
Corporate Overview - Achillion Pharmaceuticals · · 2017-12-27Achillion Complement Portfolio...
27
Corporate Overview September 2017 NASDAQ:ACHN ©2017 Achillion Pharmaceuticals. All rights reserved.
Transcript of Corporate Overview - Achillion Pharmaceuticals · · 2017-12-27Achillion Complement Portfolio...

Corporate Overview
September 2017
NASDAQ:ACHN ©2017 Achillion Pharmaceuticals. All rights reserved.
Forward-Looking Statements
This presentation includes forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 that are
subject to risks, uncertainties and other important factors that could cause actual results to differ materially from those indicated by such
forward-looking statements. Achillion may use words such as “expect”, “anticipate”, “project” “target”, “intend,” “plan,” “aim,” “believe,” “seek,”
“estimate,” “can,” “could,” “focus,” “will,” „look forward,” “continue,” “goal,” “strategy,” “may” and similar expressions to identify such forward-
looking statements. These forward-looking statements are about Achillion Pharmaceuticals, Inc. and its business and prospects, including,
without limitation, statements regarding drug discovery, research, clinical development, timing of anticipated clinical trials and clinical data
for our product candidates, our expectations regarding the potential safety, efficacy and clinical utility for our product candidates, regulatory
approval processes, market opportunities, strategic goals, our previous collaboration with Janssen in HCV, intellectual property, competition,
and financial results. To the extent that statements contained in this presentation are not descriptions of historical facts, they are forward-
looking statements reflecting management‟s current beliefs and expectations.
Various important factors may cause differences between our forward-looking statements and actual results, including without limitation,
unexpected or unfavorable safety or efficacy data, lower than expected enrollment rates in clinical trials, changes in the competitive
landscape for our product candidates, changes in the regulatory environment, changes in market conditions or future demand for our drug
candidates, the inability to protect our intellectual property, our freedom to operate under third party intellectual property, our need for future
capital, the risk of litigation or other disputes, and general market and economic conditions. These and other risks and uncertainties are
described in the reports filed by Achillion with the U.S. Securities and Exchange Commission (“SEC”), including its annual report on Form
10-K and quarterly reports on Form 10-Q, and subsequent filings with the SEC from time to time. You should read these reports, including
the Risk Factors contained in these reports with the understanding that our actual future results may be materially different from what we
expect.
All forward-looking statements contained in this presentation speak only as of the date hereof, and Achillion undertakes no obligation to
update any of these statements, except as required by law.
September 2017 Corporate Overview 2
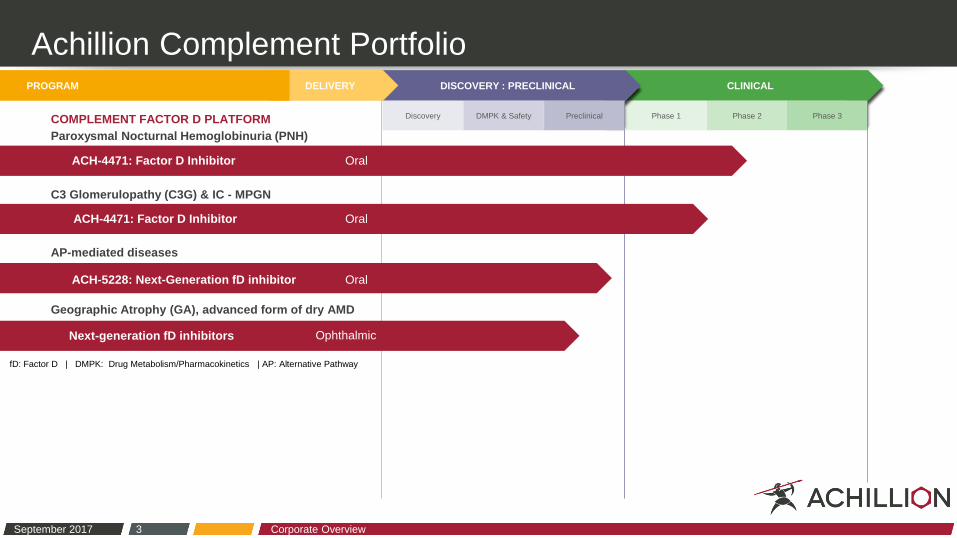
Achillion Complement Portfolio
September 2017 Corporate Overview 3
fD: Factor D | DMPK: Drug Metabolism/Pharmacokinetics | AP: Alternative Pathway
CLINICAL
Phase 1
DISCOVERY : PRECLINICAL
Discovery DMPK & Safety Preclinical Phase 2 Phase 3
DELIVERY PROGRAM
ACH-4471: Factor D Inhibitor Oral
ACH-5228: Next-Generation fD inhibitor Oral
Next-generation fD inhibitors Ophthalmic
ACH-4471: Factor D Inhibitor Oral
Paroxysmal Nocturnal Hemoglobinuria (PNH)
C3 Glomerulopathy (C3G) & IC - MPGN
Geographic Atrophy (GA), advanced form of dry AMD
AP-mediated diseases
COMPLEMENT FACTOR D PLATFORM

Mechanism Matters: Factor D Inhibition
September 2017 Corporate Overview 4
Source: Data on file. Achillion Pharmaceuticals, Inc. www.achillion.com
Factor D
A critical control point
specifically within the AP
Trigger Point Inhibitor
Prevents amplification and
modulates downstream
complement cascade

FACTOR D INHIBITOR PORTFOLIO
ACH-4471: First-in-class Complement Inhibitor
GOALS FOR INITIAL CLINICAL DEVELOPMENT
Demonstrate proof-of-mechanism with a highly innovative approach
o Lack of C3 fragment deposition on PNH red blood cells
o Reduction in plasma Bb levels
Demonstrate proof-of-concept by showing clinical efficacy
o Reduction in LDH
o Increase in hemoglobin
o Improvement in fatigue score (FACIT score)
o Increase in PNH RBC clone size
Elucidate PK/PD
o Understand plasma concentrations of ACH-4471 necessary for potential efficacy
Acceptable safety and tolerability profile
Early
development
program serves
as a gateway to
unlock broader
potential of
ACH-4471
September 2017 Corporate Overview 5

FACTOR D INHIBITOR PORTFOLIO
Unlocking the Broader Potential of ACH-4471
PLANS FOR EXPANDING CLINICAL PROGRAM
PNH
o Phase 2: Expand on-going monotherapy trial in untreated patients
o Phase 2: Add-on trial to support “switch-strategy” for patients with
suboptimal response to eculizumab
C3G & IC-MPGN
o Phase 2: 14-day dosing
o Phase 2: 6-month dosing with long-term dosing extension
o Natural history study: Ongoing study sponsored by Imperial College of
London anticipated to enroll up to 400 patients globally
September 2017 Corporate Overview 6
Pioneer
“best-in-disease”
factor D inhibition
across multiple
indications

ACH-4471 Phase 2 PNH Three-month / Long-term Extension Trials
Interim Results and Next Steps

PAROXYSMAL NOCTURNAL HEMOGLOBINURIA (PNH)
Factor D and Protection from Intra- / Extra-vascular Hemolysis
September 2017 Corporate Overview 8
Type III
PNH erythrocytes
Factor D
inhibitor
Intravascular hemolysis
No treatment
Breakthrough and
Extravascular hemolysis C3 fragment opsonization via
RES macrophages (liver, spleen)
C3
fragment
deposition
Anti-C5
therapy
Protected PNH
erythrocytes
Adapted from Luzzatto L, Risitano AM, Notaro R. Haematologica 2010;95(4):523–526.
Harder M., et al. Blood. 2017; 129(8)970-80.
PNH RBCs
treated with a fD
inhibitor may be
protected from
both intra- and
extravascular
hemolysis

Part 1
Day
1
Study Status and Interim Results
Phase 2 Trial of ACH-4471 in Untreated PNH Patients
Long-term Extension
Part 2
Three-month Dose Finding
PATIENT C Classic PNH
Total days on therapy: 44
Days on 200mg TID: 14
PATIENT B Aplastic Anemia / PNH
Total days on therapy: 126
Days on 200mg TID: 33
Extension Study
Day
28
Investigator
determines clinical
response to guide
entry into Part 2
Investigator
assessment of
benefit determines
entry into extension
trial
Long-Term
Day
84
PATIENT D Classic PNH
Total days on therapy: 9
Days on 200mg TID: --
PATIENT A Classic PNH
Total days on therapy: 132
Days on 200mg TID: 40
September 2017 Corporate Overview 9
Initial dose 100 mg TID. Protocol subsequently amended to allow:
- Newly enrolled patients to start at 150 mg TID
- Intra-patient dose escalation throughout both studies
Interim data reported by Achillion August 8, 2017
KEY INCLUSION /
EXCLUSION CRITERIA
• PNH clone size > 10%
• Anemia (Hgb < 12 g/dL)
• LDH > 1.5X ULN
• ANC > 1,000/ mm3
• Platelets > 50,000 μ/L
• Normal ALT
• Alk Phos ≤ 1.5X ULN
Enrollment: 4 to 12 pts
Objectives
• Change in LDH from baseline
• Improvements in Hgb, FACIT
• Increase PNH RBC clone size
Hgb: hemoglobin | LDH: lactose dehydrogenase|
ANC : absolute neutrophil count | ALT: alanine
aminotransferase | TID: three times daily

Male patient; diagnosed with PNH in 2011 after presentation with dermal thrombosis and
hemolytic anemia - Otherwise healthy with active lifestyle; no transfusion requirements at baseline
Phase 2 Trial of ACH-4471 in Untreated PNH Patients
Patient A: Classic PNH
September 2017 Corporate Overview 10
HgB (g/dL) LDH (U/L) FACIT
PNH clone size
(%)
C3 fragment
deposition
Current Value 14.1 272 49 43 Negative
Baseline 11.7 1848 32 11 Negative
Baseline
Days on therapy
100mg
TID*
13 days
150mg
TID*
62 days
175mg
TID*
17 days
200mg
TID**
40 days (last labs @ day 20)
LD
H (
U/m
L) H
gB
(g/d
L)
272
14.1
Status:
• Patient remains on
200 mg TID
11.7
* Median values for LDH and HgB shown.
** Individual data points shown through day 20 for 200 mg TID group.
2x ULN
1.5x ULN
6
8
10
12
14
16
0
500
1000
1500
2000 1848
Hgb: hemoglobin | LDH: lactose dehydrogenase | TID: three times daily
Interim data reported by Achillion
August 8, 2017
Baseline
Days on
therapy
150mg
TID*
13 days
175mg
TID**
14 days
200mg
TID**
14 days†
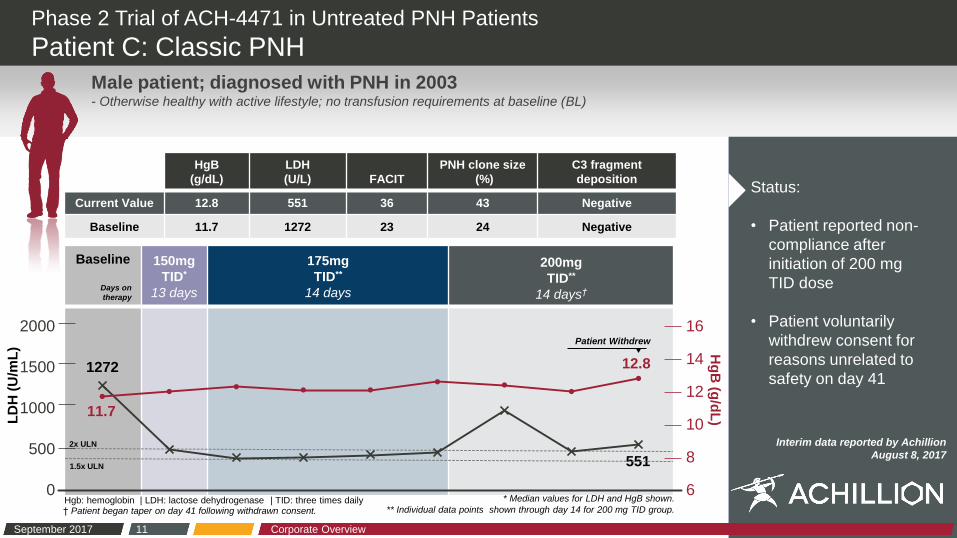
Phase 2 Trial of ACH-4471 in Untreated PNH Patients
Patient C: Classic PNH
September 2017 Corporate Overview 11
HgB
(g/dL)
LDH
(U/L) FACIT
PNH clone size
(%)
C3 fragment
deposition
Current Value 12.8 551 36 43 Negative
Baseline 11.7 1272 23 24 Negative
Hg
B (g
/dL
)
Male patient; diagnosed with PNH in 2003 - Otherwise healthy with active lifestyle; no transfusion requirements at baseline (BL)
1272
11.7
12.8
551
Status:
• Patient reported non-
compliance after
initiation of 200 mg
TID dose
• Patient voluntarily
withdrew consent for
reasons unrelated to
safety on day 41
† Patient began taper on day 41 following withdrawn consent.
6
8
10
12
14
16
0
500
1000
1500
2000 Patient Withdrew
Hgb: hemoglobin | LDH: lactose dehydrogenase | TID: three times daily
LD
H (
U/m
L)
2x ULN
1.5x ULN
* Median values for LDH and HgB shown.
** Individual data points shown through day 14 for 200 mg TID group.
Interim data reported by Achillion
August 8, 2017

Phase 2 Trial of ACH-4471 in Untreated PNH Patients
Patient D: Classic PNH
September 2017 Corporate Overview 12
HgB
(g/dL)
LDH
(U/L) FACIT
PNH clone size
(%)
C3 fragment
deposition
Current Value 12.4 504 n/a n/a n/a
Baseline 12.0 899 n/a 36 Negative
Baseline
Days on therapy
150mg
TID*
9 days
175mg
TID
--
200mg
TID
--
Hg
B (g
/dL
)
Status:
• Patient recently
enrolled
• Currently receiving
150 mg TID dose and
will be evaluated for
intra-patient dose
escalation
Male patient; diagnosed in 2012 with PNH - No history of transfusion-dependence
504
899
12.0 12.4
* Individual data points shown through day 6 for 150 mg TID group. 6
8
10
12
14
16
0
500
1000
1500
2000
Hgb: hemoglobin | LDH: lactose dehydrogenase | TID: three times daily
LD
H (
U/m
L)
2x ULN
1.5x ULN
Interim data reported by Achillion
August 8, 2017

Understanding PNH Classifications
• Two most clinically overt
presentations of PNH are:
− Classic PNH: > hemolysis
without bone marrow
failure
− AA: Overlap of both PNH
and bone marrow failure
− Both are associated with
elevated risk of
thrombosis, chronic
kidney disease, and
fatigue
− Estimated 25% PNH
patients have overlap
Classic PNH vs. PNH + Aplastic Anemia (AA)
Classic PNH AA w/
subclinical PNH
Degree of Hemolysis
Significant Moderate - Minimal Minimal to None
Segment PNH/AA
Overlap Syndrome
Bone Marrow
(BM) Status Near-Normal Evidence of BM Failure Evidence of BM Failure
September 2017 Corporate Overview 13
Source: Data on file. Achillion Pharmaceuticals, Inc. www.achillion.com

Phase 2 Trial of ACH-4471 in Untreated PNH Patients
Patient B: Aplastic Anemia PNH
September 2017 Corporate Overview
HgB
(g/dL)
LDH
(U/L) FACIT
PNH clone size
(%)
C3 fragment
deposition
Current Value 9.0 461 31 36 Negative
Baseline 7.5 941 22 20 Negative
Baseline
Days on therapy
100mg
TID*
13 days
150mg
TID*
58 days
175mg
TID*
22 days
200mg
TID**
33 days (last labs @ day 18)
Hg
B (g
/dL
)
Status:
• Patient remains on
200 mg TID
• Patient continued to
receive RBC
transfusions during
therapy
Male patient diagnosed with AA in 2008; subsequently diagnosed with PNH in 2016 - Treated with ATG, oral prednisone and cyclosporine; ending in 2012
- Baseline marrow function: platelets range 30-60K, ANC 0.7-1.5 and requires Q3-4 weekly RBC transfusions to maintain Hgb ≥ 8 g/dL
941
7.5 461
9.0
14
* Median values for LDH and HgB shown.
** Individual data points shown through day 18 for 200 mg TID group.
6
8
10
12
14
16
0
500
1000
1500
2000
AA: Aplastic Anemia | Hgb: hemoglobin | LDH: lactose dehydrogenase
ANC: absolute neutrophil count | TID: three times daily
LD
H (
U/m
L)
2x ULN
1.5x ULN
Interim data reported by Achillion
August 8, 2017

Measures of Clinical Efficacy & Safety in PNH
September 2017 Corporate Overview 15
Clinical data
generated to date
highlight the
potential role of
factor D inhibition
in PNH
Lactose dehydrogenase
(LDH) GOAL Clinically meaningful reduction in LDH
Hemoglobin
(Hgb) GOAL Stabilize / increase hemoglobin
C3 fragment deposition GOAL Observe no C3 fragment deposition on PNH RBCs
Fatigue
(FACIT scale)
GOAL Improvement over time in objective measures of
patient fatigue
PNH RBC Clone Size GOAL Increase percentage of PNH RBC clones from
baseline
Safety GOAL Good tolerability profile

C3 GLOMERULOPATHY (C3G)
A Rare Disease with No Available Treatment
C3G includes both Dense Deposit Disease (DDD) and C3
glomerulonephritis (C3GN)
Estimated prevalence of 8–12 people affected per million
in major markets
o Incidence rate of 1–2 per million patients diagnosed with C3G
on an annual basis
There are no approved treatments for patients with C3G
o Non-specific treatment approaches include blood pressure
control and broad immunosuppression
Significant unmet medical need as nearly half of C3G
patients progress to end-stage renal disease
o 30-50% progress to ESRD within 10 years
o ~70% of patients experience disease recurrence post renal
transplant, with a 50% chance of graft loss
September 2017 Corporate Overview 16
DDD AND C3GN
IMPACT ON RENAL SURVIVAL
0
25
50
75
100
0 10 20 30 40
Years from Diagnosis C3GN (n=49) DDD (n=26)
Ren
al S
urv
iva
l (%
)
Sources: Servais et al (2013); Medjeral-Thomas et al (2014); Data on File. Achillion Pharmaceuticals. 2016.
Barbour et al. (2015); NICE C3G Evidence Summary (2015);

C3 GLOMERULOPATHY (C3G)
Patient-Focused Drug Development (PFDD) Meeting
Achillion was lead sponsor of externally-led PFDD meeting
focused on C3G
o First renal disease discussed at a PFDD meeting on August 4, 2017
Led by the National Kidney Foundation
Goal is to understand the patient perspective of their disease
o PFDD meeting provides an important opportunity to us and to the
FDA to hear directly from patients / caregivers
o Understand the impact of the disease on patients’ daily lives
o Input may inform FDA’s decisions throughout the drug development
process
Patient experiences shared at the meeting highlight the unmet
need and the urgency to develop transformative therapies
September 2017 Corporate Overview 17

Extended-Release Activities for ACH-4471
ONGOING EXTENDED-RELEASE (XR) FORMULATION
Objective Develop an extended release tablet
formulation to allow for:
o Optimized trough exposures
o Reduced dosing frequency
ACH-4471 has high permeability with animal
and modeling data reporting good absorption
throughout the GI tract
Human bioavailability study for extended
release tablet is planned for 4Q 2017
September 2017 Corporate Overview 18
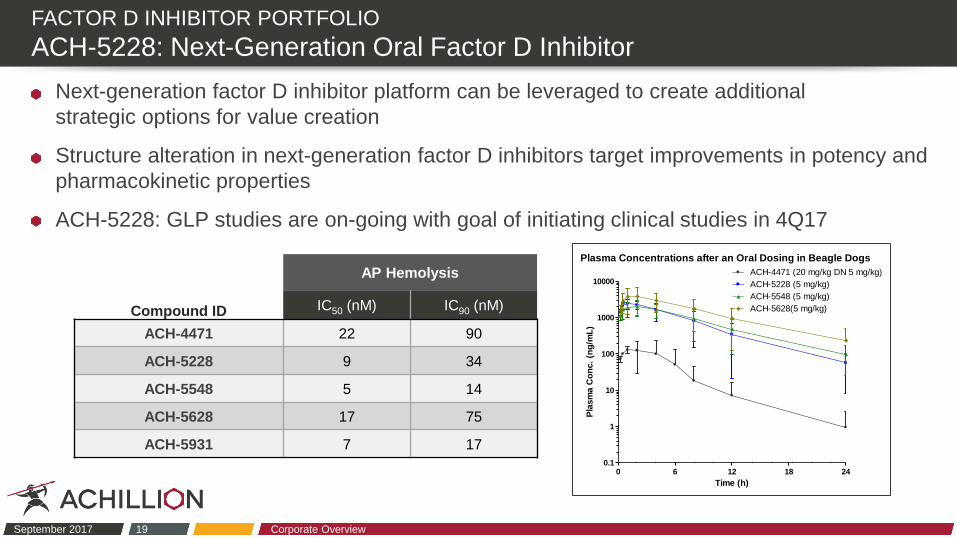
FACTOR D INHIBITOR PORTFOLIO
ACH-5228: Next-Generation Oral Factor D Inhibitor
Next-generation factor D inhibitor platform can be leveraged to create additional
strategic options for value creation
Structure alteration in next-generation factor D inhibitors target improvements in potency and
pharmacokinetic properties
ACH-5228: GLP studies are on-going with goal of initiating clinical studies in 4Q17
September 2017 Corporate Overview 19
Compound ID
AP Hemolysis
IC50 (nM) IC90 (nM)
ACH-4471 22 90
ACH-5228 9 34
ACH-5548 5 14
ACH-5628 17 75
ACH-5931 7 17
Plasma Concentrations after an Oral Dosing in Beagle Dogs
0 6 12 18 240.1
1
10
100
1000
10000
ACH-5548 (5 mg/kg)
ACH-5628(5 mg/kg)
ACH-4471 (20 mg/kg DN 5 mg/kg)
ACH-5228 (5 mg/kg)
Time (h)
Pla
sm
a C
on
c.
(ng
/mL
)
GEOGRAPHIC ATROPHY (GA) AND DRY AMD
Factor D Inhibitors in Ophthalmological Disease
Geographic Atrophy (GA) is an advanced form of dry
Age-related Macular Degeneration (dry AMD)
GA is a leading cause of impaired vision and blindness
that affects more than 2.6 million people in US & EU and
more than 5 million world-wide
Achillion is targeting treatment durations of 3 months or
longer with diverse small molecule factor D inhibitors
o Four diverse compounds and distinct delivery approaches
are advancing
o Goal of initiating IND enabling studies in 2018 for
complement-mediated ophthalmic diseases
September 2017 Corporate Overview 20
Sources: www.clinicaltrials.gov , Roche

Strength to Achieve our Goals
$369.9 million
in cash, cash
equivalents, and
interest receivable at
6/30/17 to support
clinical expansion
and factor D platform
September 2017 Corporate Overview 21
Near-term Development Plan
Compound Indication Next steps
ACH-4471 PNH Phase 2: Expand on-going
monotherapy
Phase 2: Add-on trial to support
“switch strategy” for
suboptimal responders
C3G & IC-MPGN Phase 2: 14-day dosing
Phase 2: Long-term
(6-month dosing)
Extended Release Tablet Phase 1 Bioavailability
ACH-5228 AP-mediated diseases (acute/chronic)
Phase 1 SAD/MAD
Ophthalmology Geographic Atrophy Complete Preclinical Assessment

Financial Summary: Capitalization and Ownership
September 2017 Corporate Overview 22
Balance Sheet Metrics As of 6/30/2017
Cash, cash equivalents, marketable securities
and interest receivable $369.9 million
Debt obligations $0.5 million
Shares outstanding 136.8 million
Top Shareholders† Position
Johnson & Johnson Development Corp. 18.4 million (13%)
RA Capital 13.6 million (10%)
Orbimed Advisors 13.1 million (10%)
Blackrock, Inc. 9.9 million (7%)
Vanguard Group 9.6 million (7%)
Janus Capital Management 4.5 million (3%)
State Street Global Advisors 4.0 million (3%)
Goldman Sachs & Co. 3.6 million (3%)
Biotechnology Value Fund (BVF) 3.5 million (2%)
Numeric Investors 3.0 million (2%)
† Based upon most recent SEC filings.

Corporate Overview
September 2017
NASDAQ:ACHN ©2017 Achillion Pharmaceuticals. All rights reserved.
Complement System
The Body’s Innate Defense
Complement activation and regulation are induced by more than 30 proteins that are present in plasma
(fluid phase) and on cell surfaces (solid phase)
The complement system is composed of three distinct pathways – Classical (CP), Lectin (LP) and
Alternative (AP) – which lead to a common terminal pathway
Activation of these pathways leads to:
o Recognition and elimination of pathogens
o Recruitment of adaptive immunity
o Facilitation of removal of apoptotic cells
Dysregulation of the complement alternative pathway can induce inflammation and tissue damage and is
associated with a variety of diseases
Dysregulation of the AP is the underlying cause of disease including
PNH, C3G and GA/dry AMD
September 2017 Corporate Overview 24

ACHILLION FACTOR D INHIBITORS
Advancing Novel Small Molecule Compounds
Achillion’s complement
factor D inhibitor
platform has
generated:
• ACH-4471: first potent,
specific, oral inhibitor of
fD advanced into Phase 2
• ACH-5228: Next-gen
factor D inhibitor
advancing toward clinical
development YE17
• Multiple molecules being
progressed for extended
(3+ months) ophthalmic
delivery
September 2017 Corporate Overview 25
ACH-4471:Factor D Complex
0.8 A X-ray Structure
~2,000 small molecule
factor D inhibitors
Primary
pharmacology
Secondary
pharmacology
ADME/Safety
Lead
programs
Source: Data on file. Achillion Pharmaceuticals, Inc. www.achillion.com

PAROXYSMAL NOCTURNAL HEMOGLOBINURIA (PNH)
Unmet Patient Needs
Somatic mutation results in red blood cells (RBCs) deficient in CD55 and CD59
Prevalence of approximately 4,000 U.S and 4,000 EU patients with an incidence of 3-10
cases/million/year 1
Current treatment is effective but a significant portion of PNH patients achieve sub-optimal
response 2,3,4
Even on currently available treatment, PNH patients continue to have unmet needs:
o Up to a third of patients have less than normal
hemoglobin levels
o Nearly 1 in 6 patients remain dependent on
blood transfusions
o Up to 20% of patients require increased doses
of mAb C5 inhibitor
o All patients require frequent treatment administration
by intravenous infusion
September 2017 Corporate Overview 26
Source: 1. Soliris ® Package Insert, 2013. 2. Schubert et al. Triumph, 2008, Br J Hemta. 3. Hiillmen et al, Long term follow-up, 2013, Br J Hema.
4. Brodsky et al, Shepard, 2008, Blood. Data on file. Achillion Pharmaceuticals, Inc. www.achillion.com

ACH-4471
Benchmarking to Eculizumab in PNH Hemolysis Assay
Enhance the understanding of PK/PD relationships
in PNH
Projections for efficacious dosing are based on:
o Benchmarking of ACH-4471 with eculizumab for
lysis of PNH red blood cells
o PK/PD profile of ACH-4471 from the Phase I
program
Ability to maintain exposures above necessary
trough concentrations
o ACH-4471 well absorbed throughout GI tract
o Extended release formulation in development
September 2017 Corporate Overview 27
Source: Data on file. Achillion Pharmaceuticals, Inc. www.achillion.com
ACH-4471 was benchmarked using eculizumab for
inhibition of hemolysis using PNH red blood cells


















