Core Message for Referring Physicians - Results...
2
Background: FDG-PET/CT has become an integral component of non-small cell lung carcinoma staging because it improves the detection of nodal and distant metastases and frequently alters patient man- agement (1). PET is more sensitive than CT for staging of many malignancies, including non- small cell lung carcinoma, as well as for differ- entiating lung malignancy from benign lung find- ings, such as post-obstructive atelectasis (2). The use of radiation therapy for curative treatment of lung cancer is limited by the radiosensitivity of surrounding normal structures, by difficulty in delineating the extent of malignancy using con- ventional imaging techniques and by the identifi- cation of distant metastatic disease (3). 3-DCRT and IMRT have improved the accuracy of radiation delivery leading to improved loco- regional control with reduced morbidity by facili- tating delivery of higher radiation dose to tumor while increasing normal tissue sparing (2,4). Value of PET/CT Radiation Therapy Treatment Planning in Lung Cancer Core Message for Referring Physicians Case Example 1: Case Example 1. a. CT image showing primary lung cancer in the left upper lobe. The red line defines the GTV and the yellow line defines the CTV. b. PET reveals pathological FDG uptake (purple and green area) in the left upper lobe at the same level as the CT image in a. c. The fusion image documents that FDG uptake is also present in the subcarinal region, indicating metastatic lymph node extension not visible on CT. The red line defines the GTV and the yellow line defines the CTV. In this image a part of the treatment field of radiotherapy planning is seen (yellow wedges). D. 3D conformal treatment planning was performed, choosing the volume based on FDG uptake, which encompassed lymph node disease. This figure clearly reveals the increase in GTV (red volume) and the consequent increase in CTV (yellow volume) due to inclu- sion of lymph nodes in the subcarinal region. (5) Case Example 1:
Transcript of Core Message for Referring Physicians - Results...

Background: FDG-PET/CT has become an integral component of non-small cell lung carcinoma staging because it improves the detection of nodal and distant metastases and frequently alters patient man-agement (1). PET is more sensitive than CT for staging of many malignancies, including non-small cell lung carcinoma, as well as for differ-entiating lung malignancy from benign lung find-ings, such as post-obstructive atelectasis (2).
The use of radiation therapy for curative treatment of lung cancer is limited by the radiosensitivity of surrounding normal structures, by difficulty in delineating the extent of malignancy using con-ventional imaging techniques and by the identifi-cation of distant metastatic disease (3).
3-DCRT and IMRT have improved the accuracy of radiation delivery leading to improved loco-regional control with reduced morbidity by facili-tating delivery of higher radiation dose to tumor while increasing normal tissue sparing (2,4).
Value of PET/CTRadiation Therapy Treatment Planning in Lung Cancer
Core Message for Referring Physicians
Case Example 1:
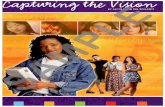
Case Example 1. a. CT image showing primary lung cancer in the left upper lobe. The red line defines the GTV and the yellow line defines the CTV. b. PET reveals pathological FDG uptake (purple and green area) in the left upper lobe at the same level as the CT image in a. c. The fusion image documents that FDG uptake is also present in the subcarinal region, indicating metastatic lymph node extension not visible on CT. The red line defines the GTV and the yellow line defines the CTV. In this image a part of the treatment field of radiotherapy planning is seen (yellow wedges). D. 3D conformal treatment planning was performed, choosing the volume based on FDG uptake, which encompassed lymph node disease. This figure clearly reveals the increase in GTV (red volume) and the consequent increase in CTV (yellow volume) due to inclu-sion of lymph nodes in the subcarinal region. (5)
Case Example 1:

Functional imaging is increasingly being utilized for treatment planning for patients with can-cer at several anatomic sites (6). PET/CT simulation for radiation therapy treatment planning requires that the patient be aligned using the same setup that will be utilized during radiation therapy. 4D CT respiratory gating can also be utilized (7).
Ashamalla, et al, determined that PET/CT planning is a valuable tool for refining traditional treatment volumes (8). Macapinlac concluded that the incorporation of FDG PET images into radiation therapy treatment planning resulted in a 15% - 60% increase or decrease in treated volumes (1). Bradley et al reported that in 30-60% of patients treated with definitive radio-therapy, PET simulation enhanced precision in coverage of the GTV (6).
Overall, there has been limited evaluation of incorporation of FDG PET/CT images into radiation therapy treatment plans. Thresholding needs to be further studied, as do new technologies such as PET gating and average CT techniques. Ultimately, improvement in outcomes will determine the widespread use of FDG PET/CT in radiation therapy treatment planning.
References1. Macapinlac H. Clinical application sof positron emission tomography/computed tomography treatment planning. Semin Nucl Med 2008;38:137-140.
2. MacManus M, Nestle U, Rosenzweig KE, et al. Use of PET and PET/CT for radiation therapy planning: IAEA expert report 2006-2007. Radiother Oncol 2008;91(1):85-94.
3. Erdi YE, Rosenzweig K, Erdi AK, et al. Radiotherapy treatment planning for patients with non-small cell lung cancer using positron emission tomography (PET). Radiother Oncol 2002;62:51-60.
4. Gregoire V, Haustermans K, Geets X, et al. PET-based treatment planning in radiotherapy: a new standard? J Nucl Med 2007;48:68S-77S.
5. Brianzoli E, Rossi G, Ancidei S, et al. Radiotherapy planning: PET/CT scanner performances in the definition of gross tumour volume and clinical target volume. Eur J Nucl Med Mol Imaging 2005;32:1392-1399.
6. Bradley J, Thorstad WL, Mutic S, et al. Impact of FDG-PET on radiation therapy volume delineation in non-small-cell lung cancer. Int J Radiation Oncology Biol Phys 2004;59(1):78-86.
7. Brunetti J, Caggiano A, Rosenbluth B, et al. Technical aspects of positron emission tomography/computed tomography fusion planning. Sem Nucl Med 2008;38:129-136.
8. Ashamalla H, Rafla S, Parikh K, et al. The contribution of integrated PET/CT to the evolving definition of treatment volumes in radiation treatment planning in lung cancer. Int J Radiation Oncology Biol Phys 2005;63(4):1016-1023.
Case Example 2. This patient presented with right upper lobe atelectasis. The FDG-PET im-ages helped to (1) differentiate the primary tumor (red arrow) from atelectasis (yellow ar-row) within the right upper lobe and (2) delin-eate abnormal-sized upper paratracheal node on CT, but showing avid FDG uptake on the PET scan (white arrow). (6)
Case Example 2: