COSMETIC - LWW Journalsjournals.lww.com/plasreconsurg/Documents/Updates_in_Aesthetic... · COSMETIC...
9
COSMETIC Lipoabdominoplasty Osvaldo R. Saldanha, M.D. Rodrigo Federico, M.D. Presper F. Daher, M.D. Andrey A. Malheiros, M.D. Paulo R. G. Carneiro, M.D. Se ´rgio F. D. Azevedo, M.D. Osvaldo R. Saldanha Filho Cristianna B. Saldanha Santos, Sa ˜o Paulo, Brazil Background: Abdominoplasty is one of the most common aesthetic opera- tions. Wide bibliographic research has revealed that there is a safe method whereby two techniques-liposuction and abdominoplasty-can be associated in the same procedure. The authors present a new abdominoplasty technique combining a selective undermining with complete abdominal liposuction. Methods: The authors standardized steps with which to perform a safe association of traditional abdominoplasty with liposuction of the entire abdomen and infracostal areas. Using selective undermining, it is possible to preserve at least 80 percent of the blood supply in the abdominal wall, causing little nervous trauma, preserving the great majority of the lymphatic vessels, and resulting in few complications compared with traditional ab- dominoplasty, including post-bariatric surgery procedures. In this study, lipoabdominoplasty was performed on 445 patients: eight male patients and 437 female patients, from 2000 to 2007. Results: The authors consider the results good and excellent, especially regarding patient evaluation, better body contour, abdominal rejuvenation, shorter scars, the form of the umbilicus, and a decrease in the abdominal measures. Conclusion: With a progressive adaptation of this technique, it is possible to achieve a harmonious body contour using a safe liposuction method on the abdominal and costal areas, with fast recovery and good to excellent results. (Plast. Reconstr. Surg. 124: 934, 2009.) T he evolution of techniques in abdominal sur- gery, with low postoperative morbidity and lower complications rates, has always moti- vated surgeons to search for innovations in plastic surgery. 1–16 Lipoabdominoplasty was developed and patterned as a safe and functional option with which to perform liposuction and abdominoplasty during the same surgical procedure, promoting the benefits of both techniques. This technique generates a better aesthetic result and can be learned quickly because surgeons are accustomed to performing each procedure, liposuction and abdominoplasty, separately. This technique is not simply using liposuction while we are performing abdominoplasty. It has a much wider concept, respecting the complete ab- dominal anatomy. The traditional undermining has been substituted with canula undermining. As a consequence, we do not stop the blood supply coming from the abdominal perforating vessels. HISTORY Undermining Evolution History shows a progressive undermining of the abdominal wall from 1899 to 1957, when the exten- sive undermining was standardized by Vernon 1–3 to facilitate umbilicus transposition. Hakme, in 1985, presented a new approach for the abdominal lipec- tomies, called the miniabdominoplasty technique and consisting of liposuction of the entire abdomen and flanks, associated with the elliptical resection of the suprapubic skin, and plication of the supraum- bilical and infraumbilical muscles, without relocat- ing the umbilicus. 8 In 1991 and 1995, Matarasso focused on the complications of combined liposuction and ab- dominoplasty methods, presenting two articles that recommended safe areas of liposuction. 9,10 In those articles, he considered the back and the From the Plastic Surgery Department, Santa Cecı ´lia University. Received for publication December 6, 2007; accepted April 9, 2009. Reprinted and reformatted from the original article published with the September 2009 issue (Plast Reconstr Surg. 2009; 124:934 –942). Copyright ©2012 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e318250a549 Disclosures: None of the authors has a financial interest to declare in relation to the content of this article. www.PRSJournal.com 77S
Transcript of COSMETIC - LWW Journalsjournals.lww.com/plasreconsurg/Documents/Updates_in_Aesthetic... · COSMETIC...

COSMETIC
LipoabdominoplastyOsvaldo R. Saldanha, M.D.
Rodrigo Federico, M.D.Presper F. Daher, M.D.
Andrey A. Malheiros, M.D.Paulo R. G. Carneiro, M.D.Sergio F. D. Azevedo, M.D.Osvaldo R. Saldanha Filho
Cristianna B. Saldanha
Santos, Sao Paulo, Brazil
Background: Abdominoplasty is one of the most common aesthetic opera-tions. Wide bibliographic research has revealed that there is a safe methodwhereby two techniques-liposuction and abdominoplasty-can be associatedin the same procedure. The authors present a new abdominoplasty techniquecombining a selective undermining with complete abdominal liposuction.Methods: The authors standardized steps with which to perform a safeassociation of traditional abdominoplasty with liposuction of the entireabdomen and infracostal areas. Using selective undermining, it is possibleto preserve at least 80 percent of the blood supply in the abdominal wall,causing little nervous trauma, preserving the great majority of the lymphaticvessels, and resulting in few complications compared with traditional ab-dominoplasty, including post-bariatric surgery procedures. In this study,lipoabdominoplasty was performed on 445 patients: eight male patients and437 female patients, from 2000 to 2007.Results: The authors consider the results good and excellent, especially regardingpatient evaluation, better body contour, abdominal rejuvenation, shorter scars, theform of the umbilicus, and a decrease in the abdominal measures.Conclusion: With a progressive adaptation of this technique, it is possible to achievea harmonious body contour using a safe liposuction method on the abdominal andcostal areas, with fast recovery and good to excellent results. (Plast. Reconstr. Surg.124: 934, 2009.)
The evolution of techniques in abdominal sur-gery, with low postoperative morbidity andlower complications rates, has always moti-
vated surgeons to search for innovations in plasticsurgery.1–16 Lipoabdominoplasty was developedand patterned as a safe and functional option withwhich to perform liposuction and abdominoplastyduring the same surgical procedure, promotingthe benefits of both techniques. This techniquegenerates a better aesthetic result and can belearned quickly because surgeons are accustomedto performing each procedure, liposuction andabdominoplasty, separately.
This technique is not simply using liposuctionwhile we are performing abdominoplasty. It has amuch wider concept, respecting the complete ab-dominal anatomy. The traditional undermininghas been substituted with canula undermining. As
a consequence, we do not stop the blood supplycoming from the abdominal perforating vessels.
HISTORYUndermining Evolution
History shows a progressive undermining of theabdominal wall from 1899 to 1957, when the exten-sive undermining was standardized by Vernon1–3 tofacilitate umbilicus transposition. Hakme, in 1985,presented a new approach for the abdominal lipec-tomies, called the miniabdominoplasty techniqueand consisting of liposuction of the entire abdomenand flanks, associated with the elliptical resection ofthe suprapubic skin, and plication of the supraum-bilical and infraumbilical muscles, without relocat-ing the umbilicus.8
In 1991 and 1995, Matarasso focused on thecomplications of combined liposuction and ab-dominoplasty methods, presenting two articlesthat recommended safe areas of liposuction.9,10 Inthose articles, he considered the back and the
From the Plastic Surgery Department, Santa CecıliaUniversity.Received for publication December 6, 2007; accepted April 9,2009.Reprinted and reformatted from the original article publishedwith the September 2009 issue (Plast Reconstr Surg. 2009;124:934–942).Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e318250a549
Disclosures: None of the authors has a financialinterest to declare in relation to the content of thisarticle.
www.PRSJournal.com 77S
flanks safe areas and did not regard the lateralregion of the abdomen as a safe area; the centralregion of the abdomen was considered prohibitedfor liposuction.17
In 1995, Lockwood reported the high lateraltension abdominoplasty, in which he used theScarpa fascia to decrease the tension of the skinclosure.12,13 Since the 1990s, the undermining hasdecreased in amplitude because of a large numberof complications (seroma, hematoma, and most ofall, necrosis), reaching zero in 1992 with the publi-cation regarding abdominoplasty mesh undermin-ing by Illouz.11,18,19 The trend of abdominolipoplastywithout or with small undermining continued until1999, when Shestak14 and Avelar15 presented thepartial abdominolipoplasty method, with no under-mining, associated with liposuction.
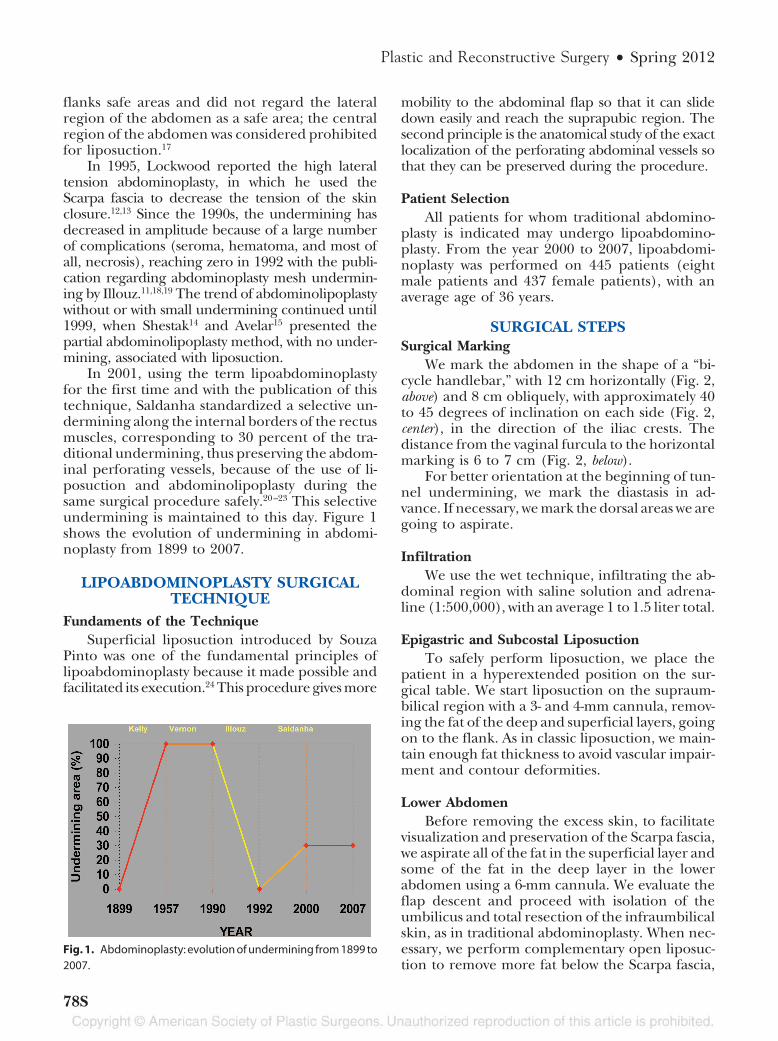
In 2001, using the term lipoabdominoplastyfor the first time and with the publication of thistechnique, Saldanha standardized a selective un-dermining along the internal borders of the rectusmuscles, corresponding to 30 percent of the tra-ditional undermining, thus preserving the abdom-inal perforating vessels, because of the use of li-posuction and abdominolipoplasty during thesame surgical procedure safely.20–23 This selectiveundermining is maintained to this day. Figure 1shows the evolution of undermining in abdomi-noplasty from 1899 to 2007.
LIPOABDOMINOPLASTY SURGICALTECHNIQUE
Fundaments of the TechniqueSuperficial liposuction introduced by Souza
Pinto was one of the fundamental principles oflipoabdominoplasty because it made possible andfacilitated its execution.24 This procedure gives more
mobility to the abdominal flap so that it can slidedown easily and reach the suprapubic region. Thesecond principle is the anatomical study of the exactlocalization of the perforating abdominal vessels sothat they can be preserved during the procedure.
Patient SelectionAll patients for whom traditional abdomino-
plasty is indicated may undergo lipoabdomino-plasty. From the year 2000 to 2007, lipoabdomi-noplasty was performed on 445 patients (eightmale patients and 437 female patients), with anaverage age of 36 years.
SURGICAL STEPSSurgical Marking
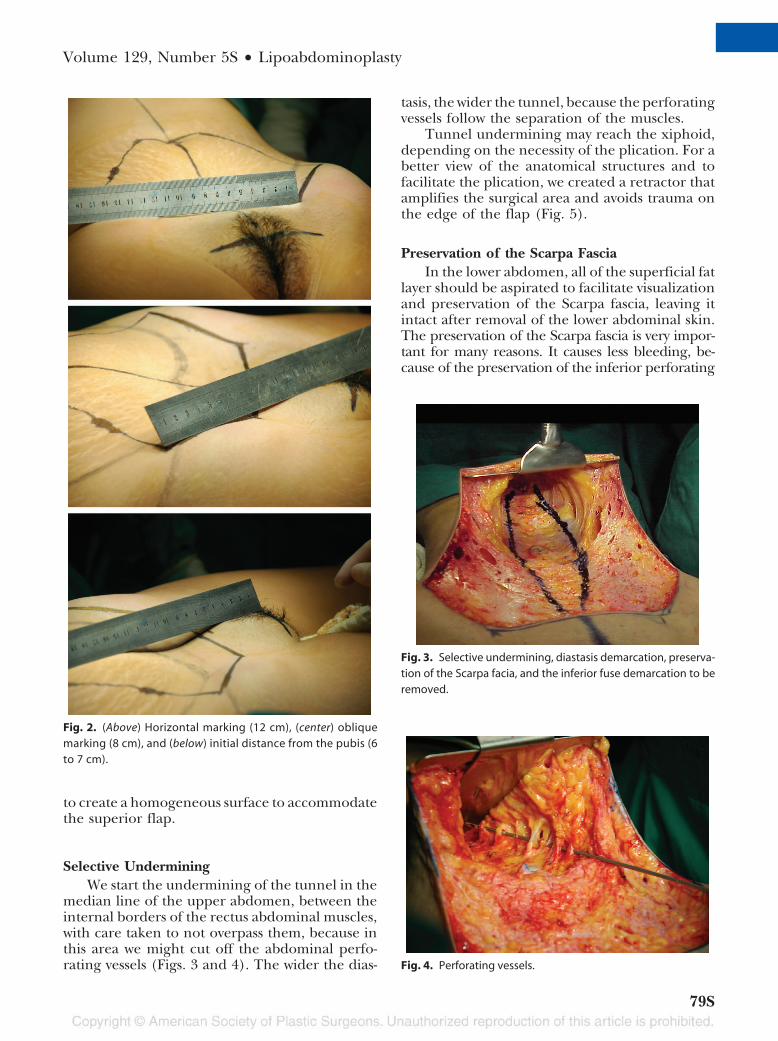
We mark the abdomen in the shape of a “bi-cycle handlebar,” with 12 cm horizontally (Fig. 2,above) and 8 cm obliquely, with approximately 40to 45 degrees of inclination on each side (Fig. 2,center), in the direction of the iliac crests. Thedistance from the vaginal furcula to the horizontalmarking is 6 to 7 cm (Fig. 2, below).
For better orientation at the beginning of tun-nel undermining, we mark the diastasis in ad-vance. If necessary, we mark the dorsal areas we aregoing to aspirate.
InfiltrationWe use the wet technique, infiltrating the ab-
dominal region with saline solution and adrena-line (1:500,000), with an average 1 to 1.5 liter total.
Epigastric and Subcostal LiposuctionTo safely perform liposuction, we place the
patient in a hyperextended position on the sur-gical table. We start liposuction on the supraum-bilical region with a 3- and 4-mm cannula, remov-ing the fat of the deep and superficial layers, goingon to the flank. As in classic liposuction, we main-tain enough fat thickness to avoid vascular impair-ment and contour deformities.
Lower AbdomenBefore removing the excess skin, to facilitate
visualization and preservation of the Scarpa fascia,we aspirate all of the fat in the superficial layer andsome of the fat in the deep layer in the lowerabdomen using a 6-mm cannula. We evaluate theflap descent and proceed with isolation of theumbilicus and total resection of the infraumbilicalskin, as in traditional abdominoplasty. When nec-essary, we perform complementary open liposuc-tion to remove more fat below the Scarpa fascia,
Fig. 1. Abdominoplasty: evolution of undermining from 1899 to2007.
Plastic and Reconstructive Surgery • Spring 2012
78S
to create a homogeneous surface to accommodatethe superior flap.
Selective UnderminingWe start the undermining of the tunnel in the
median line of the upper abdomen, between theinternal borders of the rectus abdominal muscles,with care taken to not overpass them, because inthis area we might cut off the abdominal perfo-rating vessels (Figs. 3 and 4). The wider the dias-
tasis, the wider the tunnel, because the perforatingvessels follow the separation of the muscles.
Tunnel undermining may reach the xiphoid,depending on the necessity of the plication. For abetter view of the anatomical structures and tofacilitate the plication, we created a retractor thatamplifies the surgical area and avoids trauma onthe edge of the flap (Fig. 5).
Preservation of the Scarpa FasciaIn the lower abdomen, all of the superficial fat
layer should be aspirated to facilitate visualizationand preservation of the Scarpa fascia, leaving itintact after removal of the lower abdominal skin.The preservation of the Scarpa fascia is very impor-tant for many reasons. It causes less bleeding, be-cause of the preservation of the inferior perforating
Fig. 3. Selective undermining, diastasis demarcation, preserva-tion of the Scarpa facia, and the inferior fuse demarcation to beremoved.
Fig. 4. Perforating vessels.
Fig. 2. (Above) Horizontal marking (12 cm), (center) obliquemarking (8 cm), and (below) initial distance from the pubis (6to 7 cm).
Volume 129, Number 5S • Lipoabdominoplasty
79S

vessels; it is a homogeneous support for the upperflap, which becomes thinner on its descent; and itprovides smaller scars laterally and offers better ad-herence between the flap and the deep layers.
Resection of the Infraumbilical Fuse and RectusMuscle Plication
In the median infraumbilical line, we removea vertical fuse that contains the Scarpa fascia andadipose tissue to expose the internal edges of therectus abdominal muscles and to perform the pli-cation from the xiphoid to the pubic symphysis(Figs. 6 and 7).
OmphaloplastyWe use the star-shaped omphaloplasty tech-
nique, which is a cross-demarcation on the abdom-inal wall and a rectangular demarcation on the um-bilical pedicle. The cardinal points of the umbilicalpedicle are sutured, accommodating themselves onthe cruciform incision of the abdominal wall. Weperform the resulting scar in continuous Z-plastythat offers little possibility of retraction (Fig. 8).
Suture of the LayersWe perform the suture of the abdomen in two
layers using 3-0 Monocryl (Ethicon, Inc., Somer-ville, N.J.) on the deep layer and 4-0 Monocryl onthe subdermis, attempting to take the tension offthe midline skin closure by placing more tensionlaterally, as recommended by Lockwood.17 We su-ture the skin with 5-0 mononylon, with separatestitches (Fig. 9). We use a continuous aspirationdrain (4.2 mm) for 1 or 2 days (Fig. 9). The op-eration takes approximately 2 hours and the pa-tient stays in the hospital for 1 day.
Fig. 6. Resection of the infraumbilical fuse.
Fig. 7. Rectus abdominal muscle plication.
Fig. 8. Star-shaped omphaloplasty closure.
Fig. 5. The Saldanha retractor.
Plastic and Reconstructive Surgery • Spring 2012
80S

DressingTo dress the wound, we use Micropore sur-
gical tape (3M, St. Paul, Minn.) on the suture,which is changed on the third and eighth daysafter surgery, when we remove the stitches, ex-cept those on the umbilicus, which are removedon the twelfth day after surgery. The patientneeds to use compressive mesh for 20 days aftersurgery.
Postoperative PeriodPatients who undergo lipoabdominoplasty
present an intermediary recovery between anabdominoplasty and a liposuction because thelipoabdominoplasty is less invasive and causeslittle vascular and nervous trauma other thanpresenting a discrete dead space. These factorstogether result in less morbidity. With thismethod, patients return to their social and pro-fessional activities earlier.
RESULTSThe safe association of liposuction and ab-
dominoplasty during the same surgical proce-dure improves the results, including a greaterreduction in abdominal measures and betterbody contour. The patient satisfaction resultingfrom abdominal rejuvenation leads to an in-crease in surgical demand and a decrease in theneed for surgical revisions.
We compared the incidence of complicationswith traditional abdominoplasty to that with lipo-abdominoplasty. The 940 patients who underwentabdominal surgery, as mentioned in this article,were operated on and followed by the senior au-thor (O.R.S.) from 1979 to 2007.
From 1979 to 2000, the senior author per-formed 494 traditional abdominoplasty opera-tions. In 2000, the senior author began to developlipoabdominoplasty and in 2001 it was standard-ized, corresponding to 445 procedures until 2007.In that year, there was only one traditional ab-dominoplasty because it was a specific case of skinexcess in a post-bariatric surgery patient.
In the first 8 years of technique implementa-tion, there was an increase of 100 percent in theabdominal interventions made by the senior au-thor (before 2000, there was an average of 35patients per year; in 2007, there was an average of70 patients per year). The same does not occur tointerventions in other parts of the body. There wasa 50 percent reduction in the need for surgicalrevisions in the same period.
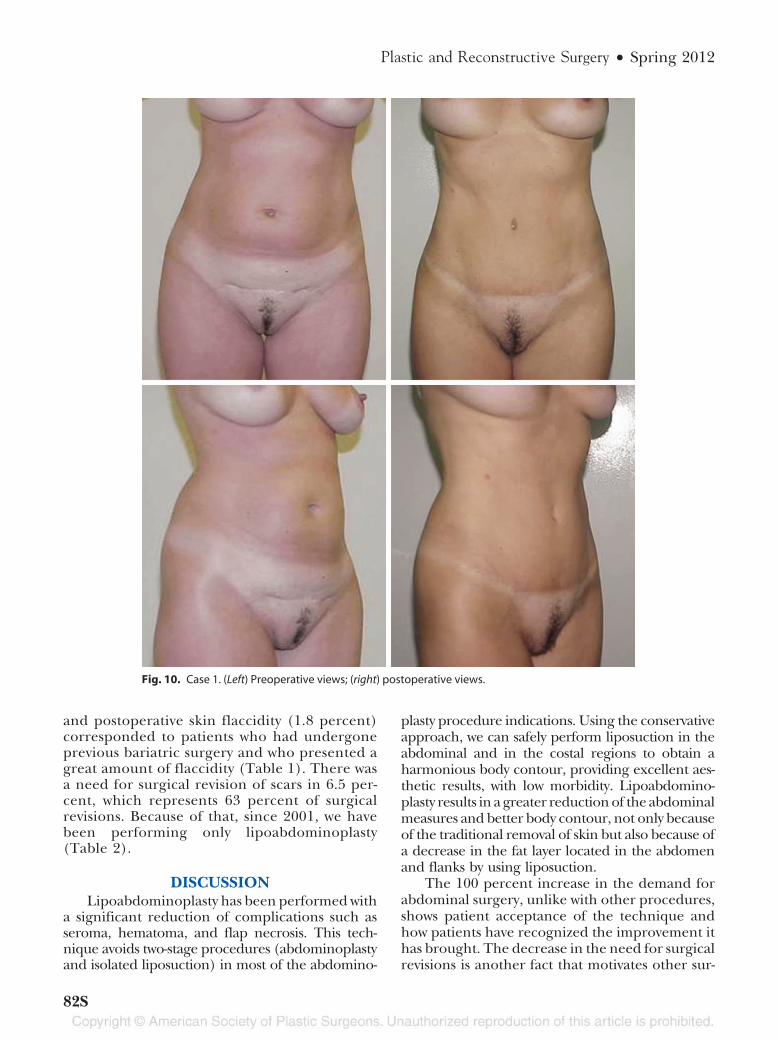
We observed a decrease in the final scar ex-tension when compared with the initial markingin 30 percent of patients. The initial line alwaysmeasured 28 cm in length: 12 cm horizontal and8 cm oblique on each side. In the 445 patients, 134had a final scar between 25 and 27 cm, with anaverage reduction of 2 cm from the initial mark-ing. This is attributable to the traction that theScarpa fascia makes on the skin. The gracefulshape of the umbilicus scar has been evaluated bythe team and the patients as good or excellent(Figs. 10 and 11).
COMPLICATIONSFollowing the surgical steps systematically and
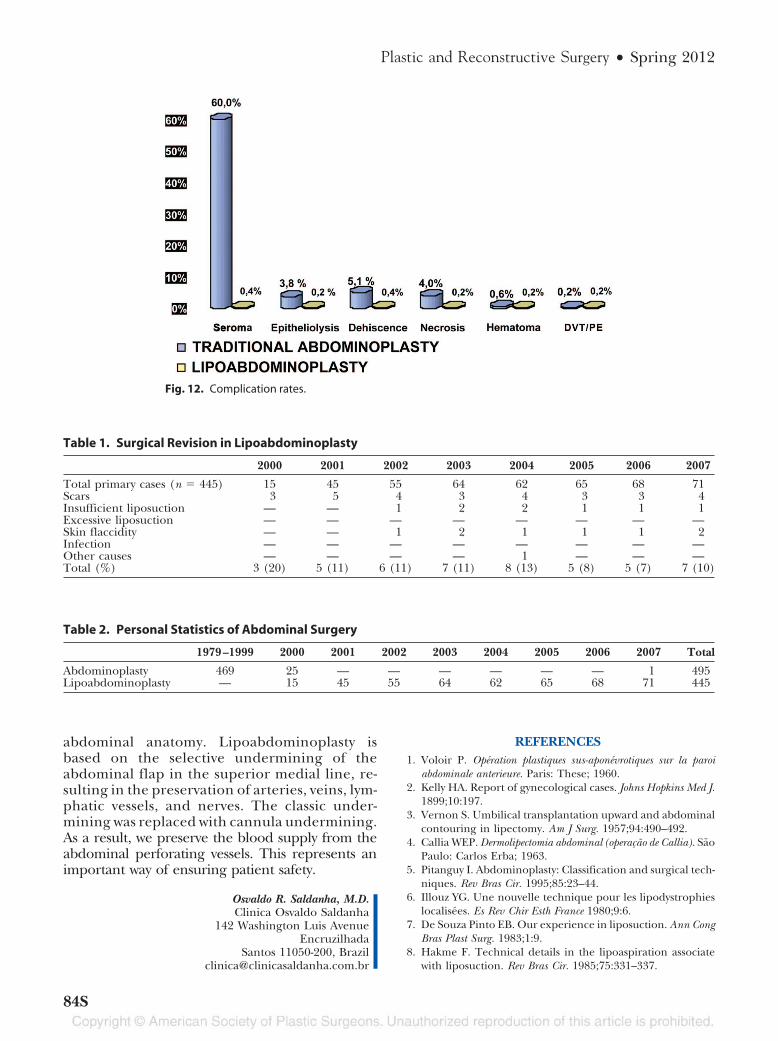
carefully reduces considerably such complicationsas abdominal flap ischemia and skin necrosis,which are difficult to treat and which can jeopar-dize the doctor-patient relationship (Fig. 12).
The reduced incidence of seroma (from 60percent to 0.4 percent, p � 0.0001), epitheliolysis(from 3.8 percent to 0.2 percent, p � 0.0003),dehiscence (from 5.1 percent to 0.4 percent, p �0.0001), and necrosis (from 4 percent to 0.2 per-cent, p � 0.0002) has statistical significance. Al-though the incidence of hematoma was reduced(from 0.6 percent to 0.2 percent) and the incidenceof deep venous thrombosis/pulmonary embolismremained the same (0.2 percent), we cannot con-sider these findings as statistically significant becauseof the small number of cases. All of these rates canbe observed if we compare traditional abdomino-plasty with lipoabdominoplasty.
In the same way, the percentage of surgicalrevisions decreased from 20 percent to 10 percentwhen only lipoabdominoplasty was performed, re-maining so for 7 years. The cases of surgical revi-sion resulting from complementary liposuction
Fig. 9. The two-layer suture.
Volume 129, Number 5S • Lipoabdominoplasty
81S
and postoperative skin flaccidity (1.8 percent)corresponded to patients who had undergoneprevious bariatric surgery and who presented agreat amount of flaccidity (Table 1). There wasa need for surgical revision of scars in 6.5 per-cent, which represents 63 percent of surgicalrevisions. Because of that, since 2001, we havebeen performing only lipoabdominoplasty(Table 2).
DISCUSSIONLipoabdominoplasty has been performed with
a significant reduction of complications such asseroma, hematoma, and flap necrosis. This tech-nique avoids two-stage procedures (abdominoplastyand isolated liposuction) in most of the abdomino-
plasty procedure indications. Using the conservativeapproach, we can safely perform liposuction in theabdominal and in the costal regions to obtain aharmonious body contour, providing excellent aes-thetic results, with low morbidity. Lipoabdomino-plasty results in a greater reduction of the abdominalmeasures and better body contour, not only becauseof the traditional removal of skin but also because ofa decrease in the fat layer located in the abdomenand flanks by using liposuction.
The 100 percent increase in the demand forabdominal surgery, unlike with other procedures,shows patient acceptance of the technique andhow patients have recognized the improvement ithas brought. The decrease in the need for surgicalrevisions is another fact that motivates other sur-
Fig. 10. Case 1. (Left) Preoperative views; (right) postoperative views.
Plastic and Reconstructive Surgery • Spring 2012
82S
geons to perform this technique. The use of vac-uum drainage is important for draining the liquidinjected during liposuction.
In addition, the technique results in the pres-ervation of suprapubic sensibility, quicker healing,faster postoperative recovery, lower morbidity,and a better appearing shape of the umbilicusscar. It also proves to be particularly indicated forsmokers because of the preservation of the per-forating abdominal vessels.
CONCLUSIONSTraditional abdominal plastic surgery is associ-
ated with a high rate of morbidity, because of thenecessity for undermining of large areas of the flap
where the perforating vessels are sectioned, takinginto consideration that they represent 80 percent ofthe blood supply of the abdominal wall, according tothe literature on this subject.25–30 Lipoabdomino-plasty is based on the selective undermining of theabdominal flap on the superior medial line, preserv-ing the great majority of the arteries, lymphatic ves-sels, veins, and nerves, which reduces the incidenceof complications. However, a progressive adaptationof this technique is necessary, starting with cases inwhich there is a large amount of skin flaccidity andsufficient adipose accumulation to permit liposuc-tion and easy liberation of the flap.
This technique is not simply using liposuctionwhile performing abdominoplasty. It represents amuch wider concept, respecting the complete
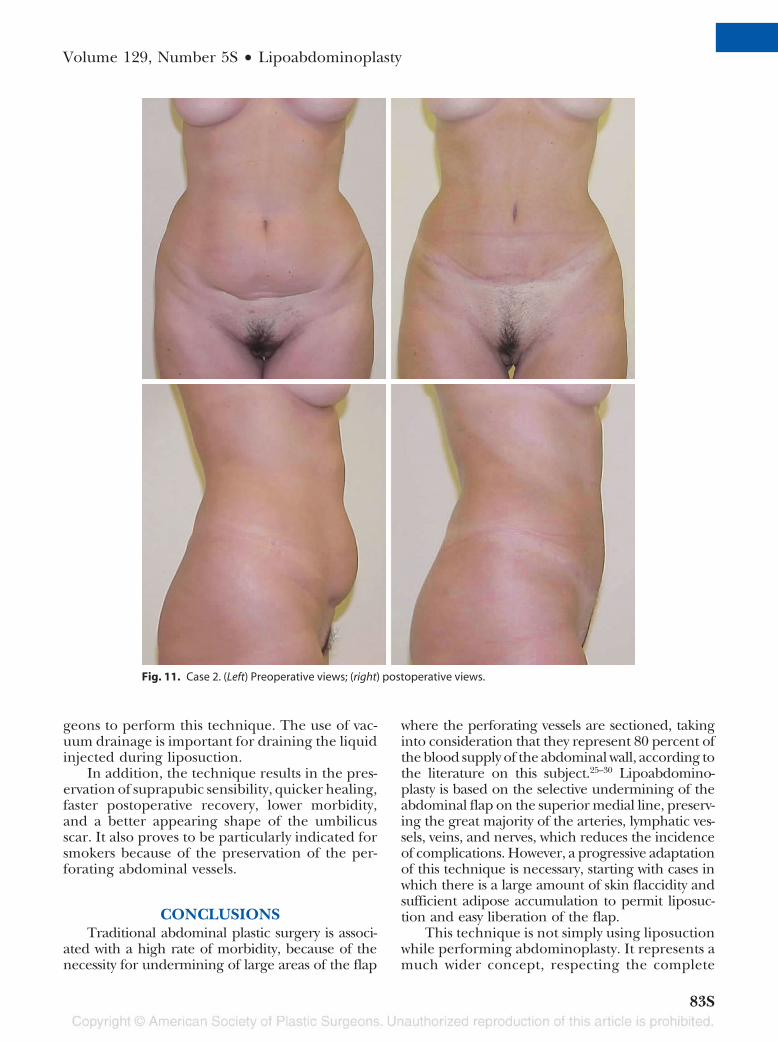
Fig. 11. Case 2. (Left) Preoperative views; (right) postoperative views.
Volume 129, Number 5S • Lipoabdominoplasty
83S
abdominal anatomy. Lipoabdominoplasty isbased on the selective undermining of theabdominal flap in the superior medial line, re-sulting in the preservation of arteries, veins, lym-phatic vessels, and nerves. The classic under-mining was replaced with cannula undermining.As a result, we preserve the blood supply from theabdominal perforating vessels. This represents animportant way of ensuring patient safety.
Osvaldo R. Saldanha, M.D.Clinica Osvaldo Saldanha
142 Washington Luis AvenueEncruzilhada
Santos 11050-200, [email protected]
REFERENCES1. Voloir P. Operation plastiques sus-aponevrotiques sur la paroi
abdominale anterieure. Paris: These; 1960.2. Kelly HA. Report of gynecological cases. Johns Hopkins Med J.
1899;10:197.3. Vernon S. Umbilical transplantation upward and abdominal
contouring in lipectomy. Am J Surg. 1957;94:490–492.4. Callia WEP. Dermolipectomia abdominal (operacao de Callia). Sao
Paulo: Carlos Erba; 1963.5. Pitanguy I. Abdominoplasty: Classification and surgical tech-
niques. Rev Bras Cir. 1995;85:23–44.6. Illouz YG. Une nouvelle technique pour les lipodystrophies
localisees. Es Rev Chir Esth France 1980;9:6.7. De Souza Pinto EB. Our experience in liposuction. Ann Cong
Bras Plast Surg. 1983;1:9.8. Hakme F. Technical details in the lipoaspiration associate
with liposuction. Rev Bras Cir. 1985;75:331–337.
Table 1. Surgical Revision in Lipoabdominoplasty
2000 2001 2002 2003 2004 2005 2006 2007
Total primary cases (n � 445) 15 45 55 64 62 65 68 71Scars 3 5 4 3 4 3 3 4Insufficient liposuction — — 1 2 2 1 1 1Excessive liposuction — — — — — — — —Skin flaccidity — — 1 2 1 1 1 2Infection — — — — — — — —Other causes — — — — 1 — — —Total (%) 3 (20) 5 (11) 6 (11) 7 (11) 8 (13) 5 (8) 5 (7) 7 (10)
Table 2. Personal Statistics of Abdominal Surgery
1979–1999 2000 2001 2002 2003 2004 2005 2006 2007 Total
Abdominoplasty 469 25 — — — — — — 1 495Lipoabdominoplasty — 15 45 55 64 62 65 68 71 445
Fig. 12. Complication rates.
Plastic and Reconstructive Surgery • Spring 2012
84S

9. Matarasso A. Abdominoplasty: A system of classification andtreatment for combined abdominoplasty and suction-as-sisted lipectomy. Aesthetic Plast Surg. 1991;15:111–121.
10. Matarasso A. Liposuction as an adjunct to full abdomino-plasty. Plast Reconstr Surg. 1995;95:829–836.
11. Illouz YG. A new safe and aesthetic approach to suctionabdominoplasty. Aesthetic Plast Surg. 1992;16:237–245.
12. Lockwood T. High-lateral-tension abdominoplasty with su-perficial fascial system suspension. Plast Reconstr Surg. 1995;96:603–608.
13. Lockwood T. The role of excisional lifting in body contoursurgery. Clin Plast Surg. 1996;23:695–712.
14. Shestak KC. Marriage abdominoplasty expands the mini-ab-dominoplasty concept. Plast Reconstr Surg. 1999;103:1020–1031.
15. Avelar JM. Abdominoplasty: A new technique without un-dermining and fat layer removal. Arq Catarinense Med. 2000;291:147–149.
16. Saldanha OR, Pinto EB, Matos WN Jr, Lucon RL, MagalhaesF, Bello EM. Lipoabdominoplasty without undermining. Aes-thet Surg J. 2001;21:518–526.
17. Vila-Rovira R. Liposuccion en cirugıa plastica y estetica. Es-pafıa: Salvat; 1988:81–85.
18. Willkinson TS, Swartz BE. Individual modifications in bodycontour surgery: The “limited” abdominoplasty. Plast Recon-str Surg. 1986;77:779–784.
19. Cardoso de Castro C, Salema R, Atias P, Aboudib JH Jr. Tabdominoplasty to remove multiple scars from the abdomen.Ann Plast Surg. 1984;12:369–373.
20. Saldanha OR, De Souza Pinto EB, Mattos WN Jr, et al. Li-poabdominoplasty with selective and safe undermining. Aes-thetic Plast Surg. 2003;22:322–327.
21. Saldanha OR. Lipoabdominoplastia. Rio de Janeiro, Brazil:Di-Livros; 2004.
22. Saldanha OR. Lipoabdominoplasty. Rio de Janeiro, Brazil:DiLivros; 2006.
23. Saldanha OR. Lipoabdominoplastia. Caracas, Venezuela: Amo-lca; 2007.
24. De Souza Pinto EB. Superficial Liposuction. Rio de Janeiro:Revinter; 1999:1–4.
25. Boyd JB, Taylor CI, Corlett R. The vascular territories of thesuperior epigastric and the deep inferior epigastric systems.Plast Reconstr Surg. 1984;73:1–16.
26. El-Mrakby HH, Milner RH. The vascular anatomy of thelower anterior abdominal wall: A microdissection study onthe deep inferior epigastric vessels and the perforatorbranches. Plast Reconstr Surg. 2002;109:539–543; discussion544–547.
27. Taylor GI, Watterson PA, Zelt RG. The vascular anatomy ofthe anterior abdominal wall: The basis for flap design. PerspectPlast Surg. 1991;5:1.
28. Munhoz AM, Ishida LH, Montag E, Sturtz G, Rodrigues L,Ferreira MC. Perforator vessels anatomy and clinical appli-cation in deep inferior epigastric perforator (DIEP) flap.Kongr Verein Deutsc Plast Chir. 2001;32:1–2.
29. Munhoz AM, Ishida LH, Sturtz G, et al. Importance of thelateral row perforator vessels in deep inferior epigastricperforator flap harvesting. Plast Reconstr Surg. 2004;113:517–524.
30. Graf R. Lipoabdominoplasty: Fluxmetry study and technicalvariation. In: Lipoabdominoplasty. Rio de Janeiro, Brazil: DiLiv-ros; 2006.
Volume 129, Number 5S • Lipoabdominoplasty
85S