Continuous Doppler Echocardiographic Measurement of...
12
504 Continuous Wave Doppler Echocardiographic Measurement of Prosthetic Valve Gradients A Simultaneous Doppler-Catheter Correlative Study Darryl J. Burstow, MB, BS, FRACP, Rick A. Nishimura, MD, Kent R. Bailey, PhD, Guy S. Reeder, MD, David R. Holmes Jr., MD, James B. Seward, MD, and A. Jamil Tajik, MD Studies correlating prosthetic valve gradients determined by continuous wave Doppler echo- cardiography with gradients obtained by cardiac catheterization have, to date, been limited to patients with mitral and tricuspid prostheses or have compared nonsimultaneous measure- ments. Simultaneous Doppler and catheter pressure gradients in 36 patients (mean age, 63+13 years) with 42 prosthetic valves (20 aortic, 20 mitral, one tricuspid, and one pulmonary) were studied. Catheter gradients were obtained using a dual-catheter technique. The simultaneous pressure tracings and Doppler flow velocity profiles were digitized at 10 -msec intervals to derive the corresponding maximal and mean gradients. The correlation between the maximal Doppler gradient and the simultaneously measured maximal catheter gradient was 0.94 (SEE=6), and that between the Doppler gradient and the simultaneously measured mean catheter gradient was 0.96 (SEE=3). There were no significant differences in correlation between gradients for the 32 mechanical valves (maximal gradients: r=0.95, SEE=6; mean gradients: r=0.96, SEE=3) and the 10 bioprosthetic valves (maximal gradients: r=0.89, SEE=6; mean gradients: r=0.93, SEE =3). In patients with mitral prostheses, Doppler gradients correlated well with the corresponding catheter gradients obtained with direct measurement of left atrial pressure (maximal gradients: r=0.96, SEE=2; mean gradients: r=0.97, SEE=1.2). A close correlation between corresponding Doppler and catheter gradients also was found in patients with aortic prostheses (maximal gradients: r=0.94, SEE=6; mean gradients: r=0.94, SEE=3). Thus, continuous wave Doppler echocardiography can accurately predict the pressure gradient across prosthetic valves. (Circulation 1989;80:504-514) Daiagnosis of prosthetic valve dysfunction remains a clinical challenge. Earlier non- invasive techniques1-3were of limited suc- cess because of their relatively low specificity and their inability to provide quantitative hemodynamic information. However, the introduction of continu- ous wave Doppler echocardiography has provided a noninvasive method for determining transvalvular pressure gradients. The recording of transvalvular flow velocity (v) with continuous wave Doppler allows pressure gradient (P) to be determined with From the Division of Cardiovascular Diseases and Internal Medicine and the Section of Biostatistics, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Supported in part by a Research Grant from the Institute for Cardiovascular Research, Brisbane, Australia, and a Travel Grant from the National Heart Foundation of Australia. Address for reprints: Rick A. Nishimura, MD, Mayo Clinic, 200 First Street SW, Rochester, MN 55905. Received December 12, 1988; revision accepted April 18, 1989. the modified Bernoulli equation: P=4v2. The clini- cal accuracy of this technique has been validated in native valve stenosis,4 right and left ventricular outflow obstruction,5,6 and right-sided7 and left- sided8 regurgitant lesions. However, because of the unique geometry and flow characteristics of pros- thetic valves, the Doppler technique cannot be assumed to remain equally accurate for calculating See p 707 prosthetic valve gradients. To date, validation stud- ies in patients with prosthetic valves have been confined to a small number of patients with mitral and tricuspid prostheses.9 Moreover, limited and conflicting data10-12 available regarding the accu- racy of the Doppler measurements of transvalvular gradients in patients with aortic prostheses. Thus, the usefulness of continuous wave Doppler echocardiography for determining a wide range of prosthetic valve gradients has not been validated by by guest on May 9, 2018 http://circ.ahajournals.org/ Downloaded from
-
Upload
nguyenkiet -
Category
Documents
-
view
216 -
download
2
Transcript of Continuous Doppler Echocardiographic Measurement of...

504
Continuous Wave Doppler EchocardiographicMeasurement of Prosthetic Valve GradientsA Simultaneous Doppler-Catheter Correlative Study
Darryl J. Burstow, MB, BS, FRACP, Rick A. Nishimura, MD, Kent R. Bailey, PhD,Guy S. Reeder, MD, David R. Holmes Jr., MD,James B. Seward, MD, and A. Jamil Tajik, MD
Studies correlating prosthetic valve gradients determined by continuous wave Doppler echo-cardiography with gradients obtained by cardiac catheterization have, to date, been limited topatients with mitral and tricuspid prostheses or have compared nonsimultaneous measure-ments. Simultaneous Doppler and catheter pressure gradients in 36 patients (mean age, 63+13years) with 42 prosthetic valves (20 aortic, 20 mitral, one tricuspid, and one pulmonary) werestudied. Catheter gradients were obtained using a dual-catheter technique. The simultaneouspressure tracings and Doppler flow velocity profiles were digitized at 10 -msec intervals to derivethe corresponding maximal and mean gradients. The correlation between the maximal Dopplergradient and the simultaneously measured maximal catheter gradient was 0.94 (SEE=6), andthat between the Doppler gradient and the simultaneously measured mean catheter gradientwas 0.96 (SEE=3). There were no significant differences in correlation between gradients forthe 32 mechanical valves (maximal gradients: r=0.95, SEE=6; mean gradients: r=0.96,SEE=3) and the 10 bioprosthetic valves (maximal gradients: r=0.89, SEE=6; mean gradients:r=0.93, SEE=3). In patients with mitral prostheses, Doppler gradients correlated well with thecorresponding catheter gradients obtained with direct measurement of left atrial pressure(maximal gradients: r=0.96, SEE=2; mean gradients: r=0.97, SEE=1.2). A close correlationbetween corresponding Doppler and catheter gradients also was found in patients with aorticprostheses (maximal gradients: r=0.94, SEE=6; mean gradients: r=0.94, SEE=3). Thus,continuous wave Doppler echocardiography can accurately predict the pressure gradient acrossprosthetic valves. (Circulation 1989;80:504-514)
Daiagnosis of prosthetic valve dysfunctionremains a clinical challenge. Earlier non-invasive techniques1-3were of limited suc-
cess because of their relatively low specificity andtheir inability to provide quantitative hemodynamicinformation. However, the introduction of continu-ous wave Doppler echocardiography has provided anoninvasive method for determining transvalvularpressure gradients. The recording of transvalvularflow velocity (v) with continuous wave Dopplerallows pressure gradient (P) to be determined with
From the Division of Cardiovascular Diseases and InternalMedicine and the Section of Biostatistics, Mayo Clinic and MayoFoundation, Rochester, Minnesota.
Supported in part by a Research Grant from the Institute forCardiovascular Research, Brisbane, Australia, and a TravelGrant from the National Heart Foundation of Australia.Address for reprints: Rick A. Nishimura, MD, Mayo Clinic,
200 First Street SW, Rochester, MN 55905.Received December 12, 1988; revision accepted April 18, 1989.
the modified Bernoulli equation: P=4v2. The clini-cal accuracy of this technique has been validated innative valve stenosis,4 right and left ventricularoutflow obstruction,5,6 and right-sided7 and left-sided8 regurgitant lesions. However, because of theunique geometry and flow characteristics of pros-thetic valves, the Doppler technique cannot beassumed to remain equally accurate for calculating
See p 707
prosthetic valve gradients. To date, validation stud-ies in patients with prosthetic valves have beenconfined to a small number of patients with mitraland tricuspid prostheses.9 Moreover, limited andconflicting data10-12 available regarding the accu-racy of the Doppler measurements of transvalvulargradients in patients with aortic prostheses.
Thus, the usefulness of continuous wave Dopplerechocardiography for determining a wide range ofprosthetic valve gradients has not been validated by
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

Burstow et al Doppler-Catheter Correlative Study 505
simultaneous measurement of transvalvular gradi-ents at cardiac catheterization. Therefore, we pro-spectively studied 36 patients at the time of cardiaccatheterization to assess the accuracy of the con-tinuous wave Doppler technique.
MethodsPatientsThe study group consisted of 36 patients (15 men,
21 women) ranging in age from 44 to 80 years(mean, 63±13 years) who were scheduled for clin-ically indicated cardiac catheterization. In 23patients, prosthetic valve dysfunction was sus-pected clinically. The remaining 13 patients under-went cardiac catheterization for evaluation of cor-onary artery disease or of a valve other than theprosthetic valve; in these patients, a complete hemo-dynamic assessment of the prosthetic valve wasthought to be warranted. Six of these patients hadtwo prosthetic valves. Thus, a total of 42 prostheticvalves were studied: 20 aortic prostheses, 20 mitralprostheses, one tricuspid prosthesis, and one pul-monary prosthesis. Of the 42 prostheses studied, 32were mechanical (15 Starr-Edwards, seven Bjork-Shiley, four Braunwald-Cutter, two Hall-Medtronic,two St. Jude, one Sorin, and one Smeloff-Cutter),and 10 were bioprosthetic (five Hancock, twoIonescu-Shiley, two Carpentier-Edwards, and oneDura Mater). Sixteen patients were in atrial fibril-lation, 13 in sinus rhythm, six in paced rhythm, andone in second-degree atrioventricular block. Com-prehensive two-dimensional and Doppler echocar-diography had been performed on all patients beforecardiac catheterization.
Continuous Wave Doppler TechniqueAll Doppler examinations were performed during
cardiac catheterization, and continuous wave Dopp-ler flow velocities and transvalvular pressure gradi-ents were recorded simultaneously. The study wasapproved by the Mayo Institutional Review Board,and informed consent was obtained from each patientbefore inclusion in the study. Doppler flow veloci-ties were recorded with an Irex Model 3B (UpperSaddle River, New Jersey) or Hewlett-PackardModel 77020 echocardiographic instrument (PaloAlto, California) using a nonimaging 2.0-MHz trans-ducer. Immediately before cardiac catheterization,a screening Doppler examination was performed toidentify the acoustic window from which the max-imal flow velocity could be obtained. For aorticprostheses, recording of flow velocities wasattempted from suprasternal, right parasternal, andapical windows. For mitral and tricuspid prosthe-ses, the apical and left parasternal windows wereused. For the pulmonary prosthesis, the left paraster-nal and suprasternal windows were used.
Cardiac Catheterization TechniqueDiazepam (2.5-15 mg i.v.) was used for sedation
during catheterization. Fluid-filled catheters (7F or8F) connected to strain-gauge pressure transducers(Gould P231D, Cleveland, Ohio) were used forpressure measurement. All pressure measurementswere recorded, with a direct-current coupler, simul-taneously with the Doppler spectral signal on acalibrated strip-chart recorder at paper speeds of 50and 100 mm/sec. The presence or absence of pros-thetic valve regurgitation was evaluated by contrastangiography after hemodynamic recordings werecompleted.Aortic prostheses. In all 20 patients with aortic
prostheses, the transvalvular pressure gradient wasmeasured by dual-catheter technique with simulta-neous recording of left ventricular and ascendingaortic pressures. Of these 20 patients, 15 had theleft ventricular pressure recorded by transseptaltechnique, and five underwent transthoracic leftventricular puncture because of the presence of amitral prosthesis.
Mitralprostheses. In all 20 patients with a mitralprosthesis, transvalvular pressure gradient was mea-sured by dual-catheter technique. In 12 of thesepatients, left atrial pressure was measured directlyby transseptal technique; in the remaining eightpatients, pulmonary capillary wedge pressure wasmeasured. In each case, wedge pressure measure-ments were confirmed by lower phasic and meanpressures compared with the pulmonary artery andby oxygen saturation of 95% or more. Left ventric-ular pressure was obtained simultaneously by ret-rograde crossing of the aortic valve in 14 patientsand by transthoracic left ventricular puncture in fivepatients because of the additional presence of anaortic prosthesis. In the remaining patient, who alsohad an aortic prosthesis, the mitral bioprosthesiswas crossed antegrade by the transseptal techniquewith a double-lumen, dual-port catheter in whichthe proximal port measured left atrial pressurewhile the distal port simultaneously measured leftventricular pressure.
Tricuspid andpulmonary prostheses. The patientwith the tricuspid prosthesis underwent right atrialcatheterization through the femoral vein and a simul-taneous transthoracic right ventricular puncture. Inthe patient with the pulmonary prosthesis, the trans-valvular gradient was measured by inserting twocatheters into the femoral vein: one placed ante-grade across the prosthesis and one in the rightventricular outflow tract.
Data AnalysisThe simultaneous catheter and Doppler flow veloc-
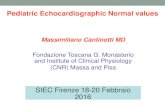
ity recordings were digitized manually on a com-puter system, as previously described.13 The instan-taneous pressure and Doppler flow velocities wereanalyzed at 10-msec intervals (Figure 1). With themodified Bernoulli equation (pressure gradient=4v2,
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

506 Circulation Vol 80, No 3, September 1989
100 200 300
Time, msec
FIGURE 1. Method used for analysis ofDoppler spectral envelopes. Panel A: Simultaneous Doppler-catheter pressurerecordings in a patient with a stenotic mitral Hancock prosthesis. Pressure gradient was measured with dual-cathetertechnique with catheters in left atrium (LA) and left ventricle (LV). Simultaneous Doppler flow velocity was recordedfrom apical transducer position with maximal velocity of 2.9 mlsec, giving a maximal Doppler gradient of 34 mm Hg.Panel B: Plot of digitization of Doppler flow velocity and left ventricular plus left atrial pressure waveforms shown inPanel A at 10-msec intervals. Phase delay of catheter (Cath) gradient compared with Doppler gradient is related to
fluid-filled catheter system. Note irregularity in contour ofcatheter gradient curve, which is related to irregularities in leftatrial and left ventricular waveforns in Panel A. Maximal catheter gradient was 31 mm Hg, and maximal Dopplergradient was 34 mm Hg. Mean gradients were obtained by calculating arithmetic mean of instantaneous pressure
gradients. Mean catheter gradient was 18 mm Hg, and mean Doppler gradient was 20 mm Hg.
in which v=velocity in meters per second), theinstantaneous Doppler velocities were then con-verted to instantaneous pressure gradients. Withthese data, maximal and mean gradients derived byboth continuous wave Doppler and catheterizationwere obtained for each patient. For aortic prosthe-ses, the widely used peak-to-peak gradient was alsoobtained by subtracting peak aortic systolic pres-sure from peak left ventricular systolic pressureobtained at cardiac catheterization. In patients withmitral prostheses in whom pulmonary capillarywedge pressure was measured, the catheter gradi-ents were also calculated before and after correc-tion for phase delay in the wedge pressure tracing.To correct for phase delay, the pulmonary capillarywedge tracing was shifted leftward until the peak ofthe V wave was bisected by the rapid downstroke ofthe left ventricular pressure decline as suggested byCarabello and Grossman.14 Mean values for cathe-ter and Doppler gradients were obtained by averag-ing five representative cardiac cycles.
Statistical AnalysisData are expressed as mean+SD. The correlation
between Doppler and catheterization gradients was
assessed by linear regression analysis with a leastsquares method. The variation between Dopplerand catheter gradients was evaluated by calculatingthe signed (+ or -) differences between the Dopp-ler and the corresponding catheter gradients. Theeffect of valve subtype (mechanical compared withtissue) and catheterization technique (pulmonarycapillary wedge compared with transseptal) on thevariation between Doppler and catheter gradientswas assessed by comparing the signed differencesfor each subgroup with a paired Student's t test. Ap value less than 0.05 was considered statisticallysignificant. Finally, the beat-to-beat correlationbetween Doppler and catheter gradients within indi-vidual patients was also assessed. This was done bycalculating, in each patient, the signed differencesbetween each of the five single gradient measure-
ments and the mean value of that measurement(obtained by averaging the five gradient measure-
ments). The signed differences from the mean (termed"cresiduals") were obtained for each Doppler andeach corresponding catheter gradient selected foranalysis. Thus, the residuals represent the directionand magnitude of beat-to-beat variation in the gradi-ent measurements from the mean value in an indi-
A B40
I
(_EEC
UGcu
Mcm
0)a-
30
20
10
00 400
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

Burstow et al Doppler-Catheter Correlative Study 507
B
* MechanicalA Bioprosthetic
S
0A
c)IEE
0~0-0CLa)
0)COCD
0)
.
n =42r=0.94SEE = 6
40
30
20
10
020 40 60 80
* MechanicalA Bioprosthetic
0
.0
.
A0
l
n =42r=0.96SEE = 3
10 20 30 40
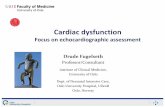
Max gradient (cath), mm Hg Mean gradient (cath), mm HgFIGURE 2. Correlation between Dopplergradients and simultaneous catheter (cath) gradients in all 42prostheses. PanelA: Plot of maximal (Max) gradients. Regression equation is Doppler gradient=1. 09xcatheter gradient-3.3. Panel B:Mean gradients. Regression equation is Doppler gradient=1. 03 xcatheter gradient-1. 2. Dotted line, regression line;solid line, line of identity.
vidual patient. The correlation between the Dopplergradient residuals and the catheter gradient residualswas assessed with linear regression analysis.
ResultsContinuous Wave Doppler RecordingsThe maximal systolic velocities recorded across
the aortic and pulmonary prostheses ranged from1.9 to 4.3 m/sec (mean, 3.1±0.6 m/sec). The acous-tic window from which the maximal velocity wasobtained was apical in 18 patients, suprasternal intwo patients, and left parasternal in the patient withthe pulmonary prosthesis. For mitral and tricuspidprostheses, the maximal diastolic velocities recordedranged from 1.4 to 2.9 m/sec (mean, 2.0±0.4 m/sec).The maximal velocity was obtained from the apicalwindow in all cases.
Correlation of Simultaneous Doppler andCatheter Pressure GradientsThe maximal Doppler gradients ranged from 8 to
74 mm Hg (mean, 29±17 mm Hg), and the simulta-neous maximal gradients measured by catheterranged from 8 to 70 mm Hg (mean, 29+15 mm Hg).The correlation between maximal Doppler gradientand the simultaneously obtained maximal cathetergradient was highly significant (r=0.94, SEE=6)(Figure 2A). The mean Doppler gradients rangedfrom 2.6 to 42 mm Hg (mean, 14±10 mm Hg), andthe mean pressure gradients measured by catheterranged from 3.6 to 40 mm Hg (mean, 15 + 10mm Hg).These gradients also showed close correlation(r=0.96, SEE=3) (Figure 2B). A low cardiac indexor the presence of significant prosthetic valve regur-gitation did not affect the correlation betweencatheter- and Doppler-derived maximal or mean
gradients (Tables 1 and 2).
In individual patients, there was good beat-to-beat correlation between Doppler and catheterpressure gradients, including those with irregularrhythm. In the 16 patients with atrial fibrillation, theDoppler gradient residuals correlated well with thecatheter gradient residuals for both maximal (r=0.91)and mean (r=0.87) gradients, an indication of closetracking of the catheter gradient by the Dopplergradient despite varying RR intervals.Aortic prosthetic valve gradients. The maximal
Doppler gradients ranged from 15 to 74 mm Hg(mean, 40±+17 mm Hg), and the simultaneous max-
imal gradients measured by catheter ranged from 13to 70 mm Hg (mean, 39+14 mm Hg) (Table 1,Figure 3). The correlation coefficient for maximalDoppler and catheter gradients was 0.94 (SEE=6)(Figure 4A). The mean Doppler gradients rangedfrom 9 to 42 mm Hg (mean, 22±10 mm Hg), and themean pressure gradient measured by catheter rangedfrom 6 to 40 mm Hg (mean, 22±9 mm Hg). For themean aortic gradients, the correlation coefficientwas 0.94 (SEE=3) (Figure 4B). The Doppler gradi-ents reliably estimated the corresponding cathetergradients; the mean difference between the maximalgradients was 1±6 mm Hg (range, -10 to +13mm Hg), and that between the mean gradients was-0.1 ±3 mm Hg (range, -6 to +6 mm Hg) (Table 3).Peak-to-peak gradient measured by catheteriza-
tion ranged from 1 to 39 mm Hg (mean, 14±10mm Hg) and was consistently lower than maximalDoppler and maximal catheter gradients (Table 3).The correlation between peak-to-peak catheter gra-dient and maximal Doppler gradient was 0.72(SEE= 11) (Figure 5A). Overall, the correlationbetween peak-to-peak gradient and mean Dopplergradient was 0.74 (SEE=6) (Figure SB).Mitral prosthetic valve gradients. The catheter-
derived transmitral gradients were obtained from
A80
60
40
20
c)IEEa)
a.
c:
0
'c
CO
CD0cc
0
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

508 Circulation Vol 80, No 3, September 1989
TABLE 1. Doppler and Catheter Data From 21 Patients With Aortic and Pulmonary Prostheses
Gradient (mm Hg)
Age (yr)/ Size Maximal Mean p pCPatient sex Prosthesis type (mm) Cath Dopp Cath Dopp gradient Regurg (1/min/m2)
1 69/F Starr-Edwards 14A 31 22 26 12 13 6 1.92 69/F Starr-Edwards 9A 23 27 27 14 14 6 2.23 50/M Starr-Edwards 12A 27 33 33 15 16 9 Severe 1.64 67/M Starr-Edwards 11A 26 36 36 22 21 15 - 2.15 71/F Starr-Edwards 9A 23 39 46 20 22 10 - 2.66 70/M Starr-Edwards 1OA 24 48 61 27 33 20 - 1.77 58/F Starr-Edwards 9A 23 54 56 28 32 20 - 3.38 59/M Starr-Edwards 8A 21 58 62 38 37 25 - 3.89 47/M Starr-Edwards 11A 26 62 74 36 42 24 Moderate 3.310 67/F Bjork-Shiley 21 38 36 20 17 9 Mild 2.211 69/M Bjork-Shiley 23 70 66 40 36 39 Mild 2.012 77/M Bjork-Shiley 23 47 42 24 21 15 Moderate 1.113 80/F St. Jude 21 33 23 16 12 6 NA14 73/F St. Jude 21 30 31 14 15 19 Mild 1.415 80/F Braunwald-Cutter 22 38 40 19 19 9 4.516 54/M Hall-Medtronic 23 13 15 6 9 2 Mild 2.217 60/M Sorin 23 27 20 13 10 1 1.918 68/F Hancock 23 24 22 13 12 1 Mild 2.019 47/F Hancock 27 37 32 25 19 25 Mild 0.820 62/M Hancock 23 50 58 30 33 21 Mild 4.721 63/F Ionescu-Shiley (PVR) 25 34 31 22 18 20 Moderate 1.9
Cath, catheter-derived; Dopp, Doppler-derived; P-P, peak-to-peak gradient; CI, cardiac index derived by cardiac catheterization(indocyanine green dye dilution technique); PVR, pulmonary valve replacement; Regurg, regurgitation; NA, not available.
both direct (transseptal technique) and indirect (pul-monary capillary wedge pressure) measurements ofleft atrial pressure. Thus, results were analyzedseparately according to the catheterization tech-nique (Table 2).For the subgroup of 12 patients in whom left atrial
pressure was measured directly with transseptaltechnique, the maximal Doppler gradients rangedfrom 13 to 33 mm Hg (mean, 19+7 mm Hg), and thesimultaneous maximal gradients measured with cath-eter ranged from 13 to 28 mm Hg (mean, 18±5mm Hg). The correlation coefficient for maximalDoppler and catheter gradients was 0.96 (SEE=2)(Figure 6A). Mean gradients derived by Dopplertechnique ranged from 4.0 to 19.0 mm Hg (mean,7.8±4.5 mm Hg), whereas the mean gradients mea-sured simultaneously with catheter ranged from 4.2to 16 mm Hg (mean, 7.8±4.0 mm Hg). For meangradients, the correlation coefficient was 0.97(SEE=1.2) (Figure 6B). Again, the Doppler gradi-ents showed little variation from the correspondingcatheter gradients; the mean difference between themaximal gradients was 1±2 mm Hg (range, -3 to+5 mm Hg), and that between the mean gradientswas 0.1 ± 1 mm Hg (range, -2 to 3 mm Hg) (Table 3).For the subgroup of eight patients in whom left
atrial pressure was measured indirectly by pulmo-nary capillary wedge pressure, the maximal Dopp-ler gradients ranged from 9 to 31 mm Hg (mean,16±7 mm Hg), and the simultaneous maximal gra-
dients measured with catheter ranged from 17 to 33mm Hg (mean, 24±7 mm Hg). The correlation coef-ficient for maximal gradient was 0.67 (SEE=5.2),which was lower than the correlation obtained withthe transseptal technique (Figure 6A and 7). TheDoppler mean gradients ranged from 2.6 to 10.0mm Hg (mean, 5.4±2.3 mm Hg), and the simulta-neous mean gradients measured by catheter rangedfrom 3.6 to 13.0 mm Hg (mean, 8.6+2.9 mm Hg).For mean gradient, the correlation coefficient was0.44 (SEE=2.2), which, as with the maximal gradi-ent, was lower than that obtained with the transsep-tal technique (Figures 6B and 7).There was also greater variation between the
Doppler and catheter gradients obtained using wedgepressure recordings when compared with the resultsobtained using the transseptal technique (Table 3).For the former, the Doppler gradients were consis-tently lower than the corresponding catheter gradi-ent; the mean difference between maximal gradientswas -7±6 mm Hg (range, -15 to +1 mm Hg), andthat between mean gradients was -3±3 mm Hg(range, -9 to -1 mm Hg). With correction forphase delay in the pulmonary capillary wedge pres-sure, the correlation coefficient for maximal gradi-ents improved to 0.87 (SEE=3.3), and the correla-tion coefficient for mean gradients improved to 0.83(SEE= 1.4). However, the variation between gradi-ents remained significantly greater than that obtainedwith the transseptal technique (Table 3).
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

Burstow et al Doppler-Catheter Correlative Study 509
TABLE 2. Doppler and Catheterization Data From 21 Patients With Mitral and Tricuspid Prostheses
Prosthesis type
Starr-Edwards 3MStarr-Edwards 3MStarr-Edwards 3MBjork-ShileyBjork-ShileyBjork-ShileyHancockHancock
54/M Hall-Medtronic71/F Smeloff-Cutter54/F Ionescu-Shiley
Carpentier-EdwardsStarr-Edwards 3MStarr-Edwards 3MStarr-Edwards 3MBraunwald-CutterBraunwald-CutterBjork-ShileyCarpentier-EdwardsDura-MaterBraunwald-Cutter (TVR)
Size(mm)303030
Cathetertechnique
TS Wedge
+
25 +31 +29292927312731303030343231273132
+
+
+
+
+
+
+
+
Gradient (mm Hg)
Maximal
Cath Dopp
13 1418 1828 32
Mean
Cath Dopp
4.2 4.05.2 4.8
14.8 13.0
Regurg
Mild12 13 5.8 4.8 Severe15 1713 1228 3320 2219181516221722
1519171616139
6.24.2
16.010.86.05.28.46.26.47.87.8
6.44.0
19.011.05.05.48.47.25.66.23.0
Severe
MildModerateMildMildMildSevere
Mild
CI(I/min/M2)
2.23.01.53.31.32.22.02.22.22.62.12.23.12.62.2
+ 24 17 8.4 5.4 Moderate 1.9+ 28 13 13.0 4.2 - 4.5+ 12 12 3.6 2.6 - NA+ 30 18 10.8 5.8 - 2.3+ 33 31 10.8 10.0- 8 8 4.2 4.0
Moderate 3.02.7
TS, transseptal; Cath, catheter-derived; Dopp, Doppler-derived; Regurg, regurgitation; TVR, tricuspid valve replacement; CI, cardiacindex derived by cardiac catheterization (indocyanine green dye dilution technique); NA, not available.
Mechanical compared with tissue prostheses.When tissue valves (n=10) and mechanical valves(n=32) were analyzed separately, the correlationbetween Doppler and catheter gradients was similarfor both prosthetic valve subtypes. For maximalgradients, the correlation coefficient was 0.89(SEE=6) for tissue valves and 0.95 (SEE=6) formechanical valves. For mean gradients, the corre-lation coefficient was 0.93 (SEE=3) for tissue valvesand 0.96 (SEE=3) for mechanical valves. In addi-tion, the mean difference between the Doppler andcatheter gradients was similar in both subgroups formaximal and mean gradients (Table 3).
Clinical OutcomeOf the 42 prosthetic valves, 26 were categorized
as functioning normally on the basis of the Dopplerand cardiac catheterization evaluation. Nine of thesevalves were inspected by the surgeon at operation,which was being performed for other reasons(replacement of other valves in seven patients,coronary bypass grafting in one patient, repair ofatrial septal defect in one patient); all nine valveswere regarded as normal by the surgeon. Seventeenvalves were in patients who were thought clinicallyto have normal-functioning valves and who did notundergo operation.Seven prosthetic valves were diagnosed as hav-
ing hemodynamically significant obstruction by bothDoppler and cardiac catheterization. Five of these
valves were replaced at reoperation (three, tissuevalve leaflet calcification; two, mechanical valvethrombosis). Two valves were in patients who wereasymptomatic and thought to have a moderatedegree of obstruction, for which medical observa-tion was elected.
In nine patients, the prosthetic valves were shownto have hemodynamically significant regurgitation.This condition was diagnosed by contrast angiogra-phy in eight instances. The comprehensive two-dimensional and Doppler examination performedbefore the study had identified seven patients whohad valves with significant regurgitation, one ofwhom underwent reoperation without contrast angi-ography. Eight of these nine patients underwentreoperation for regurgitation (tissue valve leaflet tearin four and valve dehiscence in four). One patientwith moderate regurgitation was treated medically.
DiscussionPrevious studies have shown the accuracy of
continuous wave Doppler echocardiography for thedetermination of transvalvular pressure gradients inpatients with native valve disease.4,5,8 However, theclinical accuracy of the Doppler technique for deter-mining prosthetic valve gradients has remained con-
troversial. The modified Bernoulli equation (P=4v2)excludes the effects of viscous friction, which isconsidered negligible in native valves.15 For thecomplex and multiple orifices of various prosthetic
Age (yr)/sex
69/F44/F71/M64/F77/M72/F67/F68/F
Patient
222324252627282930313233343536373839404142
67/F54/M61/F72/F74/M80/F66/M56/F67/F73/F
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

510 Circulation Vol 80, No 3, September 1989
1B*ork - Shiley
37
mean40
41 mis..EX7* n:ean67
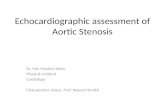
FIGURE 3. Simultaneous Doppler-catheterpressure recordingsfiom threepatients with three different aortic valve types(Panel A: Starr-Edwards; Panel B: Hancock, and Panel C: Bjoirk-Shiley) in whom left ventricular and ascending aorticpressure measurements were obtained with dual-catheter technique. Note close correlation between Doppler- andcatheter-derived maximal (max) and mean gradients throughout a broad range ofmeasured gradients. Thepeak-to-peak(p-p) gradients are lower than both the maximal and the mean gradients.
valves, this assumption may not be valid. In addi-tion, no comprehensive clinical study has corre-lated Doppler-derived pressure gradients with simul-taneous catheter-derived gradients in a large numberof patients with prosthetic valves.
Initial in vitro studies with multiple irregularobstructions16 and later prosthetic valves17,'1 showedgood correlation between Doppler-derived and man-ometric pressure gradients, although the correlationseemed to vary with the type and size of prosthesisin the report of Yoganathan et al.17 Thus far, clinicalvalidation studies have been confined to a smallnumber of patients with mitral and tricuspid pros-theses. Wilkins et a19 reported a close correlationbetween Doppler- and catheter-derived mean gradi-ents in 13 patients with mitral or tricuspid prosthe-ses. However, studies in patients with aorticprostheses10,12 have compared Doppler-derived gra-
dients with nonsimultaneous catheter-derived gra-dients, and the results have been conflicting. Thus,because of the limited data available and the reportedvariation in correlation between Doppler- andcatheter-derived gradients, we studied a large groupof patients with prostheses ofvarious types (mechan-ical and tissue) and in various intracardiac posi-tions. To show a beat-to-beat and instantaneousrelation, we used a dual-catheter technique and adirect-current coupler, which permitted superimpo-sition of calibrated catheter pressures and simulta-neously recorded Doppler signals.The present study documents that continuous
wave Doppler echocardiography accurately mea-
sures transvalvular pressure gradients across pros-thetic valves, irrespective of valve type and posi-tion. Both maximal and mean gradients determinedby the Doppler technique correlated closely with
A B
HancockC
r150
max.70
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

Burstow et al Doppler-Catheter Correlative Study 511
B0 / E~0
E
7 a~~~~~-Z/ a~~~~~~~~~~~..0.
e, 0
1 c~*0)
0~~~~n20 ~~~~~~~~~~CDr=0.94SEE=6 E
0
0 20 40 60 80
40
30
20
10
0
.
.
*. 4
0
n =20r=0.94SEE =3
0 10 20 30 40
Aortic max gradient (cath), mm Hg Aortic mean gradient (cath), mm Hg
FIGURE 4. Correlation between Doppler gradients and simultaneous catheter (cath) gradients for 20 aortic prostheses.Panel A: Plot ofmaximal (max) gradients. Regression equation is Dopplergradient=1. 12xcathetergradient-3. 9. PanelB: Plot of mean gradients. Regression equation is Doppler gradient=1.01 xcatheter gradient-0.34. Dotted line,regression line; solid line, line of identity.
the corresponding simultaneous catheter-derivedgradients. As expected, the peak-to-peak gradientcalculated for aortic prostheses correlated less wellwith the maximal and the mean Doppler gradients.Doppler-derived velocities represent an instanta-neous pressure relation and therefore would not beexpected to correlate with peak-to-peak gradient,which is obtained by arbitrarily subtracting twononsimultaneous peak pressures.
This study also showed a significant difference inthe correlation between Doppler- and catheter-derived transmitral gradients obtained with pulmo-nary capillary wedge pressure measurement andbetween Doppler- and catheter-derived transmitralgradients obtained with direct left atrial pressuremeasurement. A previous study by Schoenfeld eta119 showed that use of pulmonary capillary wedgepressure can result in overestimation of the trans-mitral gradients in patients with mitral prostheses.They proposed that these findings might be causedby the phase delay of the pulmonary wedge V waverelative to the transseptal V wave, resulting in a
higher mean diastolic pressure and higher gradient.In addition, the pulmonary capillary wedge pres-sure tracing also lacks the fidelity for rapid acceler-ation and deceleration, being a reflected pressure.This might also have contributed to the lack ofcorrelation. With correction for phase delay, thecorrelation of mean gradients improved, but thevariation between the Doppler and catheter gradi-ents remained significantly greater than that obtainedwith the transseptal technique. Our findings furtherindicate the inaccuracy of using pulmonary capil-lary wedge pressure to calculate transvalvular gra-dients in patients with mitral prostheses.The methods used in this study have several
potential limitations. Doppler examination was per-formed using a nonimaging transducer without anglecorrection. Failure to obtain a small or zero anglebetween the Doppler beam and transvalvular flowwill underestimate the valve gradient. However, thegood correlation between Doppler and cathetergradients obtained in this study shows that a metic-ulous examination using multiple transducer posi-
TABLE 3. Mean Differences Between Doppler and Catheter Gradients for Total Group and Various Subgroups
Mean differences (mm Hg)
MitralTotal Mitral Mitral PCWgroup Aortic TS PCW corrected Mechanical Tissue(n =42) (n =20) (n= 12) (n =8) (n =8) (n=32) (n= 10)
Max Dopp-max cath gradient -1+6 1±6 1+2 -7+6* -4+4* -1+6 -1+6
Mean Dopp-mean cath gradient -1+3 -0.1+3 0.1+1 -3+3* -2+1* -1+3 -1+3
Max Dopp-P-P cath gradient - 27+12 -
Mean Dopp-P-P cath gradient - 8±7 - - - - -
TS, catheter gradients measured with transseptal technique; PCW (corrected), catheter gradients measured with pulmonary capillarywedge pressure corrected for phase delay; PCW, catheter gradients measured with pulmonary capillary wedge pressure; max, maximal;Dopp, Doppler; Cath, catheter; P-P, peak-to-peak.
*p<0.01 compared with mitral (TS) group.
AC)EEE
a-00.C
.n
*0
0)
E
0D:
80
60
40
20
0
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

512 Circulation Vol 80, No 3, September 1989
B
* E.// E
l /an = 200~~~~~~~
0/ 0
/ SEE -11Q00/ 0
C
n=20 ccr=0.72 (D
SEE= 1E
0 20 40 60 80 .
40
30
20
10
0
.
0
0 0
0
.
n=20r=0.74SEE = 6
V I I I0 10 20 30 40
Aortic peak-to-peak gradient (cath), mm Hg Aortic peak-to-peak gradient (cath), mm HgFIGURE 5. Correlation between Doppler gradients and simultaneous catheter (cath) gradients in 20 aortic valveprostheses. Panel A: Plot of correlation between peak-to-peak catheter gradient and maximal (max) Doppler gradient.Regression equation is Dopplergradient=1.2xcathetergradient+22. Panel B: Plot ofcorrelation between peak-to-peakcatheter gradient and mean Doppler gradient. Regression equation is Doppler gradient=0. 75xcatheter gradient+11.Dotted line, regression line; solid line, line of identity.
tions can reduce this error to a minimum. Themodified Bernoulli equation assumes that the veloc-ity proximal to the valve is small relative to the peaktransvalvular velocity and thus can be ignored. Inaortic prostheses, the left ventricular outflow tractvelocity can be elevated in patients with significantaortic regurgitation. If this velocity is ignored, over-estimation of the pressure gradient can result. In thisstudy, 11 (55%) aortic prostheses had regurgitation,but it was moderate or severe in only two (10%).Thus, it is unlikely that this factor adversely affected
Ac)mEE
.-ZL..
0
0
a.0
0
c:0)
E
-fi
30
20
10
0
PCWn=8r=0.67SEE = 5.2
the correlation obtained in this study. In any correla-tive study, the accuracy and limitations of the refer-ence standard need to be considered. Fluid-filledcatheters, as used in this study, may not measuretransvalvular gradients accurately because of catheter-induced artifact and phase delays. The use of high-fidelity, manometer-tip catheters might have furtherimproved the correlation between Doppler and cath-eter gradients, especially for maximal gradients, inwhich a small phase delay can result in major differ-ences in the measured gradient. When possible, cath-
BCDI
E
E
1-
0
0.
0a0
0
0)
C
CD0E
20
15
10
5
0
* TSA PCW
n- TSOXol A n= 12
A r=0.97
/ SEE= 1.2
0 5 10 15 X
PCWn=8r=0.44SEE = 2.2
220
Mitral max gradient (cath), mm Hg Mitral mean gradient (cath), mm HgFIGURE 6. Correlation between Doppler gradients and simultaneous catheter (cath) gradients in 20 mitralprostheses.PCW, catheter gradients obtained with pulmonary capillary wedge pressure technique; TS, catheter gradients obtainedwith transseptal technique. Panel A: Plot of maximal (max) gradients. Regression equation (TS) is Dopplergradient=1.22xcatheter gradient-3.1. Regression equation (PCW) is Doppler gradient=0. 62xcatheter gradient+1.5.Panel B: Plot ofmean gradients. Regression equation (TS) is Dopplergradient=1. 1 xcathetergradient-0. 7. Regressionequation (PCW) isDopplergradient=0.34xcathetergradient+2.4. Dotted line, regression line; solid line, line ofidentity.
ACDz:IEE-
E..0~aCL00
E._a
0
0m9
80
60
40
20
0
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

Burstow et al Doppler-Catheter Correlative Study 513
AMitral Starr-Edwards Prosthesis
. I. a a a * .a * a a ** g ae *M a . . a 0 a .* 0 a # J a . * a * . a a a 0 . *9
B
4IProsthesis
en~ L
FIGURE 7. SimultaneousDoppler-catheter pressurerecordings in twopatients withmitral prostheses. Panel A:Left atrial pressure (LA) wasmeasured directly using trans-septal technique. Doppler andcatheter gradients are closelycorrelated. Panel B: Left atrialpressure was measured indi-rectly using pulmonary capil-lary wedge pressure (PCW).Note phase delay in pulmo-nary wedge Vwave (V), whichresulted in overestimation ofcatheter-derived maximal(max) and mean gradientscompared with correspondingDoppler-derived gradients.LV, left ventricular pressure.
:- ~ :.
1,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
EA
eters of the same size and length were used to ensureequal phase delay in each pressure tracing.As in native valve disease, the pressure gradient
alone may be insufficient to diagnose prostheticvalve dysfunction in certain clinical situations, suchas in patients with left ventricular dysfunction anddepressed cardiac output. Recent studies20,21 haveshown that the continuity equation using Dopplerflow velocity data can accurately determine aorticvalve area in patients with aortic stenosis. How-ever, this method has not been used routinely at our
institution for calculating aortic prosthetic orificearea because of, in part, uncertainty regarding theaccuracy of the Doppler flow velocity in aorticprostheses. The present study has clearly shownthat the Doppler measurement of flow velocity isaccurate in both aortic and mitral prostheses andthat further study of the Doppler determination ofprosthetic orifice area in a large patient populationappears indicated.The present study shows that the calculation of
prosthetic valve gradients by continuous wave Dopp-
SOW*~
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

514 Circulation Vol 80, No 3, September 1989
ler echocardiography provides quantitative hemo-dynamic information that is comparable in accuracyto that obtained with cardiac catheterization andthus can be substituted safely for cardiac catheter-ization for the measurement of prosthetic valvegradients. In conjunction with clinical and two-dimensional echocardiographic assessment, this tech-nique should further assist in the noninvasive assess-ment of prosthetic valve function.
References1. Effron MK, Popp RL: Two-dimensional echocardiographic
assessment of bioprosthetic valve dysfunction and infectiveendocarditis. JAm Coll Cardiol 1983;2:597-606
2. Grenadier E, Sahn DJ, Roche AHG, Valdes-Cruz LM,Copeland JG, Goldberg SJ, Allen HD: Detection of deterio-ration or infection of homograft and porcine xenograft bio-prosthetic valves in mitral and aortic positions by two-dimensional echocardiographic examination. J Am CollCardiol 1983;2:452-459
3. Kotler MN, Mintz GS, Panidis J, Morganroth J, Segal BL,Ross J: Noninvasive evaluation of normal and abnormalprosthetic valve function. JAm Coll Cardiol 1983;2:151-173
4. Currie PJ, Seward JB, Reeder GS, Vlietstra RE, BresnahanDR, Bresnahan JF, Smith HC, Hagler DJ, Tajik AJ:Continuous-wave Doppler echocardiographic assessment ofseverity of calcific aortic stenosis: A simultaneous Doppler-catheter correlative study in 100 adult patients. Circulation1985;71:1162-1 169
5. Currie PJ, Hagler DJ, Seward JB, Reeder GS, Fyfe DA,Bove AA, Tajik AJ: Instantaneous pressure gradient: Asimultaneous Doppler and dual catheter correlative study. JAm Coll Cardiol 1986;7:800-806
6. Sasson Z, Yock PG, Hatle LK, Alderman EL, Popp RL:Doppler echocardiographic determination of the pressuregradient in hypertrophic cardiomyopathy. JAm Coll Cardiol1988;11:752-756
7. Currie PJ, Seward JB, Chan K-L, Fyfe DA, Hagler DJ, MairDD, Reeder GS, Nishimura RA, Tajik AJ: Continuous waveDoppler determination of right ventricular pressure: A simul-taneous Doppler-catheterization study in 127 patients. JAmColl Cardiol 1985;6:750-756
8. Nishimura RA, Tajik AJ: Determination of left-sided pres-sure gradients by utilizing Doppler aortic and mitral regur-gitant signals: Validation by simultaneous dual catheter andDoppler studies. JAm Coll Cardiol 1988;11:317-321
9. Wilkins GT, Gillam LD, Kritzer GL, Levine RA, PalaciosIF, Weyman AE: Validation of continuous-wave Dopplerechocardiographic measurements of mitral and tricuspid
prosthetic valve gradients: A simultaneous Doppler-catheterstudy. Circulation 1986;74:786-795
10. Williams GA, Labovitz AJ: Doppler hemodynamic evalua-tion of prosthetic (Starr-Edwards and Bjork-Shiley) andbioprosthetic (Hancock and Carpentier-Edwards) cardiacvalves. Am J Cardiol 1985;56:325-332
11. Sagar KB, Wann LS, Paulsen WHJ, Romhilt DW: Dopplerechocardiographic evaluation of Hancock and Bjork-Shileyprosthetic valves. JAm Coll Cardiol 1986;7:681-687
12. Rothbart RM, Smucker ML, Gibson RS: Overestimation byDoppler echocardiography of pressure gradients across Starr-Edwards prosthetic valves in the aortic position. Am JCardiol 1988;61:475-476
13. Callahan MJ, Tajik AJ, Su-Fan Q, Bove AA: Validation ofinstantaneous pressure gradients measured by continuous-wave Doppler in experimentally induced aortic stenosis.AmJ Cardiol 1985;56:989-993
14. Carabello BA, Grossman W: Calculation of stenotic valveorifice area, in Grossman W (ed): Cardiac Catheterizationand Angiography, ed 3. Philadelphia, Lea & Febiger, 1986,pp 143-154
15. Hatle L, Angelsen B: Doppler Ultrasound in Cardiology:Physical Principles and Clinical Applications, ed 2. Phila-delphia, Lea & Febiger, 1985, pp 23-24
16. Teirstein PS, Yock PG, Popp RL: The accuracy of Dopplerultrasound measurement of pressure gradients across irreg-ular, dual, and tunnellike obstructions to blood flow. Circu-lation 1985;72:577-584
17. Yoganathan AP, Jones M, Sahn DJ, Ridgeway A, Jimoh A,Tamura T: Bernoulli gradient calculations for mechanicalprosthetic aortic valves: In vitro Doppler studies (abstract).Circulation 1986;74(suppl 2):II-391
18. Arabia FA, Talbot TL, Jones M, Clark RE: Simultaneous invitro maximum measured and Doppler derived pressuredifferences across prosthetic heart valves (abstract). Circu-lation 1987;76(suppl 4):IV-389
19. Schoenfeld MH, Palacios IF, Hutter AM Jr, Jacoby SS,Block PC: Underestimation of prosthetic mitral valve areas:Role of transseptal catheterization in avoiding unnecessaryrepeat mitral valve surgery. J Am Coll Cardiol 1985;5:1387-1392
20. Zoghbi WA, Farmer KL, Soto JG, Nelson JG, QuinonesMA: Accurate noninvasive quantification of stenotic aorticvalve area by Doppler echocardiography. Circulation 1986;73:452-459
21. Oh JK, Taliercio CP, Holmes DR Jr, Reeder GS, Bailey KR,Seward JB, Tajik AJ: Prediction of the severity of aorticstenosis by Doppler aortic valve area determination: Pro-spective Doppler-catheterization correlation in 100 patients.JAm Coll Cardiol 1988;11:1227-1234
KEY WORDS * echocardiography * catheterization * valvularregurgitation * valvular obstruction * prosthetic valves
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from

TajikD J Burstow, R A Nishimura, K R Bailey, G S Reeder, D R Holmes, Jr, J B Seward and A J
A simultaneous Doppler-catheter correlative study.Continuous wave Doppler echocardiographic measurement of prosthetic valve gradients.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1989 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.80.3.504
1989;80:504-514Circulation.
http://circ.ahajournals.org/content/80/3/504the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 9, 2018
http://circ.ahajournals.org/D
ownloaded from