation
Term Degree of pathogen destruction
Examples of technical processes
Disinfection Partial Tertiary treatment step in conventional wastewater treatment
Sanitisation / hygenisation
Most or all Primary or secondary treatment step for urine, faeces or greywater
Sterilisation All Medical routines; not practical for excreta management
Need to weigh up remaining risk versus cost of treatment The allowable risk depends on reuse application and other barriers that are in place ( we will talk about the Multiple Barrier Approach in C3U1)

There are four groups of pathogens potentially present in human excreta
Pathogen group
Pathogen Disease caused by pathogen
Bacteria Aeromonas spp.
Escherichia coli
Salmonella typhi
Salmonella spp.
Shigella. spp.
Vibrio cholerae
Enteritis *
Enteritis
Typhoid
Salmonellosis
Shigellosis
Cholera
Viruses Hepatitis A virus
Rotavirus
Hepatitis
Enteritis
Parasitic protozoa
Giardia intestinalis
Cryoptosporidium parvum
Giardiasis
Cryptosporidiosis
Helminths Ascaris lumbricoides (roundworm)
Taenia solium (tapeworm)
Ancylostoma duedenale (hookworm)
Schistosoma spp.
Ascariasis
Taeniasis
Itch, rash, cough, anaemia, protein deficiency
Schistosomiasis, bilharzia
Source: WHO (2006), p.33
Course 2 Unit 1

Factors that influence pathogen die-off
After excretion, the concentration of enteric pathogens usually declines with time by death or loss of infectivity
Bacteria may multiply under favourable environmental conditions
Protozoa and viruses are unable to grow in the environment outside the host, hence their numbers will always decrease
Time and prevailing conditions are the overall features affecting survival of pathogens in the environment
Giardia lambliaOne of the more common
parasitic organisms is Giardia lamblia. This parasite grows in
the upper GI tract and produces greasy, smelly
diarrhea.(microbiology.mtsinai.on.ca/
pig/helminth11.shtml )Source: Schönning and Stenström (2004)

Disinfection methods used in water and wastewater treatment (for reference)
Chemical agents– Chlorine and its compounds– Ozone– Various acids (to achieve pH < 3) – Various alkalines (to achieve pH > 11)– Urea
Physical agents– Time*– Heat*– Dryness*– Light
• Sunlight*• UV lamps
All of these could be used as part of ecosan concepts, but the ones highlighted with * are most commonly used (low-cost applications)

Course 2 Unit 1
Part B: General treatment aspects for urine
Note: For characteristics of urine see Course 1 Unit 2
Urine storage tank, Hengelo, the Netherlands (July 2007)
Course 2 Unit 1

Primary and secondary aims for urine treatment
Primary aim:
1. To kill viruses and pathogens
2. To enable safe reuse (for urine, that means: no (ground)water pollution; no danger for the workers; rather no ammonia evaporation)
In several countries people know very well the value of urine as a fertiliser. Here we see an example from India where you get a rupee if you use their toilet..
Secondary aims:
1. To obtain monetary value from (components in) urine in the form of fertiliser, energy, an others
2. To reduce the load to the WWTP or receiving water bodies

The easiest and most common treatment method for sanitisation of urine is by storage
Pathogen kill by storage of urine is due to:
1. Rapid conversion of urea to ammonia which increases the pH
2. Increased ammonia concentration together with the increase in pH have a sanitising effect
3. Time by itself also kills many pathogens (being away from a host)
Urine storage tank in basement of apartment block Gebers in Stockholm, Sweden (Aug. 2007) – with Anselme Vodounhessi from CREPA, Burkina Faso

Which pathogens are present in urine?
By far the most pathogens in excreta are in the faecal part. In urine also some were found: Schistosoma haematobium, Salmonella typhi, Salmonella paratyphi,
Leptospira interrogans Mycobacterium tuberculosis in urine of humans with renal TB
infection
Other pathogens come from faecal contamination – you can imagine that some of the faeces ends up in the urine opening: an average of 9.1 mg faeces/L urine was measured. Vinnerås et al., 2008)

Dilution, temperature or pH?
Storage was always thought to be the best treatment. Bjorn Vinneras et al (2008) looked into other aspects: dilution rate, temperature and ammonia concentration. They found that dilution rate is an important factor regarding the reduction in pathogenic microorganisms in urine:
At all temperatures: lower than 40 mM NH3 inactivation is slow (NH3 is regulated by total ammonia concentration,
temperature and pH)- At temperatures < 20°C: restrictions on the use of urine as a
fertiliser on food crops, as ascaris and viruses are reduced at a very slow rate.

Dilution, temperature or pH?
At 34 ° C fast inactivation of all organisms was observed, even at 1:3 dilution of urine.
If all ammonia is out, pathogens survive even at higher temperature!

How long should urine be stored for?
Centralised systems (urine from many households is mixed together)– Recommended storage time is 1-6 months, depending on
temperature and type of crop to be fertilised (see next slide)– 1 month storage sufficient if T > 20°C and crop is not to be
eaten raw Individual one-family system:
– No storage is needed (see also slide after next) Note: Urine in the storage tank should not be diluted (concentrated
urine provides a harsher environment for micoorganisms and hence more effective pathogen kill)
Source: WHO (2006)

Recommended guidelines for storage times of urine mixture
Storage temperature
Storage time Possible pathogens in the urine mixture after storage
Recommended crops
4°C > 1 month Viruses, protozoa Food and fodder crops that are to be processed
4°C > 6 months Viruses Food crops that are to be processed, fodder crops
20°C > 1 month Viruses Food crops that are to be processed, fodder crops
20°C > 6 month Probably none All crops
Urine mixture: urine which may be mixed with water
Source: Schönning and Stenström (2004) and also adopted in WHO (2006)
Course 2 Unit 1

New insights: shorter is fine, if undiluted and warm
For safe unrestricted reuse of urine, it needs to contain 40 mM or more of uncharged ammonia and be stored above 20 °C. Then the required storage time according to WHO guidelines could probably be shortened (Vinnerås et al., 2008)
21

Is urine sanitisation (by storage) really necessary?
YES, because: In a healthy individual, urine in
the bladder is sterile, but different types of bacteria are picked up in the urinary tract
Persons infected with Schistosoma haematobium excrete the eggs in urine. The eggs hatch in the freshwater environment
Urine could be contaminated by faeces if users of UD toilet are not careful
Source: Schönning and Stenström (2004)
NO, because: Urine contains few disease-
causing organisms Urine-oral transmission is
much less likely than faecal –oral transmission of disease (WHO, 2006, page 34)
A multiple barrier approach is used for reuse of urine (see also Course 3 Unit 1)
You need to weigh this up on a case by case basis
Advantages and disadvantages of storing urine compared to using it “fresh”
Advantages: Simple and effective method for pathogen kill Allows waiting for the right time for application to soils in
relationship to planting and harvesting times (See Course 3 “Safe reuse of ecosan products in agriculture”)
Disadvantages: Cost of urine storage tank Some loss of nitrogen possible during storage (via ammonia
gas)
More information on practical aspects of urine storage is provided in Course 2 Unit 3 “Storage and transport logistics”
Possible secondary treatment aims and treatment methods specific for urine (most of them require “high-tech” treatment options)
• Nitrogen recovery (to allow reuse of N in fertiliser)• Nitrogen removal (to reduce nitrogen load to WWTP)
– Biological process: nitrification and denitrification (convert ammonia to nitrate and then nitrogen gas) or ANAMMOX process
• Removal of micro-pollutants and pharmaceutical residues (to make urine even safer for reuse in agriculture)– Electrodialysis– Nanofiltration– Ozonation and advanced oxidation
Some of these treatment aims play a role in projects in the Netherlands and Switzerland (see next couple of slides). Struvite precipitation also takes place in the developing world, see the project in Nepal (STUN)

Example for high-tech treatment method for urine: vacuum evaporation
Advantages:– Allows volume reduction
Technical problems:– High energy demand– Pre-treatment necessary
to lower pH– Distillate is high in
ammonia
Source: Ecosanres Discussion Forum, Felix Tettenborn, TU Hamburg-Harburg (29 May 2006 and an update with further information on 22 February 2007)
Vacuum evaporation (lab scale). Photo: Felix Tettenborn
Course 2 Unit 1

Example for high-tech treatment method for urine: struvite precipitation
By adding magnesium, a crystal precipitates with phosphate called struvite: MgNH4PO4
Advantages:
- Struvite is a slow-release fertilizer. By separating this from the liquid phase, we have a strong reduction of volume- Easy and rapid- The effluent can be used for irrigation
For a pilot scale example, check the link here to the right
Course 2 Unit 1
Nepal: Pee proudly for healthy vegetables
(this is a link to the internet)

Example for High-tech treatment method for nitrogen removal from urine
Nitrification (biologial process) to convert ammonia to nitrate
Pilot plant at Hengelo (project of the
Waterboard Regge en Dinkel in Almelo, the Netherlands)
Pilot-scale nitrification reactor with attached growth (July 2007): treating 1 m3 of urine per week
Course 2 Unit 1
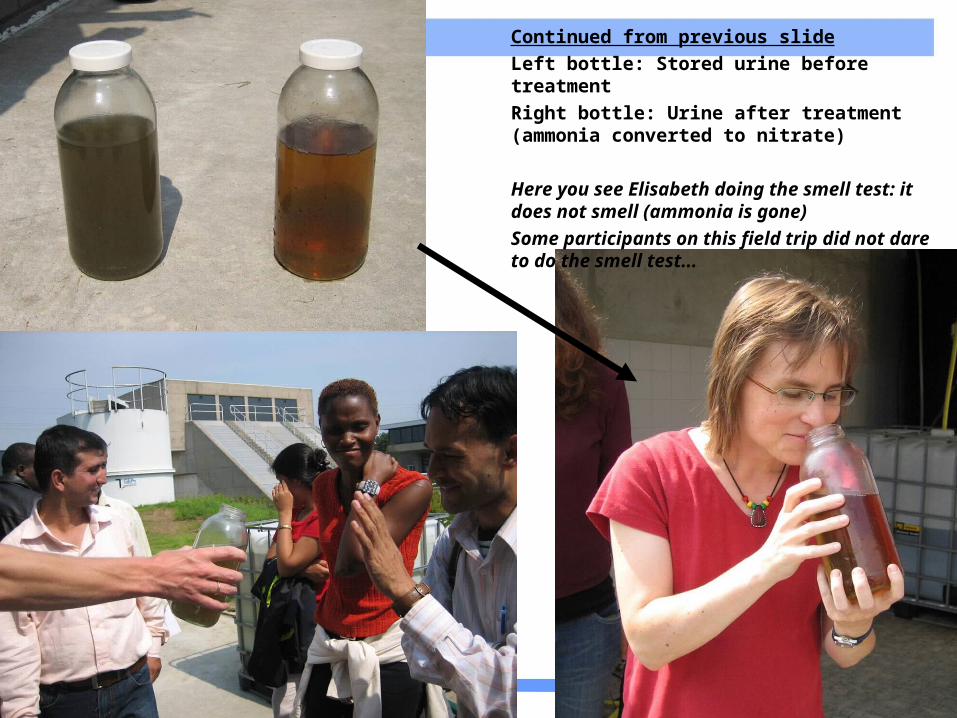
Continued from previous slideLeft bottle: Stored urine before treatmentRight bottle: Urine after treatment (ammonia converted to nitrate)
Here you see Elisabeth doing the smell test: it does not smell (ammonia is gone)Some participants on this field trip did not dare to do the smell test...

Further reading about high-tech treatment methods of urine
Maurer, M., Pronk, W. Larsen, T.A. (2006) Review: Treatment processes for source-separated urine, Water Research, 40, p. 3151 – 3166 *
Pronk, W., Zuleeg, S., Lienert, J., Escher, B., Koller, M., Berner, A., Koch, G., Boller, M. (2007) Pilot experiments with electrodialysis and ozonation for the production of a fertilizer from urine, Advanced Sanitation Conference, Aachen, Germany, 12 – 13 March *
* Also provided on the I-LE under Extra Materials for this course unit

What are alternative options if no agricultural reuse of urine is possible?
Infiltrate into ground (e.g. in Durban rural areas, South Africa) – check potential for nitrate pollution of groundwater
Add to composting operations (but loss of ammonia)
Discharge to sewer and wastewater treatment plant
If amounts are small and climate is suitable: evaporation

Other more “exotic” uses of urine (other than use as a fertiliser)
As an insecticide– See Ecosanres Discussion Forum on 11 June 2007 and earlier postings;
note: when plants have a good nutritional balance, they resist the attak of pathogens and insects – so reported insecticidal properties of urine may be a secondary effect (?) – more research is needed
As a medicine– Some people strongly believe that drinking urine is good for you! (e.g.
http://www.rotten.com/library/medicine/bodily-functions/pissing/drinking-pee/)
– As a disinfectant for wounds (smearing wounds and sores)– To improve your skin
To produce the human fertility hormone hCG– Can be extracted from urine of pregnant women and then given to other
women for fertility treatment (see my entry on Ecosanres Discussion Forum on 3 July 2007)
To use for odour control in sewers (after conversion of ammonia to nitrate)– This is being tested by the Waterboard Regge en Dinkel in the
Netherlands (in 2007)
Can you give examples of such “exotic” uses for urine?
Course 2 Unit 1
Part C: General treatment aspects for faeces
Note: For characteristics of faeces, see Course 1 Unit 2
Course 2 Unit 1

Reminder: main treatment aims for faeces
Sanitisation (= pathogen kill) protect public health ! Enable safe reuse (desirable)
Possible secondary treatment aims specific for faeces
– Volume reduction (remember faeces are about 80% water at excretion)
– Odour reduction– Prevention of groundwater pollution by pathogens in fresh
faeces– Change appearance, so that it no longer looks like faeces

Sanitising faeces: What kills pathogens in faeces?
Factor Mechanism Technology examples
Storage time * A longer storage time kills pathogens Storage *
Temperature At temperatures of 55-65°C all types of pathogens (except bacterial spores) die within hours
Composting (thermophilic); solar drying toilets
pH Highly acidic or alkaline conditions will have an inactivating effect (adding sawdust, ash or lime increases pH)
Alkali treatment
Ammonia Pathogens in excreta can be inactivated by the addition of ammonia
Addition of urease
Dryness / moisture *
Pathogens die off with lack of moisture (addition of drying agents, e.g. sand, ash)
Desiccation *
Solar radiation / UV light
Survival time of pathogens on crop and soil surface is reduced by UV radiation
Spreading faecal sludge in the open
Source: Winblad and Simpson-Hebert (2004)
* Applied in UDD toilets (UDD = urine-diversion dehydration)

Adding ash to faeces in UDD toilets: a common “pre-treatment” step
Promotes pathogen die-off through elevated pH of the ash Reduces smell Covers material
– reduces fly breeding– improves aesthetical conditions
Decreases moisture content
How much should be added? – One cup, or 200 – 500 mL ash; enough to cover faeces (WHO
(2006), p. 69)What else can be used?
– Lime, sand, soil, saw dust, leaves, compost or nothing– Note: we are not adding anything to the UDD toilet in the UNESCO-
IHE building because it has a fan (see presentation in Course 1 Unit 3 Assigned Reading)
Course 2 Unit 1
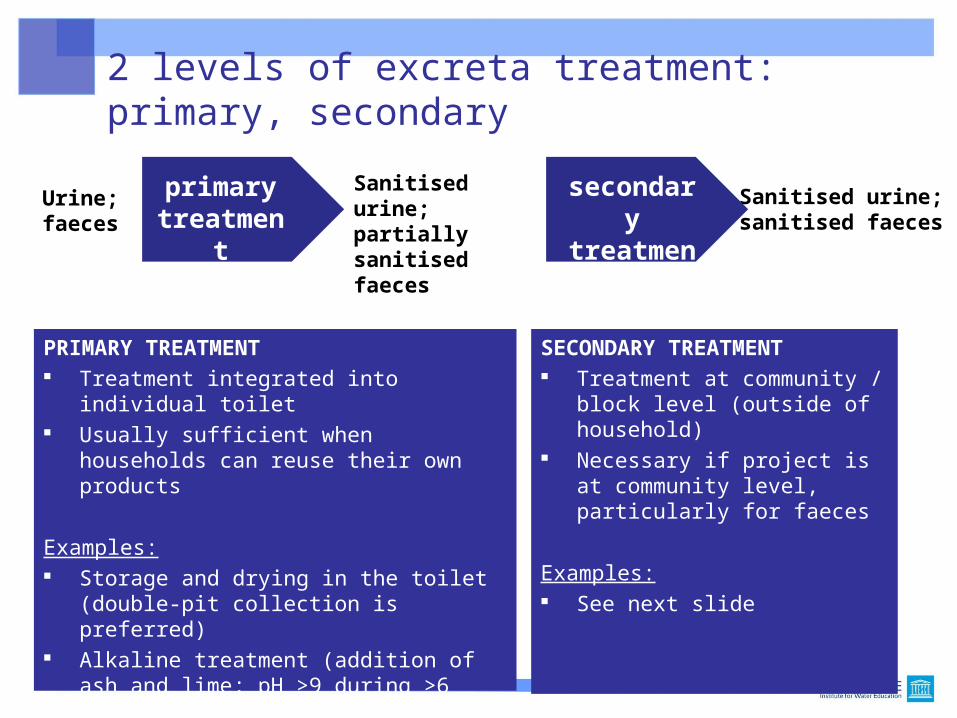
2 levels of excreta treatment: primary, secondary
Urine;faeces
Sanitised urine;sanitised faeces
Sanitised urine;partially sanitised faeces
PRIMARY TREATMENT Treatment integrated into individual toilet Usually sufficient when households can
reuse their own products
Examples: Storage and drying in the toilet (double-pit
collection is preferred) Alkaline treatment (addition of ash and lime;
pH >9 during >6 months) Composting (not recommended except for
dedicated users)
SECONDARY TREATMENT Treatment at community / block
level (outside of household) Necessary if project is at
community level, particularly for faeces
Examples: See next slide
primary treatment
secondary treatment

Secondary treatment options for faeces
Type of process Description Is it common?
Storage One year under tropical conditions (28-30 ºC) Very common
Composting Thermophilic preferred (> 50 ºC for > 1 week)
Common
Anaerobic digestion Works well in conjunction with animal manure (household biogas plants), but incomplete pathogen removal
Common in some countries (e.g. China, India, Nepal)
Chemical treatment Mixing with urea to achieve pH increase Experimental stage
Incineration Burning, reuse of ash; complete pathogen kill Not common
based on SchSchönning and Stenström (2004) önning and Stenström (2004)

Recommendations for storage treatment of dry excreta and faecal sludge before use at the household and municipal levels
Treatment Criteria Comment
Storage; ambient temperature 2-20ºC
1.5 – 2 years * Will eliminate bacterial pathogens; re-growth of E. coli and Salmonella may need to be considered if rewetted; will reduce viruses and parasitic protozoa to below risk levels. Some soil-borne ova may persist in low numbers.
Storage; ambient temperature > 20-35ºC
> 1 year Substantial to total inactivation of viruses, bacteria and protozoa; inactivation of schistosome eggs (< 1 month); inactivation of nematode (roundworm) eggs; more or less complete inactivation of Ascaris eggs
Alkaline treatment pH > 9 during > 6 months
If temperature > 35ºC and moisture < 25%, lower pH and/or wetter material will prolong the time for absolute elimination
* Note: no addition of new material: this storage period is taken from the last addition of fresh faeces to the pile
Source: WHO (2006), p. 69

Example for primary treatment of faeces: Standardised UDD toilet in Durban, South Africa
Provides primary treatment for faeces (sanitisation)
Particularly suitable for rural areas
Households reuse their own sanitised faecal matter (no secondary treatment necessary in this case)
Urine is not reused in the Durban example but infiltrated into the soil
Vault closed at bottom
Course 2 Unit 1

Durban (South Africa) rural areas:Council is planning to install 47,000 double-vault UDD toilets by 2007 (17,500 already installed in 2003-2006)
Two openings at the back for removal of dried faeces from faeces vaults (each vault has its own vent pipe) – Photos by Elisabeth,May 2005
Cost information on these toilets:See Course 4 Unit 1 “Financial, institutional, social and policy aspects”

Closed second vault
Continued from previous slide
Plastic UD pedestal and bucket with sand
Waterless urinal (plastic)

Further information on the Durban (=eThekwini) case
With the incorporation of vast rural areas into the eThekwini Municipal area, the Water Services unit identified the need for a training programme for rural communities. A facilitator training manual has been developed for a basic level water and sanitation education programme. The facilitators are chosen from a particular community and trained by Institutional and Social Development (ISD) Consultants.
• Training material is available here: http://www.durban.gov.za/eThekwini/Services/water_and_sanitation/education/sewage_education/rural_water/index_html
Chris Buckley Pollution Research GroupUniversity of KwaZulu-Natal4041 Durban, South AfricaE-mail: [email protected]
Important local experts:
Teddy GoundenManager Community Education and Councillor LiaisoneThekwini MunicipalityDurban, South AfricaE-mail: [email protected]

Further publications on the Durban UDD toilet experience
Guness, M., Pillay, S., Rodda, N., Smith, M., Buckley, C., and Macleod, N. (2006) Quality of leachate from buried urine diversion toilet waste. Water Institute of South Africa Conference, Durban, South Africa, 22-25 May 2006. Available: www.ewisa.co.za/frame.aspx?url=~/literature/default.aspx&cat=8
Moilwa, N., and Wilkinson, M. (2006) The effect of hygiene communication on emptying of urine diversion toilets. 32nd WEDC International Conference, Colombo, Sri Lanka, November 2006. Available via: http://wedc.lboro.ac.uk/index.php
Course 2 Unit 1

What are alternative options if no agricultural reuse of faeces is possible?
Take to wastewater treatment plant
Take to sanitary landfill
Dump into shallow holes and plant trees (check seepage to groundwater)
Use in aquaculture
Can be burned and disposed with household rubbish
Can you think of other options? Which of these options would be the best for your first ecosan project..??
References used in this presentation Schönning, C. and Stenström, T. A. (2004) Guidelines for the safe
use of urine and faeces in ecological sanitation systems. Report 2004-1, Ecosanres, Stockholm, www.ecosanres.org *
WHO (2006) Guidelines for the safe use of wastewater, excreta and greywater: Volume 4, Excreta and greywater use in agriculture. World Health Organisation, Geneva, available: http://www.who.int/water_sanitation_health/wastewater/gsuww/en/ *
WHO (2004) Guidelines for drinking water quality – recommendations. Geneva, World Health Organisation
Winblad and Simpson-Hébert (2004) Ecological Sanitation – revised and enlarged edition, SEI, Stockholm, Sweden, from www.ecosanres.org *
• Björn Vinnerås, Annika Nordin, Charles Niwagaba, Karin Nyberg: Inactivation of bacteria and viruses in human urine depending on temperature and dilution rate. Water Reserch 42 (2008) 4067 – 4074.
Course 2 Unit 1