Contrastenhanced harmonic endoscopic …Clinical evaluation of new diagnostic modalities of EUS for...
8
Clinical evaluation of new diagnostic modalities of EUS for pancreatobiliary diseases Contrast-enhanced harmonic endoscopic ultrasonography for pancreatobiliary diseases Masayuki Kitano, 1 Ken Kamata, 1 Hajime Imai, 1 Takeshi Miyata, 1 Satoru Yasukawa, 2 Akio Yanagisawa 2 and Masatoshi Kudo 1 1 Department of Gastroenterology and Hepatology, Kinki University Faculty of Medicine, Osaka and 2 Department of Surgical Pathology, Kyoto Prefectural University of Medicine, Kyoto, Japan The combination of second-generation ultrasound contrast agents and an endoscopic ultrasonography (EUS) system with a broad-band transducer has allowed contrast-enhanced harmonic imaging in the field of EUS. In contrast-enhanced harmonic EUS (CH-EUS), diffuse homogeneous enhancement is obtained in normal parenchyma of the pancreas. The bile duct and pancre- atic duct are depicted as non-enhanced ductal structures with strong contrast in comparison to the surrounding parenchyma. CH-EUS identifies pancreatic adenocarcinomas as solid lesions exhibiting hypo-enhancement with a sensitivity and specificity of 88–96% and 88–94%, respectively. In particular, 80–100% of false- negative cases in endoscopic ultrasound-guided fine-needle aspi- ration (EUS-FNA) are correctly classified by CH-EUS, suggesting CH-EUS complements EUS-FNA. Moreover, CH-EUS improves depiction of some subtle lesions in conventional EUS, thus facilitating EUS-FNA. For quantitative per- fusion analysis, a time–intensity curve (TIC) for the region of inter- est can be generated during CH-EUS. The maximum intensity gain and the echo intensity reduction rate from the peak at 1 min obtained by TIC can be used for differentiation of pancreatic adenocarcinoma from other tumors. CH-EUS is also useful for differentiation of invasive intraductal papillary mucinous neo- plasms (IPMN) from non-invasive IPMN, identification of malig- nant lesions in the gallbladder, and T- and N-staging of pancreatobiliary tumors. Key words: contrast-enhanced harmonic endoscopic ultraso- nography (CH-EUS), endoscopic ultrasonography (EUS), pancre- atic carcinoma, pancreatobiliary disease INTRODUCTION C ONTRAST-ENHANCED HARMONIC IMAGING was developed to enhance ultrasound images by intra- venously infusing ultrasound contrast agents composed of microbubbles of approximately 2–5 μm in diameter. 1–4 The main principle of contrast-enhanced harmonic imaging is to selectively depict signals from the microbubbles of the ultra- sound contrast agents by filtering signals from the tissue (Fig. 1). 1–4 When exposed to ultrasonic beams with a certain range of acoustic power, microbubbles are disrupted or reso- nated, and this releases a large amount of harmonic signals (Fig. 1). When tissues and microbubbles receive transmitted ultrasound waves, the harmonic content from the micro- bubbles is higher than that from the tissues (Fig. 1). Selective depiction of the second harmonic component visualizes signals from microbubbles more strongly than those from tissues. 1–4 Levovist (Bayer Schering Pharma, Berlin, Germany), the first generation of ultrasound contrast agents composed of air with a palmitic acid shell, requires high acoustic power to release harmonic signals by resonation, which the microar- ray probe for endoscopic ultrasound (EUS) does not produce. 1–3 By contrast, the second generation of ultrasound contrast agents including Sonazoid (Daiichi-Sankyo, Tokyo, Japan; GE Healthcare Milwaukee, WI, USA), SonoVue (Bracco SpA, Milan, Italy) and Definity (Lantheus Medical Imaging, Billerica, MA, USA), which are composed of other gases (perfluorobutane, sulfur hexafluoride and perflutren, respectively) with a phospholipid or lipid shell, are more suitable for a small transducer equipped with an echoendo- scope because they resonate with a lower acoustic power than Levovist. 3,4 The combination of second-generation ultrasound contrast agents and an EUS system with a broad- band transducer has allowed contrast-enhanced harmonic imaging in the field of EUS. 3,5 Corresponding: Masayuki Kitano, Department of Gastroenterol- ogy and Hepatology, Kinki University Faculty of Medicine, 377-2 Ohno-higashi, Osaka-sayama 589-8511, Japan. Email: m-kitano @med.kindai.ac.jp Received 15 December 2014; accepted 27 January 2015. Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67 doi: 10.1111/den.12454 © 2015 The Authors Digestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society 60
Transcript of Contrastenhanced harmonic endoscopic …Clinical evaluation of new diagnostic modalities of EUS for...

Clinical evaluation of new diagnostic modalities of EUS for pancreatobiliary diseases
Contrast-enhanced harmonic endoscopic ultrasonographyfor pancreatobiliary diseases
Masayuki Kitano,1 Ken Kamata,1 Hajime Imai,1 Takeshi Miyata,1 Satoru Yasukawa,2
Akio Yanagisawa2 and Masatoshi Kudo1
1Department of Gastroenterology and Hepatology, Kinki University Faculty of Medicine, Osaka and 2Departmentof Surgical Pathology, Kyoto Prefectural University of Medicine, Kyoto, Japan
The combination of second-generation ultrasound contrastagents and an endoscopic ultrasonography (EUS) system with abroad-band transducer has allowed contrast-enhanced harmonicimaging in the field of EUS. In contrast-enhanced harmonic EUS(CH-EUS), diffuse homogeneous enhancement is obtained innormal parenchyma of the pancreas. The bile duct and pancre-atic duct are depicted as non-enhanced ductal structures withstrong contrast in comparison to the surrounding parenchyma.CH-EUS identifies pancreatic adenocarcinomas as solid lesionsexhibiting hypo-enhancement with a sensitivity and specificity of88–96% and 88–94%, respectively. In particular, 80–100% of false-negative cases in endoscopic ultrasound-guided fine-needle aspi-ration (EUS-FNA) are correctly classified by CH-EUS, suggestingCH-EUS complements EUS-FNA. Moreover, CH-EUS improvesdepiction of some subtle lesions in
conventional EUS, thus facilitating EUS-FNA. For quantitative per-fusion analysis, a time–intensity curve (TIC) for the region of inter-est can be generated during CH-EUS. The maximum intensity gainand the echo intensity reduction rate from the peak at 1 minobtained by TIC can be used for differentiation of pancreaticadenocarcinoma from other tumors. CH-EUS is also useful fordifferentiation of invasive intraductal papillary mucinous neo-plasms (IPMN) from non-invasive IPMN, identification of malig-nant lesions in the gallbladder, and T- and N-staging ofpancreatobiliary tumors.
Key words: contrast-enhanced harmonic endoscopic ultraso-nography (CH-EUS), endoscopic ultrasonography (EUS), pancre-atic carcinoma, pancreatobiliary disease
INTRODUCTION
CONTRAST-ENHANCED HARMONIC IMAGINGwas developed to enhance ultrasound images by intra-
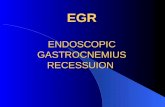
venously infusing ultrasound contrast agents composed ofmicrobubbles of approximately 2–5 μm in diameter.1–4 Themain principle of contrast-enhanced harmonic imaging is toselectively depict signals from the microbubbles of the ultra-sound contrast agents by filtering signals from the tissue(Fig. 1).1–4 When exposed to ultrasonic beams with a certainrange of acoustic power, microbubbles are disrupted or reso-nated, and this releases a large amount of harmonic signals(Fig. 1). When tissues and microbubbles receive transmittedultrasound waves, the harmonic content from the micro-bubbles is higher than that from the tissues (Fig. 1). Selective
depiction of the second harmonic component visualizessignals from microbubbles more strongly than those fromtissues.1–4
Levovist (Bayer Schering Pharma, Berlin, Germany), thefirst generation of ultrasound contrast agents composed ofair with a palmitic acid shell, requires high acoustic power torelease harmonic signals by resonation, which the microar-ray probe for endoscopic ultrasound (EUS) does notproduce.1–3 By contrast, the second generation of ultrasoundcontrast agents including Sonazoid (Daiichi-Sankyo, Tokyo,Japan; GE Healthcare Milwaukee, WI, USA), SonoVue(Bracco SpA, Milan, Italy) and Definity (Lantheus MedicalImaging, Billerica, MA, USA), which are composed of othergases (perfluorobutane, sulfur hexafluoride and perflutren,respectively) with a phospholipid or lipid shell, are moresuitable for a small transducer equipped with an echoendo-scope because they resonate with a lower acoustic powerthan Levovist.3,4 The combination of second-generationultrasound contrast agents and an EUS system with a broad-band transducer has allowed contrast-enhanced harmonicimaging in the field of EUS.3,5
Corresponding: Masayuki Kitano, Department of Gastroenterol-ogy and Hepatology, Kinki University Faculty of Medicine, 377-2Ohno-higashi, Osaka-sayama 589-8511, Japan. Email: [email protected] 15 December 2014; accepted 27 January 2015.
bs_b
s_ba
nner
Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67 doi: 10.1111/den.12454
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society
60

BASIC TECHNIQUE OF CONTRAST-ENHANCEDHARMONIC EUS
WHEN A LESION is depicted in the digestive tract orpancreatobiliary system, contrast-enhanced harmonic
EUS (CH-EUS) helps to characterize it by image enhance-ment.5 Before carrying out CH-EUS, the ideal imaging planeof each lesion for CH-EUS is determined during conven-tional EUS and the presetting is subsequently conditioned.The monitor is changed to dual imaging with the specificmode for CH-EUS (CH-EUS mode) and fundamental Bmode (monitor mode). Before infusion of the ultrasoundcontrast agent, the image on the specific mode for CH-EUSis dark.5 The MI, a unitless number that reflects the acousticpower based on the derated peak rarefactional pressure (p)and the fundamental frequency (f) (MI = p/f1/2), is set to0.2–0.4.5
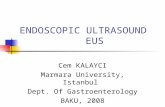
Immediately before carrying out contrast enhancement,the ultrasound contrast agents are reconstituted with sterilewater. A bolus injection of the ultrasound contrast agent isgiven through a 22-gauge cannula placed in the antecubitalvein.5 This is followed by a 10-mL saline solution flush toensure that the entire contrast agent was given into the cir-culation system. In CH-EUS mode, signals from micro-bubbles appear approximately 10 s after infusion and peak20–30 s after infusion (Fig. 2).5 When signals peak, diffusehomogeneous enhancement is obtained in normal paren-chyma of the pancreas (Fig. 2).5 The bile duct and pancreaticduct are depicted as non-enhanced ductal structures withstrong contrast in comparison to the surrounding paren-chyma (Fig. 2). Real-time observation can be continued forlonger than 1 min.
ENHANCEMENT PATTERNS OF PANCREATICSOLID LESIONS WITH CH-EUS
FOR PANCREATIC DISEASES, the main purpose ofCH-EUS is to characterize a solid lesion detected by
conventional EUS. The characterization of solid lesions, par-ticularly the differentiation of inflammatory tumors fromneoplasms, is crucial in order to make decisions regardingtreatment. However, it is sometimes difficult to characterizesolid lesions with conventional EUS alone.6,7 CH-EUS helpsthis characterization by analyzing the relative intensity ofenhancement compared with the surrounding tissue.7–11 InCH-EUS, solid lesions in the pancreas are categorized intothree to four patterns according to the intensity of enhance-ment: non-enhancement; hypo-enhancement (Fig. 3a); iso-enhancement (Fig. 3b); and hyper-enhancement (Fig. 3c).7–11
Interobserver agreement among endosonographers forCH-EUS was satisfactory (κ coefficient = 0.57–0.92).8,9,12
Non-experienced endosonographers demonstrated compa-rable interobserver agreement with experienced ones, sug-gesting that CH-EUS is an extremely reproducible tool witha short learning curve.9,12
DIAGNOSIS OF PANCREATICADENOCARCINOMAS ACCORDING TO THEENHANCEMENT PATTERNS OF CH-EUS
MOST PANCREATIC CARCINOMAS exhibit hypo-enhancement in CH-EUS (Fig. 3a).7–11 A recent meta-
analysis of reports concerning contrast-enhanced EUSshowed that this method identifies pancreatic adenocarcino-mas as solid lesions exhibiting hypo-enhancement with a
Figure 1 Principle of contrast enha-nced harmonic imaging. When exposedto ultrasonic beams with a certainrange of acoustic power, microbubblesare disrupted or resonated, and thisreleases a large amount of harmonicsignals. When tissues and micro-bubbles receive transmitted ultrasoundwaves, the harmonic content from themicrobubbles is higher than that fromthe tissues. Selective depiction ofthe second harmonic component visu-alizes signals from microbubbles morestrongly than those from tissues.
Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67 CH-EUS for pancreatobiliary diseases 61
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society

pooled sensitivity and specificity of 94% and 89%, respec-tively.10 However, this meta-analysis not only includedCH-EUS but also contrast-enhanced Doppler EUS whichsuffers from artifacts such as blooming.5,11
Fusaroli et al. reported that identification of hypo-enhancing masses with an inhomogeneous pattern inCH-EUS is a sensitive and accurate identifier of patientswith adenocarcinoma (sensitivity and accuracy of 96% and82%, respectively).7 This identification by CH-EUS is moreaccurate than the finding of a hypoechoic lesion using stan-dard EUS (sensitivity and accuracy of 85% and 58%, respec-tively).7
We previously compared CH-EUS and contrast-enhancedmultidetector-row computed tomography (MDCT) for theidentification of adenocarcinomas.8 CH-EUS (sensitivity andspecificity of 91.2% and 94.4%, respectively) was superiorto MDCT (sensitivity and specificity of 70.6% and 91.6%,respectively) in diagnosing small (≤2 cm) carcinomas(P < 0.05).8
CH-EUS FOR EUS-FNA
THREE STUDIES COMPARED CH-EUS with EUS-guided fine-needle aspiration (EUS-FNA) in the identi-
fication of adenocarcinomas.8,9,11 In these, the sensitivity andspecificity of hypo-enhancement in CH-EUS for diagnosingpancreatic adenocarcinoma were 89–96% and 88–94%,respectively, which were not significantly different from thecorresponding values in EUS-FNA of 72–95% and 100%,respectively.8,9,11 However, 80–100% of false-negative casesin EUS-FNA were correctly classified by CH-EUS.8,9,11
These results suggest that CH-EUS could help to decidebetween surgery and follow up when the results of EUS-FNA are inconclusive.
CH-EUS is also useful for identification of the target ofEUS-FNA.7,8,13 CH-EUS improves depiction of some subtlelesions in conventional EUS, thus facilitating EUS-FNA(Fig. 4).7,8,13 Moreover, CH-EUS plays an important role infinding a specific site within a lesion that would be moresuitable for EUS-FNA than other sites.14 Identification of theavascular sites in a lesion may help avoid sampling necroticareas and improve the sensitivity of EUS-FNA in the diag-nosis of pancreatic tumors.14
QUANTITATIVE PERFUSION ANALYSIS WITHTIME–INTENSITY CURVE DURING CH-EUS
FOR QUANTITATIVE PERFUSION analysis, a time–intensity curve (TIC) for region of interest (ROI) can be
generated during CH-EUS. Many variables are reported for aTIC, including the ratio of uptake inside the mass to uptakein the surrounding parenchyma, median intensity, maximumintensity, time to peak, area under the curve, and echointensity reduction rate.15–18 Imazu et al. reported thatmaximum intensity gain was the best variable to differentiate
a
b
c
Figure 2 Time course of contrast-enhanced harmonic endo-scopic ultrasonography (CH-EUS) images in a pancreas withoutany findings suggestive of lesions (pancreas head). (a) CH-EUSimage before infusion of the contrast agent. No signals frommicrobubbles can be observed. (b) CH-EUS image 13 s after infu-sion of the contrast agent. Spotty signals from microbubbles(arrows) and fine branching vessels (arrowheads) appear in thepancreas. (c) CH-EUS image 21 s after infusion of the contrastagent. Diffuse parenchymal perfusion of microbubbles can beimaged. The main pancreatic duct is depicted as an avascularstructure with strong contrast to the surrounding tissue (arrow).
62 M. Kitano et al. Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society

a
b
c
Figure 3 Typical images of pancreaticsolid tumors on contrast-enhanced har-monic endoscopic ultrasonography(EUS). (Left) Conventional EUS image.(Right) Contrast-enhanced harmonicEUS image. (a) Ductal carcinoma withhypo-enhancement. Conventional EUS(left) shows a hypoechoic area (arrow-heads) of 23 mm in diameter at the pan-creas tail. CH-EUS (right) indicates thatthe area has hypo-enhancement (arrow-heads) compared with the surroundingtissue. (b) Tumor-forming chronic pan-creatitis with iso-enhancement. Con-ventional EUS (left) shows a hypoechoicarea (arrowheads) of 22 mm in diameterat the pancreas head. CH-EUS (right)indicates that the area has homoge-neous enhancement similar to the sur-rounding tissue. The margin is notobserved on CH-EUS. (c) Neuroendo-crine tumor with hyper-enhancement.Conventional EUS (left) shows ahypoechoic area (arrowheads) of14 mm in diameter at the pancreas tail.CH-EUS (right) indicates that the areahas hyper-enhancement (arrowheads)compared with the surrounding tissue.
Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67 CH-EUS for pancreatobiliary diseases 63
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society

a
b
c
Figure 4 Contrast-enhanced harmo-nic endoscopic ultrasonography-guided fine-needle aspiration (CH-EUS-FNA for a subtle lesion in the pancreas.(a) Conventional EUS (left) shows asubtle hypoechoic lesion at the pan-creas body. CH-EUS (right) shows cleardemarcation between the lesion andthe surrounding tissue (arrowheads).(b) On real-time imaging with CH-EUS,the lesion with hypo-enhancement(arrowheads) is punctured with an EUS-FNA needle (arrow). (c) Histologicalexamination of samples obtained byCH-EUS-FNA shows relative non-cohesive, pleomorphic mononuclearcells admixed with multinucleated giantcells (arrow). The final diagnosis of thelesion is anaplastic carcinoma.
64 M. Kitano et al. Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society

autoimmune pancreatitis from pancreatic carcinoma with asensitivity of 100% and a specificity of 100%.15 On the otherhand, Matsubara et al. reported that the echo intensity reduc-tion rate from the peak at 1 min was greatest in pancreaticadenocarcinomas.16 They concluded that when TICs weregenerated during CH-EUS, sensitivity, specificity, and accu-racy increased to 95.8%, 92.6%, and 94.7%, respectively.16
Although the most reliable variable of TICs should be iden-tified by further large multicenter studies, this quantitativeperfusion analysis may be complementary to classificationaccording to enhancement patterns to characterize pancre-atic solid lesions.
DIFFERENTIATION OF MALIGNANT ANDBENIGN INTRADUCTAL PAPILLARYMUCINOUS NEOPLASMS WITHCONTRAST-ENHANCED EUS
EUS IS THE most sensitive method for detection of themural nodule in intraductal papillary mucinous neo-
plasms (IPMNs). Ohno et al. assessed whether enhance-ment patterns of contrast-enhanced EUS using colorDoppler mode differentiate malignant and benign IPMNs.19
In their report, mural nodules were classified into 4 typesaccording to the enhancement patters: low papillary nodule,polypoid nodule, papillary nodule and invasive nodule.19
When the presence of papillary module or invasive nodulewas diagnosed as evident of invasive IPMN, the sensitivity,specificity and accuracy were 84.2%, 79.4%, and 80.5%,respectively.19 Multivariable logistic regression analysisshowed that contrast (OR, 10.8) and symptomatic IPMNs(OR, 4.31) were significant for malignancy.19 They con-cluded that the type of mural nodules obtained by CE-EUSmay be the most reliable diagnostic method to differentiatemalignant from benign IPMNs. CH-EUS more clearlydepicts morphological structures of mural nodules withoutblooming artifacts than contrast-enhanced Doppler EUS(Fig. 5), and may be also useful for identification of inva-sive IPMNs.
CHARACTERIZATION OF GALLBLADDERLESIONS WITH CH-EUS
THREE ARTICLES REPORTED that characterization ofgallbladder diseases with CH-EUS.20–22 Imazu et al.
compared conventional EUS and CH-EUS for the differen-tial diagnosis of gallbladder wall thickening.20 In their report,the inhomogeneous enhanced pattern in CH-EUS was astrong predictive factor of malignant gallbladder wall thick-ening, and the overall accuracy for diagnosing malignantgallbladder wall thickening was significantly higher for
CH-EUS (94.4%) than for conventional EUS (73.1%).20
Choi et al. assessed the utility of CH-EUS for differentialdiagnosis between benign and malignant polyps of the gall-bladder.21 An irregular vessel pattern determined byCH-EUS aided the diagnosis of malignant polyps with asensitivity and specificity of 90.3% and 96.6%, respec-tively.21 The presence of perfusion defects, as determined byCH-EUS, was used to diagnose malignant polyps with asensitivity and specificity of 90.3% and 94.9%, respec-tively.21 In eight cases, management changed after carryingout contrast-enhanced EUS, suggesting that CH-EUSslightly improves diagnostic accuracy in comparison to con-ventional EUS.
STAGING OF PANCREATOBILIARY TUMORSWITH CH-EUS
FOR T-STAGING, IMAZU et al. compared conventionaltissue harmonic EUS and CH-EUS, and showed the
accuracy of CH-EUS (92.4%) was significantly higher thanthat for conventional tissue harmonic EUS (69.2%)(P < 0.05).23 In particular, CH-EUS was superior to conven-tional tissue harmonic EUS in terms of specificity for iden-tification of portal venous involvement.23 For N-staging,Kanamori et al. compared features of benign and malignantlymph nodes with contrast-enhanced Doppler EUS, andfound a defect of enhancement that diagnosed malignantlymph nodes with a sensitivity of 100% and a specificity of82%.24 The diagnostic ability of contrast-enhanced DopplerEUS was superior to the morphological classification based
Figure 5 Contrast-enhanced harmonic endoscopic ultrasonog-raphy (CH-EUS) image of an intraductal papillary mucinous neo-plasm. Slight dilatation of the main pancreatic duct (MPD; 4 mm)is observed at the pancreas head. There is a mural nodule withcontrast enhancement in the dilated duct (arrowheads).
Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67 CH-EUS for pancreatobiliary diseases 65
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society

on conventional EUS (sensitivity and specificity of 88% and77%, respectively).24 We previously assessed the CH-EUSimages of intra-abdominal lesions of undetermined origin,and classified these lesions into two types according toenhancement patterns: homogeneous (Fig. 6a) and heteroge-neous enhancement (Fig. 6b).25 The sensitivity and specific-ity with which CH-EUS differentiated malignant frombenign lesions were 96.3% and 100%, respectively, suggest-ing that CH-EUS is useful for N-staging of pancreatobiliarytumors.25
CONCLUSION
DEVELOPMENT OF CH-EUS technique allowed visu-alization of real-time perfusion imaging of the pancrea-
tobiliary system. CH-EUS improved ability of EUS indetection, characterization and staging of pancreatobiliarytumors. CH-EUS also complements EUS-FNA. However,
most studies were carried out in a small number of patientsby a single center. Further multicenter studies with largernumbers of patients would prove its utility.
CONFLICT OF INTERESTS
AUTHORS DECLARE NO conflict of interests for thisarticle.
REFERENCES
1 Kudo M. Various contrast-enhanced imaging modes afteradministration of Levovist. In: Kudo M (ed.). Contrast Har-monic Imaging in the Diagnosis and Treatment of HepaticTumors. Tokyo: Springer, 2003; 22–30.
2 Kitano M, Kudo M, Maekawa K et al. Dynamic imaging ofpancreatic diseases by contrast enhanced coded phase inversionharmonic ultrasonography. Gut 2004; 53: 854–9.
aa
b
a
b
Figure 6 Typical images of lymphnodes with contrast-enhanced har-monic endoscopic ultrasonography(EUS). (Left) Conventional EUS image.(Right) Contrast-enhanced harmonicEUS image. (a) Benign lymph node withhomogeneous enhancement. Conven-tional EUS (left) shows a lymph node of15 mm in diameter (arrowheads).Contrast-enhanced harmonic EUS(right) indicates that the lymph nodehas homogeneous enhancement(arrowheads). BD, bile duct; PV, portalvein. (b) Malignant lymph node withheterogeneous enhancement. Conven-tional EUS (left) shows a lymph node of21 mm in diameter (arrowheads).Contrast-enhanced harmonic EUS(right) indicates that the lymph nodehas heterogeneous enhancement(arrowheads).
66 M. Kitano et al. Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society

3 Kitano M, Kudo M, Sakamoto H et al. Preliminary study ofcontrast-enhanced harmonic endosonography with second-generation contrast agents. J. Med. Ultrason. 2008; 35: 11–8.
4 Quaia E. Classification and safety of microbubble-based con-trast agents. In: Quaia E (ed.). Contrast Media in Ultrasonog-raphy. Basic Principles and Clinical Applications. Berlin:Springer, 2005; 1–14.
5 Kitano M, Sakamoto H, Matsui U et al. A novel perfusionimaging technique of the pancreas: Contrast-enhanced har-monic EUS (with video). Gastrointest. Endosc. 2008; 67: 141–50.
6 Kitano M, Kudo M, Sakamoto H et al. Endoscopic ultrasonog-raphy and contrast-enhanced endoscopic ultrasonography. Pan-creatology 2011; 11 (Suppl 2): 28–33.
7 Fusaroli P, Spada A, Mancino MG et al. Contrast harmonicecho-endoscopic ultrasound improves accuracy in diagnosis ofsolid pancreatic masses. Clin. Gastroenterol. Hepatol. 2010; 8:629–34.
8 Kitano M, Kudo M, Yamao K et al. Characterization of smallsolid tumors in the pancreas: Contrast: The value of contrast-enhanced harmonic endoscopic ultrasonography. Am. J. Gastro-enterol. 2012; 107: 303–10.
9 Gincul R, Palazzo M, Pujol B et al. Contrast-harmonic endo-scopic ultrasound for the diagnosis of pancreatic adenocarci-noma: A prospective multicenter trial. Endoscopy 2014; 46:373–9.
10 Gong TT, Hu DM, Zhu Q. Contrast-enhanced EUS for differ-ential diagnosis of pancreatic mass lesions: A meta-analysis.Gastrointest. Endosc. 2012; 76: 301–9.
11 Napoleon B, Alvarez-Sanchez MV, Gincoul R et al. Contrast-enhanced harmonic endoscopic ultrasound in solid lesions ofthe pancreas: Results of a pilot study. Endoscopy 2010; 42:564–70.
12 Fusaroli P, Kypraios D, Mancino MG et al. Interobserver agree-ment in contrast harmonic endoscopic ultrasound. J. Gastroen-terol. Hepatol. 2012; 27: 1063–9.
13 Romagnuolo J, Hoffman B, Vela S et al. Accuracy of contrastenhanced harmonic EUS with a second-generation perflutrenlipid microsphere contrast agent (with video). Gastrointest.Endosc. 2011; 73: 52–63.
14 Kitano M, Sakamoto H, Komaki T et al. FNA guided bycontrast-enhanced harmonic EUS in pancreatic tumors. Gastro-intest. Endosc. 2009; 69: A328–A329.
15 Imazu H, Kanazawa K, Mori N et al. Novel quantitative perfu-sion analysis with contrast-enhanced harmonic EUS for differ-entiation of autoimmune pancreatitis from pancreaticcarcinoma. Scand. J. Gastroenterol. 2012; 47: 853–60.
16 Matsubara H, Itoh A, Kawashima H et al. Dynamic quantitativeevaluation of contrast enhanced endoscopic ultrasonography inthe diagnosis of pancreatic diseases. Pancreas 2011; 40:1073–9.
17 Gheonea DI, Streba CT, Ciurea T, Saftoiu A. Quantitative lowmechanical index contrast enhanced endoscopic ultrasound forthe differential diagnosis of chronic pseudotumoral pancreatitisand pancreatic cancer. BMC Gastroenterol. 2013; 13: 2.
18 Seicean A, Badea R, Stan-Iuga R, Mocan T, Gulei I, Pascu O.Quantitative contrast-enhanced harmonic endoscopic ultraso-nography for the discrimination of solid pancreatic masses.Ultraschall Med. 2010; 31: 571–6.
19 Ohno E, Hirooka Y, Itoh A et al. Intraductal papillary mucinousneoplasms of the pancreas: Differentiation of malignant andbenign tumors by endoscopic ultrasound findings of muralnodules. Ann. Surg. 2009; 249: 628–34.
20 Imazu H, Mori N, Kanazawa K et al. Contrast-enhanced har-monic endoscopic ultrasonography in the differential diagnosisof gallbladder wall thickening. Dig. Dis. Sci. 2014; 59: 1909–16.
21 Choi JH, Seo DW, Choi JH et al. Utility of contrast-enhancedharmonic EUS in the diagnosis of malignant gallbladder polyps(with videos). Gastrointest. Endosc. 2013; 78: 484–93.
22 Park CH, Chung MJ, Oh TG et al. Differential diagnosisbetween gallbladder adenomas and cholesterol polyps oncontrast-enhanced harmonic endoscopic ultrasonography. Surg.Endosc. 2013; 27: 1414–21.
23 Imazu H, Uchiyama Y, Matsunaga K et al. Contrast-enhancedharmonic EUS with novel ultrasonographic contrast (Sonazoid)in the preoperative T-staging for pancreaticobiliary malignan-cies. Scand. J. Gastroenterol. 2010; 45: 732–8.
24 Kanamori A, Hirooka Y, Itoh A et al. Usefulness of contrastenhanced endoscopic ultrasonography in the differentiationbetween malignant and benign lymphadenopathy. Am. J. Gas-troenterol. 2006; 101: 45–51.
25 Xia Y, Kitano M, Kudo M et al. Characterization of intra-abdominal lesions of undetermined origin by contrast-enhancedharmonic EUS (with video). Gastrointest. Endosc. 2010; 72:637–42.
Digestive Endoscopy 2015; 27 (Suppl. 1): 60–67 CH-EUS for pancreatobiliary diseases 67
© 2015 The AuthorsDigestive Endoscopy © 2015 Japan Gastroenterological Endoscopy Society