Case Report Multidetector Computed Tomography Angiography ...

Rev Port Cardiol. 2014;33(10):653---654
Revista Portuguesa de
CardiologiaPortuguese Journal of Cardiology
www.revportcardiol.org
IMAGE IN CARDIOLOGY
Contribution of cardiac computed tomographyangiography to assessment of chest pain�
Contributo da angio tomografia computorizada cardíaca naavaliacão da dor torácica
Raquel Douradoa,∗, Rute Coutob, Miguel Pachecoa, Anabela Tavaresa, Dinis Martinsa
a Hospital do Divino Espírito Santo EPE de Ponta Delgada, Ponta Delgada, Portugalb Hospital do Santo Espírito, Angra do Heroísmo, Angra do Heroísmo, Portugal
Received 18 October 2013; accepted 29 March 2014
(1) Lesion is volume based
Threshold=130 HU(102.3 mg/cm3 CaHA)
Artery Number oflesions(1)
0
0
0
0
0
LM
LAD
CX
RCA
Total
0.0
0.0
0.0
0.0
0.0
0.00
0.00
0.00
0.00
0.00
0.0
0.0
0.0
0.0
0.0
Volume[mm3](3)
Equiv. mass[mg CaHA](4)
Calciumscore(2)
Available online 18 October 2014
The authors present the case of a 47-year-old man, withhypertension and dyslipidemia as cardiovascular risk fac-tors, who had come to the emergency department in 2008for chest pain. Diagnostic exams at that time (ECG and car-diac biomarkers) revealed no signs of acute ischemia, butexercise testing was positive for myocardial ischemia. Inva-sive coronary angiography was performed, which showedno angiographically significant coronary lesions. He subse-quently underwent myocardial perfusion scintigraphy, whichrevealed no evidence of ischemia.
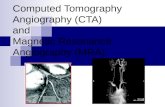
Due to persistence of symptoms, in 2012 exercise test-ing was repeated, which was positive for ischemia. In orderto clarify the clinical picture, he was referred to our hospi-tal for cardiac computed tomography (CT) angiography. Thisshowed a zero calcium score (Figure 1), corresponding tothe 25th percentile for age and gender, and revealed 50---70%stenosis with a non-calcified eccentric plaque in the distal
left main/proximal anterior descending artery (Figure 2).Invasive coronary angiography confirmed significant coro-nary artery disease (Figure 3) and the patient was referred
� Please cite this article as: Dourado R, Couto R, Pacheco M,Tavares A, Martins D. Contributo da angio tomografia computo-rizada cardíaca na avaliacão da dor torácica. Rev Port Cardiol.2014;33:653---654.
∗ Corresponding author.E-mail address: [email protected] (R. Dourado).
(2) Agatston score(3) Isotropic interpolated volume(4) Calibration Factor: 0.787
fappt
2174-2049/© 2013 Sociedade Portuguesa de Cardiologia. Published by El
Figure 1 Calcium score.
or coronary artery bypass grafting. The authors did not have
ccess to the initial coronary angiography since this waserformed in a different institution, and at referral theatient was in possession of clinical information only,ogether with the request for cardiac CT angiography.sevier España, S.L.U. All rights reserved.

654 R. Dourado et al.
Figure 2 Computed tomography angiography showin
Figure 3 Invasive coronary angiography showing significantplaque in the left main artery.
ca
E
Pda
Cft
Rd
C
T
g significant plaque in the distal left main artery.
This case highlights the important contribution thatardiac CT angiography can make to the diagnosis and char-cterization of coronary artery disease.
thical disclosures
rotection of human and animal subjects. The authorseclare that no experiments were performed on humans ornimals for this study.
onfidentiality of data. The authors declare that they haveollowed the protocols of their work center on the publica-ion of patient data.
ight to privacy and informed consent. The authorseclare that no patient data appear in this article.
onflicts of interest
he authors have no conflicts of interest to declare.