
Copyright © 2005 by Elsevier Inc. All rights reserved. Principles and Techniques of Instrument...
80
Copyright © 2005 by Elsevier Inc. All rights reserved. Principles and Techniques of Instrument Processing and Sterilization Chapter 21
-
Upload
kristina-atkins -
Category
Documents
-
view
221 -
download
0
Transcript of Copyright © 2005 by Elsevier Inc. All rights reserved. Principles and Techniques of Instrument...
Copyright © 2005 by Elsevier Inc. All rights reserved.
Principles and Techniques of Instrument Processing
and Sterilization
Chapter 21

Copyright © 2005 by Elsevier Inc. All rights reserved.
Introduction
One of the most important responsibilities of the dental assistant is to process contaminated
instruments for reuse.
Instrument processing involves much more than sterilization.
Sterilization is a process intended to kill all microorganisms and is the highest
level of microbial destruction.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Instrument Processing
• Instrument processing involves much more than sterilization. Proper processing of contaminated dental instruments is actually a seven-step process.
• Although the seven steps are not difficult to learn, it is very important for you to have a clear understanding of how and why each step is performed.

Copyright © 2005 by Elsevier Inc. All rights reserved.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Classification of Patient-Care Items
• Patient-care items are categorized into three classifications:
– Critical
– Semicritical
– Noncritical
Copyright © 2005 by Elsevier Inc. All rights reserved.
Classification of Patient-Care Items-cont’d
• The categories are based on the potential risk for infection associated with their intended use.
• The classifications are used to determine the minimal type of posttreatment processing.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Critical Instruments
• Critical instruments are items used to penetrate soft tissue or bone.
• They have the greatest risk of transmitting infection and should be sterilized by heat.
• Examples of critical instruments include forceps, scalpels, bone chisels, scalers, and burs.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Semicritical Instruments
• Semicritical items instruments touch mucous membranes or nonintact skin and have a lower risk of transmission.
• The majority of semicritical items in dentistry are heat-tolerant and they should also be sterilized.
• If the item will be damaged by heat, it should receive, at a minimum, high-level disinfection.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Noncritical Instruments
• Noncritical instruments pose the least risk of transmission of infection because they contact only intact skin, which is an effective barrier to microorganisms.
• These items should be cleaned and processed with an EPA-registered intermediate-level or low-level disinfectant after each patient use.
• Noncritical clinical devices include the position indicator device (PID) of the x-ray unit tube head, the lead apron, or the curing light that comes into contact only with intact skin.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Personal Protective Equipment
• To prevent disease agents from a previous patient being transferred to yourself, another dental team member, or the next patient, instrument processing must be performed in a consistent and disciplined manner.
• You must always use personal protective equipment (PPE), including utility gloves, mask, eyewear, and protective clothing, when processing instruments.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-1 Personal protective equipment must be worn while preparing instruments for sterilization.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Transporting and Processing Contaminated Patient-Care Items
• The dental assistant can be exposed to microorganisms through contact with contaminated instruments or other patient-care items.
• Exposure can occur through percutaneous injury (e.g., needle sticks or cuts) or contact with the mucous membranes of the eyes, nose, or mouth.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Instrument Processing Area
• The instrument processing area, or sterilization area, should be centrally located in the office to allow for easy access from all patient care areas.
• This minimizes the need to carry contaminated items through clean areas of the office (where sterilized instruments, fresh disposable supplies, and prepared trays are stored).

Copyright © 2005 by Elsevier Inc. All rights reserved.
Instrument Processing Area-cont’d
• The “ideal” instrument processing area:
• Should be dedicated only to instrument processing.
• Should be physically separated from the operatories and dental laboratory.
• Should not be a part of a common walkway.
• The area should not have a door or windows that open to the outside, because dust can enter the area.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Instrument Processing Area-cont’d
• The processing area should have good air circulation to control the heat generated by the sterilizers.
• The size of the area should accommodate all the equipment and supplies necessary for instrument processing, with multiple outlets and proper lighting, water, and an air line and vacuum line for flushing high-speed handpieces.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Instrument Processing Area-cont’d
• A deep sink should have hands-free controls for instrument rinsing and (if space permits) a foot-operated or other hands-free trash receptacle.
• The flooring should be an uncarpeted, seamless, hard surface.
• The size, shape, and accessories of the instrument- processing area vary among dental offices.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Copyright © 2005 by Elsevier Inc. All rights reserved.
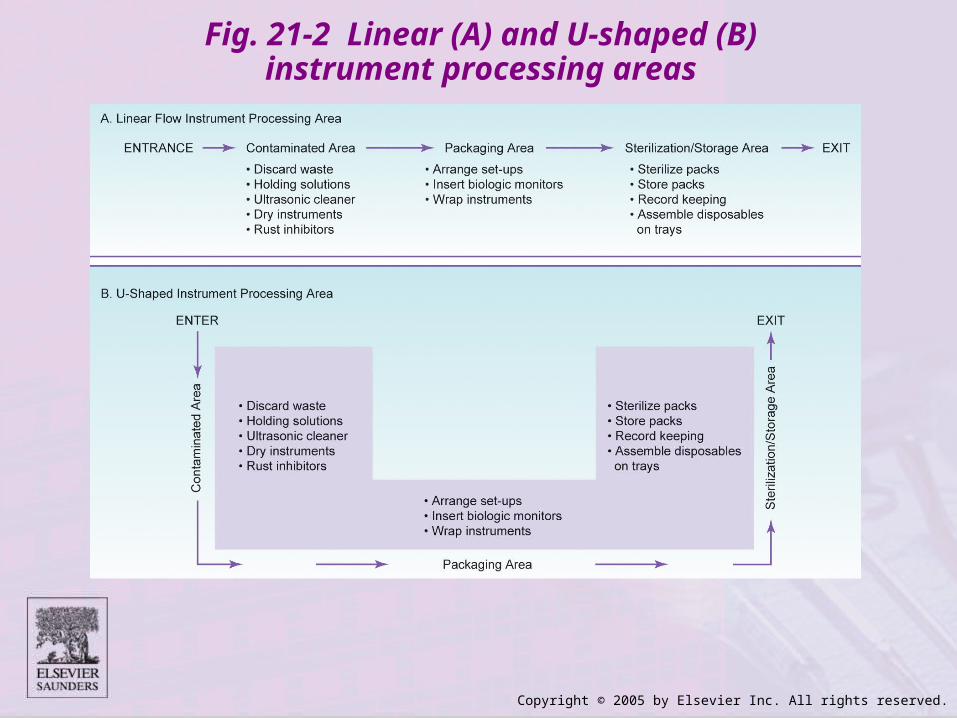
Workflow Pattern• Regardless of the size or shape of the instrument processing
area, four basic areas govern the pattern of workflow.
• Processing instruments should proceed in a single loop, from dirty, to clean, to sterile, to storage, without ever “doubling back.”
• If the instrument processing area is small, you can use signs that read:
– “Contaminated items only”
– “Precleaning area”
– “Cleaned items only”
– “Sterile items only”
– “Sterilization area”
Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-2 Linear (A) and U-shaped (B) instrument processing areas
Copyright © 2005 by Elsevier Inc. All rights reserved.
Contaminated Area
• All soiled instruments are brought into the contaminated area, the initial receiving area, where they are held for processing. Any disposable items not already discarded in the treatment room are removed from the instrument tray and disposed of as contaminated waste.
• Thorough cleaning should be done before all disinfection and sterilization processes. It should involve removal of all debris and organic materials (e.g., blood and saliva).
• The contaminated area contains clean protective eyewear and utility gloves, counter space, a sink, a waste disposal container, holding solution, ultrasonic cleaner, eyewash station, and supplies for wrapping instruments before sterilization.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-3 Waste items are properly discarded.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Preparation and Packaging Area
• In the preparation and packaging area, cleaned instruments and other dental supplies should be inspected, assembled into sets or trays, and wrapped or placed in packages for sterilization.
Copyright © 2005 by Elsevier Inc. All rights reserved.
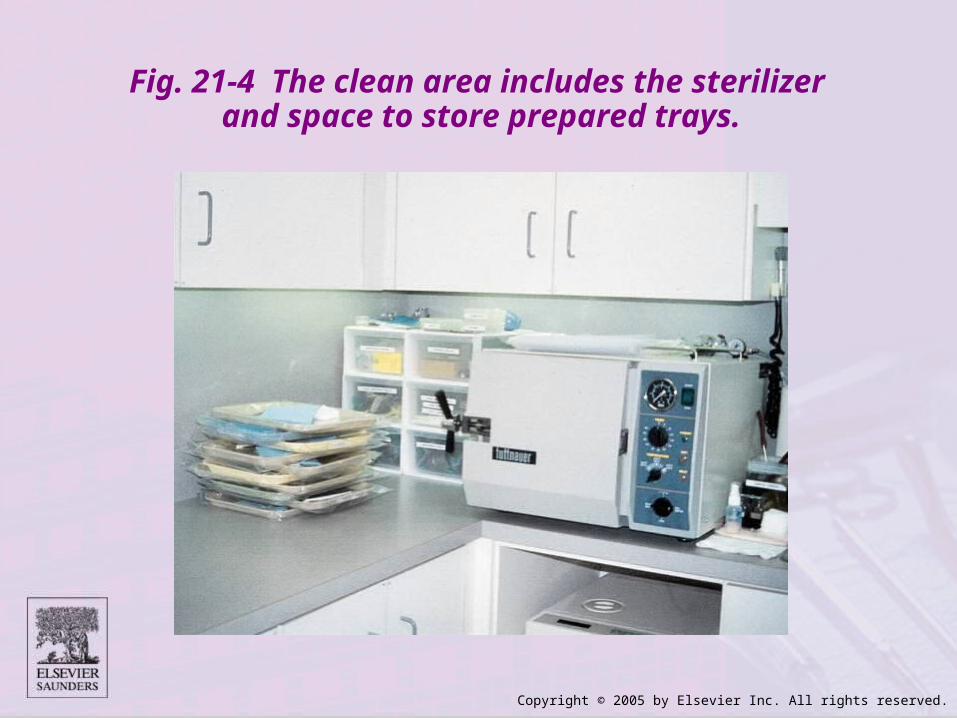
Fig. 21-4 The clean area includes the sterilizer and space to store prepared trays.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Holding Solution
• If the instruments cannot be cleaned immediately after the procedure, they should be placed in a holding solution to prevent the drying of blood and debris on the instruments.
• The holding solution may be any noncorrosive liquid. A commercial enzymatic solution that partially dissolves organic debris may be used.
• Dishwasher detergent also makes a good holding solution because it is low-cost, low-foaming, and readily available.
• It is neither cost-effective nor desirable to use a disinfectant alone as a holding solution.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Holding Solution-cont’d
• The container must have a lid and be labeled with both a biohazard label (because of the contaminated instruments) and a chemical label (because of the cleaner/detergent).
• The holding solution should be changed at least twice daily and more frequently if it becomes clouded.
• Remember, a holding solution is necessary only when contaminated instruments cannot be processed immediately.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-5 Commercial holding solutions are available for use in precleaning. (Courtesy Biotrol International.)

Copyright © 2005 by Elsevier Inc. All rights reserved.
Precleaning and Packaging Instruments
• Instruments may be precleaned in one of three ways:
– Hand scrubbing
– Ultrasonic cleaning
– Instrument washing machines.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Hand Scrubbing
• Hand scrubbing is the least desirable method of cleaning instruments because it requires direct hand contact with the contaminated instrument.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Hand Scrubbing Instruments
Wear goggle-type eyewear and puncture-resistant gloves, as well as your protective clothing. Clean only one or two instruments at a time.
Use only a long-handled brush, preferably one with a hand guard or wide surface.
• Keep items above the waterline; fully immersing them in a basin of soapy water interferes with the ability to see the sharp ends.
• Allow instruments to air-dry, or carefully pat them with thick toweling. Never rub or roll the instruments in the towel, because of the risk of accidental injury.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Ultrasonic Cleaning
• Ultrasonic cleaners are used to loosen and remove debris from instruments. These cleaners also reduce the risk of hand injuries from cuts and punctures during the cleaning process.
• Puncture-resistant utility gloves, a mask, protective eyewear, and a protective gown should always be worn when using the ultrasonic cleaner.
• To further limit contact with contaminated instruments, keep a set of tongs near the ultrasonic unit for removing instruments after the cleaning cycle.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-6 Ultrasonic cleaning system. A, Ultrasonic cleaner. B, Instrument basket. C, Beaker holder. D, Bur tray. E, Suspension
bracket. F, Beaker band. G, Beaker cover. H, Glass beaker. I, Cover. (Courtesy L & R Manufacturing Company, Kearny, NJ.)
A
B
C
DE
FG
H
I

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-7 It is important to keep the ultrasonic cleaner covered while in use to reduce splatter and contaminated aerosols.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Ultrasonic Cleaning-cont’d
• The ultrasonic cleaner works by producing sound waves beyond the range of human hearing.
• These sound waves, which can travel through metal and glass containers, cause cavitation (formation of bubbles in liquid).
• Instruments should be processed in the ultrasonic cleaner until they are visibly clean.
• The time may vary from 5 to 15 minutes, depending on the amount and type of material on the instruments, and the efficiency of the ultrasonic unit.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Ultrasonic Cleaning Solutions
• You should use ultrasonic solutions that are specially formulated for use in the ultrasonic cleaner only.
• Some ultrasonic cleaning products have enzyme activity.
• Other ultrasonic cleaning products have antimicrobial activity, which reduces the buildup of microbes in the solutions with repeated use.
• The antimicrobial activity does not disinfect the instruments; it merely prevents the microorganisms from increasing in number.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-8 A commercial all-purpose ultrasonic cleaner. (Courtesy Certol.)
Fig. 21-9 An enzyme ultrasonic cleaner in tablet form. (Courtesy Crosstex.)
Fig. 21-8 Fig. 21-9
Copyright © 2005 by Elsevier Inc. All rights reserved.
Ultrasonic Cleaning Solutions-cont’d
• Do not use other chemicals such as plain disinfectants in the ultrasonic cleaner.
• Some disinfectants can “fix” the blood and debris onto the instruments, making subsequent cleaning more difficult.
• Specific ultrasonic solutions are available that remove difficult materials, such as cements, tartar, stains, plaster, and alginate.
• Refer to the ultrasonic unit manufacturer’s instructions regarding the specific solution to be used.
• The ultrasonic cleaning unit should be labeled with both a chemical label and a biohazard label because it contains a chemical and contaminated instruments.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Care of the Ultrasonic Cleaner
• The ultrasonic cleaner solution is highly contaminated and must be discarded at least once a day or sooner if it becomes visibly cloudy.
• When changing the solution, the inside of the pan and lid should be rinsed with water, disinfected, rinsed again, and dried.
• All PPE should be worn while changing solutions in the ultrasonic cleaner.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Testing the Ultrasonic Cleaner• If you notice that the instruments are not being cleaned completely
after processing in the ultrasonic cleaner, the unit may not be functioning properly.
• To determine whether the ultrasonic cleaner is working properly, hold a 5 × 5-inch sheet of lightweight aluminum foil vertically (like a curtain) half-submerged in the fresh, unused solution.
• Run the unit for 20 seconds, and then hold the foil up toward the light.
• The surfaces that were submerged into the solution should be evenly marked with a tiny pebbling effect over the entire surface.
• An area on the foil that is greater than ½ inch without pebbling indicates that there is a problem with the unit, and that it needs servicing by the manufacturer.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Automated Washers/Disinfectors
• Automated instrument washers/disinfectors look and work similar to a household dishwasher.
• However, they must be approved by the U.S. Food and Drug Administration (FDA).
• Automated washing/disinfecting units use a combination of very hot water recirculation and detergents to remove organic material.
• Then the instruments are automatically dried. These units are classified as thermal disinfectors because they have a disinfecting cycle that subjects the instruments to a level of heat that kills most vegetative microorganisms.
• Instruments processed in the automatic washers/ disinfectors must be wrapped and sterilized before use on a patient.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Drying, Lubrication, and Corrosion Control
• Instruments and burs made of carbon steel will rust during steam sterilization.
• Rust inhibitors such as sodium nitrate or commercial products are available as a spray or dip solution and help to reduce rust and corrosion.
• An alternative to rust inhibitors is to dry the instrument thoroughly using dry heat or unsaturated chemical vapor sterilization (discussed later), which does not cause rusting.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Packaging Instruments
• Before sterilization, the instruments should be wrapped or packaged to protect them from becoming contaminated after sterilization.
• When instruments are sterilized without being packaged, they are immediately exposed to the environment as soon as the sterilizer door is opened.
• They can be contaminated by aerosols in the air, dust, improper handling, or contact with nonsterile surfaces.
• An additional advantage to packaging instruments is that they can be grouped into special setups, such as crown/bridge, amalgam, prophy, or composite.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-10 Special tartar and stain remover ultrasonic solution (Courtesy Crosstex.)

Copyright © 2005 by Elsevier Inc. All rights reserved.
Packaging Materials
• Sterilization packaging materials and cassettes are medical devices and therefore must be FDA approved.
• It is critical to use only products and materials that are labeled as “sterilization” packaging.
• Never substitute products such as plastic wraps, paper, or zipper-lock freezer bags that are not registered for this purpose. These products may melt or prevent the sterilizing agent from reaching the instruments inside.
• Specific types of packaging material are available for each method of sterilization. You should use only the type of packaging material designed for the particular method of sterilization that you are using.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Packaging Materials-cont’d
• A wide variety of sterilization packaging materials are available. Self-sealing or heat-sealed “poly” bags or tubes provide an excellent wrap.
• In addition, paper wraps and cloth wraps are available.
• If the package is not the self-sealing type, you should only use sterilization indicator tape to seal the package.
• Never use safety pins, staples, paper clips, or other sharp objects that could penetrate the packaging material.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-12 Self-seal packages provide an excellent wrap for sterilized materials. (Courtesy SPS Medical.)

Copyright © 2005 by Elsevier Inc. All rights reserved.
Sterilization of Unwrapped Instruments
• An unwrapped cycle (sometimes called flash sterilization) is a method for sterilizing unwrapped patient-care items for immediate use.
• The time for unwrapped sterilization cycles depends on the type of sterilizer and the type of item (i.e., porous or nonporous) to be sterilized.
• Unwrapped sterilization should be used only under certain conditions.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Sterilization Monitoring
• It is critical that dental instruments are properly sterilized.
• Because microorganisms cannot be seen with the naked eye, the major difficulty in sterilization is determining when an item is sterile.
• Currently, three forms of sterilization monitoring are used: physical, chemical, and biologic.
• All three processes are unique, have different functions, and must be used consistently to ensure sterility.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Physical Monitoring
• Physical monitoring of the sterilization process involves looking at the gauges and readings on the sterilizer and recording the temperatures, pressure, and exposure time.
• Although correct readings do not guarantee sterilization, an incorrect reading gives you the first signal of a problem.
• Remember that the temperature recorded is for the chamber, not the inside of the pack.
• Therefore, problems with overloading or improper packaging would not be detected from the reading on the gauges.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Chemical Monitoring
• Chemical monitoring (external and internal) involves the use of heat-sensitive chemical that changes color when exposed to certain conditions.
• The two types of chemical indicators are:
– Process indicators
– Process integrators
Copyright © 2005 by Elsevier Inc. All rights reserved.
Process Indicators
• Process indicators (external) are placed outside the instrument packages before sterilization.
• Examples are autoclave tape and color-change markings on packages or bags.
• Process indicators simply identify instrument packs that have been exposed to a certain temperature; they do not measure the duration or the pressure.
• Process indicators are useful in distinguishing between packages that were processed and those that were not processed.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-13 A, Unprocessed instruments. B, Wrapped instruments after processing. Note the color change in the tape.
(From Young AP, Kennedy DB: Kinn’s the medical assistant: an applied learning approach, ed 9, Philadelphia, 2003, Saunders.)
A B
Copyright © 2005 by Elsevier Inc. All rights reserved.
Process Integrators
• Process integrators (internal) are placed inside instrument packages.
• They respond to a combination of pressure, temperature, and time.
• Process integrators are also known as multi-parameter indicators. All sterilization factors are integrated.
• Process indicators and integrators provide immediate, visual control of sterilizing conditions.
• They do not indicate sterility and are not a replacement for biologic monitoring.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Biologic Monitoring
• Biologic monitoring, or spore testing, is the only way to determine if sterilization has occurred and all bacteria and endospores have been killed.
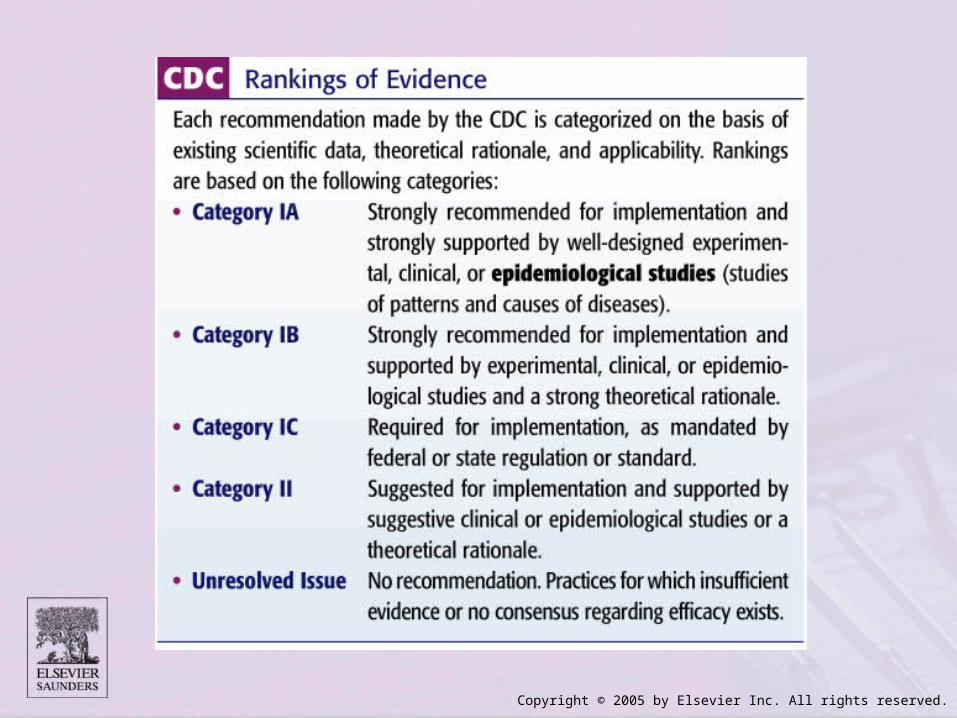
• The Centers for Disease Control and Prevention (CDC), American Dental Association (ADA), and Office of Safety and Asepsis Procedures Research Foundation (OSAP) recommend at least weekly biologic monitoring of sterilization equipment.
• Several states also require routine biologic monitoring at weekly, monthly, or cycle-specific intervals, such as spore testing every 40 hours of use or every 30 days.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Biologic Indicators (BIs)• Also known as spore tests, BIs are vials or strips of paper that
contain harmless bacterial spores (spores are highly resistant to heat).
• Three BIs are used in testing. Two BIs are placed inside instrument packs, and the sterilizer is operated under normal conditions. The third strip is set aside as a control.
• After the load has been sterilized, all BIs are cultured. If the spores survive the sterilization cycle (a positive culture), a sterilization failure has occurred.
• If the spores are killed (a negative culture), the sterilization cycle was successful.
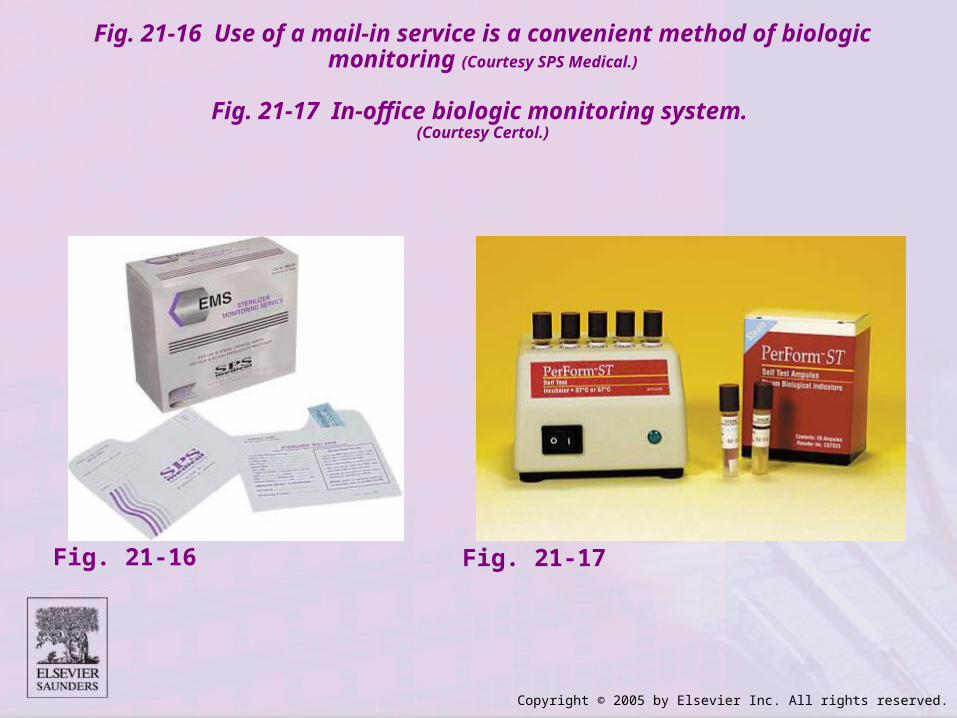
• The culturing of the spore test is usually handled through the use of a mail-in monitoring service.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-16 Use of a mail-in service is a convenient method of biologic monitoring (Courtesy SPS Medical.)
Fig. 21-17 In-office biologic monitoring system. (Courtesy Certol.)
Fig. 21-16 Fig. 21-17

Copyright © 2005 by Elsevier Inc. All rights reserved.
Methods of Sterilization• Sterilization destroys all microbial forms, including bacterial
spores. Sterile is an absolute term; there is no “partially sterile” or “almost sterile.”
• All reusable items (critical and semicritical instruments) that come in contact with the patient’s blood, saliva, or mucous membranes must be heat-sterilized.
• The three most common forms of heat sterilization in the dental office are
(1) steam sterilization
(2) chemical vapor sterilization
(3) dry heat sterilization

Copyright © 2005 by Elsevier Inc. All rights reserved.
Steam Autoclave Sterilization
• An autoclave is used to sterilize dental instruments and other items by means of steam under pressure.
• Steam sterilization involves heating water to generate steam, producing a moist heat that rapidly kills microorganisms.
• As the steam completely fills the sterilizing chamber, the cooler air is pushed out of an escape valve, which then closes and allows the pressure to increase.
• It is the heat, not the pressure, that actually kills the microorganisms.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-18 A steam autoclave

Copyright © 2005 by Elsevier Inc. All rights reserved.
Steam Autoclave Sterilization-cont’d
• Packaging material for steam sterilization must be porous enough to permit the steam to penetrate to the instruments inside.
• The packaging material may be fabric but most often is sealed film or paper pouches, nylon tubing, sterilizing wrap, or paper-wrapped cassettes.
• A disadvantage of steam sterilization is that the moisture may cause corrosion on some high-carbon steel instruments.
• Distilled water should be used in autoclaves instead of tap water, which often contains minerals and impurities. Distilled water can minimize corrosion and pitting.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Autoclave Operation Cycles
• Dental office steam sterilizers usually operate through four cycles:
• Heat-up cycle
• Sterilizing cycle
• Depressurization cycle
• Drying cycle
Copyright © 2005 by Elsevier Inc. All rights reserved.
Flash Sterilization• Rapid or “flash” sterilization of dental instruments is
accomplished by rapid heat transfer, steam, and unsaturated chemical vapor.
• Flash sterilization may be used only on instruments that are placed in the chamber unwrapped. This presents a compromise because the sterility of the instruments is defeated immediately when the instruments are removed from the sterilizer.
• Flash sterilization also should be used only for instruments that are to be promptly used on removal from the sterilizer.
• It is always the best policy to use a method of sterilization in which the instruments can be packaged before use and remain packaged until the time of use.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-20 StatIM sterilizer (Courtesy SciScan.)

Copyright © 2005 by Elsevier Inc. All rights reserved.
Chemical Vapor Sterilization
• Chemical vapor sterilization is very similar to autoclaving, except a combination of chemicals (alcohol, formaldehyde, ketone, acetone, and water) is used instead of water to create a vapor for sterilizing .
• OSHA requires a material safety data sheet (MSDS) on the chemical vapor solution because of the chemicals’ toxicity.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Advantages of Chemical Vapor Sterilization
• The major advantage of the chemical vapor sterilizer is that is does not rust, dull, or corrode dry metal instruments.
• The low water content of the vapor prevents destruction of items such as endodontic files, orthodontic pliers, wires, bands, and burs.
• A wide range of items can be sterilized routinely without damage.
• Other advantages include the short cycle time and the availability of a dry instrument after the cycle.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Disadvantages of Chemical Vapor Sterilization
• The primary disadvantage is that adequate ventilation is essential because residual chemical vapors containing formaldehyde and methyl alcohol can be released when the chamber door is opened at the end of the cycle.
• These vapors can temporarily leave an unpleasant odor in the area and may be irritating to the eyes.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Filtration and Monitoring of Chemical Vapors
• Newer sterilizers are equipped with a special filtration device that further reduces the amount of chemical vapor remaining in the chamber at the end of the cycle. Older models can usually be retrofitted.
• Formaldehyde monitoring badges also are available for employees, similar to radiation monitoring devices. The monitoring measures personal exposure to formaldehyde for a period; the badge is mailed to the monitoring service and a laboratory analysis is sent to the employee.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Packaging for Chemical Vapor Sterilization
• Standard packaging for chemical vapor sterilization includes film pouches or paper bags, nylon see-through tubing, sterilization wrap, and wrapped cassettes.
• Thick or tightly wrapped items require longer exposure because of the inability of the unsaturated chemical vapors to penetrate as well as saturated chemical vapors under pressure.
• As in autoclaving, closed containers (such as solid metal trays and capped glass vials) and aluminum foil cannot be used in a chemical vapor sterilizer because they prevent the sterilizing agent from reaching the instruments inside.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Pressure, Temperature, and Time for Chemical Vapor Sterilization
• The three major factors in chemical vapor sterilization are:
– Pressure, which should measure 20 psi
– Temperature, which should measure 270° F (131° C)
– Time, which should measure 20 to 40 minutes
Copyright © 2005 by Elsevier Inc. All rights reserved.
Dry Heat Sterilization• Dry heat sterilizers operate by heating up air and transferring that
heat from the air to the instruments.
• This form of sterilization requires higher temperatures than steam or chemical vapor sterilization.
• Dry heat sterilizers operate at approximately 320° to 375° F (160° to 190° C) depending on the type of sterilizer.
• The advantage of dry heat is that the instruments will not rust if they are thoroughly dry before they are placed in the sterilizer.
• The two types of dry heat sterilizers available are static air and forced air.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Static Air Sterilizers
• Static air sterilizers are similar to an oven: the heating coils are on the bottom of the chamber, and the hot air rises inside through natural convection.
• Heat is transferred from the static (nonmoving) air to the instruments in about 1 to 2 hours.
• The disadvantages of static dry heat are that the sterilization process is time-consuming and may not be effective if the operator makes errors in calculating the correct processing time.
• The wrapping material must be heat resistant. Aluminum foil, metal, and glass containers may be used. Paper and cloth packs should be avoided because they may burn or discolor from the intense heat.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Forced Air Sterilizers
• Forced air sterilizers, also called rapid heat transfer sterilizers, circulate the hot air throughout the chamber at a high velocity.
• This action permits a rapid transfer of heat energy from the air to the instruments, reducing the time needed for sterilization.
• Exposure time in forced air sterilizers, after the sterilizing temperature has been reached, ranges from 6 minutes for unpackaged items to 12 minutes for packaged items.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Sterilization Failures
• A load may fail to become sterilized when direct contact for the correct time is insufficient between the sterilizing agent (chemical or steam) and all surfaces of the items being processed.
• Several factors can cause the sterilization process to fail, including improper instrument cleaning or packaging and sterilizer malfunction.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Chemical Liquid Sterilization
• Not all items can withstand heat sterilization. Some types of plastics, such as some rubber dam frames, shade guides, and x-ray film-holding devices, are damaged by heat sterilization.
• Thus a liquid sterilant such as 2.0-3.4% glutaraldehyde must be used for sterilization of these items.
• Sterilization in glutaraldehyde requires a 10-hour contact time; anything less than 10 hours is disinfection, not sterilization.
• Be sure that you have an MSDS for these products. All employees should be properly trained on how to handle them.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Fig. 21-22 SPOROX II is a high level disinfectant/sterilant used for instruments that cannot tolerate heat sterilization.
(Courtesy Sultan Chemists Inc, Englewood, NJ.)
Copyright © 2005 by Elsevier Inc. All rights reserved.
Ethylene Oxide Sterilization
• Ethylene oxide gas is a recognized method of sterilization. This method operates at low temperatures, which is an advantage for plastic and rubber items that would melt in heat sterilizers.
• However, ethylene oxide sterilization requires 4 to 12 hours for sterilization, depending on the sterilizer model. Also, at least 16 hours of post-sterilization aeration is required to remove the gas molecules bound to the plastic and rubber surfaces.
• Ethylene oxide is ineffective on wet items. Toxicity is a risk if the gas is not handled properly.
• These units are often used in large clinics or hospital settings but rarely in private dental practices.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Handpiece Sterilization
• High-speed dental handpieces rotate at speeds up to 400,000 revolutions per minute (rpm).
• Blood, saliva, and tooth fragments, as well as restorative materials, may lodge in the head of the handpiece, where they may be retained and transferred to another patient.
• Therefore, dental handpieces must be properly cleaned and heat-sterilized.
Copyright © 2005 by Elsevier Inc. All rights reserved.
Handpiece Flushing Techniques
• Flushing the handpiece is the best way to remove debris from the head of the handpiece.
• To flush a dental handpiece:
• Attach a pressurized handpiece cleaner to the intake tube of the handpiece (where the air passes through).
• Flush the head of the handpiece to remove debris.
• Blow out the handpiece using compressed air to remove debris before sterilization.
• Running coolant water from the dental unit through the handpiece at chairside is insufficient. Coolant water does not run through the turbine chamber, where debris can collect.

Copyright © 2005 by Elsevier Inc. All rights reserved.
Handpiece Sterilization Techniques
• Only steam sterilization and chemical vapor sterilizers are recommended, because handpiece sterilization temperatures should not exceed 275° F (135° C).
• Unless they will be used immediately after sterilization, handpieces should be packaged in bags, wraps, or packs to protect them from contamination before use.
• Never run a handpiece “hot” out of the sterilizer, and avoid rapid cool-downs, such as running the handpiece under cold water. Handpieces use very small metal components; extreme cold changes stresses the metal.
• If handpieces need to be cooled quickly after sterilization, use an air fan to blow room-temperature air over them.


















