
Contribution of echoendoscopy to mediastinal staging - ifct.fr fileMediastinal staging zBefore PET...
28
Contribution of Contribution of echoendoscopy echoendoscopy to to mediastinal mediastinal staging staging Vincent Ninane, Saint-Pierre and Bordet Institute, Brussels, Belgium
Transcript of Contribution of echoendoscopy to mediastinal staging - ifct.fr fileMediastinal staging zBefore PET...

Contribution of Contribution of echoendoscopy echoendoscopy to to mediastinal mediastinal
stagingstaging
Vincent Ninane, Saint-Pierre and Bordet Institute, Brussels, Belgium
Mediastinal stagingMediastinal staging
Before PET introduction– Enlarged lymph nodes on CT scan– Or nearly all cases (low performance of CT scan)
After PET introduction– Positive hot spots– Additional situations (PET + N1 tumors, large
mediastinal lymph nodes, low SUV tumors, central tumors)
Purpose : to exclude– Involvement of mediastinal contralateral side– Extensive involvement of the ipsilateral side
medical management

Survival prognostic factors for Survival prognostic factors for N2 diseaseN2 disease
Unfavourable– Incomplete resection– Multi-level metastasis– Radiological N2 disease– T3-T4N2– Extranodal expansion– Number– Subcarinal node
involvement– T > 50 mm
Favourable– Complete resection– One-level metastasis– cN0-N1– T1-T2N2– Intranodal microscopic
metastasis– Without subcarinal nodal
involvement– T < 20 mm
Watanabe et al. Monduzzi editor. Proceedings of the Third International Congresson lung cancer. 1998; 131-7

Accuracy of standard cervical Accuracy of standard cervical mediastinoscopic biopsies in LCmediastinoscopic biopsies in LC
Source Years No of patients
sensitivity specificity PPV NPV prevalence
14 papers
83-99 5687 0.81 1.00 1.00 0.91 0.37
Mediastinoscopy is the gold standard !
Toloza et al. Chest 2003;123:157S-166S

Comparison of characteristics Comparison of characteristics of invasive testsof invasive tests
Tests Sensitivity %
Specificity %
FP rate %
FN rate %
Patientpopulation
Medscopy 81 100 0 9 cN0-N2
TTNA 91 100 0 22 c N2
EUS-NA 88 91 2 23 c N2
TBNA 76 96 0 29 c N2
Detterbeck et al. Chest 2003;123:167S-175S

InvasiveInvasive stagingstagingguidelinesguidelines
extensive mediastinal infiltration : confirmation of diagnosisTTNA, EUS-NA ↑ sensitivity recommend. Balternative TBNA ↓ sensitivity recommend. Bmediastinoscopy (MS) least useful
enlarged, discrete mediastinal nodes by CT :MS 1st choice ↓ FP, FN rate recommend. Balternative TBNA, TTNA, EUS-NA
↑ FN rate recommend. BLUL cancer, no other nodes involved, evaluation 5,6 :
ant. or extended MS, EUS-NA, VATS recommend. B
Detterbeck FC. Chest 2003; 123 (suppl 1): S167-S175

InvasiveInvasive stagingstagingguidelinesguidelines
normal mediastinal nodes by CT, rule out mediastinal involvementMS ↓ FN rate recommend. Bnot : TBNA, TTNA, EUS-NA ↑ FN rate recommend. D
PET + in mediastinum : confirmation necessaryMS ↓ FN rate recommend. B
PET – in mediastinum : confirmation deemed desirableMS ↓ FN rate recommend. C
Detterbeck FC. Chest 2003; 123 (suppl 1): S167-S175

EBUSEBUSSaint-Pierreexperience
2003
2004

EBUSEBUS--EUS complementarityEUS complementarity
7
1
998
EUSEBUS

PET hot spots in the PET hot spots in the mediastinummediastinum

EUSEUS--FNA in suspected/confirmed lung FNA in suspected/confirmed lung cancers with PET + mediastinumcancers with PET + mediastinum
81 patients with suspected lung cancer and PET hot spotsPositive EUS-FNA in 50 (62%) of the patients31 negative or inconclusive patients– 26 surgical staging (14 with mediastinum malignancy)– 5 follow-up with mediastinal metastases
Accuracy of decision to proceed (or not) to surgery on the basis of EUS-FNA : 77%Reduction of 40% in cost/patient
Kramer et al. Thorax 2004;59:596-601

EUSEUS--FNA in suspected/confirmed FNA in suspected/confirmed lung cancers with PET positive lung cancers with PET positive
mediastinummediastinumRef. Nb of
patientsLymphnode meansize (shortaxis, mm)
EUS-FNA diagnostic value
Sensitivity Specificity Accuracy
Annema2004Eloubeidi2005
36
104
NR
13
93 %
92.5%
100 %
100%
94 %
97%
NR : not reported
Annema et al. Lung Cancer 2004; 44:53-60; Eloubeidi et al.Ann Thorac Surg 2005;79:263-8

EBUS (miniprobes) in patients with PET EBUS (miniprobes) in patients with PET positive mediastinal lymph nodespositive mediastinal lymph nodes
Nb Positive Ebus Diagnostic TBNAAll cases after positive
EBUSAll patients 33 24 (73%) 27 (82%) 21 (88%)
Neoplastic diseasesNSCLC SCLCMelanomaColon cancer
2720511
20 (74%) 25 (93%) 19 (95%)
Non neoplastic diseases
AnthracosisSarcoidosisNormal histology Benign unknown
6
3111
4 (67%) 2 (33%) 2 (50%)
Plat et al. Eur Respir J, 2006;27:276-81
Surgical sampling avoided in 25 cases (76% of the patients)

EBUS (linear) in patients with lung cancer EBUS (linear) in patients with lung cancer and PET positive mediastinal lymph nodesand PET positive mediastinal lymph nodes
december 2004 - february 2006Total number of patients 51
– Bordet-Saint-Pierre 22– Other hospitals (n=19) 29
Indications– Proven lung cancer 21
After induction 5– Suspected lung cancer 30
Active/former smokers 23/28Male/female 38/13Mean age (yr) 62 + 11

4R PET4R PET--CT positive lymph CT positive lymph node (8,5 mm)node (8,5 mm)

EBUS and PET + LNEBUS and PET + LN
26 LN metastasis 1 anthracosis1 tuberculosis
14 non tumor LN 3 LN metastasis
17 surgicalverifications
6 cases withoutsurgical verification
23 non contributivecases
51 patients
including 3 cases of PET understaging
Eluded surgical sampling : 27/51 (53%)Mean small diameter of all LN : 11.3 + 5.9 (range : 3.3 to 27) mmSmallest confirmed malignant LN : 6X8 mm

EBUS and PET + LNEBUS and PET + LN
Prevalence of LN metastasis : 57%45 assessable patients : EBUS for LN staging– Sensitivity : 90%– Accuracy : 93%– Negative predictive value : 84%

STST--Pierre/Bordet PETPierre/Bordet PET--CTCT
LN final diagnosis
LN metastasis No tumorLN
Nbpatients
15 7
SUV(mean + SD)
11.2 + 7.7 4.2 + 2.6
P < 0.02

CT enlarged lymph nodesCT enlarged lymph nodes

Diagnostic value of EUSDiagnostic value of EUS--FNA FNA and impact on surgical stagingand impact on surgical stagingN of patients 242
LN mean size (CT) : 24 mm (range : 13-77); prevalence of LN metastasis : 71%
sensitivity 91 %
specificity 100 %
accuracy 93 %
N of avoided surgical procedures
TotalN2-N3T4N2-N3 + T4SCLCBenign D
70 %52 %4 %5 %8 %1 %
Annema et al. J Clin Oncol 2005:23:8357-8361
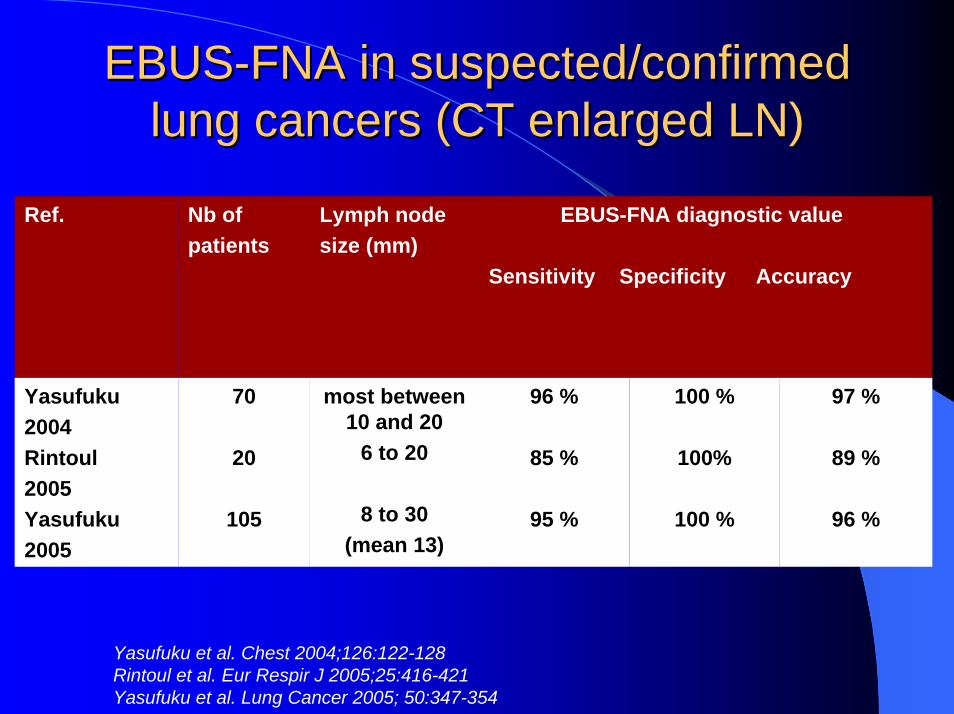
EBUSEBUS--FNA in suspected/confirmed FNA in suspected/confirmed lung cancers (CT enlarged LN)lung cancers (CT enlarged LN)
Ref. Nb ofpatients
Lymph nodesize (mm)
EBUS-FNA diagnostic value
Sensitivity Specificity Accuracy
Yasufuku2004Rintoul2005Yasufuku2005
70
20
105
most between 10 and 20
6 to 20
8 to 30(mean 13)
96 %
85 %
95 %
100 %
100%
100 %
97 %
89 %
96 %
Yasufuku et al. Chest 2004;126:122-128Rintoul et al. Eur Respir J 2005;25:416-421Yasufuku et al. Lung Cancer 2005; 50:347-354

EBUS + EUSEBUS + EUS--NA of enlarged NA of enlarged mediastinal lymph nodesmediastinal lymph nodes
160 patients; eight stations represented (20 patients/station)Crossover EBUS and EUSMean punctured lymph node size : 17 mmSuccessful biopsies– EBUS : 85 %– EUS : 78 %– EBUS + EUS : 97% with diagnoses in 94%
Herth F et al. Am J Respir Crit Care Med 2005;171:1164-1167

Normal mediastinal lymph Normal mediastinal lymph nodes by CTnodes by CT

EUS in the absence of EUS in the absence of lymphadenopathy on CTlymphadenopathy on CT
76 consecutive patients (4 lost to follow-up)10 did not undergo surgery (1 refused)– 9 (12%) because of EUS (N3 : 5; celiac LN :
1; T4 : 1; esophageal cancer : 1)62 underwent surgery– 17 N2 disease including 12 in areas explored
by EUS (5/12 were positive by FNA)
LeBlanc et al. Am J Respir Crit Care Med 2005;171:177-82

Mediastinal restagingMediastinal restaging
Assess the (pathologic) response to induction therapySelect patients who could undergo operation with complete resection– Patients with downstaging, in particular with
complete pathological response– In practice, to screen out
N3 diseaseextranodal involvementPersistent multinodal (or even uninodal?) N2

EUSEUS--FNA in mediastinal FNA in mediastinal restaging (initial N2)restaging (initial N2)
Ref. Nb ofpatients
EUS-FNA diagnostic value
PPV NPV Sensitivity Specificity Accuracy
Annema2003
19PR 14SD 5
100% 67% 75 % 100% 83%
Annema JT et al. Lung Cancer 2003;42:313-318

Initial and postInitial and post--induction induction invasive mediastinal staginginvasive mediastinal staging
Post-inductionInitial Limitations
Mediastinoscopy Remediastinoscopy Remediastinoscopytechnically difficult
EBUS and/or EUS-NA Mediastinoscopy False negative NA (~20%)
Mediastinoscopy EBUS and/or EUS-NAFalse negative NA, incompletestaging by TBNA

General conclusions : General conclusions : mediastinal stagingmediastinal staging
Mediastinoscopy is the gold standardInitial staging : needle aspiration (EBUS and EUS) will reduce invasive surgical staging and costRestaging : mediastinoscopy (and not remediastinoscopy) may then be used







![Typical and atypical radiologic manifestations of ......of radiographic staging [1,2,6]. Middle mediastinal nodes (at the left paratracheal level, subcarinal level, and level of the](https://static.fdocuments.net/doc/165x107/5f7d2ff2ec543436a327439a/typical-and-atypical-radiologic-manifestations-of-of-radiographic-staging.jpg)









