Costs, quality of life, treatment satisfaction and compliance in patients with β-thalassemia major...
13
Copyright Informa UK Limited 2008 Not for Sale or Comercial Distribution Unauthorized use prohibited. Authorised users can download, display, view and print a single copy for personal use CURRENT MEDICAL RESEARCH AND OPINIONÕ VOL. 24, NO. 7, 2008, 1905–1917 0300-7995 doi:10.1185/03007990802160834 ß 2008 Informa UK Ltd All rights reserved: reproduction in whole or part not permitted ORIGINAL ARTICLE Costs, quality of life, treatment satisfaction and compliance in patients with -thalassemia major undergoing iron chelation therapy: the ITHACA study Luciana Scalone a , Lorenzo G. Mantovani a , Marieke Krol b , Diana Rofail c , Simona Ravera d , Maria Grazia Bisconte e , Caterina Borgna-Pignatti f , Zelia Borsellino g , Paolo Cianciulli h , Domenico Gallisai i , Luciano Prossomariti j , Ippazio Stefa ` no k and Maria D. Cappellini l * a CIRFF – Centre of Pharmacoeconomics, University of Naples Federico II, Naples, Italy; CHARTA Foundation (member of COPERA), Milan, Italy b Institute for Medical Technology Assessment, Erasmus Medical Centre, Rotterdam, The Netherlands c MAPI Values, Questionnaire Development and Validation Unit, Bollington, UK d Centre of Pharmacoeconomics, University of Milan, Milan, Italy e Centro Microcitemie, Presidio Ospedaliero dell’Annunziata, Azienda Ospedaliera Cosenza, Italy f Arcispedale S. Anna Dipartimento di Medicina Clinica Sperimentale – Clinica Pediatrica Ferrara, Italy g UOC Ematologia - Emoglobinopatie, ARNAS Civico, Palermo, Italy h Ospedale S. Eugenio – Centro Microcitemie DH talassemia Roma, Rome, Italy i Istituto di Clinica Pediatrica – Universita ` degli Studi di Sassari, Sassari, Italy j Azienda Ospedaliera ‘A. Cardarelli’ UOC Microcitemie Padiglione C Centro Talassemici, Naples, Italy k Azienda Ospedaliera SS. Annunziata, Taranto, Italy l Congenital Anemia Center, IRCCS Foundation Policlinico, Mangiagalli, Regina Elena Hospitals and University of Milan, Italy Key words: Compliance – Cost analysis – HRQoL – Iron chelation therapy – Satisfaction – -Thalassemia Address for correspondence: Lorenzo G. Mantovani, CIRFF – Center of Pharmacoeconomics, Federico II University of Naples, Via Domenico Montesano 49, I-80131 Naples, Italy. Tel.: þ39 081 678657; [email protected] *For the ITHACA Study Group Paper 4215 1905 Curr Med Res Opin Downloaded from informahealthcare.com by University of Hong Kong on 09/17/13 For personal use only.
Transcript of Costs, quality of life, treatment satisfaction and compliance in patients with β-thalassemia major...
Copyri
ght In
forma U
K Limite
d 200
8
Not for
Sale or
Comerc
ial Dist
ributi
on
Unauth
orize
d use
proh
ibited
. Auth
orise
d use
rs ca
n dow
nload
,
displa
y, vie
w and p
rint a
sing
le co
py fo
r pers
onal
use
CURRENT MEDICAL RESEARCH AND OPINION�
VOL. 24, NO. 7, 2008, 1905–1917
0300-7995
doi:10.1185/03007990802160834
� 2008 Informa UK Ltd All rights reserved: reproduction in whole or part not permitted
ORIGINAL ARTICLE
Costs, quality of life, treatmentsatisfaction and compliance inpatients with �-thalassemiamajor undergoing iron chelationtherapy: the ITHACA studyLuciana Scalonea, Lorenzo G. Mantovania,Marieke Krolb, Diana Rofailc, Simona Raverad,Maria Grazia Biscontee, Caterina Borgna-Pignattif,Zelia Borsellinog, Paolo Cianciullih, Domenico Gallisaii,Luciano Prossomaritij, Ippazio Stefanok andMaria D. Cappellinil*a CIRFF – Centre of Pharmacoeconomics, University of Naples Federico II,
Naples, Italy; CHARTA Foundation (member of COPERA), Milan, Italyb Institute for Medical Technology Assessment, Erasmus Medical Centre,
Rotterdam, The Netherlandsc MAPI Values, Questionnaire Development and Validation Unit, Bollington, UKd Centre of Pharmacoeconomics, University of Milan, Milan, Italye Centro Microcitemie, Presidio Ospedaliero dell’Annunziata, Azienda
Ospedaliera Cosenza, Italyf Arcispedale S. Anna Dipartimento di Medicina Clinica Sperimentale – Clinica
Pediatrica Ferrara, Italyg UOC Ematologia - Emoglobinopatie, ARNAS Civico, Palermo, Italyh Ospedale S. Eugenio – Centro Microcitemie DH talassemia Roma, Rome, Italyi Istituto di Clinica Pediatrica – Universita degli Studi di Sassari, Sassari, Italyj Azienda Ospedaliera ‘A. Cardarelli’ UOC Microcitemie Padiglione C Centro
Talassemici, Naples, Italyk Azienda Ospedaliera SS. Annunziata, Taranto, Italyl Congenital Anemia Center, IRCCS Foundation Policlinico, Mangiagalli,
Regina Elena Hospitals and University of Milan, Italy
Key words: Compliance – Cost analysis – HRQoL – Iron chelation therapy – Satisfaction –�-Thalassemia
Address for correspondence: Lorenzo G. Mantovani, CIRFF – Center of Pharmacoeconomics,Federico II University of Naples, Via Domenico Montesano 49, I-80131 Naples, Italy.Tel.: þ39 081 678657; [email protected]
*For the ITHACA Study Group
Paper 4215 1905
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

ABSTRACT
Objectives: Iron chelation treatment (ICT) in �-thalassemia
major (�-TM) patients undergoing blood transfusions can
cause low satisfaction, low compliance, with possible
negative consequences on treatment success, patients’
wellbeing, and costs. The purpose was to estimate the
societal burden attributable to �-TM in terms of direct and
indirect costs, health-related quality-of-life (HRQoL),
satisfaction and compliance with ICT in patients undergoing
transfusions and ICT.
Research design and methods: The naturalistic,
multicenter, longitudinal Italian-THAlassemia-Cost-&-Outcomes-Assessment (ITHACA) cost-of-illness study was
conducted involving patients of any age, on ICT for at least
3 years, who were enrolled at 8 Italian Thalassemia Care
Centers. Costs were estimated from the societal perspec-
tive, quantified with tariffs, prices, or net earnings valid in
2006.
Results: One-hundred and thirty-seven patients were
enrolled (median age¼ 28.3, 3–48 years, 49.6% male) and
retrospectively observed for a median of 11.6 months.
Mean direct costs were E1242/patient/month, 55.5%
attributable to ICT, 33.2% attributable to transfusions.
Relevant quantity and quality of productivity was lost.
Both physical and mental components of HRQoL were
compromised. Little difficulties remembering to take ICT
and positive satisfaction with the perceived effectiveness
of therapy were declared, but not good levels of satisfac-
tion with acceptance, perception of side effects and
burden of ICT.
Conclusions: The management of �-TM patients
undergoing transfusions and ICT is efficacious, although
costly, but overall benefits were not always perceived as
optimal by patients. Efforts must be focused to improve
patients’ acceptance and satisfaction with their therapy;
this would contribute to a better compliance and hence an
increase in treatment effectiveness and patients’ overall
wellbeing, with expected improved allocation of human and
economic resources.
Introduction
People with hematological disorders like �-Thalassemia
Major (TM) require life-long blood transfusions as a
supportive therapy. The implementation of regular
blood transfusions in the 1960s radically changed
these patients’ life expectancy, although an important
consequence of this progress has been the increase of
the iron overload morbidity1,2: if the excess of iron is
not removed, it may damage vital organs, particularly
the liver, the heart, endocrine glands, and may lead to
death. Further progress was then made with the regular
use of iron chelation therapy (ICT), which in Italy
started with intramuscular deferoxamine in the late
1970s (the first iron chelator agent, deferoxamine,
was licensed by the FDA in 1968), then with continu-
ous intravenous and finally with subcutaneous infu-
sions to remove the excess of iron in transfused
patients3–5. Regular blood transfusion in combination
with ICT using subcutaneous deferoxamine infusions
have sensitively reduced patients’ morbidity and
increased their survival6–9. According to Zurlo et al.6
the overall survival from birth of patients born
in 1970–1974 was 97.4% at 10 years and 94.4% at
15 years. Borgna-Pignatti et al.7 recently reported data
on survival and causes of death in 977 Italian patients
with TM born since 1960, grouped according to their
year of birth: it was shown that patients born in more
recent years, treated with regular blood transfusions
and ICT, had a higher survival and a higher complica-
tions free survival.
Currently, the drug most frequently given is
deferoxamine, administered in an 8–12 h continuous
infusion, 5–7 times per week. An alternative drug to
be used is deferiprone, orally administered 3 times
per day and indicated for the treatment of iron overload
in patients with TM when deferoxamine therapy is
contraindicated or inadequate10. Recently it has been
shown that deferiprone has a better activity on removal
of iron from the heart11,12. An observed therapeutic
trend is to administer a combination of deferoxamine
and deferiprone for intensive chelation, as promising
results are attributed to a possible synergistic effect
of the two drugs13. New iron chelators seem to have
interesting properties and activities: in particular,
Deferasirox is a new oral iron chelator recently
approved by FDA and EMEA for the treatment of
transfusional iron overload14. In order to understand
the overall impact of transfusions and chelation treat-
ment in TM patients not only it is necessary to evaluate
the consequences on their morbidity and mortality, but
also on their overall wellbeing and on the health care
resources consumption necessary to treat them: in par-
ticular the treatment regimen can sensitively influence
patients’ satisfaction and compliance and their health
state perception, with possible consequences on the
effectiveness of the therapy and on health care costs.
So far little is known about the socio-economic
burden in patients affected by �-TM and undergoing
blood transfusions and ICT. The few studies available,
indicating that the costs of iron chelating therapy are
considerable, suffer from some drawbacks, as that they
do not include all relevant cost items, but only analyze
some aspects influencing the overall burden attributa-
ble to this condition and its treatment15–22. To be able
to understand the real overall burden of the phenom-
enon a number of factors should actually be taken into
account: both medical costs (such as treatment and
1906 Costs and outcomes in �-TM patients undergoing ICT � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(07)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

monitoring costs), non-medical costs (such as costs of
transportation), indirect costs, i.e. the cost attributable
to the loss of productivity by the patients and their
caregivers, the impairment of wellbeing (known as
intangible costs) and all other relevant aspects, rather
than just the cost of therapy, are important issues to be
considered to understand the overall impact of a disease
and to identify how to make efforts to reduce the
burden attributable to the disease, from both patients’,
their families’, healthcare providers’ and payer’s point
of view.
Accordingly, we conducted the Italian THAlassemiaCost & Outcomes Assessment (ITHACA) study
reported here, with the aim of estimating the societal
burden of �-thalassemia major (�-TM) managed with
blood transfusions and ICT. In particular direct costs
(e.g., cost of treatment), indirect costs (productivity
loss), intangible costs (health related quality of life),
attitude toward ICT (in terms of patients’ reported
compliance), and treatment satisfaction were estimated
in a cohort of pediatric and adult �-TM patients under-
going transfusions and ICT.
Patients and methods
Study design
A naturalistic, multicenter, retrospective, prevalence-
based cost of illness study was conducted. The techni-
que of cost of illness was chosen as appropriate to
estimate the societal burden attributable to �-TM and
its management with transfusions and ICT, according
to current clinical practice23.
Study sample
Adult and pediatric subjects of any age with �-TM
were enrolled in the ITHACA study between
November 2005 and March 2006. The patients had
to be on a transfusional regimen and ICT for at least
3 years and attending a thalassemia treatment center.
The patients who agreed to take part in the study
signed an informed consent. In the case of patients
aged less than 18 years, both they and their caregivers
were asked to sign the informed consent. The partici-
pating patients agreed that their data from hospital
charts could be stored into a database, in an anonymous
way, and that they (or their caregiver, in the case
of children) completed a one-time questionnaire to
provide the required data.
Data
To reach the objective of the ITHACA study
the following data were collected: demographic
characteristics and clinical status, direct (medical and
non-medical), indirect (i.e., loss of productivity), and
intangible costs (i.e., Health Related Quality of Life,
HRQoL), satisfaction and compliance with treatment,
as reported by the patients. A questionnaire asking
information on patients’ demographic and clinical
data and on direct medical resources consumption
occurring from January 1, 2005 was completed by
the physicians. To complete these questionnaires the
physicians used the patients’ medical charts. The
patients (or one caregiver if children) completed a
further questionnaire with questions on non-medical
resources consumption (e.g., cost of transportation to
the hospital or the physician), indirect resource con-
sumption, HRQoL, satisfaction and compliance with
their ICT.
Direct costs
The information required to estimate direct medical
costs was based on the occurrence and the amount of
medical resources absorbed during the observational
period: ICT administered, concomitant medications,
transfusions, hospitalizations, medical visits, laboratory
and instrumental tests. Costs were estimated by multi-
plying the amount of the resource consumed
(for instance the quantity of drugs used during the
observational period) by the corresponding unit cost
(price or tariff, as appropriate) applied in 2006.
In order to take into account the costs of infusion of
deferoxamine (pump, needles, syringes, and other
consumables) the physicians were further interviewed
and asked to specify which kind of device they used to
administer the deferoxamine to their patients, the aver-
age amount consumed in a month for patients treated
with deferoxamine, and the unit cost for each device.
The data collected with these interviews were used to
estimate a mean monthly cost of administration
in patients treated with deferoxamine. In order to
estimate the cost per infusion the obtained monthly
cost was divided by the average number of administra-
tions reported for the patients taking part in the study
and treated with deferoxamine. Hence, the estimated
mean cost per infusion was used to estimate the total
cost of infusions in the patients taking deferoxamine
alone or in combination with deferiprone. Direct non-
medical costs were estimated in terms of costs of travel
to reach the hospitals or the physicians’ offices for
a visit, or to reach the hospitals for transfusions or
for hospitalizations.
Indirect costs
For the estimation of indirect costs (i.e., costs due to
production losses, because patients were absent from
� 2008 Informa UK - Curr Med Res Opin 2008; 24(07) Costs and outcomes in �-TM patients undergoing ICT Scalone et al. 1907
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

work or less productive at work as a result of their
disease), a short version of the ‘Health and Labour
Questionnaire’ (SF-HLQ) was administered in subjects
aged �16 years24. It consisted of 4 modules to collect
data on absence from work, reduced productivity,
unpaid labor production, labor-related problems.
Questions referred to the previous 2 weeks.
Patients aged 12–15 years self-completed the
‘children-part’ of the HLQ. It consisted of two mod-
ules: one on absence from school, the other on times of
inability to do usual activities. Questions referred to the
previous 3 months. For patients younger than 12 years,
their caregivers completed the parent-version of the
children-part of the HLQ.
A monetary value to the loss of productivity was
applied when patients had paid work, in terms of
income-effect and by taking into consideration the
patients net earning. When the productivity loss was
related to unpaid labor (i.e., when the patients loosing
their productivity did not actually have paid employ-
ment, like children or housewives), the indirect costs
were not expressed in monetary terms. In particular,
absence from work and/or being less productive at
work were reported in terms of days/patient-week
and E/patient-week. The costs of being less able to per-
form household activities are presented in received
hours of formal and informal household care.
Health related quality of life
Health related quality of life was assessed in patients
aged from 14 years, by using a battery of 2 generic
questionnaires, the SF-36 and the EQ-5D. These ques-
tionnaires were chosen for their capability to evaluate
both the physical and psychological components of
quality of life, and because they allow the comparison
of HRQoL within and between different clinical con-
ditions and with the general population. The SF-36
questionnaire assesses eight dimensions of HRQoL,
which relate to the physical and mental components
of the individual’s health perception. Specifically, the
domains ‘physical functioning’, ‘role-physical’, ‘bodily
pain’, and ‘general health’ are more related to the
physical component, whereas the domains ‘vitality/
energy’, ‘social functioning’, ‘role-emotional’, and
‘mental health’ are more related to the psychological
component. Possible scores for each domain range from
0 (corresponding to the worst possible state) to 100
(corresponding to the best possible state). These eight
domains can be grouped into two summary scores:
the ‘physical component summary’ (PCS) evaluates
the patients’ perception of limitations or disabilities
in self-care, physical, social and role activities, the
presence of bodily pain and fatigue. The ‘mental com-
ponent summary’ (MCS) score evaluates the feelings of
psychological distress, social and role disability because
of emotional problems.
In accordance with standard procedures and using
the US algorithm, the summary scores were computed
by multiplying each of the eight individual SF-36 scores
by their specific factor score coefficients25,26. The sum-
mary scores are norm-based to allow their comparison
to the US population in which a mean of 50 and
a standard deviation of 10 are achieved. The EQ-5D
questionnaire consists of two main parts: the first part
generates a health profile (EQ-5D profile) made of
5 domains, namely ‘mobility’, ‘self care’, ‘anxiety or
depression’, ‘usual activities’, and ‘pain or discomforts’,
each one with three levels of severity (‘no problem’,
‘some or moderate problems’, ‘extreme problems’).
The second part of the questionnaire consists of a
visual analogue scale (EQ-5D VAS), measuring overall
HRQoL ranging from 0 (worst imaginable health
status) to 100 (best imaginable health state)27.
HRQoL of �-TM patients enrolled in this study was
compared with HRQoL of the general Italian popula-
tion28 and with the one of another congenital, chronic,
disabling rare disease: data from two Italian studies
on patients with moderate to severe hemophilia
were used29,30.
Satisfaction with ICT and compliance
ICT satisfaction and compliance was assessed in
patients aged from �12 years old: they completed a
Satisfaction with ICT questionnaire31 of 28 questions
measured on a 5-Likert scale: 19 items are grouped in
4 satisfaction domains: (1) satisfaction with ICT
perceived effectiveness, pertaining to the patients’ per-
ceptions of benefits of ICT; (2) acceptance (i.e., con-
venience) of ICT, exploring positive orientations
towards ICT with regard to expectations and conveni-
ence of taking ICT; (3) burden of ICT, measuring nega-
tive impact incurred from ICT on activities of
daily living, sleep, time to take ICT and dependency;
(4) side effects of ICT, assessing potential side effects of
ICT and their impact on individual appearance. The
possible scores are from 1, meaning ‘low satisfaction’,
to 5, meaning ‘high satisfaction’. Three items are on
compliance to ICT, as reported by the patients, with
questions on how often the interviewee (1) had trouble
remembering to take ICT; (2) thought about stopping
ICT; (3) followed the ICT regimen exactly as recom-
mended by his/her doctor in the previous 4 weeks.
Possible scores are 1, meaning ‘always’, to 5, meaning
‘never’. Six additional items are on worries, overall con-
cerns, and treatment preference. While this question-
naire is in the process of finalization and validation, its
initial version has been used and its psychometric
1908 Costs and outcomes in �-TM patients undergoing ICT � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(07)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

properties were checked in this study (internal consis-
tency, reliability, construct validity).
Perspective of the analysis
The society’s point of view was taken into considera-
tion in this study, in particular the Italian National
Health Service’s, the patients’ and their families’ per-
spectives were adopted as appropriate, according to
the type of data collected. In particular, direct costs
were estimated from the perspective of the Italian
NHS, patients’ and/or their caregivers. The patients’
perspective was adopted in the estimate of indirect
costs, HRQoL, treatment satisfaction and compliance.
Time horizon
Different time horizons were adopted, depending on
the type of data collected and on the instrument
adopted to collect each type of data. While the time
horizon for the clinical data and the consumption of
medical resources was around 1 year (i.e., from the
time of enrolment back to January 2005), the one
regarding the productivity loss was of 2 weeks or
3 months (depending on the age-specific version of
the labor questionnaire administered), while the time
horizon adopted to assess HRQoL, satisfaction and
compliance were referred to a period of up to
4 weeks before the interview. The results are reported
by taking into account the specific time horizons con-
sidered in each category of variables: for instance, the
direct costs will be expressed in terms of E per patient/
month, while the indirect costs as E or days per patient/
week. This approach was chosen to avoid possible
biases attributable to the adoption of different periods
to observe the occurrence of the events of interest.
Statistical analyses
A descriptive analysis was carried out using proportions
for categorical data, mean and/or median as central
tendency parameters for continuous data, with stan-
dard deviation (SD), minimum (min) and maximum
(max) values as dispersion parameters, as appropriate.
Cost were expressed in terms of mean cost per
patient-month (or per patient-week in case the time
horizon was lower than 1 month, as for the indirect
costs): this parameter can in fact be easily used to
make projections on different populations, allows the
calculations of total costs (e.g., by multiplying the mean
per patient cost by the prevalence of the disease) and is
of easy use for policy makers. Because of the highly
skewed distribution of cost variables, we report,
as a measure of variability, the distribution of costs
per patient per month, instead of standard deviations.
Stratification analyses were also conducted to investi-
gate a possible relationship between costs of transfu-
sions and of ICT and patients’ age. The internal
consistency of the SF-36 and the Satisfaction question-
naire was assessed through the calculation of
Cronbach’s alpha, for which values40.70 can be con-
sidered satisfactory32. All analyses were performed
using SPSS version 13.0 software (SPSS, Chicago, IL).
Ethical aspects
Approval for the study was granted by the Institutional
Review Board of the coordinating centre (i.e., the
Congenital Anemia Center of the IRCSS Foundation
Policlinico, Mangiagalli, Regina Elena Hospitals).
Each patient was asked to sign an informed consent
form. In the case of patients less than 18 years old,
both the patients and their parents/guide had to sign
the informed consent form.
Results
Socio-demographic and clinical data
A total of 137 patients were enrolled from eight tha-
lassemia care centers and were retrospectively observed
for 10–13 months (mean¼ 11.8, median¼ 11.6), for a
total of 1604 patient-months. Socio-demographic and
clinical data are reported in Tables 1 and 2. Details of
main characteristics are specified below. Fifty percent
of the patients were female, the median age was
28 years, with the youngest patient aged 3 years and
the oldest 48 years. The 21 patients aged not more than
15 years were attending kindergarten or school,
depending on their age. Among those aged �16 years
(116), 61 patients (52.6%) declared to have paid
employment, 55 (47.4%) did not have paid employ-
ment. It is worth noting that 6% of the patients declared
to be unable to work because of their health problems
and 18% declared that they did not have paid employ-
ment and were early retired or were receiving a pension
despite their young age, presumably for their disease.
The majority of the patients (121, 89% of the sample)
were diagnosed with �-TM by the age of 2 years
(median¼ 1 year). However 11% of the patients, who
were diagnosed later in their life (when they were 3–11
years of age), were transfusion dependent at the time of
the participation in the study. With reference to the last
detection of ferritin levels during the observational
period, almost 28% of the patients had less
than 500 ng/mL, one third had between 500 and
1000 ng/mL, and almost 40% had higher levels of fer-
ritin, in particular 34 patients, 25.4% of the study
sample, had levels higher than 1500 ng/mL.
� 2008 Informa UK - Curr Med Res Opin 2008; 24(07) Costs and outcomes in �-TM patients undergoing ICT Scalone et al. 1909
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.
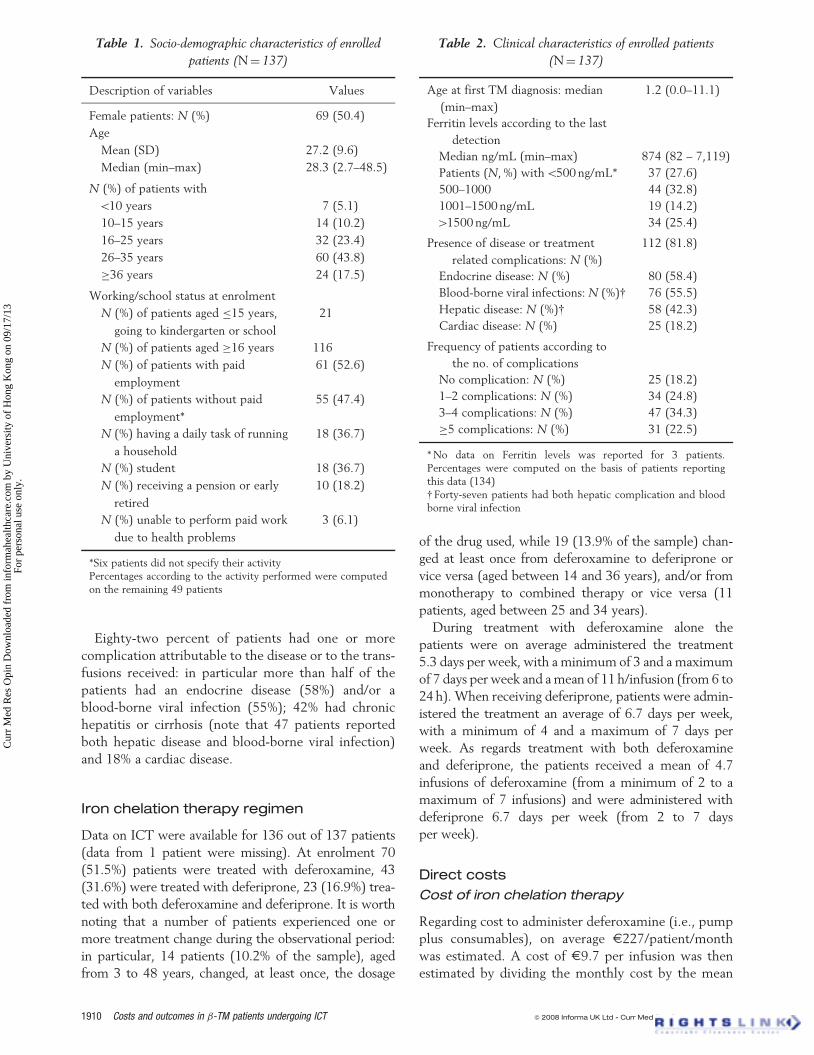
Eighty-two percent of patients had one or more
complication attributable to the disease or to the trans-
fusions received: in particular more than half of the
patients had an endocrine disease (58%) and/or a
blood-borne viral infection (55%); 42% had chronic
hepatitis or cirrhosis (note that 47 patients reported
both hepatic disease and blood-borne viral infection)
and 18% a cardiac disease.
Iron chelation therapy regimen
Data on ICT were available for 136 out of 137 patients
(data from 1 patient were missing). At enrolment 70
(51.5%) patients were treated with deferoxamine, 43
(31.6%) were treated with deferiprone, 23 (16.9%) trea-
ted with both deferoxamine and deferiprone. It is worth
noting that a number of patients experienced one or
more treatment change during the observational period:
in particular, 14 patients (10.2% of the sample), aged
from 3 to 48 years, changed, at least once, the dosage
of the drug used, while 19 (13.9% of the sample) chan-
ged at least once from deferoxamine to deferiprone or
vice versa (aged between 14 and 36 years), and/or from
monotherapy to combined therapy or vice versa (11
patients, aged between 25 and 34 years).
During treatment with deferoxamine alone the
patients were on average administered the treatment
5.3 days per week, with a minimum of 3 and a maximum
of 7 days per week and a mean of 11 h/infusion (from 6 to
24 h). When receiving deferiprone, patients were admin-
istered the treatment an average of 6.7 days per week,
with a minimum of 4 and a maximum of 7 days per
week. As regards treatment with both deferoxamine
and deferiprone, the patients received a mean of 4.7
infusions of deferoxamine (from a minimum of 2 to a
maximum of 7 infusions) and were administered with
deferiprone 6.7 days per week (from 2 to 7 days
per week).
Direct costs
Cost of iron chelation therapy
Regarding cost to administer deferoxamine (i.e., pump
plus consumables), on average E227/patient/month
was estimated. A cost of E9.7 per infusion was then
estimated by dividing the monthly cost by the mean
Table 1. Socio-demographic characteristics of enrolled
patients (N¼ 137)
Description of variables Values
Female patients: N (%) 69 (50.4)
Age
Mean (SD) 27.2 (9.6)
Median (min–max) 28.3 (2.7–48.5)
N (%) of patients with
510 years 7 (5.1)
10–15 years 14 (10.2)
16–25 years 32 (23.4)
26–35 years 60 (43.8)
�36 years 24 (17.5)
Working/school status at enrolment
N (%) of patients aged �15 years,
going to kindergarten or school
21
N (%) of patients aged �16 years 116
N (%) of patients with paid
employment
61 (52.6)
N (%) of patients without paid
employment*
55 (47.4)
N (%) having a daily task of running
a household
18 (36.7)
N (%) student 18 (36.7)
N (%) receiving a pension or early
retired
10 (18.2)
N (%) unable to perform paid work
due to health problems
3 (6.1)
*Six patients did not specify their activityPercentages according to the activity performed were computedon the remaining 49 patients
Table 2. Clinical characteristics of enrolled patients
(N¼137)
Age at first TM diagnosis: median
(min–max)
1.2 (0.0–11.1)
Ferritin levels according to the last
detection
Median ng/mL (min–max) 874 (82 – 7,119)
Patients (N, %) with5500 ng/mL* 37 (27.6)
500–1000 44 (32.8)
1001–1500 ng/mL 19 (14.2)
41500 ng/mL 34 (25.4)
Presence of disease or treatment
related complications: N (%)
112 (81.8)
Endocrine disease: N (%) 80 (58.4)
Blood-borne viral infections: N (%)y 76 (55.5)
Hepatic disease: N (%)y 58 (42.3)
Cardiac disease: N (%) 25 (18.2)
Frequency of patients according to
the no. of complications
No complication: N (%) 25 (18.2)
1–2 complications: N (%) 34 (24.8)
3–4 complications: N (%) 47 (34.3)
�5 complications: N (%) 31 (22.5)
* No data on Ferritin levels was reported for 3 patients.Percentages were computed on the basis of patients reportingthis data (134)yForty-seven patients had both hepatic complication and bloodborne viral infection
1910 Costs and outcomes in �-TM patients undergoing ICT � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(07)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.
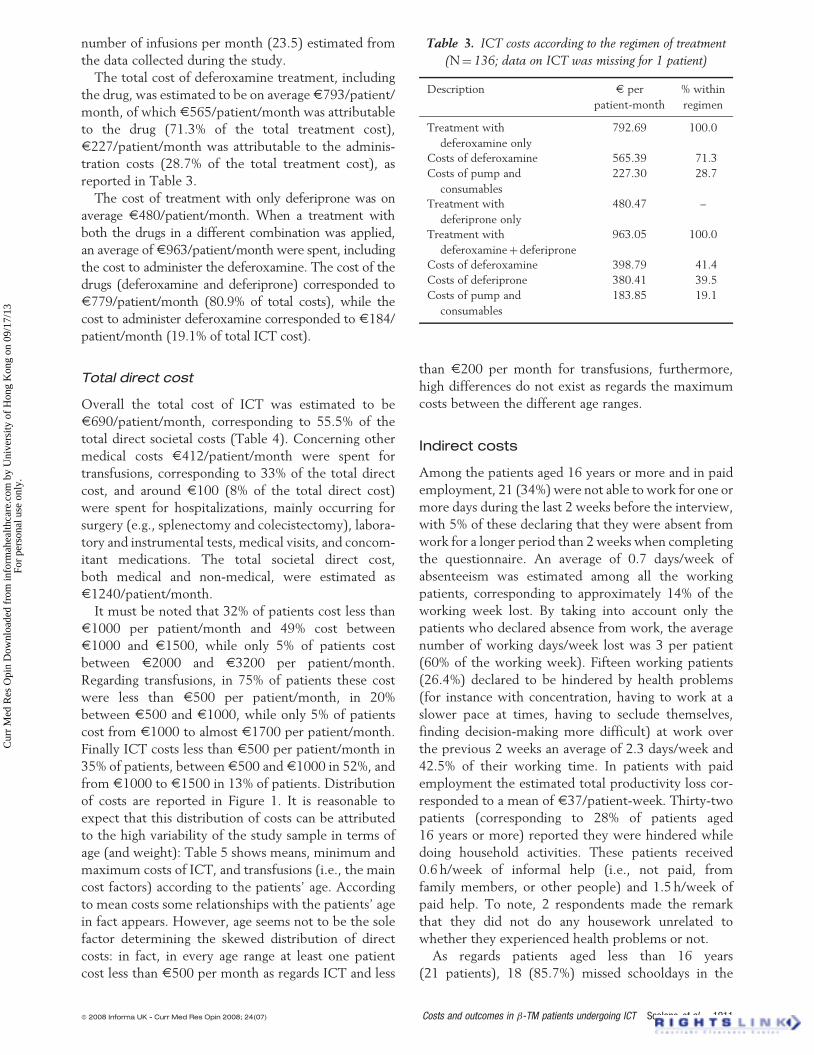
number of infusions per month (23.5) estimated from
the data collected during the study.
The total cost of deferoxamine treatment, including
the drug, was estimated to be on average E793/patient/
month, of which E565/patient/month was attributable
to the drug (71.3% of the total treatment cost),
E227/patient/month was attributable to the adminis-
tration costs (28.7% of the total treatment cost), as
reported in Table 3.
The cost of treatment with only deferiprone was on
average E480/patient/month. When a treatment with
both the drugs in a different combination was applied,
an average of E963/patient/month were spent, including
the cost to administer the deferoxamine. The cost of the
drugs (deferoxamine and deferiprone) corresponded to
E779/patient/month (80.9% of total costs), while the
cost to administer deferoxamine corresponded to E184/
patient/month (19.1% of total ICT cost).
Total direct cost
Overall the total cost of ICT was estimated to be
E690/patient/month, corresponding to 55.5% of the
total direct societal costs (Table 4). Concerning other
medical costs E412/patient/month were spent for
transfusions, corresponding to 33% of the total direct
cost, and around E100 (8% of the total direct cost)
were spent for hospitalizations, mainly occurring for
surgery (e.g., splenectomy and colecistectomy), labora-
tory and instrumental tests, medical visits, and concom-
itant medications. The total societal direct cost,
both medical and non-medical, were estimated as
E1240/patient/month.
It must be noted that 32% of patients cost less than
E1000 per patient/month and 49% cost between
E1000 and E1500, while only 5% of patients cost
between E2000 and E3200 per patient/month.
Regarding transfusions, in 75% of patients these cost
were less than E500 per patient/month, in 20%
between E500 and E1000, while only 5% of patients
cost from E1000 to almost E1700 per patient/month.
Finally ICT costs less than E500 per patient/month in
35% of patients, between E500 and E1000 in 52%, and
from E1000 to E1500 in 13% of patients. Distribution
of costs are reported in Figure 1. It is reasonable to
expect that this distribution of costs can be attributed
to the high variability of the study sample in terms of
age (and weight): Table 5 shows means, minimum and
maximum costs of ICT, and transfusions (i.e., the main
cost factors) according to the patients’ age. According
to mean costs some relationships with the patients’ age
in fact appears. However, age seems not to be the sole
factor determining the skewed distribution of direct
costs: in fact, in every age range at least one patient
cost less than E500 per month as regards ICT and less
than E200 per month for transfusions, furthermore,
high differences do not exist as regards the maximum
costs between the different age ranges.
Indirect costs
Among the patients aged 16 years or more and in paid
employment, 21 (34%) were not able to work for one or
more days during the last 2 weeks before the interview,
with 5% of these declaring that they were absent from
work for a longer period than 2 weeks when completing
the questionnaire. An average of 0.7 days/week of
absenteeism was estimated among all the working
patients, corresponding to approximately 14% of the
working week lost. By taking into account only the
patients who declared absence from work, the average
number of working days/week lost was 3 per patient
(60% of the working week). Fifteen working patients
(26.4%) declared to be hindered by health problems
(for instance with concentration, having to work at a
slower pace at times, having to seclude themselves,
finding decision-making more difficult) at work over
the previous 2 weeks an average of 2.3 days/week and
42.5% of their working time. In patients with paid
employment the estimated total productivity loss cor-
responded to a mean of E37/patient-week. Thirty-two
patients (corresponding to 28% of patients aged
16 years or more) reported they were hindered while
doing household activities. These patients received
0.6 h/week of informal help (i.e., not paid, from
family members, or other people) and 1.5 h/week of
paid help. To note, 2 respondents made the remark
that they did not do any housework unrelated to
whether they experienced health problems or not.
As regards patients aged less than 16 years
(21 patients), 18 (85.7%) missed schooldays in the
Table 3. ICT costs according to the regimen of treatment
(N¼ 136; data on ICT was missing for 1 patient)
Description E per
patient-month
% within
regimen
Treatment with
deferoxamine only
792.69 100.0
Costs of deferoxamine 565.39 71.3
Costs of pump and
consumables
227.30 28.7
Treatment with
deferiprone only
480.47 –
Treatment with
deferoxamineþ deferiprone
963.05 100.0
Costs of deferoxamine 398.79 41.4
Costs of deferiprone 380.41 39.5
Costs of pump and
consumables
183.85 19.1
� 2008 Informa UK - Curr Med Res Opin 2008; 24(07) Costs and outcomes in �-TM patients undergoing ICT Scalone et al. 1911
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

3 months before the interview, with an average of 0.6
days/patient-week, which corresponds to 10–12% of
the school week. Six patients declared they missed reg-
ular activities, like performing sport, an average of
0.02 days/patient-week.
Health related quality of life
Patients reported compromised levels of wellbeing.
The results with the EQ-5D profile show (Table 6)
that 9% of the patients reported moderate problems,
while no patient declared to have severe problems
with this domain. Only 1 patient declared to have
some problems in washing or dressing (self-care
domain), but 23% declared to have some problems in
doing usual activities (i.e., going to school, to work,
doing housework, family, or leisure activities).
Patients reporting moderate levels of pain or discomfort
were 61%, while 1 patient declared extreme pain or
discomfort, finally 40% declared to be moderately and
2.5% to be extremely anxious or depressed. The
EQ-Visual Analogue Scale score had a mean value of
73 (median¼75, from 30 to 100). Similar trends
were observed with the SF-36: details are reported
in Table 6, in particular the mean (SD) Physical
Component Summary score, which summarizes the
physical related scores, was 47.0 (8.4); the mean (SD)
Mental Component Summary score, summarizing
the mental related scores, was 45.0 (8.8). The internal
consistency of the SF-36 was good, with Cronbach
values ranging from 0.71 to 0.86 in every dimension.
As shown in Figure 2, the physical component of
HRQoL in �-TM patients on ICT was on average
worse than in the general Italian population compar-
able for sex and age, the mental component of
HRQoL was also worse than the one of the Italian gen-
eral population28. As it can be expected, the mean
Physical Component Summary score in male �-TM
patients was higher than the one in moderate to
severe adult hemophilic patients, with or without
inhibitors towards replacement therapy with coagula-
tion factor concentrates, while the mean Mental
Component Summary score was comparable with
these two categories of patients29,30.
Treatment satisfaction with ICTand compliance
Before analyzing the Satisfaction scores, the psycho-
metric properties of the Satisfaction questionnaire
were checked. All scores showed good internal
1.5%
34.6%
75.2%
30.1%
52.2%
19.7%
49.3%
13.2%
4.4%
14.0%
0.0% 0.7%5.1%
0.0% 0.0%0%
15%
30%
45%
60%
75%
90%
Fre
quen
cy o
f pat
ient
s
<500 € 500–999 € 1000–1499 € 1500–1999 € ≥2000 €Monthly per patient/costs
Total costs
ICT
Transfusions
Figure 1. Frequency of patients according to monthly direct costs, with comparisons between total (light grey bars), ICT (dark
grey bars), and transfusions (white bars) specific costs
Table 4. Total direct costs
Description of variables E per
patient-month
% on total
direct cost
ICT, any regimen, including
administration
689.63 55.5
Transfusions 412.12 33.2
Hospitalizations with surgery 41.26 3.3
Laboratory and instrumental
tests, medical visits
39.20 3.2
Concomitant medication 19.49 1.6
Total medical costs 1201.77 96.7
Non-medical costs
(travel cost)
42.78 3.4
Total direct costs 1242.66 100.0
1912 Costs and outcomes in �-TM patients undergoing ICT � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(07)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

consistency reliability: Cronbach’s alpha coefficients
were higher than 0.70 (from 0.73 to 0.83). The con-
struct validity of the scores were also good since all
items were more correlated to their own scale (as
opposed to the other scales), and correlation between
each item and its own scale, corrected for overlap, was
higher than 0.40 (except for 2 items). The Satisfaction
with ICT questionnaire was completed by all patients
�12 years of age (n¼126). As a score of 5 represents
‘Very Satisfied’ for all items in a domain, a mean of 3.5
or more suggests that most patients were rather satis-
fied with most or all of the items in the domain.
Satisfaction with ICT domains were highest for
Perceived Effectiveness with ICT (mean¼ 4.3),
followed by Burden of ICT (mean¼ 3.9), and then
Table 6. Health related quality of life results
Description of domains and levels Value
EQ-5D results
Mobility (N, %)
No problem in walking. 110 (90.9)
Some problems in walking 11 (9.1)
Confined to bed 0
Self-care (N, %)
No problem 120 (99.2)
Some problems in
washing or dressing
1 (0.8)
Unable to wash or dress 0
Usual activities (N, %)
No problem to perform
usual activities.
93 (76.9)
Some problems to perform
usual activities
28 (23.1)
Unable to perform usual activities 0
Pain/discomfort (N, %)
None 46 (38.0)
Moderate 74 (61.2)
Extreme 1 (0.8)
Anxiety/depression (N, %)
None 70 (57.9)
Moderate 48 (39.7)
Extreme 3 (2.5)
Visual Analogue Scale
Mean (SD) 73.1 (16.0)
Median (min, max) 75.0 (30–100)
SF-36 results
Physical functioning
Mean (SD) 82.8 (16.7)
Min–max (35.0–100.0)
Role–physical
Mean (SD) 68.2 (36.5)
Min–max (0–100)
Bodily pain
Mean (SD) 69.4 (24.3)
Min–max 72.0 (10–100)
(continued)
Table 6. Continued
Description of domains and levels Value
General health
Mean (SD) 52.6 (22.4)
Min–max (5–100)
Vitality/energy
Mean (SD) 64.5 (19.1)
Min–max (10–100)
Social functioning
Mean (SD) 74.1 (22.8)
Min–max (12.5–100)
Role–emotional
Mean (SD) 71.7 (39.7)
Min–max (0–100)
Mental health
Mean (SD) 70.0 (17.7)
Min–max (28–100)
Physical component summary
Mean (SD) 47.0 (8.3)
Min–max (23.2–59.3)
Mental component summary
Mean (SD) 45.0 (8.7)
Min–max (24.0–62.14)
Table 5. Costs of ICT and transfusions according to patients’ age
Patients’ age range E per patient-month
for ICT* mean (min–max)
E per patient-month for
transfusions mean (min–max)
510 years old 348.06 (194.45–497.52) 259.95 (185.25–353.92)
10–15 years old 583.64 (243.74–1400.71) 402.75 (199.38–743.87)
16–25 years old 677.85 (267.41–1472.64) 405.32 (140.40–806.55)
26–35 years old 771.64 (329.28–1331.79) 383.18 (174.04–1410.02)
435 years old 661.27 (280.63–1157.63) 543.38 (127.73–1696.80)
* Any regimen, including costs of administration
� 2008 Informa UK - Curr Med Res Opin 2008; 24(07) Costs and outcomes in �-TM patients undergoing ICT Scalone et al. 1913
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

Side Effects of ICT (mean¼ 3.6). Acceptance of ICT
was the lowest mean score (mean¼ 3.4) indicating
positive orientations towards ICT relating to expecta-
tions and convenience.
Concerning the items to measure compliance, the
mean score for ‘thinking about stopping ICT’ was 4.6
(with 1 meaning ‘always’, 5 meaning ‘never’), the mean
score for ‘following the ICT as directed by the doctor’
was 1.6, and the mean for ‘having troubles remember-
ing to take the ICT’ was 4.2.
Discussion
Although a number of studies have allowed the estima-
tion of direct costs, or more specifically ICT costs, or
compared costs and efficacy of alternative treatment
options, no information was available, to our knowl-
edge, on the overall impact attributable to �-TM and
its management from the societal perspective. The
ITHACA study was a naturalistic study conducted to
estimate the overall societal costs attributable to �-TM
and current medical strategies adopted for transfusions
and ICT. According to its objective, the technique
adopted for this study is in its nature not for making
comparisons between alternative options (as for
instance with cost-effective analyses), but for observing
the impact attributable to the disease and current
clinical practice adopted to manage the patients.
Total direct costs were estimated to correspond to an
average of E1242/patient/month from the societal
point of view. If multiplied by the number of patients
with transfusion dependent TM patients in Italy,
who are approximately 7000 persons, the total
societal direct costs corresponds to almost E107
million per year over the Italian society or, in other
terms corresponds to a cost of almost E2 per Italian
citizen per year. Fifty-six percent of direct costs is
attributable to ICT (E60 million per year) and 33%
to transfusions (E35 million per year). Treatment
with deferoxamine is 60–65% more expensive than
treatment with deferiprone, depending on the regimen
followed by the patients. The distribution of direct
costs is highly right skewed, showing that one third of
the sample cost less than E1000, almost 50% cost
between E1000 and E1500 per month, while 20%,
less than a quarter of the sample, cost E2000 per
month or more, this contributing to the high levels of
direct total costs attributable to the management of this
category of patients. Despite a slight relationship of
mean costs with age, the skewed distribution appears
to be mostly dependent on other factors, like the
patients’ clinical conditions or the treatment regimen
adopted, according to the physicians’ decisions or
patients’ requests.
Regarding indirect costs, one main point to be noted
is that one fourth of the sample declared to be
pensioned, early retired, or not able to work because
of their health status. Furthermore, patients reported a
high percentage of absenteeism and experienced sub-
stantial difficulties while working, participating at
school activities, or doing other usual activities.
Overall a percentage of 10–14% of productivity was
lost by the study sample. Among patients younger
than 16 years of age, while a high percentage of
youths missed a number of schooldays, an apparent
lower amount of time was lost in terms of regular activ-
ities. It is worth noting, in this regard, the possible
underestimate of the true loss of productivity in this
category of patients: children often go to medical
visits for their disease during school-time while other
Men
0
10
20
30
40
50
60
PCS MCS
ITHACA (aged 14–48 years; N = 60)
Italian population (aged 18–54 years; N = 621)
Moderate to severe hemophilia patients withoutinhibitors aged 18–49 years; N =178 (COCHE Study)
Moderate to severe hemophilia patients with inhibitors,aged 15–48 years; N = 42 (COCIS Study)
Women
0
10
20
30
40
50
60
PCS MCS
ITHACA (aged 14–48 years; N = 60)
Italian population (aged 18–54 years; N = 621)
(A) (B)
Figure 2. Comparison of physical and mental summary components of HRQoL from the SF-36, between �-TM, hemophilia
patients and general population comparable for age and sex
1914 Costs and outcomes in �-TM patients undergoing ICT � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(07)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

activities (e.g., sport) take place outside the physicians’
normal working time.
For instance, although no information was available
on the specific reasons of loss of productivity, like going
to the hospital for transfusions or to the physician’s
office to monitor and manage complications, or receiv-
ing infusions for ICT, the participating physicians
suggested that most of this loss was attributable to the
necessity to reach hospitals or other places for visits,
transfusions, surgical interventions etc, which can also
require a lot of travel time, above all among patients
living in places far from the clinical centers (e.g., rural
areas). By contrast, infusions for chelation therapy are
mostly administered at home, when the patient is more
available, for instance during the night. As a conse-
quence, it is likely that the respondents did not consider
the time spent for infusions (on average 11 h per infu-
sion) as lost in terms of productivity. Another possible
interpretation is that not all children carry out, outside
their school-time, specific activities such as sport: they
probably did not consider missing activities for their
disease simply because they did not have to give up
any of them. Hence, this estimate should be considered
as conservative, although it does show that a high
amount of productivity was lost by both adult and
pediatric patients and, when present, by their care-
givers. This cost significantly contributes to the high
overall cost of this illness and is, therefore, an issue
that the health care system should take into considera-
tion to increase the efficiency of treatment strategies.
In general, the current health state perception among
�-TM patients undergoing transfusions and ICT was
impaired if compared to the one among the general
population, comparable for age and sex: reasons of
poor wellbeing can be attributed both to the disease
and to the treatment that patients receive and that can
be perceived cumbersome and not satisfactory. In fact
the patients reported, in general, non-optimal levels of
satisfaction with their ICT (with deferoxamine, defer-
iprone or combination of the 2 drugs): while on average
the patients were satisfied with the perceived effective-
ness of the therapy, lower levels of satisfaction were
reported as regards other aspects related to ICT, in par-
ticular they were on average poorly satisfied with the
convenience of ICT, the perception of side effects, and
of the burden attributable to the regimen treatment.
These results suggest that despite the clinical benefits
derived from the current medical interventions, which
have improved survival and reduced the risk and sever-
ity of complications, dealing with things like for
instance, way, duration and frequency of administra-
tions, perception of pain, consequent limitations
on doing daily activities and having a normal life, can
actually contribute to reduce patients’ wellbeing.
A consequence of this can be a poor compliance with
treatment, with a likely impairment of the overall real
benefits of the treatment. The patients participating in
this study declared, in general, to be adherent to the
prescribed ICT at enrolment. It should be remembered
in this regard that only patients undergoing ICT from at
least 3 years were eligible for this study: it is possible
that those who were more compliant and for this reason
were receiving the ICT for a relatively longer period,
actually participated in this study. This might be the
cause of an overestimate of the levels of satisfaction of
ICT among the overall target population. However, it
must be noted that 14% of patients actually changed
the regimen of treatment: this may correspond to a
result of poor compliance or, in the case of switching
to combined therapy, may correspond to a clinical need
of intensive chelation.
In fact, different reasons for changing the drug or the
dosage were reported by the physicians participating
in the study, like ferritin levels, but also the patients’
compliance, which caused the physicians’ decision or
even the patients’ request to change dosage or drug.
Physicians in general decided to switch from a mono-
therapy to a combined therapy when they recognized
that their patients needed intensive chelation therapy
due to severe iron overload, while switched to mono-
therapy when the iron overload was less severe.
According to the results of a recent literature review
of 18 studies on compliance with deferoxamine com-
pared with deferiprone therapy33, the compliance may
improve with an oral drug, which is easier and quicker
to be administered. Poor compliance with ICT results in
increased risk of cardiac disease and endocrinopathies,
as well as lower survival, with the additional
consequence of increased overall costs. One point that
is worth noting, however, is that what was observed in
our study could also be a consequence of the absence of
a standardized, homogeneous, agreed procedure and
the presence of different approaches decided by the
physicians, according to their personal experience and
opinions. In fact, the first recommendations on how to
optimally manage TM patients have only recently been
published, by the Italian Society of Hematology34.
The results of the ITHACA study show that the
current clinical practice allows, although at high costs,
transfusion dependent �-TM patients to receive effica-
cious treatment based on transfusions and iron chela-
tion therapy. However, optimal benefits have not been
reached yet, as shown by the results in terms of
HRQoL, satisfaction, and attitude toward ICT. This
picture of the current medical practice highlights the
necessity of further efforts aimed at improving patients’
acceptance and satisfaction with their therapy35, in
order to increase their compliance, hence to improve
� 2008 Informa UK - Curr Med Res Opin 2008; 24(07) Costs and outcomes in �-TM patients undergoing ICT Scalone et al. 1915
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

the effectiveness of treatment. As a result of a better
compliance with and acceptance of the prescribed ICT,
the treatment can be expected to be more successful in
reducing iron overload in these patients and improving
their clinical status and overall wellbeing. As a further
consequence, a likely reduction of both direct and
indirect costs, for instance, an optimization of resources
allocation, can be expected for the health care system
and overall society’s benefit.
One potential limitation of this study is
attributable to the fact that only a sample of Italian
patients were involved: however, we do not have ele-
ments suggesting that the results of the ITHACA
cannot be considered valid in other populations of
patients with similar characteristics as those participat-
ing in this study. It is worth noticing that possible
differences may be present in the values expressed in
monetary terms, depending on possible different payers
for the healthcare services (e.g., insurances rather
than the National Health Service) in the different
countries, and/or on the different prices or tariffs
applied. However, the amount of the resources
adsorbed are reported and could be used for compari-
sons or projections.
Conclusion
The ITHACA study shows that the modern strategies
applied to manage �-TM patients undergoing transfu-
sions and ICT generates high costs to society but are
efficacious in clinical terms, even though optimal levels
of benefits have still to be reached, in terms of treat-
ment satisfaction and overall wellbeing. Efforts must be
made to improve patients’ acceptance and satisfaction
with their therapies, in order to increase their compli-
ance, to improve the effectiveness of treatment, hence
the patients’ general wellbeing. This would allow a
more appropriate use of the resources. In particular,
a more flexible regimen for ICT, such as an oral treat-
ment, adhering to good levels of safety, can be consid-
ered an objective to be reached, in order to ensure that
patients can receive a therapy they can comply with.
This objective may well be reached by the introduction
of a new oral iron chelator agent, deferasirox, of which
promising results have been shown in a randomized
phase III trial35, although these still need to be con-
firmed with further research and real use in clinical
practice.
As a result of a better accepted therapy, higher clin-
ical and perceived benefits can be expected, with pos-
sible positive consequences on the perspective of both
the National Health Service (the main payer, in Italy,
for direct costs), patients and their families, who mostly
pay for loss of productivity (indirect costs) and
wellbeing (intangible costs).
Further research is now advocated to compare the
overall costs and consequences attributable to the avail-
able options, with the specific objective to identify and
to inform decision makers about the most efficient
strategy to adopt in this category of patients.
Acknowledgments
Declaration of interest: An unrestricted grant was
provided by Novartis Pharmaceutical Corporation,
East Hanover, NJ, USA, for this study.
L.G.M. and M.D.C. designed the study. S.R. mana-
ged the collection of the data from the participating
centers. S.R., L.S., M.K., and D.R. analyzed the data.
L.S., M.D.C., L.G.M. wrote the paper. M.B., C.B-P.,
C/B P.C., D.G., L. P., I.S, S.R., M.K., and D.R.
reviewed and integrated the paper by adding further
information that helped to interpret the results. The
other co-investigators, listed as ITHACA study group
members, contributed with the collection of the data.
The views expressed in the paper are those of the
authors.
We thank the patients and caregivers who took part
in this study. Thanks also to Dr. Jean-Francois Baladi.
Other ITHACA study group members were:
M. Capra, L. Cuccia, from U.O.C. Ematologia –
Emoglobinopatie, A.R.N.A.S. Civico, Di Cristina,
Ascoli – Palermo; F. Sorrentino, from Ospedale
S. Eugenio – Centro Microcitemie DH talassemia
Roma; M. Viala, from Mapi Valued Questionnaire
Design and Validation Unit – Bollington, Cheshire,
UK; C. Uyl-de Groot, from Institute for Medical
Technology Assessment, Erasmus Medical Centre,
Rotterdam, The Netherlands.
The results of this study have been presented
at a national and some international Congresses:
poster at The 11th EHA Congress, Amsterdam
(The Netherlands) June 15–18, 2006; posters at The
9th Annual European Congress of ISPOR,
Copenhagen (Denmark), October 29–31, 2006; oral
presentation at The IV National Congress of SOSTE
(Societa per lo Studio delle Talassemie ed
Emoglobinemie), Rome (Italy), November 18–19,
2006; posters at The ASH Congress, Orlando (USA),
December 9–12, 2006.
References1. Wolman IJ. Transfusion therapy in Cooley’s anemia: growth and
health as related to long-range hemoglobin levels, a progressreport. Ann NY Acad Sci 1964;119:736-52
1916 Costs and outcomes in �-TM patients undergoing ICT � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(07)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.

2. Piomelli S, Danoff SJ, Becker MH, et al. Prevention of bonemalformations and cardiomegaly in Cooley’s anemia by earlyhypertransfusion regimen. Ann NY Acad Sci 1969;165:427-36
3. Barry M, Flynn DN, Letsky EA, et al. Long-term chelation ther-apy in thalassemia major: effect on liver iron concentration, liverhistology and clinical progress. Br Med J 1974;2:16-20
4. Hussain MA, Green N, Flynn DM, et al. Subcutaneous infusionand intramuscular injection of desferrioxamine in patients withtransfusional iron overload. Lancet 1976;2:1278-80
5. Modell CB, Beck J. Long-term desferrioxamine therapy inthalassemia. Ann NY Acad Sci 1974;232:201-10
6. Zurlo MG, De Stefano P, Borgna-Pignatti C, et al. Survival andcauses of death in thalassaemia major. Lancet 1989;8653:27-30
7. Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survival andcomplications in patients with thalassemia major treated withtransfusion and deferoxamine. Haematologica 2004;89:1187-93
8. Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survival anddisease complications in thalassemia major. Ann NY Acad Sci1998;850:227-31
9. Olivieri NF, Nathan DG, MacMillan JH, et al. Survival in medi-cally treated patients with homozygous �-thalassemia. NewEngl J Med 1994;331:574-8
10. Cohen AR, Galanello R, Piga V, et al. Safety and effectivenessof long-term therapy with the oral iron chelator deferiprone.Blood 2003;102:1583-7
11. Piga A, Gaglioti C, Fogliacco E, et al. Comparative effects ofdeferiprone and deferoxamine on survival and cardiac disease inpatients with thalassemia major: a retrospective analysis.Haematologica 2003;88:489-96
12. Pennell DJ, Berdoukas V, Karagiorga M, et al. Randomizedcontrolled trial of deferiprone or deferoxamine in �-thalassemiamajor patients with asymptomatic myocardial siderosis. Blood2006;107:3738-44
13. Tanner MA, Galanello R, Dessi C, et al. A randomized, placebo-controlled, double-blind trial of the effect of combined therapywith deferoxamine and deferiprone on myocardial iron inthalassemia major using cardiovascular magnetic resonance.Circulation 2007;115:1876-84
14. Cappellini MD, Cohen A, Piga A, et al. A phase 3 study ofdeferasirox (ICL670), a once-daily oral iron chelator, in patientswith beta-thalassemia. Blood 2006;107:3455-62
15. Woods K, Karrison T, Koshy M, et al. Hospital utilizationpatterns and costs for adult sickle cell patients in Illinois.Public Health Rep 1997;112:44-51
16. Ginsberg G, Tulchinsky T, Filon D, et al. Cost benefit analysis ofa national thalassaemia prevention programme in Israel. J MedScreen 1998;5:120-6
17. Nietert PJ, Abboud MR, Zoller JS, et al. Costs, charges, andreimbursements for persons with sickle cell disease. J PediatrHematol Oncol 1999;21:389-96
18. Karnon J, Zeuner D, Brown J, et al. Lifetime treatment costs ofbeta-thalassaemia major. Clin Lab Haematol 1999;21:377-85
19. Wayne AS, Schoenike SE, Pegelow CH. Financial analysis ofchronic transfusion for stroke prevention in sickle cell disease.Blood 2000;96:2369-72
20. Mayer ML, Konrad TR, Dvorak CC. Hospital resource utiliza-tion among patients with sickle cell disease. J Health Care PoorUnderserved 2003;14:122-35
21. Desrosiers MP, Payne K, Proskorovsky I, et al. Estimated totalannual costs of infused iron chelation therapy in the United
Kingdom. Poster presented at the 11th Congress of the
European Hematology Association (EHA). Abstract 0810 pub-
lished in Haematologica/The Hematology Journal 2006;91(s1),
(EHA), Amsterdam, The Netherlands, 17th June 200622. Brun-Strang C, Bachir D, De Montalembert M, et al. Socio-
economic impact of infused iron chelation therapy in France:
ISOSFER study results. Poster presented at the American
Society of Hematology (ASH) Congress in 2006. Abstract
3354 published in Blood| 2006;108, 48th Annual Congress,
Orlando, Florida, US, 9-11 December 200623. Drummond MF, O’Brien B, Stoddart GL, et al. Methods for the
economic evaluation of health care programmes. Oxford (UK):
Oxford University Press; 199724. Van Roijen L, Essink-Bot ML, Koopmanschap MA, et al. Labor
and health status in economic evaluation of health care. The
Health and Labor Questionnaire. Int J Technol Assess Health
Care 1996;12:405-1525. Ware Jr J, Kosinski M, Keller SD. SF-36 physical and mental
health summary scales: a user’s manual. Boston (MA): The
Health Institute; 199426. Ware Jr J, Gandek B, Kosinski M, et al. The equivalence of SF-36
summary health scores estimated using standard and country-
specific algorithms in 10 countries: results from the IQOLA
project [International Quality of Life Assessment]. J Clin
Epidemiol 1998;51:1167-7027. Brooks R. Euroqol: the current state of play. Health Policy
1996;37:53-7228. Apolone G, Mosconi P, Ware Jr JE. Questionario sullo Stato di
Salute SF-36. Manuale d’uso e guida all’interpretazione dei
risultati. Milano (Italy): Guerini e Associati; 199729. Gringeri A, Mantovani LG, Scalone L, et al. Cost of care and
quality of life for patients with haemophilia complicated by
inhibitors: the COCIS Study Group. Blood 2003;102:2358-6330. Mantovani LG, Scalone L, Mannucci PM, et al. The cost of care
of hemophilic patients without inhibitors: the COCHE study.
Poster presented at the World Federation of Hemophilia
(WFH) Congress in 2006. Abstract 28 PO 880, published in
Haemophilia| 2006;12(S2):133–531. Abetz L, Baladi JF, Jones P, et al. The development of a
treatment satisfaction questionnaire for iron overload (IO)
patients on chelation therapy (CT). International Society
for Pharmacoeconomics and Outcomes Research 8th
Annual European Congress, November 6–8, 2005;
Florence, Italy. Abstract n. PMC27 published in Value in
Health 2005;8;A7232. Cronbach LJ. Coefficient alpha and the internal structure of
tests. Psychometrika 1951;16:297-33433. Delea TE, Edelsberg J, Sofrygin O, et al. Consequences and
costs of non-compliance with iron chelation therapy in patients
with transfusion-dependent thalassemia: a literature review.
Transfusion 2007;47:1919-2934. Angelucci E, Barosi G, Camaschella C, et al. Italian Society of
Hematology practice guidelines for the management of iron
overload in thalassemia major and related disorders.
Haematologica 2008;93:1-1235. Cappellini MD, Bejaoui M, Agaoglu L, et al. Prospective
evaluation of patient-reported outcomes during treatment
with deferasirox or deferoxamine for iron overload in patients
with beta-thalassemia. Clin Ther 2007;29:909-17
CrossRef links are available in the online published version of this paper:
http://www.cmrojournal.com
Paper CMRO-4215_5, Accepted for publication: 25 April 2008
Published Online: 27 May 2008
doi:10.1185/03007990802160834
� 2008 Informa UK - Curr Med Res Opin 2008; 24(07) Costs and outcomes in �-TM patients undergoing ICT Scalone et al. 1917
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f H
ong
Kon
g on
09/
17/1
3Fo
r pe
rson
al u
se o
nly.