
Copyright restrictions may apply Impact of Cleft Width in Clefts of Secondary Palate on the Risk of...
12
Copyright restrictions may apply Impact of Cleft Width in Clefts of Secondary Palate on the Risk of Velopharyngeal Insufficiency Lam DJ, Chiu LL, Sie KCY, Perkins JA. Impact of cleft width in clefts of secondary palate on the risk of velopharyngeal insufficiency. Arch Facial Plast Surg. Published online April 16, 2012. doi:10.1001/archfacial.2012.169.
-
Upload
deborah-lee -
Category
Documents
-
view
217 -
download
0
Transcript of Copyright restrictions may apply Impact of Cleft Width in Clefts of Secondary Palate on the Risk of...

Copyright restrictions may apply
Impact of Cleft Width in Clefts of Secondary Palate on the
Risk of Velopharyngeal Insufficiency
Lam DJ, Chiu LL, Sie KCY, Perkins JA. Impact of cleft width in clefts of secondary palate on the risk of velopharyngeal insufficiency. Arch Facial Plast Surg. Published online April 16, 2012. doi:10.1001/archfacial.2012.169.

Copyright restrictions may apply
Introduction
• The goals of palatoplasty are to restore structural competence of the hard and soft palates to allow closure of the velopharyngeal port during speech and swallowing.
• Velopharyngeal insufficiency (VPI), characterized by hypernasal resonance and nasal air escape during speech, is a common sequela after cleft palate repair.
• The impact of cleft width on VPI resulting after cleft palate repair has not been previously reported.

Copyright restrictions may apply
Purpose
• The purpose of this study was to assess the impact of cleft width on the development of VPI after cleft palate repair in clefts of the secondary palate.

Copyright restrictions may apply
Relevance to Clinical Practice
• VPI is a common sequela in patients with repaired cleft palates, but most studies investigating the risk factors for VPI have focused on demographic factors, surgical technique, or the type of palatal cleft.
• There can be wide variation of cleft width and severity, even among isolated clefts of the secondary palate.
• Elucidating the association between cleft width and development of VPI can help the clinician to prognosticate the risk of VPI after palate repair and tailor surgical and follow-up planning accordingly.

Copyright restrictions may apply
Methods
• This was a retrospective cohort study of consecutive patients with isolated clefts of the secondary palate (Veau type 2) who underwent palatoplasty between 2003 and 2009.
• Patients with other Veau types were excluded.
• All patients underwent either a Furlow double-opposing Z-plasty or a combined Furlow palatoplasty and V to Y pushback depending on the severity of clefting.
• Measurements of cleft width and length were taken at the time of primary palatoplasty.
• Patients were followed up postoperatively by a speech language pathologist for development of VPI for a minimum of 1 year.
• Logistic regression analysis was used to assess the unadjusted and adjusted associations between cleft width and diagnosis with VPI.

Copyright restrictions may apply
Patient Characteristics
• Insert table or figure here
Characteristic Total (N = 73)
Cleft Width <10 mm(n = 45)
Cleft Width >10 mm(n = 28)
P Value
Cleft Size, mean (SD), mm Width Length
8.2 (3.2)28.5 (10.6)
--23.7 (5.3)
--34.8 (12.4) <.001
Age at surgery, mean (SD), mo 12.5 (2.9) 12.0 (3.3) 13.3 (1.9) .07
Male, No. (%) 24 (33) 14 (31) 10 (36) .80
Type of repair, No. (%) Furlow Furlow plus V-Y pushback
31 (42)42 (58)
28 (62)17 (38)
3 (11)25 (89) <.001
Syndrome presence, No. (%) Yes No
10 (14)60 (86)
6 (14)36 (86)
4 (14)24 (86) >.99
Fistula presence, No. (%) Yes No
2 (3)65 (97)
--40 (100)
2 (7)25 (93) .16
VPI presence, No. (%) Yes No
23 (32)50 (68)
8 (18)37 (82)
15 (54)13 (46) .002
Copyright restrictions may apply
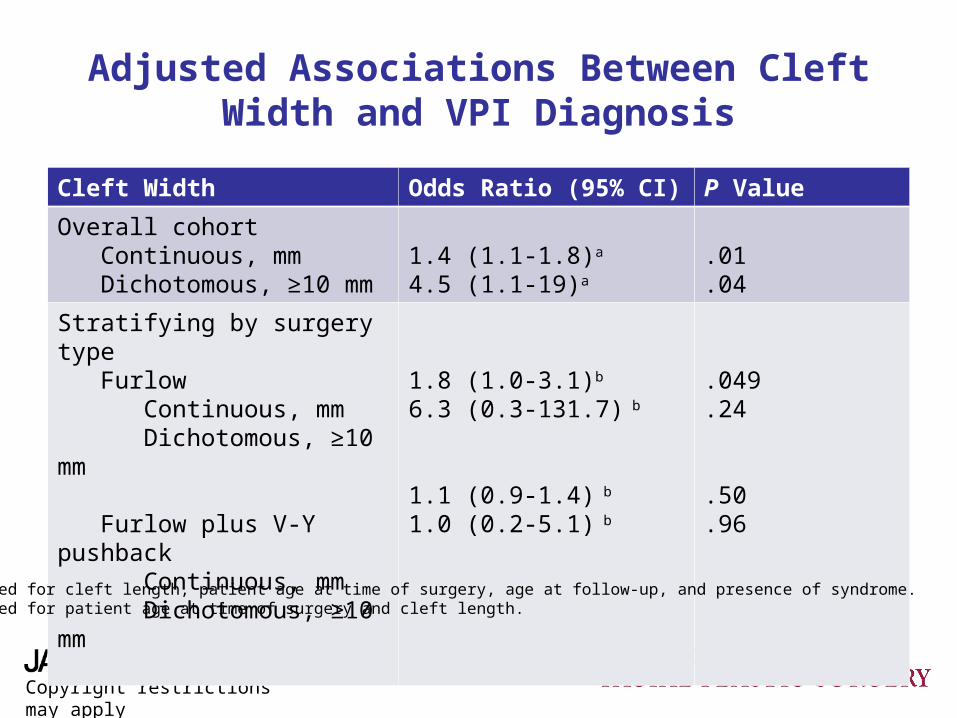
Adjusted Associations Between Cleft Width and VPI Diagnosis
Cleft Width Odds Ratio (95% CI) P Value
Overall cohort Continuous, mm Dichotomous, ≥10 mm
1.4 (1.1-1.8)a
4.5 (1.1-19)a
.01
.04
Stratifying by surgery type Furlow Continuous, mm Dichotomous, ≥10 mm
Furlow plus V-Y pushback Continuous, mm Dichotomous, ≥10 mm
1.8 (1.0-3.1)b
6.3 (0.3-131.7) b
1.1 (0.9-1.4) b
1.0 (0.2-5.1) b
.049
.24
.50
.96
a Adjusted for cleft length, patient age at time of surgery, age at follow-up, and presence of syndrome.b Adjusted for patient age at time of surgery and cleft length.
Copyright restrictions may apply
Controversies and Consensus
• Cleft lip and palate severities have traditionally been categorized based on Veau classification.
• Several studies have reported a nonlinear association between speech outcomes and Veau classification.
• Multiple studies have demonstrated that palatoplasty techniques such as the Furlow double-opposing Z-plasty that lengthen the palate and restore the palatal sling result in better speech outcomes.
• Although it is generally recognized that increased cleft severity has higher risk of poor outcomes, the impact of cleft width on speech outcomes has not been previously reported.

Copyright restrictions may apply
Comment
• Our results indicate that risk of VPI after isolated cleft palate repair increases by 40% with every millimeter increase in cleft width.
• 54% of patients with cleft width ≥10 mm were later diagnosed with VPI.
• Compared with patients with cleft width <10 mm, patients with cleft width ≥10 mm have 4.5 times the likelihood of developing VPI.
Copyright restrictions may apply
Comment
• This study is limited by the inclusion of only isolated clefts of the secondary palate (Veau type 2) and the use of only Furlow or Furlow plus V-Y pushback palatoplasty repairs.
• Future studies should include other types of clefts and other methods of repair to allow greater generalization.
Copyright restrictions may apply
Conclusions
• Our results suggest that cleft width should be considered as a prognostic indicator of postoperative VPI.
• In patients with very wide palatal clefts, careful consideration should be given to maximizing velopharyngeal closure at the time of primary palate repair.

Copyright restrictions may apply
Contact Information
• If you have questions, please contact the corresponding author:
–Derek J. Lam, MD, MPH, Department of Otolaryngology–Head and Neck Surgery, MLC 2018, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, Cincinnati, OH 45229-3039 ([email protected]).


















