Coordinating Care in the Total Cost of Care...
31
Coordinating Care in the Total Cost of Care Environment Stacy Garrett-Ray, MD, MPH, MBA January 9, 2018 1
Transcript of Coordinating Care in the Total Cost of Care...

Coordinating Care in theTotal Cost of Care Environment
Stacy Garrett-Ray, MD, MPH, MBAJanuary 9, 2018
1

2
Agenda
• Review Local Landscape with Value Based Care
• Medicare Performance Adjustment and Total Cost of Care
• Care Coordination Strategies to Manage Under Total Cost
of Care
• Lessons Learned
Confidential and Proprietary
3
Disclosures
I have no relevant financial or other disclosures.
Confidential and Proprietary

4
Current State of Health Care:
Searching for Value
Sources: M. Bittle, Population Health and Population Health Management: “What it is and What it isn’t” November 2018
Graphic: J. Colmers, Commissioner, Health Services Cost Review Commission, Maryland

5
Current State of Health Care:
Searching for Value

6
Rapid Rise of Healthcare Insurance Premiums
Sources: (left) Kaiser Family Foundation/Health Research and Educational Trust, Employer Health Benefits Annual Surveys, 1999–2012; (right)
authors’ estimates based on CPS ASEC 2001–12, Kaiser/HRET 2001–12, CMS OACT 2012–21.
Projected average family premium as
a percentage of median family
income, 2013–2021
Cumulative changes in insurance
premiums and workers’ earnings,
1999–2012
PercentPercent
180%
47%
38%
Projected
172%

7
• Intermittent, episodic care– Fosters fragmentation
• Lack of coordination throughout
continuum of care– No accountability to perform as a
healthcare system
• Systems built to treat the sick
• Rewards utilization/volume
(Traditional Fee for Service)
Reactive, Volume Based
Care
Current State
Current State of Health Care:
Searching for Value
Confidential and Proprietary

8
• Coordinated
• Continuous, Proactive
• Connected care – Streamlined, easier to
use and focused on prevention– Utilize technology to monitor, prevent conditions,
and assist with intervention and diagnoses
– Predictive Analytics
– Artificial Intelligence
• Individualized, genomics
• Reimbursement based to value and
management of total cost of care– Lower cost
– Better experience
– Better quality
– Better outcomes
Proactive,
Value Based Care
Future State
Future State of Health Care:
Searching for Value
Confidential and Proprietary

9
Payors Are Implementing New Reimbursement
Models to Influence Health Care Delivery
Maryland’s physician value based contracting models are advancing similar to
other areas of the country where providers have opportunities to assume financial
risk to manage populations.
• Patient Centered Medical Home (PCMH) is a voluntary program and providers who
participate can earn additional reimbursement increases of three types – increased fee
schedules, care plan development/maintenance fees, additional fee schedule rewards
for reduced cost.
• Most dominant value based program in Maryland.
• Other commercial and federal payers and have created Accountable Care
Organization (ACO) models that reward for reduced utilization and increased quality.
• Goal is to move providers toward taking greater financial and clinical risk.
6

10
Maryland’s Medicare Waiver
Phase I (2014-2018)
Controlling and reducing
the rate of growth in
per capita hospital
expenditures for Maryland
residents
Phase 2 (2019-2023)
Controlling and reducing the
rate of growth in total health
care cost per Medicare
Beneficiary in Maryland
Primary Care
Offices
Home
Confidential and Proprietary

11
Highlights of
Maryland Primary Care Program (MD PCP)
UTILIZATION
CMS will assess practice performance on utilization measures. For the 2018 Measurement Period, we will focus on the following two utilization measures
from the Healthcare Effectiveness Data and Information Set (HEDIS®)
•Inpatient hospitalization utilization per 1,000 attributed beneficiaries
•Emergency department utilization per 1,000 attributed beneficiaries
QUALITY AND PATIENT EXPERIENCE
This model aims to improve the beneficiary quality and experience of care and decrease the total cost of care.
To assess quality performance and eligibility for the CPC+ performance-based incentive payment, CMS will require Track 1 and 2 practices to annually report
electronic clinical quality measures (eCQMs) and patient experience of care measures (Consumer Assessment of Healthcare Providers & Systems [CAHPS]).
Performance
Alignment with
Medicare Hospital Goals
Based on CMS
Comprehensive Primary
Care Plus (CPC+) program
Launch- January 2019
12
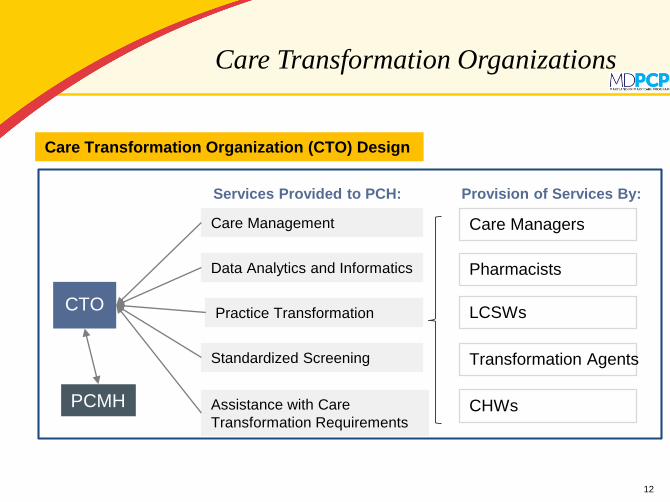
Care Transformation Organizations
Care Transformation Organization (CTO) Design
CTO
Care Management
Data Analytics and Informatics
Practice Transformation
Assistance with Care
Transformation Requirements
Standardized Screening
PCMH
Care Managers
Pharmacists
LCSWs
Transformation Agents
CHWs
Services Provided to PCH: Provision of Services By:

13
And
Risk Stratified
Care Management
Behavioral Health Consults and
Telepsychiatry
Pharmacy Expertise and
Medication Management
Practice Transformation
Specialists
LCSWs, Social Risk Assessment
Transitions of Care Support
Quality Improvement
Activities
Data Analytics
Our patient-centered care model uses a team-based approach to work collaboratively with
providers on care delivery transformation that is tailored to their individual needs.
Confidential and Proprietary

14
Definition of Population Health Management
The capability to successfully manage care for a group of
individuals in order to reduce unnecessary utilization and cost
and improve quality, outcomes, and experience.
Key elements:
• A high performing network of providers---community and hospital based
• A “population health bundle” of people, processes, and information technologies that
are utilized by network providers to successfully manage care

15
Population Health Management
Confidential and Proprietary

16
Source: Thomson Reuters Marketscan Database
The 70/10 Rule
Major factor in Effectively Managing TCOC
Focus care management on “high cost” populations

17
Risk Stratification:
Focus of Interdisciplinary Care Teams
Confidential and Proprietary

18
Appropriate Documentation and Coding is
Necessary to Accurately Reflect Population
Accurate
Documentation and Coding
allows us to provide
appropriate care
management resources for
patientsConfidential and Proprietary

19
CMS Hierarchical Condition Category
(HCC) Risk Adjustment Factors
• HCC model is built off the Medicare FFS population –which is
the “denominator.”
• Average risk score of 1.0 and cost an average of $9,367.51 in
2018.
• The RAF weighting can be multiplied against that value to
estimate how much cost is associated with each condition.
Announcement of Calendar Year 2017 MA Capitation Rates and Medicare Advantage and Part D Payment Policies
* - Source:BCHD White Paper: State of Health in Baltimore (Winter 2016)- https://health.baltimorecity.gov/state-health-baltimore-winter-2016
Per ACO Data,
Average Risk Score in Baltimore City is 0.85 in 2017.
“[Baltimore
City] has a
mortality rate
30% higher
than the rest
of the state,
and ranks last
on key health
outcomes
compared to
other
jurisdictions
in
Maryland.”*
RAF Score Expected Expenditures
Diabetes without complications 0.104 $974
Diabetes with complications 0.318 $2,978
Confidential and Proprietary

20
Know the Population:
Coordinating Care Across the Continuum
Community Connect
Confidential and Proprietary

21
- High Utilization (multiple ER visits and/or
admissions in last 12 months)
- Polypharmacy (>10 medications)
- High risk medications (e.g., Warfarin)
- Multiple chronic conditions
- Poorly controlled disease states
- High medical and pharmacy costs
- Problems with adherence to treatment plan
- Multiple providers; multiple caregivers
- High potential for negative outcome within next
year without care management intervention
(Predictive Analytics)
Criteria for Targeting High Risk
Patients for Complex CM Enrollment
Confidential and Proprietary

22
Population Health Management
Engage: Interventions to Support Operations
Portfolio MD
Confidential and Proprietary

23
Home Care
High Risk Clinics
Complex Care and Disease Management
Self-Management & Health Education
Programs
Additional
Medical
Management
Infrastructure
Costs (per
patient
treatment per
month)
Home Care ManagementProvides in-home medical care management by specialized physicians, nurse care
managers and social workers for chronically frail seniors that have physical, mental,
social and financial limitations. Chronically disabled patients receive specialized
integrated home care programs
Complex Care and Disease ManagementProvides long-term whole person care enhancement for the
population using a multidisciplinary team approach.
Diabetes, COPD, CHF, CKD, Depression, Dementia, Organ transplant
and Cancer.
Self Management, PCPProvides self-management for people with
chronic disease and prevention services.
High Risk Clinics and Care ManagementProvides one-on-one physician /nurse, and case management for highest risk
population. As risk is reduced, patient transferred to Level 2. Physicians and
care managers are integrated into community resources, physician offices, or
clinics. Chronically mentally ill are directed to specialized medical clinics
Hospice/Palliative Care
Matching the Patient
to the Care That They Need
Confidential and Proprietary

24
Population Health Management
Manage: Optimize Performance and Outcomes
Confidential and Proprietary

25
Key Areas of Focus
1. Leadership support and governance
- Culture change for community practices and hospitals to partner together as a
network to enhance quality of care and outcomes
2. Strategy, sustainability, and transformation
- What does it take to develop and maintain a sustainable model (i.e. network vs.
individual practice provided services, SOPs, Training, Onboarding)
- Share promising practices
- Engage providers and practices to actively become necessary change agents for
transformation
3. Network composition and access.
- Ideal network size and provider mix to care for population including community
partners
4. Population health management capability
- Identify and build services including data analytics and
infrastructure required to support the network
- Prioritization process for system approach
Adapted from: Corneliuson et al. Super Clinically Integrated Networks: 8 Components to Consider http://blog.thecamdengroup.com/blog/topic/clinically-
integrated-networks Confidential and Proprietary

26
Key Areas of Focus
5. Clinical care models and coordination
- Identify potential clinical care models to assist with
the management of high cost, chronic disease
patient groups
- Identify gaps and optimal approaches to integrate care to gain
across the network
6. Quality, value and transparency
- Identify quality metrics being measured and tracked and reporting
process and identify gaps and develop communications plan and
strategy to address
7. Financial management and reimbursement
- Develop financial incentives and risk sharing supporting TCOC
goals (i.e. MDPCP, TCOC)
8. Provider/Patient experience and activation
- Develop communications, educational, and community support
programs to engage providers and patients and improve compliance
Adapted from: Corneliuson et al. Super Clinically Integrated Networks: 8 Components to Consider http://blog.thecamdengroup.com/blog/topic/clinically-
integrated-networks Confidential and Proprietary

27
Lessons Learned
• It’s all about execution - People, processes and technology.
• Standardization using best practices is important to operate
effectively.
• Commit to continuous improvement and innovation.
• Allow the data drive your initiatives. The business case is
based on improving outcomes, quality of care and cost
avoidance---building and adhering to sophisticated, rigorous
financial models is important.
• Building population health capabilities takes time!
• It take a team! – Community Providers and Resources
in Collaboration with HospitalsConfidential and Proprietary

28
Thank you
Thank you to the
University of Maryland Quality Care Network/
Transform Health MD Team
for your hard work and dedication!
Confidential and Proprietary

29
Questions

30
MDPCP Financial Opportunity
• Based on CMS
Hierarchical Condition
Categories (HCC)
• Factors in demographic
factors, chronic
conditions
• Increased care
management fees by risk
score allows providers to
better manage care
• PBPM= Per Beneficiary
Per Month
Track 1 Track 2
Risk TierCriteria
PBPM
CMF Criteria
PBPM
CMF
Tier 1 01-24% HCC $6 01-24% HCC $9
Tier 2 25-49% HCC $8 25-49% HCC $11
Tier 3 50-74% HCC $16 50-74% HCC $19
Tier 4 75-89% HCC $30 75-89% HCC $33
Complex
90+ HCC or
persistent and
severe mental
illness, substance
use disorder or
dementia $50
90+ HCC or
persistent and
severe mental
illness, substance
use disorder or
dementia $100
Care Management Fees

31
Population Health Management
Confidential and Proprietary


















