Converging Epidemics of Diabetes and Tuberculosis...
104
Converging Epidemics of Diabetes and Tuberculosis: Epidemiology and Public Health Consequences Julia Critchley, Fiona Pearson, Peijue Huangfu, Daniel Grint, Reinout van Crevel, Susanne Awad, Yoko Laurence TANDEM team EC FP7 funding QNRF
Transcript of Converging Epidemics of Diabetes and Tuberculosis...

Converging Epidemics of Diabetes and Tuberculosis: Epidemiology and Public Health Consequences
Julia Critchley, Fiona Pearson, Peijue Huangfu, Daniel Grint, Reinout van Crevel, Susanne Awad, Yoko LaurenceTANDEM team EC FP7 fundingQNRF

Global Burden of TB and of DM
• 10.4 million TB cases• 1/4 global population infected
with LTBI• 1.7 million deaths, 95% of which
occur in LMIC
• 424.9 million with diabetes, 50% undiagnosed
• >90% Type II
• 79% living in LMIC• Increase to 629 million by 2045
• 4 million deaths
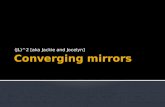
Estimated TB incidence 2016
Estimated DM prevalence 2017

Is DM associated with TB?
• Association historically noted and treatment was given in specialist centres (Avicenna, Susutra,
Morton; 1950’s tx centres in UK)
• Evidence synthesised in several distinct reviews (Stevenson 2007; Jeon 2008, Al-Rifai 2017)
• Recently updated - 44 studies from 16 countries
• Prospective: DM ~ 3.6-fold higher TB risk (2.3-5.7)
• Higher in low-income and high-incidence
• Higher in Asia compared to Europe/USA
• Higher for confirmed TB and blood tested DM

Hyperglycaemia / Glycaemic control & TB risk / outcomes
• Limited evidence – e.g.• Leung et al 2008 HK• Lee et al. 2016 Taiwan• Leegard et al 2011 Denmark• Pealing et al 2015 UK
• Some suggestions of higher TB risk among those with poorly controlled DM
• Recent systematic review of 8 studies (Shewade et al. Plos One 2017) could not reach any conclusions
• Association may be non-linear
• Unclear to what extent it might be reversible?
• English primary care data 2010-2015 (>85,000 DM patients, >150,000 controls)
• 24% of TB among DM patients in UK attributable to poor • glycemic control Critchley J, Diabetes Care 2018

TB treatment outcomes amongst those with DM
• 2011 review suggested DM worsens treatment outcomes among TB patients [Baker et al. 2011],recently updated [Huangfu et al 2019, in press IJLTD]
• Included studies: relatively poor in quality (observational data)
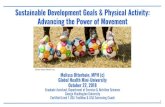
• New review; 102 studies in total including 44 reporting on mortality (56,122 individuals with TB-DM and 243,035 with TB)
• Death OR=2.83, 95%CI: 1.45-5.52;
I2=47% among studies that
controlled for key confounders
(age, sex, HIV)
5
Odds Ratio 95% CI
2 month culture +ve 1.88 1.59 - 2.21
Death 1.64 1.29 - 2.08
Relapse 1.98 1.51 - 2.60
Death and Relapse 1.90 1.43 – 2.53
MDR-TB 1.86 1.51 – 2.28

Prevalence of DM in TB patients; TB-DM hotspots ...
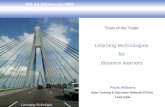
• Overall prevalence of DM 15·3% (95% prediction interval 2·5–36·1; I2 99·8%), varying from 0·1% in Latvia to 45·2% in Marshall Islands [200 studies; 2,291,571 people with active tuberculosis
Noubiap et al, Lancet Global Health 2019
• South India. 209 pulmonary TB, ~45 years, BMI ~20• 54% diabetes (OGTT, HbA1c), 21% pre-diabetes• 25% euglycemic Kornfeld et al, Chest 2016
• Kiribati, Pacific. 275 TB cases, ~37 years, BMI 22.5• 37% diabetes (>50% in those >35 years) vs. 18% in matched controls• 55% previously undiagnosed DM
Viney et al, TMIH 2015
• Southern Texas/ Mexico. 233 TB cases, ~44 years, 25% obese• 37% diabetes, ~ 2-3-fold more compared to background population• DM responsible for 25% of TB (versus HIV: 5%)
Restrepo, Bull WHO 2011

Daniel Grint et alBull WHO 2018
Tuesday, 19 May 2015 2nd Progress Meeting
Day 2
Work Package 3 Chair: Jackie Cliff
9.00 – 11.00 WP3 Bioprofiling analysis in TB, TB-DM and DM patients
Introduction: WP Status Update & Relevant Literature: Jackie Cliff (LSHTM)
Selection of platform, location, samples for cross-sectional analysis: Jackie Cliff MLPA gene panel (brief update): Simone Joosten (LUMC)
Immune Assays at SUN: Katharina Ronacher (SUN)
11.00 – 11.30 Coffee Break 11.30 – 12.20 Two open presentations about TANDEM and TB-DM (Indonesian & foreign speaker) 12.20 – 13.30 Lunch & Meeting with National TB and DM Representatives Work Package 4 Chair: Macarena Beigier 13.30 – 15.00 WP4 Cellular basis accounting for the causal link between diabetes
and TB
Introduction: WP Status Overview: Macarena Beigier (MPIIB) Adipocytes and TB: Macarena Beigier (MPIIB) Macrophage studies: Simone Joosten (LUMC) In-vitro studies in Nijmegen: Ekta Lachmandas (RUNMC) Genetic susceptibility and eQTL of TB and DM: Vinod Kumar (UMCG)
15.00 – 15.30 Coffee Break WPs: Where do we stand (break-out in 2 groups) 15.30 – 16.45 Planned vs. actual work progress
Next objectives and action tasks
Indonesia
Peru
Romania
South Africa

• Practical screening algorithms• Characteristics of DM drugs• Glycemic control• Cardiovascular risk management• TB treatment issues• combined HIV, diabetes and TB• ….
Yan Lin, Tony Harries ..
Issued by the TB Union and World Diabetes Foundation
What should be done for a TB patient diagnosed in a TB clinic who is
diagnosed with new DM or who is already receiving treatment for DM?
The following steps should be carried out:
• Glycaemic control should be assessed either by measurement of HbA1c or
measurement of FBG. This assessment can be done in the TB clinic if blood glucose
can be measured. If assessment has to be done at the DM clinic or a general health
clinic, this is best postponed until at least two weeks or even 2 months of TB treatment
have been completed. Guidance for newly diagnosed patients or those already
receiving DM treatment is shown in Table 3.
• Document cigarette smoking status and counsel if still smoking.
• Ask about history of cardiovascular disease (myocardial infarction, stroke, peripheral
arterial disease). If yes, then start/continue low-dose aspirin (75-150 mg once a day).
• After 8 weeks (at the end of the initial intensive phase of TB treatment for drug-
susceptible TB), measure blood pressure and start / increase antihypertensive
medication if systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥
90mm Hg, considering possible drug-interactions with rifampicin.
• After 8 weeks (at the end of the initial intensive phase of TB treatment for drug- susceptible TB), start/continue statin if age > 40 years or there is established
cardiovascular disease.
Table 3: Management of HbA1c or blood glucose at the start of TB treatment
HbA1c or FBG at the start
of
anti-TB treatment
Diagnosed with
new DM
Already receiving
treatment for DM
If HbA1c <8% or FBG < 10.0
mmol/l (180 mg/dl)
No further immediate
action is taken; re-assess
blood glucose levels at 2
months and again at the
end of TB treatment
No further action is
taken; the patient
continues on current
medication for DM
If HbA1c ≥8% but less than
10% or FBG ≥ 10 mmol/l (180 mg/dl) but less than15 mmol/l
(270 mg/dl)
Start metformin 500 mg
once a day, reassess in two weeks and increase the
dose to 500 mg twice a day or refer if blood glucose
levels have not improved
Intensify current glucose
lowering treatment and reassess one - two weeks
later
If HbA1c ≥10% or FBG ≥
15mmol/l (270 mg/dl)
Start metformin 500 mg
twice a day and seek
specialist advice.
Seek specialist advice
and consider the need for
hospital admission for
better glucose control

What is the population impact? - INDIA
INDIA - TB-DM dynamic mathematical model
199014.5% (95% UI: 9.5%-18.2%) TB-
related deaths
11.4% (95% UI: 6.3%-14.4%) TB incidence
2050 42.8% (95% UI: 28.7%-53.1%) TB deaths
33.3% (95% UI: 19.0%-44.1%) TB incidence
effects of DM on TB disease progression and infectiousness
Sensitivity analyses suggested that the impact could be even greater
16/09/2016 9Awad S et al 2019 (in press) Journal of Global Health; Awad et al 2019 (in press) Scientific Reports

Conclusions
• DM increases TB disease risk and risk of poor TB treatment outcomes (mortality)• DM is often common in TB patients, and often undiagnosed• Higher glucose / HbA1c levels – higher risks – reversible?• Need for screening and better clinical management of TB-DM
• Screening TB patients for DM (YES), less clear on screening DM for TB• TWO step screening (using RPG, or a risk score as first step) may be most
cost-effective, screening needs repeating later in TB treatment also• What happens to patients identified with DM at the end of TB treatment?
• POPULATION IMPACT - In India, one in every five TB disease cases could potentially be attributed to DM, and by 2050, one in every three could potentiallybe attributed to DM
• Heterogeneity of both DM and TB-DM, interactions with HIV, other multi-morbidities?

Potential effects of TB-DM interventions
16/09/2016 12
TB Vaccination targeted at people with DM Screening and treating people with TB for DM

• English primary care data 2010-2015 (>85.000 DM patients, >150.000 controls)• Consistently higher risk of infection compared to non-DM, higher risk with higher HbA1c• 24% of TB among DM patients in UK is a result of poor glycemic control
• Critchley J, Diabetes Care 2018
Any infection Hospital after infection Death from infection
No DM
Rising HbA1c

TANDEM: DM prevalence (1856 pulmonary TB)
0
5
10
15
20
25
Indonesia Peru Romania SouthAfrica
crude
ageadjusted
country-data
0
5
10
15
20
25
Indonesia Peru Romania SouthAfrica
crude
ageadjusted
country-data
DM
pre
vale
nce
0
5
10
15
20
25
30
35
40
18-34 35-49 50+ 18-34 35-49 50+ 18-34 35-49 50+ 18-34 35-49 50+
Indonesia Peru South Africa Romania
%
Pink = newGrey = known
73% of DM previously known
(“neglected”)
TANDEM consortium, Ugarte-Gll et al; Clinical Infectious Diseases 2019 and Grint et al Bulletin of WHO 2018

or more progression to active TB?
• 651 DM patients in Indonesia
• Sex- and age-matched TB household contacts
DM patients TB household contacts
Active TB 4.9% 1.2%
Latent TB (IGRA) 38.6% 68.6%
Ratio active/latent 1:8 1:57
Koesoemadinata et al. Tr Royal Soc Trop Med H 2017

Updated systematic review –also increases risk of culture positivity at 2 months, death and failure, relapse, MDR-TB
16/09/2016 25
NOTE: Weights are from random effects analysis
Overall (I-squared = 84.2%, p = 0.000)
Touré, 2007
Pina, 2006
Viswanathan, 2014
Lin, 2014
Alisjahbana, 2007Vasankari, 2007
Dooley, 2009
Reis-Santos, 2013
Alavi-Naini, 2013
Mathew, 2006
Jiménez-Corona, 2013
Tabarsi, 2014
Kitahara, 1994
Moosazadeh, 2014
Reed, 2013Sulaiman, 2013
Chen, 2015
Chiang, 2009
Viswanathan, 2014
Burgielski, 1985
Fielder, 2002
Amnuaiphon, 2009
Study
Ambrosetti, 1997 report
Singla, 2006
Sangral, 2012
Maâlej, 2009
Alo, 2014
Tatar, 2009
Cavanaugh, 2015
Mboussa, 2003
Mi, 2013
Wang, 2009
Ribeiro Macedo, 2013
Kourbatova, 2006
Nandakumar, 2013
Ambrosetti, 1996 report
Magee, 2014
Centis, 1998 report
Oursler, 2002Centis, 1999 report
Ambrosetti, 1995 report
Wu, 2015
Orofino Rde, 2011
Bashar, 2001
Chiang, 2015
Uchimura, 2013
Vasankari, 2010
Hasibi, 2008Senegal
Spain
India
Taiwan
IndonesiaFinland
U.S.
Brazil
Iran
Russia
Mexico
Iran
Japan
Iran
R.O.K.Malaysia
China
Taiwan
India
Poland
U.S.
Thailand
Country
Italy
K.S.A
India
Tunisia
Fiji
Turkey
Kiribati
Congo
China
Taiwan
Brazil
Russia
India
Italy
U.S.
Italy
U.S.Italy
Italy
Taiwan
Brazil
U.S.
Taiwan
Japan
Finland
Iran18/86
8/73
1/89
65/182
2/9422/92
6/42
73/703
40/108
8/44
11/363
1/37
3/71
26/140
21/16219/342
9/182
52/241
0/96
38/90
13/22
376/4188
n/N
1/41
1/134
2/23
5/60
3/53
2/78
4/101
8/32
2/97
13/74
39/323
5/20
42/667
4/50
16/151
5/41
8/182/40
3/32
1645/7637
4/14
7/50
79/705
1193/5622
7/26
3/6
TB-DM
6/88
97/1438
1/120
184/565
0/54086/537
20/255
995/17047
35/607
75/1872
36/847
1/67
14/449
123/824
30/49542/914
9/944
137/886
5/149
19/90
29/152
19/290
n/N
43/666
3/384
16/257
0/82
11/335
0/78
2/174
8/100
2/483
11/143
712/12472
87/440
71/2127
19/773
66/1167
49/1059
14/10826/852
29/737
3939/26214
15/294
1/105
61/768
6282/28077
25/205
6/44
TB-nonDM
2.10 (1.76, 2.51)
3.62 (1.36, 9.62)
1.70 (0.79, 3.65)
1.35 (0.08, 21.92)
1.15 (0.81, 1.63)
29.22 (1.39, 613.44)1.65 (0.97, 2.80)
1.96 (0.74, 5.20)
1.87 (1.45, 2.40)
9.61 (5.72, 16.15)
5.32 (2.39, 11.85)
0.70 (0.35, 1.40)
1.83 (0.11, 30.19)
1.37 (0.38, 4.90)
1.30 (0.81, 2.07)
2.31 (1.28, 4.16)1.22 (0.70, 2.13)
5.40 (2.12, 13.81)
1.50 (1.05, 2.15)
0.14 (0.01, 2.49)
2.73 (1.42, 5.27)
6.13 (2.39, 15.70)
1.41 (0.87, 2.27)
Odds ratio (95% CI)
0.36 (0.05, 2.70)
0.95 (0.10, 9.26)
1.43 (0.31, 6.67)
16.35 (0.89, 301.66)
1.77 (0.48, 6.56)
5.13 (0.24, 108.62)
3.55 (0.64, 19.72)
3.83 (1.30, 11.27)
5.06 (0.70, 36.39)
2.56 (1.08, 6.03)
2.27 (1.61, 3.20)
1.35 (0.48, 3.82)
1.95 (1.32, 2.88)
3.45 (1.13, 10.56)
1.98 (1.11, 3.51)
2.86 (1.08, 7.62)
5.37 (1.81, 15.91)1.67 (0.38, 7.31)
2.53 (0.73, 8.77)
1.55 (1.46, 1.66)
7.44 (2.09, 26.51)
16.93 (2.02, 141.78)
1.46 (1.03, 2.08)
0.93 (0.87, 1.00)
2.65 (1.01, 6.94)
6.33 (1.03, 38.98)
100.00
1.91
2.47
0.37
3.89
0.313.24
1.91
4.20
3.29
2.36
2.71
0.37
1.36
3.47
3.043.15
2.00
3.87
0.34
2.81
1.99
3.44
Weight
0.66
0.53
1.03
0.34
1.30
0.31
0.86
1.69
0.68
2.20
3.91
1.77
3.74
1.61
3.09
1.91
1.681.09
1.40
4.56
1.36
0.60
3.89
4.56
1.94
0.78
%
2.10 (1.76, 2.51)
3.62 (1.36, 9.62)
1.70 (0.79, 3.65)
1.35 (0.08, 21.92)
1.15 (0.81, 1.63)
29.22 (1.39, 613.44)1.65 (0.97, 2.80)
1.96 (0.74, 5.20)
1.87 (1.45, 2.40)
9.61 (5.72, 16.15)
5.32 (2.39, 11.85)
0.70 (0.35, 1.40)
1.83 (0.11, 30.19)
1.37 (0.38, 4.90)
1.30 (0.81, 2.07)
2.31 (1.28, 4.16)1.22 (0.70, 2.13)
5.40 (2.12, 13.81)
1.50 (1.05, 2.15)
0.14 (0.01, 2.49)
2.73 (1.42, 5.27)
6.13 (2.39, 15.70)
1.41 (0.87, 2.27)
Odds ratio (95% CI)
0.36 (0.05, 2.70)
0.95 (0.10, 9.26)
1.43 (0.31, 6.67)
16.35 (0.89, 301.66)
1.77 (0.48, 6.56)
5.13 (0.24, 108.62)
3.55 (0.64, 19.72)
3.83 (1.30, 11.27)
5.06 (0.70, 36.39)
2.56 (1.08, 6.03)
2.27 (1.61, 3.20)
1.35 (0.48, 3.82)
1.95 (1.32, 2.88)
3.45 (1.13, 10.56)
1.98 (1.11, 3.51)
2.86 (1.08, 7.62)
5.37 (1.81, 15.91)1.67 (0.38, 7.31)
2.53 (0.73, 8.77)
1.55 (1.46, 1.66)
7.44 (2.09, 26.51)
16.93 (2.02, 141.78)
1.46 (1.03, 2.08)
0.93 (0.87, 1.00)
2.65 (1.01, 6.94)
6.33 (1.03, 38.98)
100.00
1.91
2.47
0.37
3.89
0.313.24
1.91
4.20
3.29
2.36
2.71
0.37
1.36
3.47
3.043.15
2.00
3.87
0.34
2.81
1.99
3.44
Weight
0.66
0.53
1.03
0.34
1.30
0.31
0.86
1.69
0.68
2.20
3.91
1.77
3.74
1.61
3.09
1.91
1.681.09
1.40
4.56
1.36
0.60
3.89
4.56
1.94
0.78
%
1.1 .5 1 2.11 5 10 15
Huangfu et al, 2019 Int J Tub Lung Dis (in press)
NOTE: Weights are from random effects analysis
Overall (I-squared = 46.7%, p = 0.095)
Dooley, 2009
Magee, 2016
Study
Reed, 2013
Wang, 2009
Mundra, 2017
Oursler, 2002
U.S.
USA
Country
R.O.K.
Taiwan
India
U.S.
6/42
10/42
n/N
21/162
13/74
./.
8/18
TB-DM
20/255
32/327
n/N
30/495
11/143
./.
14/108
TB-nonDM
2.83 (1.45, 5.52)
6.50 (1.11, 38.20)
1.19 (0.54, 2.63)
ratio (95% CI)
2.18 (1.10, 4.33)
7.60 (1.98, 29.16)
1.30 (0.16, 10.53)
6.70 (1.57, 28.67)
Odds
100.00
10.40
25.17
Weight
27.59
15.09
8.07
13.67
%
2.83 (1.45, 5.52)
6.50 (1.11, 38.20)
1.19 (0.54, 2.63)
ratio (95% CI)
2.18 (1.10, 4.33)
7.60 (1.98, 29.16)
1.30 (0.16, 10.53)
6.70 (1.57, 28.67)
Odds
100.00
10.40
25.17
Weight
27.59
15.09
8.07
13.67
%
1.1 .5 1 2.83 5 10 15
NOTE: Weights are from random effects analysis
.
.
1: High income
Ambrosetti, 1995 report
Ambrosetti, 1996 report
Ambrosetti, 1997 report
Centis, 1998 report
Centis, 1999 report
Singla, 2006
Chiang, 2009
Uchimura, 2013
Choi, 2014
Chiang, 2015
Barss, 2016
Lee, 2017
Leung, 2017
Subtotal (I-squared = 83.7%, p = 0.000)
2: Upper/Lower-middle/Low
Mboussa, 2003
Morsy, 2003
Anunnatsiri, 2005
Namukwaya, 2011
Orofino Rde, 2011
Sangral, 2012
Jimenez-Corona, 2013
Mi, 2013
Nandakumar, 2013
Tabarsi, 2014
Alo, 2014
Viswanathan, 2014
Viswanathan, 2014
Cavanaugh, 2015
Hongguang, 2015
Delgado-Sanchez, 2015
Abdelbary, 2016
Satung, 2016
Siddiqui, 2016
Workneh, 2016
Ma, 2017
Perez-Navarro, 2017
Subtotal (I-squared = 87.3%, p = 0.000)
Study
Italy
Italy
Italy
Italy
Italy
K.S.A.
Taiwan
Japan
R.O.K.
Taiwan
Canada
South Korea
Hong Kong
Congo
Egypt
Thailand
Uganda
Brazil
India
Mexico
China
India
Iran
Fiji
India
India
Kiribati
China
Mexico
Mexico
Thailand
India
Ethiopia
China
Mexico
Country
3/32
5/50
2/41
5/41
2/40
1/134
60/241
1281/5622
./.
101/705
./.
8/238
317/3206
13/32
31/40
4/38
2/2
4/14
4/23
28/363
12/97
74/667
2/37
3/53
4/96
8/89
5/101
15/182
2594/29535
136/2121
73/556
3/37
16/109
19/157
19/184
n/N
TB-DM
33/737
20/773
45/666
61/1059
28/852
7/384
161/886
6578/28077
./.
78/768
./.
31/764
1152/17488
13/100
88/198
11/188
48/148
21/294
20/257
55/847
13/483
148/2127
3/67
12/335
6/149
1/120
4/174
14/944
12131/114249
543/6310
1228/7251
12/150
56/1205
74/1156
21/325
n/N
TB-nonDM
2.21 (0.64, 7.62)
4.18 (1.50, 11.66)
0.71 (0.17, 3.03)
2.27 (0.86, 6.00)
1.55 (0.36, 6.74)
0.40 (0.05, 3.32)
1.49 (1.06, 2.09)
0.96 (0.90, 1.03)
1.78 (1.07, 2.96)
1.48 (1.08, 2.03)
3.02 (1.64, 5.56)
0.82 (0.37, 1.81)
1.56 (1.37, 1.77)
1.52 (1.17, 1.98)
4.58 (1.83, 11.43)
4.31 (1.95, 9.52)
1.89 (0.57, 6.30)
10.36 (0.49, 220.01)
5.20 (1.50, 18.00)
2.49 (0.77, 8.04)
1.20 (0.75, 1.93)
5.10 (2.25, 11.56)
1.67 (1.24, 2.24)
1.22 (0.19, 7.65)
1.62 (0.44, 5.92)
1.04 (0.28, 3.77)
11.75 (1.44, 95.78)
2.21 (0.58, 8.44)
5.97 (2.83, 12.59)
0.81 (0.78, 0.85)
0.73 (0.60, 0.88)
0.74 (0.58, 0.96)
1.01 (0.27, 3.80)
3.53 (1.95, 6.40)
2.01 (1.18, 3.43)
1.67 (0.87, 3.19)
1.90 (1.43, 2.53)
Odds ratio (95% CI)
3.46
4.59
2.68
4.95
2.63
1.40
12.38
15.45
9.84
12.73
8.43
6.42
15.03
100.00
4.37
4.93
3.29
0.78
3.16
3.39
6.55
4.81
7.38
1.84
2.99
3.01
1.49
2.88
5.15
7.99
7.72
7.53
2.93
5.93
6.24
5.65
100.00
Weight
%
2.21 (0.64, 7.62)
4.18 (1.50, 11.66)
0.71 (0.17, 3.03)
2.27 (0.86, 6.00)
1.55 (0.36, 6.74)
0.40 (0.05, 3.32)
1.49 (1.06, 2.09)
0.96 (0.90, 1.03)
1.78 (1.07, 2.96)
1.48 (1.08, 2.03)
3.02 (1.64, 5.56)
0.82 (0.37, 1.81)
1.56 (1.37, 1.77)
1.52 (1.17, 1.98)
4.58 (1.83, 11.43)
4.31 (1.95, 9.52)
1.89 (0.57, 6.30)
10.36 (0.49, 220.01)
5.20 (1.50, 18.00)
2.49 (0.77, 8.04)
1.20 (0.75, 1.93)
5.10 (2.25, 11.56)
1.67 (1.24, 2.24)
1.22 (0.19, 7.65)
1.62 (0.44, 5.92)
1.04 (0.28, 3.77)
11.75 (1.44, 95.78)
2.21 (0.58, 8.44)
5.97 (2.83, 12.59)
0.81 (0.78, 0.85)
0.73 (0.60, 0.88)
0.74 (0.58, 0.96)
1.01 (0.27, 3.80)
3.53 (1.95, 6.40)
2.01 (1.18, 3.43)
1.67 (0.87, 3.19)
1.90 (1.43, 2.53)
Odds ratio (95% CI)
3.46
4.59
2.68
4.95
2.63
1.40
12.38
15.45
9.84
12.73
8.43
6.42
15.03
100.00
4.37
4.93
3.29
0.78
3.16
3.39
6.55
4.81
7.38
1.84
2.99
3.01
1.49
2.88
5.15
7.99
7.72
7.53
2.93
5.93
6.24
5.65
100.00
Weight
%
1.2 .5 1 2 3 5 10 15

DM: worse TB outcome, more resistance
• Slower bacteriological response
• More TB treatment failure
• More TB recurrence
• More early deaths
• More MDR-TB
Tegegne Syst Rev 2018
Baker, BMC Med 2011Faruholt-Jespen, TMIH 2013Reed, Plos One 2010
Huangfu et al SR 2019
Low quality of evidence base:timing and selection for DR testingadjustment for confounders?primary versus acquired?
NOTE: Weights are from random effects analysis
Overall (I-squared = 48.0%, p = 0.011)
Subhash, 2003
Fisher-Hoch, 2008
Fisher-Hoch, 2008
Hongguang, 2015
Viswanathan, 2014
Ribeiro Macedo, 2013
Wang, 2001
Salindri, 2016
Study
Reis-Santos, 2013
Chang, 2011
Delgado-Sanchez, 2015
Bashar, 2001
Baghaei, 2016
Perez-Navarro, 2017
Perez-Navarro, 2015
Nissapatorn, 2005
Zhang, 2009
Siddiqui, 2016
Nandakumar, 2013
India
U.S.
Mexico
China
India
Brazil
Taiwan
Georgia
Country
Brazil
Taiwan
Mexico
U.S.
Iran
Mexico
Mexico
Malaysia
China
India
India
19/72
18/401
33/287
2/182
1/95
2/323
TB-DM
5/75
11/36
n/N
4/703
3/60
67/672
18/50
2/62
26/174
15/146
2/241
36/203
0/36
5/667
89/289
31/1041
79/1149
4/944
0/148
44/12472
TB-nonDM
29/376
41/232
n/N
60/17047
1/132
126/1614
10/105
0/64
16/318
5/263
4/1410
163/1938
4/150
5/2127
1.98 (1.51, 2.60)
0.81 (0.45, 1.44)
1.53 (0.85, 2.77)
1.76 (1.15, 2.70)
2.61 (0.47, 14.36)
4.71 (0.19, 116.93)
1.76 (0.42, 7.29)
0.85 (0.32, 2.28)
2.05 (0.93, 4.50)
Odds ratio (95% CI)
1.62 (0.59, 4.47)
6.89 (0.70, 67.71)
1.31 (0.96, 1.79)
5.34 (2.24, 12.76)
5.33 (0.25, 113.30)
3.32 (1.73, 6.37)
5.91 (2.10, 16.61)
2.94 (0.54, 16.15)
2.35 (1.58, 3.48)
0.45 (0.02, 8.47)
3.21 (0.93, 11.11)
100.00
8.70
8.56
10.65
2.14
0.67
2.89
%
4.97
6.52
Weight
4.76
1.27
12.21
5.79
0.74
7.86
4.64
2.14
11.11
0.79
3.56
1.98 (1.51, 2.60)
0.81 (0.45, 1.44)
1.53 (0.85, 2.77)
1.76 (1.15, 2.70)
2.61 (0.47, 14.36)
4.71 (0.19, 116.93)
1.76 (0.42, 7.29)
0.85 (0.32, 2.28)
2.05 (0.93, 4.50)
Odds ratio (95% CI)
1.62 (0.59, 4.47)
6.89 (0.70, 67.71)
1.31 (0.96, 1.79)
5.34 (2.24, 12.76)
5.33 (0.25, 113.30)
3.32 (1.73, 6.37)
5.91 (2.10, 16.61)
2.94 (0.54, 16.15)
2.35 (1.58, 3.48)
0.45 (0.02, 8.47)
3.21 (0.93, 11.11)
100.00
8.70
8.56
10.65
2.14
0.67
2.89
%
4.97
6.52
Weight
4.76
1.27
12.21
5.79
0.74
7.86
4.64
2.14
11.11
0.79
3.56
1.1 .5 1 1.98 3 5 10 15
NOTE: Weights are from random effects analysis
Overall (I-squared = 0.0%, p = 0.453)
Jimenez-Corona, 2013
Hung, 2015
Perez-Navarro, 2017
Tipayamongkholgul, 2016
Study
Lee, 2014
Mexico
Taiwan
Mexico
Thailand
Country
Taiwan
41/352
44/165
21/183
20/.
n/N
102/170
TB-DM
66/811
108/595
10/324
79/.
n/N
198/430
TB-nonDM
1.86 (1.51, 2.28)
1.76 (1.11, 2.79)
1.51 (1.04, 2.18)
1.86 (1.10, 3.14)
2.76 (1.66, 4.60)
ratio (95% CI)
1.96 (1.22, 3.15)
Odds
100.00
19.57
30.66
15.22
16.07
Weight
18.48
%
1.86 (1.51, 2.28)
1.76 (1.11, 2.79)
1.51 (1.04, 2.18)
1.86 (1.10, 3.14)
2.76 (1.66, 4.60)
ratio (95% CI)
1.96 (1.22, 3.15)
Odds
100.00
19.57
30.66
15.22
16.07
Weight
18.48
%
1 1.86 3 5

Call to Action

• Extended to become an age-structured deterministic compartmental model
• TB natural history was modulated by specific effects of having concurrent DM
Natural history of TB with
DM

Key assumptions for the DM-on-TB effects
Effect Description Effect size
Effects of DM on TB natural history (TB infection and TB disease)
Effect 1-Susceptibility DM increases susceptibility to TB infection 1.50
Effect 2-Fast progression DM increases the proportion of TB infections entering latent-fast state as opposed to latent-slow state 2.20
Effect 3-Reactivation DM increases the rate of developing TB disease among those with latent TB infection 1.00 (no effect)
Effect 4-Latent reinfection DM increases the susceptibility to TB reinfection among those with latent-slow TB infection 1.00 (no effect)
Effect 5-Smear positivity DM increases the proportion of new PTB# disease cases progressing to SP-PTB* as opposed to SN-PTB
Effect 6-Disease infectiousness
DM increases the infectiousness of PTB (SP-PTB and SN-PTB) for untreated and treated TB disease cases 1.46
Effect 7-TB mortality DM increases the hazard of TB-related mortality for untreated and treated TB disease cases 2.11
Effects of DM on TB treatment outcomes
Effect 8-Treatment failureDM reduces the proportion of successful treatment (through increased risk of treatment failure and MDR-TB)
1.00 (no effect)
Effect 9-RecoveryDM reduces the rate of TB recovery (i.e., prolongs the recovery time) for those who recover naturally or due to treatment
0.82
Effect 10-Cured reinfection DM increases susceptibility to TB reinfection among those treated or recovered from TB disease 1.80
1.25
0.67
DM role was investigated using a conservative approach whereby DM-
on-TB effect was set at its lowest likely value or set at the null value

• TB incidence and mortality rates were projected to decrease from 215 to 116 and from 40.7 to 15.7 per 100,000 population per year
• Annual number of incident and TB deaths cases were projected to decrease from 2.8 to 2.0 million and from 534,000 to 287,000
Model Fitting

DM in India
DM prevalence in India was projected to increase from 8.5% in 2017 to 12.1% in 2050

Proportion of TB incident
and mortality cases attributed to DM
TB incident cases
2017: 21.9% (95% UI: 12.1-26.4%)
2050: 33.3% (95% UI: 19.0%-44.1%)
TB-related deaths
2017: 28.9% (95% UI: 18.9%-34.1%)
2050: 42.8% (95% UI: 28.7%-53.1%)
The burgeoning DM epidemic in India was predicted to become a
leading driver of TB disease incidence and mortality over the coming
decades

Setting effect sizes of some of the effects based on best quality evidence → as much as half of TB disease cases and TB-related deaths could be attributed to DM by 2050
Could DM impact be
Underestimated?

Age-dependence of the TB-DM association also resulted in a larger impact on TB disease incidence and mortality
Age-dependence of the
TB-DM association
TB incident cases were
attributed to DM
2017: 27.9%
2050: 39.2%
TB-related deaths were attributed to DM
2017: 33.3%
2050: 45.41%

TB-DM bi-directionality resulted in a slightly larger impact on TB disease incidence and mortality
Implication of TB-DM
synergy

Different TB disease incidence trajectories over the next few decades resulted in minimal changes in the impact of DM on TB incidence and mortality
TB disease incidence
trajectories

• Exploring the TB-DM synergy implications assuming no change in the susceptibility to TB reinfection resulted in slightly larger impact for DM on TB disease incidence and mortality
• Exploring the TB-DM synergy implications assuming a 35% increase in the susceptibility to TB for reinfection, resulted in a relatively larger impact for DM on TB disease incidence and mortality
Risk of reinfection
rather than protective immunity

If young adults were assumed to be at higher risk of developing latent fast compared to older TB individuals, the impact of DM on TB disease incidence and mortality was reduced
Could DM impact be
Overestimated?
TB incident cases were
attributed to DM
2017: 12.6%
2050: 20.4%
TB-related deaths were
attributed to DM
2017: 17.7%
2050: 28.6%

Conclusions
• Currently one in every five TB disease cases is attributed to DM, and by 2050, one in every three will be attributed to DM
• DM is emerging as a leading driver of TB incidence and mortality in India, and possibly elsewhere
• Only a country-by-country approach, following the concept of “know your epidemic, know your response” for managing TB, has the potential to advance TB efforts towards TB elimination by 2050
• Intervention strategies should target DM patients before onset of TB disease, which is unfortunately more or less overlooked in the current TB strategies/guidance

• Objective 1: Develop a conceptual framework of DM effects on TB natural history and treatment outcomes, and to assess theoretically the implications of the DM effects on TB epidemiology for an improved understanding of the TB-DM synergy
• Objective 2: Quantify the effect of past and future trends in DM on TB incidence, prevalence and related deaths at the population level in a selected TB endemic country.
• Objective 3: Estimate the impact of interventions aimed at controlling TB transmission among people with DM

Clinical management of TB-DM
• TB treatment: longer? Higher dose rifampicin? TDM?
• How to attain glycemic control? Is this useful?
• More toxicity? need to monitor TB-DM more intensively?
• What explains higher mortality? Statins? Aspirin? Smoking cessation?
• Appreciate the heterogeneity of DM and TB-DM
• Need for more studies ‘beyond screening’ for TB-DM • including (pragmatic) clinical trials
• Transient hyperglycaemia – need to repeat screening tests later on in TB treatment
• WHAT HAPPENS AFTER THE END OF TB TREATMENT? [health systems development for multi-morbidity, referral to DM services]
Riza A et al, Lancet Diabetes 2016. Clinical management of concurrent TB and DMVan Crevel et al. IJTLD (in press). Clinical management of combined TB and DM

Effect of HIV on TB-DM?
16/09/2016 48
Oni et al 2017 Faurholt-Jepson 2011
Bailey et al 2016

TANDEM experience
• Variable TB-DM prevalence and phenotype across sites
• DM screening in TB pts: yes. TB screening in DM pts: maybe?
• Cost-effectiveness supports 2 step screening
• Repeated at end of treatment
• Appreciate the heterogeneity of DM / hyperglycaemia
• “Transient hyperglycaemia”: follow-up of patients (on-going, magnitude, effect on TB outcomes, prognosis…)
• Glycemic control: insulin or metformin? intensive monitoring?
• How important is glycemic control for TB outcomes?
• We should consider other treatments for DM pts (CVD risk)?
• Need for studies on clinical management of TB-DM
• Including (pragmatic) clinical trials aiming to improve joint management

Biological Plausibility• It is biologically plausible that the risk of developing DM is higher after TB disease
• Studies have shown IH and/or IGT during the early phases of active TB. Such metabolic states are linked with progression to overt DM amongst 20-50% of individuals after 3 to 5 years.
• TB disease may identify individuals at higher risk of progression to DM, as gestational DM identifies groups at high risk of progression to overt DM
• Changes in body composition during and following acute illness; limited evidence from cohort studies suggests weight re-gain during treatment could increase the proportion of body fat in recovered TB patients thus increasing future DM risk
• However, previous studies find hyperglycaemia observed amongst TB patients is intermittent, reversing after the early, acute phase of disease.
• T2DM is often undiagnosed due to the natural history of disease so misclassification bias could be occurring
• We excluded individuals <1 yr follow-up after TB diagnosis, and those developing DM within 1 year; this made little difference to the results, suggesting risk of DM among former TB patients cannot simply be a treatment effect
• Longer follow-up periods are required to fully tease out temporality

If findings are validated there are important clinical and public health implications: • Continuing health care of those with a TB history, not routinely longitudinally assessed
for DM may need to be amended• Lifetime risk of DM is already very high in many TB endemic countries; it could be highly
cost-effective to screen former TB patients at regular intervals for DM; reducing risks of complications and improving HR-QOL
• TB patients with DM also appear to be more infectious (higher bacterial load, and longer smear positivity) and experience more recurrent TB. This suggests TB patients at risk of, or already with, overt DM may be driving continued TB transmission disproportionately to their number and may require different treatment guidelines
• Whilst findings are likely of most importance for population health in high TB-DM burden countries, they may also be important among high risk groups; for example in the UK it has recently been estimated that 20% of PTB in Asian men can be statistically attributable to DM
• Co-morbid individuals: are more likely to be sputum positive, take longer to become sputum negative, have a higher risk of death or relapse.
Implications

Strengths and Weaknesses
• Cohort design and size allowing for temporal analyses and analyses by sub-type
• Inability to control for confounders due to aggregated data format• Recent analysis of UK CPRD primary care data found no effect modification from ethnicity,
age or duration of DM (Pealing). Similar findings with US NHANES data (Corris)• Low BMI is associated with TB, and high BMI with DM. TB patients also lose weight which is
rapidly regained on treatment, so single measures are not sufficient to adjust. More detailed analyses, potentially treating BMI as a time-varying exposure, are required. However, it is unlikely a 5 fold increased risk would be entirely due to residual confounding
• Loss to follow up due to migration
• Potential for Berksonian bias
• Misclassification bias

TANDEM: TB and Diabetes Mellitus
http://www.tandem-fp7.eu/

TANDEM
Aims
• Improve knowledge of the link between TB-DM
• Improve screening and management of DM among TB patients
• Impact on control of TB-DM co-morbidity
Consortium
• Multidisciplinary team of clinicians, epidemiologists and laboratory scientists
• Collaborating centres:• Indonesia• Romania• Peru• South Africa• European labs (Germany, UK,
Netherlands, Romania)

TANDEM data
• Approximately 2000 TB patients screened for DM
• Approx 150 clinical trial of increased glucose monitoring
• Strength of the study is in the breadth of data collected and longitudinal data
Data collected:
• Demographics
• Anthropometric measures
• Clinical data: family history, drugs, comorbidities
• Residential/employment status
• Range of DM glucose markers
• TB sputum smear and culture, CXR
• Smoking/alcohol intake
• Economic / Cost data (incl overheads, patient costs)
• Quality of life
• TB treatment outcomes, changes in hyperglycaemia over time

All newly diagnosed PTB patients (target n=2000)• history of DM
• Accredited Laboratory HbA1c (gold standard)
• POC HbA1c, RPG/RCG, FPG, urine dipstick,
• diabetes “risk scores” (alone/combination)
Screening TB patients for DM and DM patients for TB
6/21/201958
Feasibility, accuracy, and cost of those modalities
Previously known DM patients (target n=2000)• Symptom screen• CXR• OR clinical suspicion of TB • and followed by sputum / culture examination
•Most DM identified in TB patients was pre-existing not newly diagnosed DM

Screening TB patients for DM

Diabetes Screening
Aims
• Estimate prevalence of DM among patients presenting with PTB
• Assess the feasibility and accuracy of screening TB patients for DM and vice versa
Methods
• Crude and age-standardised prevalence estimated with exact binomial CI
• New and previously diagnosed DM included
• DM defined consistently using laboratory determined repeated HbA1c (>6.5%)

DM diagnosis in TB patients: any of these +
RPG >=6.1 mmol/l?
Yes
RPG>=11.1 mmol/l?
Yes:DM Symptoms?
Yes:
DM+
No: Take FBG
NoTake FBG.FBG>=7.0?
Yes:DM+
No: Stop
NoStop
Lab HbA1c >=6.5%
Yes
Repeat lab HbA1c>=6.5%
Yes:DM+
No:FBG >=7.0
NoStop
No: Stop
Yes:DM+

DM risk scoresFindrisc
(Age, BMI, WC, BP medication, Previous high glucose, Physical activity, Diet)
Indian Risk Score
(Age, BMI, WC, Family history, Physical activity)
Oman Risk Score
(Age, Sex, BMI, WC, Family history, Hypertension)
Full TANDEM score
• POC HbA1c
• RPG
• Age
Restricted TANDEM score
• RPG
• Age
• BMI
• Physical activity

Baseline dataIndonesia
(N=728)
Peru
(N=562)
Romania
(N=436)
South Africa
(N=259)
DM Marker N Median N Median N Median N Median
DM Cases 49 17 30 18
Age 728 36.7 562 28.8 436 41.8 259 33.7
Male 415 57.0% 328 58.4% 305 70.3% 166 64.1%
BMI 721 18.1 562 22.0 435 20.2 258 18.4
RPG 726 5.5 558 5.4 407 5.8 258 5.7
FBG 128 4.6 432 4.9 433 5.0 0
POC HbA1c 715 5.8 542 5.8 400 5.5 250 5.5
HbA1c (No DM) 679 5.6 545 5.5 406 5.8 241 5.8
HbA1c (DM Case) 49 10.7 17 7.9 30 6.7 18 6.8

Diagnostic Accuracy
Aims
• Identify the most accurate markers of DM among TB patients
• Are cheap clinical diagnostic risk scores a viable alternative to blood testing?
• Which combination of tests provides the best diagnostic accuracy?
Methods
• New DM cases defined consistently using laboratory HbA1c >6.5%
• Diagnostic accuracy assessed using AUROC, sensitivity and specificity
• Fractional polynomial functions considered for continuous predictors

Available Data
Indonesia (N=737) Peru (N=562) Romania (N=467) South Africa (N=259)
DM Marker N Median N Median N Median N Median
DM Cases 55 17 31 18
Age 737 36.9 562 28.8 467 41.9 259 33.7
BMI 731 18.1 562 22.0 466 20.2 258 18.4
RPG 735 5.5 558 5.4 432 5.8 258 5.7
FBG 132 4.6 446 4.9 463 4.9 0
POC HbA1c 724 5.8 542 5.8 407 5.5 250 5.5
Lab HbA1c (No DM) 682 5.6 545 5.5 436 5.8 241 5.8
Lab HbA1c (DM) 55 10.5 17 7.9 31 6.7 18 6.8

Overall diagnostic accuracyDM Marker AUROC (95% CI) Cut-point Sensitivity (95% CI) Specificity (95% CI)
POC HbA1c + Age 0.89 (0.86 - 0.92)
POC HbA1c 0.88 (0.85 - 0.91) ≥ 6.0 92.3 (0.9 - 100.0) 75.5 (43.1 - 92.6)
≥ 6.5 58.1 (1.6 - 99.2) 91.9 (62.9 - 98.7)
RPG + Age 0.84 (0.80 - 0.88)
RPG 0.82 (0.78 - 0.86) ≥ 6.1 76.0 (29.9 - 95.9) 66.4 (47.9 - 80.9)
FBG 0.77 (0.72 - 0.83) ≥ 6.0 47.3 (0.7 - 99.1) 91.5 (29.5 - 99.6)
Age 0.77 (0.73 - 0.80) ≥ 40 80.4 (44.1 - 95.5) 62.7 (42.3 - 79.4)
Oman Risk Score 0.76 (0.72 - 0.80) ≥ 7 82.7 (31.0 - 98.1) 58.3 (44.1 - 71.3)
Indian Risk Score 0.75 (0.71 - 0.79) ≥ 30 70.8 (38.7 - 90.3) 61.5 (46.1 - 74.9)
Findrisc Score 0.74 (0.70 - 0.79) ≥ 5 46.8 (18.0 - 77.9) 80.3 (62.7 - 90.9)
WHR 0.69 (0.64 - 0.73)
Urine Dipstick 0.68 (0.63 - 0.74) ≥ trace 32.8 (3.1 - 88.2) 98.4 (6.5 - 100.0)
BMI 0.67 (0.62 - 0.72)

Diagnostic accuracy – Stratified by country
DM Marker Cut-Point Sensitivity (%) Specificity (%) Sensitivity (%) Specificity (%)
Indonesia Peru
RPG/POC HbA1c HbA1c ≥6.5% 91.7 96.1 70.6 92.7
TANDEM Score ≥8.1 95.7 87.3 82.4 84.5
POC HbA1c ≥6.5% 91.5 87.6 88.2 81.1
RPG ≥11.1mmol/l 66.7 99.3 35.3 99.6
Romania South Africa
RPG/POC HbA1c HbA1c ≥6.5% 24.0 97.3 22.2 96.6
HbA1c ≥6.0% 40.0 87.7 22.2 90.6
TANDEM Score ≥8.1 50.0 78.4 33.3 90.5
POC HbA1c ≥6.5% 16.7 97.9 33.3 92.7
RPG ≥11.1mmol/l 15.4 98.7 11.1 99.6
FBG ≥ 5.8 mmol/l 46.7 82.4

Distribution of laboratory HbA1c in TB patients newly diagnosed with DM

Diagnostic accuracy by test and site

New DM cases confirmed with repeat HbA1c or FBG following TB treatment
DM Marker Cut-point AUROC Sensitivity (%) Specificity (%)
RPG/POC HbA1c
Combination1
POC HbA1c ≥ 6.0% 0.97 (0.92 - 1.00) 93.3 (79.2 – 99.2) 73.1 (52.2 – 88.4)
POC HbA1c ≥ 6.5% 93.8 (79.2 – 99.2) 100.0 (86.2 – 100.0)
POC HbA1c
≥ 6.2% 0.96 (0.92 – 1.0) 96.9 (83.8 - 99.9) 76.9 (56.4 – 91.0)
≥ 6.5% 93.8 (79.2 - 99.2) 92.3 (74.9 – 99.1)
≥ 7.0% 87.5 (71.0 – 96.5) 100.0 (86.8 – 100.0)
RPG 95.6 (87.6 - 99.1) 37.7 (35.5 - 39.9)
≥ 6.9mmol/l 0.87 (0.78 - 0.93) 87.7 (71.8 - 96.6) 57.7 (36.9- 76.6)
≥ 11.1mmol/l 66.7 (48.2 – 82.0) 100.0 (86.8 – 100.0)
16/09/2016 83Of the initial 121 newly diagnosed DM patients, 59 (48%) had a confirmatory test for DM following TB treatment. Of this 59, 33 had DM status confirmed by this test (56%)
These 59 patients were from Indonesia (25), Peru (3), Romania (22) and South Africa (9).

How to screen in practice? –agreement between POC & Lab HbA1c
Why “Error Grid”? Visually assess disagreement (POC & laboratory tests)
Clinically important difference
Alter clinical management of DM in TB patients
Our cut-points
6.5%: threshold for DM diagnosis
9% : pragmatic assessment of severe hyperglycaemia
New guidelines for TB-DM management 8% : changes in management might be needed (e.g. change
of medication, referral to DM services)
10% : urgent referral, hospitalisation
21/06/2019 84Huangfu et al, IUALTD 2019 (in press)

Results – individual level difference
Variables Mean(POC-Lab)
mean-2SD, mean+2SDP value
Total sample 0.15 -1.56, 1.84 <0.001
Age group <30yrs 0.19 -1.36, 1.73 Ref
30-39yrs 0.27 -1.79, 2.33 0.340
40-49yrs -0.001 -1.54, 1.54 0.017
50-59yrs 0.02 -1.39, 1.43 0.010
60yrs+ 0.13 -1.71, 1.97 0.704
Country Indonesia 0.26 -1.10, 1.62 Ref
Peru 0.55 -1.48, 2.58 <0.001
Romania -0.37 -1.47, 0.74 <0.001
South Africa -0.23 -1.70, 1.25 <0.001
Anaemia Non-anaemia 0.12 -1.58, 1.82 Ref
Mild anaemia 0.11 -1.55, 1.78 0.920
Moderate anaemia 0.20 -1.45, 1.85 0.523
Severe anaemia 1.07 -0.93, 3.06 0.038
Lab HbA1c <5.7 0.37 -1.33, 2.07 Ref
5.7-6.4 -0.11 -1.32, 1.11 0.014
6.5-8.9 -0.60 -2.16, 0.97 0.011
9+ -0.13 -3.09, 2.82 0.020
21/06/2019 85
For example, a person
with POC of 6.5% lab
HbA1c 5.0% - 7.9%
Huangfu et al, IUALTD 2019 (in press)

Pragmatic 2-step Combination
• POC HbA1c testing most accurate (and supported by TB-DM guidelines). However, it is expensive.
• Non-fasting plasma glucose (RPG) is much cheaper but with lower anticipated accuracy.
• Combining these two measurements, using RPG as an initial screen could increase diagnostic accuracy and reduce cost (by about 70% in TANDEM).
The 2-step process:• Every individual is tested with RPG
o RPG ≥11.1mmol/l is determined to be DM. No further test performed
o RPG <6.1mmol/l is determined not to be DM. No further test performed
• Everyone else is then tested with POC HbA1c
o POC HbA1c ≥6.5% is determined to be DM

Cost per case accurately diagnosed TB screening and diagnostic tests (Bandung, Indonesia)
21/06/2019 90
Diagnostic
approach
Unit
cost, US$
N people
screened
Sensitivity /
Specificity
Cost per case
accurately
diagnosed
Incremental
cost
GOLD STANDARD
Repeated HbA1c$29.10 672 1.0 / 1.0 $29.12 $14.57
RPG then GOLD
STANDARD$30.16 671 0.30 / 1.0 $34.84 $33.47
POC RPG $1.06 672 0.93 / 0.76 $1.38
Omani Risk Score
(>30)$0.7 642 0.84 / 0.57 $1.18
POC HbA1c $7.19 665 1.0 / 0.635 $11.02
RPG
POC HbA1c$8.25 671 0.923 /
0.915
$11.53 $10.15

Feasibility of DM screening• Simple point-of-care methods of
screening for DM have good diagnostic accuracy in some sites
• RPG followed by POC HbA1c maximises sensitivity / efficiency
No one-size-fits-all approach
• Diagnostic accuracy depends on undiagnosed DM disease “severity”
Why is there so much heterogeneity by country/region?
• Are national healthcare systems already finding DM cases?
• Delay in TB treatment?
• “Stress hyperglycaemia”

Cost per case accurately diagnosed TB screening and diagnostic tests (Bandung, Indonesia)
21/06/2019 104
Diagnostic
approach
Unit
cost,
US$
N people
screened
Sensitivity /
Specificity
N
needing
confirmat
ory tests
Cost per case
accurately
diagnosed
Incremental
cost
GOLD STANDARD
(smear +culture)$45.66 112 0.56 / 1.0 5 $47.99 $34.01
Symptom Screen $2.07 809 0.91 / 0.55 370 $3.74
CXR $17.51 802 0.91 / 0.90 57 $19.42
Stepped
symptoms then
two ZN smears
£14.98 809 0.273 / 0.998 4 $17.93 $14.20
Stepped
symptoms then
CXR
$23.95 809 0.82 / 0.94 57 $23.95 $20.22

Feasibility of Bi-Directional TB-DM ScreeningScreening for DM among TB
• Prevalence >10% in each setting
• Prevalence >30% in those aged 50+
• Associations with BMI and family history of DM
• 2 step combinations (RPG, HbA1c) may be feasible and most cost-effective
• Heterogeneity between sites
• Repeat screening at end of TB treatment to confirm diagnosis
Screening for TB among DM
• Prevalence of 1% for probably/definite TB
• Prevalence of 3-16% for any previous/current occurrence of TB
• Associations with longer duration of DM and education level

Further work / Unanswered questions• Describe the degree of transient hyperglycaemia & its associations with TB
outcomes and longer term outcomes (where possible) • Co-morbidities• Age• Initial FBG
• Altering cut-points (data driven) in places where algorithms performed less well (Romania)
• HbA1c and FPG – patient characteristics, associations with longer term outcomes

TANDEM experience
• Variable TB-DM prevalence and phenotype across sites
• DM screening in TB pts: yes. TB screening in DM pts: maybe?
• Cost-effectiveness supports 2 step screening
• Repeated at end of treatment
• Appreciate the heterogeneity of DM / hyperglycaemia
• “Transient hyperglycaemia”: follow-up of patients (on-going, magnitude, effect on TB outcomes, prognosis…)
• Glycemic control: insulin or metformin? intensive monitoring?
• How important is glycemic control for TB outcomes?
• We should consider other treatments for DM pts (CVD risk)?
• Need for studies on clinical management of TB-DM
• Including (pragmatic) clinical trials aiming to improve joint management

TANDEM Sites
Indonesia Peru

TANDEM Sites
Romania South Africa

113
Thanks to all the members of TANDEM, all the field staff and patients
• Bandung: Bachti Alisjabana, Rovina Ruslami, Raspati Koesoemadinata
• Craiova: Mihai Ioana, Nicolae Panduru, Anca Riza
• Lima: Cesar Ugarte-Gill• Stellenbosch: Katharina
Ronacher, Gerhard Walzl, Stephane Malherbe
• Nijmegen: Reinout van Crevel• Otago: Philip Hill, Sue
McAllister• St Georges London: Julia
Critchley, Sarah Kerry, Daniel Grint, Fiona Pearson
• LSHTM: Dave Moore, Ulla Griffiths, Yoko Laurence, Hazel Dockrell

TANDEM Funding
114
TANDEM: Tuberculosis and Diabetes Mellituswww.tandem-fp7.eu

Diagnostic Accuracy
Aims
• Identify the most accurate markers of DM among TB patients
• Are cheap clinical diagnostic risk scores a viable alternative to blood testing?
• Which combination of tests provides the best diagnostic accuracy?
Methods
• New DM cases defined consistently using laboratory HbA1c >6.5%
• Diagnostic accuracy assessed using AUROC, sensitivity and specificity
• Fractional polynomial functions considered for continuous predictors

Available Data
Indonesia (N=737) Peru (N=562) Romania (N=467) South Africa (N=259)
DM Marker N Median N Median N Median N Median
DM Cases 55 17 31 18
Age 737 36.9 562 28.8 467 41.9 259 33.7
BMI 731 18.1 562 22.0 466 20.2 258 18.4
RPG 735 5.5 558 5.4 432 5.8 258 5.7
FBG 132 4.6 446 4.9 463 4.9 0
POC HbA1c 724 5.8 542 5.8 407 5.5 250 5.5
Lab HbA1c (No DM) 682 5.6 545 5.5 436 5.8 241 5.8
Lab HbA1c (DM) 55 10.5 17 7.9 31 6.7 18 6.8

Overall diagnostic accuracyDM Marker AUROC (95% CI) Cut-point Sensitivity (95% CI) Specificity (95% CI)
POC HbA1c + Age 0.89 (0.86 - 0.92)
POC HbA1c 0.88 (0.85 - 0.91) ≥ 6.0 92.3 (0.9 - 100.0) 75.5 (43.1 - 92.6)
≥ 6.5 58.1 (1.6 - 99.2) 91.9 (62.9 - 98.7)
RPG + Age 0.84 (0.80 - 0.88)
RPG 0.82 (0.78 - 0.86) ≥ 6.1 76.0 (29.9 - 95.9) 66.4 (47.9 - 80.9)
FBG 0.77 (0.72 - 0.83) ≥ 6.0 47.3 (0.7 - 99.1) 91.5 (29.5 - 99.6)
Age 0.77 (0.73 - 0.80) ≥ 40 80.4 (44.1 - 95.5) 62.7 (42.3 - 79.4)
Oman Risk Score 0.76 (0.72 - 0.80) ≥ 7 82.7 (31.0 - 98.1) 58.3 (44.1 - 71.3)
Indian Risk Score 0.75 (0.71 - 0.79) ≥ 30 70.8 (38.7 - 90.3) 61.5 (46.1 - 74.9)
Findrisc Score 0.74 (0.70 - 0.79) ≥ 5 46.8 (18.0 - 77.9) 80.3 (62.7 - 90.9)
WHR 0.69 (0.64 - 0.73)
Urine Dipstick 0.68 (0.63 - 0.74) ≥ trace 32.8 (3.1 - 88.2) 98.4 (6.5 - 100.0)
BMI 0.67 (0.62 - 0.72)

Diagnostic accuracy – Stratified by country
DM Marker Cut-Point Sensitivity (%) Specificity (%) Sensitivity (%) Specificity (%)
Indonesia Peru
RPG/POC HbA1c HbA1c ≥6.5% 91.7 96.1 70.6 92.7
TANDEM Score ≥8.1 95.7 87.3 82.4 84.5
POC HbA1c ≥6.5% 91.5 87.6 88.2 81.1
RPG ≥11.1mmol/l 66.7 99.3 35.3 99.6
Romania South Africa
RPG/POC HbA1c HbA1c ≥6.5% 24.0 97.3 22.2 96.6
HbA1c ≥6.0% 40.0 87.7 22.2 90.6
TANDEM Score ≥8.1 50.0 78.4 33.3 90.5
POC HbA1c ≥6.5% 16.7 97.9 33.3 92.7
RPG ≥11.1mmol/l 15.4 98.7 11.1 99.6
FBG ≥ 5.8 mmol/l 46.7 82.4

Diagnostic accuracy by test and site

Diagnostic accuracy – Romania/RSA
DM Marker AUROC (95% CI) Cut-point Sensitivity (95% CI) Specificity (95% CI)
RPG/POC HbA1c 2-step HbA1c ≥ 6.0 49.2 (36.4 - 62.1) 88.0 (85.4 - 90.3)
HbA1c ≥ 6.5 27.0 (16.6 - 39.7) 94.2 (92.3 - 95.8)
POC HbA1c + Age 0.80 (0.75 - 0.86)
RPG + Age 0.78 (0.72 - 0.84)
Age 0.76 (0.70 - 0.82) ≥ 40 81.5 (70.0 - 90.1) 62.6 (59.0 - 66.1)
Oman Risk Score 0.70 (0.63 - 0.77) ≥ 7 81.5 (70.0 - 90.1) 57.6 (54.0 - 61.2)
POC HbA1c 0.69 (0.62 - 0.76) ≥ 6.0 55.6 (42.5 - 68.1) 71.9 (68.4 - 75.1)
≥ 6.5 27.0 (16.6 - 39.7) 87.7 (85.1 - 90.0)
Indian Risk Score 0.68 (0.62 - 0.74) ≥ 30 64.6 (51.8 - 76.1) 62.2 (58.6 - 65.7)
RPG 0.68 (0.60 - 0.76) ≥ 6.1 65.1 (52.0 - 76.7) 63.6 (60.0 - 67.1)
≥ 6.5 55.6 (42.5 - 68.1) 73.5 (70.1 - 76.6)
FBG 0.66 (0.57 - 0.74) ≥ 6.0 35.9 (24.3 - 48.9) 89.0 (86.4 - 91.3)
Urine Dipstick 0.63 (0.55 - 0.71) ≥ trace 29.4 (15.1 - 47.5) 96.7 (94.9 - 98.0)

Pragmatic 2-step Combination• It is anticipated that POC HbA1c testing will be the most
accurate. However, it is expensive. Non-fasting plasma glucose (RPG) is much cheaper but with lower anticipated accuracy.
• Combining these two measurements, using RPG as an initial screen could increase diagnostic accuracy and reduce cost (by about 70% in TANDEM).
The 2-step process:• Every individual is tested with RPG
o RPG ≥11.1mmol/l is determined to be DM. No further test performed
o RPG <6.1mmol/l is determined not to be DM. No further test performed
• Everyone else is then tested with POC HbA1c
o POC HbA1c ≥6.5% is determined to be DM

Distribution of laboratory HbA1c (new DM)

New and previous DM

Effects of DM on TB treatment outcomes: systematic review and meta-analysis
Peijue Huangfu, Cesar Ugarte
134

Systematic Review of TB outcomes amongst those with DM
• 2011 review (33 studies): suggested diabetes worsens the treatmentoutcomes among TB patients [Baker et al. 2011]
• Included studies: relatively poor in quality (observational data)
• Modest effect size (RR for death or treatment failure - 1.69, 95% CI 1.36 to 2.12), possibly influenced by publication bias, study quality (e.g. little control of confounding; only 4 of 33 studies attempted any adjustment!)
• 2011-2015, many more studies have emerged—some better designed
• Aim: update this systematic review, assess effects of study quality on outcomes and over time
135

Method
• Databases 1980-2015: PubMed, EMBASE and regional databases (e.g.LILACS and WHO Regional libraries, Cochrane Libraries)
• Comprehensive search including terms for outcomes and exposure• TB AND DM
• TB AND Risk factors OR Treatment Outcomes [and synonyms]
• Reduce risk of bias from identifying only studies which mention diabetes in the title or abstract [or MeSH headings]
136

Methods• Outcomes (WHO guidelines):
• 1. Failure and death
• 2. Death
• 3. Relapse
• 4. Recurrence
• 5. Multi-drug resistant TB (MDRTB)
• Inclusion criteria: all cohort and case-control studies (all languages)
• Exclusion criteria: severely ill patients and MDRTB at baseline
• Data extraction:
• Study design
• Study characteristics
• Key treatment outcomes
• Aspects of study quality137

Statistical analyses
• Random effects meta-analysis due to expected heterogeneity
• Subgroup analysesControl of confounding
Study designs
Diabetes definition
138

Study selection process
139
Records screened(n= 12611)
Full-text articles assessed for eligibility
(n=355)
Records excluded(n= 12256)
Studies included in qualitative and
quantitative syntheses(n=90)
Full-text articles excluded (n=267)
• case series (n=4)• review article (n=8)• Letter to editor (n=3)• No DM exposure comparator (n=90)• Editorial (n=2)• No standard TB treatment popn
(n=14)• Conference abstract (n=29)• Not available for abstraction (n=66)• Patients with severe conditions (n=6)• No TB treatment recorded (n=45)
Scre
enin
gEl
igib
ility
Incl
usi
on

Results- 1. Death
140
48 unadjusted studies: diabetes doubled the risk of death among DM-TB patients4 adjusted studies: 4 times the risk of deathamong DM-TB patients
Overall (I-squared = 62.7%, p = 0.045)
Reed, 2013
Study
Wang, 2009
Oursler, 2002
Dooley, 2009
R.O.K.
Country
Taiwan
U.S.
U.S.
21/162
n/N
13/74
TB-DM
8/18
6/42
30/495
n/N
11/143
TB-nonDM
14/108
20/255
4.04 (2.70, 6.05)
2.18 (1.21, 3.93)
ratio (95% CI)
7.60 (3.22, 17.93)
Odds
6.70 (2.26, 19.85)
6.50 (2.45, 17.27)
100.00
47.02
Weight
22.11
%
13.81
17.05
4.04 (2.70, 6.05)
2.18 (1.21, 3.93)
ratio (95% CI)
7.60 (3.22, 17.93)
Odds
6.70 (2.26, 19.85)
6.50 (2.45, 17.27)
100.00
47.02
Weight
22.11
%
13.81
17.05
11 2 4.04 6 15 30

NOTE: Weights are from random effects analysis
Overall (I-squared = 79.1%, p = 0.000)
Chen, 2015
Viswanathan, 2014
Orofino Rde, 2011
Singla, 2006
Ambrosetti, 1996 report
Chiang, 2015
Morsy, 2003
Study
Mboussa, 2003
Anunnatsiri, 2005
Ambrosetti, 1997 report
Jiménez-Corona, 2013
Cavanaugh, 2015
Nandakumar, 2013
Namukwaya, 2011
Choi, 2014
Mi, 2013
Viswanathan, 2014
Centis, 1999 report
Chiang, 2009
Tabarsi, 2014
Centis, 1998 report
Sangral, 2012
Uchimura, 2013
Ambrosetti, 1995 report
Alo, 2014
China
India
Brazil
K.S.A.
Italy
Taiwan
Egypt
Country
Congo
Thailand
Italy
Mexico
Kiribati
India
Uganda
R.O.K.
China
India
Italy
Taiwan
Iran
Italy
India
Japan
Italy
Fiji
15/182
8/89
4/14
1/134
5/50
101/705
31/40
n/N
13/32
4/38
2/41
TB-DM
28/363
5/101
74/667
2/2
./.
12/97
4/96
2/40
60/241
2/37
5/41
4/23
1281/5622
3/32
3/53
14/944
1/120
21/294
7/384
20/773
78/768
88/198
n/N
13/100
11/188
45/666
TB-nonDM
55/847
4/174
148/2127
48/148
./.
13/483
6/149
28/852
161/886
3/67
61/1059
20/257
6578/28077
33/737
12/335
2.08 (1.58, 2.74)
5.97 (2.83, 12.59)
11.75 (1.44, 95.78)
5.20 (1.50, 18.00)
0.40 (0.05, 3.32)
4.18 (1.50, 11.66)
1.48 (1.08, 2.03)
4.31 (1.95, 9.52)
Odds ratio (95% CI)
4.58 (1.83, 11.43)
1.89 (0.57, 6.30)
0.71 (0.17, 3.03)
1.20 (0.75, 1.93)
2.21 (0.58, 8.44)
1.67 (1.24, 2.24)
10.36 (0.49, 220.01)
1.78 (1.09, 2.92)
5.10 (2.25, 11.56)
1.04 (0.28, 3.77)
1.55 (0.36, 6.74)
1.49 (1.06, 2.09)
1.22 (0.19, 7.65)
2.27 (0.86, 6.00)
2.49 (0.77, 8.04)
0.96 (0.90, 1.03)
2.21 (0.64, 7.62)
1.62 (0.44, 5.92)
100.00
5.02
1.42
3.04
1.41
3.78
7.19
4.79
Weight
4.23
3.16
2.48
%
6.44
2.76
7.28
0.74
6.33
4.67
2.89
2.43
7.09
1.75
4.00
3.26
7.90
3.05
2.87
2.08 (1.58, 2.74)
5.97 (2.83, 12.59)
11.75 (1.44, 95.78)
5.20 (1.50, 18.00)
0.40 (0.05, 3.32)
4.18 (1.50, 11.66)
1.48 (1.08, 2.03)
4.31 (1.95, 9.52)
Odds ratio (95% CI)
4.58 (1.83, 11.43)
1.89 (0.57, 6.30)
0.71 (0.17, 3.03)
1.20 (0.75, 1.93)
2.21 (0.58, 8.44)
1.67 (1.24, 2.24)
10.36 (0.49, 220.01)
1.78 (1.09, 2.92)
5.10 (2.25, 11.56)
1.04 (0.28, 3.77)
1.55 (0.36, 6.74)
1.49 (1.06, 2.09)
1.22 (0.19, 7.65)
2.27 (0.86, 6.00)
2.49 (0.77, 8.04)
0.96 (0.90, 1.03)
2.21 (0.64, 7.62)
1.62 (0.44, 5.92)
100.00
5.02
1.42
3.04
1.41
3.78
7.19
4.79
Weight
4.23
3.16
2.48
%
6.44
2.76
7.28
0.74
6.33
4.67
2.89
2.43
7.09
1.75
4.00
3.26
7.90
3.05
2.87
1.2 .5 1 2.08 3 5 10 15
Results- 2. Failure and death
141
25 studies: 2 times the risk of treatment failure and death among DM-TB patients. 6 adjusted studies: 5 times the risk of treatment failure and death among DM-TB patients
Overall (I-squared = 57.7%, p = 0.037)
Wang, 2009
Study
Anunnatsiri, 2005
Morsy, 2003
Dooley, 2009
Oursler, 2002
Reed, 2013
Taiwan
Country
Thailand
Egypt
U.S.
U.S.
R.O.K.
13/74
n/N
4/38
31/40
6/42
8/18
TB-DM
21/162
11/143
n/N
11/188
88/198
20/255
14/108
TB-nonDM
30/495
4.96 (3.52, 7.00)
7.60 (3.22, 17.93)
ratio (95% CI)
7.20 (2.16, 23.95)
9.32 (4.22, 20.60)
6.50 (2.45, 17.27)
6.70 (2.26, 19.85)
Odds
2.18 (1.21, 3.93)
100.00
16.12
Weight
8.22
18.87
12.43
10.07
%
34.28
4.96 (3.52, 7.00)
7.60 (3.22, 17.93)
ratio (95% CI)
7.20 (2.16, 23.95)
9.32 (4.22, 20.60)
6.50 (2.45, 17.27)
6.70 (2.26, 19.85)
Odds
2.18 (1.21, 3.93)
100.00
16.12
Weight
8.22
18.87
12.43
10.07
%
34.28
11 2 4.96 8 15 30

Results- 3. Relapse/Recurrence
16/09/2016 142
Diabetes associated with 2 fold increased risk of TB relapse
NOTE: Weights are from random effects analysis
Overall (I-squared = 55.8%, p = 0.007)
Wang, 2015
Study
Jiménez-Corona, 2013
Mboussa, 2003
Bashar, 2001
Pérez-Navarro, 2011
Maâlej, 2009
Zhang, 2009
Lee, 2014
Fisher-Hoch, 2008
Singla, 2006
De Oliveira, 2000
Wada, 2000
El Sahly, 2004
Taiwan
Country
Mexico
Congo
U.S.
Mexico
Tunisia
China
Taiwan
U.S.
K.S.A.
Brazil
Japan
U.S.
279/12688
n/N
41/352
6/32
10/50
./.
4/55
33/165
102/170
23/401
2/130
6/11
7/61
10/42
TB-DM
597/43195
n/N
66/811
9/100
4/105
./.
1/82
9/170
198/430
52/1041
3/367
50/150
4/284
76/302
TB-nonDM
1.80 (1.40, 2.30)
1.60 (1.39, 1.85)
ratio (95% CI)
1.49 (0.99, 2.25)
2.33 (0.76, 7.16)
6.31 (1.87, 21.30)
1.22 (0.83, 1.79)
6.35 (0.69, 58.44)
4.47 (2.07, 9.68)
1.76 (1.23, 2.52)
1.16 (0.70, 1.92)
1.90 (0.31, 11.47)
2.40 (0.70, 8.25)
9.07 (2.57, 32.07)
0.93 (0.44, 1.98)
Odds
100.00
18.39
Weight
12.76
3.94
3.45
13.43
1.18
6.79
13.88
10.85
1.74
3.37
3.24
6.98
%
1.80 (1.40, 2.30)
1.60 (1.39, 1.85)
ratio (95% CI)
1.49 (0.99, 2.25)
2.33 (0.76, 7.16)
6.31 (1.87, 21.30)
1.22 (0.83, 1.79)
6.35 (0.69, 58.44)
4.47 (2.07, 9.68)
1.76 (1.23, 2.52)
1.16 (0.70, 1.92)
1.90 (0.31, 11.47)
2.40 (0.70, 8.25)
9.07 (2.57, 32.07)
0.93 (0.44, 1.98)
Odds
100.00
18.39
Weight
12.76
3.94
3.45
13.43
1.18
6.79
13.88
10.85
1.74
3.37
3.24
6.98
%
1.5 1 1.8 5 10 15

143
NOTE: Weights are from random effects analysis
Overall (I-squared = 48.8%, p = 0.020)
Fisher-Hoch, 2008
Chang, 2011
Subhash, 2003
Viswanathan, 2014
Nandakumar, 2013
Study
Ribeiro Macedo, 2013
Fisher-Hoch, 2008
Reis-Santos, 2013
Chen, 2015
Nissapatorn, 2005
Zhang, 2009
Wang, 2001
Perez-Navarro, 2015
Bashar, 2001
U.S.
Taiwan
India
India
India
Country
Brazil
Mexico
Brazil
China
Malaysia
China
Taiwan
Mexico
U.S.
18/401
3/60
19/72
1/95
5/667
TB-DM
n/N
2/323
33/287
4/703
2/182
2/241
36/203
5/75
15/146
18/50
31/1041
1/132
89/289
0/148
5/2127
TB-nonDM
n/N
44/12472
79/1149
60/17047
4/944
4/1410
163/1938
29/376
5/263
10/105
2.04 (1.45, 2.85)
1.53 (0.85, 2.77)
6.89 (0.70, 67.71)
0.81 (0.45, 1.44)
4.71 (0.19, 116.93)
3.21 (0.93, 11.11)
Odds ratio (95% CI)
1.76 (0.42, 7.29)
1.76 (1.15, 2.70)
1.62 (0.59, 4.47)
2.61 (0.47, 14.36)
2.94 (0.54, 16.15)
2.35 (1.58, 3.48)
0.85 (0.32, 2.28)
5.91 (2.10, 16.61)
5.34 (2.24, 12.76)
100.00
11.67
1.93
11.84
1.03
5.22
%
Weight
4.28
14.11
6.85
3.20
3.21
14.63
7.13
6.69
8.21
2.04 (1.45, 2.85)
1.53 (0.85, 2.77)
6.89 (0.70, 67.71)
0.81 (0.45, 1.44)
4.71 (0.19, 116.93)
3.21 (0.93, 11.11)
Odds ratio (95% CI)
1.76 (0.42, 7.29)
1.76 (1.15, 2.70)
1.62 (0.59, 4.47)
2.61 (0.47, 14.36)
2.94 (0.54, 16.15)
2.35 (1.58, 3.48)
0.85 (0.32, 2.28)
5.91 (2.10, 16.61)
5.34 (2.24, 12.76)
100.00
11.67
1.93
11.84
1.03
5.22
%
Weight
4.28
14.11
6.85
3.20
3.21
14.63
7.13
6.69
8.21
1.1 .5 1 2.04 3 5 10 15
Results- 4. MDR-TB
Diabetes associated with 2 fold increased risk of MDR-TB

144
NOTE: Weights are from random effects analysis
.
.
1: Medical/self-reported
Burgielski, 1985
Kitahara, 1994
Ambrosetti, 1995 report
Ambrosetti, 1996 report
Ambrosetti, 1997 report
Centis, 1998 report
Bashar, 2001
Fielder, 2002
Centis, 1999 report
Oursler, 2002
Mathew, 2006
Pina, 2006
Kourbatova, 2006
Vasankari, 2007
Hasibi, 2008
Amnuaiphon, 2009
Maâlej, 2009
Chiang, 2009
Vasankari, 2010
Orofino Rde, 2011
Sangral, 2012
Jiménez-Corona, 2013
Sulaiman, 2013
Reis-Santos, 2013
Ribeiro Macedo, 2013
Magee, 2014
Moosazadeh, 2014
Lin, 2014
Wu, 2015
Chiang, 2015
Subtotal (I-squared = 54.6%, p = 0.000)
2: Blood glucose
Mboussa, 2003
Singla, 2006
Alisjahbana, 2007
Touré, 2007
Dooley, 2009
Wang, 2009
Tatar, 2009
Uchimura, 2013
Mi, 2013
Alavi-Naini, 2013
Reed, 2013
Nandakumar, 2013
Tabarsi, 2014
Alo, 2014
Viswanathan, 2014
Viswanathan, 2014
Cavanaugh, 2015
Chen, 2015
Subtotal (I-squared = 87.8%, p = 0.000)
Study
Poland
Japan
Italy
Italy
Italy
Italy
U.S.
U.S.
Italy
U.S.
Russia
Spain
Russia
Finland
Iran
Thailand
Tunisia
Taiwan
Finland
Brazil
India
Mexico
Malaysia
Brazil
Brazil
U.S.
Iran
Taiwan
Taiwan
Taiwan
Congo
K.S.A
Indonesia
Senegal
U.S.
Taiwan
Turkey
Japan
China
Iran
R.O.K.
India
Iran
Fiji
India
India
Kiribati
China
Country
38/90
3/71
3/32
4/50
1/41
5/41
7/50
13/22
2/40
8/18
8/44
8/73
5/20
22/92
3/6
376/4188
5/60
52/241
7/26
4/14
2/23
11/363
19/342
73/703
39/323
16/151
26/140
65/182
1645/7637
79/705
8/32
1/134
2/94
18/86
6/42
13/74
2/78
1193/5622
2/97
40/108
21/162
42/667
1/37
3/53
0/96
1/89
4/101
9/182
n/N
TB-DM
19/90
14/449
29/737
19/773
43/666
49/1059
1/105
29/152
26/852
14/108
75/1872
97/1438
87/440
86/537
6/44
19/290
0/82
137/886
25/205
15/294
16/257
36/847
42/914
995/17047
712/12472
66/1167
123/824
184/565
3939/26214
61/768
8/100
3/384
0/540
6/88
20/255
11/143
0/78
6282/28077
2/483
35/607
30/495
71/2127
1/67
11/335
5/149
1/120
2/174
9/944
n/N
TB-nonDM
2.73 (1.42, 5.27)
1.37 (0.38, 4.90)
2.53 (0.73, 8.77)
3.45 (1.13, 10.56)
0.36 (0.05, 2.70)
2.86 (1.08, 7.62)
16.93 (2.02, 141.78)
6.13 (2.39, 15.70)
1.67 (0.38, 7.31)
5.37 (1.81, 15.91)
5.32 (2.39, 11.85)
1.70 (0.79, 3.65)
1.35 (0.48, 3.82)
1.65 (0.97, 2.80)
6.33 (1.03, 38.98)
1.41 (0.87, 2.27)
16.35 (0.89, 301.66)
1.50 (1.05, 2.15)
2.65 (1.01, 6.94)
7.44 (2.09, 26.51)
1.43 (0.31, 6.67)
0.70 (0.35, 1.40)
1.22 (0.70, 2.13)
1.87 (1.45, 2.40)
2.27 (1.61, 3.20)
1.98 (1.11, 3.51)
1.30 (0.81, 2.07)
1.15 (0.81, 1.63)
1.55 (1.46, 1.66)
1.46 (1.03, 2.08)
1.83 (1.56, 2.13)
3.83 (1.30, 11.27)
0.95 (0.10, 9.26)
29.22 (1.39, 613.44)
3.62 (1.36, 9.62)
1.96 (0.74, 5.20)
2.56 (1.08, 6.03)
5.13 (0.24, 108.62)
0.93 (0.87, 1.00)
5.06 (0.70, 36.39)
9.61 (5.72, 16.15)
2.31 (1.28, 4.16)
1.95 (1.32, 2.88)
1.83 (0.11, 30.19)
1.77 (0.48, 6.56)
0.14 (0.01, 2.49)
1.35 (0.08, 21.92)
3.55 (0.64, 19.72)
5.40 (2.12, 13.81)
2.65 (1.55, 4.52)
Odds ratio (95% CI)
3.59
1.30
1.35
1.62
0.56
2.01
0.51
2.14
1.00
1.70
2.74
2.94
1.83
4.61
0.68
5.16
0.28
6.56
2.07
1.30
0.93
3.39
4.39
7.96
6.74
4.23
5.26
6.64
9.87
6.64
100.00
6.66
3.45
2.31
6.99
6.99
7.39
2.30
9.11
4.07
8.40
8.22
8.70
2.60
5.89
2.47
2.63
4.71
7.12
100.00
Weight
%
2.73 (1.42, 5.27)
1.37 (0.38, 4.90)
2.53 (0.73, 8.77)
3.45 (1.13, 10.56)
0.36 (0.05, 2.70)
2.86 (1.08, 7.62)
16.93 (2.02, 141.78)
6.13 (2.39, 15.70)
1.67 (0.38, 7.31)
5.37 (1.81, 15.91)
5.32 (2.39, 11.85)
1.70 (0.79, 3.65)
1.35 (0.48, 3.82)
1.65 (0.97, 2.80)
6.33 (1.03, 38.98)
1.41 (0.87, 2.27)
16.35 (0.89, 301.66)
1.50 (1.05, 2.15)
2.65 (1.01, 6.94)
7.44 (2.09, 26.51)
1.43 (0.31, 6.67)
0.70 (0.35, 1.40)
1.22 (0.70, 2.13)
1.87 (1.45, 2.40)
2.27 (1.61, 3.20)
1.98 (1.11, 3.51)
1.30 (0.81, 2.07)
1.15 (0.81, 1.63)
1.55 (1.46, 1.66)
1.46 (1.03, 2.08)
1.83 (1.56, 2.13)
3.83 (1.30, 11.27)
0.95 (0.10, 9.26)
29.22 (1.39, 613.44)
3.62 (1.36, 9.62)
1.96 (0.74, 5.20)
2.56 (1.08, 6.03)
5.13 (0.24, 108.62)
0.93 (0.87, 1.00)
5.06 (0.70, 36.39)
9.61 (5.72, 16.15)
2.31 (1.28, 4.16)
1.95 (1.32, 2.88)
1.83 (0.11, 30.19)
1.77 (0.48, 6.56)
0.14 (0.01, 2.49)
1.35 (0.08, 21.92)
3.55 (0.64, 19.72)
5.40 (2.12, 13.81)
2.65 (1.55, 4.52)
Odds ratio (95% CI)
3.59
1.30
1.35
1.62
0.56
2.01
0.51
2.14
1.00
1.70
2.74
2.94
1.83
4.61
0.68
5.16
0.28
6.56
2.07
1.30
0.93
3.39
4.39
7.96
6.74
4.23
5.26
6.64
9.87
6.64
100.00
6.66
3.45
2.31
6.99
6.99
7.39
2.30
9.11
4.07
8.40
8.22
8.70
2.60
5.89
2.47
2.63
4.71
7.12
100.00
Weight
%
1.2 .5 1 2 3 5 10 15 20
Subgroup analyses: death(medical records/self-reported - equivalent to previously diagnosed diabetes surrogate measures e.g. blood glucose, HbA1c includes previously diagnosed and newly diagnosed DM)
The association was stronger amongst studies using surrogate DM measures

16/09/2016 145NOTE: Weights are from random effects analysis
.
.
1: High incomeBurgielski, 1985Kitahara, 1994Ambrosetti, 1995 reportAmbrosetti, 1996 reportAmbrosetti, 1997 reportCentis, 1998 reportBashar, 2001Fielder, 2002Centis, 1999 reportOursler, 2002Mathew, 2006Pina, 2006Singla, 2006Kourbatova, 2006Vasankari, 2007Dooley, 2009Wang, 2009Chiang, 2009Vasankari, 2010Uchimura, 2013Reed, 2013Magee, 2014Lin, 2014Wu, 2015Chiang, 2015Subtotal (I-squared = 86.4%, p = 0.000)
2: Upper/Lower-middle/LowMboussa, 2003Alisjahbana, 2007Touré, 2007Hasibi, 2008Amnuaiphon, 2009Maâlej, 2009Tatar, 2009Orofino Rde, 2011Sangral, 2012Jiménez-Corona, 2013Mi, 2013Alavi-Naini, 2013Sulaiman, 2013Nandakumar, 2013Reis-Santos, 2013Ribeiro Macedo, 2013Tabarsi, 2014Alo, 2014Viswanathan, 2014Viswanathan, 2014Moosazadeh, 2014Cavanaugh, 2015Chen, 2015Subtotal (I-squared = 71.0%, p = 0.000)
Study
PolandJapanItalyItalyItalyItalyU.S.U.S.ItalyU.S.RussiaSpainK.S.ARussiaFinlandU.S.TaiwanTaiwanFinlandJapanR.O.K.U.S.TaiwanTaiwanTaiwan
CongoIndonesiaSenegalIranThailandTunisiaTurkeyBrazilIndiaMexicoChinaIranMalaysiaIndiaBrazilBrazilIranFijiIndiaIndiaIranKiribatiChina
Country
38/903/713/324/501/415/417/5013/222/408/188/448/731/1345/2022/926/4213/7452/2417/261193/562221/16216/15165/1821645/763779/705
8/322/9418/863/6376/41885/602/784/142/2311/3632/9740/10819/34242/66773/70339/3231/373/530/961/8926/1404/1019/182
n/NTB-DM
19/9014/44929/73719/77343/66649/10591/10529/15226/85214/10875/187297/14383/38487/44086/53720/25511/143137/88625/2056282/2807730/49566/1167184/5653939/2621461/768
8/1000/5406/886/4419/2900/820/7815/29416/25736/8472/48335/60742/91471/2127995/17047712/124721/6711/3355/1491/120123/8242/1749/944
n/NTB-nonDM
2.73 (1.42, 5.27)1.37 (0.38, 4.90)2.53 (0.73, 8.77)3.45 (1.13, 10.56)0.36 (0.05, 2.70)2.86 (1.08, 7.62)16.93 (2.02, 141.78)6.13 (2.39, 15.70)1.67 (0.38, 7.31)5.37 (1.81, 15.91)5.32 (2.39, 11.85)1.70 (0.79, 3.65)0.95 (0.10, 9.26)1.35 (0.48, 3.82)1.65 (0.97, 2.80)1.96 (0.74, 5.20)2.56 (1.08, 6.03)1.50 (1.05, 2.15)2.65 (1.01, 6.94)0.93 (0.87, 1.00)2.31 (1.28, 4.16)1.98 (1.11, 3.51)1.15 (0.81, 1.63)1.55 (1.46, 1.66)1.46 (1.03, 2.08)1.92 (1.55, 2.37)
3.83 (1.30, 11.27)29.22 (1.39, 613.44)3.62 (1.36, 9.62)6.33 (1.03, 38.98)1.41 (0.87, 2.27)16.35 (0.89, 301.66)5.13 (0.24, 108.62)7.44 (2.09, 26.51)1.43 (0.31, 6.67)0.70 (0.35, 1.40)5.06 (0.70, 36.39)9.61 (5.72, 16.15)1.22 (0.70, 2.13)1.95 (1.32, 2.88)1.87 (1.45, 2.40)2.27 (1.61, 3.20)1.83 (0.11, 30.19)1.77 (0.48, 6.56)0.14 (0.01, 2.49)1.35 (0.08, 21.92)1.30 (0.81, 2.07)3.55 (0.64, 19.72)5.40 (2.12, 13.81)2.41 (1.74, 3.33)
Odds ratio (95% CI)
4.752.112.182.550.993.060.903.211.672.663.894.100.792.825.643.063.596.993.128.645.225.327.048.657.04100.00
4.531.004.982.357.631.081.003.792.986.472.077.407.208.078.678.291.163.651.091.177.682.565.17100.00
Weight%
2.73 (1.42, 5.27)1.37 (0.38, 4.90)2.53 (0.73, 8.77)3.45 (1.13, 10.56)0.36 (0.05, 2.70)2.86 (1.08, 7.62)16.93 (2.02, 141.78)6.13 (2.39, 15.70)1.67 (0.38, 7.31)5.37 (1.81, 15.91)5.32 (2.39, 11.85)1.70 (0.79, 3.65)0.95 (0.10, 9.26)1.35 (0.48, 3.82)1.65 (0.97, 2.80)1.96 (0.74, 5.20)2.56 (1.08, 6.03)1.50 (1.05, 2.15)2.65 (1.01, 6.94)0.93 (0.87, 1.00)2.31 (1.28, 4.16)1.98 (1.11, 3.51)1.15 (0.81, 1.63)1.55 (1.46, 1.66)1.46 (1.03, 2.08)1.92 (1.55, 2.37)
3.83 (1.30, 11.27)29.22 (1.39, 613.44)3.62 (1.36, 9.62)6.33 (1.03, 38.98)1.41 (0.87, 2.27)16.35 (0.89, 301.66)5.13 (0.24, 108.62)7.44 (2.09, 26.51)1.43 (0.31, 6.67)0.70 (0.35, 1.40)5.06 (0.70, 36.39)9.61 (5.72, 16.15)1.22 (0.70, 2.13)1.95 (1.32, 2.88)1.87 (1.45, 2.40)2.27 (1.61, 3.20)1.83 (0.11, 30.19)1.77 (0.48, 6.56)0.14 (0.01, 2.49)1.35 (0.08, 21.92)1.30 (0.81, 2.07)3.55 (0.64, 19.72)5.40 (2.12, 13.81)2.41 (1.74, 3.33)
Odds ratio (95% CI)
4.752.112.182.550.993.060.903.211.672.663.894.100.792.825.643.063.596.993.128.645.225.327.048.657.04100.00
4.531.004.982.357.631.081.003.792.986.472.077.407.208.078.678.291.163.651.091.177.682.565.17100.00
Weight%
1.2 .5 1 2 3 5 10 1520
Subgroup analyses: Death(Income level)
The association was slightly stronger amongst low income countries

NOTE: Weights are from random effects analysis
.
.
1: Medical/self-reported
Ambrosetti, 1995 report
Ambrosetti, 1996 report
Ambrosetti, 1997 report
Centis, 1998 report
Centis, 1999 report
Morsy, 2003
Anunnatsiri, 2005
Chiang, 2009
Orofino Rde, 2011
Sangral, 2012
Jiménez-Corona, 2013
Choi, 2014
Chiang, 2015
Subtotal (I-squared = 29.8%, p = 0.146)
2: Blood glucose
Mboussa, 2003
Singla, 2006
Namukwaya, 2011
Uchimura, 2013
Mi, 2013
Nandakumar, 2013
Tabarsi, 2014
Alo, 2014
Viswanathan, 2014
Viswanathan, 2014
Cavanaugh, 2015
Chen, 2015
Subtotal (I-squared = 84.3%, p = 0.000)
Study
Italy
Italy
Italy
Italy
Italy
Egypt
Thailand
Taiwan
Brazil
India
Mexico
R.O.K.
Taiwan
Congo
K.S.A.
Uganda
Japan
China
India
Iran
Fiji
India
India
Kiribati
China
Country
3/32
5/50
2/41
5/41
2/40
31/40
4/38
60/241
4/14
4/23
28/363
./.
101/705
13/32
1/134
2/2
1281/5622
12/97
74/667
2/37
3/53
4/96
8/89
5/101
15/182
n/N
TB-DM
33/737
20/773
45/666
61/1059
28/852
88/198
11/188
161/886
21/294
20/257
55/847
./.
78/768
13/100
7/384
48/148
6578/28077
13/483
148/2127
3/67
12/335
6/149
1/120
4/174
14/944
n/N
TB-nonDM
2.21 (0.64, 7.62)
4.18 (1.50, 11.66)
0.71 (0.17, 3.03)
2.27 (0.86, 6.00)
1.55 (0.36, 6.74)
4.31 (1.95, 9.52)
1.89 (0.57, 6.30)
1.49 (1.06, 2.09)
5.20 (1.50, 18.00)
2.49 (0.77, 8.04)
1.20 (0.75, 1.93)
1.78 (1.09, 2.92)
1.48 (1.08, 2.03)
1.81 (1.43, 2.29)
4.58 (1.83, 11.43)
0.40 (0.05, 3.32)
10.36 (0.49, 220.01)
0.96 (0.90, 1.03)
5.10 (2.25, 11.56)
1.67 (1.24, 2.24)
1.22 (0.19, 7.65)
1.62 (0.44, 5.92)
1.04 (0.28, 3.77)
11.75 (1.44, 95.78)
2.21 (0.58, 8.44)
5.97 (2.83, 12.59)
2.29 (1.38, 3.79)
Odds ratio (95% CI)
3.23
4.50
2.42
4.94
2.37
6.85
3.41
18.81
3.22
3.58
13.74
13.09
19.84
100.00
10.11
4.16
2.30
15.12
10.83
14.42
5.03
7.55
7.59
4.18
7.32
11.38
100.00
Weight
%
2.21 (0.64, 7.62)
4.18 (1.50, 11.66)
0.71 (0.17, 3.03)
2.27 (0.86, 6.00)
1.55 (0.36, 6.74)
4.31 (1.95, 9.52)
1.89 (0.57, 6.30)
1.49 (1.06, 2.09)
5.20 (1.50, 18.00)
2.49 (0.77, 8.04)
1.20 (0.75, 1.93)
1.78 (1.09, 2.92)
1.48 (1.08, 2.03)
1.81 (1.43, 2.29)
4.58 (1.83, 11.43)
0.40 (0.05, 3.32)
10.36 (0.49, 220.01)
0.96 (0.90, 1.03)
5.10 (2.25, 11.56)
1.67 (1.24, 2.24)
1.22 (0.19, 7.65)
1.62 (0.44, 5.92)
1.04 (0.28, 3.77)
11.75 (1.44, 95.78)
2.21 (0.58, 8.44)
5.97 (2.83, 12.59)
2.29 (1.38, 3.79)
Odds ratio (95% CI)
3.23
4.50
2.42
4.94
2.37
6.85
3.41
18.81
3.22
3.58
13.74
13.09
19.84
100.00
10.11
4.16
2.30
15.12
10.83
14.42
5.03
7.55
7.59
4.18
7.32
11.38
100.00
Weight
%
1.2 .5 1 2 3 5 10 15
Subgroup analyses: Failure and death(medical records/self-reported - equivalent to previously diagnosed diabetes surrogate measures e.g. blood glucose, HbA1c includes previously diagnosed and newly diagnosed DM)
146
The association was stronger amongst studies using surrogate DM measures

Subgroup analyses: Failure and death(Income level)
147
NOTE: Weights are from random effects analysis
.
.
1: High income
Ambrosetti, 1995 report
Ambrosetti, 1996 report
Ambrosetti, 1997 report
Centis, 1998 report
Centis, 1999 report
Singla, 2006
Chiang, 2009
Uchimura, 2013
Choi, 2014
Chiang, 2015
Subtotal (I-squared = 70.4%, p = 0.000)
2: Upper/Lower-middle/Low
Mboussa, 2003
Morsy, 2003
Anunnatsiri, 2005
Namukwaya, 2011
Orofino Rde, 2011
Sangral, 2012
Jiménez-Corona, 2013
Mi, 2013
Nandakumar, 2013
Tabarsi, 2014
Alo, 2014
Viswanathan, 2014
Viswanathan, 2014
Cavanaugh, 2015
Chen, 2015
Subtotal (I-squared = 57.6%, p = 0.003)
Study
Italy
Italy
Italy
Italy
Italy
K.S.A.
Taiwan
Japan
R.O.K.
Taiwan
Congo
Egypt
Thailand
Uganda
Brazil
India
Mexico
China
India
Iran
Fiji
India
India
Kiribati
China
Country
3/32
5/50
2/41
5/41
2/40
1/134
60/241
1281/5622
./.
101/705
13/32
31/40
4/38
2/2
4/14
4/23
28/363
12/97
74/667
2/37
3/53
4/96
8/89
5/101
15/182
n/N
TB-DM
33/737
20/773
45/666
61/1059
28/852
7/384
161/886
6578/28077
./.
78/768
13/100
88/198
11/188
48/148
21/294
20/257
55/847
13/483
148/2127
3/67
12/335
6/149
1/120
4/174
14/944
n/N
TB-nonDM
2.21 (0.64, 7.62)
4.18 (1.50, 11.66)
0.71 (0.17, 3.03)
2.27 (0.86, 6.00)
1.55 (0.36, 6.74)
0.40 (0.05, 3.32)
1.49 (1.06, 2.09)
0.96 (0.90, 1.03)
1.78 (1.09, 2.92)
1.48 (1.08, 2.03)
1.48 (1.08, 2.01)
4.58 (1.83, 11.43)
4.31 (1.95, 9.52)
1.89 (0.57, 6.30)
10.36 (0.49, 220.01)
5.20 (1.50, 18.00)
2.49 (0.77, 8.04)
1.20 (0.75, 1.93)
5.10 (2.25, 11.56)
1.67 (1.24, 2.24)
1.22 (0.19, 7.65)
1.62 (0.44, 5.92)
1.04 (0.28, 3.77)
11.75 (1.44, 95.78)
2.21 (0.58, 8.44)
5.97 (2.83, 12.59)
2.71 (1.87, 3.93)
Odds ratio (95% CI)
4.89
6.49
3.78
7.00
3.70
1.98
17.64
22.10
14.26
18.15
100.00
7.79
8.82
5.80
1.34
5.57
5.99
11.91
8.60
13.50
3.21
5.26
5.30
2.59
5.06
9.24
100.00
Weight
%
2.21 (0.64, 7.62)
4.18 (1.50, 11.66)
0.71 (0.17, 3.03)
2.27 (0.86, 6.00)
1.55 (0.36, 6.74)
0.40 (0.05, 3.32)
1.49 (1.06, 2.09)
0.96 (0.90, 1.03)
1.78 (1.09, 2.92)
1.48 (1.08, 2.03)
1.48 (1.08, 2.01)
4.58 (1.83, 11.43)
4.31 (1.95, 9.52)
1.89 (0.57, 6.30)
10.36 (0.49, 220.01)
5.20 (1.50, 18.00)
2.49 (0.77, 8.04)
1.20 (0.75, 1.93)
5.10 (2.25, 11.56)
1.67 (1.24, 2.24)
1.22 (0.19, 7.65)
1.62 (0.44, 5.92)
1.04 (0.28, 3.77)
11.75 (1.44, 95.78)
2.21 (0.58, 8.44)
5.97 (2.83, 12.59)
2.71 (1.87, 3.93)
Odds ratio (95% CI)
4.89
6.49
3.78
7.00
3.70
1.98
17.64
22.10
14.26
18.15
100.00
7.79
8.82
5.80
1.34
5.57
5.99
11.91
8.60
13.50
3.21
5.26
5.30
2.59
5.06
9.24
100.00
Weight
%
1.2 .5 1 2 3 5 10 15
The association was slightly stronger amongst low income countries

Summary of results
• More recent studies continue to support a significant association: diabetes & TB treatment outcome
• If anything, risk of poor TB treatment outcome appears higher than before with this update• A small number of studies suggested better glycaemic control among TB patients may improve
outcomes? [still few studies available]
• Better designed studies (blood screening for DM; appropriate control of confounding) seem to find the strongest associations with poor TB treatment outcomes
• Increasing evidence that diabetes is associated with multi-drug resistant TB?
• Studies still being poorly described and analysed (despite EQUATOR Network / STROBE guidelines): important to start dialogue with National TB Programme Managers
148

Discussion• Heterogeneity – high in many forest plots, reduced in some sub-group analyses
• Although there are studies from LMIC, the “higher quality” evidence comes more from developed countries with lower TB incidence
• Control of confounding: not adjusted or many studies may be over-adjusted
• Neglected competing risk: longer term follow-up studies mostly used regression modelling rather than survival analyses (TB relapse or recurrence cannot compete with death!)
• Few studies reported on “diabetes variables” (e.g. BMI, glycaemic control)
149

Acknowledgements
• Co-authors (Cesar Ugarte Gill, Julia Critchley, Fiona Pearson, Johnathan Golub)
• This publication was made possible by NPRP grant number 7-627-3-167 from the Qatar National Research Fund (a member of Qatar Foundation). The statements made herein are solely the responsibility of the authors. The funder had no role in the design, conduct, or analysis of the study.
• It was also partially supported by grants from the TANDEM (TB and DM) EC FP7 consortium
• Support with translation from: Royusuke Omori, Varvara Bashkirova, Anna Kolodziejczyk, Yuki Nitta.
150

Research Questions
1. Is there an increased risk of TB among DM patients and is the association bidirectional?
2. If any associations are seen between TB and DM are they limited to specific disease subtypes?

The Health Improvement Network
• To answer such questions large data sets or long term follow-up is needed• THIN is a very large set of UK primary care health data• Contains data from 479 practices with a total of 9.1 million patients
• 1/3 are actively registered; the rest are historically active but have left their practice or died
Institute ofHealth&Society
Data & Methods
• Exposure and reference cohorts were constructed in order
to carry out a set of retrospective cohort analyses
Active THIN Population

• Data are organised in relational files separated by contributing GP (four standardised and one linked file per practice)
• Data is interpreted using ancillary look up tables and dictionaries. Medical events use the Read system and prescriptions a Multi-lexical and BNF code
Linked by patient ID
Linked by patient ID
Linked by practice ID
Patient file
Data on demographics
Therapy file
Data on prescriptions
Medical file
Data on medical eventsAdditional Health Data (AHD) file
Data on prevention, lifestyle and
diagnostics
Drug codes
Encrypted Multilex
code linked to
generic medicine
description
DosageDosage code
linked to
dosage string
Medical codes
Linked to
description of sign,
symptom,
procedure etc
Anonymised comments
Linked by text ID
Pack size
Free text
linked to pack
size code
Postcode Variable
Indicators
Variables linked to patient ID
derived from patients’
ward/location.
AHD codes
Description of codes
and context of
dependant variables
Research file
Patient demographics and selected
completeness of recording by year. Linked
by practice ID
Staff roles linked
by staff ID
Consult
Can be linked to therapy, AHD and
medical events. Data on location,
time and length of consultation
Practice file
Contains dates of last collection, Vision date, AMR,
computerisation etc
The Health Improvement Network

Methods
• Dynamic exposure and reference cohorts constructed using data from 2003-2009• Date of entry taken as date of first exposure or reference condition episode• Date of exit taken as date of subsequent outcome episode, txr date, date of death or end of
study period
• Key variables defined using a sensitive combination of Read codes from multiple fields of interest (265 codes for TB and 479 for DM)
• Individuals with missing data excluded (randomly patterned <1%)• Data were checked for over-dispersion (strong assumption) and IRRs were calculated
using negative binomial regression adjusted for age, sex and smoking status• An adjustment was made to IRRs to account for the potential confounding effect of
ethnicity

Data validation checks
• Consults and prescriptions are comparable to UK level• Deaths reported are as expected for practice demographic structure and are
comparative to national stats prior to study start date
• ID is unique• Either male or female• DOB is present and in correct format (≤ registration date, ≤ first data collection,age is not implausibly large)
• Individuals GP registration date is present and in correct format (≤ practice lastcollection date and/or txr date and/or death date)
• If not labelled as txr’d/dead has no txr out/death date• If labelled as txr’d or dead there is a corresponding date which is > DOB and
registration, ≤ last data collection date
• Has at least one health record

Sex, Age, SES and Smoking distributionVariable % of % of % of Categories TB PTB EPTBSex Male 49.3 53.9 43.7
Female 50.7 46.1 56.3Age 0-15 7.2 4.2 6.7Group 16-30 19 14.9 17.4
31-45 19.3 16.4 23.846-60 20.3 20.7 21.161-75 23.2 29.8 22.676+ 10.7 13.8 8.5
Townsend Quintile1 14.1 13.2 15.12 14.6 14.7 13.53 18.6 17.6 21.54 21.8 23.7 22.05 22.9 22.9 21.1
Smoker Yes 26.5 26.4 25.2Past 40.9 49.2 40.8No 32.6 24.4 34.0
Variable % of % of % of Categories DM T1DM T2DMSex Male 54.9 55.2 55.1
Female 45.1 44.8 44.9Age 0-15 1.3 6.1 0.1Group 16-30 3.9 12.6 1.5
31-45 13.1 20.1 11.546-60 28.5 23.9 29.961-75 35.7 26.7 38.776+ 17.4 10.6 18.3
Townsend Quintile1 20.3 20.4 20.12 19.8 19.4 19.93 20.1 20.3 20.24 19.3 19.4 19.45 14.5 14.5 14.6
Smoker Yes 27.7 29.5 28.1Past 53.3 47.8 54.9No 19.0 22.8 17.0
Mean age of entry into DM cohorts was 60 years and into TB cohorts 50 years Average f/up for each cohort was 4 years

Risk of TB amongst people with DMExposure Outcome
condition condition Adjusted IRR (95% CI)1 P-value
DM TB 1.50 (1.27-1.76) <0.001
T1DM TB 1.455 (1.104-1.917) 0.008
T2DM TB 1.536 (1.296-1.822) <0.001
DM PTB 1.237 (0.934-1.638) 0.137
T1DM PTB 1.304 (0.787-2.160) 0.303
T2DM PTB 1.243 (0.923-1.673) 0.152
DM EPTB 1.434 (0.993-2.071) 0.055
T1DM EPTB 2.088 (1.190-3.664) 0.010
T2DM EPTB 1.388 (0.934-2.062) 0.105 1Adjusted for age, sex, region, Townsend score and smoking status

Adjustment for ethnicity as an “external confounder”
• In the UK TB is highly concentrated among South Asian and Black Afro-Caribbean ethnic minorities, who also have highest risks of T2DM
• Degree of confounding=𝑐𝑜𝑛𝑓𝑜𝑢𝑛𝑑𝑒𝑑𝑅𝑅
𝑡𝑟𝑢𝑒𝑅𝑅=
100−𝑝1 +𝑅𝑅𝑠𝑝1
100−𝑝0 +𝑅𝑅𝑠𝑝0
• p1—% with “BAC or SA ethnicity” in the exposed group; p0—percentage of subjects with “BAC or SA ethnicity” in the unexposed group
• RR for “BAC or SA ethnicity” & outcome (TB or DM) e.g. approx. 6 for DM
• IRRs 1.95- to 2.43-fold by residual confounding by ethnicity
• IRR 5.65 2.33 (95%CI 2.14-2.53)-2.90 (95%CI 2.66-3.16)
16/09/2016 158

Summary• Significant associations between TB and DM after controlling for key confounders
were found (as previously)• The magnitude of risk identified (1.3 fold) is lower but in line with recent studies from
developed countries
• Lower findings likely reflect low TB burden and a strong primary health care system with good glycaemic control and management of DM co-morbidities
• A substantial increase in risk of DM among individuals with prior TB (2-5 fold) has been identified.
• Although bi-directionality has been speculated, as far as we are aware, no other prospective cohort studies have been able to quantify this
• Further studies in high TB incidence countries are needed to confirm our finding and its importance
• Probably difficult to carry out in practice, due to the large sample size and length of f/up required. Alternatively further analysis of similarly sized datasets could be completed

Summary• Significant associations between TB and DM after controlling for key confounders
were found (as previously)• The magnitude of risk identified (1.3 fold) is lower but in line with recent studies from
developed countries
• Lower findings likely reflect low TB burden and a strong primary health care system with good glycaemic control and management of DM co-morbidities
• A substantial increase in risk of DM among individuals with prior TB (2-5 fold) has been identified.
• Although bi-directionality has been speculated, as far as we are aware, no other prospective cohort studies have been able to quantify this
• Further studies in high TB incidence countries are needed to confirm our finding and its importance
• Probably difficult to carry out in practice, due to the large sample size and length of f/up required. Alternatively further analysis of similarly sized datasets could be completed

Summary• Significant associations between TB and DM after controlling for key confounders
were found (as previously)• The magnitude of risk identified (1.3 fold) is lower but in line with recent studies from
developed countries
• Lower findings likely reflect low TB burden and a strong primary health care system with good glycaemic control and management of DM co-morbidities
• A substantial increase in risk of DM among individuals with prior TB (2-5 fold) has been identified.
• Although bi-directionality has been speculated, as far as we are aware, no other prospective cohort studies have been able to quantify this
• Further studies in high TB incidence countries are needed to confirm our finding and its importance
• Probably difficult to carry out in practice, due to the large sample size and length of f/up required. Alternatively further analysis of similarly sized datasets could be completed

Contributing factors
• Host immunity• T-cells, B-cells, macrophages,
• neutrophils …
• Neuropathy, microangiopathy, wound healing
• Obesity
• More S aureus carriage
• Glycosuria
• More health-care associated infections• More hospitalisation, more instrumentation
• poor glycemic control?:
• more infections, more admissions, higher mortality
Casquiero et al 2012