Correlation of Genetic Instability with Mismatch Repair ... · Correlation of Genetic Instability...
9
Advances in Brief Correlation of Genetic Instability with Mismatch Repair Protein Expression and p53 Mutations in Non-Small Cell Lung Cancer 1 Jer-Wei Chang, Yi-Chun Chen, Chih-Yi Chen, Jung-Ta Chen, Shin-Kuang Chen, and Yi-Ching Wang 2 Institute of Toxicology, Chung Shan Medical College, Taichung [J- W. C., Y-C. C., S-K. C.]; Departments of Thoracic Surgery [C-Y. C.] and Pathology [J-T. C.], Veterans General Hospital–Taichung, Taichung; and Department of Biology, National Taiwan Normal University, Taipei [Y-C. W.], Taiwan, Republic of China Abstract To examine the etiological association of genetic insta- bility in lung tumorigenesis, we investigated the frequency of microsatellite instability (MI) of eight dinucleotide repeat markers in 68 patients with non-small cell lung cancer. Twenty-eight patients (41.2%) evidenced instability in mul- tiple tested microsatellite markers ranging from 3–7 and were defined as MI-positive patients. MI occurred more frequently in patients suffering from squamous cell lung carcinoma (P 5 0.004). We examined the association be- tween MI and expression of hMLH1 mismatch repair pro- tein by immunohistochemical analysis of hMLH1 protein in paraffin-embedded tumors from 64 patients. Twenty MI- positive patients (76.9%) had no expression of hMLH1 pro- tein. The data showed that MI was associated with altered hMLH1 expression (P 5 0.03). To examine the role of genetic instability in the previous identified small intragenic deletion of the p53 gene, we explored the association between MI and p53 gene mutations. All patients, except one, con- taining small intragenic deletion in p53 gene showed MI (P 5 0.018). In addition, we found that MI was not associ- ated with the prognosis. Our data suggest that MI plays a significant role in non-small cell lung cancer tumorigenesis in Taiwan and that MI is associated with the altered ex- pression of hMLH1 mismatch repair protein. In addition, MI may be involved in frequent small intragenic deletions of p53 gene. Introduction MI 3 represents expansions or contractions of the short- tandem repeat sequences (microsatellites) in one or both alleles in tumor DNA as compared with matching normal DNA. Mi- crosatellites are prone to strand-slippage during replication and defective mismatch repair (1). MI has been shown to be a marker for genetic instability in HNPCC and is thought to reflect multiple replication errors from abnormalities of the mismatch repair genes, such as hMSH2 and hMLH1 (2– 4). The MI phenotype has also been found in a substantial number of sporadic colon carcinomas (5–7) and in tumors of several other organs (reviewed in Ref. 8). However, the cause of MI in sporadic tumors is less clear. Somatic mutations of mismatch repair genes have been shown in only a proportion of colon and endometrial tumors with MI (9, 10). However, immunohisto- chemical analysis has demonstrated that loss of mismatch repair protein (mainly hMLH1) occurs frequently in sporadic colon cancer and gastric cancer with MI (6, 7, 11, 12). MI has also been described in LC. In SCLC, 45–76% of primary tumors are found to have MI in the form of deletion or expansion of dinucleotide or tetranucleotide repeats (13, 14). However, in the other major subtype of LC, NSCLC, there have been conflicting data regarding MI frequencies (ranging from 0 – 69%) and patterns (15–25). For example, no MI was found in 87 LC patients in Finland (21). Significantly different results were reported, however, in another study of 35 NSCLC patients in whom instabilities occurred at a rate of 69% and affected several microsatellite markers concurrently (22). In addition, there has been little evidence in NSCLC that the MI is associ- ated with an alteration of mismatch repair genes. In our previous study on the mutation spectrum of the p53 tumor suppressor gene in LC patients, distinct patterns of p53 gene mutation were observed (26). Seven of the 11 mutations detected (64%) were deletions of 1–12 bp at G:C bp, or at bp in the immediate vicinity of repetitive sequences and/or tandem repeat sequences. Our data suggest that a distinct environmental factor(s) and/or genetic factor(s) that specifically induces short deletions in repeat sequences is involved in lung tumorigenesis in Taiwan. These deletion mutations may be produced during the progression of lung tumorigenesis resulting from endoge- nous mechanisms, such as DNA polymerase replication errors and/or mismatch DNA repair deficiencies. To examine the eti- ological association of MI in lung tumorigenesis and the possi- ble involvement of genetic instability of patients with small intragenic deletions from the p53 gene, we investigated the frequency of the MI of eight polymorphic markers in 68 NSCLC patients. We also explored the association between acquisition Received 10/20/99; revised 2/23/00; accepted 2/24/00. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported in part by Grant DOH86-HR-611 from the National Health Research Institute (Department of Health, The Executive Yuan, Repub- lic of China) and by Grants NSC 87-2314-B-040-024 and NSC 89-2318- B-003-001-M51 from the National Science Council (The Executive Yuan, Republic of China). 2 To whom requests for reprints should be addressed, at Department of Biology, National Taiwan Normal University, No. 88, Sec. 4, Tingchou Road, Taipei 116, Taiwan, Republic of China. Phone: 886-2-29336876, ext. 211; Fax: 886-2-29312904; E-mail: [email protected]. 3 The abbreviations used are: MI, microsatellite instability; SQ, squa- mous cell carcinoma; AD, adenocarcinoma; LC, lung cancer; NSCLC, non-small-cell LC; HNPCC, hereditary nonpolyposis colorectal cancer; RII gene, transforming growth factor b type II receptor gene. 1639 Vol. 6, 1639 –1646, May 2000 Clinical Cancer Research Research. on July 8, 2020. © 2000 American Association for Cancer clincancerres.aacrjournals.org Downloaded from
Transcript of Correlation of Genetic Instability with Mismatch Repair ... · Correlation of Genetic Instability...

Advances in Brief
Correlation of Genetic Instability with Mismatch Repair ProteinExpression andp53 Mutations in Non-Small Cell Lung Cancer1
Jer-Wei Chang, Yi-Chun Chen, Chih-Yi Chen,Jung-Ta Chen, Shin-Kuang Chen, andYi-Ching Wang2
Institute of Toxicology, Chung Shan Medical College, Taichung [J-W. C., Y-C. C., S-K. C.]; Departments of Thoracic Surgery [C-Y. C.]and Pathology [J-T. C.], Veterans General Hospital–Taichung,Taichung; and Department of Biology, National Taiwan NormalUniversity, Taipei [Y-C. W.], Taiwan, Republic of China
AbstractTo examine the etiological association of genetic insta-
bility in lung tumorigenesis, we investigated the frequency ofmicrosatellite instability (MI) of eight dinucleotide repeatmarkers in 68 patients with non-small cell lung cancer.Twenty-eight patients (41.2%) evidenced instability in mul-tiple tested microsatellite markers ranging from 3–7 andwere defined as MI-positive patients. MI occurred morefrequently in patients suffering from squamous cell lungcarcinoma (P 5 0.004). We examined the association be-tween MI and expression of hMLH1 mismatch repair pro-tein by immunohistochemical analysis of hMLH1 protein inparaffin-embedded tumors from 64 patients. Twenty MI-positive patients (76.9%) had no expression of hMLH1 pro-tein. The data showed that MI was associated with alteredhMLH1 expression (P 5 0.03). To examine the role ofgenetic instability in the previous identified small intragenicdeletion of thep53gene, we explored the association betweenMI and p53 gene mutations. All patients, except one, con-taining small intragenic deletion in p53 gene showed MI(P 5 0.018). In addition, we found that MI was not associ-ated with the prognosis. Our data suggest that MI plays asignificant role in non-small cell lung cancer tumorigenesisin Taiwan and that MI is associated with the altered ex-pression of hMLH1 mismatch repair protein. In addition,MI may be involved in frequent small intragenic deletions ofp53 gene.
IntroductionMI3 represents expansions or contractions of the short-
tandem repeat sequences (microsatellites) in one or both allelesin tumor DNA as compared with matching normal DNA. Mi-crosatellites are prone to strand-slippage during replication anddefective mismatch repair (1). MI has been shown to be amarker for genetic instability in HNPCC and is thought toreflect multiple replication errors from abnormalities of themismatch repair genes, such ashMSH2andhMLH1 (2–4). TheMI phenotype has also been found in a substantial number ofsporadic colon carcinomas (5–7) and in tumors of several otherorgans (reviewed in Ref. 8). However, the cause of MI insporadic tumors is less clear. Somatic mutations of mismatchrepair genes have been shown in only a proportion of colon andendometrial tumors with MI (9, 10). However, immunohisto-chemical analysis has demonstrated that loss of mismatch repairprotein (mainly hMLH1) occurs frequently in sporadic coloncancer and gastric cancer with MI (6, 7, 11, 12).
MI has also been described in LC. In SCLC, 45–76% ofprimary tumors are found to have MI in the form of deletion orexpansion of dinucleotide or tetranucleotide repeats (13, 14).However, in the other major subtype of LC, NSCLC, there havebeen conflicting data regarding MI frequencies (ranging from0–69%) and patterns (15–25). For example, no MI was found in87 LC patients in Finland (21). Significantly different resultswere reported, however, in another study of 35 NSCLC patientsin whom instabilities occurred at a rate of 69% and affectedseveral microsatellite markers concurrently (22). In addition,there has been little evidence in NSCLC that the MI is associ-ated with an alteration of mismatch repair genes.
In our previous study on the mutation spectrum of thep53tumor suppressor gene in LC patients, distinct patterns ofp53gene mutation were observed (26). Seven of the 11 mutationsdetected (64%) were deletions of 1–12 bp at G:C bp, or at bp inthe immediate vicinity of repetitive sequences and/or tandemrepeat sequences. Our data suggest that a distinct environmentalfactor(s) and/or genetic factor(s) that specifically induces shortdeletions in repeat sequences is involved in lung tumorigenesisin Taiwan. These deletion mutations may be produced duringthe progression of lung tumorigenesis resulting from endoge-nous mechanisms, such as DNA polymerase replication errorsand/or mismatch DNA repair deficiencies. To examine the eti-ological association of MI in lung tumorigenesis and the possi-ble involvement of genetic instability of patients with smallintragenic deletions from thep53 gene, we investigated thefrequency of the MI of eight polymorphic markers in 68 NSCLCpatients. We also explored the association between acquisition
Received 10/20/99; revised 2/23/00; accepted 2/24/00.The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisementin accordance with 18 U.S.C. Section 1734 solely toindicate this fact.1 Supported in part by Grant DOH86-HR-611 from the National HealthResearch Institute (Department of Health, The Executive Yuan, Repub-lic of China) and by Grants NSC 87-2314-B-040-024 and NSC 89-2318-B-003-001-M51 from the National Science Council (The ExecutiveYuan, Republic of China).2 To whom requests for reprints should be addressed, at Department ofBiology, National Taiwan Normal University, No. 88, Sec. 4, TingchouRoad, Taipei 116, Taiwan, Republic of China. Phone: 886-2-29336876,ext. 211; Fax: 886-2-29312904; E-mail: [email protected].
3 The abbreviations used are: MI, microsatellite instability; SQ, squa-mous cell carcinoma; AD, adenocarcinoma; LC, lung cancer; NSCLC,non-small-cell LC; HNPCC, hereditary nonpolyposis colorectal cancer;RII gene,transforming growth factorb type II receptor gene.
1639Vol. 6, 1639–1646, May 2000 Clinical Cancer Research
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Table 1 Clinicopathological and molecular data of 68 NSCLC patients
Case Sex AgeSmoking
habits Typea StagehMLH1b
expressionp53c
mutation
Microsatellite markersd
D3S1215 D3S1292 D9S126 D9S162 D10S185 D13S170 D17S5 D17S786
MI-positive patientse
1 M 75 Y SQ IIIa Yes Del 1 1 1 1 12 M 66 Y SQ IIIa – Pt 1 1 1 1 13 M 72 Y AD IIIa – Pt 1 1 1 1 14 M 82 Y SQ I Yes Del LOH 1 1 1 15 M 68 Y SQ IIIa – Del 1 1 1 16 F 40 N SQ I – Del 1 1 17 M 73 Y SQ I – Del LOH 1 1 18 M 73 Y SQ IIIa – Del LOH 1 1 19 M 70 Y SQ I – – 1 1 1 1 1 1 1
10 M 76 Y SQ I Yes – 1 1 1 1 1 111 M 70 Y SQ II – – 1 1 1 1 1 112 F 46 N AD IIIa – – 1 1 1 1 1 113 M 68 Y SQ II Yes – 1 1 1 1 114 F 59 N LC IIIa ND – LOH 1 1 1 1 115 M 68 Y SQ I – – 1 1 1 116 M 72 Y SQ I – – 1 1 1 117 M 69 Y SQ I – – 1 1 1 118 M 66 Y SQ II – – 1 1 1 119 M 73 Y SQ IIIa – – 1 1 1 120 F 68 N AD I – – 1 1 1 121 M 70 Y AD II ND – 1 1 1 122 M 75 Y AD IIIa – – 1 1 1 123 M 57 Y SQ I Yes – LOH 1 1 124 M 75 Y SQ I Yes – 1 1 1 LOH25 M 50 Y SQ II – – 1 1 126 M 76 Y SQ II – – LOH 1 1 127 M 77 Y SQ II – – 1 1 128 F 76 N AD I – – 1 1 1
MI-negative patients29 M 69 Y SQ IIIa – – 1 130 M 67 N AD I Yes – 1 131 M 76 Y AD I Yes – 1 132 M 67 Y AD II – – LOH 1 133 M 67 Y AS II Yes – 1 134 M 72 Y AS IIIa Yes – 1 135 M 75 Y SQ IIIa ND Del 1 136 M 69 N AS IIIa – Pt 1 137 M 72 N SQ II – Pt 138 M 67 Y SQ I Yes – 139 M 74 Y SQ II – – 140 M 70 Y SQ IIIa – – 141 M 86 Y AD I – – 142 M 68 Y AD I Yes – 143 M 69 N AD I Yes – 144 M 69 Y AD II Yes – 145 M 68 Y AD III – – 146 M 51 N AD IIIa Yes – 147 F 64 N AD IIIa – – 148 M 61 Y AS IIIa Yes – 149 M 68 Y AS IIIa Yes – 1 LOH50 M 70 Y LC I Yes –51 M 80 Y SQ II – –52 M 67 Y AD I – –53 F 74 N SQ I Yes –54 M 70 Y AD I – –55 M 78 Y SQ II – –56 M 70 N SQ II – –57 F 43 N AD IIIa Yes –58 M 80 Y AD IIIa – –59 M 73 Y AD I – –60 M 68 Y SQ I Yes –61 M 69 Y AD IIIa – –62 M 62 Y SQ IV – –63 M 70 Y SQ IIIb Yes ND64 M 68 N AD I Yes –65 F 69 N AD I ND ND66 M 72 Y SQ IIIa – ND67 M 48 N AD IIIa Yes –68 M 76 Y SQ I Yes ND
a LC, large cell carcinoma; AS, adenosquamous carcinoma.b Yes, with hMLH1 expression; –, without hMLH1 expression.c Del, small intragenic deletion; Pt, point mutation; –, withoutp53 gene mutation; ND, not determined.d 1, patients with instability at the indicated marker; LOH, loss of heterozygosity.e MI-positive patients were defined as instability in three or more markers.
1640Genetic Instability and p53 Mutation in NSCLC
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

of a replication error phenotype, mismatch repair alteration, andp53 mutation. The clinical importance of MI was also investi-gated with regard to prognosis.
Materials and MethodsSamples and Preparation of DNA. Surgical specimens
were obtained from 68 patients with NSCLC (36 SQs, 25 ADs, 5adenosquamous carcinomas, and 2 large cell carcinomas). Thetumor types and stages were determined according to the WHOclassification method (27) and the tumor-node-metastasis system(28), respectively. The duration and amount of smoking beforediagnosis of LC patients were obtained from hospital records. Acumulative cigarette pack-year history for each patient was thencalculated. The patients were classified into smoking and nonsmok-ing groups. The number of years since last smoking for all ex-smokers was,10 yr. Therefore, the smoking group included bothcurrent smokers and ex-smokers. Follow-up of all patients wasperformed at 2-month intervals in the 1st yr after surgery and at3-month intervals thereafter, at outpatient clinics or by routinephone calls. The end of the follow-up period was defined asNovember 15, 1998, for all patients. The mean follow-up period forall patients was 18.9 months (range, 0.5–51). For the 22 patientswho survived the follow-up period (censored patients), the meanfollow-up time was 24.7 months. For the 46 patients who diedduring the follow-up period, the mean follow-up time was 11.9months. Representative proportions of well-separated normal lungtissues and tumoral lung tissues were taken after surgical resection,
immediately snap-frozen, and subsequently stored in liquid nitro-gen. Genomic DNA was prepared using proteinase K digestion andphenol/chloroform extraction, followed by ethanol precipitation.
Analysis of MI. MI was analyzed in all 68 patients byPCR using eight microsatellite markers on five differentchromosomes obtained as MAPPAIRS primers from Re-search Genetics (Huntsville, AL): D3S1215 (3q13), D3S1292(3q21–25.2), D9S126 (9p21), D9S162 (9p22–23), D10S185(10q23–24), D13S170 (13q22–31), D17S5 (17p13.3), andD17S786 (17p13.1). These markers were selected on thebasis of the fact that they had been analyzed in previousstudies (e.g., D3S1215, D3S1292, D9S162, D10S185,D13S170, and D17S5) and/or were located near the knowntumor suppressor genes (e.g., D9S162 and D17S786 arelocated near theCDKN2 and p53 tumor suppressor gene,respectively). For all markers, the following PCR conditionswere used: 0.5mM of each primer, 200mM dNTP, 2.5 units ofTaq polymerase, a standard polymerase buffer supplied withenzyme (1.5 mM MgCl2), and 150 ng of genomic DNA. Thetotal volume of the PCR mix was 25ml. The PCR tempera-ture program was: 95°C denaturation for 5 min; 35 cycles of1 min each at 95°C, 1.75 min at 55°C, and 1.75 min at 72°C;and a final extension run at 72°C for 10 min. The PCRproducts were denatured for 3 min at 95°C and run on a 6%polyacrylamide gel containing 7 M urea at 20 W for 4 –5 h.The gels were dried and exposed to radiographic film(X-OMAT; Kodak). MI was revealed by the presence of one
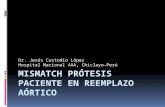
Fig. 1 Representative figures of microsatellite analysis of normal (N) and tumor (T) DNA of LC patients at theD3S1215,D3S1292,D9S126,D9S162,D10S185,D13S170,D17S5, andD17S786loci. The patient number (Pt’s no) is designated above each block. MI is shown as the contractionor expansion of a single band or a ladder of bands of the tumor DNA compared with the normal DNA. Loss of heterozygosity can be seen in the tumorDNA of patient 26 atD3S1215and of patients 49 and 24 atD17S5.
1641Clinical Cancer Research
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

or more novel bands (expansions or contractions of repeats)in the tumors, but absent in the paired normal DNA. MIpositive was defined as instability in three or more markers.This definition can be used to score MI positive unequivo-cally (29).
Analysis of hMLH1 Protein Expression–Immunohisto-chemistry Assay. Paraffin blocks of 64 tumors were cut into5-mm slices and then processed using standard deparaffinizationand rehydration techniques. A monoclonal antibody, G168-278(1:250; PharMingen), was used as the primary antibody to detecthMLH1 protein expression. The primary antibody was detectedusing biotinylated secondary antibody (DAKO LSAB KitK675), used as recommended by the manufacturer. The sectionswere then counterstained with hematoxylin. The normal stainingpattern for hMLH1 was nuclear. Tumor cells that exhibited anabsence of nuclear staining in the presence of nonneoplasticcells and infiltrating lymphocytes with nuclear staining wereconsidered to have an abnormal pattern. In addition, a section ofnormal colon was served as a positive control for immunohis-tochemical assay. The samples were assayed in batches, includ-ing both MI-positive and MI-negative patients. The stainingresults were examined without knowledge of the MI status. Eachsample was assayed by repeating analyses at least twice.
Analysis of p53 Mutation. PCR/single-stranded confor-mational polymorphism was used to detect the presence ofmutations in thep53 tumor suppressor gene of 64 patients.Oligodeoxynucleotide primers and thermocycle PCR conditionsdesigned to produce DNA fragments ofp53 gene exons 4–11are described in Ref. 30. PCR products were subjected toelectrophoresis at 30 W for 4–5 h in a 6% nondenaturingpolyacrylamide gel with 5% glycerol and fan-cooled at roomtemperature. Abnormal DNA fragments detected during PCR/single-stranded conformational polymorphism analysis were se-quenced using the dideoxy chain termination method, witha-35S-dATP, PCR-amplified primers, and a sequenase II kit(United States Biochemical Corporation).
Statistical Analysis. The Pearsonx2 test was used tocompare the possibility of MI among cases and between variousclinicopathological parameters. Type III censoring was per-formed on subjects who were still alive at the end of the study(31). The Kaplan-Meier method was used to estimate the prob-ability of survival as a function of time and the median survival(32). The log rank test was used to assess the significance of thedifference between pairs of survival probabilities (33).
ResultsMI in Lung Tumors. We examined MI in tumor DNA
from 68 NSCLC patients using eight dinucleotide repeat mark-ers. Table 1 lists the results of MI of analyzed lung tumors andincludes relevant clinical information. Twenty-eight patients(41.2%) evidenced instability in multiple-tested microsatellitemarkers ranging from 3–7 and are defined as MI-positive pa-tients. Patients 1–3 and 9–14 showed MI in five or moremarkers. Microsatellite marker alterations were mostly observedat D13S170 (45.6%), D9S162 (39.7%), D17S786 (33.8%),D10S185 (32.4%), and D3S1292 (30.9%). The frequencies ofMI in the remaining markers were 11.8% for D3S1215, 20.6%for D9S126, and 0% for D17S5. Representative results of the
MI analysis are shown in Fig. 1. The instability seemed as eitherexpansion or compression of a single band or a ladder of bands.
To examine the association of MI with the clinical charac-teristics of patients, the occurrence of MI was compared with thepatients’ clinicopathological parameters (Table 2). The inci-dence of MI positive was higher in SQ patients (61.1%, 22 of36) than in AD patients (24.0%, 6 of 25;P 5 0.004). However,similar ages, sexes, smoking histories, and clinical stages werenoted in both groups of patients, those with and without insta-bility.
Correlation with Altered Expression of hMLH1 Pro-tein. The paraffin-embedded tumors were available from 64patients. The expression of hMLH1 mismatch repair protein wasexamined in these patients, including 26 MI-positive patientsand 38 MI-negative patients (Table 1). The incidence of nega-tive hMLH1 expression was higher in MI-positive patients(76.9%, 20 of 26) than in MI-negative patients (50.0%, 19 of 38;Table 2). The data show that MI was associated with an alteredhMLH1 expression (P5 0.03). Representative results of theimmunohistochemistry analysis are shown in Fig. 2.
Correlation with p53Gene Mutations. Tumors from 64patients were analyzed for both MI andp53gene mutation. Fourpatients had a point mutation, and seven had a small intragenicdeletion in thep53 gene (Table 1). Fig. 3 shows the represent-
Table 2 Clinical features of MI-positive and -negative patients
Clinicalparameters Patient no.
No. (%) with MI
Pb1a —
Patient no. 68 28 (41.2) 40 (58.8)Age range
(mean6 SD)40–77 (686 9) 43–86 (696 8) 0.986
SexMale 59 23 (39.0) 36 (61.0) 0.347Female 9 5 (55.6) 4 (44.4)
Smoking habitsSmokers 51 22 (43.1) 29 (56.9) 0.569Nonsmokers 17 6 (35.3) 11 (64.7)
Tumor typesSQ 36 22 (61.1) 14 (38.9) 0.004c
AD 25 6 (24.0) 19 (76.0)AS 5 1 (20.0) 4 (80.0)LC 2 1 (50.0) 1 (50.0)
Tumor stagesI 1 II 42 19 (45.2) 23 (54.8) 0.387III 1 IV 26 9 (34.6) 17 (65.4)
hMLH1expressiond
Yes 25 6 (24.0) 19 (76.0) 0.030No 39 20 (51.3) 19 (48.7)
p53 intragenicdeletionc
Yes 7 6 (85.7) 1 (14.3) 0.018No 57 22 (38.6) 35 (61.4)
a MI-positive (1) was defined as instability in three or moremarkers.
b These results were analyzed by Pearsonx2 test, except for agerange between patients with and without MI, which was analyzed by atwo-samplet test.
c This result was based on comparison of the frequency of MIbetween SQ and AD patients.
d A total of 64 patients were analyzed for hMLH1 expression.e A total of 64 patients were analyzed forp53 gene mutation.
1642Genetic Instability and p53 Mutation in NSCLC
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

ative autographs of 6 of the 7 deletion mutations detected, whichwere deletions of 1–12 bp at G:C bp, or at bp in the immediatevicinity of repetitive sequences and/or tandem repeat sequences.Of these seven deletion patients, six (85.7%) evidenced insta-bility at three or more markers. There was a significant associ-ation betweenp53small intragenic deletion and MI (P5 0.018,Table 2).
Correlation with Cancer Prognosis. The survival ofpatients whose tumors showed MI positive was similar to thoseof MI negative (median survival times of 26 months for patientswith and without MI;P . 0.05 by the log rank test; Fig. 4). Inthe SQ group, survival was also not influenced by MI (data notshown).
DiscussionIn this study, 28 patients (41.2%) evidenced instability in
tested microsatellite markers ranging from 3–7 and were definedas MI-positive patients. The data indicated that TaiwaneseNSCLC patients had high frequencies of MI in multiple loci. InNSCLCs, the data on MI have been conflicting in regard tofrequencies and patterns (15–25). One proposed explanation forthe conflicting results is that MI is associated with specifictumor type and/or stage and that cancers of different types andstages were analyzed in the contrasting studies. It is also pos-sible that there are geographical and/or ethnic factors that causeMI. In addition, the varying results may be due, in part, todifferences in the types and number of primers analyzed, as wellas to the differences in the definition of MI. Microsatellite locion various chromosomes may have differing frequencies ofinstability. For instance, the frequencies of MI in the variousloci examined ranged from 0–45.6% in the present study.However, when comparing the MI frequency between differentstudies, the existence of common microsatellite marker(s)should be taken into consideration. For example, the frequency
of instability of D9S162 was 39.7% in our study, whereas thisfrequency was 0% and 1.8% in two previous studies on NSCLC(16, 21). Therefore, MI plays a significant role in NSCLCtumorigenesis in Taiwan.
We found that LC patients withp53 small intragenicdeletion had frequent MI. To our knowledge, this is the firststudy to demonstrate that MI occurs frequently in patientswith small intragenic deletion in thep53 gene. The highfrequency of small intragenic deletions in repetitive se-quences and/or tandem repeats is probably conservative inother regions of the genome of these patients. We proposethat the relatively high frequency of instability of the poly-morphic microsatellite sequences indicates a destabilizationof the genome that may affect other genes preferentially inrepetitive sequences and/or tandem repeats. In a subgroup ofNSCLCs, MI may predispose to further genetic alterations.The mutation spectrum analysis of other genes involved intumorigenesis was required to confirm this hypothesis.
A higher frequency of MI in SQ patients compared withAD patients suggests a difference in the genetic changes con-tributing to the tumorigenesis of SQ and AD in Taiwan. In fact,our analysis also indicated a higher frequency ofp53 mutationin SQ compared with that in AD (26). Furthermore, the fre-quency of MI was similar between early and advanced stages ofLC, whereas thep53 mutations occurred more frequently inpatients with advanced stages of LC (26). In addition, MI occursmore often than does thep53 mutation. These observationssuggest that MI may be an earlier molecular event comparedwith the p53 mutation during the pathogenesis of lung tumori-genesis in Taiwan.
Changes in the length of certain microsatellites have beencorrelated with changes in the expression of mismatch repairgenes in HNPCC and in other somatic tumors (6, 7, 11, 12).However, the data on mismatch repair protein expression in LC
Fig. 2 Representative figures of immunohistochemical analysis of hMLH1 protein in paraffin sections of lung tumor specimens. Nuclearimmunoreactivity was found in patient 48 (A) and patient 49 (B).C, negative tumor was from patient 2 with MI in multiple markers. Originalmagnification:A, 3200; B andC, 3100.
1643Clinical Cancer Research
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

is scarce. To our knowledge, this is the first report of a highfrequent alteration of hMLH1 mismatch repair protein in LC.We found a close relationship between hMLH1 mismatch repairprotein expression and MI status. Twenty (76.9%) MI-positivepatients showed no expression of hMLH1 mismatch repairprotein. However, six MI-positive patients showed a positivenuclear stain for hMLH1 protein. It is possible that there isaltered expression or mutation in one of the other mismatchrepair genes (hMSH2, hMSH3, hMSH6, or hPMS2) in thesepatients (34). Note that all patients, except two containingdeletion of thep53 gene, had a negative expression of hMLH1mismatch repair protein. However, due to the small numberanalyzed, no statistical correlation could be made regarding theeffect of hMLH1 alteration onp53 small intragenic deletion.
The association of MI with the altered expression ofhMLH1 mismatch repair protein and thep53 small intragenicdeletion may be unique to NSCLC in Taiwan. We are currentlyinvestigating the mRNA expression and the methylation statusof several mismatch repair genes, includinghMLH1 andhMSH2,in NSCLC patients. It is also very important to clarifywhether somatic mutations of known mismatch repair genes orcomponents involved in the replication system are responsiblefor the acquisition of MI in NSCLC in Taiwan. Alterations ofhMSH2and hMLH1 mismatch repair genes would point to anacquired mutator phenotype (3, 4). Mutations in theRII genehave also been shown to preferentially occur at microsatelliteregions and in tumors with genomic instability (34). In thesearch for genes and mechanisms involved in the instability of
Fig. 3 Autoradiographs of sequencing analyses of patients exhibiting deletion mutations of thep53 tumor suppressor gene. All sequences shown areof the sense strand. Some patients also exhibited wild-type alleles, which are also shown in the figure.A-F are from patients 1, 4, 8, 6, 7, and 35,respectively. Bases encoded by same amino acid are inbrackets.M, bases deleted. The areas around deleted bases are also shown. These data aretaken from Ref. 26.
1644Genetic Instability and p53 Mutation in NSCLC
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

lung tumors, we have also started a mutation analysis ofhMSH2andhMLH1 genes, as well as theRII gene.
AcknowledgmentsWe are grateful to Profs. Yuh-Shan Jou and Ming-Chei Maa for
critical revision of the manuscript.
References1. Strand, M., Prolla, T. A., Liskay, R. M., and Peters. T. D. Destabi-lization of tracts of simple repetitive DNA in yeast by mutations affect-ing DNA mismatch repair. Nature (Lond.),365: 274–276, 1993.2. Aaltonen, L. A., Peltomaki, P., Leach, F. S., Sistonen, P., Pylkkanen,L., Meckline, J. P., Jarvinen, H., Powell, S. M., Jen, J., Hamilton, S. R.,Petersen, G. M., Kinzler, K. W., Vogelstein, B., and De La Chapelle, A.Clues to the pathogenesis of familial colorectal cancer. Science (Wash-ington DC),260: 812–816, 1993.3. Fishel, R., Lescoe, M. K., Rao, M. R. S., Copeland, N. G., Jenkins,N. A., Garber, J., Kane, M., and Kolodner, R. The human mutator genehomologMSH2and its association with hereditary nonpolyposis coloncancer. Cell,75: 1027–1038, 1993.4. Bronner, C. E., Baker, S. M., Morrison, P. T., Warren, G., Smith, L. G.,Lescoe, M. K., Kane, M., Earabino, C., Lipford, J., Lindblom, A., Tanner-gard, P., Bollag, R. J., Godwin, A. R., Ward, D. C., Nordenskjold, M.,Fishel, R., Kolodner, R., and Liskay, R. M. Mutation in the DNA mismatchrepair gene homologuehMLH1 is associated with hereditary non-polyposiscolon cancer. Nature (Lond.),368: 258–261, 1994.5. Thibodeau, S. N., Bren, G., and Schaid, D. Microsatellite instabilityin cancer of the proximal colon. Science (Washington DC),260: 816–819, 1993.6. Thibodeau, S. N., French, A. J., Roche, P. C., Cunningham, J. M.,Tester, D. J., Lindor, N. M., Moslein, G., Baker, S. M., Liskay, R. M.,
Burgart, L. J., Honchel, R., and Halling, K. C. Altered expression ofhMSH2andhMLH1 in tumors with microsatellite instability and genetic alterationsin mismatch repair genes. Cancer Res.,56: 4836–4840, 1996.
7. Kane, M. F., Loda, M., Gaida, G. M., Lipman, J., Mishra, R.,Goldman, H., Jessup, J. M., and Kolodner, R. Methylation of thehMLH1 promoter correlates with lack of expression of hMLH1 insporadic colon tumors and mismatch repair-defective human tumor celllines. Cancer Res.,57: 808–811, 1997.8. Arzimanoglou, I. I., Gilbert, F., and Barber, H. R. K. Microsatelliteinstability in human solid tumors. Cancer (Phila.),82: 1808–1820,1998.9. Børresenn, A. L., Lothe, R. A., Meling, G. I., Lystad, P., Morrison,P., Lipford, J., Kane, M. F., Rognum, T. O., and Kolodner, R. D.Somatic mutations in thehMNSH2 gene in microsatellite unstablecolorectal carcinomas. Hum. Mol. Genet.,4: 2065–2072, 1995.10. Katabuchi, H., Van Rees, B., Lambers, A. R., Ronnett, B. M.,Blazes, M. S., Leach, F. S., Cho, K. R., and Hedrick, L. Mutations inDNA mismatch repair genes are not responsible for microsatellite in-stability in most sporadic endometrial carcinomas. Cancer Res.,55:5556–5560, 1995.11. Herman, J. G., Umar, A., Polyak, K., Graff, J. R., Ahuja, N., Issa,J. P. J., Markowitz, S., Willson, J. K. V., Hamilton, S. R., Kinzler,K. W., Kane, M. F., Kolodner, R. D., Vogelstein, B., Kunkel, T. A., andBaylin, S. B. Incidence and functional consequences ofhMLH1 pro-moter hypermethylation in colorectal carcinoma. Proc. Natl. Acad. Sci.USA, 95: 6870–6875, 1998.12. Leung, S. Y., Yuen, S. T., Chung, L. P., Chu, K. M., Chan, A. S. Y.,and Ho, J. C. I.hMLH1 promoter methylation and lack ofhMLH1expression in sporadic gastric carcinomas with high-frequency micro-satellite instability. Cancer Res.,59: 159–164, 1999.13. Merlo, A., Mabry, M., Gabrielson, E., Vollmer, R., Baylin, S. B.,and Sidransky, D. Frequent microsatellite instability in primary smallcell lung cancer. Cancer Res.,54: 2098–2101, 1994.14. Chen, X. Q., Stroun, M., Magnenat, J-L., Nicod, L. P., Kurt, A-M.,Lyautey, J., Lederrey, C., and Anker, P. Microsatellite alterations inplasma DNA of small cell lung cancer patients. Nat. Genet.,2: 1033–1037, 1996.15. Shridhar, V., Siegfried, J., Hunt, J., Del Mar Alonso, M., and Smith,D. I. Genetic instability of microsatellite sequences in many non-smallcell lung carcinomas. Cancer Res.,54: 2084–2087, 1994.16. Adachi, J-I., Shiseki, M., Okazaki, T., Ishimaru, G., Noguchi, M.,Hirohashi, S., and Yokota, J. Microsatellite instability in primary andmetastatic lung carcinomas. Genes Chromosomes Cancer,14: 301–306,1995.17. Fong, K. M., Zimmerman, P. V., and Smith, P. J. Microsatelliteinstability and other molecular abnormalities in non-small cell lungcancer. Cancer Res.,55: 28–30, 1995.18. Ryberg, D., Lindstedt, B. A., Zienolddiny, S., and Haugen, A. Ahereditary genetic marker closely associated with microsatellite insta-bility in lung cancer. Cancer Res.,55: 3996–3999, 1995.19. Miozzo, M., Sozzi, G., Musso, K., Pilotti, S., Incarbone, M., Pastorino,U., and Pierotti, M. A. Microsatellite alterations in bronchial and sputumspecimens of lung cancer patients. Cancer Res.,56: 2285–2288, 1996.20. Pifarre, A., Rosell, R., Monzo, M., De Anta, J. M., Moreno, I.,Sanchez, J. J., Ariza, A., Mate, J. L., Martınez, E., and Sanchez, M.Prognostic value of replication errors on chromosomes 2p and 3p innon-small-cell lung cancer. Br. J. Cancer,75: 184–189, 1997.21. Pylkkanen, L., Karjalainen, A., Anttila, S., Vainio, H., and Hus-gafvel-Pursiainen, K. No evidence of microsatellite instability but fre-quent loss of heterozygosity in primary resected lung cancer. Environ.Mol. Mutagen.,30: 217–223, 1997.22. Rosell, R., Pifarre, A., Monzo, M., Astudillo, J., Lopez-Cabrerizo,M. P., Calvo, R., Moreno, I., Sanchez-Cespedes, M., Font, A., andNavas-Palacios, J. J. Reduced survival in patients with stage-I non-small-cell lung cancer associated with DNA-replication errors. Int. J.Cancer,74: 330–334, 1997.23. Froudarakis, M. E., Sourvinos, G., Fournel, P., Bouros, D.,Vergnon, J-M., Spandidos, D. A., and Siafakas, N. M. Microsatellite
Fig. 4 The Kaplan-Meier survival curves with respect to MI.Ps wereobtained using the log rank test. The MI-positive group had similarprognoses as the MI-negative group (P5 0.81). Median survival timeswere both 26 months for patients with and without MI.
1645Clinical Cancer Research
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

instability and loss of heterozygosity at chromosomes 9 and 17 innon-small-cell lung cancer. Chest,113: 1091–1094, 1998.24. Gasparian, A. V., Laktionov, K. K., Belialova, M. S-O., Pirogova,N. A., Tatosyan, A. G., and Zborovskaya, I. B. Allelic imbalance andinstability of microsatellite loci on chromosome 1p in human non-small-cell lung cancer. Br. J. Cancer,77: 1604–1611, 1998.25. Suzuki, K., Ogura, T., Yokose, T., Sekine, I., Nagai, K., Kodama,T., Mukai, K., Nishiwaki, Y., and Esumi, H. Microsatellite instability infamilial clustering of malignancy. Br. J. Cancer,77: 1003–1008, 1998.26. Wang, Y-C., Chen, C-Y., Chen, S-K., Cherng, S-H., Ho, W-L., andLee, H. High frequency of deletion mutations inp53 gene from squa-mous-cell lung cancer patients in Taiwan. Cancer Res.,58: 328–333,1998.27. WHO. Histological typing of lung tumors. Am. J. Clin. Pathol.,77:123–126, 1982.28. Mountain, C. F. A new international staging system for lung cancer.Chest,89: 225–233, 1986.29. Dietmaier, W., Wallinger, S., Bocker, T., Kullmann, F., Fishel, R.,and Ruschoff, J. Diagnostic microsatellite instability: definition and
correlation with mismatch repair protein expression. Cancer Res.,57:4749–4756, 1997.
30. Lehman, T. A., Bennett, W. P., Metcalf, R. A., Welsh, J. A., Ecker,J., Modali, R. V., Ullrich, S., Romano, J. W., Appella, E., Testa, J. R.,Gerwin, B. I., and Harris, C. C.p53 mutations,ras mutations, andp53-heat shock 70 protein complexes in human lung carcinoma celllines. Cancer Res.,51: 4090–4096, 1991.
31. Lee, E. T. Statistical Methods for Survival Data Analysis, Ed. 2, pp.1–7. New York: John Wiley & Sons, Inc., 1992.32. Kaplan, E. L., and Meier, P. Nonparametric estimation from incom-plete observation. J. Am. Stat. Assoc.,53: 457–481, 1958.33. SAS Institute, Inc.. The lifetest procedure.In: SAS Technical Re-port: P-179. Additional SAS/STAT Procedures, Release 6.03, pp. 49–90. Cary, NC: SAS Institute, Inc., 1988.34. Markowitz, S., Wang, J., Myeroff, L., Parsons, R., Sun, L., Lutter-baugh, J., Fan, R. S., Zborowska, E., Kinzler, K. W., Vogelstein, B.,Brattain M., and Wilson, J. K. V. Inactivation of the type II TGF-breceptor in colon cancer cells with microsatellite instability. Science(Washington DC),268: 1336–1338. 1995.
1646Genetic Instability and p53 Mutation in NSCLC
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2000;6:1639-1646. Clin Cancer Res Jer-Wei Chang, Yi-Chun Chen, Chih-Yi Chen, et al.
Mutations in Non-Small Cell Lung Cancerp53Expression and Correlation of Genetic Instability with Mismatch Repair Protein
Updated version
http://clincancerres.aacrjournals.org/content/6/5/1639
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/6/5/1639.full#ref-list-1
This article cites 31 articles, 16 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/6/5/1639.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/6/5/1639To request permission to re-use all or part of this article, use this link
Research. on July 8, 2020. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from