Cosmetic Surgical Anatomy of the Ligamentous Attachments ... · PDF fileSurgical Anatomy of...
16
Cosmetic Surgical Anatomy of the Ligamentous Attachments in the Temple and Periorbital Regions Christopher J. Moss, M.B., B.S., F.R.A.C.S., Dip.Anat., Bryan C. Mendelson, F.R.C.S.(E), F.R.A.C.S., F.A.C.S., and G. Ian Taylor, F.R.C.S., F.R.A.C.S., M.D. Melbourne, Australia This study documents the anatomy of the deep attach- ments of the superficial fasciae within the temporal and periorbital regions. A highly organized and consistent three-dimensional connective tissue framework supports the overlying skin and soft tissues in these areas. The regional nerves and vessels display constant and predictable relationships with both the fascial planes and their ligamentous attachments. Knowledge of these rela- tionships allows the surgeon to use the tissue planes and soft-tissue ligaments as intraoperative landmarks for the vital neurovascular structures. This results in improved efficiency and safety for aesthetic procedures in these regions. (Plast. Reconstr. Surg. 105: 1475, 2000.) The patterns of arrangement of the layers of superficial fascia in the cheek, 1–9 forehead, 10 –13 scalp, 14 and temple 15,16 have been well de- scribed. This superficial fascia in the temple, forehead, and periorbital regions meets the definition of a SMAS layer as described in the midface. 1 The superficial fascia thus extends like a mask throughout the whole of the face. The descriptions of these layers have found wide application to aesthetic surgery. 17–19 The areolar tissue plane beneath the fibrous layer of the superficial fascia of the temple has been given numerous names. 14,20 A subsuperfi- cial fascial plane is located deep to the galea in the upper face, the SMAS in the midface, and the platysma in the neck. The ease of dissec- tion along this plane in the scalp and forehead results from the relative paucity of connective tissue attachments between the galea and the underlying deep fascia or pericranium. The superficial fascial layer is retained by a complex system of deep attachments that arise from the underlying deep fascia/periosteum. The subSMAS plane that contains these attach- ments is therefore not always a simple cleavage plane. This explains why surgical dissection is considerably more complicated in the midfa- cial, temporal, and periorbital regions than in the scalp. In the cheek, these deep attachments have been defined as the zygomatic, masseteric, and mandibular-cutaneous ligaments. 21,22 These lig- aments provide a lateral line of fixation for the mobile tissues of the medial cheek. Release of these retaining ligaments is fundamental to the extended SMAS technique of “deep-plane” sur- gery. 18,19,23,24 The ligaments act as markers to the position of the facial nerve branches in the cheek. 19 The zygomatic and buccal branches emerge from the masseteric fascia and cross the subSMAS plane to the underside of the SMAS. This pas- sage occurs just medial to the cheek ligaments. The ligaments therefore retain the overlying SMAS and protect the facial nerve branches as they cross this glide plane. In facial rejuvenation surgery, the deep- plane method achieves a tightening of the me- dial cheek soft tissues. After the retaining liga- ments are released, the superficial fascia can be drawn posteriorly. The facial nerve branches are simultaneously identified and preserved during surgical ligament release. Previous authors have provided a great deal Dr. Taylor is from the Department of Plastic and Reconstructive Surgery at the Royal Melbourne Hospital. Received for publication June 1, 1999; revised August 27, 1999. Presented at the 30th Scientific Congress of the American Society for Aesthetic Plastic Surgery, in New York, New York, on May 3, 1997. 1475
Transcript of Cosmetic Surgical Anatomy of the Ligamentous Attachments ... · PDF fileSurgical Anatomy of...

Cosmetic
Surgical Anatomy of the LigamentousAttachments in the Temple and PeriorbitalRegionsChristopher J. Moss, M.B., B.S., F.R.A.C.S., Dip.Anat.,Bryan C. Mendelson, F.R.C.S.(E), F.R.A.C.S., F.A.C.S., and G. Ian Taylor, F.R.C.S., F.R.A.C.S., M.D.Melbourne, Australia
This study documents the anatomy of the deep attach-ments of the superficial fasciae within the temporal andperiorbital regions. A highly organized and consistentthree-dimensional connective tissue framework supportsthe overlying skin and soft tissues in these areas.
The regional nerves and vessels display constant andpredictable relationships with both the fascial planes andtheir ligamentous attachments. Knowledge of these rela-tionships allows the surgeon to use the tissue planes andsoft-tissue ligaments as intraoperative landmarks for thevital neurovascular structures. This results in improvedefficiency and safety for aesthetic procedures in theseregions. (Plast. Reconstr. Surg. 105: 1475, 2000.)
The patterns of arrangement of the layers ofsuperficial fascia in the cheek,1–9 forehead,10–13
scalp,14 and temple15,16 have been well de-scribed. This superficial fascia in the temple,forehead, and periorbital regions meets thedefinition of a SMAS layer as described in themidface.1 The superficial fascia thus extendslike a mask throughout the whole of the face.The descriptions of these layers have foundwide application to aesthetic surgery.17–19
The areolar tissue plane beneath the fibrouslayer of the superficial fascia of the temple hasbeen given numerous names.14,20 A subsuperfi-cial fascial plane is located deep to the galea inthe upper face, the SMAS in the midface, andthe platysma in the neck. The ease of dissec-tion along this plane in the scalp and foreheadresults from the relative paucity of connectivetissue attachments between the galea and theunderlying deep fascia or pericranium.
The superficial fascial layer is retained by a
complex system of deep attachments that arisefrom the underlying deep fascia/periosteum.The subSMAS plane that contains these attach-ments is therefore not always a simple cleavageplane. This explains why surgical dissection isconsiderably more complicated in the midfa-cial, temporal, and periorbital regions than inthe scalp.
In the cheek, these deep attachments havebeen defined as the zygomatic, masseteric, andmandibular-cutaneous ligaments.21,22 These lig-aments provide a lateral line of fixation for themobile tissues of the medial cheek. Release ofthese retaining ligaments is fundamental to theextended SMAS technique of “deep-plane” sur-gery.18,19,23,24
The ligaments act as markers to the positionof the facial nerve branches in the cheek.19 Thezygomatic and buccal branches emerge fromthe masseteric fascia and cross the subSMASplane to the underside of the SMAS. This pas-sage occurs just medial to the cheek ligaments.The ligaments therefore retain the overlyingSMAS and protect the facial nerve branches asthey cross this glide plane.
In facial rejuvenation surgery, the deep-plane method achieves a tightening of the me-dial cheek soft tissues. After the retaining liga-ments are released, the superficial fascia can bedrawn posteriorly. The facial nerve branchesare simultaneously identified and preservedduring surgical ligament release.
Previous authors have provided a great deal
Dr. Taylor is from the Department of Plastic and Reconstructive Surgery at the Royal Melbourne Hospital. Received for publication June 1,1999; revised August 27, 1999.
Presented at the 30th Scientific Congress of the American Society for Aesthetic Plastic Surgery, in New York, New York, on May 3, 1997.
1475

of information on the deep attachments in thecheek.18,21 Recently, studies have begun to in-vestigate deep attachments found in the tem-poral12,25 and periorbital regions.26,27 These ar-eas are therefore the focus of this article.
The origin and pattern of migration of theembryonic facial muscles that occur in the mid-face also occur in the upper face.28,29 Accord-ingly, it could be expected that the upper facewould display similar tissue and neurovasculararrangements.
The relationships of the facial nerve16,30–32
and sensory nerves33 to the fascial planes in theupper face have received much attention. Al-though helpful in identifying the layer of pas-sage of the facial nerve branches, these studiesdo not define their exact course. Currently,surface anatomy landmarks are widely used inlocating the facial nerve.34,35 However, surfaceanatomy is not sufficiently precise for intraop-erative dissection when facial nerve branchesare involved.
This investigation commenced with the hy-pothesis that, as in the cheek, the internal soft-tissue ligaments of the temporal and perior-bital regions display a constant anatomy withpredictable relationships to the temporalbranches of the facial nerve. The aim of thestudy was therefore to define this not previ-ously described anatomy. Although the datareported in this article pertain only to the tem-poral and periorbital regions, they are derivedfrom a comprehensive study investigating thesuperficial tissues of the whole face and neck.
MATERIALS AND METHODS
This study involved dissection of 22 facialhalves. All were performed on fresh cadavers ofnormal body mass index with ages rangingfrom 60 to 78 years. Preserved (formalinized)cadavers were excluded because they distortedthe delicate connective tissue and facial nerveanatomy. Of the 22 dissections, 10 were per-formed following intraarterial vascular injec-tion with a lead oxide mixture36,37 and 12 wereperformed in fresh specimens without arterialinjection. These data were combined with theanatomic recordings from several hundred in-traoperative dissections including open coro-nal brow and temporal lifts and endoscopictemple lifts.
Dissection was performed under 33 loupemagnification according to a standardizedtechnique that commenced with a coronal in-cision, entered the subgalea plane, and then
proceeded in a caudal direction over the fore-head and the temporal, periorbital, and facialregions. Loose areolar tissue was gently dis-sected away, preserving the dense connectivetissue attachments between the deep and su-perficial tissues. The precise locations of theseattachments were recorded on a standardizedworksheet with reference to specific fixed bonylandmarks. The relationships of the major neu-rovascular structures to both the connectivetissue attachments and the fixed skeletal land-marks were documented carefully with appro-priate measurements.
The cadavers that underwent initial vascularinjection were dissected with an identical tech-nique and provided additional information onthe relationships between the arterial supplyand both the connective tissue layers and theirattachments. The uninjected specimens pro-vided detailed information on the cutaneoussensory nerves and fine motor branches of thefacial nerve.
RESULTS
Arrangement of the Tissue Layers
The tissues are arranged into two basic layersthat may be summarized under the headings ofthe superficial and the deep fasciae. A contin-uous layer of superficial fascia comprises thegalea occipitofrontalis, the superficial tempo-ral fascia, the SMAS of the zygomatic andcheek regions, and the platysma. This SMASsystem receives the insertion of those facialmuscles arising directly from bone such as thezygomaticus major and minor; it also envelopsthe flat muscles such as orbicularis oculi thathave important attachments around their pe-rimeter to the SMAS layers.
An easily developed surgical plane exists be-tween these deep and superficial tissue planes.This subsuperficial fascial plane is a potentialspace that mainly contains loose areolar orfibro-fatty tissue. In predictable locations, dis-section through this plane is limited by thefibrous and muscular attachments that retainthe superficial tissues.
Classification of Ligament Morphology
The fibrous attachments retaining the SMASlayer and skin to the deep tissues may be col-lectively referred to as the ligamentous attach-ments of the superficial tissues. The individualligaments have predictable and constant loca-
1476 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

tions; however, they vary in the density of theirfibrous tissue.
Clear description of the ligamentous anat-omy in the superficial tissues of the head andneck has required the introduction of a num-ber of new terms. The ligaments have beenclassified according to three morphologicalforms: true ligaments, septa, and adhesions(Fig. 1).
True ligament. A true ligament is similar to askeletal ligament in that it is a discrete cylin-
drical arrangement of fibrous tissue that is sur-rounded by fatty tissue. True ligaments werefound in the medial midface and lower face andprovided the greatest latitude of movement ofall the attachments (Fig. 1). True ligamentsarise from either the deep fascia or the perios-teum. They then cross the subSMAS plane tothe undersurface of the SMAS, where they di-vide into numerous branches in a tree-like fash-ion. These branches then distribute the attach-ment of the ligament to the dermis through a
FIG. 1. Classification of ligamentous morphology. The major tissue planes from deep tosuperficial include the deep fascia/pericranium, the subSMAS plane, the SMAS/galea, subcu-taneous tissue, and the skin. The diagram shows the three morphologic forms of ligaments thatpass through the subSMAS plane to the superficial tissues. These are classified into true ligaments,septa, and adhesions.
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1477

subcutaneous fascial system, the retinacula cu-tis.9,14,38 Examples include the zygomatic andmasseteric ligaments (Fig. 1).
Septum. A septum is a fibrous wall passingbetween the deep fascia and the undersurfaceof the SMAS (Fig. 1). This arrangement permitsmobility only in a plane perpendicular to thedeep line of attachment of the septum. Most ofthe septa defined within the head and neck arelocated in the temporal and periorbital regions.Examples include the inferior temporal sep-tum, the superior temporal septum, and theperiorbital septum (Fig. 1).
Adhesion. The third form is a low-densityarea of fibrous or fibro-fatty adhesion betweenthe deep fascia/pericranium and the superfi-cial fascia (Fig. 1). Basically a two-dimensionalstructure, an adhesion restricts mobility in alldirections and to the greatest degree of thethree forms. It is important to note that septa
and adhesions retain the SMAS plane only, andconsiderable mobility may still occur at moresuperficial layers. Aside from the preauricularand parotid regions, adhesions were found onlyin the forehead and temporal regions. Exam-ples include the temporal (Fig. 1) and the su-praorbital ligamentous adhesions.
The deep attachments of the superficial fas-cia in the temporal and periorbital regionscomprised only septa and adhesions. No trueligaments were seen in these regions.
The Temporal Ligamentous Adhesion
The temporal ligamentous adhesion (tem-poral ligament) supports the region immedi-ately superior to the eyebrow at the junction ofits middle and lateral thirds (Figs. 2 and 3).Located at the intersection of the temporal,frontal, and periorbital regions, it is a well-
FIG. 2. Periorbital and temporal ligamentous attachments with major neurovascular rela-tionships: lateral view. Temporal ligamentous adhesion (TLA), supraorbital ligamentous adhe-sion (SLA), superior temporal septum (STS), inferior temporal septum (ITS), periorbital septum(PS), lateral brow thickening of periorbital septum (LBT), lateral orbital thickening of perior-bital septum (LOT), sentinel vessel (SV), temporal branches of facial nerve (TFN), zygomati-cotemporal nerve (ZTN), zygomaticofacial nerve (ZFN).
1478 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

FIG. 3. Periorbital and temporal ligamentous attachments with major neurovascular rela-tionships: anterior view. Temporal ligamentous adhesion (TLA), supraorbital ligamentous ad-hesion (SLA), superior temporal septum (STS), inferior temporal septum (ITS), periorbitalseptum (PS), lateral brow thickening of periorbital septum (LBT), lateral orbital thickening ofperiorbital septum (LOT), sentinel vessel (SV), temporal branches of facial nerve (TFN), zy-gomaticotemporal nerve (ZTN), zygomaticofacial nerve (ZFN).
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1479

defined keystone structure in that three liga-ments radiate from each of its angles. Theseare the superior temporal septum, the inferiortemporal septum, and the supraorbital adhe-sion (Figs. 4 through 6). The temporal liga-ment arises from the frontal bone periosteumas an expansion at the anterior end of thesuperior temporal septum.
The temporal ligament inserts into the su-perficial fascia at the junction of the superficialtemporal fascia and the galea on the deepsurface of the frontalis muscle (Fig. 4). Thisligament is approximately 20 mm high and 15mm at its base (Fig. 3). It allows 6 mm of
horizontal mobility of the overlying galeal lay-ers. The base is located parallel to the arcusmarginalis of the orbital rim at a distance of 10mm above it.
The superior temporal septum. This septumarises from the periosteum along the superiortemporal line of the skull and inserts into theline of junction between the superficial tempo-ral fascia and the galea (Fig. 1). Anteriorly, thisline of junction occurs between the superficialtemporal fascia and the galea lining the deepsurface of the lateral border of the frontalismuscle. Whereas it more closely resembles aseptum posteriorly, it becomes a broad adhe-
FIG. 4. Right temple. Subject’s nose is to the right. Hairline incision across the forehead with retraction of the flap. Theretractor is in the superficial temporal fascia (STF). The scissors are releasing the temporal ligamentous adhesion (TLA) at theanterior end of the superior temporal septum (STS), which separates the frontal periosteum (FP) medially from the deeptemporal fascia (DTP) laterally. The superior extension of the temporal ligamentous adhesion is the superior temporal septum(STS). The location of the deep and superficial attachments of the inferior temporal septum (ITS) are defined by the line ofthe fine blue suture.
FIG. 5. Further elevation of the superficial fascia, deep to the superficial temporal fascia (STF), by releasing the inferiortemporal septum. The temple is divided into two parts by the line of attachment of the inferior temporal septum. Above, novital anatomy is present. In the lower compartment lies the detailed neurovascular anatomy. This contains lobulated fat on thefloor. Unnamed minor ligamentous attachments (marked with blue ink) are seen centrally and related to the emerging branchesof the zygomaticotemporal nerve (ZTN, yellow beads). The sentinel vessel (SV) crosses the lower temporal compartment inferiorto the inferior temporal septum (ITS) just posterior to the frontal process of the zygoma. The green background and green beadsdisplay the temporal branches of the facial nerve (TFN) within the fatty layer deep to the superficial temporal fascia, which formsthe roof of the triangular compartment. The dotted blue line demarcates the upper border of the supraorbital ligamentous adhesion(SLA).
1480 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

sion at its anterior termination 30 mm from thesupraorbital rim. This expanded end is the tem-poral ligamentous adhesion (Figs. 2 and 4).
The inferior temporal septum. This septumtakes an oblique course along a line extendingfrom the lateral corner of the temporal liga-ment toward the external acoustic meatus (Fig.1). It comprises criss-crossed fibers that reflectfrom the deep temporal fascia to their insertioninto the deepest layers of the superficial tem-poral fascia (Figs. 7 and 8).
The septum is found an average of 27 mmabove the zygoma at the level of the temporalborder of the frontal process of the zygomaand 21 mm above the superior border of thezygoma at its midportion. The average heightsfor the level of the division of the deep tempo-ral fascia into its deep and superficial leaves are37 mm and 27 mm above the zygoma, respec-tively. The division of the deep temporal fasciainto superficial and deep leaves is thereforeabove the level of the inferior temporal sep-tum.
The inferior temporal septum forms the su-perior border of a triangular fibro-fatty com-partment between the superficial temporal fas-cia and the underlying deep temporal fascia(Fig. 6). Cephalad to this septum is an easilydeveloped dissection plane beneath the super-ficial temporal fascia. Within the lower tempo-ral (triangular) compartment, the planes aremore adherent because of numerous fine, fi-brous adhesions contained within a variableamount of adipose tissue. These fibrousstrands have related vessels and cutaneousnerve branches (Figs. 5 and 9 through 12).Inferiorly these fibrous attachments becomeincreasingly condensed. At the level of the
lower zygoma they comprise the named zygo-matic (true) ligaments.
The supraorbital (ligamentous) adhesion. Thedensity of this fibrous adhesion varies widely.The more dense adhesions maintain a greaterrestraining effect on the superficial fascia of thebrow, thus reducing brow mobility.
The supraorbital ligamentous adhesionarises from the frontal bone above the orbitalrim, extending between the temporal ligamentand the origin of the corrugator muscle (Fig.3). The well-defined inferior border is located6 mm above the deep attachment of the peri-orbital septum. The upper border of this originis less distinct and extended a variable 20 to 40mm above the orbital rim. The ligament iscondensed around the branches of the su-praorbital nerve and the corrugator muscleorigin.
The supraorbital adhesion supports thedeep galea which encloses a fat pad and thelower frontalis muscle. The adhesion allowedminimal mobility, and therefore retained thedeep tissues of the lower brow. The corrugatorand procerus muscles assist in providing animportant dynamic support to the medialbrow. Significant mobility of the medial eye-brow can still occur within the tissues superfi-cial to the superficial fascial layer.
The periorbital septum. This well-defined fi-brous septum gains origin from three-quartersof the circumference of the orbital rim, extend-ing from the corrugator origin around to theinferomedial bony origin of the orbicularis oc-uli (Fig. 3). It is continuous with two morebroad adhesions, which are named the lateralbrow and the lateral orbital ligamentous thick-enings.
FIG. 6. Further elevation of the superficial temporal fascia. The three boundaries of the lower temporal compartment (L.T.C.,shaded area) are seen, i.e., the upper border of the zygomatic arch (ZA), the posterior border of the frontal process (FPZ), andthe inferior temporal septum (ITS). The smooth surface of the deep temporal fascia above the inferior temporal septum formsthe floor of the upper temporal compartment (U.T.C.). SV, sentinel vessel.
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1481
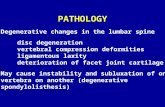
FIG. 7. Right temple, shown from above, looking down toward the zygomatic arch. The subject’s orbit is to the left, ear tothe right. Skin hooks are elevating the superficial temporal fascia from the deep temporal fascia to demonstrate the uppertemporal compartment. The attachments of the inferior temporal septum (ITS) are marked by the upper blue line on the undersideof the superficial temporal fascia (STF) and the lower blue line on the deep temporal fascia (DTF). The tip of the scissors is inthe lower triangular compartment. The inferior temporal septum terminates anteriorly by merging with the temporal ligamen-tous adhesion (TLA).
FIG. 8. Same orientation as in Figure 7 after completion of the release of the inferior temporal septum (ITS) and releaseof the temporal ligamentous adhesion (TLA, triangular adhesion outlined with ink). To the left is the supraorbital ligamentousadhesion (SLA) attached above the supraorbital rim. The released deep attachment of the temporal ligamentous adhesion iscontinuous with the supraorbital ligamentous adhesion. The scissors are beneath the orbital (internal) surface of the periorbitalseptum (PS). A nonadherent area devoid of ligamentous attachments exists between the periorbital septum and the temporal/supraorbital ligamentous adhesions. STF, superficial temporal fascia.
FIG. 9. Dissection continued inferior to the inferior temporal septum (ITS) within the lower triangular compartment of thetemple. Note the fatty tissue within this lower compartment compared with the areolar tissue within the upper compartment.The sentinel vessel (SV) is on the left. The scissors are between the medial and lateral branches of the zygomaticotemporal nerve(ZTN), which are protected by fibrous tissue.
1482 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

FIG. 10. Dissection of the underside of the roof of the lower temporal compartment. Multiple temporal facial nerve branches(TFN) are contained within a layer of fibrofatty tissue adherent to the deep surface of the superficial temporal fascia (STF). Thesebranches pass perpendicular to the branches of the zygomaticotemporal nerve (ZTN) as they perforate the superficial temporalfascia. SV, sentinel vein; ITS, inferior temporal septum.
FIG. 11. Complete elevation of the superficial flap to the boundaries of the lower temporal compartment. The continuous blueline defines the upper border of the zygomatic arch (ZA). The temporal branches of the facial nerve (TFN) are already locatedin the roof of the compartment at the inferior border of the compartment. They do not cross to the roof within the boundariesof the compartment. Zygomaticotemporal nerve branches (ZTN) do cross the lower compartment and are clearly defined; theirfibrous protection has been dissected free. The fine fibrous attachments (X) at the upper border of the zygomatic arch becomeprogressively more concentrated until the lower border of the arch, where a true ligament can be identified. ITS, inferior temporalseptum.
FIG. 12. Dissection inferior to the lower temporal space extending over the zygomatic arch (ZA). The ear is seen on the rightside. The course of the temporal branches of the facial nerve (TFN, highlighted by green background and indicated by arrows)is defined. These emerge from beneath the lower border of the zygomatic arch (ZA) and pass to the underside of the superficialtemporal fascia. In this passage through soft, yellow fat they are protected by definite ligamentous condensations, which attachthe superficial temporal fascia to the zygomatic arch.
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1483

Superiorly, the orbicularis oculi and frontalismuscles merge in an aponeurosis, each with alayer of galeal fascia on their deep surface. Theorbicularis oculi fibers passed superficial tothose of the frontalis. The periorbital septuminserts at a T-junction into the deep galea lin-ing the deep surface of the flat facial muscles.The superior arc of the periorbital septumtherefore provides an indirect bony origin forboth the frontalis and the orbicularis oculimuscles and plays a significant role in restrain-ing the brow and upper eyelid soft tissues.
At the inferolateral orbital rim, the septuminserts into the deep surface of the orbitalcomponent of the orbicularis oculi muscle.Dissected toward its origin at the arcus margi-nalis, the periorbital septum separates into twofascial layers. Internal to the orbital rim, theperiorbital septum continues as the orbital sep-tum; external to the orbital rim, it continues asthe fibrous periosteum.
The thin periorbital septum varies from 1 to3 mm in thickness, with a height of 7 mm (Fig.8). The lateral orbital thickening is 7 3 10 mmat its base and is located immediately supero-lateral to the lateral canthal tendon insertion.The smaller lateral brow thickening is 3 3 11mm and arises from a bony crest on the lateralsupraorbital rim. It does not arise from thezygomaticofrontal suture. Both of these liga-ments insert into and retain the deep surfaceof the orbicularis oculi muscle fascia.
Fascial Compartments
The upper face and brow are separated intoa number of fascial compartments by the ar-rangement of the temporal (ligamentous) ad-hesion, the three ligaments that radiate fromit, and the periorbital septum (Fig. 2).
The inferior temporal septum divides thetemple into the upper temporal compartmentand the lower temporal compartment (Fig. 6).The upper temporal compartment is the po-tential space above the inferior temporal sep-tum. Its upper border is the superior temporalseptum. The lower temporal compartment islocated below the inferior temporal septum; itis bounded inferiorly by the zygomatic archand anteriorly by the frontal process of thezygoma. The upper compartment has no spe-cific structures crossing and is safe for dissec-tion. However, the triangular lower compart-ment contains the temporal branches of thefacial nerve.(Fig. 10). There is no well-definedseptum limiting inferior dissection over the
anterior zygoma until the defined zygomaticligaments are reached.
The forehead compartment is limited later-ally by the superior temporal septum and infe-riorly by the supraorbital ligamentous adhe-sion.
The periorbital septum divides the subsuper-ficial fascial space of the orbital region into twocompartments: orbital and periorbital (Fig. 2).The subsuperficial fascial space of the orbitalregion, located internal to the orbital rim be-tween the palpebral portion of the orbicularisoculi and the orbital septum, contains looseareolar tissue only. The superficial fascia itselfcontains fat within its deepest layers in theregion of the orbital rim. The subsuperficialfascial compartment of the periorbital regionlies external to the rim and contains the attach-ments between the orbital portion of the orbic-ularis oculi and the underlying pericranium.
Relationships between Ligaments and Nerves
Facial nerve. The 2 to 4 temporal branches ofthe facial nerve leave the superior pole of theparotid gland by perforating its capsule at thelevel of the lower border of the zygomatic arch.The nerves then cross the subSMAS plane in-ferior to the zygomatic arch (Fig. 12) to reachthe deep surface of the SMAS (Fig. 10). In cross-ing this mobile plane, the nerve branches areprotected by fibrous condensations passingfrom the zygomatic arch to a fat pad on the deepsurface of the superficial temporal fascia. Theythen run in an anterosuperior direction towardthe insertion of the temporal ligament (Fig. 2).
At the level of the temporal ligament, themain branches of the temporal nerve divideinto numerous filamentous branches. Thesesupply the frontalis, corrugator, and upper or-bicularis oculi muscles through their deep sur-face. The nerve to the corrugator passes in anarrow compartment deep to frontalis,bounded superiorly by the supraorbital adhe-sion and inferiorly by the periorbital septum.
The sentinel vein39,40 is located immediatelyinferior to the inferior temporal septum (Fig.9). The temporal nerve branches display a vari-able relationship to the sometimes duplicatedsentinel vein. Although the temporal nervebranches are found both superior and inferiorto this vein, they are predominantly locatedcephalad to the sentinel vein (Fig. 2). Incon-stant smaller nerve branches are found caudalto the sentinel vein.
The inferior temporal septum is therefore a
1484 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

reliable and identifiable marker for the loca-tion of the temporal nerves as it inserts into thesuperficial temporal fascia along a line imme-diately cephalad to the most superior temporalnerve branches (Fig. 5). Dissecting in an infe-rior direction, the release of the inferior tem-poral septum (Fig. 7) exposes the temporalnerves. They are surrounded by loose adiposetissue and plastered to the deep surface of thesuperficial temporal fascia by a thin areolarfascia (Fig. 10).
Sensory nerves. Each of the major cutaneousnerves in the region cross the mobile subsuper-ficial fascia plane in association with a namedligamentous attachment.
The supraorbital nerve branches pass alongthe upper periorbital septum to reach the deepgalea. The supraorbital ligamentous adhesionis condensed along the course of the nerves.Branches of the infraorbital nerve to the lowereyelid region follow the inferior periorbitalseptum. Where the periorbital septum attachesto the superficial fascia the respective nervesdivide into two groups of branches: those tothe eyelid and those to the periorbital tissues.The supratrochlear nerve is an exception,crossing the plane between the heads of thecorrugator muscle.
The anterior branch of the zygomaticotem-poral nerve is usually related to the lateralorbital ligament; the smaller posteriorbranches within the lower temporal compart-ment are associated with minor fibrous attach-ments and fine veins (Figs. 5 and 11). Thezygomaticofacial nerve emerges through a sin-gle or duplicate foramen in the zygoma and isthen associated with the inferolateral portionof the periorbital septum.
The zygomaticotemporal and supraorbitalcutaneous nerves perforate the superficial fas-cia along the line of the facial nerves branches(Fig. 10). They could therefore be used asadditional markers for the location of the facialnerve branches (Fig. 11).
DISCUSSION
Definition of a Ligament
This study raises the important issue of whatexactly is the definition of a “ligament.” TheOxford Dictionary41 defines a ligament as “a bandof fibrous tissue binding bones together or anymembrane keeping an organ in position.” Al-though the word ligament traditionally de-
scribes a connective tissue that restrainsbones,42 this definition has subsequently beenwidened to include “cutaneous retaining liga-ments.” These are fibrous attachments anchor-ing skin to the underlying deep fascia or peri-osteum and have been described in variouslocations including the digits,43,44 the face,18,21
and the breast.45,46
Furnas21 introduced the term “retaining lig-aments” in the face. He documented four cu-taneous ligaments in the cheek, naming themthe zygomatic, mandibular, platysma-auricular,and anterior platysma ligaments. The first twoof these ligaments passed from bone directlyinto the dermis, whereas the second two passedfrom the superficial fascia (platysma) to thedermis. Traction on the deep end of the cutligament dimpled the skin. The ligamentsfanned out as they approached the dermis andwere notably absent in about 10 percent ofdissections.
Stuzin et al.18 further elaborated on the def-inition of these retaining ligaments, also divid-ing them into two groups: the previously de-scribed true osteocutaneous ligaments and asecond group that consisted of a coalescencebetween the deep and superficial fasciae of theface. This therefore widened the definition ofretaining ligaments to include defined adhe-sions retaining the superficial to the deep fas-cia. These adhesions retain the overlying skinindirectly through a separate system of fibroussepta that extend from the superficial fasciainto dermis.9,14,38 They differ from the discreteosteocutaneous ligaments, which run directlyfrom periosteum to a focal area of dermis.
Knize13 recently suggested that, to be consid-ered a retaining ligament, a structure shouldinsert directly into dermis. However, it is im-portant to recognize the vital role of thoseother ligaments that attach to the superficialfascia yet retain the overlying skin indirectlythrough the retinacula cutis.
The septa and adhesions in the temporaland periorbital regions pass to the superficialfascia and exert their effect on the skin, pre-sumably thorough the retinacula cutis. Thetrue (cutaneous) ligaments branch as they passthrough the superficial fascia to the dermis.The three forms of fibrous attachment de-scribed in this article fulfill the criteria of “lig-aments of the superficial tissues” and insertinto either the superficial fascia or the dermis.
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1485

Surgical Applications
Connective tissue anatomy. The arrangementof the ligamentous fixation between the under-side of the superficial fascia and the perioste-um/deep temporal fascia provides landmarkinformation for the surgeon operating in thisarea. The ligamentous attachments demarcatethe anatomic spaces in the forehead, temple,and periorbital regions and localize the facialnerve and sensory branches.
This superior temporal septum has been re-ferred to by Knize12 as the “zone of fixation.” Atthe anterior end of this structure is an expan-sion providing strong attachment to the frontalperiosteum medial to the deep temporal fascia.This would seem to be what Knize calls theorbital ligament; however, our observations dif-fer in that this temporal ligament does notextend to the orbital rim. The supraorbitalligamentous adhesion has been noted byKnize,12 who describes it as zone B of fixationin the lower 2 cm of the forehead. It would
seem that the periorbital septum has not beendescribed as such before; however, close exam-ination of Knize’s12 histologic studies (Fig. 6 ofKnize’s article, middle sagittal section) shows afascial septum passing from the deep galea tothe orbital rim.
Although there was a condensation of theconnective tissue in the region of the zygomat-icofacial suture, we did not find a definite lig-ament as described in Knize’s article. Therewas a thickening of the periorbital septum, thelateral brow thickening, which attaches to theorbital rim superior to the zygomaticofacialsuture.
Relationship of the temporal nerves to the liga-ments. Surgeons have long been cautiousabout operating in the temple because of therisk of damaging the temporal branch of thefacial nerve. This concern has prompted nu-merous anatomic studies to define the trajec-tory or course of the branches.30–32 However,these studies have not fully satisfied the intra-
FIG. 13. Periorbital and temporal ligamentous attachments indicating the required amount of surgical ligamentous release:lateral view. Green, release for lateral brow lift; yellow, additional release required for upper cheek lift through the temple.Temporal ligamentous adhesion (TLA), supraorbital ligamentous adhesion (SLA), superior temporal septum (STS), inferiortemporal septum (ITS), periorbital septum (PS), lateral brow thickening of periorbital septum (LBT), lateral orbital thickeningof periorbital septum (LOT), sentinel vessel (SV), temporal branches of facial nerve (TFN), zygomaticotemporal nerve (ZTN),zygomaticofacial nerve (ZFN).
1486 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

operative requirement of the surgeon in relat-ing the nerve to the planes of dissection as theyhave referred to external soft-tissue landmarksor to measurements along the zygomatic arch.The temporal ligament and the inferior tem-poral septum are reliable soft-tissue ligamentsand provide accurate internal landmarks forpredicting the neurovascular anatomy of theregion.
The inferior temporal septum divides thesubsuperficial fascial space in the temple intotwo separate compartments. The triangularlower temporal compartment contained all the“at risk” anatomic structures of the temple.This is significant for the surgeon in that dis-section can be readily performed within thelarger upper temporal compartment all theway to the septum when an abrupt change ofapproach is required. The inferior temporalseptum is readily identified by its criss-crossedfibers that provide a barrier to the dissection. Itis best defined by blunt dissection. This septumvaries in thickness between individuals and canbe quite fine in some.
After operating through this septum it isimperative that the level of dissection hug thefloor of the space, that is, directly on the deeptemporal fascia. This is because the temporalbranches of the facial nerve course throughthe roof of the lower temporal compartmentimmediately abutting the inferior temporalseptum. They run parallel to the line of attach-ment of the inferior septum to this roof. Thetemporal branches are at risk here because theseptum “fixes” the roof of the space close to thefloor. The branches run within a wafer-thin fatpad on the underside of the superficial tempo-ral fascia. For the purposes of description,these nerves should be considered to be in theceiling, rather than in the roof, of the space.Further, these nerves enter the lower temporalcompartment already in the ceiling (this oc-curs just caudal to the inferior border of thezygoma), and they remain in the ceiling at alltimes.
The sentinel vessels and both branches ofthe zygomaticotemporal nerve cross the lowertemporal space, floor to ceiling, related to theinferomedial surface of the inferior temporalseptum. They can also be safely spared at thisjuncture by judicious dissection. The majorityof the facial nerve branches in the ceiling arein the narrow cephalad space between the sen-tinel vessels and the inferior temporal septum.Accordingly, dissection through the lower tem-
poral compartment can be quite safe in regardto the facial nerve, provided the ceiling is liftedoff the plane of dissection. Further, dissectioncan then continue readily inferiorly and ante-riorly across the lower temporal space over thebody of the zygoma, or to the periorbital at-tachments.
Relationship of the temporal nerves to the sentinelvessels. Previous studies39,40 have related thetemporal nerve branches to perforating vessels,which enter the superficial temporal fascia 1 cmlateral to the superolateral angle of the orbit.De la Plaza has named these the “sentinel vesselsof the lateral wall of the orbit,” and he makesthe point that they must be electrocoagulateddeep to avoid damage to the temporal nerves.The sentinel vessels provide a landmark for thetemporal branches of the facial nerve duringendoscopic forehead dissection.47
Because the relationship between the senti-nel veins and the temporal nerve branches issomewhat variable, the vessels should be usedas a relative landmark for facial nerve anatomy.Sometimes the sentinel vessels are duplicatedwith tributaries at different vertical levels. Al-though temporal nerve branches are foundjust cephalad to the sentinel vessels, some alsopass caudal to the vessels in an unpredictablefashion.
Surgical ligamentous release. Gravitational ag-ing changes of the brow and also the uppercheek can be corrected by surgical reposition-ing after dissection beneath the superficial fas-cial plane.
As in deep-plane surgery of the cheek, enbloc mobilization of the ptotic superficial fas-cia allows it to be repositioned.24,38 An overcor-rection of the position of the superficial fasciais required so that the laxity between it and thedermis is taken up. The skin position can thenbe corrected without direct skin traction.
The technique of ligamentous release differsbetween the temple and the cheek. In the tem-ple, the facial nerve is not in immediate dangerbecause it enters the region within the plane ofthe superficial fascia and therefore does notcross the plane of dissection. The only area ofpotential danger to the nerve is along the lineof the inferior temporal septum. This is be-cause the nerve branches that cross the templeimmediately caudal to the septum are held bythe septum close to the deep fascia.
Accordingly, a swift blunt dissection can beperformed in the subgaleal plane of the uppertemporal compartment and the forehead with
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1487

the knowledge that blunt dissection shouldcease at the inferior temporal septum. All vitalanatomy is inferior to this septum in the lowertemporal compartment. The inferior septum isthen judiciously released by sharp dissectionwith small blunt scissors, at all times remainingdirectly applied to the surface of the deep fas-
cia as the temporal branches lie immediatelysuperficial. Once inside the inferior temporalcompartment these branches are kept re-tracted out of the field.
The inferior temporal compartment isopened by blunt spreading dissection to pro-tect the zygomaticotemporal nerves. Release of
FIG. 14. Periorbital and temporal ligamentous attachments indicating the required amount of surgical ligamentous release:anterior view. Green, release for lateral brow lift; yellow, additional release required for upper cheek lift through the temple.Temporal ligamentous adhesion (TLA), supraorbital ligamentous adhesion (SLA), superior temporal septum (STS), inferiortemporal septum (ITS), periorbital septum (PS), lateral brow thickening of periorbital septum (LBT), lateral orbital thickeningof periorbital septum (LOT), temporal branches of facial nerve (TFN), zygomaticotemporal nerve (ZTN), zygomaticofacial nerve(ZFN).
1488 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000

the ligaments, other than the inferior temporalseptum, requires sharp dissection. This can beperformed with relative impunity once thetemporal branches of the facial nerve are pro-tected by the retractor.
The morphology of the ligaments deter-mines the dissection technique. The cheek at-tachments are true ligaments, which have adiscrete cylindrical nature. After specific re-lease of these localized attachments, no furtherdissection is necessary. Unlike the true liga-ments of the cheek, the ligaments of the tem-ple and forehead are septa and adhesions, andtherefore involve wide areas of attachment be-tween the deep and superficial fasciae. Releaseof these regions therefore involves extensivedissection beneath the superficial fascia. Ac-cordingly, elevation of the lateral brow re-quires more extensive ligamentous releasethan might be expected. Release of only thetemporal ligamentous adhesion and the tem-poral septa is insufficient. The supraorbital lig-amentous adhesion and the lateral brow thick-ening of the periorbital septum must also bereleased (Figs. 13 and 14). The supraorbitalligamentous adhesion usually needs release allthe way to the supraorbital nerve, being mind-ful that the lateral branch of the supraorbitalnerve is at risk as it approaches the superiortemporal septum. If the intended benefit is toinclude the lateral canthal and upper zygo-matic regions, the periorbital release must beextended to include the lateral orbital thicken-ing at the lateral canthus. To benefit furtheraround to the lateral lower lid, the periorbitalseptal release is extended around to the zygo-maticofacial nerve.
Ligamentous fixation. After the retaining lig-aments are released, the superficial fascia is re-positioned without being placed under tension.The fascia is maintained in its new location bysuture fixation between the deep temporal fas-cia and the 2-cm-long temporal ligamentousadhesion (Fig. 3, inset). The remnants of theretaining ligament provide reinforced fibrousanchorage points for the sutures that replicatethe temporal ligamentous adhesion. Knowl-edge of the relationship between the nerves andthese ligaments allows this phase of the proce-dure to be performed safely.
Aging
The development of brow ptosis affects thelateral third of the brow and the temporalregion earlier than it affects the medial
brow.10,12 The pathogenesis of this complicatedaging process is partly explained by the liga-mentous anatomy of these regions. The super-ficial fascial layers of the medial face arestrongly retained by connective tissue attach-ments including the temporal ligament, thesupraorbital adhesions, and the periorbital sep-tum.
In the temporal and lateral brow regions, thesuperficial tissues are restrained by only thetwo temporal septa, which provide less fixationthan the many strong medial supports. Thistemporal ligament is located above the junc-tion of the lateral and middle thirds of theeyebrow. Lateral to this the reduction in liga-mentous attachment of the superficial fasciahelps explain the earlier ptosis.
Bryan C. Mendelson, F.R.C.S.(E), F.R.A.C.S.,F.A.C.S.
109 Mathoura RoadToorak 3142Melbourne, [email protected]
ACKNOWLEDGMENT
The authors express their thanks to Kari Colen for herinvaluable assistance with the dissections.
REFERENCES
1. Mitz, V., and Peyronie, M. The superficial musculo-apo-neurotic system (SMAS) in the parotid and cheekarea. Plast. Reconstr. Surg. 58: 80, 1976.
2. Jost, G., and Levet, Y. Parotid fascia and face lifting: Acritical evaluation of the SMAS concept. Plast. Reconstr.Surg. 74: 42, 1984.
3. Dzubow, L. M. The fasciae of the face: An anatomic andhistologic analysis. J. Am. Acad. Dermatol. 14: 502, 1986.
4. Bosse, J., and Papillon, J. Surgical Anatomy of the SMASat the Malar Region. In Transactions of the 9th Interna-tional Congress of Plastic and Reconstructive Surgery. NewYork: McGraw-Hill, 1987.
5. Wassef, M. Superficial fascial and muscular layers in theface and neck: A histological study. Aesthetic Plast. Surg.11: 171, 1987.
6. Thaller, S. R., Kim, S., Patterson, H., Wildman, M., andDaniller, A. The submuscular aponeurotic system(SMAS): A histologic and comparative anatomy eval-uation. Plast. Reconstr. Surg. 86: 690, 1990.
7. Barton, F. E., Jr. The SMAS and the nasolabial fold.Plast. Reconstr. Surg. 89: 1054, 1992.
8. Gosain, A. K., Yousif, N. J., Madiedo, G., Larson, D. L.,Matloub, H. S., and Sanger, J. R. Surgical anatomy ofthe SMAS: A reinvestigation. Plast. Reconstr. Surg. 92:1254, 1993.
9. Yousif, N. J., Gosain, A., Matloub, H. S., Sanger, J. R.,Madiedo, G., and Larson, D. L. The nasolabial fold:An anatomical and histological reappraisal. Plast. Re-constr. Surg. 93: 60, 1994.
10. Lemke, B. N., and Stasior, O. G. The anatomy of eye-brow ptosis. Arch. Ophthalmol. 100: 981, 1982.
Vol. 105, No. 4 / SURGICAL ANATOMY OF LIGAMENTOUS ATTACHMENTS 1489

11. Casanova, R., Cavalcante, D., Grotting, J. C., Vasconez,L. O., and Psillakis, J. M. Anatomic basis for vascu-larized outer-table calvarial bone flaps. Plast. Reconstr.Surg. 78: 300, 1986.
12. Knize, D. M. An anatomically based study of the mech-anism of eyebrow ptosis. Plast. Reconstr. Surg. 97: 1321,1996.
13. Knize, D. M. Reassessment of the coronal incision andsubgaleal dissection for foreheadplasty. Plast. Reconstr.Surg. 102: 478, 1998.
14. Tolhurst, D. E., Carstens, M. H., Greco, R. J., and Hurwitz,D. J. The surgical anatomy of the scalp. Plast. Recon-str. Surg. 87: 603, 1991.
15. Abul-Hassan, H. S., von Drasek-Ascher, G., and Acland,R. D. Surgical anatomy and blood supply of the fas-cial layers of the temporal region. Plast. Reconstr. Surg.77: 17, 1986.
16. Campiglio, G. L., and Candiani, P. Anatomical study onthe temporal fascial layers and their relationships withthe facial nerve. Aesthetic Plast. Surg. 21: 69, 1997.
17. Owsley, J. Q., Jr. Platysma-fascial rhytidectomy: A pre-liminary report. Plast. Reconstr. Surg. 59: 843, 1977.
18. Stuzin, J. M., Baker, T. J., and Gordon, H. L. The re-lationship of the superficial and deep facial fascias:Relevance to rhytidectomy and aging. Plast. Reconstr.Surg. 89: 441, 1992.
19. Mendelson, B. C. Correction of the nasolabial fold: Ex-tended SMAS dissection with periosteal fixation. Plast.Reconstr. Surg. 89: 822, 1992.
20. Carstens, M. H., Greco, R. J., Hurwitz, D. J., and Tolhurst,D. E. Clinical applications of the subgaleal fascia.Plast. Reconstr. Surg. 87: 615, 1991.
21. Furnas, D. W. The retaining ligaments of the cheek.Plast. Reconstr. Surg. 83: 11, 1989.
22. Furnas, D. Strategies for nasolabial fold levitation. Clin.Plast. Surg. 22: 265, 1995.
23. Hamra, S. T. Composite rhytidectomy. Plast. Reconstr.Surg. 90: 1, 1992.
24. Hamra, S. T. The deep-plane rhytidectomy. Plast. Re-constr. Surg. 86: 53, 1990.
25. Mendelson, B. C., Moss, C. J., and Taylor, G. I. TheSurgical Anatomy of the Ligamentous Attachments inthe Temporal and Periorbital Regions. Presented atthe 30th Scientific Congress of the American Societyfor Aesthetic Plastic Surgery, New York, May 3, 1997.
26. Psillakis, J. M., Rumley, T. O., and Camargos, A. Sub-periosteal approach as an improved concept for cor-rection of the aging face. Plast. Reconstr. Surg. 82: 383,1988.
27. Meyer, D. R., Linberg, J. V., Wobig, J. L., and McCormick,S. A. Anatomy of the orbital septum and associatedeyelid connective tissues. Ophthalmic Plast. Reconstr.Surg. 7: 104, 1991.
28. Gasser, R. F. The development of the facial muscles inman. Am. J. Anat. 120: 357, 1965.
29. Patten, B. M. Human Embryology, 3rd Ed. New York:McGraw-Hill, 1968.
30. Liebman, E. P., Webster, R. C., Berger, A. S., and Del-laVecchia, M. The frontalis nerve in the temporalbrow lift. Arch. Otolaryngol. 108: 232, 1982.
31. Stuzin, J. M., Wagstrom, L., Kawamoto, H. K., and Wolfe,S. A. Anatomy of the frontal branch of the facialnerve: The significance of the temporal fat pad. Plast.Reconstr. Surg. 83: 265, 1989.
32. Ishikawa, Y. An anatomical study on the distribution ofthe temporal branch of the facial nerve. J. Craniomax-illofac. Surg. 18: 287, 1990.
33. Fatah, M. F. Innervation and functional reconstructionof the forehead. Br. J. Plast. Surg. 44: 351, 1991.
34. Furnas, D. W. Landmarks for the trunk and the tem-porofacial division of the facial nerve. Br. J. Surg. 52:694, 1965.
35. Pitanguy, I., and Ramos, A. S. The frontal branch of thefacial nerve: The importance of its variations infacelifting surgery. Plast. Reconstr. Surg. 38: 352, 1966.
36. Taylor, G. I., and Palmer, J. H. The vascular territories(angiosomes) of the body: Experimental study andclinical applications. Br. J. Plast. Surg. 40: 113, 1987.
37. Rees, M. J., and Taylor, G. I. A simplified lead oxidecadaver injection technique. Plast. Reconstr. Surg. 77:141, 1986.
38. Mendelson, B. C. Extended sub-SMAS dissection andcheek elevation. Clin. Plast. Surg. 22: 325, 1995.
39. Hinderer, U. T., Urriolagoitia, F., and Vildosola, R. Theblepharo-periorbitoplasty: Anatomical basis. Ann.Plast. Surg. 18: 437, 1987.
40. De la Plaza, R., Valiente, E., and Arroyo, J. M. Supra-periosteal lifting of the upper two thirds of the face.Br. J. Plast. Surg. 44: 325, 1991.
41. Sykes, J. B. (Ed.). The Concise Oxford Dictionary of English,7th Ed. Oxford: Clarendon Press, 1984.
42. Williams, P. L., and Warwick, R. (Eds.). Gray’s Anatomy,36th Ed. Edinburgh: Churchill Livingston, 1980.
43. Grayson, J. The cutaneous ligaments of the digits.J. Anat. 75: 164, 1941.
44. Cleland. On the cutaneous ligaments of the phalanges.J. Anat. Physiol. 12: 526, 1878.
45. Cooper, A. Anatomy and Diseases of the Breast. Philadel-phia: Lea and Blanchard, 1845. P. 49.
46. Wuringer, E., Mader, N., Posch, E., and Holle, J. Nerveand vessel supplying ligamentous suspension of themammary gland. Plast. Reconstr. Surg. 101: 1486, 1998.
47. Trinei, F. A., Januszkiewicz, J., and Nahai, F. The sen-tinel vein: An important reference point for surgery inthe temporal region. Plast. Reconstr. Surg. 101: 27,1998.
1490 PLASTIC AND RECONSTRUCTIVE SURGERY, April 2000